Embed Size (px)
Citation preview

Pathologic Findings in Total Esophagectomy Specimens After lntracavitary and External-Beam Radiotherapy
BRIAN BERRY, MD,*,t ROBERTA R. MILLER, MD,*,t ANDREW LUOMA, MD,t,* BILL NELEMS, MD.t.3 JOHN HAY, MD.§.II AND ALBINO D. FLORES, MD,§.II
Pathologic findings in 21 esophagectomy specimens from patients having preoperative combined intra- cavitary radiotherapy (ICR) and external-beam radiotherapy (EBR) are described. Eleven patients received 1500 cCy ICR and 4000 cGy EBR (Group 1) and ten patients received 1500 cGy plus 2000 to 3000 cGy EBR (Group 2). Effectiveness of radiotherapy was expressed as the ratio between depth of radiation effect and depth of tumor invasion. Depth was expressed as one of four levels: Level 1, not deeper than the muscularis mucosa; Level 2, involving but not deeper than submucosa; Level 3, involving but not deeper than muscularis propria; and Level 4, involving periesophageal soft tissue. The depth of radiation damage to tumor cells was comparable hetween the two groups. However, residual tumor was present in the periesophageal tissue in only one of 11 patients after high-dose EBR compared to eight of ten patients with lower dose EBR (P < 0.01, chi-square test). A ratio of one between radiation effect and depth of tumor invasion was present in six patients receiving high-dose EBR and one patient receiving lower dose EBR (P < 0.05). The authors conclude that ICR combined with EBR affords good local tumor control in the majority of patients. Higher doses of EBR give a better radiation effect in deeper layers of the esophageal wall. The ratio between depth of radiation effect and tumor invasion provides a simple and objective approach to the pathologic analysis of esophagectomy specimens.
Cancer 64:1833-1837, 1989.
WIDE RANGE OF THERAPEUTIC MODALITIES have A been used in the treatment of cancer of the esoph- agus, including surgery, radiotherapy, chemotherapy,' and endoscopic laser therapy.* However, the outcome remains discouragingly poor. Palliation is the treatment intent for most patients although there is a small number for whom surgical cure is still possible. Surgical intervention' and external-beam radiotherapy4 (EBR) have been the main- stays of treatment with either palliative or curative intent, although both have disadvantages related to morbidity and recurrence, respectively.
Options for radiation management of this disease in- clude both intracavitary and external sources. Historically, intracavitary radiation was technically difficult and placed medical personnel at high risk of radiation e x p ~ s u r e . ~ , ~
From the tVancouver General Hospital. IlCancer Control Agency of British Columbia, and University of British Columbia, *Department of Pathology, *Division of Thoracic Surgery. and $Department of Radiation Oncology, Vancouver. British Columbia.
The authors thank Dr. K. G. Evans, Division of Thoracic Surgery. Vancouver General Hospital, who was the surgeon for several of these patients. and Dr. N. L. Muller, Department of Radiology. Vancouver General Hospital. for helpful comments on the manuscript.
Address for reprints: Roberta R . Miller. MD. Department of Pathology, Vancouver General Hospital. 855 West 12th Avenue, VSZ I M9, Van- couver. British Columbia, Canada.
Accepted for publication May 12, 1989.
With the advent of afterloading techniques, there has been renewed interest in intracavitary treatment in combina- tion with EBR as a means of palliation, and in conjunction with surgery for curative intent6 A pilot study has been undertaken at the Cancer Control Agency of British Co- lumbia and Vancouver General Hospital in which patients with cancer of the esophagus receive intracavitary and EBR as their primary treatment. After this combined ra- diotherapy, a select group of patients come to surgical resection with curative intent. This report describes the pathologic findings in the resection specimens from the first 2 1 patients who have been so treated.
