Embed Size (px)
Citation preview

9 JClin Pathol 1997;50:294-298
Intra-abdominal sepsis: an immunocytochemicalstudy of the small intestine mucosa
H B Coutinho, T I Robalinho, V B Coutinho, A M S Amorim, A F Furtado, A Ferraz,E Ferraz, F Walker, G King, H F Sewell, D Wakelin
Centro de PesquisasAggeuMagalhaes/FIOCRUZ,Recife, BrazilH B CoutinhoT I RobalinhoV B CoutinhoA M S AmorimA F Furtado
Departamento deCirurgia, UniversidadeFederal dePernambuco, Recife,BrazilA FerrazE Ferraz
Department ofPathology, UniversityofAberdeen,Aberdeen, UnitedKingdomF WalkerG King
University ofNottingham,Nottingham, UnitedKingdom: DepartmentofImmunologyH F Sewell
Department of LifeScienceD Wakelin
Correspondence to:Professor D WakelinDepartment of Life Science,University of Nottingham,University Park, NottinghamNG7 2RD, United Kingdom.
Accepted for publication3 February 1997
AbstractAim-To investigate immunocytochemi-cal changes in intestinal tissues frompatients with intra-abdominal sepsis, andto relate the changes to the possibility ofenhanced bacterial adhesion and translo-cation.Methods-Tissues from 17 patients suffer-ing from intra-abdominal sepsis and fromcontrols were sectioned and stained im-munocytochemically for IgA, IgM, secre-
tory component, J chain, and HLA-DR.Differences in the distribution and char-acteristics of positively staining cells be-tween the patient groups were assessed.Results-Patients with intra-abdominalsepsis had noticeable reductions in num-bers of IgA and IgM plasma cells, reducedJ chain staining, and had little immuno-globulin on the surfaces of enterocytes. Incontrast, HLA-DR positive cells were
increased in the sepsis compared with thecontrol group. The plasma cells presentshowed cytological changes suggestive ofapoptosis.Conclusions-Stress associated with sep-
sis and its immediate causes might resultin increased plasma glucocorticoid levelsthat bring about apoptosis of mucosalplasma cells (or their precursors). Theconsequent reduction in expression ofIgAand IgM may favour bacterial adhesion tothe enterocytes and facilitate bacterialtranslocation into the tissues.(7 Clin Pathol 1997;50:294-298)
Keywords: intra-abdominal sepsis; bacterial adhesion;bacterial translocation; apoptosis
The concept that organisms from the gastroin-testinal tract play a major role in the genesisand perpetuation of sepsis in critically illpatients'-3 is supported by the correlationbetween the microbial species colonising theproximal intestine and the organisms causingendogenous infection in intensive care units.2This phenomenon reflects bacterial transloca-tion across the mucosa, which can be attributedto alterations in the barrier function of thesmall intestine.The immunological defences of the small
intestine include substantial numbers oflamina propria plasma cells, the majority ofwhich produce IgA. In its dimeric form, linkedby J chain, this immunoglobulin passes throughthe overlying epithelium where secretory com-ponent is added, and reaches the lumenal sur-
face to be trapped in the mucous layer. Smaller
amounts of IgM reach the lumen in a similarmanner.
Studies on this immunological component incritically ill patients are limited by ethical andtherapeutic constraints; however, suitable tis-sues may be obtained from patients whosecondition necessitates surgical removal of partof the small bowel. A series of such specimenswas retrieved for the present study. Tissuesfrom near the excision margins consideredviable by the surgeons and judged to berelatively remote from the primary intra-abdominal damage by the pathologists-wereselected for immunohistochemical studies.
