Embed Size (px)
Citation preview
5/22/2017
1
Part IIQuality improvement in long-term care: Partnership of infection prevention and
environmental services
Using the Centers for Medicare and Medicaid Services (CMS) Quality Assurance Performance Improvement
(QAPI) Performance Improvement Project (PIP)
Deb Patterson Burdsall PhD, RN-BC, CIC, FAPIC

5/22/2017
2
DisclosuresThe following speaker discloses no actual or potential conflicts of interest in relation to this program/presentation:
• Deb Patterson Burdsall PhD, RN-BC, CIC, FAPIC
The following planning staff report no actual or potential conflicts of interest in relation to this program/presentation:
• Carol McLay, DrPH, MPH, RN, CIC
• Charu Malik
• Colin Richardson
• Kristen Henry
Learning Objectives
• Understand how answers to questions from Part I relate to the current environmental cleaning and disinfecting processes
• Learn about the collaborative approach between infection prevention and environmental services for quality improvement
• Understand how the CMS Quality Assurance Performance Improvement (QAPI) toolkit can help
• Learn how to implement the QAPI-PIP model

5/22/2017
3
Conclusions from Part I
• Environmental cleaning and disinfecting require explicit knowledge and training and dedicated staff
• The facility Infection Preventionist (IP) has responsibility for the EVS program as it relates to infection prevention and control
• There are manufacturers, distributors and service companies with healthcare EVS expertise
Break the Chain of Infection
6
Image: Pickit Free Images

5/22/2017
4
Question: Who Is Listening Today?
1. Front-line staff (nurses, CNAs, housekeeping/environmental services (EVS) staff)
2. Directors and Assistant Directors of Nursing who are also Infection Preventionists
3. Infection Preventionists with no other job responsibilities
4. EVS Directors, Managers, Supervisors
5. Administrators, VPs of services
6. Owners, board members, CEOs, CFOs
Addressing questions from Webinar Part I
• APIC Certificate of Training in Infection Prevention in the Long-Term Care Setting?
• Bleach solutions?
• Johnny mops?
• Effective and low toxicity cleaning and disinfecting?

5/22/2017
5
APIC Certificate of Training in Infection Prevention in the Long-Term Care Setting
• This course teaches the basics of infection prevention in the long-term care setting, including:– Infection Prevention and Control (IPCP) program and risk assessment development– Facility-wide assessment and Quality Assurance and Performance Improvement
(QAPI) program as it relates to the IPCP– QAPI infection prevention Performance Improvement Projects (PIP)– Antibiotic stewardship– LTC infection surveillance, using and reporting data– Multi drug-resistant and extensively drug-resistant organisms (MDRO and XDRO)– National Healthcare Safety Network (NHSN) reporting– Standard and transmission-based precautions
• An online version of this class is scheduled to be available during the last quarter of 2017. APIC will provide both face to face or online options for completing the course before November 28, 2019
Mixing Bleach Solutions and Human Factors
• Mixing bleach is difficult
• Lots of room for human error
• 5.25% to 6.0% bleach considered hazardous: 2012 OSHA Hazard Communication Standard
• Category 1 health hazard and corrosive
• Requires ventilation, gowns/aprons, gloves, and eye protection
Science Photo
5/22/2017
6
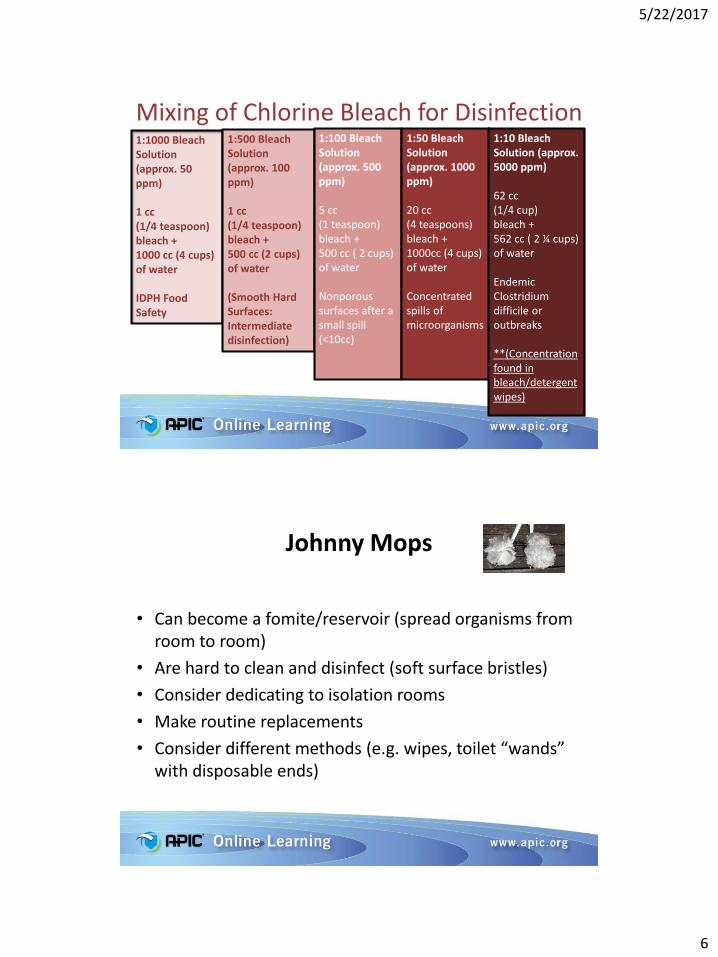
Mixing of Chlorine Bleach for Disinfection1:1000 Bleach Solution (approx. 50 ppm)
1 cc (1/4 teaspoon) bleach +1000 cc (4 cups) of water
IDPH Food Safety
1:500 Bleach Solution (approx. 100 ppm)
1 cc (1/4 teaspoon) bleach +500 cc (2 cups) of water
(Smooth Hard Surfaces: Intermediate disinfection)
1:100 Bleach Solution (approx. 500 ppm)
5 cc (1 teaspoon)bleach +500 cc ( 2 cups) of water
Nonporous surfaces after a small spill (<10cc)
1:50 Bleach Solution (approx. 1000 ppm)
20 cc (4 teaspoons)bleach +1000cc (4 cups) of water
Concentrated spills of microorganisms
1:10 Bleach Solution (approx. 5000 ppm)
62 cc(1/4 cup)bleach +562 cc ( 2 ¼ cups) of water
Endemic Clostridium difficile or outbreaks
**(Concentration found in bleach/detergent wipes)
Johnny Mops
• Can become a fomite/reservoir (spread organisms from room to room)
• Are hard to clean and disinfect (soft surface bristles)
• Consider dedicating to isolation rooms
• Make routine replacements
• