Embed Size (px)
DESCRIPTION
Pathways Residential Care Journal is a quarterly newsletter written with our colleagues in assisted living (and independent and dementia care facilities) in mind. Recent articles discussed topics such as: "Bright Light Improves Dementia Symptoms"; "Interruptions Are Linked to Medication Errors"; "Pharmacists Improve Patient Outcomes"; "How Morphine Can Help in Heart Failure"; "Sitting is a Risk Factor for Death".
Citation preview
Issue 3
More Seniors Living Beyond 90
1.9 million Americans have reached the age of at least 90 years according to a recent report by the National Institute on Aging and the US Census Bureau. This is nearly 4.7% of the entire population.
Over the last 30 years, the size of this age group has tripled, creating changes in the landscape of elder housing and elder care. Nearly 20% of those 90 and older live in nursing homes. Senior living facilities are home not only to older, but sicker, residents now.
“Traditionally, the cutoff age for what is considered the ‘oldest old’ has been age 85,” Census Bureau demographer Wan He said. “But increasingly people are living longer and the older population itself is getting older. Given its rapid growth, the 90-and-older population merits a closer look.”
The complete report can be found at: www.census.gov/prod/2011pubs/acs-17.pdf.
What You Say Without SpeakingIt’s estimated that up to 93% of all communication is nonverbal. That means facial expressions, gestures and the way we stand all say something—of which we are often unaware.
For nearly 20 years medical schools have been required to teach communication skills, but, writes New York Times columnist Pauline Chen, few schools offer courses on facial expressions and body language, “despite a growing body of research suggesting that nonverbal communication may be as important as verbal communication.“
One of the most powerful tools we have is eye contact, and how much we are willing to give to residents. It tells them they are being listened to. Do you nod to let them know they have your full attention, or does it look like you are a million miles away while they talk to you?
Experts suggest healthcare professionals note their body language: Do you cross your arms, look away or make notes while residents are speaking? Or do you look engaged, touch their hands, and appear unrushed? Experts say nothing is more powerful than imagining yourself in the resident’s place to put things in perspective.
Pathways
Residential CareJournal
Pathways
Residential CareJournal
Pathways Residential Care Journal
Alzheimer’s Tracks Mapped
Surprising results of recent research show that Alzheimer’s disease (AD) seems to spread from one brain cell to the next. For many years researchers tried to unravel the mystery of how AD spreads. Did lesions pop up here and there throughout
the brain, or did it spread outward from the memory center where it first starts?
The solution to the question was mice. Their brains were injected with the abnormal human protein that causes AD. Researchers tracked the presence of the protein in the mice over the next two years. As researchers mapped it they saw that the protein spread outward along the same paths as in humans. Since human proteins could not spontaneously appear in isolated pockets of mouse brains, they could only arrive at other areas through spread from cell to cell.
This means that theoretically the disease could be stopped by halting transmission from cell to cell—maybe with an antibody that blocks the protein. The study results will have immediate implications for developing new treatments, according to the researchers working at Columbia and Harvard Universities. They imagine treatments for stopping the disease like treating cancer while in its early stages before it has spread.
“You matter because you are you. You matter to the last moment of your life, and we will do all we can, not only to help you die peacefully, but also to live until you die.”
-- Dame Cicely Saunders
Gentle Thoughts
Advance Health Care DirectivesA Gift to FamiliesAn advance health care directive tells your family and doctor what you want done if you can’t make decisions for yourself. Your family and doctor don’t have to guess what you would have wanted. What would be the highest priority? It might be to be pain free, or to not be on a ventilator, or to have everything done to keep you alive as long as possible. This isn’t just for older people, all adults should make one. After all, young people can be injured in accidents that leave them unable to speak.
Three PartsAn advance health care directive has three parts. In the first part you name a person to be your agent (and alternates in case the agent is not available). The agent can legally make health care decisions for you and is called a Durable Power of Attorney for Health Care. In the second part, you state in detail the treatments you would want, or would not want, and under what circumstances—things like feeding tubes, ventilators and what to do if your heart and breathing stop. In the third part you can say if you want to be an organ or tissue donor.
Choosing an AgentThe person you choose as an agent must be 18 years old, and someone who knows you well and who will honor your wishes, even if they are different from yours. A husband or wife is not automatically
recognized as a patient’s spokesperson in California. The agent may be a family member, a friend, or even an attorney, but caregivers in a facility cannot be agents for residents. Agents may choose a doctor, hospital, skilled facility or hospice for you. The agent may also accept or refuse treatments on your behalf, and consent to organ donation.