MethodsPATIENTS AND TISSUESBlocks from the small intestines of 17 patientswere taken from the files of the Department ofPathology, Aberdeen Royal Infirmary, Scot-land (12 patients: six males, aged 54-78; sixfemales, aged 34-79), and the Department ofSurgery, Universidade Federal de Pernam-buco, Recife, Brazil (five patients: one male,aged 39; four females, aged 57-79). All of theAberdeen cases had presented with an acuteabdomen; 11 had infarction of the small bowelattributed to a variety of thrombotic ormechanical causes. The Recife cases met thesame criteria for selection. One Aberdeen casehad a perforated ulcer. Controls were normalsmall intestine from two transplant donors.Tissues had been fixed in 10% neutral bufferedformalin and processed to paraffin wax.Sections of 4 ztm were cut onto 3-amino-propyltriethoxysilane-subbed slides and driedat 60°C for 30 minutes.
IMMUNOHISTOLOGYSections were first dewaxed in xylene andendogenous peroxidase blocked using 1.5%hydrogen peroxide in methanol. Optimal un-masking of antigens other than IgM wasobtained by placing sections in 10 mM citratebuffer, pH 6.0, in an 800 W microwave ovenoperated on full power for 20 minutes,maintaining the level of buffer at 600 ml. Sec-tions were left in hot buffer on the bench for afurther 20 minutes prior to transferring to Trisbuffered saline (TBS). IgM was exposed bydigestion in 0.1% trypsin in 0.1% calciumchloride at 37°C, pH 7.8, for 30 minutes,followed by five-minute washes in runningwater (once) and TBS (twice).Murine monoclonal antibodies against IgM
(Oxoid, Basingstoke, UK, MF02) andHLA-DR (Dako, High Wycombe, UK,M0646) were used at dilutions of 1:160 and
294
on March 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.4.294 on 1 April 1997. D
ownloaded from

Intra-abdominal sepsis: an immunocytochemical study of the small intestine mucosa
1:40, respectively, and incubated for 60 min-utes. Rabbit polyclonal antibodies against IgA(Behring, Lewes, UK, ORCI 03/05), J chain(Nordic, Maidenhead, UK, 9-480), and secre-tory component (Dako A0187) were used atdilutions of 1:2000, 1:600, and 1:1000, respec-tively, and incubated for 30 minutes. FollowingTBS washes, biotin labelled species specificsecondary antibodies were applied for 30 min-utes. For mouse primary antibodies the sec-ondary antibody was rabbit antimouse/biotin(Dako E0343) at a dilution of 1:150 in TBScontaining 4% heat inactivated normal humanAB serum, and for rabbit primary antibodies,swine antirabbit/biotin (Dako E0345) at adilution of 1:200 containing 4% heat inacti-vated normal human AB serum. Slides werethen washed in TBS after which sABC (DakoK0377), diluted as per kit instructions, wasapplied for 90 minutes (for polyclonal primaryantibodies), or 30 minutes (for monoclonalprimary antibodies), followed by TBS washes.Demonstration of HRP was with the substrate3'3-diaminobenzidine tetrahydrochloride, im-mediately following which the sections wereplaced into 0.5% cupric sulphate in saline todarken the DAB reaction product to brown/black. Sections were then counterstained inHarris haematoxylin, dehydrated, cleared, andmounted in DPX.Known positive control sections were in-
cluded in each batch of immunostained speci-mens. Negative controls were provided byincubating sections from the same block withTBS in place of mouse monoclonal primaryantibody, or normal rabbit immunoglobulinfraction (Dako X0903) at a dilution of 1:1000in place of rabbit polyclonal primary antibody.
ResultsIgAControls IgA was present in the cytoplasm ofcytologically well preserved plasma cells lo-cated in the lamina propria of the villi or in theloose connective tissue around the intestinalcrypts. Small granules of IgA positivity wereobserved throughout the cytoplasm of thecrypt cells and concentrated at the apical poles.The apical surface of the enterocytes lining thevilli was also IgA positive (fig 1A).Intra-abdominal sepsis There was a strikingabsence of morphologically normal IgA posi-tive plasma cells. However, rare small cellscould be detected immunocytochemically, theIgA within these cells being detected in theform of coarse cytoplasmic granules. Thesecells lacked the classical chromatin pattern andconspicuous nucleoli associated with plasmacells, showing instead a dense chromatinnucleus. No IgA was present in the cytoplasmof the crypt cells or lining the enterocytesurfaces (fig IB).
