Embed Size (px)
Citation preview

Review
Pathogen Molecular Pattern Receptor Agonists:Treating Cancer by Mimicking InfectionMark Aleynick1, Judit Svensson-Arvelund1, Christopher R. Flowers2,Aur�elien Marabelle3, and Joshua D. Brody1,4
Abstract
Immunotherapies such as checkpoint blockade haveachieved durable benefits for patients with advanced stagecancer and have changed treatment paradigms. However, thesetherapies rely on a patient's own a priori primed tumor-specificT cells, limiting their efficacy to a subset of patients. Becausecheckpoint blockade ismost effective in patients with inflamedor "hot" tumors, a priority in the field is learning how to "turncold tumors hot." Inflammation is generally initiated by innateimmune cells, which receive signals through pattern recogni-tion receptors (PRR)–a diverse family of receptors that sense
conserved molecular patterns on pathogens, alarming theimmune system of an invading microbe. Their immuno-stimulatory properties can reprogram the immune suppressivetumor microenvironment and activate antigen-presenting cellsto present tumors antigens, driving de novo tumor-specificT-cell responses. These features, among others, make PRR-targeting therapies an attractive strategy in immuno-oncology.Here, we discuss mechanisms of PRR activation, highlightingongoing clinical trials and recent preclinical advances focusedon therapeutically targeting PRRs to treat cancer.
IntroductionThe interplay between cancer and the immune system is a
double edged sword; the inflammation that recruits and acti-vates intratumoral immune cells can either eliminate cancercells or drive tumor progression in a context-dependent man-ner (1). Pattern recognition receptors (PRR) are a key family ofproteins involved in the inflammatory response. They areexpressed on a wide variety of innate and adaptive immunecells, as well as tumor cells, and recognize both foreignpathogen-associated molecular patterns (PAMP) and self-derived damage-associated molecular patterns (DAMP) result-ing from injury or cell death (1–3). There are five families ofPRRs: toll-like receptors (TLR), nucleotide-binding oligomeri-zation domain (NOD)-like receptors (NLR), C-type lectinreceptors (CLR), RIG-I–like receptors (RLR), and cytosolic DNAsensors (CDS; ref. 2). Each PRR family possesses distinctimmunomodulatory properties, making them attractive immu-notherapeutic targets. Here, we discuss PRR mechanisms andclinical implications to provide a detailed overview of the roleof PRRs in immuno-oncology.
TLRs in Cancer ImmunotherapyTLRs are the most widely studied PRR family, acknowledged in
the 2011 Nobel Prize awarded to Drs. Steinman, Beutler, andHoffman. Therehave been10TLRs identified inhumans and13 inmice (4); here we focus on the former. Structurally, TLRs are type Itransmembrane proteins characterized by a ligand-binding Nterminal ectodomain containing leucine-rich repeats, a singletransmembrane domain, and a cytosolic Toll/IL1R homologydomain responsible for signal transduction (2). TLRs 1, 2, and4–6 are located on the cell surface and recognize bacterial mem-brane components such as lipids, proteins, lipoproteins (Fig. 1;refs. 2, 3), as well as several self-molecules, including extracellularmatrix components, HSPs, and nuclear high-mobility groupbox 1 (HMGB1), often released as DAMPs from apoptotic ornecrotic cells (1, 3).
Intracellular TLRs 3 and 7–9 are locatedwithin endosomes, andrecognize viral and bacterial nucleic acids resulting from micro-bial replication or degradation upon entry into the cell (Fig. 1;refs. 1–3). Their localization normally prevents intracellular TLRsfrom binding self-nucleic acids. However, breakdown of thisspatial separation may trigger autoimmune disease through rec-ognition of self-nucleic acids (3, 5). Although TLR10 exists inhumans, it has been difficult to study as it is nonfunctional inmice. Recent work suggests it may serve as a negative regulator ofTLR signaling (6, 7). TLRs dimerize upon binding their cognateligand (Fig. 1), causing conformational changes that allow for therecruitment of adapter molecules (MyD88, TIRAP, TRIF, andTRAM), initiating signaling cascades that ultimately induce tran-scription of inflammatory mediators (2, 3, 8).
As TLRs are highly expressed on antigen-presenting cells (APC),targeting TLRs can activate APCs and trigger adaptive immuneresponses; intratumorally, this may shift a tolerogenic tumormicroenvironment (TME) to become immunogenic. However,because TLR signaling triggers inflammatory and cell survivalmechanisms, and certain tumors express TLRs, TLR activation
1Precision Immunology Institute, Icahn School of Medicine at Mount Sinai,New York, New York. 2Winship Cancer Institute of Emory University,Emory University School of Medicine, Atlanta, Georgia. 3Cancer Immuno-therapy Program, Gustave Roussy, Villejuif, France. 4Hematology andMedical Oncology, Icahn School of Medicine at Mount Sinai, New York,New York.
Corresponding Author: Joshua D. Brody, Icahn School of Medicine atMount Sinai, New York, NY 10029. Phone: 212-241-5426; Fax: 646-537-9268; E-mail: [email protected]
Clin Cancer Res 2019;XX:XX–XX
doi: 10.1158/1078-0432.CCR-18-1800
�2019 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org OF1
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

could instead be tumorigenic in certain settings (1, 9). BothTLR7 and TLR8 signaling have been implicated in driving lungcancer cell survival and chemotherapy resistance mechanisms(10, 11). TLR4 signaling in breast cancer both enhances chemo-therapeutic resistance and promotes angiogenesis and lymphaticmetastasis (12, 13). Tumor cells may also secrete HSPs andextracellular matrix factors as DAMPs, stimulating an immuno-suppressive program in tumor-associated macrophages (TAM)to promote angiogenesis and metastasis (14, 15). One recentstudy demonstrated that mice lacking TLR3/7/9 cleared implant-ed tumors through spontaneous induction of an adaptive anti-tumor response (16). Similar effects are observed with otherPRR families; galectin-9 signaling through the CLR dectin-1 onTAMs is protumorigenic in mouse models of pancreatic ductaladenocarcinoma, although signaling through this receptor inother cancers may have the opposite effect (17). While several
of these reports implicate DAMPs in tumor initiation and pro-gression through chronic inflammation, other studies demon-strate that DAMPs released from dying tumor cells are thehallmark of immunogenic cell death, activating APCs in theTME to present tumor antigen (9, 18). Despite the nuancedrole of PRR signaling in cancer, in many contexts, therapiestargeting PRR pathways have the ability to overcome immuno-suppression or drive a de novo antitumor response by activatingAPCs to enhance tumor antigen presentation (Fig. 2). For theremainder of this review, we will focus on clinical trials andpreclinical studies utilizing PRRs in this setting.
One of the few FDA-approved TLR-targeting therapies inoncology is Bacillus Calmette-Gu�erin (BCG), a strain ofMycobacterium bovis initially developed as a tuberculosis vaccine.Used as a urogenital cancer therapeutic for over 35 years, a largebody of work has dissected its mechanism, demonstrating that
RIG-I
5’-PPPshort dsRNA Long
dsRNA
dsRNATLR4 TLR3
TLR7/8 TLR9
ssRNACpGDNA
TriAcyllipo-
protein
DiAcyllipo-
proteinLPS
TLR4 TLR1/2 TLR2/6 TLR5
Flagellin
LGP2
MDA5
TBK1 IKK-i
TAB2 TAB3
RIP2
IKKα IKKβ
IL-1βPro-IL-1βPro-IL-18
Caspase-1
TAK1
NEMO
NF-κB AP-1
ISRE3
IRF7
ISRE7
Type 1 interferons Proinflammatory cytokines
NF-κB AP-1
TRAF3
MAV
S
NLRX1
TRAF6
MYD88TIRAP
CD
14
Endosome
Mitochondria
Cytosol
Cytosol
Plasma membrane
Nucleus
MYD88TIRAP
MYD88
IRAK4IRAK1 and/or
IRAK2
MAPKsignaling
MYD88
CARD9 BCL10MALT1
TIRAP
IRF3
LPB MD2
SYK
IL-18
ProCaspase-1ASCNLRP3
Alum
MDPFlagellin
iE-DAP
ProCaspase-1ASCNLRC4
ProCaspase-1ASCAIM2
cGAS
cGAMP
CytoslicdsDNA
NAIPNOD2NOD1
β-glucan
Dectin-1
Mannan
Dectin-2
TRAMTRIF
TRIFMYD88
MYD88
FCRγ
Endoplasmreticulum
STING
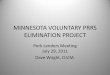
Figure 1.
Proinflammatory signaling pathways downstream of PRRs. Upon binding their respective ligands, each PRR conveys signal through specific adaptormolecules and signaling pathways, ultimately converging on production of proinflammatory cytokines and type 1 IFNs. Printed with permission fromMount Sinai Health System.
Aleynick et al.
Clin Cancer Res; 2019 Clinical Cancer ResearchOF2
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

BCG triggers an immune response by activating TLRs 2, 4, and9, and the NLR NOD2 (1, 19, 20). Several trials are combiningBCG therapy with checkpoint blockade or have expanded BCGto other cancers, with varying degrees of success (21).