Making it LegalAn advance health care directive does not need to
continued on next page Advance Health Care Directives
Helping Neighbors on Life’s Journey
Power of MusicMusic is a powerful force that can stimulate strong emotions within us. Harnessing that power can benefit the seriously ill by improving their quality of life. In a 3-year study Sandi Curtis, a music therapy professor at Concordia University in Montreal, Canada, divided
university music therapy students and musicians in to pairs working with 371 participating terminally ill patients from 18 to 101 years old. Participants were seen for a single music therapy sessions from 15 to 60 minutes long with the goal of enhancing pain relief, relaxation, mood and quality of life.
“Our study showed how music therapy was effective in enhancing pain relief, comfort, relaxation, mood, confidence, resilience, life quality and well-being in patients,” said Curtis. The study was published in the journal Music and Medicine.
Helping neighbors on life’s journey for 35 years and counting...
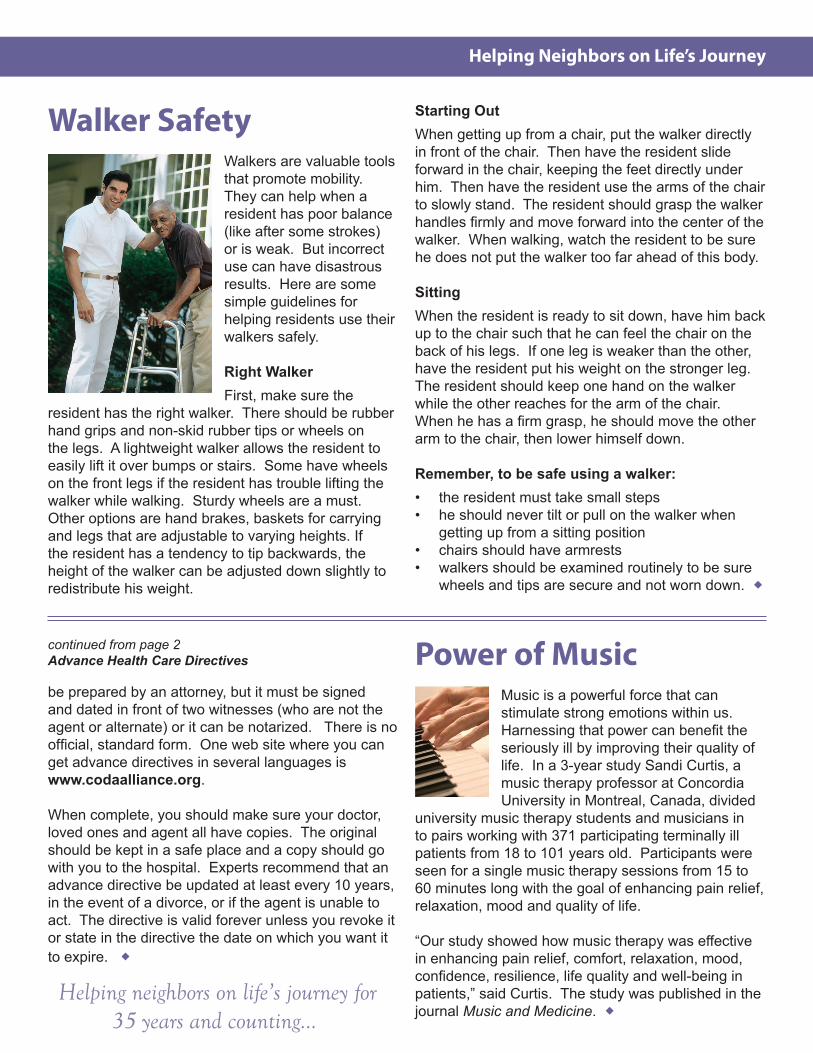
Walker Safety
Walkers are valuable tools that promote mobility. They can help when a resident has poor balance (like after some strokes) or is weak. But incorrect use can have disastrous results. Here are some simple guidelines for helping residents use their walkers safely.
Right WalkerFirst, make sure the
resident has the right walker. There should be rubber hand grips and non-skid rubber tips or wheels on the legs. A lightweight walker allows the resident to easily lift it over bumps or stairs. Some have wheels on the front legs if the resident has trouble lifting the walker while walking. Sturdy wheels are a must. Other options are hand brakes, baskets for carrying and legs that are adjustable to varying heights. If the resident has a tendency to tip backwards, the height of the walker can be adjusted down slightly to redistribute his weight.
Starting OutWhen getting up from a chair, put the walker directly in front of the chair. Then have the resident slide forward in the chair, keeping the feet directly under him. Then have the resident use the arms of the chair to slowly stand. The resident should grasp the walker handles firmly and move forward into the center of the walker. When walking, watch the resident to be sure he does not put the walker too far ahead of this body.
