-
Pathology of Rotator Cuff
Tendonopathy
Bing Wu, MB
Centre for Orthopaedic Research, Department of Surgery
The University of Western Australia
This thesis is presented for the degree of Master of Medical
Science
of the University of Western Australia
2008
The work presented in this thesis was performed in the
University of Western Australia Centre for Orthopaedic
Research,
Queen Elizabeth II Medical Centre, Nedlands, Western
Australia
-
– 1 –
Publication and presentation
BING WU, JIMIN CHEN, TAMMYL DELA ROSA, YU QIAN, ALLAN WANG,
JIAKE XU and MING-HAO ZHENG. Autophagic cell death in rotator
cuff
tendonopathy. Manuscript in preparation.
JIMIN CHEN, BING WU, TAMMYL DELA ROSA, YU QIAN, ALLAN WANG,
JIAKE XU and MING-HAO ZHENG Autophagic cell death in rotator
cuff
tendonopathy: a preliminary result. Proceeding of ASBMR Annual
Meeting 2008.
-
– 2 –
Contents
Contents
......................................................................................................................................................
2
Abstract
.......................................................................................................................................................
5
Acknowledgements
.....................................................................................................................................
7
List of figures
..............................................................................................................................................
8
List of tables
................................................................................................................................................
9
Abbreviations
...........................................................................................................................................
10
1. Introduction
....................................................................................................................................
122
1.1. Anatomy
............................................................................................................................................
13
1.2. Aetiology
...........................................................................................................................................
15
1.2.1. Extrinsic mechanisms
..........................................................................................................
15
1.2.1.1. Impingement and acromial shape
..................................................................................
15
1.2.1.2. Age
.................................................................................................................................
16
1.2.1.3. Smoking
..........................................................................................................................
17
1.2.2. Intrinsic mechanisms
...........................................................................................................
17
1.2.2.1. Degeneration
..................................................................................................................
17
1.2.2.2. Cuff vascularity
..............................................................................................................
19
1.2.2.3. Neural factors
................................................................................................................
19
1.2.3. Overuse
................................................................................................................................
20
1.3. Pathology
..........................................................................................................................................
21
1.3.1. Histology of the normal tendon
...........................................................................................
21
1.3.2. Pathology of tendonopathy
..................................................................................................
23
1.3.3. Healing response
..................................................................................................................
24
1.3.3.1. Acute healing process
....................................................................................................
25
1.3.3.2. Chronic healing process
................................................................................................
26
1.4. Diagnosis
...........................................................................................................................................
26
1.5. Treatment
..........................................................................................................................................
28
1.5.1. Conservative treatment
........................................................................................................
28
1.5.1.1. Rest
.................................................................................................................................
28
1.5.1.2. NSAIDs
...........................................................................................................................
28
1.5.1.3. Corticosteroid injections
................................................................................................
29
1.5.1.4. Exercise
..........................................................................................................................
29
1.5.1.5. Physical modalities
........................................................................................................
30
1.5.2. Surgical treatment
................................................................................................................
30
1.5.2.1. Partial-thickness tears
...................................................................................................
31
1.5.2.2. Full-thickness tears
........................................................................................................
32
-
– 3 –
1.6. Summary
...........................................................................................................................................
33
2. Hypothesis and aims
.........................................................................................................................
35
2.1. Hypothesis
.........................................................................................................................................
36
2.2. Aims
..................................................................................................................................................
36
3. Materials and methods
.....................................................................................................................
39
3.1.
Materials............................................................................................................................................
39
3.1.1. Chemical reagents
................................................................................................................
39
3.1.2.
Enzymes...............................................................................................................................
39
3.1.3. Antibodies
............................................................................................................................
40
3.1.4. Commercial kit
....................................................................................................................
40
3.1.5. Buffer and solutions
.............................................................................................................
40
3.1.6. Other materials
....................................................................................................................
42
3.2. Methods
.............................................................................................................................................
42
3.2.1. Human sample collection
....................................................................................................
42
3.2.2. Tissue preparation
................................................................................................................
43
3.2.2.1. HE staining
....................................................................................................................
44
3.2.2.2. Immunohistochemistry
...................................................................................................
44
3.2.2.3. TUNEL assay
.................................................................................................................
45
3.2.3. Evaluation of fibril matrix degeneration
..............................................................................
46
4. Results: the variety of cellularity in the disruption of the
fibril matrix ....................................... 49
4.1. General description
...........................................................................................................................
50
4.2. Comparisons
......................................................................................................................................
53
4.2.1. Normal fields vs degenerative
fields....................................................................................
53
4.2.2. Cell density in the different matrix grades
...........................................................................
54
4.3. Discussion
.........................................................................................................................................
54
5. Results: the role of apoptosis in the disruption of the
fibril matrix ............................................. 59
5.1. General description
...........................................................................................................................
59
5.2. Comparisons
......................................................................................................................................
60
5.2.1. Normal fields vs degenerative
fields....................................................................................
63
5.2.2. Percentage of apoptotic cells in the different matrix
grades ................................................ 64
5.3. Discussion
.........................................................................................................................................
65
5.3.1. Limitations
...........................................................................................................................
67
6. Results: the role of autophagic cell death in the disruption
of the fibril matrix ......................... 70
6.1. General description
...........................................................................................................................
70
6.2. Comparisons
......................................................................................................................................
73
6.2.1. Normal fields vs degenerative
fields....................................................................................
74
-
– 4 –
6.2.2. Percentage of autophagic cell death in the different
matrix grades ..................................... 76
6.3. Discussion
.........................................................................................................................................
78
6.3.1. Limitation
............................................................................................................................
80
7. Results: the role of myofibroblasts in the disruption of the
fibril matrix .................................... 82
7.1. General description
...........................................................................................................................
82
7.2. Comparisons
......................................................................................................................................
84
7.2.1. Normal fields vs degenerative
fields....................................................................................
86
7.2.2. Percentage of myofibroblasts in the different matrix
grades ............................................... 87
7.3. Discussion
.........................................................................................................................................
87
8. General discussion
............................................................................................................................
93
8.1. Future
directions................................................................................................................................
98
9. References
.......................................................................................................................................
101
-
– 5 –
Abstract
Tendonopathy, resulting in the loss of mechanical strength of a
tendon, is a serious health
problem affecting many people. The common symptom of
tendonopathy is pain –
patients‟ daily activities, their participation in sport and
exercise, and their ability to work
are greatly compromised. Tendonopathy is considered to be a
degenerative disorder
caused by repetitive injury of the tendon. The most common
tendon lesions are Achilles
tendon rupture, lateral epicondylitis (tennis elbow) and rotator
cuff tear.
However, in spite of its clinical significance, our knowledge
about tendonopathy is still
very poor. This research was undertaken to investigate the
pathology of tendonopathy. It
is proposed that apoptosis, autophagic cell death and
myofibroblasts play a role in the
progression of tendonopathy in the rotator cuff; the aim of this
study was therefore to
determine if this was indeed the case.
Tendon tissues were collected from 30 patients suffering from
rotator cuff tears. A
terminal deoxynucleotidyl transferase biotin-dUTP nick end
labelling (TUNEL assay)
was performed to detect apoptosis. Autophagic cell death of the
tenocytes in the ruptured
rotator cuff tendon was detected by immunohistochemical staining
for ubiquitin.
Myofibroblasts were identified immunohistochemically with
anti-alpha-smooth muscle
actin (anti--SMA) antibody. The distribution of apoptosis,
autophagic cell death and
myofibroblasts, as well as the total cell density, were assessed
respectively and were
correlated using a four-category (i.e. graded from 0-3)
degeneration of collagen matrix.
-
– 6 –
The results showed that apoptosis, autophagic cell death and
myofibroblasts were
observed in all of the samples. The highest percentage of
autophagic cell death was
evidenced in the Grade 2 matrix, while the percentage of
apoptosis increased significantly
with the increase of matrix degeneration from Grade 0-3; a
similar pattern was found for
myofibroblasts. The total cell numbers varied among the matrix
grades, with the
maximum and minimum percentages occurring in Grades 1 and 3,
respectively.
It can be concluded that apoptosis, autophagic cell death and
myofibroblasts might be
closely related to the damage of the extracellular matrix (ECM)
structure.
-
– 7 –
Acknowledgements
The work described in this thesis was performed in the Centre
for Orthopaedic Research,
School of Surgery, University of Western Australia. I would like
to express my sincere
gratitude and appreciation to my two supervisors, Professor
Ming-Hao Zheng and
A/Professor Jiake Xu. Without your guidance, support and
inspiration, this work would
never have been accomplished. Thank you very much for your
constant encouragement.
