Embed Size (px)
Citation preview
12/9/2009
1
Pathophysiology:Heart Failure
Mat Maurer, MDAssociate Professor of Clinical Medicine
ObjectivesAt the conclusion of this seminar, learners will be able to:1. Define heart failure as a clinical syndrome2 Define and employ the terms preload afterload contractilty remodeling2. Define and employ the terms preload, afterload, contractilty, remodeling,
diastolic dysfunction, compliance, stiffness and capacitance.3. Describe the classic pathophysiologic steps in the development of heart
failure. 4. Delineate four basic mechanisms underlying the development of heart
failure5. Interpret pressure volume loops / Starling curves and identify contributing
mechanisms for heart failure statemechanisms for heart failure state.6. Understand the common methods employed for classifying patients with
heart failure.7. Employ the classes and stages of heart failure in describing a clinical
scenario
12/9/2009
2
Heart Failure
• Not a disease• Not a disease• A syndrome
– From "syn“ meaning "together“ and "dromos" meaning "a running“.
– A group of signs and symptoms that occur together d h t i ti l b litand characterize a particular abnormality.
• Diverse etiologies• Several mechanisms
Heart Failure: Definitions
• An inability of the heart to pump blood at a sufficient rate to meet the metabolic demands of the body (e.g. oxygen and cell nutrients) at rest and during effort or to do so only if the cardiac filling pressures are abnormally high.
• A complex clinical syndrome characterized by abnormalities in cardiac function and neurohormonal regulation, which are accompanied by effort intolerance, fluid retention and a p y ,reduced longevity
• A complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood.
12/9/2009
3
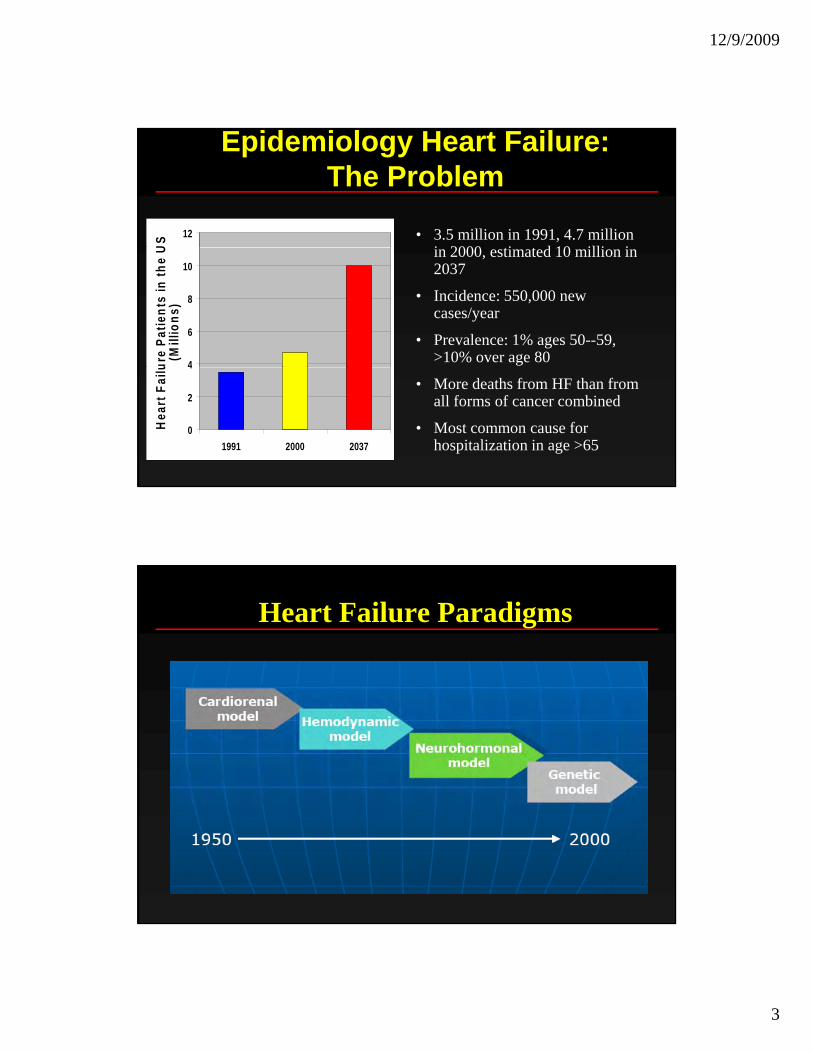
Epidemiology Heart Failure: The Problem
12
US • 3.5 million in 1991, 4.7 million
i 2000 ti t d 10 illi i
4
6
8
10
ure
Patie
nts
in th
e U
(Mill
ions
)
in 2000, estimated 10 million in 2037
• Incidence: 550,000 new cases/year
• Prevalence: 1% ages 50--59, >10% over age 80
0
2
4
1991 2000 2037
Hea
rt F
ailu
• More deaths from HF than from all forms of cancer combined
• Most common cause for hospitalization in age >65
Heart Failure Paradigms
12/9/2009
4
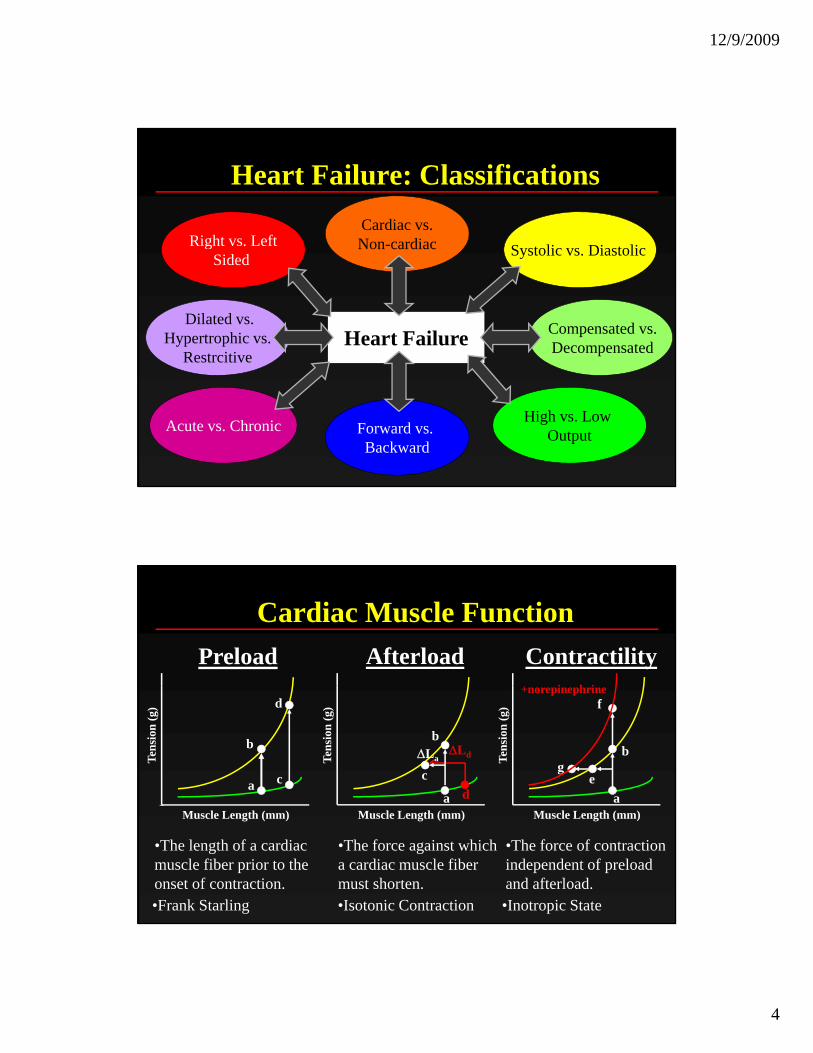
Heart Failure: Classifications
S t li Di t liRight vs. LeftCardiac vs.Non-cardiac
Heart Failure
Systolic vs. Diastolic gSided
Non cardiac
Dilated vs.Hypertrophic vs.
Restrcitive
Compensated vs.Decompensated
High vs. Low OutputAcute vs. Chronic Forward vs.
Backward
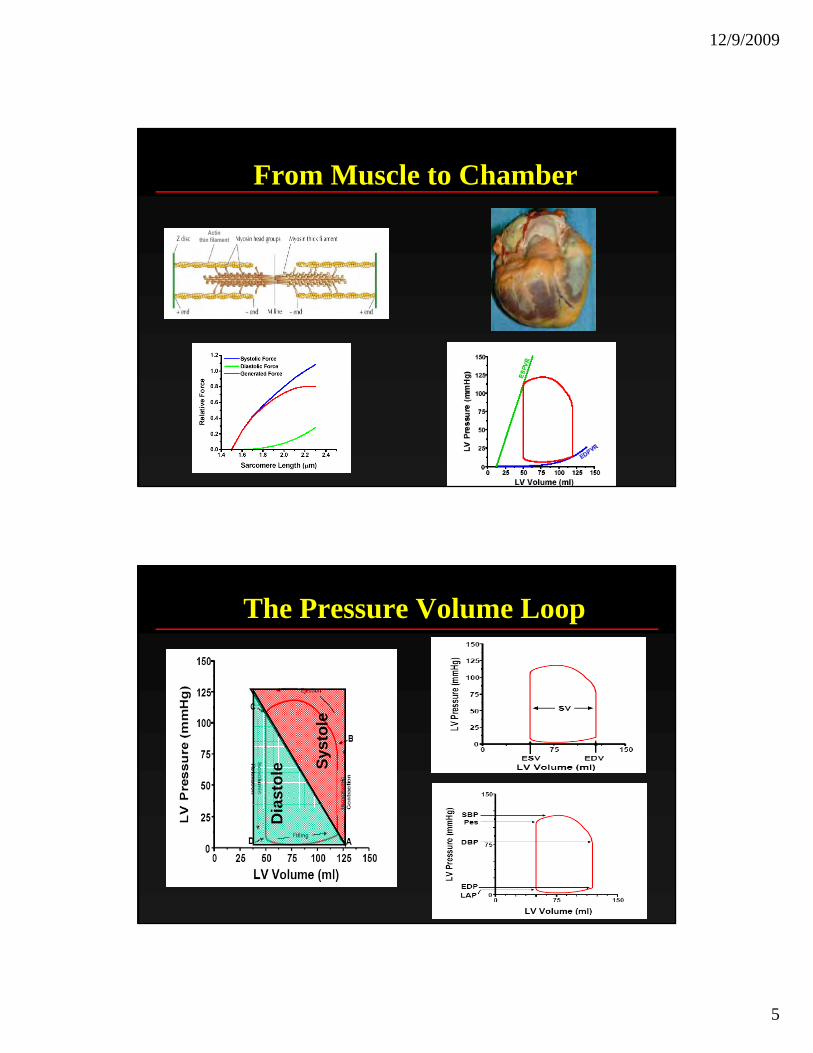
Cardiac Muscle FunctionPreload Afterload Contractility
i i
Tens
ion
(g)
b
a c
d
Tens
ion
(g)
d
ΔLd Tens
ion
(g)
a
g
f
b
e
+norepinephrine
a
b
c ΔLa
•The length of a cardiacmuscle fiber prior to theonset of contraction.
Muscle Length (mm) Muscle Length (mm)
•The force against whicha cardiac muscle fiber must shorten.
Muscle Length (mm)
•The force of contractionindependent of preloadand afterload.
•Frank Starling •Isotonic Contraction •Inotropic State
12/9/2009
5
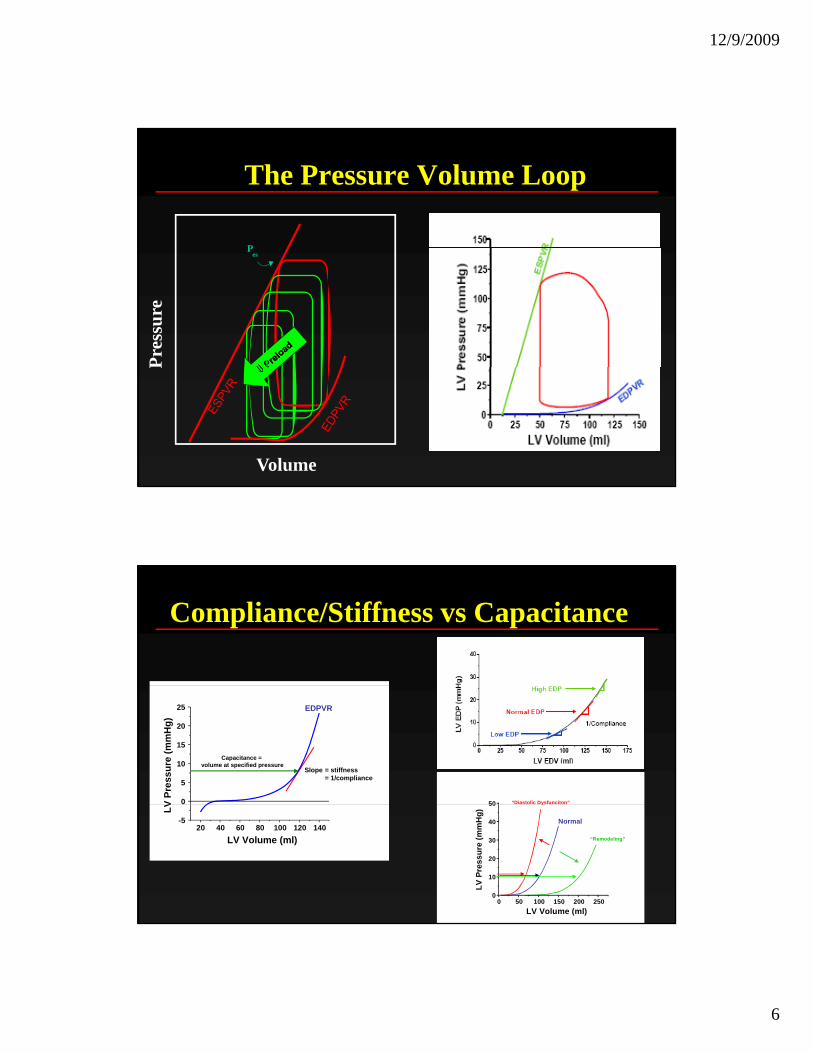
From Muscle to Chamber
The Pressure Volume Loop
Syst
ole
asto
leD
ia
12/9/2009
6
The Pressure Volume Loop
P
Pres
sure
esP
Volume
P
Compliance/Stiffness vs Capacitance
0
5
10
15
20
25
V Pr
essu
re (m
mH
g)
Slope = stiffness= 1/compliance
Capacitance = volume at specified pressure
EDPVR
50 “Diastolic Dysfunciton”
20 40 60 80 100 120 140-5
LV Volume (ml)
LV
0 50 100 150 200 2500
10
20
30
40
50
LV Volume (ml)
LV P
ress
ure
(mm
Hg)
Normal
y
“Remodeling”
12/9/2009
7
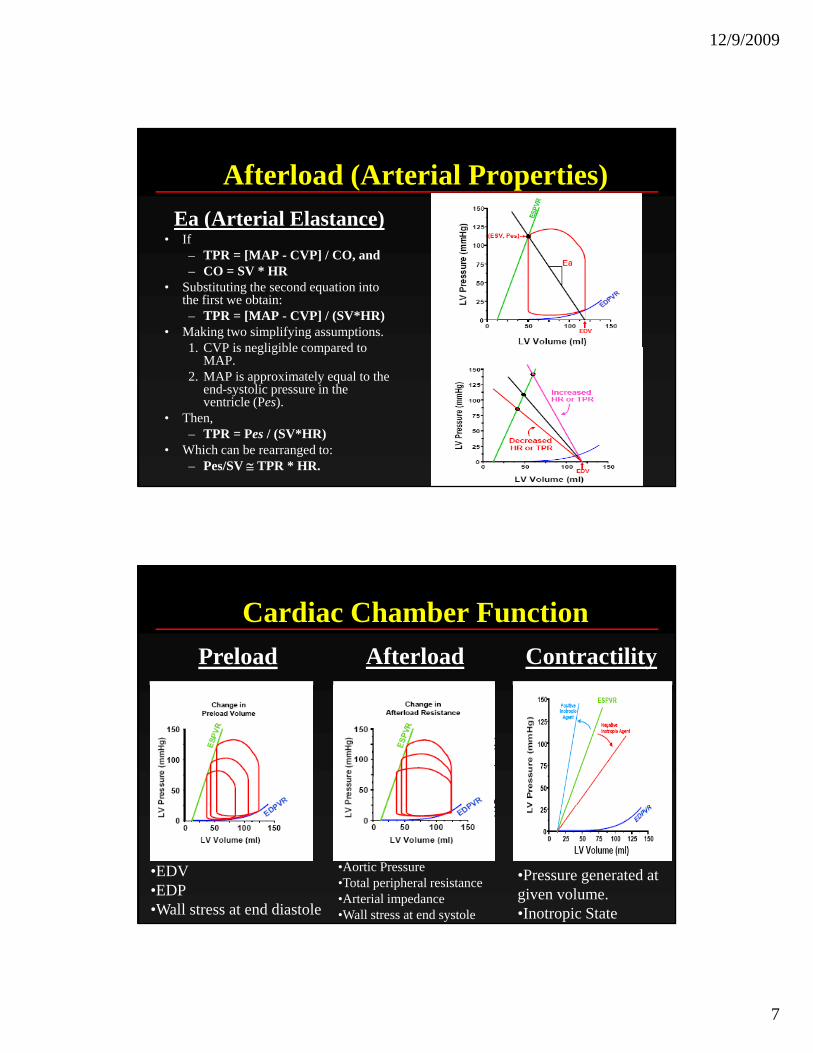
Afterload (Arterial Properties)Ea (Arterial Elastance)
• If – TPR = [MAP - CVP] / CO, and – CO = SV * HR
• Substituting the second equation into the first we obtain: – TPR = [MAP - CVP] / (SV*HR)
• Making two simplifying assumptions. 1. CVP is negligible compared to
MAP.2. MAP is approximately equal to the
end-systolic pressure in the ventricle (Pes).
• Then,– TPR = Pes / (SV*HR)
• Which can be rearranged to: – Pes/SV ≅ TPR * HR.
Cardiac Chamber FunctionPreload Afterload Contractility
•EDV•EDP•Wall stress at end diastole
•Aortic Pressure•Total peripheral resistance•Arterial impedance•Wall stress at end systole
•Pressure generated at given volume. •Inotropic State
12/9/2009
8
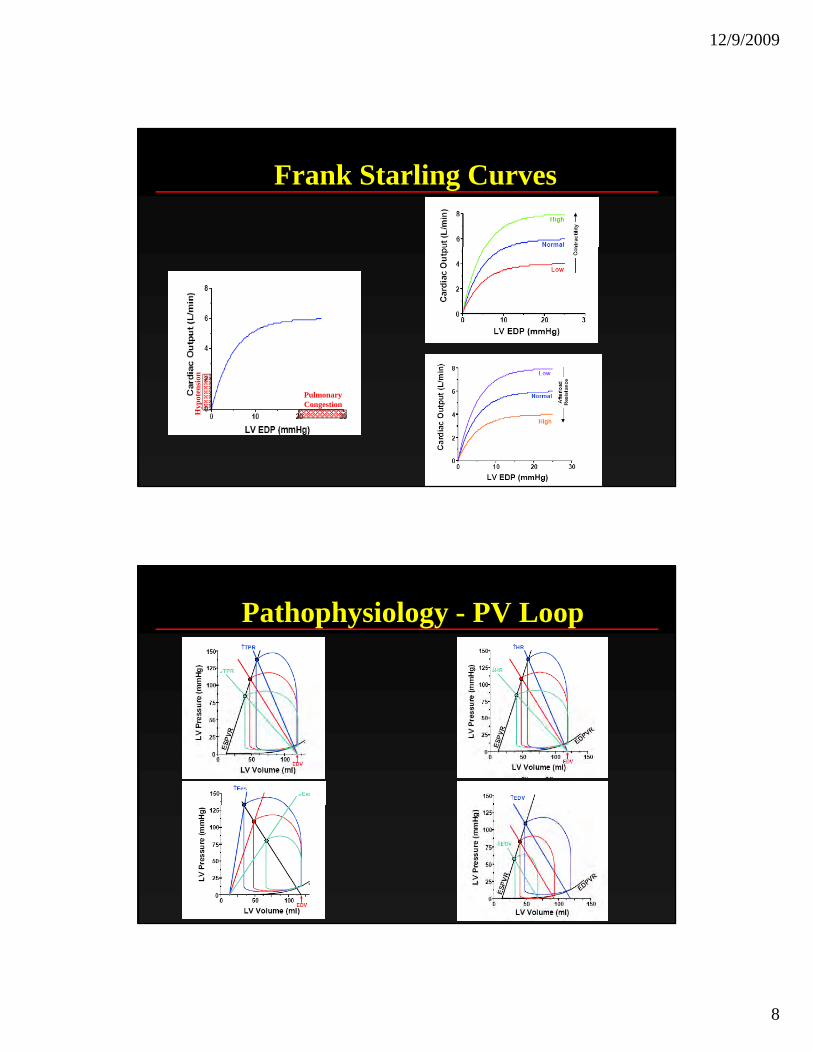
Frank Starling Curves
PulmonaryCongestion
Hyp
oten
sion
Pathophysiology - PV Loop
12/9/2009
9
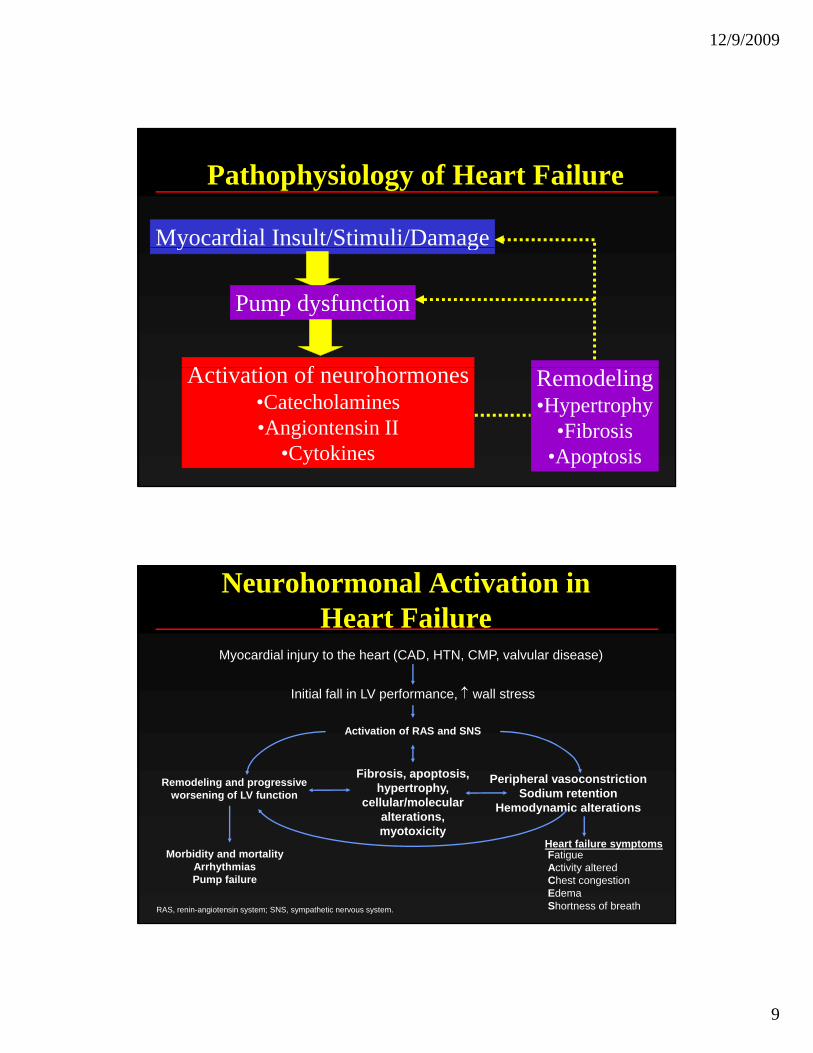
Pathophysiology of Heart Failure
Myocardial Insult/Stimuli/Damagey g
Pump dysfunction
A i i f hActivation of neurohormones•Catecholamines•Angiontensin II
•Cytokines
Remodeling•Hypertrophy
•Fibrosis•Apoptosis
Myocardial injury to the heart (CAD, HTN, CMP, valvular disease)
Neurohormonal Activation in Heart Failure
Initial fall in LV performance, ↑ wall stress
Peripheral vasoconstrictionSodium retention
H d i lt ti
Remodeling and progressiveworsening of LV function
Activation of RAS and SNS
Fibrosis, apoptosis,hypertrophy,
cellular/molecular
RAS, renin-angiotensin system; SNS, sympathetic nervous system.