IgMControls The apparent number of IgM positiveplasma cells was fewer than those which wereIgA positive. They were located in the laminapropria of the villi adjacent to intestinal crypts.The apical poles of the crypt cells were rich indeeply stained IgM granules. In contrast to
IgA, enterocytes presenting a superficial liningofsIgM were observed only in the basal third ofthe villi (fig 1 C).Intra-abdominal sepsis IgM positive cells withnormal plasma cell morphology were notdetectable. However, as with IgA, immunocy-tochemistry revealed rare IgM positivity in cellswith dense chromatin nuclei that were devoidof nucleoli. No IgM positivity was noted in thecrypt cells or on the enterocytes (fig 1D).
J CHAINControls The lamina propria of the villi and theloose connective tissue around the intestinalcrypts contained numerous J chain positiveplasma cells (fig 2A).Intra-abdominal sepsis As with IgA and IgM,morphologically normal plasma cells with Jchain positivity were not detectable. The slightJ chain positive staining of the apical pole of thecrypt cells in normal individuals was absent inseptic patients (fig 2B).
SECRETORY COMPONENTControls Secretory component was noted in thecrypt cells of normal human jejunum, concen-trated in the Golgi area. Small secretorycomponent positive granules were observed onthe surface of the enterocytes located at thebasal third of the villi (fig 2C).Intra-abdominal sepsis Cytoplasmic secretorycomponent was noted in the whole crypt area.Beside the conspicuous staining of the Golgiarea, cytoplasmic secretory component positivegranules were noted in the epithelium of theentire villus (fig 2D).
HLA-DR
In both controls and sepsis cases the apicalpoles of the enterocytes showed linearHLA-DR positive small granules. In septicpatients HLA-DR positive cells were strikinglymore numerous in the intestinal lamina propria(figs 2E and 2F). These cells presumablyincluded antigen presenting cells and manyhad the morphology of macrophages.
DiscussionThese results indicate a drastic reduction ofsIgA and sIgM on the apical surfaces of jejunalenterocytes during intra-abdominal sepsis.There were also morphological indications thatthis lack of lumenal sIg may have resulted fromthe death of plasma cells located in the neigh-bourhood of the intestinal crypts, the cells ofwhich are known to be responsible forsecretory component mediated transfer ofthese immunoglobulins from the lamina pro-pria to the crypt lumen. Tissues from sepsispatients showed fewer IgA positive, IgMpositive, and J chain positive plasma cells thanthose from the normal controls.
In normal specimens, IgA and IgM plasmacells had cytoplasm filled with small granules ofpositively staining IgA and IgM, and nucleiwith well defined chromatin granules and con-spicuous nucleoli. Conversely, in tissues frompatients with intra-abdominal sepsis, morpho-
295
on March 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.4.294 on 1 April 1997. D
ownloaded from

Coutinho, Robalinho, Coutinho, Amorim, Furtado, Ferraz, et al
_,. W. s .r~~~~~~~~~otiW*.!*I,+f E.X ~ ~ ~ ~ AW
.<<u_ .k,#:., .........j~pn
N~~~~~~~A:#eXa'4M-,&>5GR~~~~~~~~~~~~~..... .L
w i. iE's 0 ;-0is'r
I
t.."* 4 '. 91 ..,-1461,
11 'i.,'X
I
..:....
--\11|t se:
% ,>:-.W. :' .'is.4 ,. :@
.t f t g /_
P)s>. ts* i F: :Xe -S.