I would also like to thank Jimin Chen for technical guidance, Yu
Qian for statistical
support, and Zhen Lin for useful advice. Many thanks also to my
lab colleagues, Dr Sky
Feng, Ms Jamie Tan, Ms Bo Qian, Mr Cheng Loon Leong, Mr Craig
Willers, Dr Zi Qiang
Zhou, Mr Ee-Cheng Khor, Ms Estabelle, Dr Felixc Yao, Dr Jacky
Chim, Ms Jasreen, Ms
Katherine Mackie, Ms Lesley Gasmier, Ms Pei Ying Ng, Ms Samuel
Shee, Mr Tak Sum
and Ms Tamara Davey.
Most importantly, my gratitude to my family. Thank you all so
much for the love and
support you have always given me throughout my life. Without
you, this thesis would
never have been possible.
Special dedication
This thesis is dedicated to my parents for their unconditional
and endless love, guidance
and support throughout my life.
-
– 8 –
List of figures
Figure 1.1. The rotator cuff muscles
........................................................................................................
13
Figure 1.2. Rotator cuff tear types
............................................................................................................
14
Figure 1.3. The three types of acromions
.................................................................................................
16
Figure 1.4. Possible pathways of tendon degeneration under
oxidative stress ......................................... 18
Figure 1.5. The stress versus strain relationship for the
progressive loading of a tendon ........................ 20
Figure 1.6. The anatomy of a normal tendon
...........................................................................................
22
Figure 3.1. ECM classification
.................................................................................................................
47
Figure 4.1. ECM grades
...........................................................................................................................
51
Figure 4.2. Blood vessels in torn rotator cuff tendons
..............................................................................
52
Figure 4.3. The torn edge of a tendon
......................................................................................................
52
Figure 4.4. Comparison of cell density in normal fields and
degenerative fields .................................... 54
Figure 4.5. Comparison of cell density in different
ECMs.......................................................................
55
Figure 5.1. Apoptotic cells assessed by TUNEL assay
............................................................................
61
Figure 5.2 Endothelial lining showing apoptosis
....................................................................................
62
Figure 5.3. Comparison of the percentage of apoptotic cells in
normal fields and degenerative
fields
......................................................................................................................................
64
Figure 5.4. Comparison of the percentage of apoptotic cells in
different ECMs ..................................... 65
Figure 6.1. A conceptual model of
autophagy..........................................................................................
72
Figure 6.2. Autophagic cell death
............................................................................................................
74
Figure 6.3. The endothelial lining showing autophagic cell death
........................................................... 75
Figure 6.4. Comparison of the percentage of autophagic cell
death in normal fields and
degenerative fields
.................................................................................................................
76
Figure 6.5. Comparison of the percentage of autophagic cell
death in different ECMs ........................... 77
Figure 7.1. Myofibroblasts
.......................................................................................................................
84
Figure 7.2. Smooth muscle cells surround blood vessels
.........................................................................
85
Figure 7.3. Comparison of the percentage of myofibroblasts in
normal fields and degenerative
fields
......................................................................................................................................
87
Figure 7.4. Comparison of the percentage of myofibroblasts in
different ECMs ..................................... 88
Figure 8.1. A hypothetical model of chronic tendon injury
.....................................................................
97
-
– 9 –
List of tables
Table 3.1. Patient data
.............................................................................................................................
43
Table 4.1. Cell density comparison: significance probability (P
value) between the four matrix
grades
.....................................................................................................................................
55
Table 5.1. Apoptosis comparison: significance probability (P
value) between the four matrix
grades
.....................................................................................................................................
65
Table 6.1. Autophagic cell death comparison: significance
probability (P value) between the four
matrix grades
..........................................................................................................................
77
Table 7.1. Myofibroblast comparison: significance probability (P
value) between the four matrix
grades
.....................................................................................................................................
88
-
– 10 –
Abbreviations
ANOVA Analysis of variance
anti - -SMA anti-alpha-smooth muscle actin
-SMA alpha-smooth muscle actin
DAB Diaminobenzidine
DDW Double distilled water
DEPC Diethylpyrocarbonate
DPX p-xylene-bis-pyridinium bromide
ECM Extracellular matrix
FBS Foetal bovine serum
HE Haematoxylin-eosin
MRI Magnetic resonance imaging
NSAIDs Non-steroidal anti-inflammatory drugs
PBS Phosphate-buffered saline
PCD Programmed cell death
TBS Tris-buffered saline
Tris-HCl Tris (hydroxymehtyl) aminomethane hydrochloride
TUNEL assay Terminal deoxynucleotidyl transferase biotin-dUTP
nick end labelling
US Ultrasonography
-
– 11 –
Chapter 1
Introduction
-
– 12 –
1. Introduction
The rotator cuff is an anatomical term for a group of muscles
and their tendons that
stabilise the shoulder by holding the head of the humerus in the
small and shallow glenoid
fossa of the scapula. During elevation of the arm, the rotator
cuff compresses the
glenohumeral joint, thereby helping the large deltoid muscle
elevate the arm further.
Without the rotator cuff, the humeral head would ride up
partially out of the glenoid
fossa, and the efficiency of the deltoid muscle would be
lessened [105].
A rotator cuff tear is one of the most common injuries seen in
orthopaedic practice. The
tendons of the rotator cuff, not the muscles, are most commonly
torn. The tear causes
significant pain and restricted movement of the arm, thereby
greatly compromising
patients‟ daily activities, their participation in sport and
exercise, and their ability to
work. The injury is frequently seen in athletes using repeated
overhead motions or
forceful pulling motions such as baseball pitchers, swimmers and
tennis players [28, 33,
112, 121, 124, 154, 156, 218].
In the USA, approximately $US7 billion is spent every year on
the treatment of shoulder
pain, mainly rotator cuff related injury [163]. In Australia,
around 14,000 rotator cuff
repairs are carried out each year, with an estimated cost of
$A250 million [Australian
Government Medicare statistics]. More alarmingly, more than 40%
of surgery fails
within 12 months, albeit with symptoms relieved [56, 79].
Clearly, this disease affects a
wide range of people, and further studies focusing on this
disease and offering potential
for the improvement of treatment options are therefore
required.
http://en.wikipedia.org/wiki/Glenoid_fossahttp://en.wikipedia.org/wiki/Glenoid_fossahttp://en.wikipedia.org/wiki/Deltoid_musclehttp://en.wikipedia.org/wiki/Baseballhttp://en.wikipedia.org/wiki/Pitcher
-
– 13 –
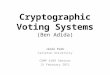
1.1. Anatomy
The rotator cuff consists of four muscles, subscapularis,
supraspinatus, infraspinatus and
teres minor (Figure 1.1). These four muscles are separately
attached to the scapula, and
then blend into a single tendon sheet approximately 0.5-0.75
inches from the point of
their attachment to the humerus [57, 68]. The long portion of
the bicep adheres to the
glenohumeral capsule and attaches to the humeral head [68].
Figure 1.1. The rotator cuff muscles
The rotator cuff plays an important role in stabilising the
glenohumeral joint and rotating
the outside of the humerus [68]. The term „force couples‟ is
used to describe the
relationship between intrinsic and extrinsic muscles. The force
couples depend on the
function of the rotator cuff [105]. Further, the rotator cuff
helps to maintain the integrity
of the joint space and prevents synovial fluid from leaking; it
is therefore important in
cartilage nutrition and in the prevention of cuff tear
arthropathy [177]. Therefore, any
factor that disrupts the force couples is also likely to
contribute to shoulder dysfunction.
-
– 14 –
Rotator cuff tears are tears of one or more of the four tendons
of the rotator cuff muscles.
Most rotator cuff tears are located in the tendinous part of the
cuff, where the tendons
from the corresponding muscles are not individualised [68]. The
tears can be classified
into two types, partial-thickness or full-thickness,
irrespective of whether they are due to
impingement or to traumatic or degenerative ischaemic aetiology
[92]. Patte proposed a
classification system for rotator cuff tears [183] and Ellman‟s
classification for their
evaluation is also used in many studies [63, 204] – the quality
and mobility of the rotator
cuff tissue is classified by tear pattern, size, retraction and
chronicity, and the tear type
(Figure 1.2) is classified by tendon retraction, tear size, cuff
mobility and tissue quality
[204].
Figure 1.2. Rotator cuff tear types
A. Transverse tear. B. Anterior L-shaped tear. C. Posterior
L-shaped tear. D. Tongue-shaped tear.