Patients and Methods
Between March 1985 and August 1988,2 1 patients with squamous cell carcinoma or adenocarcinoma of the esophagus and gastroesophageal junction were treated with combined radiotherapy followed by resection. All patients received intracavitary radiotherapy (ICR) at a dose of 1500 cGy at 1 cm from the midline of a 10-cm linear source in 1.5 hours as described in detail by Flores et ~ 1 . ~ The patients received additional EBR using three fields to deliver between 2000 and 4000 cGy to the tumor either before or after the ICR. Thc time interval required to complete radiotherapy was 3 to 5 weeks. After com-
I833

1834 CANCER November 1 1989 Vol. 64
bined radiotherapy, all patients were evaluated clinically and radiologically and found to be resectable with curative intent. Staging laparotomy was performed approximately 6 weeks after radiotherapy was completed. Nineteen pa- tients had esophagectomy without thoracotomy using a modification of Orringer’s technique’ and two were re- sected via a discontinuous laparotomy, right t horacotom y, and left neck incisions.
The patients included 18 men and three women (age range, 33-79 years). They were divided into two groups on the basis of preoperative therapy: group 1 (N = 11) included those patients who received ICR and 4000 cGy of EBR; group 2 (N = 10) was comprised ofthose patients receiving lesser doses of EBR. There had been no pre- treatment or preoperative selection between these two groups. Rather, group 1 patients were treated later in the course of this study after standardized treatment protocols had been agreed upon. Further clinical details including follow-up information are described in detail elsewhere.*
All esophagectomy specimens were photographed, and
fixed in either formalin or Bouin’s fixative before dissec- tion. In cases in which no mass effect was found, the entire distal esophagus and esophagogastric junction were sub- mitted for full-thickness histologic examination. In cases of residual grossly identifiable tumor, at least six full- thickness sections were taken. In addition, proximal and distal resection margins, random sections of esophagus and stomach, and all resected nodal tissue were assessed histologically.
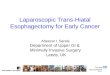
Light microscopic evaluation was performed on sec- tions stained with hematoxylin and eosin. Cell type, max- imal depth in the esophageal wall reached by viable look- ing tumor cells, predominant depth reached by tumor cells with radiation damage, and the presence and viability of lymph node metastases were all noted. Criteria for di- agnosis of radiation damage to tumor were as previously described,’.’’ including tumor giant cells with pyknotic multilobate nuclei, rare and abnormal mitotic figures, and condensation or vacuolization of the cytoplasm (Figs. 1A and 1B).
FIGS. 1A AND 1B. (A) Histologic appearance of viable looking nodal metastases from the resection specimen of patient No. 15 (H&E X25). (B) Radiated esophagus from patient No. 15 showing radiation damage of tumor cells with relative cellular enlargement, nuclear pyknosis, and multi- nucleation (H&E X25).

No. 9 ESOPHAGEAL RADIATION EFFECT - Berry et al. 1835
Depth of involvement of the esophageal wall was ex- pressed as one of four levels: level 1, not deeper than the muscularis mucosa; level 2, involving but no deeper than submucosa; level 3 , involving but no deeper than the muscularis propria; and level 4, involving periesophageal soft tissue. Thus the ratio of depth of radiation damage to depth of identifiable tumor was proportional to the local effectiveness of preoperative treatment. For example, if there was no radiation effect on tumor even at the mu- cosal level in a tumor that penetrated to the periesophageal soft tissue, then the value given would be 0/4 and the effectiveness considered poor. If radiation effect on tumor extended to the submucosa and recognizable tumor ex- tended to the periesophageal soft tissues, the value would be 2/4 and the effectiveness considered moderate. If rec- ognizable tumor involves muscularis propria but all of it shows radiation damage, the value would be 313 and the effectiveness considered good. When assessing depth of radiation effect (numerator), the level at which all tumor cells showed evidence of radiation damage was assigned. When assessing depth of recognizable tumor (denomi- nator), the level of the point of deepest invasion was as- signed.
Results
The treatment regimens and pathologic findings are summarized in Table 1.