;BU ;_
.r ' '*if * ^ bi 1!1'IL
_o
P:. siEl,;, t .s
ts <v O' tr
.: _ .iEe :. . \. _7ii | 1) tgtl
w /.. e . 4#_ 4:
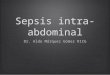
.:<; " fS'.&- ai-. *: : .v."< .. '.E'Figure 1 Immunocytochemistry ofsmall intestinal tissues stainedfor IgA and IgM. (A, C) Normal tissues. (B, D) Tissues from patients withintra-abdominal sepsis. (A) IgA positive plasma cells are present in the lamina propria and IgA positive granules are concentrated in the apical poles ofcrypt cells; (B) only apoptotic plasma cells are present, IgA positive granules are absentfrom crypt cells; (C) IgM positive plasma cells are located nearintestinal crypts and IgM positive granules are accumulated in the apical poles of crypt cells; (D) one apoptotic plasma cell is shown, crypt cells are IgMnegative.
logically normal plasma cells were notdetected. However, the rare cells detected withimmunocytochemical positivity for IgA andIgM were reduced in size, their immunoglobu-lins were in the form of compact, coarse gran-ules, the nuclei were devoid of nucleoli andwithout apparent chromatin granules. Thesechanges are equivalent to some of the featuresassociated with cellular apoptosis. Presumablythese were degenerating cells which had not yetbeen phagocytosed. Whereas in degenerationby necrosis cells become vacuolated, in apop-totic cells DNA cleavage leads to a reduced cellvolume and chromatin compaction, oftenfollowed by nuclear fragmentation and phago-cytosis. Apoptotic cells are commonly recog-nised and removed by macrophages.45
Apoptosis in B lymphocytes is thought toresult from programmed cell death or to beinduced by an increase in plasma glucocorti-coid levels. The decrease in the number andpercentage of blood lymphocytes and eosi-nophils seen during stress may be the result ofapoptosis.5
Bacterial translocation, the passage of viablebacteria through the epithelial intestinal barrierinto the lamina propria' is a significant factor inthe aetiology of sepsis. It requires initial attach-ment of bacteria to intestinal enterocytes, thecell membranes of which are then ruptured,allowing the bacteria to penetrate and reach the
basal membrane.3 Once this is achieved, intes-tinal lymphatic drainage carries bacteria to themesenteric lymph nodes for dissemination toother organs and tissues. This disseminationmay lead to sepsis syndrome, multiple organfailure, and death of the patient.8 Bacterialtranslocation has been reported in a variety ofpathological conditions including intestinalobstruction,9 surgical trauma,lo drugcytotoxicity," thermal injury,'2 13 intravenousfeeding,'4 haemorrhagic shock,'5 parenterallyadministered endotoxin,'6 and hyperpyrexia.7These have in common an association withtrauma that induces severe patient stress.
Following trauma, both humoral and cellmediated immunity are affected adversely.'8Stress triggers the hypothalamic-pituitary-adrenal axis with a subsequent rise in serum
levels of many hormones including somatosta-tin, corticotrophin, angiotensin, insulin, sub-stance P, adrenaline, glucagon, and glucocorti-coids. Stress and sepsis have a strong impact onthe blood levels of lymphocytes,4'5 8 effectsrelated to the release of glucocorticoids.18 Glu-cocortoids have a variety of immunosuppres-sive effects, including downregulation of mac-rophage function, prevention of monocytedifferentiation, inhibition of synthesis ofinterferon-,y, interleukin (IL)-1, IL-6, andtumour necrosis factor,'9 20 and suppression ofB cell maturation.'8 21 In rats, the number and
ii '..
296
.. 4AW,..ddlk I .:.?.
I-.Na- .il.i,Ipr-"I' 'NO,
ik
on March 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.4.294 on 1 April 1997. D
ownloaded from

Intra-abdominal sepsis: an immunocytochemical study of the small intestine mucosa
~~~~~~~~~~- , u:>-yE:tVEE ::n@II
Figure 2 Immunocytochemistry of smaUl intestinal tissues stainedforJ chain, secretory component, and HLA-DR. (A, C, E) Normal tissues. (B, D, F)Tissues from patients with intra-abdominal sepsis. (A) Numerous J chain positive plasma ceUls are present in the lamina propria; (B) J chain positiveplasma cells are greatly reduced; (C) secretory component is expressed in the Golgi of crypt cells; (D) secretory component positive granules are noted incrypt cells and enterocytes; (E) HLA-DR granules are present in the apical poles of enterocytes and in macrophages; (F) the macrophage population isincreased in the lamina propria.
percentage of lymphocytes decreases when theanimals experience a mild acute stress.6 Lym-phopenia and increase of plasmatic glucocorti-coid level have also been noted during humansepsis.