E. V-shaped tear. F. U-shaped tear. G. U-shaped tear before and
after mobilisation. Figure
courtesy of Sallay et al. [204].
http://en.wikipedia.org/wiki/Tendonhttp://en.wikipedia.org/wiki/Rotator_cuff
-
– 15 –
1.2. Aetiology
Despite their frequency and significance, the aetiology of
rotator cuff tears is still not
fully understood. There are many factors that contribute to the
progression of rotator cuff
disease, these can be grouped into three main areas – extrinsic
mechanisms, intrinsic
mechanisms and overuse [178].
1.2.1. Extrinsic mechanisms
Extrinsic mechanism factors include impingement, acromial shape,
age and smoking.
1.2.1.1. Impingement and acromial shape
In a study of more than 400 patients with rotator cuff tears,
Neer and Poppen state that
95% were caused by impingement associated with lesions, with the
anterior third of the
acromion being principally responsible [176, 177]. Normally, the
cuff rubs against the
anterior edge of the acromion and the coracoacromial arch when
the upper arm is
abducted, flexed and internally rotated. Bigliani et al. [23,
24] related the degree of such
impingements to acromial shape and classified them into three
types – type I, flat
acromions, were seen in 17% of cuff tears; type II, curved
acromions, in 43% of cuff
tears; and type III, hooked acromions, in 39% of cadaveric
full-thickness cuff tears
(Figure 1.3). Further, in a study of more than 200 patients,
Wang et al. showed that the
success of conservative management decreased with changes among
these three types of
acromion shapes – type I responded in 89% of cases, type II in
73% and type III in 58.3%
(P
-
– 16 –
Figure 1.3. The three types of acromions
Type I is a flat acromion that provides plenty of room for the
rotator cuff; type II is a curved
acromion, leaving less room; type III is hooked acromion,
providing little room for rotator
tendon. (Adapted from Jobe CM: Gross anatomy of the shoulder. In
Rockwood CA Jr., Matsen
FA III, editors: The Shoulder, Philadelphia, 1990, WB
Saunders.)
1.2.1.2. Age
Current studies suggest that acromial shape is age-related. Wang
and Shapiro studied the
acromial morphologic characteristics in 272 patients and found a
statistical progression
from type I to type III acromion with age [237]. Furthermore,
Shah et al. provided
histological and radiographic evidence that acromial shape is
acquired through traction
forces rather than congenital abnormalities [210].
Histological analysis has indicated that the incidence and
severity of rotator cuff tears
correlate with aging and with the morphology of the acromion
[182]. An ultrasound
examination of more than 400 asymptomatic volunteers showed that
the frequency
of
rotator cuff tears increased from the youngest group (13%, aged
50-59 years) to the oldest
group (51%, aged 70-79 years) [224]. The same study even
suggested that this high tear
prevalence in asymptomatic volunteers should, to a certain
extent, be regarded as
-
– 17 –
„normal‟ degenerative attrition, not necessarily causing pain
and functional impairment.
Furthermore, a study of 588 patients found that the average age
for patients with no
rotator cuff tear was 48.7 years, rising to 58.7 years for those
with a unilateral tear, and to
67.8 years for those with a bilateral tear [253]. All this
indicates that age might be one of
the mechanisms for rotator cuff tendonopathy.
1.2.1.3. Smoking
Smoking has also been related to rotator cuff disease,
especially in the process of healing.
A 10-year study of 224 patients (95 smokers and 129 non-smokers)
who had undergone
rotator cuff repair indicated that the non-smokers had less pain
and better results
postoperatively than the smokers [153]. This was also confirmed
in a rotator cuff animal
(rat) model, which indicated that nicotine might delay the
tendon-to-bone healing process
[80].
1.2.2. Intrinsic mechanisms
Intrinsic mechanism factors include degeneration, cuff
vascularity and neural factors.
1.2.2.1. Degeneration
Degeneration is the most common histological finding in tendon
ruptures. Investigation
of 891 tendons from acute, subacute and chronic cuff ruptures
and 445 control tendons,
showed that 97% of the 891 ruptured tendons presented
degenerative changes; the
changes were found in only 33% of the control tendons [118].
Consistent with an earlier
study, the degenerative changes existed in all 74 patients with
an Achilles tendon rupture,
suggesting that these changes might result from intrinsic
abnormalities before the rupture
[12].
-
– 18 –
Degenerative changes in tendons might lead to a decrease in
tensile strength and a
predisposition to rupture. They are age-related and are
typically not seen in younger
individuals [21, 130]. They might also be a result of the
accumulation of reactive oxygen
species, thereby leading to oxidative stress and increased
apoptotic cells; this has been
implicated in damage to some other tissues [59]. Indeed, an
excessive percentage of
apoptosis has been detected in torn rotator cuffs compared with
a normal control [230,
256]. This study found evidence that oxidative stress might play
an important role in
tendon degeneration by inducing tenocytes to perform apoptosis
via a metalloproteinase
within the extracellular matrix (ECM) and c-Jun N-terminal
protein kinase within the
intracellular environment [31, 155, 235]. These possible
pathways of tendon
degeneration under oxidative stress is outlined in Figure 1.4
[235].
Figure 1.4. Possible pathways of tendon degeneration under
oxidative stress
Figure courtesy of Wang et al. [235].
-
– 19 –
1.2.2.2. Cuff vascularity
In 1934, Codman [48] identified a so-called „critical zone‟
where cuff rupture usually
occurs, located about 1-1.5cm proximal to the humeral insertion
of the supraspinatus
tendon [143]. However, histologic and immunohistochemical
analyses have reported
relative hyperperfusion at this critical zone [77]. This is
supported by intraoperative laser
doppler flowmetry that showed no hypoperfusion in vivo and
hyperperfusion at the tear
edge [221]; it was thought that this hyperperfusion resulted
from the proliferation in the
subsynovial layer after injury [232]. Based on this,
hypovascularity did not appear to be a
reason for rotator cuff tears. However, a possible role for
hypovascularity might still
exist. In 1970, Rathbun et al. observed that rotator cuff
perfusion reduced markedly when
the arm was fully adducted [190]. In this position, the
supraspinatus is compressed at the
humeral head, which might be a contributory factor to
hypovascularity. Further, the
assessment of vascular patterns after rotator cuff repair showed
that a robust vascular
response after injury decreased with time in the repaired
rotator cuff [69]. This study
seemed to show that rotator cuff blood flow had the potential to
change in different
conditions, such as before or after injury.
1.2.2.3. Neural factors
A microarray analysis of the supraspinatus tendon in rats after
overuse showed increased
expression of a range of glutamate signalling proteins
associated with central nervous
system signalling [6, 167]. Further, an increased concentration
of substance P was found
in diseased rotator cuffs [89]. It could therefore be
hypothesised that neural
overstimulation, in response to overuse, results in the
recruitment of inflammatory cells,
-
– 20 –
in turn leading to painful symptoms and cuff structural
disruption, followed by cuff
damage [97]. However, the theory is still not well
elucidated.
1.2.3. Overuse
Overuse has been implicated in the aetiology of this disease for
a long time and many
studies support this theory. Rees et al. reviewed this as a
mechanical theory [192]. The
study proposed that a tendon without any mechanical load has a
wavelike structure. Al
loaded tendon, however, passes through two stretch regions. The
first is the toe stretch
region; stretching out of its crimped structure, only a small
amount of force is required to
straighten it out [53]. Once the force surpasses this range,
stretching will continue past the
toe region and enter into the second region, thereby becoming a
linear relationship
between strain and force (Figure 1.5) [192]. The strain is
directly taken up by the collagen
fibrils and the force versus strain values are therefore
determined directly by the
physiological properties of the collagen fibrils.
Figure 1.5. The stress versus strain relationship for the
progressive loading of a tendon
This shows three distinct regions (toe, linear and partial
failure) prior to complete rupture.
Approximate stress forces (MPa) and strain values (% strain) are
shown. Figure courtesy of Rees
et al. [192].
http://rheumatology.oxfordjournals.org/cgi/content/full/45/5/508#FIG3#FIG3
-
– 21 –
Tendons are composed of two parts, one for low strains and the
other for higher strains.
The latter part is usually loaded during locomotion and plays an
important role in elastic
energy stores. Strain values of up to 4-8% might be
physiological [53, 122, 151, 161, 173,
213]. Within the physiological range, particularly towards a
higher range, microscopic
degeneration in the tendon might occur, especially with repeated
and/or prolonged
loading. This repeated microtrauma might eventually lead to a
decrease in the mechanical
properties of the tendon [20, 53, 170, 252]. Following such
microtrauma, the
degenerative tendon is easier to partially rupture, and can lead
to a full-thickness tear if
the tendon becomes further weakened [178].
