Embed Size (px)
Citation preview

Pathophysiology of acute pancreatitis and identification of steps having
potential for intervention in order to control severity
Moderator- Prof. Anoop SarayaSpeaker- Dr. Moka Praneeth

Contents
• Introduction
• Animal models
• Pathophysiology & clinical phases
• Pathogenesis & possible interventions at each step
• Nutrition
• Probiotics & Antibiotics
• Therapeutic trials

Introduction
• Pathogenesis of AP elusive despite significant advances in the last
25 years
• Upto 25% of patients suffer from a severe attack of acute
pancreatitis
• A complex cascade of immunological events not only affects the
pathogenesis but also the course of the disease

Animal models
• Cerulein (Hyperstimulating - CCK analog) model
• Obstructive (Ligating the pancreatic duct) model
• Duct perfusion (induced by antegrade and retrograde infusion of
Sodium taurocholate) model
• Closed (distal & proximal to junction of hepatopancreatic duct)
duodenal loop models
• Choline-deficient and Ethionine supplement diet → severe
hemorrhagic acute pancreatitis with changes in CNS, liver)models


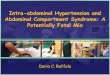
1st week 2nd weekHours 3rd-4th week
EARLY MIDDLEINITIAL LATE
Inappropriateactivation of
proteases
Necrosis
Microcirculatorydisorders
Progression ofnecrosis
Gut and biliarybacteria
Infection of necrosis
Altered intra-acinar protein traffic
Accumulation of trypsinogen in the interstitial space Macrophage
activation
PHASE
TIMING
MAJOREVENTS
? 19% 37%32% 12%DEATHS??
0 012% 28%
26%0%
0%5%
M.O.F.
InfectionCauses
R. Pezzilli, et al. Ospedali Italiani Chirurgia 2004; 10: 314-23. [1]
Pathophysiology and Clinical Phases of Acute Pancreatitis

ACUTE PANCREATITIS
TIME COURSE
0 12 24 36 48 60 72 84 96
hours from pain onset
ER presentation cytokine release organ failure



Cathepsin B blockade
Intravenous administration of Cathepsin B inhibitor, CA-074me (10
mg/kg) before induction of either secretagogue-elicited pancreatitis in
mice or duct infusion-elicited pancreatitis in rats markedly reduced the
extent of intrapancreatic trypsinogen activation and substantially
reduced the severity of both pancreatitis models
Van Acker GJ et al. Am J Physiol Gastrointest Liver Physiol. 2002

Trypsin activation and pH
Trypsinogen autoactivation requires an acidic pH and is enhanced in
the presence of Ca2+
The affinity of pancreatic trypsin inhibitor is greatest at a neutral pH
and is reduced at an acidic pH.
The generation of low-pH compartments within the acinar cell during
experimental pancreatitis may be important to trypsinogen activation
Figarella et al. Biol Chem Hoppe-Seyler 1988


Factors that determine the cellular fate of pancreatic acinar cell.


Pancreatic necrosis vs apoptosis
• Necrosis has classically been considered the major form of cell death in acute
pancreatitis , whereas apoptosis was suggested to mediate atrophy in the organ
• Severe acute pancreatitis (e.g., that induced by PD ligation in the opossum, by
choline-deficient and ethionine-supplemented diet in the mouse, and by
cerulein in the mouse) is associated primarily with necrosis, whereas mild acute
pancreatitis (e.g., that induced by PD ligation and by caerulein in the rat) is
associated primarily with apoptotic cell death

Apoptosis- affects severity
• Crambene (1-cyano 2-hydroxy 3-butene) administered 12 hours
before cerulein (in mice) results in a maximal time-dependent
pancreatic acinar cell apoptosis and reduces the severity of acute
pancreatitis maximally
Bhatia M et al. Biochem Biophys Res Commun. 1998

Inflammation
• Acinar cells are the site of onset of inflammatory cascade before the
innate immune response sets in
• NF-kB activation takes place in the acinar cells
• Nuclear translocation of NF-kB dimer p50/p65 causes transcription
of proinflammatory cytokines

Inflammation
• TNF-α is secreted by the acinar cells in cerulein model of acute
pancreatitis
• Pancreatic stellate cells, ductal cells and resident macrophages may
take part in the initial inflammatory activity

Pathophysiology of disease progression in Acute Pancreatitis

Innate immune response
• Neutrophils infiltrate the pancreas within 3 hours of initiating
experimental acute pancreatitis
• Neutrophils mediate their effects through MPO and proteases (eg:
elastase)
• Monocytes secrete IL-1, IL-6 and TNF-α
• IL-6 levels in the blood correlate with organ injury and severity of
pancreatitis in humans


Experimental Treatment of Acute Pancreatitis
More than 2,000 papers on the treatment of acute pancreatitis in
experimental models have been published in the last 10 years
About a half of these studies were carried out on edematous pancreatitis
Only a few of the substances tested in these studies have been applied in
clinical practice

Infliximab, a monoclonal TNF antibody, was tested in 100 rats randomly
assigned to 10 groups
In acute edematous pancreatitis and in severe necrotizing pancreatitis, the
drug significantly decreased serum amylase activity and the histopathologic
score
In severe necrotizing pancreatitis, it ameliorated both parenchymal and
fatty tissue necrosis of the pancreas
It also alleviated alveolar edema and ARDS-like pulmonary complications,
but this difference was not significant
Infliximab in Acute Pancreatitis
Oruc N, et al. Pancreas 2004; 28:E1-8. [26]

Targeting PAF – key molecule in murine models
• 290 patients with APACHE-2 score > 6
• Randomised to Lexipafant 100 mg/day i.v. × 7 days commenced within
72 hours of onset of symptoms
• Overall, 80/138 (58%) patients in the placebo group and 85/148 (57%) in
the lexipafant group developed one or more organ failures.
• The primary hypothesis was invalidated by the unexpected finding that
44% of patients had organ failure on entry into the study; only 39 (14%)
developed new organ failure.
• Deaths attributable to acute pancreatitis were not significantly different.
Johnson CD et al. Gut. 2001

Zou WG, et al. J Surg Res 2002; 103:121-6. (modified) [29]
0
20
40
60
80
100
IL-10 PlaceboN
ew o
rgan
fai
lure
(%
)
P NS
Villoria A, et al. Pancreatology 2003; 3:466. [30]
Interleukin-10 in Acute Pancreatitis
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8Days
Sur
viva
l (%
)
IL-10Untreated
P<0.05
Efficacy in experimental studyNo effect in humans

Neutrophil elastase
• 75 patients with acute pancreatitis were matched to 20 controls
• NE activity was assessed using venous blood samples obtained on
patient admission and after 1, 2 and 14 days.
• NE activity was higher overall in patients with predicted severe AP
than in those with predicted mild AP (p = 0.027).
• Patients with respiratory failure had higher NE activity than those
without (p = 0.0024).
Novovic S et al. Scand J Clin Lab Invest. 2013

Resveratrol-mechanisms
• Administration of resveratrol can inhibit NF-kB activity as well as
reduce the concentrations of TNF-alpha, IL-6 and IL-1.
• It can also scavenge reactive oxygen species that are capable of
extensive tissue damage.
• Furthermore, resveratrol also exhibits anti-apoptotic properties via
regulation of apoptotic mediators such as Bax, Bcl-2, and caspase-3.
• It prevents Calcium overload, improves microcirculation and
alleviates SAP-induced histopathological distortions in the pancreas.
Jha RK et al. Front Biosci (Schol Ed). 2010

Resveratrol in Acute Pancreatitis
To evaluate the protective and antioxidative effect of resveratrol, a
stilbene derivative, in acute pancreatitis induced by tert-butyl
hydroperoxide injection
Changes in pancreata were much less pronounced in the rats which
received resveratrol for 8 days prior to tert-butyl hydroperoxide
injection
In this way it seems that stilbene derivatives may prevent pancreatic
cells from undergoing structural changes during acute pancreatitis
experimentally induced in rats
Lawinski M, et al. Pancreas 2005; 31:43-7. [27]

Resveratrol-therapeutic effect
• 72 male Sprague-Dawley rats randomised into sham operation
group, SAP group and RESV-group
• Pancreatitis was induced by intraductal administration of 0.1 mL/kg
4% sodium taurocholate.
• RESV was given intravenously at a dose of 20 mg/kg body weight.
LI ZD et al. World J Gastroenterol. 2006

Resveratrol-therapeutic effect
• All animals were killed at 3, 6, 12 h after induction of the model.
• RESV’s protective effect aginst lipid peroxidation reduced cellular
oxidative damage, as reflected by lower serum amylase, less severe
pancreatic lesions, normal pancreatic MDA levels, as well as
diminished neutrophil infiltration in pancreas.
LI ZD et al. World J Gastroenterol. 2006

Treatment of Acute Pancreatitis with Protease
Inhibitors
10 RCTs (n = 1036) evaluating the effects of protease inhibitors (Aprotinin
275000-800000 Units/day i.v. – 4 studies and Gabexate 600-4000 mg/day
i.v. infusion – 6 studies) in acute pancreatitis
Treatment with protease inhibitors did not significantly reduce the mortality
rate from acute pancreatitis (pooled risk difference, -0.03).
Seta T, et al. Eur J Gastroenterol Hepatol 2004; 16:1287-93. [37]

Treatment of Acute Pancreatitis with Protease Inhibitors
Subgroup analyses showed that protease inhibitors significantly
reduced the mortality rate in patients with moderate to severe
pancreatitis (pooled risk difference, -0.07)
There was no significant difference between protease inhibitors and
placebo in the formation of pancreatic pseudocysts, intra-abdominal
abscesses and need of surgery
Seta T, et al. Eur J Gastroenterol Hepatol 2004; 16:1287-93.

Microcirculatory alterations
• 88 male sprague Dawley rats randomised to controls (n =18), mild
AP (n=18), moderate AP (n=18), severe AP (n = 34)
• Within each group, rats were studied 0.5, 3.0, or 6.0 hours after
induction of pancreatitis, with DRS
• Total hemoglobin content in the pancreas remained constant
in all groups.
Bassi et al. J Am Coll Surg. 1994

Microcirculatory alterations
• Hemoglobin oxygenation increased significantly in rats in the control
group and in rats with mild pancreatitis for the duration of the
experiment, but not in rats with moderate or severe pancreatitis.
• Rats with severe pancreatitis had a significant decrease in ISO2 six
hours after the induction of pancreatitis compared with baseline
values as well as rats in control group studied after 6 hours
Bassi et al. J Am Coll Surg. 1994

Microcirculatory alterations
• There was marked variability in IHb and ISO2 at different locations
within the same pancreas in rats with severe pancreatitis, which
was not observed in the control group or in the rats with mild or
moderate pancreatitis.
Bassi et al. J Am Coll Surg. 1994

Modulating microrheological changes
• In female rats, 10 μg/kg cerulein s.c. was administered and 2 hours
later, microcirculation was tested by laser Doppler flowmetry on the
tongue and after performing laparotomy on the small intestine,
liver and pancreas prior to terminal blood sampling.
• From blood samples hematological parameters, blood pH, lactate
concentration, erythrocyte deformability, osmoscan parameters
and erythrocyte aggregation were tested.
Szentkereszty Z. Clin Hemorheol Microcirc. 2013

Modulating microrheological changes
• Compared to normal control in acute pancreatitis group severe
deterioration was noted in tissue microcirculation together with
impaired erythrocyte deformability and enhanced aggregation,
accompanied by acidic pH and increasing lactate concentration
• Improvement was found when using flunixin (s.c.), pentoxifylline
(i.p.) or enoxaparin (s.c.).
Szentkereszty Z. Clin Hemorheol Microcirc. 2013

Modulating microrheological changes
• These drugs could partly improve the blood flux on the surface of
the investigated organs
• Flunixin had the most expressed improving effects on micro-
rheological parameters.
• The improving effect of pentoxifylline on micro-rheological
parameters was not obvious (RBC deformability did not improve
better than in the other treated groups)
Szentkereszty Z. Clin Hemorheol Microcirc. 2013

Early fluid resuscitation reduces morbidity among patients with acute pancreatitis
• A retrospective study
• Stratification into early (: receiving ≥ 1/3 of total 72-hour fluid
volume within 24 hours of presentation) (n=340) or late (n= 94)
resuscitation
• Early resuscitation was associated with decreased SIRS at 24 hours
(15% vs 32%), 48 hours and 72 hours, as well as reduced organ
failure (5% vs 10%) at 72 hours and a reduced length of hospital stay
Warndorff et al. Clin Gastroenterol Hepatol. 2011

Type of fluids to be administered- RL vs NS
• RCT of 40 patients
• The volumes of fluids administered during a 24 hour period were
similar among patients given goal-directed or standard fluid
resuscitation.
• Goal-directed resuscitation did not significantly reduce incidence of
SIRS, compared with standard resuscitation (11.8% vs 13.0%, P = .85)
or levels of CRP after 24 hours (P = .75).
• There was a significant reduction in SIRS after 24 hours among
subjects resuscitated with RL vs NS (84% reduction vs 0% ; P = .035)
• Administration of RL also reduced levels of CRP, compared with NS
(51.5 vs 104 mg/dL; P = .02). Wu Bu et al. Clin Gastroenterol Hepatol. 2011

Quantity of fluids to be given
• Prospective cohort study of 247 adults with acute pancreatitis
• Administration of >4.1 l during the initial 24 h was significantly and
independently associated with persistent OF, acute collections, respiratory
insufficiency, and renal insufficiency.
• Administration of <3.1 l during the initial 24 h was not associated with OF, local
complications, or mortality.
• Patients who received between 3.1 and 4.1 l during the initial 24 h had an
excellent outcome.
Caution: Continuous monitoring should be done and cardiovascular and
renal morbidities should be taken into account
de Madaria et al. Am J Gastroenterol. 2011

September 1st, 2013
September 7th, 2013
October 26th, 2013
The Prevention of Infection of the Necrosis

Nutrition - Rationale
Hyper metabolic state
Total energy expenditure 1.5 x resting energy requirement
Nutrition depletion
Starvation
Preexisting protein-calorie malnutrition & micronutrient
deficiency
Crit care Med 1991;19:484-90; J parenter Enter Nutr 1989;13:26-29.

Parenteral Nutrition
Rationale against :
Pancreatic rest Poorly defined
Increased risk of sepsis Gut atrophy - increased bacterial translocation Hyperglycemia
Greater costs

Nutrition – who needs it?
Mild AP
70-80% recover within 4-7 days
Moderate to severe AP
– Ranson score > 3
– APACHE II > 8
– Necrotic pancreas
– Organ failure
Windsor et al. Gut 1998,42:431-35;
Kalfatentzos et al. Br J Surg 1997,84:1665-69

Parenteral Nutrition
Nine uncontrolled retrospective studies
Safe, well tolerated with few complications
No impact on the outcome

TPN
Prospective randomized controlled trial
54
TPN IV F
Duration of hospital stay 16 10
Line sepsis 10 1
Sax et al. Am J Surg 1987,153:117-22Sax et al. Am J Surg 1987,153:117-22

Enteral feeding vs Total parenteral nutrition
6 RCTs of patients with APACHE-2 score ≥ 8
Randomised to TEN vs TPN
Compared with TPN, EN was associated with a significantly lower incidence of:
pancreatic infection complications (P < .001), MOF (P = .003), surgical interventions (P < .001), and mortality (P = .167).
There was no statistic significance in non-pancreatitis-related complications (P = .017).
However, EN had a significantly higher incidence of non-infection-related complications (RR = 2.697, 95% CI 1.947∼3.735, P = .994).
Heming Quan et al. Gastroenterol Res Pract. 2011

Early Naso-Gastric vs. Naso-Jejunal Feeding
in Severe Acute Pancreatitis – meta-analysis
3 RCTs involving a total of 157 patients of predicted severe acute pancreatitis
82 were randomized to NG feeding vs 75 to NJ feeding
Comparable demographics between both the groups
No significant differences in:
the incidence of mortality (RR = 0.69, 95% CI: 0.37 to 1.29, P = 0.25); tracheal aspiration (RR = 0.46, 95% CI: 0.14 to 1.53, P = 0.20); diarrhea (RR = 1.43, 95% CI: 0.59 to 3.45, P = 0.43); exacerbation of pain (RR = 0.94, 95% CI: 0.32 to 2.70, P = 0.90); and meeting energy balance (RR = 1.00, 95% CI: 0.92 to 1.09, P = 0.97) between the two groups.
NG feeding was safe and well-tolerated as compared with NJ feeding
Y Chang et al. Critical Care. 2013


Evolution in Nutrition
Fasting
TPN is better
Early jejunal feeding is safe
Early jejunal feeding is superior
Gastric feeding is as good as jejunal feeding
Sax et al. Am J Surg 1987,153:117-22

Glutamine supplementation
12 RCTs of 505 patients with acute pancreatitis
Glutamine supplementation resulted in a significantly reduced risk of
mortality (RR 0.30; 95% CI, 0.15 to 0.60; P < 0.001) and total infectious
complications (RR 0.58; 95% CI, 0.39 to 0.87; P = 0.009) but not length
of hospital stay (MD -1.35; 95% CI, -3.25 to 0.56, P = 0.17).
In the subgroup analyses, only patients who received parenteral
nutrition and those who received glutamine in combination with other
immunonutrients demonstrated a statistically significant benefit in
terms of all the studied outcomes.
Asrani et al. Pancreatology. 2013

Polyunsaturated Fatty Acids in Acute Pancreatitis
0
20
40
60
80
100
IL-10 values(pg/mL)
Urine output(mL)
Respiratorydysfunction (%)
Fish oil Placebo
P<0.05
P<0.01
P<0.05
0
20
40
60
80
100
Lenght ofhospitalization
(days)
Jejunal feeding(days)
New complications(%)
Fish oil Placebo
P<0.05 P<0.05
P NS
Foitzik T, et al. JPEN 2002; 26:351-6. [31] Lasztity N, et al. Clin Nutr 2005; 24:198-205. [32]
Efficacy in experimental study …… and in humans

Probiotics in severe acute pancreatitis (PROPATRIA)
298 patients with predicted Severe acute pancreatitis were
randomly assigned within 72 hours of onset of symptoms
to receive a multispecies probiotic (n=153) or placebo
(n=145) given enterally BD for 28 days
Groups comparable at baseline in terms of patient’s
characteristics and disease severity
Infectious complications occurred in 46 (30%) patients in
the probiotics group and 41 (28%) of those in the placebo
group..

Probiotics in severe acute pancreatitis (PROPATRIA)
24 (16%) patients in the probiotics group died,
compared with nine (6%) in the placebo group. 9
patients in the probiotics group developed bowel
ischaemia (8 with fatal outcome), compared with none
in the placebo group (p=0.004).
In patients with predicted severe acute pancreatitis,
probiotic prophylaxis with this combination of probiotic
strains did not reduce the risk of infectious
complications and was associated with an increased risk
of mortality

Prophylactic antibiotics in severe acute pancreatitis
Early studies in 1970’s looked at all acute pancreatitis (mild to
severe), also used antibiotics now known to have poor pancreatic
penetrance, showed no benefit for antibiotic prophylaxis
Newer studies have looked at only severe pancreatitis, with drugs
now known to have good bioavailability in viable pancreatic tissue
tissue.

Pooling the Data:
Cochrane Review 2003:
4 studies examined, looking at prophylactic antibiotics in CTdiagnosed necrotizing pancreatitis. (Pederzoli 1993, Saino 1995, Schwarz 1997, Nordback 2001)
Conclusions:
Mortality advantage with Abx: (6/109 pts vs 18/109 pts, p=0.02)
Infected pancreatitis advantage with Abx: (23/109 pts vs 35/109 pts,
p=0.04)
No significant difference for extra-pancreatic infections, operative
interventions

The full results of the international meropenem study…
Dellinger et al, 2007:
Prospective, Double-Blinded RCT
100 pts, 50 in control (placebo), vs 50 in treatment group (meropenem)
Administration of study drug < 120 hrs after onset of sx
CT-proven pancreatic necrosis >30%, OR Balthazar Grade E on CT with
CRP >120 or MOD >2