NWe surmise that the stress related increasesin glucocorticoid levels resulting from theaforementioned pathologies may promote apop-
tosis of the mucosal plasma cells (or their B celllineage progenitors) responsible for secretionof IgA and IgM." Such a reduction of secretedimmunoglobulins would interfere with thenormal barrier mechanism and facilitate adhe-sion of intestinal bacteria to the surface of the
enterocytes-the initial step in the chain ofevents that may evolve to sepsis and multipleorgan failure. It is well established that sIgApresent in mucus located on the enterocyteglycocalyx prevents bacterial adhesion.23 24 Al-banese et al," using the Ussing model, haveshown that Escherichia coli bound to sIgA couldnot cross a morphologically intact segment ofviable intestinal tissue.
Cytoplasmic secretory component was in-creased in the crypt cells and the enterocytes ofseptic patients compared with normal indi-viduals (figs 2C and 2D). This may indicatethat increased glucocorticoid levels had not
297
on March 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.4.294 on 1 April 1997. D
ownloaded from

Coutinho, Robalinho, Coutinho, Amorim, Furtado, Ferraz, et al
interfered with secretory component synthesis,and may indeed have led to an increase insecretory component. Although secretory com-ponent molecules normally leave the crypt cellsattached to dimeric IgA or pentameric IgM toform the respective sIgs, the absence ofIgA andIgM may result in the cytoplasmic accumula-tion of secretory component in crypt cells andcrypt derived enterocytes by a positive feed-back process.
Ayala et a'26 reported a decrease in antigenpresenting cells associated with the loss ofmajor histocompatibility class II followinghaemorrhage. In contrast, we noted an increasein the number ofHIA-DR positive cells, prob-ably macrophages (figs 2E and 2F). There wasalso an apparent increase of the cytoplasmiccontent of HIA-DR in lamina propria macro-phages and dendritic cells. These findingsappear consistent with well documented re-ports that macrophages participate in remov-ing cellular debris resulting from cellular apop-tosis.
This work was supported by The British Council/FACEPE,European Union Contract TS3-CT93.0227, Bank of BrazilFoundation, and Conselho Nacional de Pesquisas.
1 Berg RD, Carlington AW. Translocation of certain indig-enous bacteria from the gastrointestinal tract to themesenteric lymph nodes and other organs in a gnotobioticmouse model. Infect Immun 1979;23:403-1 1.
2 Marshall JC, Christou NV, HorJn R, Meakins JL. Themicrobiology of multiple organ failure. Arch Surg 1988;123:309.
3 Alexander JW, Boyce ST, Babcock GF, Gianotti L, PeckMD, Dunn DL, et al. The process of microbial transloca-tion. Ann Surg 1990;212:496-512.
4 Arends MJ, Wyllie AH. Apoptosis: mechanism and role inpathology. Int Rev Exp Pathol 1991;32:223-54.
5 Cox G. Glucocorticoid treatment inhibits apoptosis inhuman neutrophils-separation of survival and activationoutcomes. J Immunol 1995;154:4720-5.
6 Dhabhar FS, Miller AH, McEwen BS, Spencer RL. Effectsof stress on immune cell distribution-dynamics andhormonal mechanisms. J Immunol 1995;154:5511-27.
7 Norwell A, Mandick L, Monroe G. Engagement of theantigen-receptor on immature murine B lymphocytesresults in death by apoptosis. J Immunol 1995;154:4404-13.