In addition to the above factors, other studies found damage to
the tendon can be caused
by overuse and intrinsic injury, overuse and extrinsic
compression, as well as overuse
alone [40]. Further, without an additional factor, such as
overhead activity, extrinsic
compression alone might be insufficient to cause tendon injury,
supporting the role of
multiple factors in the aetiology of some rotator cuff injuries
[217]. Overuse might
therefore play an important role in the progression of
tendonopathy, with or without
extrinsic and intrinsic factors.
1.3. Pathology
1.3.1. Histology of the normal tendon
A tendon is a tough band of fibrous connective tissue that
usually connects muscle to
bone and is capable of withstanding tension. Healthy tendons are
brilliant white in colour,
have a fibroelastic texture [211] and are composed of parallel
arrays of collagen fibres
http://en.wikipedia.org/wiki/Fibrous_connective_tissuehttp://en.wikipedia.org/wiki/Musclehttp://en.wikipedia.org/wiki/Bonehttp://en.wikipedia.org/wiki/Tension_%28physics%29http://en.wikipedia.org/wiki/Collagen
-
– 22 –
closely packed together (Figure 1.6). Collagen is arranged in
hierarchical levels of
increasing complexity, beginning with tropocollagen, a
triple-helix polypeptide chain,
which combines into fibrils, fibres (primary bundles), fascicles
(secondary bundles),
tertiary bundles, and the tendon itself [171, 211].
Figure 1.6. The anatomy of a normal tendon
Figure courtesy of Sharma & Maffulli [211].
Most collagen are classified as type I; however, small
quantities of other collagen (for
example collagen II, III, IV and V) are also present [47, 215].
The amount of the collagen
fibres is different from tendon to tendon, depending on the
location and function of the
tissue; a different mechanical property could lead to a
different mixture of these collagen
types [25]. Furthermore, not all collagen arrange in a
longitudinal style; collagen fibrils
also transverse each other, providing a good buffer against the
longitudinal, transversal,
horizontal as well as rotational forces during movement and
capacity [42, 113].
-
– 23 –
Fibroblast-like cells in tendons known as tenocytes are the only
cells that populate
tendons; these are arranged sparsely and evenly in a parallel
rows between the parallel
collagen fibrils [194, 203] and respond to cell-matrix
interaction [19, 60, 100, 132]. In
haematoxylin-eosin (HE) staining, fibroblasts appear satellite
when the tendon is cut as a
cross section, that is they lie between the fibres. In
longitudinal sections, fibroblasts are
evenly arranged in parallel rows between the collagen fibrils
and the nuclei are typically
flattened and wavy [164].
1.3.2. Pathology of tendonopathy
The term tendinosis was used for many years to describe
asymptomatic tendon
degeneration with various histologic features [110, 189]. A
number of clinicians still use
the terms tendinitis or tendonitis, implying that the aetiology
of this disease is
inflammatory. Nowadays, the term tendonopathy as a generic
descriptor of the clinical
conditions in and around tendons is more often used, while the
terms tendinosis and
tendinitis are used only after histopathological examination
[148].
Tendons that are commonly affected by tendonopathy include the
supraspinatus and long
head of biceps in the shoulder, the medial and lateral extensors
of the elbow, the patellar,
the Achilles tendon and the posterior tibialis [194]. In most
cases, except for the Achilles
tendon, the site affected is at or near the insertion in a
fibrocartilaginous region of the
tendon [51]. These sites have common features – they are highly
stressed, are often
exposed to repeated strains, including shear or compressive
forces, and are relatively less
vascularised [51].
-
– 24 –
Histological examinations of tendonopathy show loss of fibre
organisation, scattered
vascular ingrowth, decreased fibril diameter, changes in cell
density (both increased and
decreased), cell rounding, an absence of inflammatory cell,
glycosaminoglycan (GAG)
accumulation, hyalinisation, microtears, lipid accumulation and
calcification [15, 43,
118, 195, 223]. Collagen I is predominant in the normal tendon,
alongside small
quantities of other collagen such as collagen II and III [47,
215]; degenerative tendons are
found to contain much higher levels of collagen III [197].
Indeed, the presence of high
levels of collagen III is a characteristic of the repair
process; this will be substituted by
collagen I in normal tendon recovery. Under an electron
microscope it can been seen that
collagen fibrils do not form fascicles, do not connect with each
other and become
segmented [127]. A repair in tendonopathy is therefore not a
total repair; the tendon is
liable to degenerate and it seldom attains the structural
integrity and mechanical strength
of normal, healthy tendon [22, 193, 206].
1.3.3. Healing response
Most of the knowledge of tendon healing after injury can be
divided into two categories –
acute macrotraumatic injury response and chronic microtraumatic
injury response [134].
The former is usually seen in situations of significant tendon
trauma as a result of tissue
loss or damage; cumulative effects usually cause the latter. A
number of animal studies
have focused on the repair process; however, most are concerned
with the acute injury
response, and the chronic response is less understood.
-
– 25 –
1.3.3.1. Acute healing process
The healing response to acute trauma is generally divided into
four overlapping stages. In
the first stage, the injury site is filled with blood clots full
of cytokines that recruit
peripheral cells such as polymorphonuclear leukocytes, platelets
and lymphocytes into
the wound. These recruited cells expand the inflammatory
response and recruit other
types of cells [74, 103].
The next stage starts 24-48 hours later. Macrophages arrive,
perform phagocytosis of
necrotic tissues and secrete the growth factors that stimulate
neovascularisation and form
granulation tissue. Together with other cells, macrophages
release multitype cytokines
such as platelet derived growth factor, epidermal growth factor
and basic fibroblasts
growth factor; these trigger the third stage [174, 184].
The third stage of the response starts after 2 days and is
characterised by protein
synthesis, including collagen proteins and non-collagen
proteins. The tendon, a normally
inactive tissue, becomes a hotbed of cellular activity as the
fibroblasts begin to produce
collagen. These fibroblasts are the mixture of the native
fibroblasts or tenocytes (the
intrinsic response) and those recruited from the epitenon (the
extrinsic response) [201].
Typically, collagen III is deposited followed by the production
of collagen I to substitute
collagen III. The total collagen content of the repairing tendon
is greater than that of a
normal one, but the concentration of the collagen decreases and
the collagen matrix
remains disorganised. This process can last up to 6-8 weeks.
The final stage is associated with the remodelling of the new
tendon that matures step by
step. The matrix becomes denser and more oriented
longitudinally. The cell population
-
– 26 –
and synthetic activity decrease and the proportion of collagen I
to III begins to approach
normal levels. However, as mentioned previously, the remodelled
tissue seldom attains
the structural integrity and tensile strength of a normal,
healthy tendon [22, 73, 104, 245].
1.3.3.2. Chronic healing process
The response of tendons to chronic injury differs from that of
acute injury. In the chronic
process, degeneration is a significant feature. Normal tendons
predominantly contain
collagen I, with a small quantities of collagen III, whilst the
degenerative tendon is found
to posses significantly higher levels of collagen III [148,
197]. After the initial injury,
fibroblasts attempt to repair the injury, and collagen III is
synthesised. In the acute
healing process, the increased collagen III is replaced by
collagen I which is more
resistant to mechanical stress. However, the existing injury
factors keep the level of
collagen III production high, which finally results in the
failure of shift from the
immature to the mature. This gradually weakens the tendon tissue
and eventually
contributes to irreversible tendon injury, causing the
chronically injured tendon to rupture
even at a normal physiologic load [94].
1.4. Diagnosis
Tendonopathy is characterised by symptoms such as the gradual
onset of morning
stiffness in the injured tendon, dysfunction, localised swelling
and sometimes
neovascularisation [30, 121]. Diagnosis is usually based on
patient complaints of pain,
alongside palpation of the tendon, its surrounding tissue and
its insertion. However,
Fredberg et al. found that diagnosis simply based on clinical
examination was, for many
-
– 27 –
patients, incorrect [75]. Therefore, ultrasonography (US) and
magnetic resonance
imaging (MRI), two of the current clinical choices, are
recommended for diagnosis,
especially in cases where shooting pain appears or the injury
seems to be not responding
to treatment [2, 121].
MRI has been widely investigated for the assessment of shoulder
joint diseases as
appropriate surface coils are available [92]. It has been used
on athletes‟ posterior glenoid
impingement with a typical, sports-related tendon injury [227].
MRI also has been used to
detect or exclude complete rotator cuff tears with reasonable
accuracy, and it is also
suitable to diagnose further pathologies of the shoulder joint
[92]. MRI arthrography is
valuable in confirming subtle anatomic details and in further
improving the
differentiation of rotator cuff diseases [92].
Compared with MRI, US has several significant advantages.