TLR3 is one of the most actively explored TLR targets, with54 ongoing clinical trials using TLR3 agonists as single agents orin combination with other therapies to treat a broad list ofmalignancies (clinicaltrials.gov). TLR3 recognizes viral double-stranded RNA (dsRNA), and can be targeted using syntheticdsRNA analogs such as polyinosinic-polycytidylic acid (poly-IC;refs. 2, 3, 22). Poly-IC initially showed high toxicity and limitedtherapeutic benefit, but several poly-IC derivatives were subse-quently created to improve efficacy (22). One such derivativeis poly-ICLC, modified with poly-L-lysine and carboxymethylcel-lulose (Hiltonol, Oncovir) to increase stability in vivo, improvingits interferon (IFN) response to levels similar to those seen withattenuated viral infections (23, 24). Another derivative, poly-IC12U (rintatolimod/Ampligen, Hemispherx Biopharma), addsunpaired bases that reduce stability, effectively reducing toxicitywhile generating robust dendritic cell (DC)/T-cell responses (25).Preclinical data also suggests that rintatolimod recruits fewerregulatory T cells to the TME versus unmodified poly-IC, possiblyby losing ability to bind cytosolic RLRs (26). Recently completed
trials using poly-ICLC demonstrate its potent ability to induceadaptive immune responses against a range of solid and hemato-poietic cancers. A phase I study evaluating peptide-pulsed DCvaccination in combination with poly-ICLC for pancreatic cancershowed promise with a 7.7 month median survival, an improve-ment over the 4.2–4.9 month survival seen with second-linechemotherapy in metastatic pancreatic cancer (27). A phase I/IIatrial in smolderingmultiple myeloma recently demonstrated thatpeptide þ poly-ICLC vaccination increased numbers of antigen-specific CD8 T-cells with an effector memory phenotype (28).Another study pinpointed TLR3þ DCs as key mediators of tumorantigen cross-presentation, where an in situ vaccination combin-ing poly-ICLC, Flt3 ligand, and local irradiation induced bothpartial and complete responses in patients with non-Hodgkinlymphoma (29). A pilot study in patients with transplant-ineligible hepatocellular carcinoma showed survival benefitcompared with historical controls using local tumor irradiationfollowed by intratumoral poly-ICLC administration (30). Simi-larly, studies treating patients with glioblastoma demonstratedimpressive survival outcomes by combining poly-ICLC withirradiation and/or alkylating chemotherapy (31, 32). In the pre-clinical setting, next-generation DC vaccines are being explored,employing nanoparticles to selectively deliver tumor antigens þ
Tumorcells
Oncolyticvirus
Chemotherapy
Cytotoxic antitumorimmune response
CD8+T cell
NK cell
Dendriticcell
TLRNLR
Tumorantigencross-
presentation
CLR
CDS
RLR
BCG
RLR
TLRTAM
RLR
Immunogeniccell death
CDS
Poly-ICLC
Viral genomeTumor DNATumor-associated antigenCytokines, chemokines,type 1 interferons
Radiotherapy
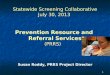
Figure 2.
PRR pathways in antitumor immunity. Therapeutic activation of PRR pathways can induce immunogenic cell death in cancer cells, releasing DAMPsand tumor-associated antigens. PRR ligands can reprogram immunosuppressive TAMs, and activate DCs to cross-present tumor antigens, stimulatinga cytotoxic antitumor immune response. Printed with permission from Mount Sinai Health System.
Pattern Recognition Receptors in Immuno-oncology
www.aacrjournals.org Clin Cancer Res; 2019 OF3
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

poly-IC to DCs in vivo, eliminating the need for ex vivo DCmanipulation (33). In addition, several groups have also dem-onstrated that TLR3 activation can help overcome resistance tocheckpoint blockade, leading to ongoing academic and pharmatrials planning to accrue >400 patients studying combinations ofpoly-ICLC with PD-1, PD-L1, or CTLA-4 blockade to treat variouscancers (e.g., NCT03121677 and NCT03633110).
TLR4 is canonically involved in the recognition of bacteriallipopolysaccharide (LPS), although it is also indirectly involv-ed in viral infection by recognizing DAMPs, such as HMGB1,HSPs, and extracellular matrix components released frominfected or dying cells (1, 3, 8). Ongoing clinical efforts withTLR4 ligands in cancer immunotherapy include the FDA-approved TLR4 agonist AS04 (GlaxoSmithKline), a monopho-sphoryl lipid A (MPLA) LPS derivative in alum. AS04 is used asan adjuvant in the (human papillomavirus) HPV-16/18 vaccineCervarix, which in a landmark trial was shown to not onlyprotect women from cervical cancer from the vaccine-inclusivestrains, but was also cross-reactive against other oncogenicforms of HPV (34). Interestingly, two recent phase III trialsof a MAGE-A3 vaccine with AS15 (GlaxoSmithKline), an adju-vant containing MPLA and a TLR9 agonist, both failed toimprove patient survival, citing low CD8 T-cell responses inpatients (35, 36). Another TLR4 agonist, a synthetic analog ofglucopyranosyl lipid A engineered to decrease heterogeneityand minimize toxicity over natural lipid A formulated in astable emulsion (GLA-SE/G100; Immune Design), showedpromise in a phase I study of Merkel Cell Lymphoma, where2 of 10 patients had durable sustained antitumor responses,whereas 2 others had complete responses (37). Similarly,encouraging clinical responses were seen in 26 patients withfollicular lymphoma receiving intratumoral G100 and radio-therapy with or without PD-1 blockade, where >80% diseasecontrol rates were seen in both groups, and addition of anti-PD-1 benefited relapsed and chemo-refractory patients (38).
TLR5 is unique in that it does not recognize DAMPs as itsonly ligand is bacterial flagellin, making it a potentially usefulimmunotherapeutic target (39). Two TLR5 agonists in clinicaldevelopment, entolimod and mobilan (Cleveland Bio Labs),have shown preclinical efficacy in several tumor models(39–41). Entolimod is a flagellin derivative engineered to reducetoxicity, currently being investigated in a phase II trial as aneoadjuvant therapy for colorectal cancer (NCT02715882;ref. 42). Mobilan is an adenovirus construct that upon infectioninduces co-expression of TLR5 and a secreted form of entolimod,creating an autocrine signaling loop and inflammatory sig-nature in the TME (41). Mobilan has shown preclinical efficacyfor prostate cancer, which expresses high levels of the adenovirusreceptor necessary for its entry, and is now in a phase I/II trial(NCT02844699; ref. 41).
Both TLR7 and TLR8 are functional in humans, whereas miceonly have functional TLR7. TLR7/8 recognizes single-strandedRNA from RNA viruses, although RNA from certain bacterialstrains may also ligate these TLRs (8). TLR7/8 also recognizespurine analogs such as imidazoquinolines, as well as guaninederivatives and certain siRNA (3). Ligation of TLR7/8 triggersrobust proinflammatory cytokine production, and is critical forthe activation of plasmacytoid DC (pDC), a key source of type 1IFNs (3, 8). The only FDA-approved TLR7/8 agonist is imiquimod(Aldara; 3MPharmaceuticals), an imidazoquinoline topical agentfor the treatment of basal-cell carcinoma (BCC) that both
enhances local immune response and directly induces apoptosisin BCC cells (43). Imiquimod is being investigated in phase IIIstudies as a treatment for gynecologic cancers with promisingearly results (44), and in dozens of phase I and II trials in variouscancers, either alone or combination (clinicaltrials.gov). Otherimidazoquinoline derivatives in the clinic include a topical gelformulation of resiquimod, a more potent imidazoquinolineinvestigated as an adjuvant to NY-ESO-1 vaccination for patientswith melanoma that has been shown to induce NY-ESO-specificCD8 T-cell responses (45). DSP-0509 (Boston Biomedical), aTLR7/8 agonist formulated for intravenous delivery, has shownpreclinical efficacy in several tumor models and is now beinginvestigated in a phase I trial (NCT03416335; ref. 46).MEDI9197(3M-052; Medimmune) is an imidazoquinoline formulated forintratumoral injection and optimal tumor retention to improvesafety. Preliminary phase I results (NCT02556463) demonstrateintratumoral immune cell infiltration and low serum MEDI9197levels, indicating effective retention in the TME (47). Similarly,NKTR-262 (Nektar Therapeutics) is a TLR7/8 agonist formulatedfor intratumoral retention to minimize systemic exposure (48)and has shown potent efficacy, where treatment of one tumor siteled to clearance of untreated contralateral tumors in multiplepreclinical models, an abscopal effect often considered the holygrail of intratumoral immunotherapy. These promising resultsled to a recently opened phase I/II study of NKTR-262 in com-bination with a CD122 agonistic antibody and checkpointblockade (NCT03435640; ref. 49). A recent randomized studyof platinum-based chemoimmunotherapy for head/neck can-cers demonstrated no overall survival benefit by adding theTLR8 agonist motolimod (Array Biopharma/Celgene), althoughmotolimod did improve survival in subsets of patients withHPVþ tumors (50).
TLR9 recognizes unmethylated 20-deoxyribo(cytidine-phosphate-guanosine) (CpG) motifs, which occur more fre-quently in prokaryotic DNA. Similar to TLRs 7/8, TLR9 is highlyexpressed on pDCs, as well as on B cells, and is critical in theimmune response to DNA viruses (3, 8). Synthetic CpG oligo-deoxynucleotides (ODN) potently activate TLR9-expressingimmune cells and have been divided into four classes: Class A,B, C, and P (51, 52). Class A ODNs contain palindromic phos-phodiester CpG central sequences with phosphorothioate Grich ends, allowing tetrad formation, enhanced stability, endo-somal uptake, and robust activation of pDC type 1 IFN responses.Class B ODNs are short, linear phosphorothioate backbonessDNA strands, and potent activators of B and natural killer(NK) cells. Class C ODNs combine properties of class Aand B, activating both B and NK cells, as well as type 1 IFNpDC responses. Class P ODNs feature multiple palindromicsequences and form multimeric structures, enhancing stabilityand immunostimulatory responses (52). The first ODN inhuman trialswas CpG7909 (agatolimod/PF-3512676/ProMune;Pfizer), a class B ODN, which showed early promise both asan in situ vaccination and chemotherapy adjuvant (53–55).However, a phase III lung cancer trial of chemotherapy with orwithout this ODN concluded that CpG7909 increased adverseevents without benefiting survival, curtailing its development.Two other phase III trials that investigated CpG7909 as part ofa MAGE-A3 vaccination also failed to demonstrate clinicalbenefit (35, 36).
