-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
1/24
R B C
MORPHOLOGYAug. 2011
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
2/24
0 Anemia- defined as a reduction in the total quantityof red
cells or hemoglobin (Hb) in the circulation.
0 RBC provide a mode of transport of Hb to deliveroxygen to the
tissues and carbon dioxide from the
tissues.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
3/24
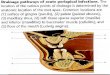
ERYTHROCYTE MATURATION
1. Proerythroblast (14-19 m): Nucleus is large with
fine chromatin and nucleoli; cytoplasm is scant and
basophilic.
2. Basophilic erythroblast (12-17 m): Slightly smaller
nucleus with slight chromatin condensation; increasedcytoplasm
and intensely blue (RNA abundance); no
granules and no nucleoli present.
3. Polychromatophilic erythroblast (12-15 m):
Moderately condensed chromatin; lighter, grayish
cytoplasm. The color of the cytoplasm is due to coloring
by both acidic and basic components of the stain.Basophilia is
from staining of ribosomes and acidophilia
from hemoglobin. The nucleus is condensed and
intensely basophilic with coarse heterochromatin granules
giving a characteristic checkerboard appearance.
4. Orthochromatophilic erythroblast (8-12 m): Dark,
opaque nucleus; gray-red cytoplasm (trace blue). The
nucleus has become pyknotic and there is abundant
acidophilic hemoglobin.
5. Reticulocyte (7-10 m)Nucleus has been extruded;
cytoplasm is reddish-pale blue. RNA is still present.
6. Erythrocyte (7-8 m): No nucleus; orange-red
cytoplasm; RNA is lost
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
4/24
0 RBC morphology- determined through peripheral blood smear ( in
the thinpart, atfeathery edge )
0 Why at the feathery edge of the smear?1. Distribution- cells
not in this edge are stacked (patong-patong)2. Cell contents
(nucleus, cytoplasm) are clearly seen3. passage of light through
thin partmorphology can be determined4. WBC are numerous at the
THICK part because they are bigger .
Indications for requesting for RBC morphology:1. For diagnosis
of malaria hospitals have specific tests for malaria but still
use
the smear to confirm
2. To detect anemia- any defect in RBC will produce anemia3. To
confirm sickle cell anemia; to concretize the diagnosis of the type
of anemia
Other specimens tested for RBC/for diagnosis of anemia:1. Bone
marrow aspirate2. Urine- identification ofhematuria in patients w/
renal problems, doc looks for
dysmorphic RBCs
Anemia-Pallor: pale conjunctiva, decreased capillary refill (at
nail beds), pale skin (ifperson is dark-skin, check the mucosa)
0*CBC only used for RBC count(amount/quantity), not the form of
RBCs
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
5/24
DEFINITION OF TERMS
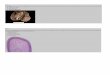
0 CRENATION- the RBC are with shrunken or irregularborders,tiny
smooth projection(ruffles) in their membrane.
This results from loss of intracorpuscular water through
osmosis and not a significant diagnostic indicator of any
disease state can be drugs, dehydration, etc.
0 ACANTHOCYTES-similar to crenated RBC; however the
projections are irregularly spaced and at the apex of
theprojections are sharp points. Seen in px with metabolic
dysfunction (dec. lipoprotein absorption in GIT )
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
6/24
0BURR CELLS similar to elongated crenated rbc and
often assume irregular shapes such as that of
quarter moon. Seen in px with bleeding gastric
ulcers and renal insufficiency.
0TARGET CELLS dark-staining periphery and
darker central area with a lighting between the 2
dark areas.Seen in px with hemoglobinopathies such
as thalassemia and liver disease.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
7/24
0PYKNOCYTES observed during the 1sttrimester of life
in the newborns.Have similar appearance tospherocytes with small
spinal projections.Seen in px
with G-6-PD dificiency.
0 SICKLE CELL mature RBCs that have become
crescent-shaped.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
8/24
0ELLIPTOCYTES are mature RBCs that assume an
elliptical or oval shape. Seen in px with
hereditaryelliptocytosis, some forms of anemia. Believed to be
a defect in the integrity of corpuscular membrane.
0 SCHISTOCYTES fragments of RBC still in the
peripheral circulation. Formed in the spleen and
intravascular fibrin clot. Indication ofhemolysis.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
9/24
0 SPHEROCYTES smaller than normocytes and
contains abnormally large amount of Hb. Seen in
px with hereditary spherocytosis.
0MICROCYTES smaller RBC in diameter.0 ( 6.0 um or less)
0MACROCYTES ave. diameter of9.0 um in
diameter or greater.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
10/24
0 The red blood cells here are normal, happy RBC's. Theyhave a
zone ofcentral pallor about 1/3 the size of the
RBC. The RBC's demonstrate minimal variation in
size(anisocytosis) and shape (poikilocytosis). A few smallfuzzy
blue platelets are seen. In the center of the field are aband
neutrophil on the left and a segmented neutrophil onthe right.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
11/24
0 The RBC's here are smaller than normal and have anincreased
zone of central pallor. This is indicative of a
hypochromic (less hemoglobin in each RBC) microcytic(smaller
size of each RBC) anemia. There is also increasedanisocytosis
(variation in size) and poikilocytosis(variation in shape).