Heart failure symptomsFatigueActivity altered Chest congestionEdemaShortness of breath
Morbidity and mortalityArrhythmiasPump failure
Hemodynamic alterationscellular/molecular alterations,myotoxicity
12/9/2009
10
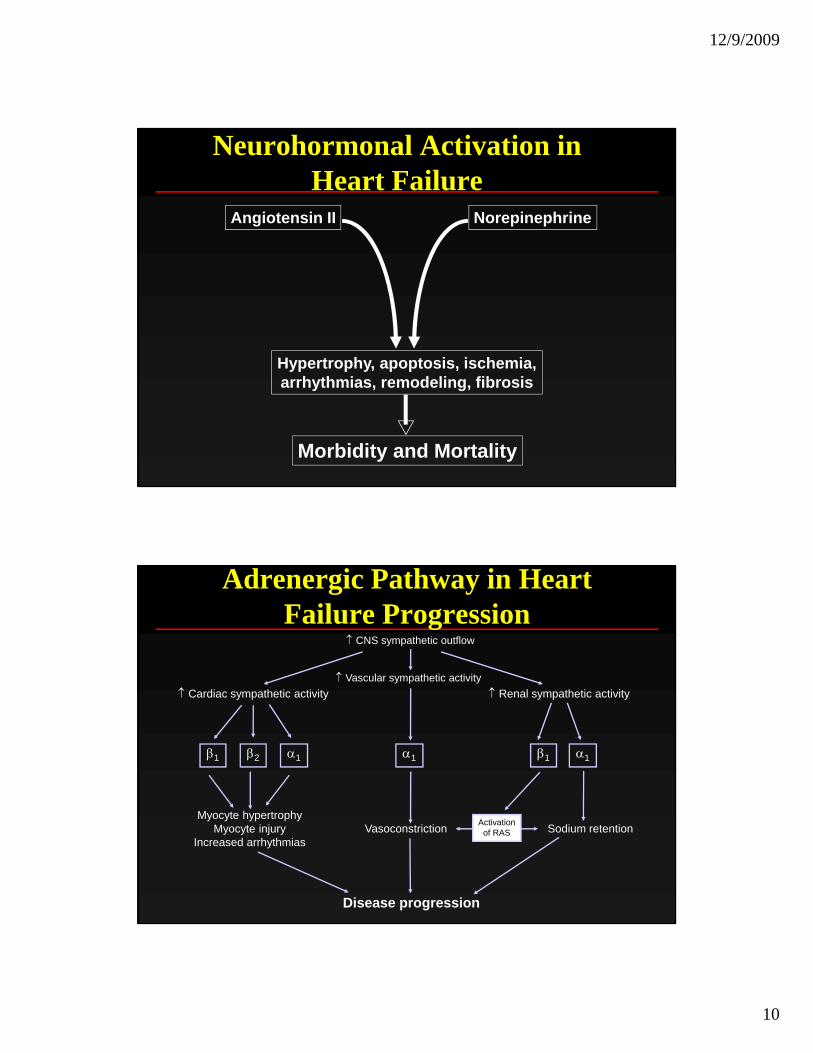
Neurohormonal Activation in Heart Failure
Angiotensin II Norepinephrine
Hypertrophy, apoptosis, ischemia,Hypertrophy, apoptosis, ischemia,arrhythmias, remodeling, fibrosis
Morbidity and Mortality
↑ CNS sympathetic outflow
↑ Vascular sympathetic activity
Adrenergic Pathway in Heart Failure Progression
↑ Cardiac sympathetic activity ↑ Renal sympathetic activity
α1β1β1 β2 α1 α1
Sodium retentionMyocyte hypertrophy
Myocyte injuryIncreased arrhythmias
Disease progression
Vasoconstriction Activationof RAS
12/9/2009
11
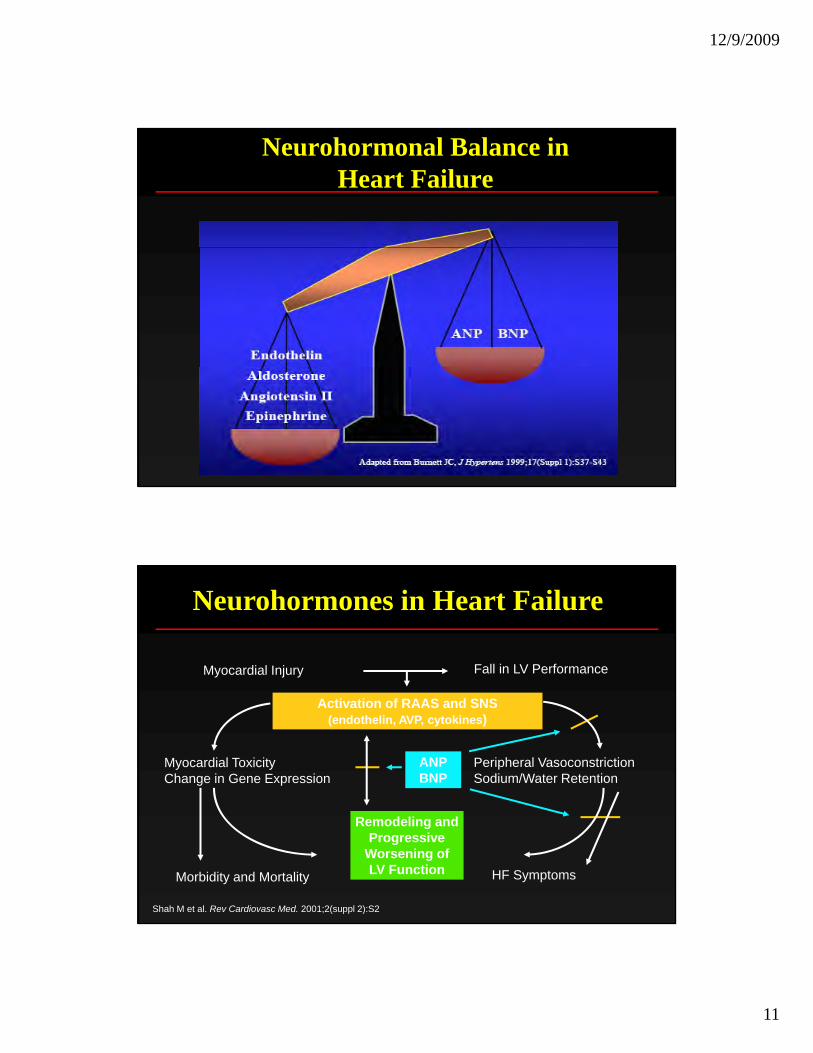
Neurohormonal Balance in Heart Failure
Myocardial Injury Fall in LV Performance
Neurohormones in Heart Failure
ANPBNP
Activation of RAAS and SNS(endothelin, AVP, cytokines)
Myocardial ToxicityChange in Gene Expression
Peripheral Vasoconstriction Sodium/Water Retention
HF SymptomsMorbidity and Mortality
Remodeling andProgressive
Worsening ofLV Function
Shah M et al. Rev Cardiovasc Med. 2001;2(suppl 2):S2
12/9/2009
12
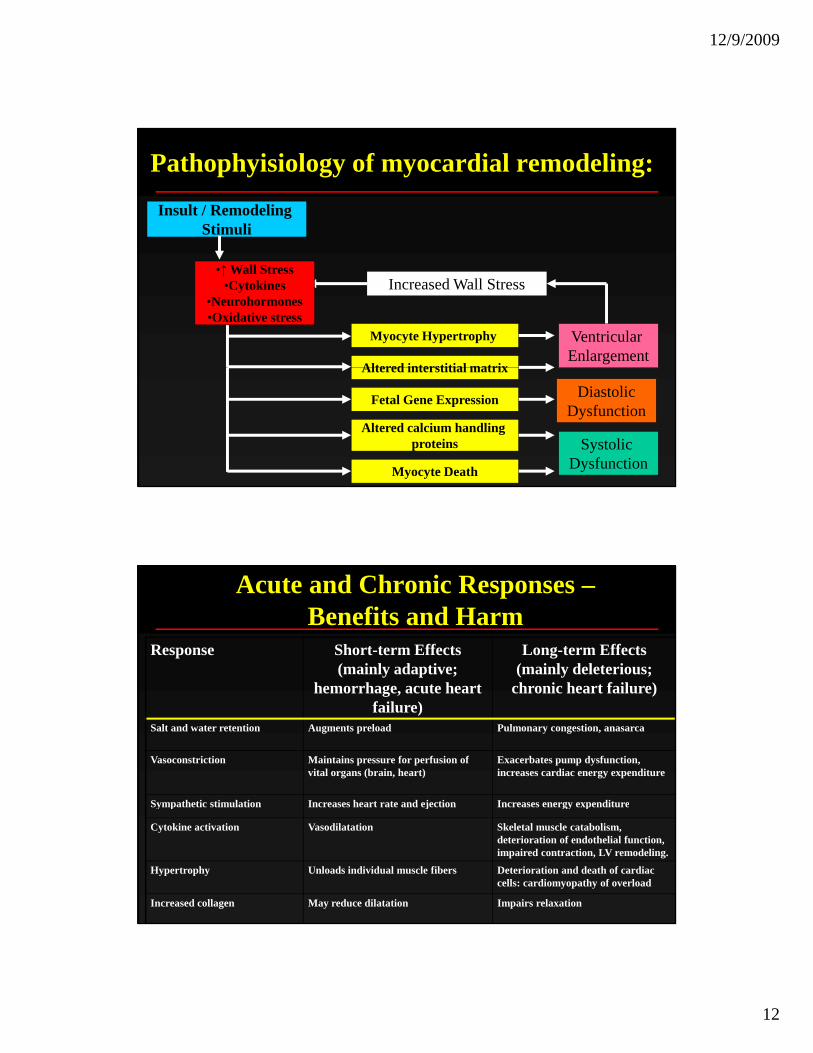
Pathophyisiology of myocardial remodeling:
Insult / Remodeling Stimuli
Myocyte Hypertrophy
Altered interstitial matrix
Ventricular Enlargement
Increased Wall Stress•↑ Wall Stress
•Cytokines•Neurohormones•Oxidative stress
Altered interstitial matrix
Fetal Gene Expression
Altered calcium handling proteins
Myocyte Death
Systolic Dysfunction
DiastolicDysfunction
Response Short-term Effects (mainly adaptive;
h h t h t
Long-term Effects (mainly deleterious; h i h t f il )
Acute and Chronic Responses –Benefits and Harm
hemorrhage, acute heart failure)
chronic heart failure)
Salt and water retention Augments preload Pulmonary congestion, anasarca
Vasoconstriction Maintains pressure for perfusion of vital organs (brain, heart)
Exacerbates pump dysfunction, increases cardiac energy expenditure
Sympathetic stimulation Increases heart rate and ejection Increases energy expenditureSympathetic stimulation Increases heart rate and ejection Increases energy expenditure
Cytokine activation Vasodilatation Skeletal muscle catabolism, deterioration of endothelial function, impaired contraction, LV remodeling.
Hypertrophy Unloads individual muscle fibers Deterioration and death of cardiac cells: cardiomyopathy of overload
Increased collagen May reduce dilatation Impairs relaxation
12/9/2009
13
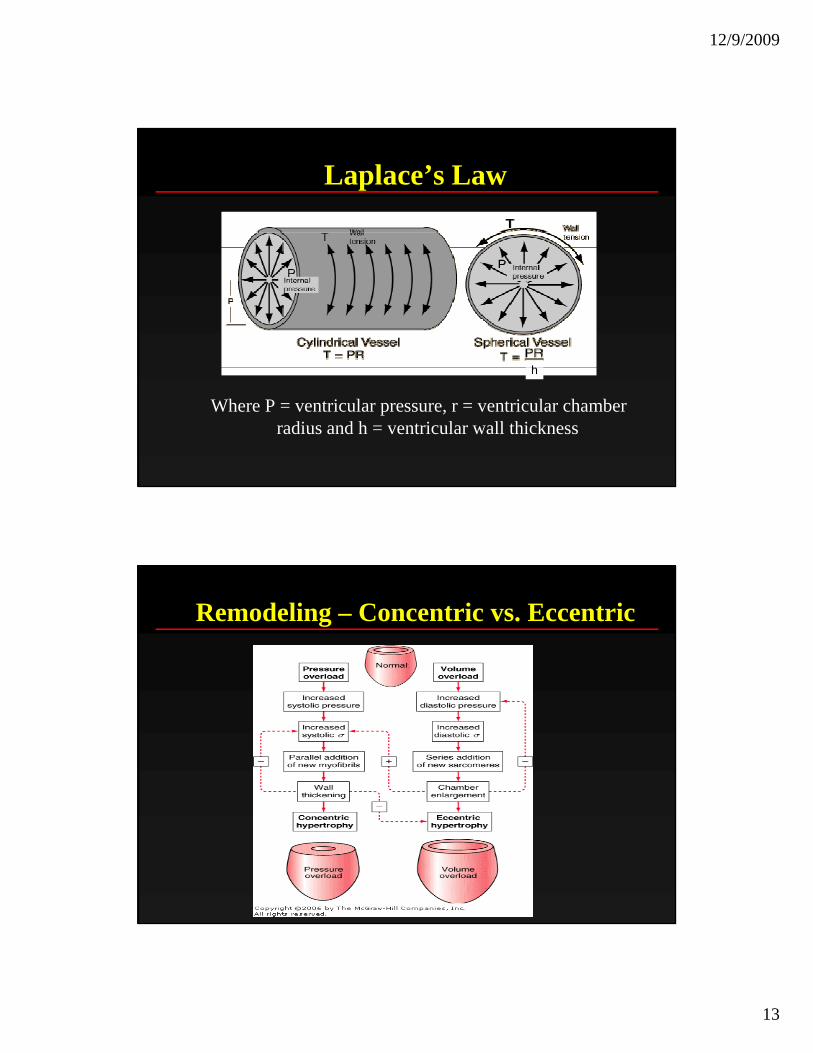
Laplace’s Law
h
Where P = ventricular pressure, r = ventricular chamber radius and h = ventricular wall thickness
h
Remodeling – Concentric vs. Eccentric
12/9/2009
14
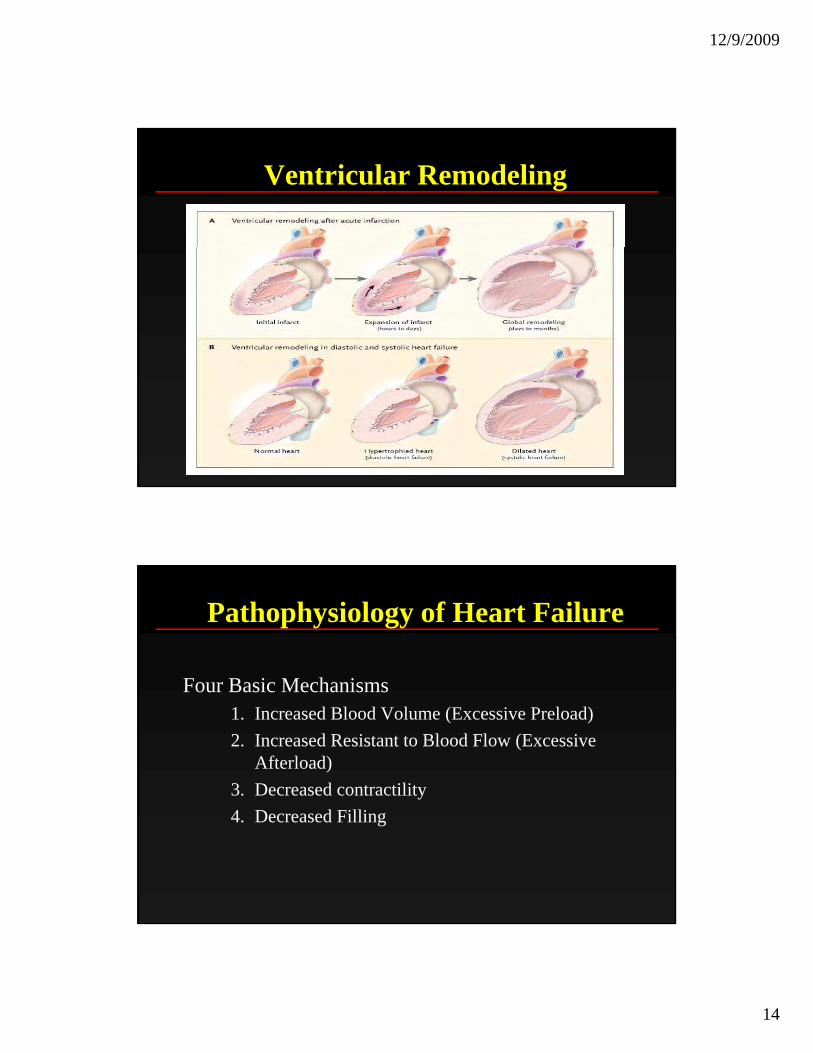
Ventricular Remodeling
Pathophysiology of Heart Failure
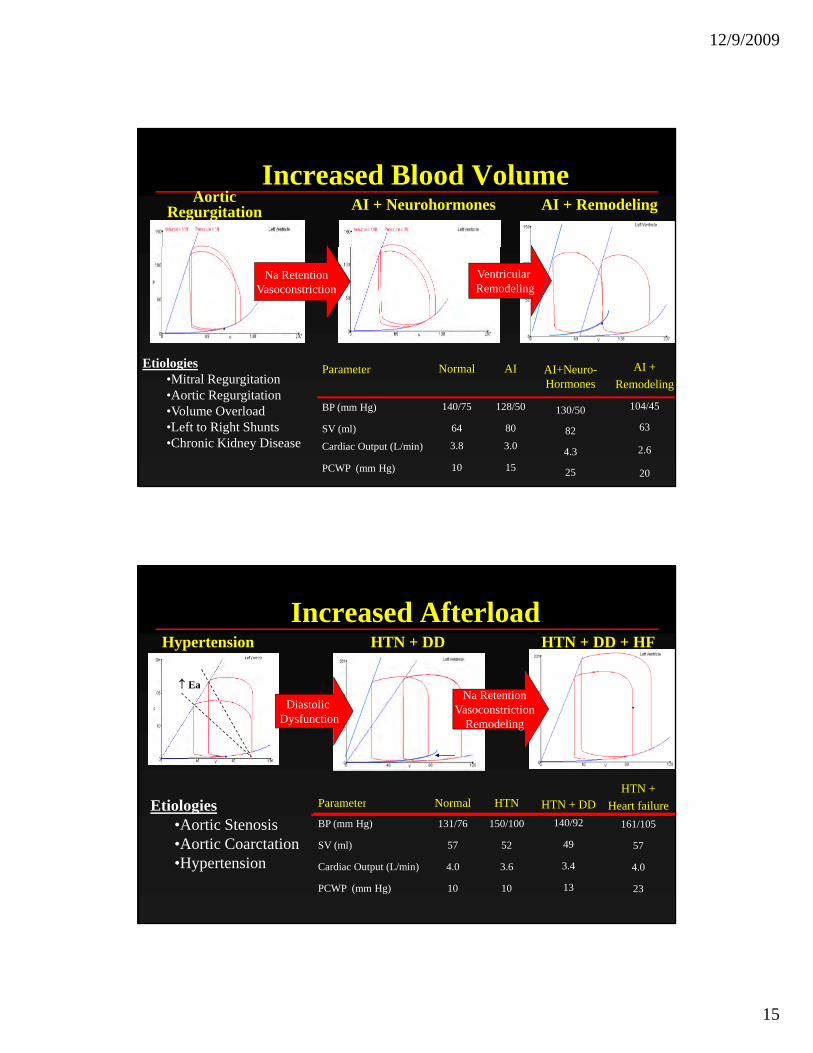
Four Basic MechanismsFour Basic Mechanisms1. Increased Blood Volume (Excessive Preload)2. Increased Resistant to Blood Flow (Excessive
Afterload)3. Decreased contractility4. Decreased Filling
12/9/2009
15
Increased Blood VolumeAortic
Regurgitation AI + Neurohormones AI + Remodeling
AI +Etiologies AINormalP t AI+N
Na RetentionVasoconstriction
VentricularRemodeling
AI + Remodeling
104/45
63
2.6
20
Etiologies•Mitral Regurgitation•Aortic Regurgitation•Volume Overload•Left to Right Shunts•Chronic Kidney Disease
15
3.0
80
128/50
AI
10PCWP (mm Hg)
3.8Cardiac Output (L/min)
64SV (ml)
140/75BP (mm Hg)
NormalParameter
25
4.3
82
130/50
AI+Neuro-Hormones
Increased AfterloadHypertension
↑ Ea
HTN + DD HTN + DD + HF
Etiologies Parameter Normal HTNHTN +
Heart failureHTN + DD
↑ Ea
Diastolic Dysfunction
Na RetentionVasoconstriction
Remodeling
Etiologies•Aortic Stenosis•Aortic Coarctation•Hypertension
Parameter Normal HTN
BP (mm Hg) 131/76 150/100
SV (ml) 57 52
Cardiac Output (L/min) 4.0 3.6
PCWP (mm Hg) 10 10
Heart failure161/105
57
4.0
23
HTN + DD140/92
49
3.4
13
12/9/2009
16
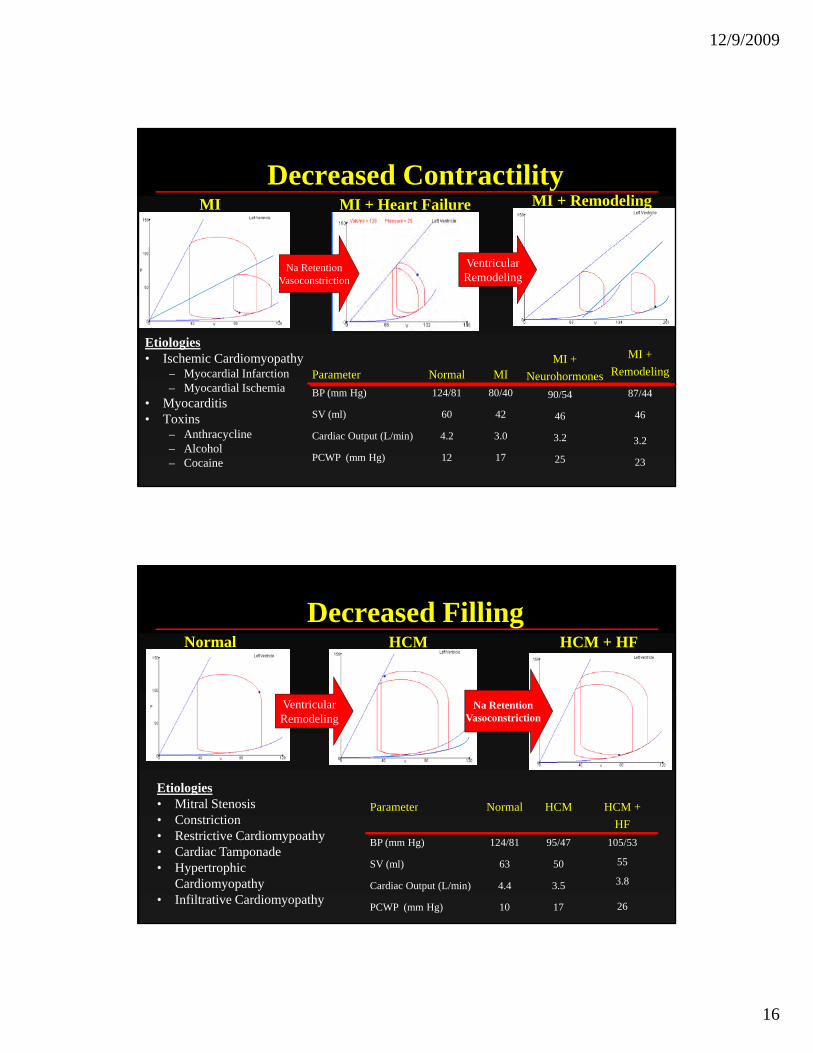
Decreased ContractilityMI MI + Heart Failure MI + Remodeling
Etiologies • Ischemic Cardiomyopathy MI + MI +
d li
Na RetentionVasoconstriction
VentricularRemodeling
– Myocardial Infarction– Myocardial Ischemia
• Myocarditis• Toxins
– Anthracycline – Alcohol– Cocaine
Neurohormones90/54
46
3.2
25
Remodeling
87/44
46
3.2
23
Parameter Normal MIBP (mm Hg) 124/81 80/40
SV (ml) 60 42
Cardiac Output (L/min) 4.2 3.0
PCWP (mm Hg) 12 17
Decreased FillingNormal HCM HCM + HF
Etiologies • Mitral Stenosis
VentricularRemodeling
P t N l HCM HCM +
Na RetentionVasoconstriction
• Mitral Stenosis• Constriction• Restrictive Cardiomypoathy• Cardiac Tamponade• Hypertrophic
Cardiomyopathy• Infiltrative Cardiomyopathy
Parameter Normal HCM
BP (mm Hg) 124/81 95/47
SV (ml) 63 50
Cardiac Output (L/min) 4.4 3.5
PCWP (mm Hg) 10 17
HCM +HF
105/53
55
3.8
26
12/9/2009
17
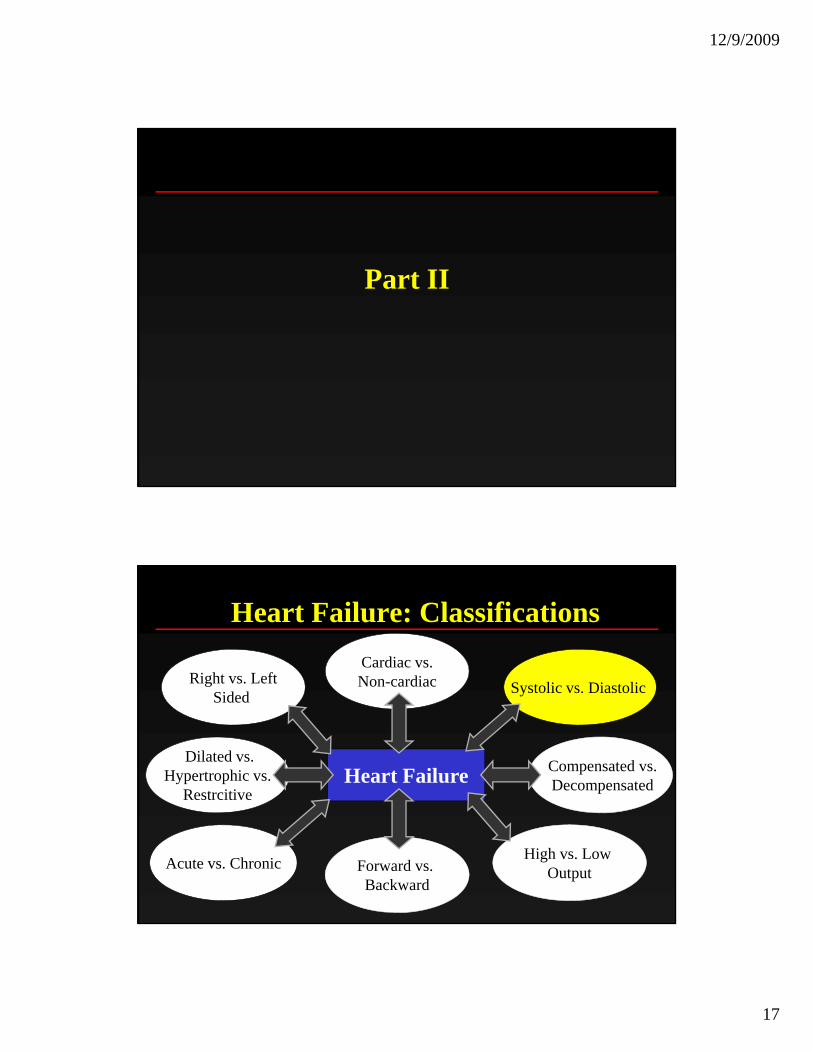
Part II
Heart Failure: Classifications
S t li Di t liRight vs. LeftCardiac vs.Non-cardiac
Heart Failure
Systolic vs. Diastolic gSided
Non cardiac
Dilated vs.Hypertrophic vs.
Restrcitive
Compensated vs.Decompensated
High vs. Low OutputAcute vs. Chronic Forward vs.
Backward
12/9/2009
18
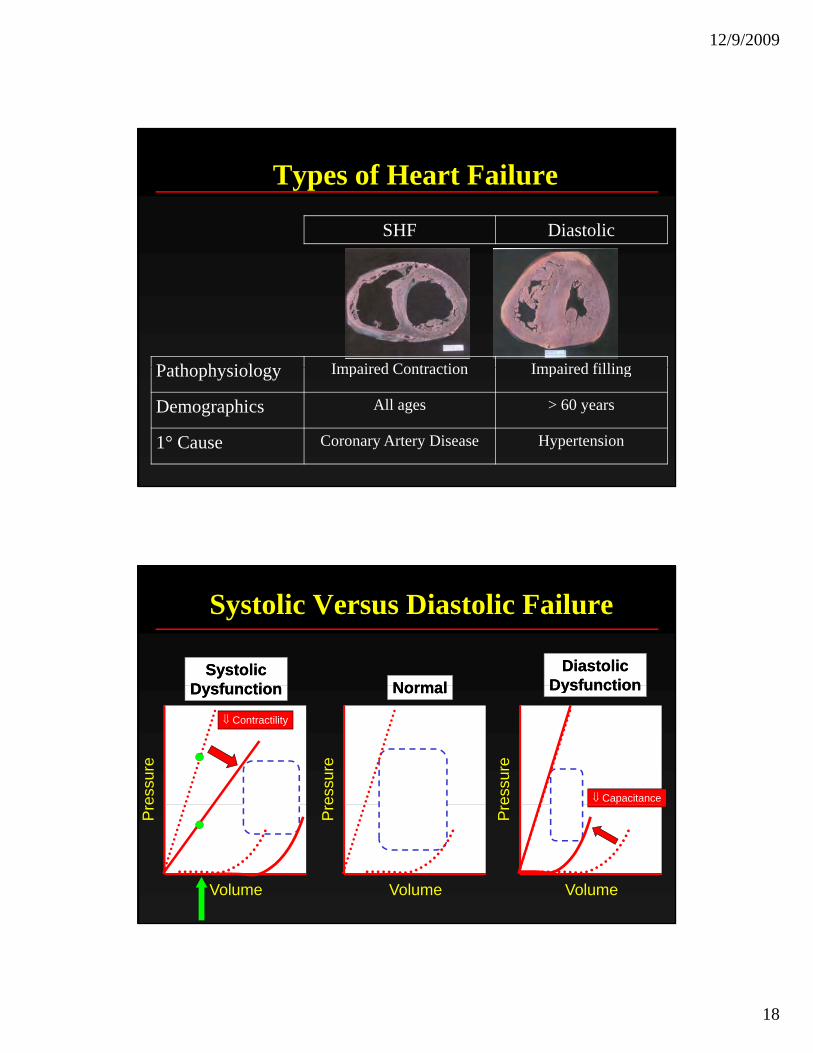
Types of Heart Failure
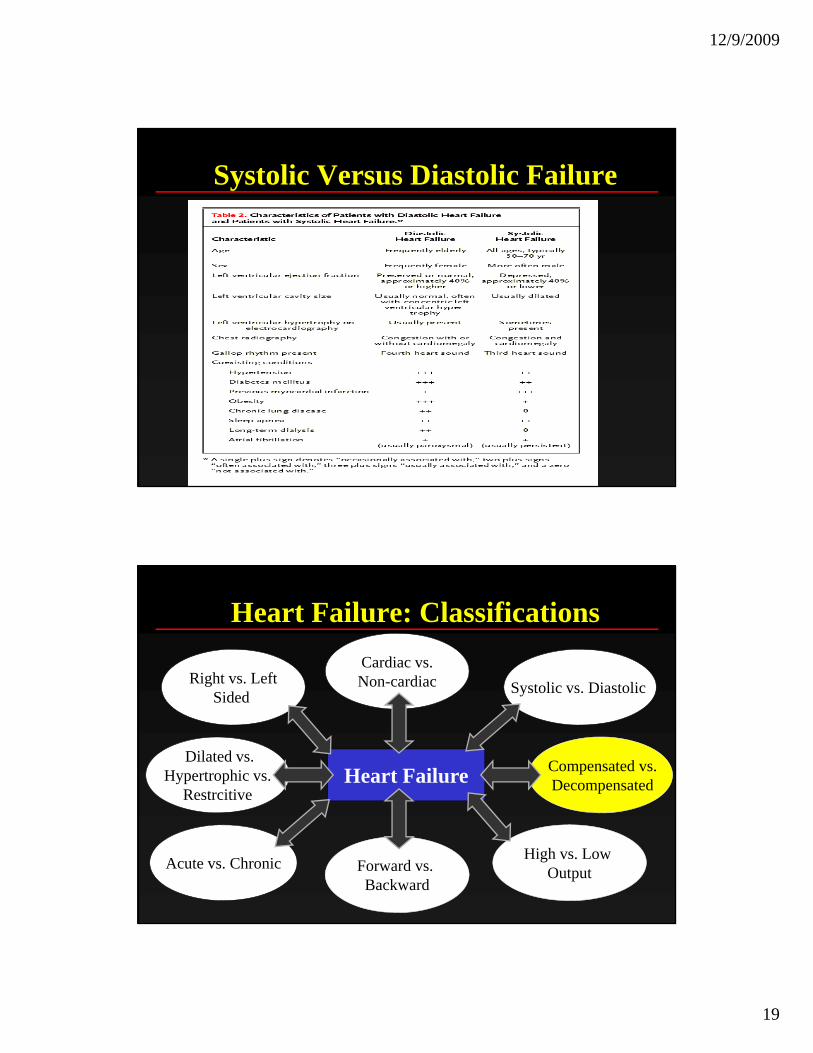
SHF Diastolic
P th h i l Impaired Contraction Impaired fillingPathophysiology Impaired Contraction Impaired filling
Demographics All ages > 60 years
1° Cause Coronary Artery Disease Hypertension
Systolic Versus Diastolic Failure
NormalNormalSystolicSystolic
D f tiD f tiDiastolicDiastolic
DysfunctionDysfunction
essu
re
essu
re
essu
re
NormalNormalDysfunctionDysfunction
⇓ Contractility
⇓ Capacitance
DysfunctionDysfunction
Volume
Pr
Volume
Pr
Volume
Pr
12/9/2009
19
Systolic Versus Diastolic Failure
Heart Failure: Classifications
S t li Di t liRight vs. LeftCardiac vs.Non-cardiac
Heart Failure
Systolic vs. Diastolic gSided
Non cardiac
Dilated vs.Hypertrophic vs.