SittingWhen the resident is ready to sit down, have him back up to the chair such that he can feel the chair on the back of his legs. If one leg is weaker than the other, have the resident put his weight on the stronger leg. The resident should keep one hand on the walker while the other reaches for the arm of the chair. When he has a firm grasp, he should move the other arm to the chair, then lower himself down.
Remember, to be safe using a walker:• the resident must take small steps • he should never tilt or pull on the walker when
getting up from a sitting position• chairs should have armrests• walkers should be examined routinely to be sure
wheels and tips are secure and not worn down.
be prepared by an attorney, but it must be signed and dated in front of two witnesses (who are not the agent or alternate) or it can be notarized. There is no official, standard form. One web site where you can get advance directives in several languages is www.codaalliance.org.
When complete, you should make sure your doctor, loved ones and agent all have copies. The original should be kept in a safe place and a copy should go with you to the hospital. Experts recommend that an advance directive be updated at least every 10 years, in the event of a divorce, or if the agent is unable to act. The directive is valid forever unless you revoke it or state in the directive the date on which you want it to expire.
continued from page 2 Advance Health Care Directives
FAST Assessment for Dementia Ready for Hospice?
The FAST Scale is one good way to assess if someone with dementia may be ready for hospice. FAST stands for Functional Assessment Staging. This is a 7-step scale, with detailed sub-steps. A resident who reaches step 7A is usually appropriate for hospice if he also has at least one• Aspiration due to difficulty swallowing
of the following:
• Upper urinary tract infection (kidneys) • Sepsis (infection of the blood) • Multiple stage 3-4 pressure ulcers • Persistent fever • Weight loss of at least 10% in the last 6 months • Laboratory blood albumin level less than 2.5
FUNCTIONAL ASSESSMENT STAGING (FAST) SCALE 1. No difficulties; appears normal 2. Becoming increasingly forgetful 3. Decreased job functioning and unable to organize 4. Difficulty with complex tasks and some ADLs 5. Requires supervision and coaching with ADLs 6. Needs assistance with all ADLs and incontinent 7. A. Ability to speak limited to six words
B. Ability to speak limited to single word C. Loss of ambulation D. Unable to sit E. Unable to smile F. Unable to hold head up
TYPICAL TIME COURSE OF ALZHEIMER’S DISEASE (AD)
DIAGNOSIS: QUESTIONABlE MIlD MODERATE MOD-SEvERE SEvERE
FAST Stage 3 4 5 6 7
FAST Sub-stage A B C D E A B C D E F
Years: 0 7 to 9 10.5 13 to 19
Usual point of death is around Stage 7 C
Pathways Home Health & Hospice585 North Mary Avenue Sunnyvale, CA 94085-2905 1.888.755.7855 / www.pathwayshealth.org
NONPROFIT ORGU.S. POSTAGE
P A I DSUNNYvAlE, CAPERMIT NO. 172
Serving San Francisco, San Mateo, Santa Clara, Alameda & Western Contra Costa Counties from offices in Oakland, South San Francisco and Sunnyvale.
FAST Assessment for Dementia The FAST Scale is one good way to assess if someone with dementia may be ready for hospice. FAST stands for Functional Assessment Staging. This is a 7-step scale, with detailed sub-steps. A resident who reaches step 7A is usually appropriate for hospice if he also has at least one of the following:• Aspiration due to difficulty swallowing• Upper urinary tract infection (kidneys)• Sepsis (infection of the blood)• Multiple stage 3-4 pressure ulcers• Persistent fever• Weight loss of at least 10% in the last 6 months• laboratory blood albumin level less than 2.5
FUNCTIONAL ASSESSMENT STAGING (FAST) SCALE
1. No difficulties; appears normal (not on scale)2. Becoming increasingly forgetful (not on scale)3. Decreased job functioning and unable to organize 4. Difficulty with complex tasks and some ADls 5. Requires supervision and coaching with ADls 6. Needs assistance with all ADls and incontinent 7. A. Ability to speak limited to six words
B. Ability to speak limited to single word C. loss of ambulation D. Unable to sit E. Unable to smile F. Unable to hold head up
















![[20170216][Journal Club][Enhanced recovery pathways versus standard care after cystectomy][Chia-Ching, Chen]](https://img.pdfslide.us/doc/110x75/5a647abd7f8b9a52568b478b/20170216journal-clubenhanced-recovery-pathways-versus-standard-care-after.jpg)