Despite failures with CpG7909, several CpG ODNs modifiedto enhance efficacy and safety are in development. CMP-001
Aleynick et al.
Clin Cancer Res; 2019 Clinical Cancer ResearchOF4
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

(Checkmate Pharmaceuticals), a class A ODN packaged withina virus-like particle, potently activates intratumoral pDCs andovercomes resistance to checkpoint blockade; five trials withthis ODN are ongoing for various solid tumors (clinicaltrials.gov; ref. 56). Tilsotolimod (IMO-2125; Idera Pharmaceuticals)is another TLR9 agonist that is being investigated in checkpointblockade refractory patients. In patients who failed anti-PD-1therapy, tilsotolimod combined with ipilimumab CTLA-4blockade improved objective tumor responses over ipilimu-mab alone, and this combination has entered a phase III trial(NCT03445533; ref. 57). Lefitolimod (MGN1703, MologenAG) is a novel class of ODN that lacks phosphorothionatebackbone modifications and is instead "dumbbell shaped" toprevent degradation (51). Demonstrating favorable safety andclinical efficacy, lefitolimod has initiated a phase III trial inmetastatic colorectal cancer (NCT02077868; refs. 58, 59).Another class C agonist, SD-101 (Dynavax), is being investi-gated in several trials, after showing both preclinical andclinical efficacy in melanoma and as an in situ vaccination forlymphoma, in combination with checkpoint blockade andagonistic antibodies for T-cell costimulation (55, 60–62).DV281, a TLR9 agonist formulated for inhalation, is beinginvestigated as an adjuvant for PD-1 checkpoint blockadetherapy in lung cancer (NCT03326752), where intratumoralinjection of adjuvant is more challenging. Notably, anotherDynavax TLR9 agonist tested in a large randomized trial diddemonstrate superior immunogenicity (seroconversion) whencombined with HBsAg as compared with standard HBV vacci-nation, leading to its FDA approval. Potentially, this immu-nostimulatory effect could portend success in cancer therapy asnow shown with pathogen vaccines.
NLR in Cancer ImmunotherapyNLRs are intracellular PRRs that recognize a diverse set of
ligands including bacterial and viral PAMPs, as well as DAMPs(reviewed in ref. 61; refs. 2, 3, 8, 63). Of several NLR families,the NLRC and NLRP families are the most well-studied (2, 63).NOD1 and NOD2 are prominent NLRC family members,which all contain N-terminal CARD domains. Similar to TLR2,NOD1 and NOD2 recognize components of the peptidoglycanbacterial cell wall, where NOD1 specifically recognizes gamma-D-glutamyl-meso-diaminopemelic acid and NOD2 recognizesmuramyl dipeptide (Fig. 1; refs. 8, 63). NLRPs, NLRP3 beingthe most well characterized, form part of the inflammasome,which leads to production of proinflammatory IL-1b/IL-18(Fig. 1). Besides several bacterial ligands, environmental pol-lutants such as asbestos and silica are known to initiate NLRinflammasomes (64).
Mifamurtide, a synthetic analog of muramyl tripeptide andNOD2 agonist, is approved in the European Union in combi-nation with chemotherapy to treat osteosarcoma (4, 65). TheTLR8 agonist, motolimod, is also a potent stimulator of theNLRP3 inflammasome, likely because of the molecule's lipo-philic structure; however the specific mechanism is still underinvestigation (50, 66). In addition, particulate adjuvants suchas alum and saponins, often used in cancer vaccine formula-tions including HPV and the previously mentioned MAGE-A3vaccine studies (35, 36), are potent activators of the NLRP3inflammasome, producing inflammatory cytokines to engenderadaptive immune responses (67, 68).
CLR in Cancer ImmunotherapyCLRs are a large family of receptors that contain at least one
carbohydrate recognition domain, recognizing mannose, fructose,andglucanspresentonpathogens (reviewed inref.67; refs.2,8,69).Although classically associated with antifungal and mycobacterialimmune responses, more recent evidence suggests CLRs areinvolved in sensing numerous pathogens including bacteria, virus-es, and helminths, as well as DAMPs (69–71). CLRs are mainlyexpressed by DCs, although monocytes/macrophages, B cells, andneutrophils may also express CLRs. Most CLR family members aretransmembrane receptors, although a few may be released assoluble proteins, such as mannose-binding-lectin (4, 69). Uponligation, CLRs transduce signal by either associating with kinasesand phosphatases directly, or by recruiting ITAM-containing co-receptors such as FcRg (Fig. 1; refs. 8, 69). Signaling ultimatelyconverges on MAPK and NF-kB, allowing CLRs to influencesignaling cascades fromother PRRs, tailoring the immune responseagainst specific pathogens. In addition,manyCLRs are internalizedafter activation, bringing their ligand cargo within the cell fordegradation and subsequent antigen presentation, a critical processin activating the adaptive immune response (69).
Strategies targeting CLRs date back over two decades. Random-ized studies with a mannan-MUC1 fusion protein targeting man-nose receptor (MR), vaccinating patients with breast cancer aftersurgical resection, showed significant protection from recurrence,demonstrating the efficacy of CLR targeting and the importanceof adaptive immunity in preventing recurrence (72). Anti-CLRantibodies have also been used to target CLR-expressing DCs.CDX-1307 (Celldex Therapeutics) is an MR-specific antibodyfused tohuman chorionic gonadotropinbeta-chain (HCG-b), com-monly overexpressed in various cancers (73). Vaccinating withCDX-1307, GM-CSF, poly-ICLC, and/or resiquimod to matureDCs, most treated patients developed humoral response againstHCG-b, and some developed T-cell responses. CombiningCDX-1401 (Celldex Therapeutics), an anti-DEC-205 antibodyfused to NY-ESO-1 antigen, with poly-ICLC and/or resiquimod,yielded humoral and T-cell responses in most patients that cor-related with stable disease (74). In addition, several patientswho progressed saw dramatic benefit with subsequent check-point blockade, warranting studies of this combination therapy.CDX-1401 is currently being investigated in gynecologic(NCT02166905) and hematologic (NCT03358719) malignancies.CMB305 (Immune Design) is a Sindbis virus engineered to useDC-SIGN as an attachment receptor, selectively infecting andexpressing NY-ESO-1 protein in DCs for antigen presentation(75). CMB305 is being investigated in a phase III trial in syno-vial sarcoma (NCT03520959). Another therapy, Imprime PGG(Biothera), uses IV yeast-derived soluble b-glucan, a dectin-1ligand, to sensitize patients and boost efficacy of targeted therapyand anti-PD-1 blockade, and is being investigated in several phase Iand II studies (clinicaltrials.gov) with promising early results.Interestingly, Imprime PGG shows amoderate toxicity profile, with22% of patients discontinuing treatment due to adverse events,possibly because of the route of administration and the drug'spotent activation of the complement cascade (76).
Cytosolic Viral Sensors–RLR and CDSWhile TLR3 is responsible for detecting viral dsRNA within
endosomal compartments, RLRs retinoic acid–inducible gene I(RIG-I), melanoma differentiation–associated gene 5 (MDA5),
Pattern Recognition Receptors in Immuno-oncology
www.aacrjournals.org Clin Cancer Res; 2019 OF5
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

and laboratory of genetics and physiology 2 (LGP2) recognizecytosolic dsRNA (Fig. 1; reviewed in ref. 75; ref. 77). These sen-sors are critical in the host antiviral response and are expressedwithin most cell types, including cancer cells (4). Structurally,RLR family members contain a C-terminal RNA binding domain,a DExD/H central domain for ATP catalysis and activation, andan N-terminal CARD domain that interacts with the downstreameffector molecule MAVS (also referred to as IPS-1) to conveysignaling. Short dsRNA with 50 triphosphate (50-PPP) ends arepreferentially recognized by RIG-I, whereas MDA5 recognizeslonger dsRNA fragments, including poly-IC. While LGP2 alsorecognizes dsRNA, this family member cannot convey down-stream signaling because it lacks a CARD domain, and is insteadimportant in regulating RIG-I and MDA5 activation (8, 77).Stimulation of epithelial ovarian cancer cells with a RIG-I–specific agonist triggers type I IFN release and immunogenicapoptosis, which effectively matures DCs upon phagocytosisof these apoptotic cancer cells (78). In addition, activation ofRIG-I using 50-PPP RNA or MDA5 using poly-IC causes apoptosisin human melanoma cells both in vitro and in vivo, whereasadjacent nonmalignant cells are spared because of intact anti-apoptotic BCL-XL signaling (79).
The multimodal action of RLRs in immune cell activationwhile simultaneously triggering immunogenic cell death incancer cells makes this pathway a particularly attractive immu-notherapeutic target. The successes of poly-ICLC in clinicaltrials can in part be attributed to its dual agonistic activity onTLR3 and MDA5. BO-112 (Bioncotech) is another poly-ICderivative that potently activates RLR signaling in addition toTLR3, and is currently in phase I trials with promising earlyresults (NCT02828098; ref. 80). One synthetic RIG-I–specificligand, RGT100/MK-4621 (Merck) has initiated human trials,after preclinical data demonstrated potent antitumor activity inmelanoma and colon carcinoma models (81). A phase I/II trialin solid tumors began in 2017 (NCT03065023), yielding onlystable diseases as best response with intratumoral therapy (82).Pharmacokinetic studies show intratumorally administeredMK-4621 is well retained in the TME, helping minimize adverseevents due to systemic toxicity. Numerous RLR agonistsare currently in active preclinical development and will likelybe seen in the clinic soon.