Firstly, the internal
architecture of the examined tendon is more clearly shown than
in MRI [116]. Secondly,
US has nearly no limitations in examining the site of injured
tendon and any site of
reported pain can be related with real-time scanning, providing
a side-to-side comparison
[66, 76]. Thirdly, US can present the neovascularisation
associated with this disease. It is
also able to highlight which features of the tendon are as a
result of chronic injury. These
include any thickening of the tendon, discontinuity of fibres,
focal hypoechoic
intratendinous areas, loss of fascicle organisation,
intratendinous focal calcification,
partial or complete ruptures, as well as any thickening of the
hypoechoic paratenon with
poorly defined borders, bursitis and adherences between the
epitenon and paratenon [27,
71, 86].
-
– 28 –
1.5. Treatment
Treatment of rotator cuff tears is difficult due to the lack of
understanding of the healing
response to chronic trauma. Treatment is therefore based on the
assumption that a tendon
responds to chronic injury factors in the same way as it does to
an acute injury. The goal
of treatment for rotator cuff disease is to promote healing,
eliminate pain and restore
shoulder function. Current treatment options are twofold –
conservative and surgical.
1.5.1. Conservative treatment
Conservative treatments are often the priority when the symptom,
such as restricted
shoulder function or pain, first appears. Treatments include
rest, non-steroidal
anti-inflammatory drugs (NSAIDs), corticosteroid injection,
exercise and physical
modalities.
1.5.1.1. Rest
In the early stage, relative rest, therefore avoiding mechanical
overload, is an effective
choice to halt the continuing injury, thereby giving the tendon
a chance to repair itself.
1.5.1.2. NSAIDs
Anti-inflammatory drugs are used quite commonly to control pain
and inflammation.
However, the use of these drugs still remains controversial. In
the acute stage, it is
debatable whether blocking the acute inflammatory response is
helpful or not, while in
the chronic stage, it is argued that there is little or no
inflammatory infiltration [244].
Nevertheless, the drug might have an analgesic effect, possibly
independent of the
anti-inflammatory action. Wang & Shapiro found pain was
relieved in five out of nine
controlled studies using NSAIDs in the treatment of tendonopathy
[237]. The use of
-
– 29 –
NSAIDs in tendon injuries on animals has also been studied. Some
showed the drug
increased tendon tensile strength, while others presented a
decrease in mechanical
property [72, 129, 234].
1.5.1.3. Corticosteroid injections
Steroid injections are used in the treatment of tendonopathy for
anti-inflammation and
pain relief. Their usage can effectively decrease the pain at
the site of injury and can
recover the range of motion exercises to prevent stiffness [26,
55]. However, the
proportion of recurrence is high and, as with NSAIDs,
corticosteroid injections remain
controversial. The absence of inflammatory cells, at least in
the later stages of
tendonopathy, provides no rational basis to treat the
tendonopathy with either NSAIDs or
corticosteroid injection. In addition, this treatment was found
to have no effect on the
disease [162] and even to weaken the mechanical property of the
tendon [226, 248].
1.5.1.4. Exercise
Exercise therapy has been accepted as one of the mainstays of
conservative treatment for
chronic tendon injury and is important in both prevention and
treatment of this disease.
Studies show that exercise plays a role in prospective,
randomised trials in athletic
patients [5, 150]. Mechanical exercises might stimulate the
metabolism of the tenocyte
and promote increased mechanical property, improving the
strength and flexibility of the
shoulder [107, 119]; an immobilised tendon could lose up to 40%
of it‟s ground substance
[179, 181]. However, it is argued that there is little evidence
of a positive effect on
clinical outcomes, such as relief of pain or improvement of
function [251].
-
– 30 –
1.5.1.5. Physical modalities
Physical modalities such as therapeutic ultrasound, laser and
heat have been frequently
performed to stimulate collagen production, improve the
mechanical properties of the
healing tendon, and alter the local vascular supply to relieve
pain [65, 93, 108, 180, 191].
Evaluation of the success of these conservative treatments shows
it depends on the
different treatment protocols and the different criteria for the
selection of patients; the
percentage varies from less than 50% to about 80% [44, 88, 107,
168, 205, 222].
However, current reviews of these studies show a decrease of the
initial successful
percentage due to recurrence on longer follow-ups. The high
levels of failure or
recurrence of conservative treatments indicate that rotator cuff
tendonopathy is not
self-limiting and that current conservative treatment needs to
be improved and developed.
1.5.2. Surgical treatment
Surgery is often considered the last option in the treatment of
tendonopathy [9]. Patients
who exhaust all non-operative options and fail to improve after
a period tend to be
subjected to the surgery. This period might last between 6-18
months [62, 177]; however,
in some conditions, earlier surgery is indicated, for example,
in an acute full-thickness
tear in a younger patient with loss of function [231].
The aim of surgical treatment is to alleviate or eradicate pain
and correct functional
deficit [231]. In the operation process, the rupture in the
tendon needs to be repaired to
restore the continuity of the tendon, that is, the surgery aims
to provide a more suitable
environment for healing of the injured tendon. Removal of a part
of the tendon does not
influence the healing process. For example, the mechanical
property increased when the
-
– 31 –
central third of canine patellar tendons were removed [36, 39]
and greater cross-sectional
diameters were found in rabbit Achilles tendons after tenotomy
[135].
Surgery to repair torn rotator cuffs date back to 1911 [49]. In
1972, Neer reported his
outcomes after studying anterior acromioplasty combined with the
release and repair of
torn tendons [176], and emphasised four findings – release of
the cuff in order to mobilise
the tendon-muscle unit and a strong attachment to the greater
tuberosity, subacromial
release via the division of the coracoacromial ligament and
acromioplasty, painstaking
repair of the deltoid, and appropriate postoperative
rehabilitation therapy consisting
chiefly of passive movements [68]. These principles are widely
accepted and have
contributed to an improvement in surgical techniques. Early
primary anatomic repair and
carefully controlled rehabilitation after surgery are the
principle treatments for nearly all
rotator cuff tears [185]. Based on this, many surgical
techniques have been developed to
restore the structure and function of the damaged rotator cuff,
such as acromioplasty,
tendon to bone trough repair, and extensive tendon mobilisation
techniques.
1.5.2.1. Partial-thickness tears
The treatment for symptomatic partial-thickness rotator cuff
tears is controversial.
Regardless of a decompression for primary impingement or a
stabilisation procedure for
instability, correction of the underlying pathology should be
the initial focus [231]. There
are several options, including leaving the partial tear alone or
addressing it with either a
debridement or a repair, either open or arthroscopically [10,
62, 160, 241]. At present,
acromioplasty seems efficient in treating partial-thickness
tears [82, 202].
-
– 32 –
1.5.2.2. Full-thickness tears
The choice of surgical management for full-thickness rotator
cuff tears that have failed
with conservative treatments is multifactorial. Traditionally,
the size of the tear is the
predominant factor, but the position of the tear, chronicity,
fatty infiltration, and scarring
also play a role in determining appropriate treatment [231];
patients‟ symptoms are
another significant consideration [231]. Tendon repair is the
mainstay of the treatment,
with anterior acromioplasty as a common adjunct. Numerous open
and arthroscopic
surgeries have now been performed for the repair of
full-thickness rotator cuff tears
which have relied on adequate mobilisation of the cuff edges,
particularly the
arthroscopic techniques [64, 83, 98, 99]. If the tear is massive
and cannot be repaired,
partial repair, local muscle advancement, or distant muscle
transfer can be performed [35,
85, 165, 199].
Since 1987, when the arthroscope was first used for the surgical
treatment of rotator cuff
tears [61], arthroscopic techniques have improved surgical
management. Compared with
open surgery, arthroscopic techniques enable the surgeons to
find the extrinsic
impingement signs with higher probability. Under the
arthroscope, the subacromial
„roughness‟ such as bursal thickening and subacromial spurs that
need to be addressed
surgically in the initial cuff repair can be seen more regularly
than open surgical treatment
[246].
Acromioplasty is performed to enlarge the anterior subacromial
space to accommodate
the rotator cuff and repair tissue as well as relieve the pain,
even if the rotator cuff repair
fails to heal. It has been reported that arthroscopic
acromioplasty results in adequate
-
– 33 –
decompression comparable to the open surgery manner [82, 140,
200]; anterior
acromioplasty, however, does not alter the functional outcome
nor the rate of clinic
recurrence after repair [133]. Goldberg et al. reported that 27
full-thickness cuff repairs
without acromioplasty avoided the possibility of deltoid
detachment, and altered deltoid
mechanics, anterior-superior instability and tendon scaring to
the cancellous undersurface
of the acromion [87]. They concluded that statistically
significant improvements in
shoulder comfort and specific shoulder functions could be seen
in patients with
full-thickness rotator cuff tears after repair without
acromioplasty.