8 Baue AE. The Horror Autotoxicus and multiple-organ fail-ure. Arch Surg 1992;127:1451-62.
9 Deitch E. Simple intestinal obstruction causes bacterialtranslocation in man. Surgery 1989;124:699-701.
10 Rhodes RS, Karnowsky MJ. Loss of macromolecular barrierfunction associated with surgical trauma to the intestine.Lab Invest 1971;25:220-9.
11 Fox AD, Kripke SA. de-Paula J, Berman JM, Settle RG,Rombeau JL. Effect of a glutamine-supplemented enteraldiet on methotrexate-induced enterocolitis. J Parent EntNutr 1988;12:325-31.
12 Maejima K, Deitch EA, Berg RD. Bacterial translocationfrom the gastrointestinal tracts of rats receiving thermalinjury. Infect Immun 1994;43:6-10.
13 Jones WG, Minei JP, Barber AE, Raeburn JL, Faher TJ,Shires GT. Bacterial translocation and intestinal atrophyafter thermal injury and burn wound sepsis. Ann Surg1990;211:399-406.
14 Alvery JC, Aoys E, Moss GS. Total parenteral nutrition pro-motes bacterial translocation from the gut. Surgery1988;104: 185-90.
15 Rush BF, Sori AJ, Murphy TF, Smith S, Flanagan JJ,Machido GW. Endotoxemia and bacteremia during hemor-rhagic shock. The link between trauma and sepsis? AnnSurg 1988;207:549-54.
16 Deitch EA, Berg RG. Endotoxin promotes the translocationof bacteria from the gut.Arch Surg 1987;122:185-92.
17 Gathiram P, Gaffin SL, Brock-Ukne JG, Wells MT. Timecourse of endotoxemia and cardiovascular changes in heat-stressed primates. Aviation Space Environ Med 1987;58:1061-74.
18 Cech AC, Shou J, Gallagher H, Daly JM. Glucocorticoidreceptor blockage reserves postinjury macrophage suppres-sion. Arch Surg 1994;129:1227-32.
19 Snyder DS, Unanue ER. Corticosteroids inhibit murinemacrophage-Ia expression and interleukin-1 production. JImmunol 1982;129:1803-5.
20 Fertsch D, Schoenberg DR, Germain RN, Tou JYL, VogelSN. Induction of macrophage Ia antigen expression byIFN-alpha/beta and dexamethasone are mediated bychanges in steady state levels of Ia mRNA. _7 Immunol1987;139:244-9.
21 Petty HR, Martin SM. Combinative ligand-receptor inter-action effects of cAMP, epinephrine and met-enkephalinon RAW264 macrophage morphology, spreading, adher-ence and microfilaments. J Cell Physiol 1989;138:247-56.
22 Motyka B, Bhogal HS, Reynolds JD. Apoptosis of ileal Pey-er's patch B cells is increased by glucocorticoids oranti-immunoglobulin antibodies. Eur J Immunol 1995;25:1865-71.
23 Brandtzaeg P, Nilssen DE, Rognum TO, Thrane PS.Ontogeny of the mucosal immune system and IgAdeficiency. In: Gastroenterology clinics of North America.Edinburgh: WB Saunders 1991:397-440.
24 Mestecky J, Lue C, Russell MW. Selective transport of IgA:cellular and molecular aspects. In: Gastroenterology clinics ofNorth America, Edinburgh: WB Saunders, 1991:441-72.
25 Albanese CT, Smith SD, Watkins S, Kurtchubasche A, Sim-mons RL, Rowe MI. Effect of secretory IgA on transepithe-lial passage ofbacteria across the intact ileum in vitro.JAmColl Surg 1994;179:679-88.
26 Ayala A, Perrin MM, Chaudry IH. Defective macrophageantigen presentation following haemorrhage is associatedwith the loss of MHC class II (Ia) antigens. Immunology1990;70:33-9.
298
on March 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.50.4.294 on 1 April 1997. D
ownloaded from