The full results of the international meropenem study…
Dellinger et al, 2007:
Pancreatic/peripancreatic infection: Meropenem: n = 9/50 (18%) vs
Placebo: n = 6/50 (12%). (p=0.401)
Time to Onset of Infection: Meropenem: 21 days, vs Placebo: 21 days
Operative/Percutaneous Intervention: Meropenem: 13/50 (26%), vs
Placebo: 10/50 (20%). (p=0.476)
Non-Pancreatic Infections: Meropenem: 16/50 (32%), vs Placebo: 24/50
(48%). (p<0.20)
Mortality: Meropenem: 10/50 (20%), vs Placebo: 9/50 (18%)

Antibiotic therapy for prophylaxis against infection of pancreatic (CT-proven) necrosis
in acute pancreatitis 404 patients from 7 RCTs
Conclusions:
Antibiotic vs control: No significant differences in mortality (8.4 vs 14.4%), infected pancreatic necrosis (19.7 vs 24.4%), nonpancreatic infections (23.7 vs 36%), operative interventions
Beta-Lactam vs control: No significant difference in mortality (9.4% vs 15%), infected pancreatic necrosis (16.8 vs 24.2%), nonpancreatic infections (21 vs 32.5%), operative interventions
Imipenem vs control: No significant difference in mortality, infected pancreatic necrosis, operative intervention but there was Significant difference in infections overall (25.6% vs 52.4%, p=0.02)
Villatoro E, Bassi C, Larvin M. Cochrane Database of Systematic Reviews 2010, Issue 5.

Antibiotic prophylaxis in severe acute pancreatitis
No reduced risk of mortality, infection of necrotic pancreas, operative interventions
Studies are underpowered, heterogeneous in inclusion
criteria/treatment type/duration.
Trends do exist but are non-statistically significant
Potential for production of antibiotic resistant
organisms, fungal infection
While no definite increase in mortality, studies are small
Known increased mortality in resistant infection in VAP, bacteremia

Goals of Treatment
Limit systemic injury support and resuscitation – effective decrease pancreatic secretion – ineffective /
harmful? inhibit inflammatory mediators – (in) effective ? inhibit circulating trypsin – ineffective (too late)
Prevent necrosis – how?
Prevent infection antibiotics (imipenem and ciprofloxacin) – probably
ineffective in necrotic pancreatitis Probiotics- harmful Enteral nutrition

A Critical Appraisal of the Clinical Trials in Acute
Pancreatitis
ColipaseElastase
ChymotrypsinPhospholipase A2
Xanthynedehydrogenase
KallycreinC3aC5a
PlasminogenXIIa Factor
Systemic circulation
Alfa2 + TrypsinAlfa2-M
RESLiver
SpleenBone marrow
Nodes
Clearance
ProcolipaseProelastase
ChymotrypsinogenProphospholipase A2
Xanthynedehydrogenase
ProkallycreinC3C5PlasminogenXII Factor
Kininogens
Kinins
Trypsinogen
Trypsin
Trypsin
PSTI + TrypsinPSTI
Alfa1-AT + TrypsinAlfa1-AT
MesotrypsinEnzyme Y
Several steps may have to be blocked at the same time and this may be achieved by using combinations of several drugs at the same time or by the multiple actions of a single drug
Norman J. Am J Surg 1998; 175:76-83. (modified) [2]
Acute Pancreatitis
Complications: • Vascular leakage• Hypovolemia• Shock• ARDS• Acute renal tubular necrosis
IL-1 TNF
N.O. PAF
IL-6IL-8
Other leucocyte products
Oxygen radicalsElastaseIFN-α,γIL-10IL-2

Designing Future Clinical Trials in Acute Pancreatitis
Mason J, Siriwardena AK. Pancreatology 2005; 5:113-5. [33]
Therapeutic trials need to record the time from onset of symptoms to intervention
There is the need of using widely accepted prognostic indices to categorize the severity of acute pancreatitis
There is the need for relevant and interpretable end-points: Mortality is important but more work is necessary in developing patient
outcomes Good alternatives include the measurement of permanent target organ
damage, disability, quality of life, pain scores, category of intervention, surgery, in-patient stay and return to work
There is the need of including patients with a single etiology of acute pancreatitis, or at least only patients with a predominant etiology of the disease in the specific country

Conclusion
Knowing the various steps of pathophysiology of acute pancreatitis will
help in designing new therapeutic trials and in finding new therapeutic
targets
Adequate hydration, early enteral feeding definitely reduce the severity
of acute pancreatitis

Thank you