1.6. Summary
Rotator cuff tendonopathy, resulting in the loss of mechanical
strength of a tendon, is a
serious health problem affecting many people. In spite of its
clinical significance, our
knowledge about tendonopathy is still very poor. Current
theories are not concise enough
to explain why the tendon suffers degeneration, nor the
histological characteristic of this
disease. Furthermore, neither of the two current treatment
options, conservative or
surgical, can repair the tendon to the same structural integrity
and tensile strength of a
normal tendon. There is therefore a need for a better
understanding of this disease in order
to improve treatment options.
-
– 34 –
Chapter 2
Hypothesis and Aims
-
– 35 –
2. Hypothesis and aims
There is a high recurrence rate of tendonopathy due to tendon
degeneration. Typical
tendonopathy changes include rounding of nuclei, adipose tissue
deposit, vascular
hyperplasia, variation in cellular population and, most
importantly, disruption of the
ECM [15, 43, 118, 195, 223]. Tendon ECM is composed largely of
type I collagen; this
provides structural integrity and accounts for mechanical
strength. The disruption of
collagen fibres, characterised by the loss of longitudinal
alignment and the fragmentation
of collagen bundles, directly decreases the mechanical property
of tendons and might
eventually result in tendon rupture.
Tendon cell death (apoptosis) has been linked to degeneration of
tendon tissue. Recent
studies suggest that apoptosis plays an important role in the
development of tendonopathy
[6, 10, 12, 13]. Excessive apoptosis was found in degenerative
human tendon tissue and
was considered to be responsible for cell loss and decreased
collagen synthesis, resulting
in the progression of tendon degeneration [10, 12]. In addition,
another type of
programmed cell death – autophagic cell death – is found to play
an important role in
degenerative diseases such as neurodegeneration, muscular
disorder and liver conditions
[4, 5, 8, 11]. Therefore, autophagic cell death may also exist
and be responsible for the
tendon degeneration to a certain degree. These two types of cell
death possibly lead to the
variation of cell number in the ECM, which may be associated
with the disruption of the
ECM. Furthermore, in torn tendons, tendon cells were found to
differentiate into
myofibroblasts, that is the cells with a contractile ability;
this was not the case in normal
-
– 36 –
tendons [3, 9]. All of these cellular events suggest that the
fate of tendon cells might be
related to the process of tendon degeneration.
2.1. Hypothesis
This study was based on three hypotheses, namely that:
Autophagic tendon cell death occurs in a torn human tendon.
Two types of cell death in the injured tendon, autophagic cell
death and apoptosis,
play a role in the progression of tendonopathy in rotator
cuff.
Cell differentiation into myofibroblasts in the injured tendon
plays a role in the
progression of tendonopathy in rotator cuff.
2.2. Aims
The aims of this study were therefore to:
Determine if variety of cellularity was related to the
disorganisation of the fibril
matrix – semi-quantitative microscopic analysis was used to
determine the
relationship between cell density and the fibril structure with
different degrees of
degeneration. This is discussed in Chapter 4.
Determine if rotator cuff tendonopathy was related to apoptosis
– TUNEL assay
was used to confirm the existence of apoptosis in torn rotator
cuff and
semi-quantitative microscopic analysis was used to determine the
relationship
between the percentage of apoptosis and the fibril structure
with different degrees
of degeneration. This is discussed in Chapter 5.
-
– 37 –
Determine if rotator cuff tendonopathy was associated with
autophagic cell death –
immunohistochemistry was used to confirm the existence of
autophagic cell death
in torn rotator cuff and semi-quantitative microscopic analysis
was used to
determine the relationship between the percentage of autophagic
cell death and the
fibril structure with different degrees of degeneration. This is
discussed in Chapter
6.
Determine if cell differentiation was associated with the
process of tendon
degeneration – immunohistochemistry was used to confirm the
existence of
myofibroblasts in the torn rotator cuff and semi-quantitative
microscopic analysis
was used to determine the relationship between the percentage of
myofibroblasts
and the fibril structure with different degrees of degeneration.
This is discussed in
Chapter 7.
-
– 38 –
Chapter 3
Materials and
Methods
-
– 39 –
3. Materials and methods
3.1. Materials
A number of different materials were used in the study. They are
outlined below.
3.1.1. Chemical reagents
The chemical reagents used in the study are listed below.
Chloroform [Merck, VIC, Australia].
3% hydrogen peroxide [chemsupply, Gilman, SA, Australia].
DePeX mounting medium [BDH Chemicals Ltd, Poole, England].
Diaminobenzidine (DAB) [k3468, DAKO, Glostrup, Denmark].
Diethylpyrocarbonate (DEPC) [Sigma Chemical Co. St. Louis, Mo,
USA].
Eosin [BDH Chemicals Ltd, Poole, England].
Ethanol [BDH Chemicals Ltd, Poole, England].
Foetal bovine serum (FBS) [Commonwealth Serum Laboratories].
Haematoxylin [Sigma Chemical Co. St. Louis, Mo, USA].
Paraffin wax [BDH Chemicals Ltd, Poole, England].
Phosphate-buffered formalin [BDH Chemicals Ltd, Poole,
England].
Tris (hydroxymethyl) aminomethane hydrochloride (Tris-HCl)
[Sigma Chemical
Co. St. Louis, Mo, USA].
Xylene [BDH Chemicals Ltd, Poole, England].
3.1.2. Enzymes
The enzymes used in the study are shown below.
-
– 40 –
Proteinase K [BDH Chemicals Ltd, Poole, England].
Trypsin [ICN Pharmaceuticals, Inc. Costa Mesa, USA].
3.1.3. Antibodies
The antibodies used in the study are shown below.
Anti--SMA primary antibody [M0851, DAKO, Glostrup, Denmark].
Anti-ubiquitin antibody [Z0458, DAKO, Glostrup, Denmark].
Second antibody [K0675, DAKO, Glostrup, Denmark].
3.1.4. Commercial kit
The commercial kit used in the study was the In-situ Cell Death
Detection-AP Kit
[1684817 Roche Diagnostics GmbH, Mannheim, Germany].
3.1.5. Buffer and solutions
A number of different buffers and solutions were used. These are
outlined below.
95% ethanol: 100% ethanol 950ml/L. Solution was made with
DEPC-treated water
and stored at -20oC.
70% ethanol: 100% ethanol 700ml/L. Solution was made with
DEPC-treated water
and stored at -20oC.
Alcohol/xylene (1/1): Alcohol 1 volume, xylene 1 volume.
Solution was mixed by
gentle inversion and stored at room temperature
DEPC water: DEPC 2ml, absolute ethanol 20ml. DEPC was dissolved
in ethanol
and mixed with double distilled water (DDW) to make 2L,
incubated at room
-
– 41 –
temperature in a fume hood overnight, then autoclaved and stored
at room
temperature.
1% eosin: 20g eosin was dissolved in 2L 95% alcohol and stored
at 4oC.
Gills haematoxylin (1.5L): ethylene glycol 375ml, haematoxylin
6.0g, sodium
iodate 0.6g, aluminium sulphate 42.8g, glacial acetic acid 50ml.
Dissolved in
1075ml DDW and stored at room temperature.
Permeabilisation solution (TUNEL) 100ml: 10% triton-X 1ml, 0.1%
sodium citrate
99ml. Dissolved in reagents and stored at room temperature.
10% phosphate buffered formalin: Formalin 100ml/L. Diluted in
1xPBS and stored
at room temperature.
20% FBS: DMEM-F/12 400ml, FBS 100ml, L-ascorbic acid 0.5ml,
penicillin-streptomycin (2x) 2.5ml. Solution mixed and stored at
4oC.
PBS (1x): 10xPBS 100ml. Solution mixed with DEPC water,
autoclaved and stored
at room temperature.
Proteinase K: Proteinase K 1L, 0.1 M Tris 1ml, EDTA (pH=8.0)
0.05ml. Solution
was fresh and was stored on ice before use.
10mM Tris-HCl (100 ml): 2M Tris-HCl 50L. Diluted in 100ml DEPC
water,
autoclaved and stored at room temperature.
Scott‟s tap water: Sodium bicarbonate 7.0g. magnesium sulphate
40g, tap water 2L,
crystal thymol (a few crystals). Mixed and stored at 4oC.
-
– 42 –
Tris-buffered saline (TBS) (10x): Tris 30.25g, NaCl 42.5g, HCl
-17ml, Milli Q
water 500ml pH 7.6 in solution (pH=7.6). Mixed and stored at
room temperature.
TBS (1x): 10xTBS 100ml, Milli Q water 900ml. Solution mixed and
stored at room
temperature.