TABLE 1. Treatment Details and Pathologic Findings
Cell Mass Effectiveness Nodal Patient Radiation tvDe effect ratio metastases
Group 1 1 ICR/4000 2 4000/ICR 3 ICR/4000 4 ICR/4000 5 ICR/4000 6 ICR/4000 7 ICR/4000 8 1CR/4000 9 4000/ICR
10 ICR/4000 11 4000/1CR
Group 2 12 ICR/2000 13 ICR/2000 14 ICR/2000 15 1CR/2500 16 ICR/3000 17 ICR/3000 18 ICR/3000 19 ICR/3000 20 ICR/3000 21 1CR/3000
sq Sq sq Ad Ad Ad Ad Ad Ad Ad Ad
sq sq sq Ad Ad Ad Ad Ad Ad Ad
Yes No No No No No No No No No No
No Yes No No No No No No No No
No No Yes No No Yes No No No Yes Yes
Yes No No Yes Yes Yes Yes Yes Yes Yes
Sq: squamous; Ad: adenocarcinoma. * No viable-looking tumor cells in esophageal wall. t No tumor cells identified in esophageal wall.
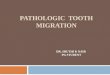
FIG. 2. Typical gross appearance of esophagectomy specimen following combined radiotherapy, showing erosion and slight mural thickening without mass effect.
There were 15 cases of adenocarcinoma and six cases of squamous cell carcinoma. In all cases, the tumor pri- marily involved distal esophagus or esophagogastric junc- tion. In no instance could extensive Barrett’s esophagus be identified, although radiation-induced mucosal erosion may have obscured focal underlying changes of this kind. In no instance did the lesion appear to be a gastric primary, secondarily involving the esophagus. No notable differ- ence in morphologic reaction to therapy was identified between the two cell types.
In only two of the 21 cases was a residual gross mass found. In the remaining specimens, the appearance was one of surface erosion or shallow ulceration with variable degrees of fibrous thickening of the esophageal wall (Fig. 2). Microscopically, the cases showed a variable degree of surface epithelial denudation and replacement with cel- lular granulation tissue.
The depth of radiation damage to tumor cells was com- parable between groups 1 and 2 (Table 2). However, only one of 1 1 patients in group 1 had involvement of peri- esophageal soft tissue as compared to eight of ten patients in group 2 (Table I), ( P 0.01, chi-square test). Similarly, although six patients in group 1 had no viable-looking residual tumor cells in the esophageal wall after treatment (Figs. 1A and 1 B), this was the case for only one patient in group 2 ( P < 0.05, Chi-square test).
Lymph node metastases were identified in 12 patients: four in group I and eight in group 2. Most of these in- volved lymph nodes were identified in the proximal per-

1836 CANCER November 1 1989 Vol. 64
TABLE 2. Penetration of Radiation E k t
Level of radiation damage
7 Patient group 0- I - 3 4 Total
I 3 4 3 0 1 o* 2 4 4 2 0 10
One patient could not be evaluated due to absence of tumor remnants in esophageal wall.
igastric serosa and showed no radiation damage. The proximal resection margin was negative for malignancy in all cases. The distal resection margin was positive for tumor cells in two cases of adenocarcinoma and negative for malignancy in all cases of squamous carcinoma.
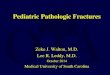
All but two cases showed moderate to marked mural fibrosis which was responsible for the grossly noted mural thickening. There was no instance of perforation. Variable degrees of mucosal atypia in areas adjacent to surface ero- sion was present in most cases. This atypia was charac- terized by architectural disorder, nuclear enlargement and hyperchromasia, and cellular enlargement. These changes were believed to be radiation induced particularly when involving mucosa of different type from the existing rna- lignancy, although this could not be proven (Fig. 3).
Discussion
Carcinoma of the esophagus in western countries carries a poor prognosis, the great majority of patients having high stage disease at presentation.' Survival figures vary among series according to patient selection and treatment protocols, but the overall 5-year survival of patients with this disease is said to be approximately 5%." Therefore, the primary aim of therapy to date has been good pallia- tion with as little morbidity as possible. The most common modalities used to achieve palliation have been surgery and EBR. Surgical bypass in general affords excellent pal- liation but carries the unavoidable morbidity and mor- tality of a major surgical p roced~re .~ External-beam ra- diation is less morbid than surgery, but the palliation it provides is less reliable and less durable.'' Effective che- motherapy regimens are being but are exper- imental so far.