As cellular DNA is ordinarily restricted to the nucleus andmitochondria, aberrant cytosolic DNA arising from viral infec-tion or cell damage triggers immunogenic signaling by activat-ing ubiquitously expressed CDS. To date, several pathways forsensing cytosolic DNA have been described. DNA can be tran-scribed in the cytosol, generating a dsRNA molecule that can berecognized by RIG-I, triggering an inflammatory response tocytosolic DNA in an RLR-dependent fashion (8). In addition,cytosolic DNA can be recognized by absent in melanoma2 (AIM2), prompting inflammasome assembly, resulting inIL-1b/IL-18 production (Fig. 1; ref. 8). Perhaps the most impact-ful CDS is the stimulator of interferon genes (STING) pathway.Knockout studies indicate that STING is critical for host type IIFN and NF-kB responses to synthetic and viral DNA, whereasSTING deletion had no impact on AIM2-mediated IL-1b pro-duction and the TLR9 CpG DNA response (83). STING is alsoessential for a successful adaptive immune response to DNAvaccination. Several other CDSs such as DNA-dependent acti-vator of IFN-regulatory factors (DAI) have been identified;however, deletion studies indicate they may serve redundant
function (8, 83, 84). In the context of infection, STING is a keymediator of the immune response against intracellular bacteria,DNA viruses, and retroviruses; however, its ability to detectgenomic DNA from dying tumor cells makes the STING path-way potentially important for antitumor immune responses.
The ability of the STING pathway to drive adaptive antitumorresponses has generated significant interest, and recent studiessuggest that efficacy of numerous DNA-damaging cancer ther-apies can in part be attributed to STING signaling. Chemother-apeutic agents cause DNA leakage into the cytosol, triggering aSTING-dependent type I IFN response (Fig. 2; ref. 85). STINGsignaling is also required for successful activation of adaptiveimmunity and tumor clearance in response to both radiother-apy (86) and T-cell checkpoint blockade, as cGAS-STING sig-naling enhances DC-mediated T-cell priming. Administrationof adjuvant cGAMP synergized with checkpoint blockade invivo, presumably by increasing the tumor reactive T-cellpool (87). Such studies highlight the importance of STINGand type I IFNs in DC cross-presentation of tumor antigens forantitumor T-cell priming.
Several STING-specific agonists recently entered clinical devel-opment. Originally investigated as a vascular disrupting agent,STING agonist DMXAA (ASA404/vadimesan, Antisoma/Novar-tis) showed preclinical efficacy, but failed in a pivotal phase IIItrial as a combination treatment with chemotherapy in non–small cell lung cancer (NSCLC; ref. 88). It was later shown to beineffective in patients due to STING polymorphisms that preventDMXAA binding (84, 89). MIW815 (ADU-S100, Aduro Biotech)is a cyclic dinucleotide human STING agonist currently in phase Itrials in combination with PD-1 (NCT03172936) or CTLA-4blockade (NCT02675439). MK-1454 (Merck), a similar cyclicdinucleotide agonist currently in a phase I trial in combinationwith PD-1 blockade (NCT03010176) has shown favorablesafety profiles and an objective response rate of 20% acrossseveral cancer types, with a median depth of response of approx-imately 80% (90). In addition, tumor clearance mediated byantibody blockade of CD47, a classical "do not eat me" signal,is STING dependent, where enhanced phagocytosis resultingfrom CD47 blockade ultimately requires STING and type I IFNsignaling toprimeT cells and inhibit tumor growth (91). Blockadeof CD47 is currently the focus of several clinical trials inboth hematopoietic and solid tumors (clinicaltrials.gov).
Oncolytic VirusesAmong the most rapidly evolving therapeutic approaches
in immuno-oncology is the use of oncolytic viruses (OV).Either through the intrinsic permissiveness of tumor cells forunchecked replication (including viral replication) or by direct-ly engineering the viral genome, OVs can selectively infect andkill tumor cells. Tumors are specifically susceptible to viralinfection and replication, as many of the pathways requiredfor oncogenesis can be coopted by OVs. While loss of tumorsuppressors such as p53 and RB, activation of RAS and similaroncogenes, disruption of IFN signaling components, as wellas a generally immunosuppressive TME all enable immuneescape and promote tumor growth, these pathways con-currently promote OV infection, replication, and inhibit viralclearance, creating a permissive space for OV growth that ispreferential to nontransformed tissue (92). OV infection inturn results in the immunogenic cell death of infected tumor
Aleynick et al.
Clin Cancer Res; 2019 Clinical Cancer ResearchOF6
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

Table 1. Ongoing clinical trials using TLR agonists
PRR Target Agent Combination Cancers investigated Phase Results Identifier
TLR2/4/9 þNOD2
BCG aPD-L1 Non–muscle-invasive bladdercancer
III Ongoing NCT03528694
BCG aPD-1 Non–muscle-invasive bladdercancer
III Ongoing phase IIresults (104)
NCT03711032
BCG Mitomycin C High risk non–muscle-invasivebladder cancer
III Ongoing NCT02948543
BCG Non–muscle-invasive bladdercancer
III Ongoing NCT03091660
TLR3 Rintatolimod þ tumor celllysate vaccination
Ovarian, fallopian tube, and primaryperitoneal cancer
I/II Ongoing NCT01312389
Rintatolimod þ peptidevaccination
GM-CSF Breast cancer I/II Ongoing NCT01355393
Poly-ICLC þ DC vaccine Metastatic pancreatic cancer I Results (27) NCT01410968Poly-ICLC þ peptidevaccination
Smoldering multiple myeloma I/IIa Results (28) NCT01718899
Poly-ICLC þ peptidevaccination
Breast cancer I Results (105) NCT01532960
Poly-ICLC Cyclophosphamide þradiotherapy
Hepatocellular cancer I/II Results (30) NCT00553683
Poly-ICLC CDX-301 þRadiotherapy
Low-grade B-cell lymphoma I/II Ongoing NCT01976585
Poly-ICLC þ peptidevaccination
aPD-1 þ Rituximab Follicular lymphoma I Ongoing NCT03121677
Poly-ICLC þ peptidevaccination
aPD-1 Melanoma, NSCLC, head and necksquamous cell carcinoma,urothelial, and renal cell carcinoma
I/II Ongoing NCT03633110
TLR4 þ TLR9 þNLRP3
AS15 þ MAGE-A3 vaccine Stage III melanoma III Results (35) NCT00796445
AS15 þ MAGE-A3 vaccine NSCLC III Results (36) NCT00480025TLR4 G100 Merkel cell carcinoma I Results (37) NCT02035657
G100 Cutaneous T-cell lymphoma II Ongoing NCT03742804G100 aPD-1 þ Rituximab Follicular low-grade non-Hodgkin
lymphomaI/II Ongoing NCT02501473
GSK1795091 aOX40, aICOS, or aPD-1 Advanced solid tumors I Ongoing NCT03447314GLA-SE þ MART-1 Antigenvaccine
Stage II–IV melanoma N/A Ongoing NCT02320305
TLR5 Entolimod Colorectal cancer II Ongoing NCT02715882Entolimod Advanced ormetastatic solid tumors I Results (42) NCT01527136Mobilan Prostate cancer I/II Ongoing NCT02844699
TLR7/8 Imiquimod Cervical intraepithelial neoplasia III Results (44) NCT00941252Resiquimod þ NY-ESO-1vaccine
Melanoma I Results (45) NCT00821652
DSP-0509 Neoplasms I Ongoing preclinicalresults (46)
NCT03416335
MEDI9197 aPD-L1 Solid tumors I Results (47) NCT02556463NKTR-262 aIL-2Rb þ aPD-1 Locally advanced or metastatic
solid tumorsI Ongoing NCT03435640
preclinical results (49)TLR8 þ NLRP3 Motolimod Cetuximab þ aPD-1 Head and neck squamous cell
carcinomaI Results (50) NCT02124850
TLR9 CMP-001 aPD-L1þ Radiotherapy NSCLC I Ongoing NCT03438318CMP-001 aPD-1 þ aCTLA-4 þ
RadiotherapyMetastatic colorectal cancer I Ongoing NCT03507699
CMP-001 aPD-1 Melanoma I Ongoing NCT03618641CMP-001 aPD-1 Advanced melanoma Ib Ongoing early
results (56)NCT03084640
CMP-001 aPD-1 Melanoma I Ongoing NCT02680184Tilsotolimod aCTLA-4 Anti-PD-1 refractory melanoma III Ongoing phase II
results (57)NCT03445533
Tilsotolimod aCTLA-4 or aPD-1 Metastatic melanoma I/II Ongoing NCT02644967Lefitolimod Metastatic colorectal cancer III Ongoing phase II
results (58)NCT02077868
Lefitolimod aCTLA-4 Advanced solid tumors 1 Ongoing NCT02668770SD-101 Radiotherapy Low-grade B-cell lymphoma I/II Results (55) NCT02266147SD-101 aPD-1 Metastatic melanoma/head and
neck cancerIb/II Ongoing early
results (60)NCT02521870
SD-101 Anti-OX40 Antibody þradiotherapy
Low-grade B-cell non-Hodgkinlymphomas
I Ongoing preclinicalresults (61)
NCT03410901
DV281 aPD-1 NSCLC I Ongoing NCT03326752
Pattern Recognition Receptors in Immuno-oncology
www.aacrjournals.org Clin Cancer Res; 2019 OF7
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

cells, initiating de novo antitumor immune responses or boost-ing existing responses through mechanisms discussed in theabove sections (Fig. 2). Cancer cells infected with the polio OVPVSRIPO (Istari Oncology) release DAMPs (HMGB1, HSP60/70/80) and PAMPs (viral dsRNA), activating DCs to drive atumor-antigen–specific cytotoxic T-cell response (93). Similarto other intratumorally delivered PRR agonists, the innate–adaptive immune axis is critical for OV therapy, as the ability toinduce systemic antitumor immunity is antigen restricted to theOV infected site. Using a Newcastle disease OV and contralat-eral B16 and MC38 tumors, Zamarin and colleagues demon-strate that OV injection of one tumor results in immunity onlyagainst that same tumor type (94). Talimogene laherparepvecor T-VEC (Amgen), a modified herpes virus expressing GM-CSF,was approved in 2015 for the treatment of late-stage metastaticmelanoma, earning a place for OV therapy in the clinic. In alandmark phase III study, intratumoral injection of T-veccaused complete resolution in 47% of injected lesions, as wellas 22% of noninjected visceral lesions, highlighting the powerof OV therapy to induce systemic antitumor immunity (95). T-VEC has already been effectively combined with CTLA-4 block-ade, where a randomized phase II study demonstrated anincrease in objective response rates from 18% with CTLA-4monotherapy to 39% in the combination group (96), and isbeing investigated aggressively, including combinations withPD-1 blockade (NCT02965716), with neoadjuvant chemother-apy (NCT02779855), and with preoperative radiotherapy(NCT02453191). Other promising OV platforms in late devel-opment include Pexa Vec (JX-594, SillaJen), a vaccinia virusalso engineered to express GM-CSF, currently in a phase III trialfor hepatocellular carcinoma in combination with the kinaseinhibitor sorafenib (NCT02562755). A modified Coxsackievirus, CAVATAK (Viralytics), is currently in phase II trials forseveral indications (clinicaltrials.gov). Moving beyond GM-CSF
as the genetic payload, Swedish biotech Lokon recently openeda trial of their lead candidate LOAd703, an adenovirus encod-ing the costimulatory ligands CD40L and 4-1BBL(NCT03225989). Upon infection, tumor and other cells in theTME begin to express costimulatory ligands, helping to activateNK effector cells and remodel the TME (97). OVs without atherapeutic payload, including Pelareorep (Reolysin, OncolyticsBiotech) and PVSRIPO, are in active clinical development aswell. Recently published phase I data shows PVSRIPO increased36 month overall survival to 21% in patients with recurrentglioblastoma, a major increase from the 4% survival seen inhistorical controls (98). Taken together, all of these differentsuccessful approaches with OVs substantiate the idea that induc-tion of immunogenic tumor cell death in combination with PRRagonism can drive effective adaptive immune responses.