Restrcitive
Compensated vs.Decompensated
High vs. Low OutputAcute vs. Chronic Forward vs.
Backward
12/9/2009
20
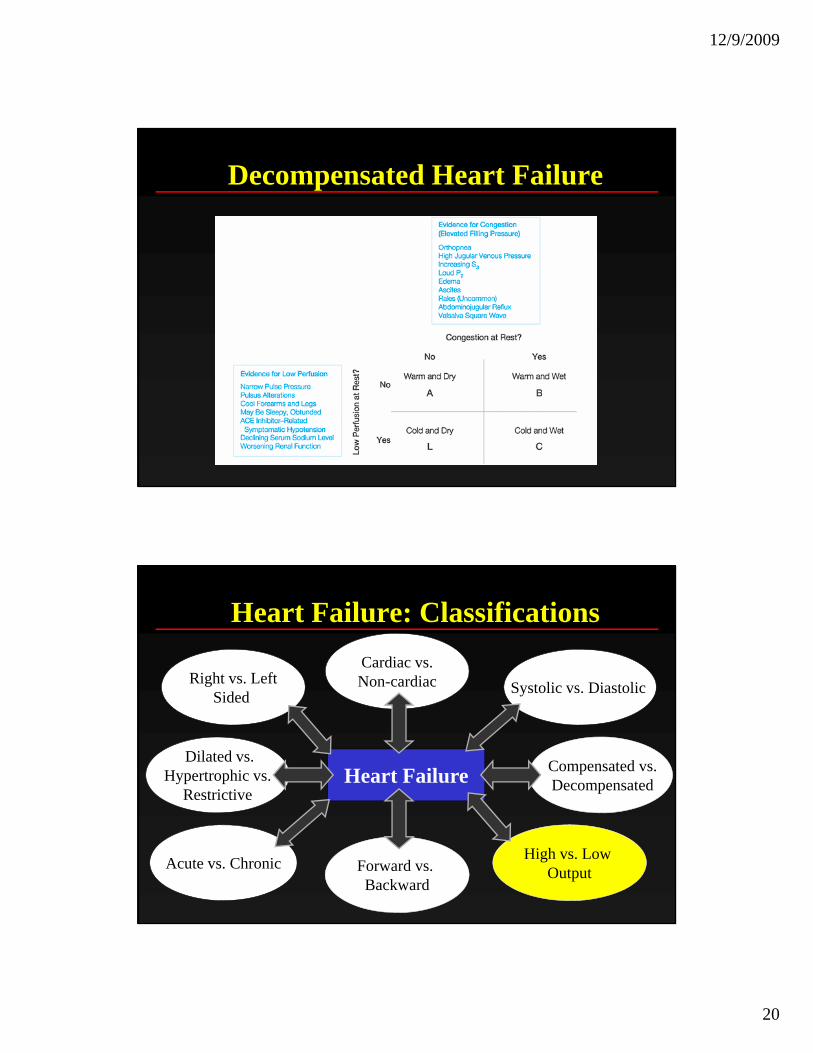
Decompensated Heart Failure
Heart Failure: Classifications
S t li Di t liRight vs. LeftCardiac vs.Non-cardiac
Heart Failure
Systolic vs. Diastolic gSided
Non cardiac
Dilated vs.Hypertrophic vs.
Restrictive
Compensated vs.Decompensated
High vs. Low OutputAcute vs. Chronic Forward vs.
Backward
12/9/2009
21
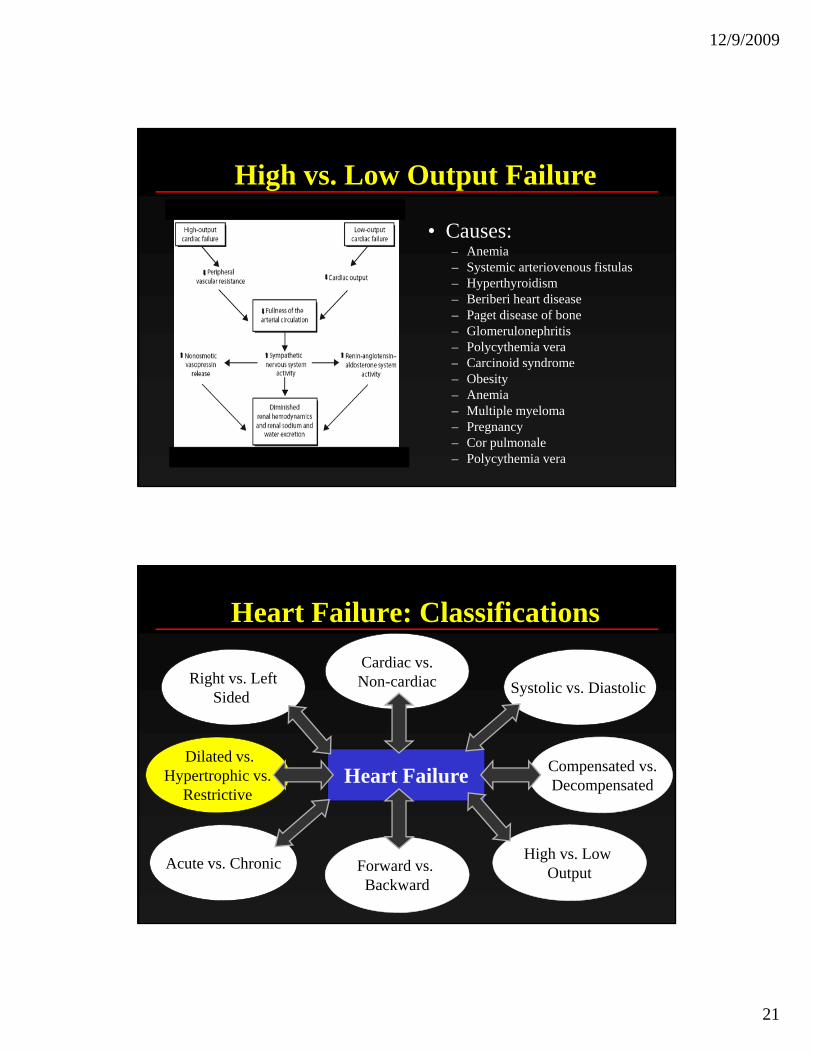
High vs. Low Output Failure
• Causes:A i– Anemia
– Systemic arteriovenous fistulas – Hyperthyroidism – Beriberi heart disease – Paget disease of bone – Glomerulonephritis – Polycythemia vera – Carcinoid syndrome y– Obesity– Anemia – Multiple myeloma – Pregnancy – Cor pulmonale – Polycythemia vera
Heart Failure: Classifications
S t li Di t liRight vs. LeftCardiac vs.Non-cardiac
Heart Failure
Systolic vs. Diastolic gSided
Non cardiac
Dilated vs.Hypertrophic vs.
Restrictive
Compensated vs.Decompensated
High vs. Low OutputAcute vs. Chronic Forward vs.