3.1.6. Other materials
Other materials used in the study are shown below.
Aperio‟s 120-slide ScanScope XT system [Aperio Technologies,
Vista, CA, USA].
Hettich Rotofix 32A Benchtop Centrifuge [HD Scientific Supplies
Pty Ltd, NSW,
Australia].
NIS-elements image software [Nikon, Japan].
p-xylene-bis-pyridinium bromide (DPX) permount [14208-10-7
Sigma-Aldrich,
Castle Hill, NSW, Australia].
Reichert-Jung 2030 microtome [Meyer Instruments Inc. TX,
USA].
Tissue Tek vacuum infiltration processor [Sakaraus Firetek, USA
Inc, USA].
3.2. Methods
3.2.1. Human sample collection
Sample collection was approved by the human ethics committee of
UWA. Rotator cuff
tendon samples were harvested from 26 male patients and four
female patients (age range
33-74 years; average age 57 years) with rotator cuff tears who
were undergoing shoulder
surgery. Patient information included age, sex, lateral side and
duration of the disease
(Table 3.1). The ruptured rotator cuffs were obtained 2-84 weeks
after rupture. The
-
– 43 –
samples were sourced from the ragged edges of the torn tendons
that were trimmed prior
to surgical repair. No additional tissue was obtained. The
samples were fixed, embedded
and cut into 5m thick sections for HE staining,
immunohistochemical staining for
ubiquitin and alpha-smooth muscle actin (-SMA), and TUNEL
assay.
Table 3.1. Patient data
All data were presented as mean ± SEM.
No. patients (F/M) Age (years) Duration of symptoms (mths)
Lateral (right / left)
30 (4/26) 57±2 12±2 22/8
3.2.2. Tissue preparation
The samples harvested during surgery were fixed in 10%
phosphate-buffered formalin for
at least 24 hours. All the tissue samples were then processed in
a Miles Scientific Tissue
Tek vacuum infiltration processor overnight at 37oC. They were
then put in 70% ethanol
for 1 hour, 95% ethanol for 1 hour, 100% ethanol twice for 1
hour each, 100% ethanol
twice for 30 minutes, chloroform twice for 2 hours, chloroform
once for 1 hour, and
finally molten wax at 60oC twice for 2 hours, followed by being
embedded in paraffin.
The tissues were then cut into 5m thick sections by a
Reichert-Jung 2030 microtome,
and floated on a water bath at 40oC; they were then picked up
onto slides and dried
overnight at 37oC.
The paraffin-embedded sections were dissolved by treatment in
three solutions of 100%
xylene (RNase free) for 2 minutes each. They were then
rehydrated by successive
immersion in three changes of 100% ethanol, 95% ethanol and 70%
ethanol for 1 minute
each. Finally, the slides were placed in DEPC-treated water.
-
– 44 –
3.2.2.1. HE staining
The sections were then immersed in Gills haematoxylin for 3
minutes and rinsed in tap
water to remove any excessive stain. The slides were then placed
in Scott‟s tap water for 2
minutes and rinsed again in running tap water for 3 minutes.
They were then immersed in
70% ethanol and 90% ethanol for 3 minutes each and
counterstained with 1% eosin for 1
minute. Finally, dehydration was carried out by immersion in the
following solutions in
succession for 3 minutes each – 100% ethanol (three solutions)
and absolute
alcohol/xylene (1/1). The sections were cleared in xylene (3
minutes, 3 times) and the
slides were mounted in DePeX and left to dry overnight.
3.2.2.2. Immunohistochemistry
Granular cytoplasmic ubiquitin inclusion by immunohistochemistry
can be used as a
measure to detect autophagic cell death in human pathologies on
tissue sections [123,
125, 157, 166, 216]. After removal of paraffin and rehydration
of the sections, slides were
digested in 0.1% trypsin for 20 minutes, and were then washed by
Milli Q water.
Endogenous peroxidase was quenched with 3% hydrogen peroxide for
5 minutes. The
sections were then washed with TBS for 5 minutes. Next, 20% FBS
was used to block
non-specific sites on the tissues for 30 minutes and the tissue
sections were incubated
with anti-ubiquitin antibody (1:200) for 3 hours at room
temperature. Negative controls
were prepared by omitting the primary antibody.
TBS was then used to wash the tissues. Then the second antibody
was added into the
tissue for 15 minutes, the tissues were washed by TBS (5
minutes, 3 times), then stained
with DAB for 10 minutes, and were then rinsed off with TBS.
Cells positive for
-
– 45 –
immunohistochemistry showed brown. Finally, the tissues were
counterstained in
Mayer‟s haematoxylin, dehydrated through graded alcohol to
xylene, and mounted with
DPX permount.
Immunohistochemical staining for myofibroblasts was also
performed according to the
same protocol with an anti--SMA primary antibody (1:50). Smooth
muscle cells
surrounding blood vessels were used as internal positive
control.
3.2.2.3. TUNEL assay
TUNEL assay was used to identify apoptotic cells by labelling
nuclear DNA fragments.
The procedure of TUNEL assay is described as follows. After
removal of paraffin and
rehydration of the sections, sections were incubated with
proteinase K (20mg/ml in
10mM Tris/HCl, pH 7.4-8.0 for 15-30 minutes at 21-37oC), then
incubated in 0.1% Triton
X-100 in 0.1% sodium citrate for 8 minutes, and rinsed off twice
with PBS. The TUNEL
reaction was prepared in accordance with the instructions from
the In-situ Cell Death
Detection-AP Kit. 50L TUNEL reaction mixture (enzyme solution:
label solution = 1:9)
was added onto each slide; 50L label solution without enzyme
solution was added to the
negative control slide. The slides were placed in a humidified
chamber for 60 minutes at
37oC.
Next, the slides were rinsed three times in PBS, and 50L
Convert-AP (provided in kit)
was added to each slide, followed by another incubation in a
humidified chamber for 30
minutes at 37oC. Then they were rinsed again three times in PBS.
DAB was added for
colour development, and the slides were incubated for 10 minutes
at room temperature.
Cells positive for TUNEL assay showed brown. Finally, they were
counterstained in
-
– 46 –
Mayer‟s haematoxylin, dehydrated through graded alcohol to
xylene, and mounted with
DPX permount.
3.2.3. Evaluation of fibril matrix degeneration
All slides were scanned by Aperio‟s 120-slide ScanScope XT
system. Aperio‟s digital
pathology information management software and NIS-elements image
software, which
were able to zoom freely between 0-40 times magnification, were
used to analyse the
digital images. All of the sections were examined by the
histopathologists and classified
according to the following criteria [149, 220, 223]:
Grade 0 – normal tendon, straight parallel packed fibres, some
with slight waviness.
Grade 1 – slight changes, some separation of fibres, increased
waviness, slight loss
of parallel arrangement, discontinuous fibres.
Grade 2 – moderate changes, larger separation of fibres,
increased waviness,
moderate loss of parallel arrangement with deterioration of
fibres.
Grade 3 – severe changes, total loss of fibre structure and
hyalinisation, total loss of
parallel arrangement, no discernible orientation of fibres.
Under x20 magnification, 30 fields (0.183mm2 each) (Figure 3.1)
were randomly selected
from each section. It was difficult to classify the ECM in the
section detected by
immunohistochemistry or TUNEL assay, therefore the same area in
the HE-staining
section from the same sample was used (Figure 3.1).
-
– 47 –
Figure 3.1. ECM classification
The same areas in the HE-staining section (red) were used to
classify the ECM in the section
detected by immunohistochemistry or TUNEL assay. Each green box
presented one chosen area
for analysis (0.183mm2 each).
The process of grading the collagen matrix structure was
performed by two independent
individuals. The boundary between the grades has some impact on
the assessment, but the
final assessment was consistent. The respective numbers of
positive cells for apoptosis,
autophagic cell death and myofibroblasts, as well as the total
tenocyte number in each
chosen field, were counted. The percentage of positive rate was
calculated as: (positive
cells number / total cell number) x 100. In addition, cell
density (cells/mm2) was also
reported as: number of the total cells from the chosen field /
the area of analysis.
All the values in the test and figures were expressed as mean ±
SEM; statistical analysis
among the different graded areas in the samples was performed
using analysis of variance
(ANOVA) [SPSS 16.0] [125, 256]. The confidence limit was
predetermined at a
probability level of p
-
– 48 –
Chapter 4
Results: the variety of
cellularity in the
disruption of the fibril
matrix
-
– 49 –
4. Results: the variety of cellularity in the disruption of
the
fibril matrix
Rotator cuff tendonopathy, resulting in the loss of mechanical
strength of tendon, is
considered to be a degenerative disorder characterised by the
disruption of the fibril
matrix. The aim of this study was to investigate the
relationship between this disruption
and the variety of cellularity in the degeneration of rotator
cuff. Tendon tissues were
collected from 30 patients suffering from rotator cuff tears and
HE staining was used to
analyse the degree of degeneration of their fibril matrix
structure. The distribution of cell
density was assessed, and was correlated with the disruption of
fibril matrix, which was
graded on a scale of 0-3 using a customised scoring system.