PerspectivesPattern recognition receptors present potentially powerful
weapons in the cancer immunotherapy armory. Their ability tomodulate numerous aspects of the tumor microenvironment,fromAPCs and their cross-talk with T cells, to directlymodulatingcancer cells themselves, allow these pathways to shape andultimately drive an antitumor immune response. As PRR agonistsand oncolytic viruses trigger innate cells to activate adaptiveimmunity, combining these approaches with checkpoint block-ade therapy effectively presses the gas pedal while cutting thebrakes, unleashing the full potential of immune effector cells. PRRagonism could additionally reverse resistance in checkpointrefractory tumors (99), and synergize with standard-of-care ther-apies including chemotherapy (100) and anti-CD20 targetingagainst lymphoma (101); a variety of combinatorial approachesare being actively explored in clinical trials (Tables 1–4). Preclin-ical approaches focused on developing next-generation agonists
Table 2. Ongoing clinical trials using NLR and CLR agonists
PRR Target Agent Combination Cancers investigated Phase Results Identifier
NOD2 Mifamurtide Chemotherapy High risk osteosarcoma II Ongoing NCT03643133DEC-205 þ TLR3 þ TLR7 CDX-1401 Poly-ICLC þ resiquimod Advanced cancers I/II Results (74) NCT00948961DEC-205 þ TLR3 CDX-1401 Poly-ICLC þ epacadostat Ovarian, fallopian tube, and primary
peritoneal cancer in remissionI/II Ongoing NCT02166905
CDX-1401 Poly-ICLC þ aPD-1 þ decitabine Myelodysplastic syndrome or acutemyeloid leukemia
I Ongoing NCT03358719
DC-SIGN CMB305 Synovial sarcoma III Ongoing earlyphase IIresults (106)
NCT03520959
Dectin-1 Imprime PGG Cetuximab þ paclitaxel þcarboplatin
NSCLC II Results (76) NCT00874848
Imprime PGG aPD-1 NSCLC Ib/II Ongoing NCT03003468Imprime PGG aPD-1 Advanced melanoma, triple-
negative breast cancerII Ongoing NCT02981303
Imprime PGG Rituximab Relapsed indolent non-Hodgkinlymphoma
II Ongoing NCT02086175
Imprime PGG aPD-L1 þ Bevacizumab Metastatic colorectal cancer I/II Ongoing NCT03555149
Table 3. Ongoing clinical trials using RLR and CDS agonists
PRR Target Agent Combination Cancers investigated Phase Results Identifier
RIG-I MK4621 Advanced solid tumors I/II Results (82) NCT03065023MK4621 aPD-1 Advanced solid tumors I Ongoing NCT03739138
STING MIW815 aPD-1 Advanced solid tumors or lymphomas I Ongoing NCT03172936MIW815 aCTLA-4 Advanced solid tumors or lymphomas I Ongoing NCT02675439MK-1454 aPD-1 Advanced solid tumors or lymphomas I Ongoing NCT03010176
Early results (90)
Aleynick et al.
Clin Cancer Res; 2019 Clinical Cancer ResearchOF8
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

are underway; one group recently developed an OV-packagedanti-CTLA4 antibody construct, effectively combining OV andcheckpoint therapy into a single injection (102). Others havefused Resiquimod nanoparticles to PD-1–targeting antibodies,allowing PD-1þ T cells to selectively deliver the TLR7 agonist tothe tumor, reshaping the TME to improve T-cell infiltration anddisease control (103). These approaches highlight the immuno-modulatory potency of PRRs, where their ability to overcomeimmunosuppression and drive adaptive immunity effectivelyenhances efficacy of concurrently administered therapies. Withsomany novel agonists being investigated preclinically and in theclinic, continued exploration andunderstanding of PRRpathwaysand targeting will help to shape treatment paradigms in immuno-oncology.
Disclosure of Potential Conflicts of InterestC. R. Flowers reports receiving other commercial research support from
Abbvie, Acerta, BeiGene, Celgene, Gilead, Genentech/Roche, Janssen Pharma-ceuticals, Millennium/Takeda, Pharmacyclics, and TG Therapeutics, and is aconsultant/advisory board member for Abbvie, AstraZeneca, Bayer, BeiGene,Celgene, Denovo Biopharma, Genentech/Roche, Gilead, Karyopharm, Phar-macyclics/Janssen, and Spectrum. A. Marabelle reports receiving commercialresearch grants from Transgene, speakers bureau honoraria from Amgen andMSD, and is a consultant/advisory board member for AstraZeneca, LytixPharma, MSD, Bioncotech, and Oncovir. J.D. Brody reports receiving commer-cial research grants from Merck, Genentech, and Bristol-Myers Squibb. Nopotential conflicts of interest were disclosed by the other authors.
Received January 29, 2019; revised April 8, 2019; accepted May 16, 2019;published first May 23, 2019.
References1. Rakoff-Nahoum S, Medzhitov R. Toll-like receptors and cancer. Nat Rev
Cancer 2009;9:57–63.2. Kawai T, Akira S. Toll-like receptors and their crosstalk with other innate
receptors in infection and immunity. Immunity 2011;34:637–50.3. Kawai T, Akira S. The role of pattern-recognition receptors in innate
immunity: update on toll-like receptors. Nat Immunol 2010;11:373–84.
4. Shekarian T, Valsesia-Wittmann S, Brody J,MichalletMC,Depil S, CauxC,et al. Pattern recognition receptors: immune targets to enhance cancerimmunotherapy. Ann Oncol 2017;28:1756–66.
5. Barton GM, Kagan JC. A cell biological view of toll-like receptor function:regulation through compartmentalization. Nat Rev Immunol 2009;9:535–42.
6. Oosting M, Cheng S-C, Bolscher JM, Vestering-Stenger R, Plantinga TS,Verschueren IC, et al. Human TLR10 is an anti-inflammatory pattern-recognition receptor. Proc Natl Acad Sci U S A 2014;111:E4478–84.
7. Lee SM-Y, Yip T-F, Yan S, Jin D-Y, Wei H-L, Guo R-T, et al. Recognition ofdouble-stranded RNA and regulation of interferon pathway by toll-likereceptor 10. Front Immunol 2018;9:516.
8. Takeuchi O, Akira S. Pattern recognition receptors and inflammation. Cell2010;140:805–20.
9. Pradere JP, Dapito DH, Schwabe RF. The Yin and Yang of toll-likereceptors in cancer. Oncogene 2014;33:3485–95.
10. Chatterjee S, Crozet L, Damotte D, Iribarren K, Schramm C, Alifano M,et al. TLR7 promotes tumor progression, chemotherapy resistance, andpoor clinical outcomes in non-small cell lung cancer. Cancer Res 2014;74:5008–18.
11. Cherfils-Vicini J, Platonova S, Gillard M, Laurans L, Validire P, CaliandroR, et al. Triggering of TLR7 and TLR8 expressed by human lung cancer cellsinduces cell survival and chemoresistance. J Clin Invest 2010;120:1285–97.
12. Yang H, Wang B, Wang T, Xu L, He C, Wen H, et al. Toll-like receptor 4prompts human breast cancer cells invasiveness via lipopolysaccharidestimulation and is overexpressed in patients with lymph nodemetastasis.PLoS One 2014;9:e109980.
13. Volk-Draper L, Hall K, Griggs C, Rajput S, Kohio P, DeNardo D, et al.Paclitaxel therapy promotes breast cancermetastasis in a TLR4-dependentmanner. Cancer Res 2014;74:5421–34.
14. Li D, Wang X, Wu J-L, Quan W-Q, Ma L, Yang F, et al. Tumor-producedversican V1 enhances hCAP18/LL-37 expression in macrophages throughactivation of TLR2 and vitamin D3 signaling to promote ovarian cancerprogression in vitro. PLoS One 2013;8:e56616.