Backward
12/9/2009
22
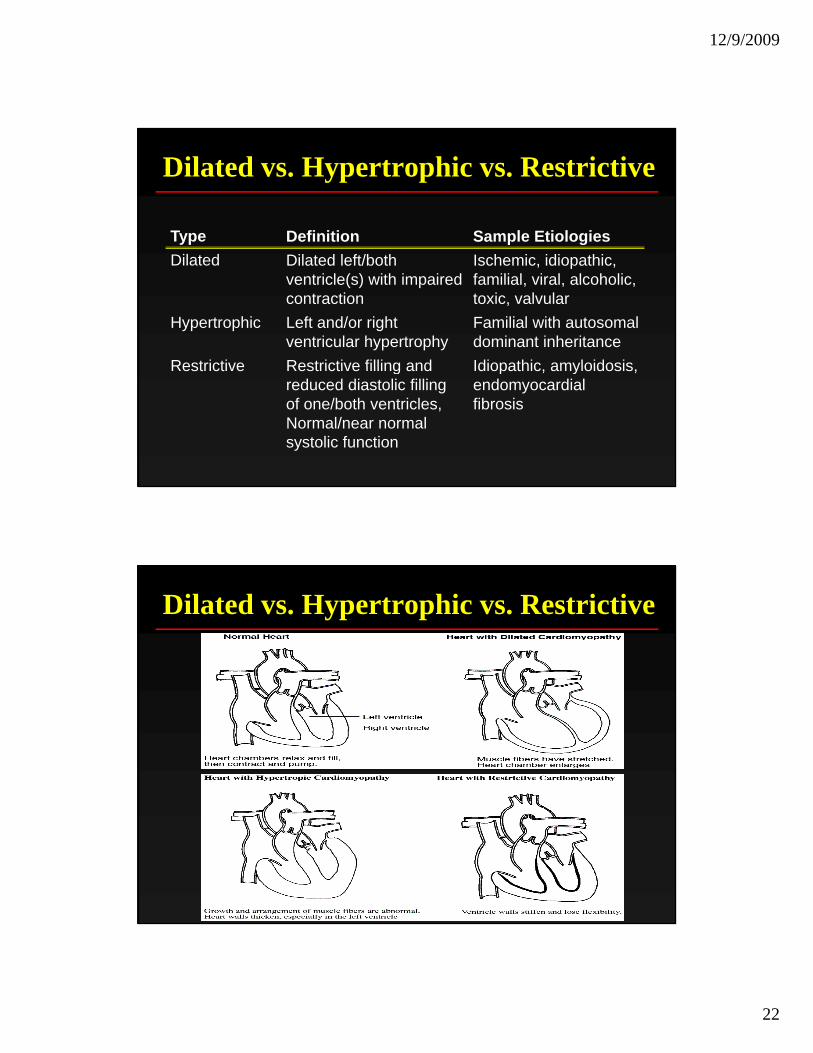
Dilated vs. Hypertrophic vs. Restrictive
Type Definition Sample EtiologiesDilated Dilated left/both
ventricle(s) with impaired contraction
Ischemic, idiopathic, familial, viral, alcoholic, toxic, valvular
Hypertrophic Left and/or right ventricular hypertrophy
Familial with autosomal dominant inheritance
Restrictive Restrictive filling and Idiopathic amyloidosisRestrictive Restrictive filling and reduced diastolic filling of one/both ventricles, Normal/near normal systolic function
Idiopathic, amyloidosis, endomyocardial fibrosis
Dilated vs. Hypertrophic vs. Restrictive
12/9/2009
23
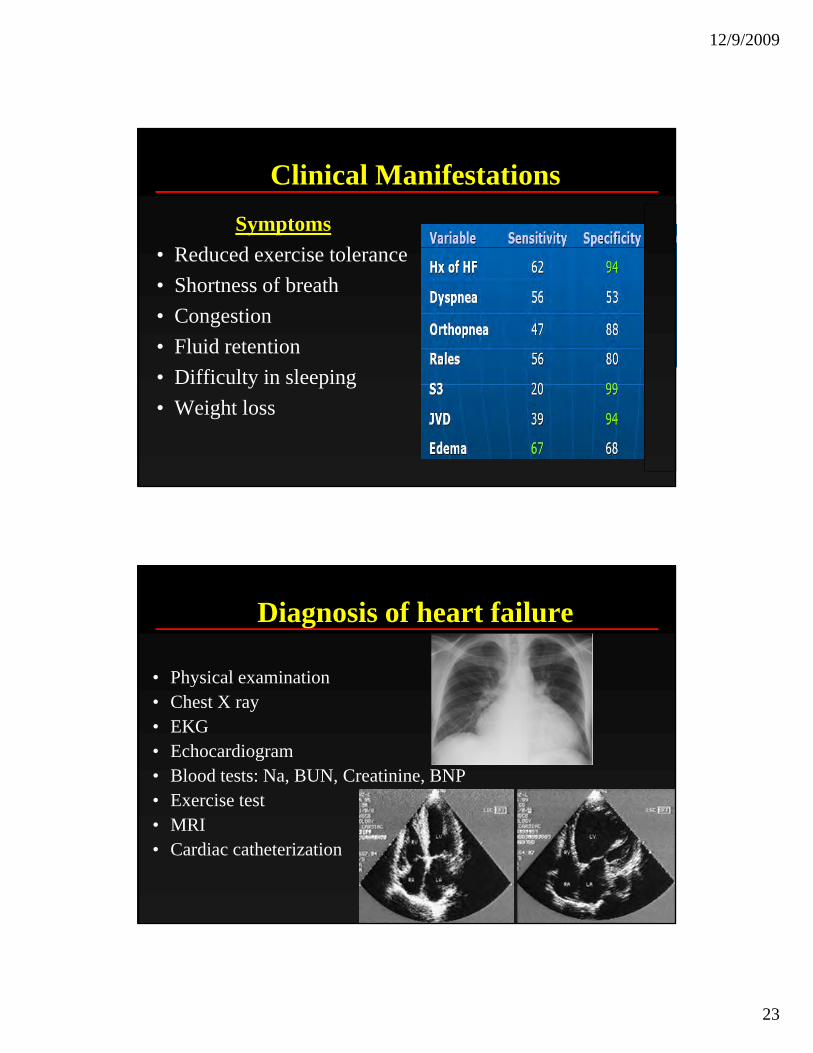
Clinical ManifestationsSymptoms
R d d i l• Reduced exercise tolerance• Shortness of breath• Congestion• Fluid retention• Difficulty in sleeping• Weight loss
Diagnosis of heart failure
• Physical examinationy• Chest X ray• EKG• Echocardiogram• Blood tests: Na, BUN, Creatinine, BNP• Exercise testExercise test• MRI• Cardiac catheterization
12/9/2009
24
II
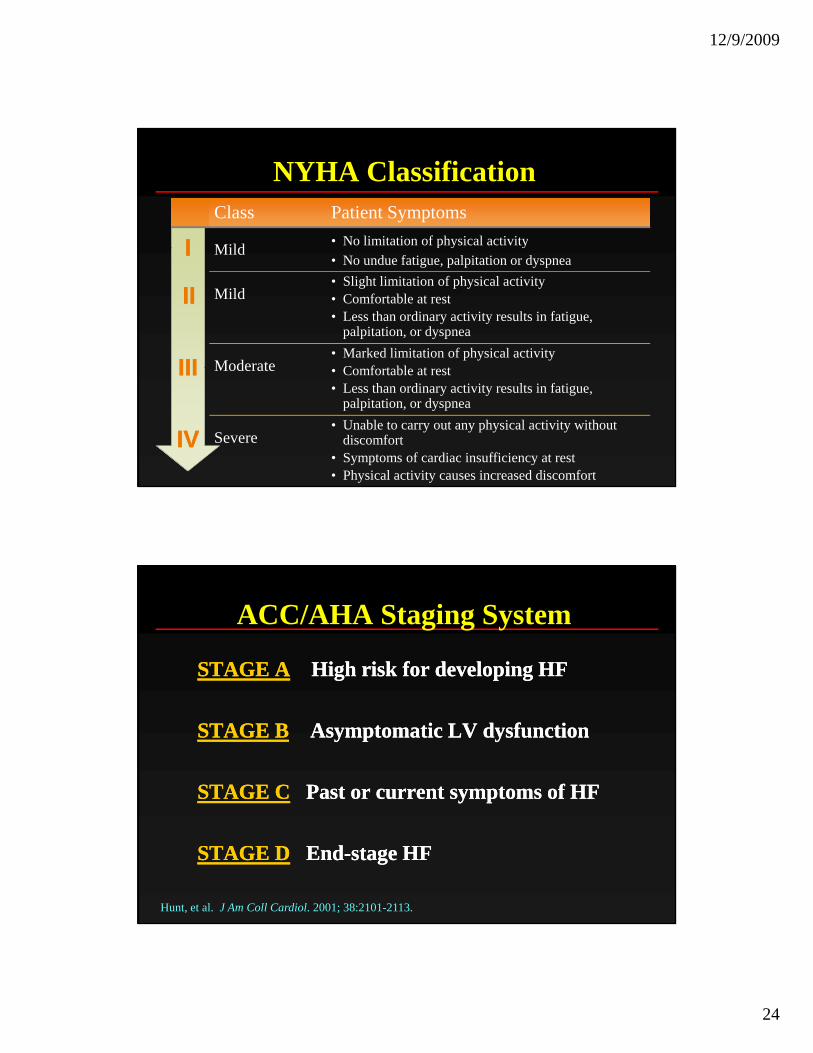
NYHA ClassificationClass Patient Symptoms
Mild • No limitation of physical activityII
IIII
IIIIII
Mild p y y• No undue fatigue, palpitation or dyspnea
Mild• Slight limitation of physical activity• Comfortable at rest• Less than ordinary activity results in fatigue,
palpitation, or dyspnea
Moderate• Marked limitation of physical activity
C f t bl t tIIIIII
IVIV
Moderate • Comfortable at rest• Less than ordinary activity results in fatigue,
palpitation, or dyspnea
Severe• Unable to carry out any physical activity without
discomfort• Symptoms of cardiac insufficiency at rest• Physical activity causes increased discomfort
ACC/AHA Staging System
STAGE ASTAGE A High risk for developing HFHigh risk for developing HF
STAGE BSTAGE B Asymptomatic LV dysfunctionAsymptomatic LV dysfunction
STAGE CSTAGE C Past or current symptoms of HFPast or current symptoms of HF
STAGE DSTAGE D EndEnd--stage HFstage HF
Hunt, et al. J Am Coll Cardiol. 2001; 38:2101-2113.
12/9/2009
25
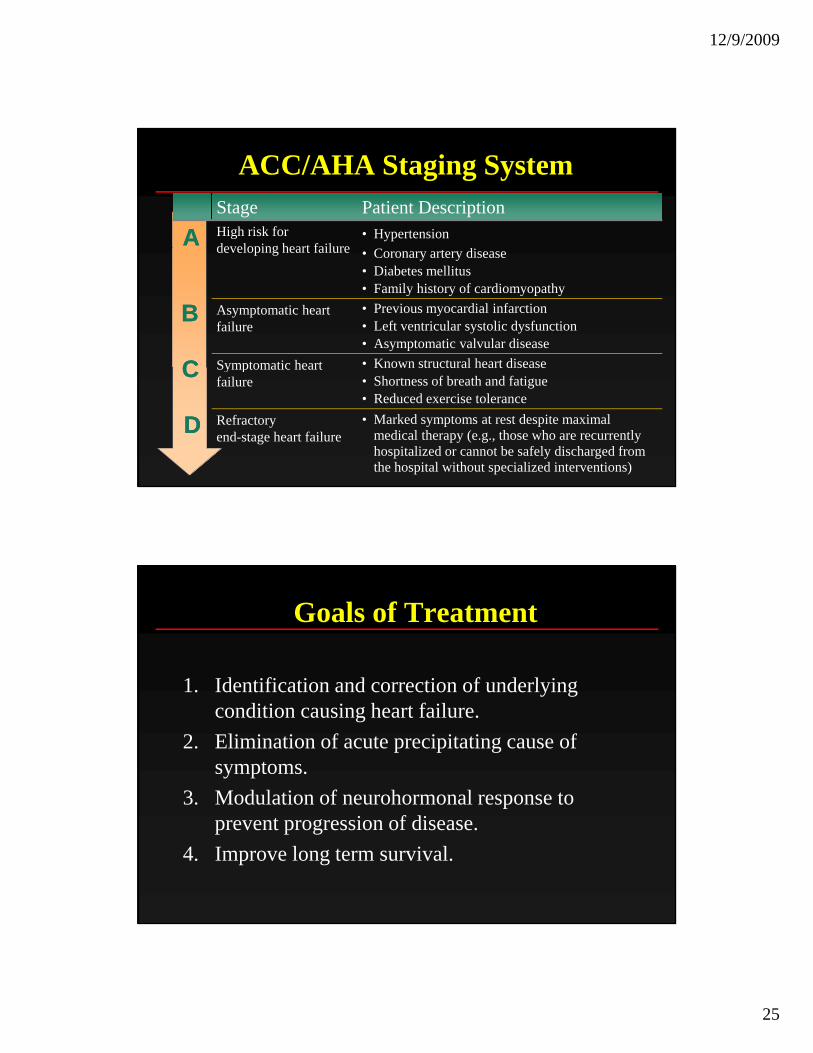
Stage Patient DescriptionHigh risk for developing heart failure
• Hypertension
ACC/AHA Staging System
AA developing heart failure • Coronary artery disease• Diabetes mellitus• Family history of cardiomyopathy
Asymptomatic heart failure
• Previous myocardial infarction• Left ventricular systolic dysfunction• Asymptomatic valvular disease
Symptomatic heart • Known structural heart disease
BB
CC Symptomatic heart failure
Known structural heart disease• Shortness of breath and fatigue• Reduced exercise tolerance
Refractory end-stage heart failure
• Marked symptoms at rest despite maximal medical therapy (e.g., those who are recurrently hospitalized or cannot be safely discharged from the hospital without specialized interventions)
CC
DD
Goals of Treatment
1 Identification and correction of underlying1. Identification and correction of underlying condition causing heart failure.