The torn human rotator cuff tendon shows characteristics of
degeneration according to
the number of inflammatory cells. The total cell density varied
among the fibril matrix,
with maximal cell population (674±27mm-2
) in the Grade 1 section of the matrix, and
with minimal cell population (395±17mm-2
) in the Grade 3 section. A significant
difference existed between all four grades in the matrix. The
results indicated that a
variety of cellularity might be closely related to damage of the
ECM structure.
Tendons possess a highly organised fibrillar matrix; this is
maintained by resident
tenocytes through a continuous process of matrix remodelling
[194]. During chronic
injury due to overuse or microtrauma from repetitive loading,
the remodelling for repair
is probably mediated by resident tenocytes [212]. However, the
damaged tendon heals
very slowly and seldom attains the structural integrity and
mechanical strength of a
-
– 50 –
normal, healthy tendon [22]. The immature collagen that cannot
be shifted to the mature
leads to a decrease in mechanical property and an increase in
the risk for rupture.
Furthermore, chronic injuries also influence the function of
tendon cells, affecting the
rate of collagen synthesis. Eventually the tendon with a chronic
injury presents with
disruption of collagen fibre, one of the most important features
of tendonopathy.
The initial phase of this research used a semi-quantitative
classification to investigate the
histopathology of the fibril matrix structure in order to find
out the relationship between a
variety of cellularity and different degrees of degenerative
fibril matrix structure.
4.1. General description
The ruptured rotator cuff samples demonstrated in HE staining
revealed a highly variable
collagen structure and cellular morphology. Areas where the
fibres were highly organised
were also the areas where the most cells exhibited normal
spindle shapes and lined in a
parallel pattern (Figure 4.1 A, A1, A2). Conversely, the cells
in the areas where the fibril
matrix were disorganised were more likely to present rounded in
shape and lined
randomly (Figure 4.1 B-D). The number of rounded and plump
nuclei was numerous
compared to the normal spindle-shaped nuclei. In addition, there
was no presence of
neutrophils, macrophages or lymphocytes, and there was an almost
total absence of
inflammatory cells.
-
– 51 –
Figure 4.1. ECM grades
A. Grade 0, representing nearly normal. B. Grade 1. C. Grade 2.
D. Grade 3, showing the most
abnormal. A1, B1, C1, D1 The boxed areas (black) in Figure A, B,
C, D are shown at a higher
magnification. A2, B2, C2, D2 The boxed areas (black) in Figure
A1, B1, C1, D1 are shown at a
higher magnification. Bar is 50m in all pictures.
Further, proliferation of small blood vessels was seen in the
majority of samples (21 out
of 30), the normal parallel pattern of the blood supply was lost
and the vessels seemed
randomly oriented (Figure 4.2). A number of the small vessels
were surrounded by
uncharacteristic circular patterns of collagen matrix. The edges
of the tears were lined by
a layer of fibroblasts oriented at an angle to the normal
orientation of the tendon fibre and
fibroblast-like cells, and paralleled to the edge of the torn
tendon (Figure 4.3). These
layers were frequently in hypercellularity and consisted of
rounded and / or
spindle-shaped cells.
-
– 52 –
Figure 4.2. Blood vessels in torn rotator cuff tendons
Blood vessels are arrowed.
Figure 4.3. The torn edge of a tendon
It can be seen where tendon cells have formed a dense layer of
cells.
-
– 53 –
Collagen structure was noted as a lack of normal parallel
pattern, and was graded from
0-3 based on a semi-quantitative four-point grading scale
(Figure 4.1 A-D). A mixture of
at least two grades was observed from each section, and no slide
was homogenous with a
single grade in all chosen areas. In the 900 chosen fields (30
fields from each sample),
there were 57 fields in the Grade 0 section of the matrix, 246
in the Grade 1 section, 358
in Grade 2, and 239 in Grade 3. In the Grade 0 section, nearly
all the tenocytes were lined
in parallel orientation with spindle-shaped nuclei. As the grade
for the collagen matrix
structure increased, the distribution of tendon cells, mostly
with rounded or
plump-shaped nuclei, lost the parallel arrangement throughout
the tissue and had no
discernible pattern (Figure 4.1 A-D).
4.2. Comparisons
4.2.1. Normal fields vs degenerative fields
In order to investigate the distribution of tendon cells in
tendonopathy, the chosen fields
were divided into two groups. Group I consisted of those fields
with a normal
arrangement of fibril matrix, namely the areas that were graded
0 (57 fields). Group II
was composed of the remaining fields (843 fields) that showed
cell degeneration, from a
slight change to total deterioration. The mean cell density in
areas with absence of
degeneration was 555±41, while the fields with an abnormal
fibril structure presented a
comparatively lower result (553±12) (Figure 4.4). It can
therefore be determined that no
significant difference existed between these two groups
(P=0.658).
-
– 54 –
Figure 4.4. Comparison of cell density in normal fields and
degenerative fields
Mean ± SEM. * p
-
– 55 –
Figure 4.5. Comparison of cell density in different ECMs
Mean ± SEM. * p
-
– 56 –
such as vacuolisation [118, 134]; this was suggested to drive
the tendon cells to have a
different metabolic activity from normal cells.
Besides cell function, the number of cells in the degenerative
tendon was also found to be
significantly different from that in the normal tendon, another
feature of tendon
degeneration [15, 43, 118, 195, 223]. From the Grade 0 section
with a normal aspect, the
cell density increased to reach a peak in the Grade 1 section,
and then dropped in the
Grade 2 section and hit the bottom in the Grade 3 section with
the worst degeneration
(Figure 4.4). The increased cell numbers in the Grade 1 section
was considered a result of
repair – the injury drove the tissue to proliferation to
increase collagen synthesis [212].
However, the chronic injury did not stop damaging the tendon
tissue, thereby
deteriorating the fibril matrix structure. Thus, many cells did
not survive in such harsh
conditions and cell density began to decrease.
Most tendons derive nutrition from the synovial sheath [211].
Blood vessels coming from
the muscle-tendon junction or tendon-bone insertion also provide
some part of nutrition
[146]. However, the blood supply to the tendon is considered
poorer than that in muscle
or bone. In a normal tendon, the vessels are not present within
the fascicles of tendon. In
this study, many samples (21 in 30) presented proliferation of
small blood vessels; their
normal parallel pattern was lost and they seemed randomly
oriented (Figure 4.2). An
electron microscope found abnormal structures in these vessels,
including thick basal
lamina, several layers of lining cells with contractile
elements, lipid vacuoles and rich
endoplasmic reticulum [118]. Therefore, it is argued whether
these small vessels
contribute to repair.
-
– 57 –
In 900 chosen fields, most (358 fields) lost their paralleled
arrangement, some (239
fields) even lined in a no discernible pattern, only 57 fields
looked normal and 246 fields
presented nearly normal. It was supposed that most of samples
were taken from the
patients whose rotator cuff were in moderate or even severe
degeneration, and that
therefore the entire spectrum of degeneration was not
represented in these samples.
In summary, this histological study enabled us to look inside
the cellular response of
tendon cells after injury and lead us to further research to
investigate the relationship
between the fibril matrix and tendon cells in tendonopathy.
-
– 58 –
Chapter 5
Results: the role of
apoptosis in the
disruption of the fibril
matrix
-
– 59 –
5. Results: the role of apoptosis in the disruption of the
fibril matrix
Rotator cuff tendonopathy is considered a degenerative disorder
characterised by the
disruption of fibril matrix. One aim of this study was to
investigate the relationship
between the disruption of fibril matrix and apoptosis in the
degeneration of rotator cuff.
Tendon tissues were collected from 30 patients suffering from
rotator cuff tears. A
TUNEL assay was performed to detect apoptosis. HE staining was
used to analyse the
degree of degeneration of fibril matrix structure in torn human
tendons. The distribution
of apoptosis was assessed, and was correlated with the
disruption of fibril matrix, which
was graded from 0-3 using a customised scoring system. The
percentage of apoptosis
significantly increased as the fibril matrix degenerated – the
percentage was the lowest
(21.4±2.2%) in the Grade 0 section of the matrix, increased in
the Grade 1 section
(26.0±1.4%) and became higher in the Grade 2 section
(31.0±1.2