15. Kim S, Takahashi H, Lin WW, Descargues P, Grivennikov S, Kim Y, et al.Carcinoma-produced factors activate myeloid cells through TLR2 tostimulate metastasis. Nature 2009;457:102–6.
16. Klein JC,Moses K, ZelinskyyG, Sody S, Buer J, Lang S, et al. Combined toll-like receptor 3/7/9 deficiency on host cells results in T-cell-dependentcontrol of tumour growth. Nat Commun 2017;8:14600.
17. Daley D, Mani VR, Mohan N, Akkad N, Ochi A, Heindel DW, et al. Dectin1 activationonmacrophages by galectin9promotes pancreatic carcinomaand peritumoral immune tolerance. Nat Med 2017;23:556–67.
18. Mellman I, Coukos G, Dranoff G. Cancer immunotherapy comes of age.Nature 2011;480:480–9.
19. Biot C, Rentsch C, Gsponer J, Birkh€auser FD, Jusforgues-Saklani H,Lema�tre F, et al. Preexisting BCG-specific T cells improve intravesicalimmunotherapy for bladder cancer. Sci Transl Med 2012;4:137ra72.
20. DivangahiM,Mostowy S, Coulombe F, Kozak R, Guillot L, Veyrier F, et al.NOD2-deficient mice have impaired resistance to mycobacterium tuber-culosis infection through defective innate and adaptive immunity.J Immunol 2008;181:7157–65.
21. Marabelle A, Kohrt H, Caux C, Levy R. Intratumoral immunization: a newparadigm for cancer therapy. Clin Cancer Res 2014;20:1747–56.
Table 4. Ongoing clinical trials using oncolytic viruses
Virus Agent Combination Cancers investigated Phase Results Identifier
Herpes simplex T-Vec aCTLA-4 Melanoma Ib/II Results (96) NCT01740297T-Vec aPD-1 Stage III/IV melanoma II Ongoing NCT02965716T-Vec Paclitaxel Triple-negative breast cancer I/II Ongoing NCT02779855T-Vec Radiotherapy Soft tissue sarcoma I/II Ongoing NCT02453191
Vaccinia poxvirus Pexa Vec Sorafenib Hepatocellular carcinoma III Ongoing NCT02562755Pexa Vec aPD-1 Renal cell carcinoma Ib Ongoing NCT03294083Pexa Vec aPD-1 Hepatocellular carcinoma I/IIa Ongoing NCT03071094
Coxsackievirus CAVATAK Stage IIIC–IV melanoma II Results (107) NCT01636882CAVATAK aCTLA-4 Advanced melanoma I Ongoing NCT02307149CAVATAK aPD-1 Advanced NSCLC I Ongoing NCT02824965
Adenovirus LOAd703 Pancreatic, ovarian, biliary, and colorectal cancer I/II Ongoing NCT03225989Enterovirus PVSRIPO Recurrent glioblastoma I Results (98) NCT01491893
PVSRIPO Unresectable melanoma I Ongoing NCT03712358Reovirus Pelareorep Paclitaxel Metastatic breast cancer II Results (108) NCT01656538
Pelareorep aPD-1 Advanced pancreatic cancer II Ongoing NCT03723915
Pattern Recognition Receptors in Immuno-oncology
www.aacrjournals.org Clin Cancer Res; 2019 OF9
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

22. Martins KA, Bavari S, Salazar AM. Vaccine adjuvant uses of poly-IC andderivatives. Expert Rev Vaccines 2015;14:447–59.
23. CaskeyM, Lefebvre F, Filali-Mouhim A, CameronMJ, Goulet J-P, HaddadEK, et al. Synthetic double-stranded RNA induces innate immuneresponses similar to a live viral vaccine in humans. J Exp Med 2011;208:2357–66.
24. Stahl-Hennig C, Eisenbl€atter M, Jasny E, Rzehak T, Tenner-Racz K,Trumpfheller C, et al. Synthetic double-stranded RNAs are adjuvantsfor the induction of T helper 1 and humoral immune responses tohuman papillomavirus in rhesus macaques. PLoS Pathog 2009;5:e1000373.
25. Navabi H, Jasani B, Reece A, Clayton A, Tabi Z, Donninger C, et al. Aclinical grade poly I:C-analogue (Ampligen) promotes optimal DC mat-uration and Th1-type T cell responses of healthy donors and cancerpatients in vitro. Vaccine 2009;27:107–15.
26. Theodoraki M-N, Yerneni S, Sarkar SN, Orr B, Muthuswamy R, Voyten J,et al. Helicase-driven activation of NFkB-COX2 pathway mediates theimmunosuppressive component of dsRNA-driven inflammation in thehuman tumor microenvironment. Cancer Res 2018;78:4292–302.
27. Mehrotra S, Britten CD, Chin S, Garrett-Mayer E, Cloud CA, Li M, et al.Vaccination with poly(IC:LC) and peptide-pulsed autologous dendriticcells in patients with pancreatic cancer. J Hematol Oncol 2017;10:82.
28. Nooka AK, Wang ML, Yee AJ, Kaufman JL, Bae J, Peterkin D, et al.Assessment of safety and immunogenicity of PVX-410 vaccine with orwithout lenalidomide in patients with smoldering multiple myeloma.JAMA Oncol 2018;4:e183267.
29. Hammerich L, Marron TU, Upadhyay R, Svensson-Arvelund J, DhainautM, Hussein S, et al. Systemic clinical tumor regressions and potentiationof PD1 blockade with in situ vaccination. Nat Med 2019;25:814–24.
30. De La Torre AN, Contractor S, Castaneda I, Cathcart CS, Razdan D, KlydeD, et al. A Phase I trial using local regional treatment, nonlethal irradi-ation, intratumoral and systemic polyinosinic-polycytidylic acid polyly-sine carboxymethylcellulose to treat liver cancer: in search of the abscopaleffect. J Hepatocell Carcinoma 2017;2017:4–111.
31. Butowski N, Chang SM, Junck L, DeAngelis LM, Abrey L, Fink K, et al. Aphase II clinical trial of poly-ICLC with radiation for adult patients withnewly diagnosed supratentorial glioblastoma: a North American BrainTumor Consortium (NABTC01-05). J Neurooncol 2009;91:175–82.
32. Rosenfeld MR, Chamberlain MC, Grossman SA, Peereboom DM, LesserGJ, Batchelor TT, et al. Amulti-institution phase II study of poly-ICLC andradiotherapy with concurrent and adjuvant temozolomide in adults withnewly diagnosed glioblastoma. Neuro Oncol 2010;12:1071–7.
33. Han HD, Byeon Y, Jang J-H, Jeon HN, Kim GH, Kim MG, et al. In vivostepwise immunomodulation using chitosan nanoparticles as a platformnanotechnology for cancer immunotherapy. Sci Rep 2016;6:38348.
34. Paavonen J, Naud P, Salmer�on J, Wheeler C, Chow S-N, Apter D, et al.Efficacy of humanpapillomavirus (HPV)-16/18AS04-adjuvanted vaccineagainst cervical infection and precancer caused by oncogenic HPV types(PATRICIA): final analysis of a double-blind, randomised study in youngwomen. Lancet 2009;374:301–14.
35. Dreno B, Thompson JF, Smithers BM, Santinami M, Jouary T, Gutzmer R,et al. MAGE-A3 immunotherapeutic as adjuvant therapy for patients withresected, MAGE-A3-positive, stage III melanoma (DERMA): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol 2018;19:916–29.
36. Vansteenkiste JF, ChoBC, Vanakesa T,De Pas T, ZielinskiM, KimMS, et al.Efficacy of the MAGE-A3 cancer immunotherapeutic as adjuvant therapyin patients with resected MAGE-A3-positive non-small-cell lung cancer(MAGRIT): a randomised, double-blind, placebo-controlled, phase 3trial. Lancet Oncol 2016;17:822–35.
37. Bhatia S, Miller NJ, Lu H, Vandeven NV, Ibrani D, Shinohara M, et al.Intratumoral G100, a TLR4 agonist, induces anti-tumor immuneresponses and tumor regression in patients with Merkel cell carcinoma.Clin Cancer Res 2019;25:1185–95.
38. Flowers C, PanizoC, Isufi I, Herrera AF,Okada C, Cull EH, et al. Long termfollow-up of a phase 2 study examining intratumoral G100 alone and incombination with pembrolizumab in patients with follicular lymphoma[abstract]. In: Proceedings of the 60th Annual Meeting and Exposition;2018 Dec 1–4; Washington, DC.
39. Brackett CM, Kojouharov B, Veith J, Greene KF, Burdelya LG, Gollnick SO,et al. Toll-like receptor-5 agonist, entolimod, suppresses metastasis and
induces immunity by stimulating an NK-dendritic-CD8þ T-cell axis.Proc Natl Acad Sci U S A 2016;113:E874–83.
40. Leigh ND, Bian G, Ding X, Liu H, Aygun-Sunar S, Burdelya LG, et al.A flagellin-derived toll-like receptor 5 agonist stimulates cytotoxiclymphocyte-mediated tumor immunity. PLoS One 2014;9:e85587.
41. Mett V, Komarova EA, Greene K, Bespalov I, Brackett C, Gillard B, et al.Mobilan: a recombinant adenovirus carrying Toll-like receptor 5 self-activating cassette for cancer immunotherapy. Oncogene 2018;37:439–49.
42. Bakhribah H, Dy GK, Ma WW, Zhao Y, Opyrchal M, Purmal A, et al. Aphase I study of the toll-like receptor 5 (TLR5) agonist, entolimod inpatients (pts) with advanced cancers. J Clin Oncol 2015;33:3063.