The technique of combined ICR and EBR offers several potential advantages over the other approaches. The major contraindication to combined treatment is an airway- esophageal tumor fistula,6 so fewer patients are excluded compared to surgical or radical radiation therapy. Whereas fistula formation has been described as a complication of ICR,I4.l5 we have not encountered serious morbidity or mortality as the result of this procedure6. Since there is minimal penetration of radiation from the intracavitary source beyond the esophageal wall, the therapeutic ratio
is higher. Good palliation with restoration of swallowing is rapidly achieved with this technique.' Although dura- bility of local control is not ideal, it is better than that achieved with EBR only. Thirty percent to 40% of patients develop local recurrence requiring further treatment.6.'4%15
Pathologic analysis of esophagectomy specimens after EBR for squamous cell carcinoma have been reported. Akakura el u I . ~ noted the gross appearance of such cases to usually consist of a small reepithelialized ulcer with mural fibrosis. Microscopically, approximately 65% of their cases showed definite cytologic radiation effect, as defined by mitotic incompetence, nuclear pyknosis, cy- toplasmic vacuolization and/or tumor cell disappearance. Hambraeus et ul." expanded these analyses, and found that evaluation of cytologic features, mitotic activity, depth and pattern of invasion following EBR is helpful
FIG. 3 . Radiation induced atypia in gastric mucosa of patient No. 14, whose esophageal tumor was a squamous carcinoma (H&E X25).

No. 9 ESOPHAGEAL RADIATION EFFECT - Berry el al. 1837
in predicting prognosis. Hishikawa et al.” compared au- topsy findings in 16 patients treated with ICR and EBR with autopsy findings in 19 patients given EBR only, and reported tumor sterilization at the primary site in 56% of patients in the former group but only 5% in the latter. To our knowledge, there have been no detailed pathologic reviews of esophagectomy specimens after combined ICR and EBR.
The rationale for combining ICR with EBR is straight- forward. Intracavitary radiotherapy is intended to provide high doses to the luminal aspects of the tumor, which may be more hypoxic and hence relatively radioresistent. However, the effective dose from the ICR is limited to the most central 5 to 10 mm of the tumor.6 External- beam radiotherapy is intended to treat the tumor in the deep esophageal wall and periesophageal soft tissues. For this reason, our method of pathologic analysis emphasized depth of tumor cell damage as a function of total depth of recognizable tumor (viable or nonviable) in the esoph- ageal wall. Penetration of radiation effect relative to mural tumor depth is expressed as a ratio which is roughly pro- portional to poorly, moderately and very effective cate- gories. A high ratio reflects viable tumor remaining only in the deeper layers, if at all, whereas viable tumor re- maining at or near the mucosa is expressed as a low ratio and is considered poor penetration. Overall, in this series, seven of 2 1 cases showed poor radiation penetration (levels 0 or 1). The other 14 cases showed radiation effect at least to the level of the submucosa. Tumor sterilization was achieved in seven of these 14, and six of these seven had received 4000 cGy of EBR.
In all but two cases no gross mass effect was found, although the gross appearance did not correlate well with histologic level of tumor. Nevertheless, the absence of an intraluminal mass correlates well with the clinical obser- vation of rapid restoration of swallowing after ICR. The histologic finding of moderate to very effective local con- trol in 14 of 21 cases correlates with the clinical obser- vation of excellent palliation in 60% to 70% of patients treated with combined radiotherapy only. Although the degree of effectiveness of intraluminal tumor control was similar regardless of EBR dose, our results support the hypothesis that higher EBR doses provide better control of tumor in the deeper layers of the esophageal wall, and higher rates of local tumor sterilization.