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
12/24
0 The RBC's here have stacked together in long chains. This
isknown as "rouleaux formation" and it happens with
increased serum proteins, particularly fibrinogen andglobulins.
Such long chains of RBC's sediment more readily.This is the
mechanism for the sedimentation rate, whichincreases
non-specifically with inflammation andincreased "acute phase" serum
proteins.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
13/24
0 The most common cause for a hypochromic microcyticanemia is
iron deficiency. The most common nutritional
deficiency is lack of dietary iron. Thus, iron deficiencyanemia
is common. Persons most at risk are children andwomen in
reproductive years (from menstrual blood lossand from
pregnancy).
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
14/24
0 Here is a hypersegmented neutrophil that is present
withmegaloblastic anemias. There are 8 lobes instead of the
usual 3 or 4. Such anemias can be due to folate or to
B12deficiency. The size of the RBC's is also
increased(macrocytosis, which is hard to appreciate in a
bloodsmear).
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
15/24
0 There are numerous fragmented RBC'sseen here. Some ofthe
irregular shapes appear as "helmet" cells. Such
fragmented RBC's are known as "schistocytes" and they
areindicative of a microangiopathic hemolytic anemia(MAHA) or other
cause for intravascular hemolysis. Thisfinding is typical for
disseminated intravascularcoagulopathy (DIC)
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
16/24
Spherocytes
0 This peripheral blood smear demonstrates many larger
bluish
reticulocytes as well as smaller RBC's lacking central
pallor--spherocytes. This patient had an autoimmune hemolytic
anemia.Antibody coated the RBC's, and portions of the RBC's were
removed,decreasing cell size. Many RBC's were removed entirely,
resulting inanemia and a bone marrow response with increased
erythropoiesis andelevated reticulocyte count (20%). The patient
developed an indirecthyperbilirubinemia as well.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
17/24
Tear drop cells
0 This peripheral blood smear demonstrates tear drop cells.These
characteristically shaped RBC's can be seen inpatients with
myelofibrosis and those who underwentradiation
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
18/24
0 The RBC in the center of the field contains several
Howell-
Jolly bodies, or inclusions of nuclear chromatin remnants.There
is also a nucleated RBC just beneath this RBC.Abnormal and aged
RBC's are typically removed by thespleen. The appearance of
increased poikilocytosis,anisocytosis, and RBC inclusions suggests
that a spleen isnot present.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
19/24
Spherocytes
0 The size of many of these RBC's is quite small, with lack
of
the central zone of pallor. These RBC's are spherocytes.
Inhereditary spherocytosis, there is a lack of spectrin, a keyRBC
cytoskeletal membrane protein. This producesmembrane instability
that forces the cell to the smallestvolume--a sphere. In the
laboratory, this is shown byincreased osmotic fragility. The
spherocytes do not
survive as long as normal RBC's.
No central pallor
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
20/24
0The nucleated RBC in the center containsbasophilic stippling of
the cytoplasm. This
suggests a toxic injury to the bone marrow, suchas with lead
poisoning. Such stippling may alsoappear with severe anemia, such
as a megaloblasticanemia.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
21/24
0 This peripheral blood smear demonstrates markedpoikilocytosis
(abnormally shaped RBC's) as well as some
anisocytosis (variation in RBC size), though many are
small(microcytes). This patient had beta-thalassemia, ahereditary
disorder of beta globin chain synthesis that leadsto ineffective
erythropoiesis and a microcytic anemia. Someof the RBC's resemble
jigsaw puzzle pieces.
Poikilocytosis
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
22/24
0 This is sickle cell anemia in sickle cell crisis. The
abnormalhemoglobin SS is prone to crystallization when oxygen
tension is low, and the RBC's change shape to long, thinsickle
forms that sludge in capillaries, further decreasingblood flow and
oxygen tension. Persons with sickle cell trait(Hemoglobin AS) are
much less likely to have this happen.
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
23/24
0 In the center of the field is a rectangular RBC that
isindicative ofHemoglobin SCdisease. Both hemoglobin S
and hemoglobin C are present. The RBC's may sickle, butnot as
commonly as with Hemoglobin SS disease. Thehemoglobin C leads to
the formation of "target" cells--RBC's that have a central reddish
dot.
HbSC
HbC
-
8/4/2019 Patho[Lab Ppt Trans]_2-2_RBC Morphology (1)
24/24
0
Malaria is a parasitic disease caused by the genusPlasmodium, of
which there are four species that affectman. Shown here are "ring
forms" of Plasmodiumvivax in red blood cells. This disorder can
producehemolysis and anemia.