43. Vidal D, Matias-Guiu X, Alomar A. Open study of the efficacy andmechanism of action of topical imiquimod in basal cell carcinoma.Clin Exp Dermatol 2004;29:518–25.
44. Grimm C, Polterauer S, Natter C, Rahhal J, Hefler L, Tempfer CB, et al.Treatment of cervical intraepithelial neoplasia with topical imiquimod.Obstet Gynecol 2012;120:152–9.
45. Sabado RL, Pavlick A, Gnjatic S, Cruz CM, Vengco I, Hasan F, et al.Resiquimod as an immunologic adjuvant for NY-ESO-1 protein vacci-nation in patients with high-risk melanoma. Cancer Immunol Res 2015;3:278–87.
46. Ota Y, Otsubo T, Koroki J, Hirose Y, Koga-Yamakawa E, Murata M, et al.Novel intravenous injectable TLR7 agonist, DSP-0509, synergisticallyenhanced antitumor immune responses in combination with anti-PD-1antibody [abstract]. In: Proceedings of the AACR Annual Meeting; 2018Apr 14–18; Chicago, IL. Philadelphia (PA): AACR; 2018. Abstract nr.4726.
47. Gupta S, Grilley-Olson J, Hong D, Marabelle A, Munster P, Aggarwal R,et al. Safety and pharmacodynamic activity of MEDI9197, a TLR 7/8agonist, administered intratumorally in subjects with solid tumors[abstract]. In: Proceedings of the AACR Annual Meeting; 2017 Apr 1–5; Washington, DC. Philadelphia (PA): AACR; 2017. Abstract nr. CT091.
48. Lee M. NKTR-262: prodrug pharmacokinetics in mice, rats, and dogs[abstract]. In: Proceedings of the AACR Annual Meeting; 2018 Apr 14–18;Chicago, IL. Philadelphia (PA): AACR; 2018. Abstract nr. 2755.
49. Kivim€ae S, Rubas W, Pena R, Mclaughlin J, Hennessy M, Kirksey Y, et al.Harnessing the innate and adaptive immune system to eradicate treatedand distant untreated solid tumors. J Immunother Cancer 2017;5:P275.
50. Ferris RL, Saba NF, Gitlitz BJ, Haddad R, Sukari A, Neupane P, et al. Effectof addingmotolimod to standard combination chemotherapy and cetux-imab treatment of patients with squamous cell carcinomaof the head andneck. JAMA Oncol 2018;4:1583–8.
51. Kapp K, Schneider J, Schneider L, Gollinge N, J€ansch S, Schroff M, et al.Distinct immunological activation profiles of dSLIM� and ProMune�
dependon their different structural context. Immunity InflammDis 2016;4:446–62.
52. Samulowitz U,WeberM,Weeratna R, Uhlmann E, Noll B, Krieg AM, et al.A novel class of immune-stimulatory CpG oligodeoxynucleotides unifieshigh potency in type I interferon induction with preferred structuralproperties. Oligonucleotides 2010;20:93–101.
53. Brody JD, Ai WZ, Czerwinski DK, Torchia JA, Levy M, Advani RH, et al.In situ vaccination with a TLR9 agonist induces systemic lymphomaregression: a phase I/II study. J Clin Oncol 2010;28:4324–32.
54. Manegold C, van Zandwijk N, Szczesna A, Zatloukal P, Au JSK, Blasinska-Morawiec M, et al. A phase III randomized study of gemcitabine andcisplatin with or without PF-3512676 (TLR9 agonist) as first-line treat-ment of advanced non-small-cell lung cancer. Ann Oncol 2012;23:72–7.
55. Frank MJ, Reagan PM, Bartlett NL, Gordon LI, Friedberg JW, CzerwinskiDK, et al. In situ vaccination with a TLR9 agonist and local low-doseradiation induces systemic responses in untreated indolent lymphoma.Cancer Discov 2018;8:1258–69.
56. MilhemM, Gonzales R, Medina T, Kirkwood JM, Buchbinder E, Mehmi I,et al. Intratumoral toll-like receptor 9 (TLR9) agonist, CMP-001, incombination with pembrolizumab can reverse resistance to PD-1 inhi-bition in a phase Ib trial in subjects with advanced melanoma [abstract].In: Proceedings of the AACR Annual Meeting; 2018 Apr 14–18; Chicago,IL. Philadelphia (PA): AACR; 2018. Abstract nr. CT144.
57. Diab A, Rahimian S, Haymaker CL, Bernatchez C, Andtbacka RHI, JamesM, et al. A phase 2 study to evaluate the safety and efficacy of Intratumoral(IT) injection of the TLR9 agonist IMO-2125 (IMO) in combination with
Aleynick et al.
Clin Cancer Res; 2019 Clinical Cancer ResearchOF10
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

ipilimumab (ipi) in PD-1 inhibitor refractory melanoma. J Clin Oncol36,2018 (suppl; abstr 9515). Available from: https://meetinglibrary.asco.org/record/159086/abstract.
58. Thomas M, Ponce-Aix S, Navarro A, Riera-Knorrenschild J, Schmidt M,Wiegert E, et al. Immunotherapeutic maintenance treatment withtoll-like receptor 9 agonist lefitolimod in patients with extensive-stage small-cell lung cancer: results from the exploratory, controlled,randomized, international phase II IMPULSE study. Ann Oncol 2018;29:2076–84.
59. Krarup AR, Abdel-Mohsen M, Schleimann MH, Vibholm L, Engen PA,Dige A, et al. The TLR9 agonist MGN1703 triggers a potent type Iinterferon response in the sigmoid colon. Mucosal Immunol 2018;11:449–61.
60. Ribas A,Medina T, Kummar S, Amin A, Kalbasi A, Drabick JJ, et al. SD-101in combinationwith pembrolizumab in advancedmelanoma: results of aphase 1b, multicenter study. Cancer Discov 2018;8:1250–7.
61. Sagiv-Barfi I, Czerwinski DK, Levy S, Alam IS,Mayer AT, Gambhir SS, et al.Eradication of spontaneous malignancy by local immunotherapy.Sci Transl Med 2018;10:eaan4488.
62. Levy R, Reagan PM, Friedberg JW, Bartlett NL, Gordon LI, Leung A, et al.SD-101, a novel class C CpG-oligodeoxynucleotide (ODN) toll-likereceptor 9 (TLR9) agonist, given with low dose radiation for untreatedlow grade B-cell lymphoma: interim results of a phase 1/2 trial. Blood2016;128:2974.
63. Saxena M, Yeretssian G. NOD-like receptors: master regulators of inflam-mation and cancer. Front Immunol 2014;5:327.
64. Dostert C, Petrilli V, Van Bruggen R, Steele C, Mossman BT, Tschopp J.Innate immune activation through Nalp3 inflammasome sensing ofasbestos and silica. Science 2008;320:674–7.
65. Chou AJ, Kleinerman ES, KrailoMD, Chen Z, Betcher DL, Healey JH, et al.Addition of muramyl tripeptide to chemotherapy for patients withnewly diagnosed metastatic osteosarcoma: a report from the Children'sOncology Group. Cancer 2009;115:5339–48.
66. Dietsch GN, Lu H, Yang Y, Morishima C, Chow LQ, Disis ML, et al.Coordinated activation of toll-like receptor8 (TLR8) and NLRP3 by theTLR8 agonist, VTX-2337, ignites tumoricidal natural killer cell activity.PLoS One 2016;11:e0148764.
67. Li H, Willingham SB, Ting JP-Y, Re F. Cutting edge: inflammasomeactivation by alum and alum's adjuvant effect are mediated by NLRP3.J Immunol 2008;181:17–21.
68. Cibulski SP, Rivera-Patron M, Mourglia-Ettlin G, Casaravilla C, YendoACA, Fett-Neto AG, et al. Quillaja brasiliensis saponin-based nanoparti-culate adjuvants are capable of triggering early immune responses. Sci Rep2018;8:13582.
69. Geijtenbeek TBH, Gringhuis SI. Signalling through C-type lectin recep-tors: shaping immune responses. Nat Rev Immunol 2009;9:465–79.
70. Yamasaki S, Ishikawa E, SakumaM,Hara H, Ogata K, Saito T. Mincle is anITAM-coupled activating receptor that senses damaged cells.Nat Immunol 2008;9:1179–88.
71. Zhang JG,Czabotar PE, Policheni AN,Caminschi I, SanWanS, Kitsoulis S,et al. The dendritic cell receptor Clec9A binds damaged cells via exposedactin filaments. Immunity 2012;36:646–57.
72. Vassilaros S, Tsibanis A, Tsikkinis A, Pietersz GA, McKenzie IFC,Apostolopoulos V. Up to 15-year clinical follow-up of a pilot Phase IIIimmunotherapy study in stage II breast cancer patients using oxidizedmannan-MUC1. Immunotherapy 2013;5:1177–82.
73. Morse MA, Chapman R, Powderly J, Blackwell K, Keler T, Green J, et al.Phase I study utilizing a novel antigen-presenting cell-targeted vaccinewith toll-like receptor stimulation to induce immunity to self-antigens incancer patients. Clin Cancer Res 2011;17:4844–53.
74. Dhodapkar MV, Sznol M, Zhao B, Wang D, Carvajal RD, Keohan ML,et al. Induction of antigen-specific immunity with a vaccine targetingNY-ESO-1 to the dendritic cell receptor DEC-205. Sci Transl Med 2014;6:232ra51.
75. Pollack SM. The potential of the CMB305 vaccine regimen to target NY-ESO-1 and improve outcomes for synovial sarcoma and myxoid/roundcell liposarcoma patients. Expert Rev Vaccines 2018;17:107–14.
76. Thomas M, Sadjadian P, Kollmeier J, Lowe J, Mattson P, Trout JR, et al.A randomized, open-label, multicenter, phase II study evaluating theefficacy and safety of BTH1677 (1,3-1,6 beta glucan; Imprime PGG) incombination with cetuximab and chemotherapy in patients with
advanced non-small cell lung cancer. Invest New Drugs 2017;35:345–58.