Lymph node metastases were found in 12 of 2 I patients in our series, in contrast to 80% as reported in autopsy cases after combination therapy.” However, these two populations are not entirely comparable. All of our pa- tients were Stage l, ll, or 111, whereas 50% of the patients
in the series of Hishikawa et aLL7 were Stage 111 or IV, and higher stage involvement is known to be associated with a higher rate of nodal involvement. In addition, since extrathoracic esophagectomy, as performed in 19 of our patients, does not allow for mediastinal node assessment, nodal metastases may have been underdiagnosed in our series.
REFERENCES
1. MacFarlane SD, Hill LD, Jolly PC. Kozarek RA, Anderson RP. Improved results of surgical treatment for esophageal and gastroesoph- ageal junction carcinomas after preoperative combined chemotherapy and radiation. J Thoruc Cardiovusc Surg 19 88: 95:4 15-422.
2. Karlin DA, Fisher RS, Krevsky B. Prolonged survival and effective palliation in patients with squamous cell carcinoma of the esophagus following endoscopic laser therapy. Cancer 1987; 59: 1969- 1972.
3. Wong J. Esophageal resection for cancer: The rationale of current practice. Am J Surg 1987; 153: 18-24.
4. ORourke IC, Tiver K, Bull C, Gebski V, Langlands AO. Swallowing performance after radiation therapy for carcinoma of the esophagus. Cancer 1988; 61:2022-2026.
5. George F W 111. Radiation management in esophageal cancer. A m
6. FIores AD, Stoller JL, Nelems B, Hay J, Jackson SM. Combined primary treatment of cancer of the esophagus and cardia by intracavitary and external irradiation. In: Sirwert JR, Hoischco AH, eds. Diseases of Esophagus. New York: Springer-Verlag, 1987; 741-749.
7. Orringer MB. Technical aids in performing transhiatal esophagec- tomy without thoracotomy. Ann Thoruc Surg 1984: 38: 128-132.
8. Luoma A, Nelems B, Miller RR. Flores AD, Evans KG, Hay J . Surgical implications of combined intracavitary and external beam ra- diotherapy for carcinoma of the lower esophagus and cardia. Chest (sub- mitted).
9. Akakura I, Nakamura Y, Kakegawa T, Nakayama R, Watanabe H, Yamashita H. Surgery ofcarcinoma ofthe esophagus with preoperative radiation. Chest 1970; 57:47-57.
10. Fajardo L. Morphologic changes in irradiated tumors. In: Fajardo L, ed. Pathology of Radiation Injury. New York Masson, 1982; 244- 251.
1 1. Hancock SL, Glatstein E. Radiation therapy of esophageal cancer. Semin Oncol 1984; 11:144-158.
12. Coia LR, Paul AR, Engstrom PF. Combined radiation and che- motherapy as primary management of adenocarcinoma of the esophagus and gastroesophageal junction. Cancer 1988; 6 1:643-649.
13. Hilgenberg AD, Carey RW, Wilkins EW Jr, Choi NC, Mathisen DJ. Grillo HC. Preoperative chemotherapy, surgical resection, and se- lective postoperative therapy for squamous cell carcinoma of the esoph- agus. Ann Thorac Sztrg 1988; 45:357-363.
14. Hishikawa Y, Kamikonya N, Tanaka S, Miura T. Radiotherapy of esophageal carcinoma: Role of high-dose-rate intracavitary irradiation. Radiother Oncol 1987; 9: 13-20,
15. Hyden EC, Langholz B. Tilden T et ul. External beam and intra- luminal radiotherapy in the treatment of carcinoma of the esophagus. J Thoruc Cardiovusc Surg 1988; 96:237-241.
16. Hambraeus GM. Mercke CE, Willen R ef (I/. Prognostic factors influencing survival in combined radiotherapy and surgery of squamous cell carcinoma of the esophagus with special reference to a histopathologic grading system. Cancer 1988; 62:895-904.
17. Hishikawa Y, Taniguchi M, Kamikonya N, Tanaka S, Miura T. External beam radiotherapy alone or combined with high-dose-rate in- tracavitary irradiation in the treatment of cancer of the esophagus: Au- topsy findings in 35 cases. Radiother Oncol 1988; 11:223-227.
J SZrrg 1980; 139:795-804.