2. Elimination of acute precipitating cause of symptoms.
3. Modulation of neurohormonal response to pprevent progression of disease.
4. Improve long term survival.
12/9/2009
26
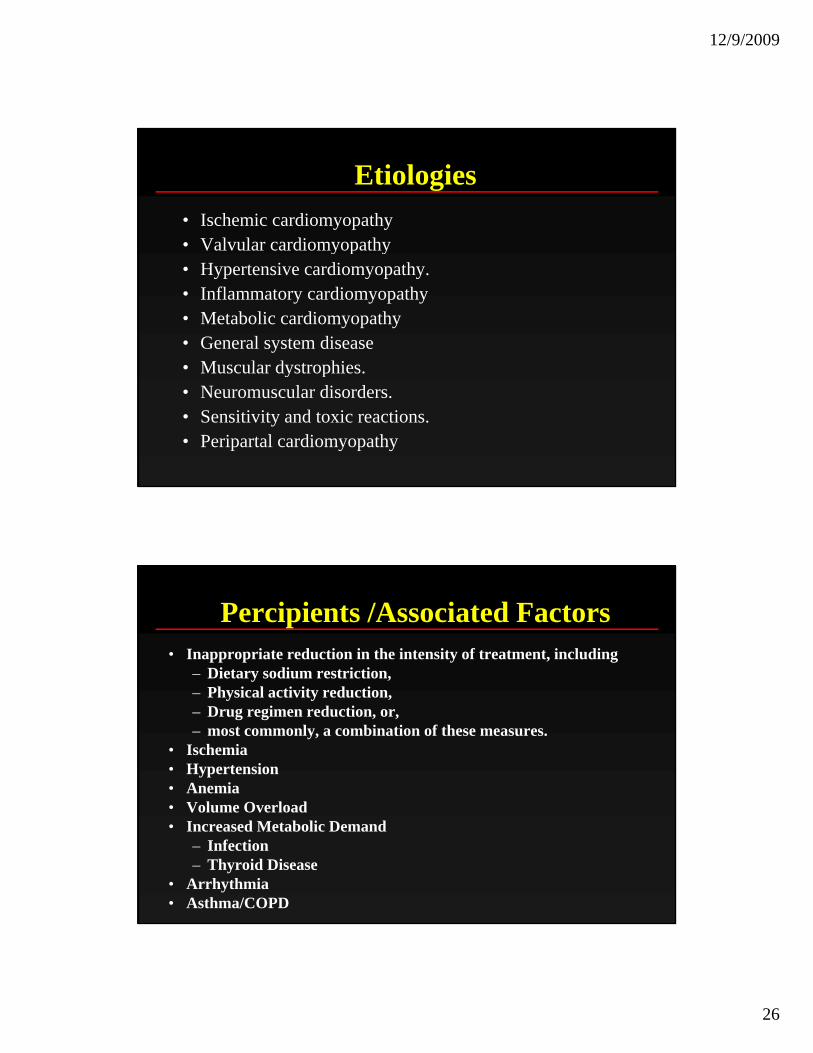
Etiologies• Ischemic cardiomyopathy • Valvular cardiomyopathyValvular cardiomyopathy • Hypertensive cardiomyopathy.• Inflammatory cardiomyopathy • Metabolic cardiomyopathy • General system disease• Muscular dystrophies• Muscular dystrophies.• Neuromuscular disorders.• Sensitivity and toxic reactions.• Peripartal cardiomyopathy
Percipients /Associated Factors• Inappropriate reduction in the intensity of treatment, including
– Dietary sodium restriction,– Physical activity reduction,– Drug regimen reduction, or, – most commonly, a combination of these measures.
• Ischemia• Hypertension• Anemia
V l O l d• Volume Overload• Increased Metabolic Demand
– Infection– Thyroid Disease
• Arrhythmia• Asthma/COPD
12/9/2009
27
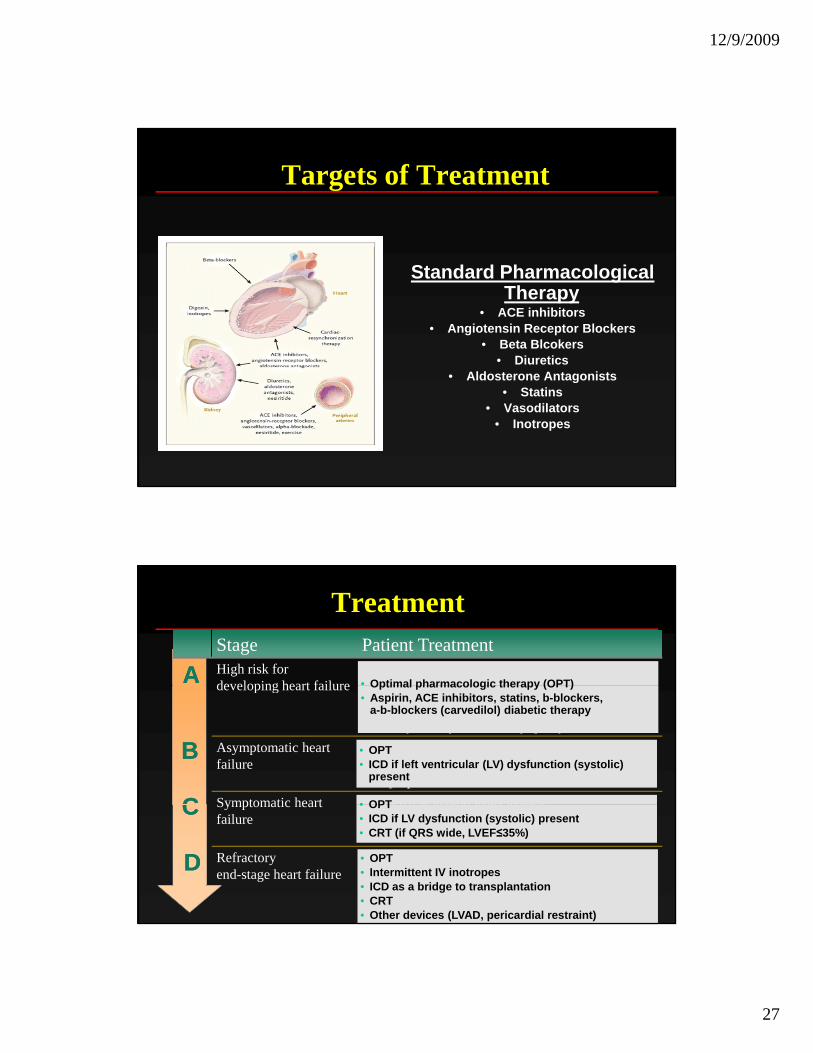
Targets of Treatment
Standard Pharmacological Therapy
• ACE inhibitors• Angiotensin Receptor Blockers
• Beta Blcokers• Diuretics
• Aldosterone Antagonists• Statins
• Vasodilators• Inotropes
Stage Patient TreatmentHigh risk for developing heart failure
• Hypertension
Treatment
AA • Optimal pharmacologic therapy (OPT)developing heart failure • Coronary artery disease• Diabetes mellitus• Family history of cardiomyopathy
Asymptomatic heart failure
• Previous myocardial infarction• Left ventricular systolic dysfunction• Asymptomatic valvular disease
Symptomatic heart • Known structural heart disease
BB
CC • OPT
Optimal pharmacologic therapy (OPT)• Aspirin, ACE inhibitors, statins, b-blockers,
a-b-blockers (carvedilol) diabetic therapy
• OPT• ICD if left ventricular (LV) dysfunction (systolic)
present
Symptomatic heart failure
Known structural heart disease• Shortness of breath and fatigue• Reduced exercise tolerance
Refractory end-stage heart failure
• Marked symptoms at rest despite maximal medical therapy (e.g., those who are recurrently hospitalized or cannot be safely discharged from the hospital without specialized interventions)
CC
DD
• OPT• ICD if LV dysfunction (systolic) present• CRT (if QRS wide, LVEF≤35%)
• OPT• Intermittent IV inotropes• ICD as a bridge to transplantation• CRT • Other devices (LVAD, pericardial restraint)
12/9/2009
28
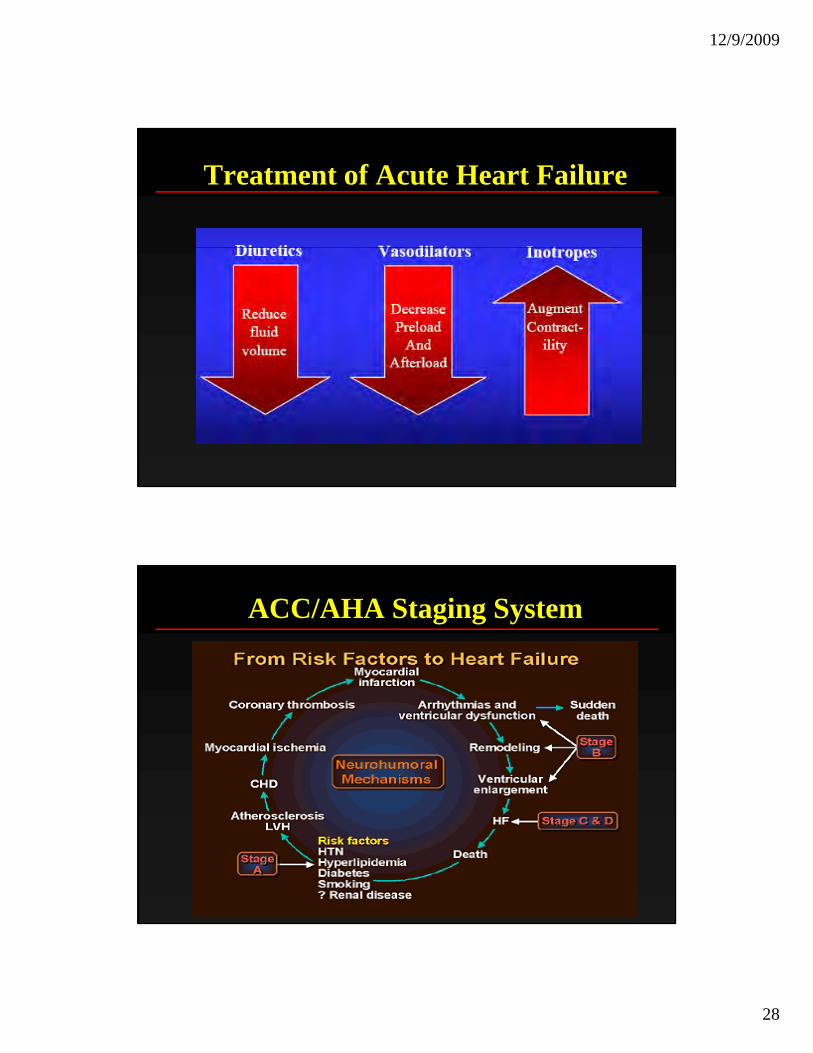
Treatment of Acute Heart Failure
ACC/AHA Staging System
12/9/2009
29
Summary
• Complex Clinical Syndrome• Complex Clinical Syndrome• Multiple Etiologies and Classification Systems• Physiologic Understanding Essential
htt // l bi d /it /h / di l/h t i /http://www.columbia.edu/itc/hs/medical/heartsim/
![Pathophysiology: Heart Failure - Columbia University Heart Failure ... ÐTPR = [MAP - CVP] / CO, and ÐCO = SV * HR ... ¥Anemia ¥Volume Overload ¥Increased Metabolic Demand](https://img.pdfslide.us/doc/110x75/5aa356057f8b9ab4208e3270/pathophysiology-heart-failure-columbia-heart-failure-tpr-map-cvp-.jpg)













![Heart Failure [Read-Only] · PDF file6 Types of Heart Failure 1° Cause Coronary Artery Disease Hypertension Demographics All ages > 60 years Pathophysiology Impaired Contraction Impaired](https://img.pdfslide.us/doc/110x75/5a8e45427f8b9a4a268d21fc/heart-failure-read-only-types-of-heart-failure-1-cause-coronary-artery-disease.jpg)



![Pathophysiology: Heart Failure - Columbia University Heart Failure ... – TPR = [MAP - CVP] / CO, and ... – Anemia – Systemic arteriovenous fistulas – Hyperthyroidism](https://img.pdfslide.us/doc/110x75/5aa356057f8b9ab4208e3286/pathophysiology-heart-failure-columbia-heart-failure-tpr-map-cvp.jpg)