77. Loo YM, Gale M. Immune signaling by RIG-I-like receptors. Immunity2011;34:680–92.
78. K€ubler K, Gehrke N, Riemann S, B€ohnert V, Zillinger T, Hartmann E, et al.Targeted activation of RNA helicase retinoic acid - Inducible gene-Iinduces proimmunogenic apoptosis of human ovarian cancer cells.Cancer Res 2010;70:5293–304.
79. Besch R, Poeck H, Hohenauer T, Senft D, H€acker G, Berking C, et al.Proapoptotic signaling induced by RIG-I and MDA-5 results in type Iinterferon–independent apoptosis in human melanoma cells. J ClinInvest 2009;119:2399–411.
80. Calles A, Rodriguez-Ruiz M, Soria A, Marquez Rodas I, Ponz-Sarvis�e M,Martín M, et al. Intratumoral BO-112, a double-stranded RNA (dsRNA),alone and in combination with systemic anti-PD-1 in solid tumors.Ann Oncol 2018;29:732.
81. Barsoum J, Renn M, Schuberth C, Jakobs C, Schwickart A, Schlee M, et al.Abstract B44: Selective stimulation of RIG-I with a novel synthetic RNAinduces strong anti-tumor immunity in mouse tumor models [abstract].In: Proceedings of the AACR Special Conference on Tumor Immunologyand Immunotherapy; 2016 Oct 20–23; Boston, MA. Philadelphia (PA):AACR; Cancer Immunol Res 2017. Abstract nr B44.
82. Middleton MR, Wermke M, Calvo E, Chartash E, Zhou H, Zhao X, et al.Phase I/II, multicenter, open-label study of intratumoral/intralesionaladministration of the retinoic acid–inducible gene I (RIG-I) activatorMK-4621 inpatientswith advancedor recurrent tumors. AnnOncol 2018;29:mdy424–016.
83. Ishikawa H, Ma Z, Barber GN. STING regulates intracellular DNA-mediated, type I interferon-dependent innate immunity. Nature 2009;461:788–92.
84. Chen Q, Sun L, Chen ZJ. Regulation and function of the cGAS–STINGpathway of cytosolic DNA sensing. Nat Immunol 2016;17:1142–9.
85. H€artlova A, Erttmann SF, Raffi FA, Schmalz AM, Resch U, Anugula S, et al.DNA damage primes the type I interferon system via the cytosolic DNAsensor STING to promote anti-microbial innate immunity. Immunity2015;42:332–43.
86. Deng L, Liang H, Xu M, Yang X, Burnette B, Arina A, et al. STING-dependent cytosolic DNA sensing promotes radiation-induced type Iinterferon-dependent antitumor immunity in immunogenic tumors.Immunity 2014;41:843–52.
87. Wang H, Hu S, Chen X, Shi H, Chen C, Sun L, et al. cGAS is essential forthe antitumor effect of immune checkpoint blockade. Proc Natl Acad SciU S A 2017;114:1637–42.
88. Lara PN Jr, Douillard J-Y, Nakagawa K, von Pawel J, McKeage MJ, Albert I,et al. Randomized phase III placebo-controlled trial of carboplatin andpaclitaxel with or without the vascular disrupting agent vadimezan(ASA404) in advanced non-small-cell lung cancer. J Clin Oncol 2011;29:2965–71.
89. Corrales L, Glickman LH, McWhirter SM, Kanne DB, Sivick KE, KatibahGE, et al.Direct activation of STING in the tumormicroenvironment leadstopotent and systemic tumor regression and immunity. Cell Rep2015;11:1018–30.
90. Harrington KJ, Brody J, InghamM, Strauss J, Cemerski S, Wang M, et al.Preliminary results of the first-in-human (FIH) study of MK-1454,an agonist of stimulator of interferon genes (STING), as monotherapyor in combination with pembrolizumab (pembro) in patientswith advanced solid tumors or lymphomas. Ann Oncol 2018;29:mdy424.015.
91. Liu X, Pu Y, Cron K, Deng L, Kline J, Frazier WA, et al. CD47 blockadetriggers T cell-mediated destruction of immunogenic tumors. Nat Med2015;21:1209–15.
92. Pikor LA, Bell JC, Diallo J-S. Oncolytic viruses: exploiting cancer's dealwith the devil. Trends Cancer 2015;1:266–77.
93. Brown MC, Holl EK, Boczkowski D, Dobrikova E, Mosaheb M,Chandramohan V, et al. Cancer immunotherapy with recombinantpoliovirus induces IFN-dominant activation of dendritic cells and tumorantigen-specific CTLs. Sci Transl Med 2017;9:eaan4220.
94. Zamarin D, Holmgaard RB, Subudhi SK, Park JS, Mansour M, Palese P,et al. Localized oncolytic virotherapy overcomes systemic tumor resis-tance to immune checkpoint blockade immunotherapy. Sci Transl Med2014;6:226ra32.
Pattern Recognition Receptors in Immuno-oncology
www.aacrjournals.org Clin Cancer Res; 2019 OF11
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

95. Andtbacka RHI, Ross M, Puzanov I, Milhem M, Collichio F, Delman KA,et al. Patterns of Clinical Response with Talimogene Laherparepvec(T-VEC) in Patients with Melanoma Treated in the OPTiM Phase IIIClinical Trial. Ann Surg Oncol 2016;23:4169–77.
96. Chesney J, Puzanov I, Collichio F, Singh P, Milhem MM, Glaspy J, et al.Randomized, open-label phase II study evaluating the efficacy and safetyof talimogene laherparepvec in combination with ipilimumab versusipilimumab alone in patients with advanced, unresectable melanoma.J Clin Oncol 2018;36:1658–67.
97. Eriksson E,Milenova I,Wenthe J, HleMS, Leja-Jarblad J, Ullenhag G, et al.Shaping the tumor stroma and sparking immune activation by CD40 and4-1BB signaling induced by an armed oncolytic virus. Clin Cancer Res2017;23:5846–57.
98. Desjardins A, Gromeier M, Herndon JE, Beaubier N, Bolognesi DP,Friedman AH, et al. Recurrent glioblastoma treated with recombinantpoliovirus. N Engl J Med 2018;379:150–61.
99. Fu J, KanneDB, LeongM, Glickman LH,McWhirter SM, Lemmens E, et al.STING agonist formulated cancer vaccines can cure established tumorsresistant to PD-1 blockade. Sci Transl Med 2015;7:283ra52.
100. Li J, Song W, Czerwinski DK, Varghese B, Uematsu S, Akira S, et al.Lymphoma immunotherapy with CpG oligodeoxynucleotides requiresTLR9 either in the host or in the tumor itself. J Immunol 2007;179:2493–500.
101. Cheadle EJ, Lipowska-Bhalla G, Dovedi SJ, Fagnano E, Klein C, Honey-church J, et al. A TLR7 agonist enhances the antitumor efficacy ofobinutuzumab in murine lymphoma models via NK cells and CD4 Tcells. Leukemia 2017;31:1611–21.
102. Hamilton JR, Vijayakumar G, Palese P. A recombinant antibody-expressing influenza virus delays tumor growth in a mouse model.Cell Rep 2018;22:1–7.
103. SchmidD, ParkCG,Hartl CA, SubediN, Cartwright AN, Puerto RB, et al. Tcell-targeting nanoparticles focus delivery of immunotherapy to improveantitumor immunity. Nat Commun 2017;8:1747.
104. de Wit R, Kulkarni GS, Uchio E, Singer EA, Krieger L, Grivas P, et al. 864OPembrolizumab for high-risk (HR) non–muscle invasive bladder cancer(NMIBC) unresponsive to bacillus Calmette-Gu�erin (BCG): phase IIKEYNOTE-057 trial. Ann Oncol 2018;29:mdy283.073.
105. Dillon PM, Petroni GR, Smolkin ME, Brenin DR, Chianese-Bullock KA,Smith KT, et al. A pilot study of the immunogenicity of a 9-peptide breastcancer vaccine plus poly-ICLC in early stage breast cancer. J ImmunotherCancer 2017;5:92.
106. Chawla S, Van Tine BA, Pollack S, Ganjoo K, Elias A, Riedel RF, et al. Aphase 2 study of CMB305 and atezolizumab in NY-ESO-1þ soft tissuesarcoma: Interim analysis of immunogenicity, tumor control and surviv-al. Ann Oncol 2017;28:mdx387.007.
107. Andtbacka RH, Curti BD, Hallmeyer S, Feng Z, Paustian C, Bifulco C,et al. Phase II calm extension study: Coxsackievirus A21 deliveredintratumorally to patients with advanced melanoma induces immune-cell infiltration in the tumor microenvironment. J Immunother Cancer2015;3:P343.
108. Bernstein V, Ellard SL, Dent SF, Tu D, Mates M, Dhesy-Thind SK, et al. Arandomized phase II study of weekly paclitaxel with or without pelar-eorep in patients with metastatic breast cancer: final analysis of CanadianCancer Trials Group IND.213. Breast Cancer Res Treat 2018;167:485–93.
Clin Cancer Res; 2019 Clinical Cancer ResearchOF12
Aleynick et al.
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800

Published OnlineFirst May 23, 2019.Clin Cancer Res Mark Aleynick, Judit Svensson-Arvelund, Christopher R. Flowers, et al. Cancer by Mimicking InfectionPathogen Molecular Pattern Receptor Agonists: Treating
Updated version
10.1158/1078-0432.CCR-18-1800doi:
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/early/2019/07/16/1078-0432.CCR-18-1800To request permission to re-use all or part of this article, use this link
Research. on March 4, 2021. © 2019 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 23, 2019; DOI: 10.1158/1078-0432.CCR-18-1800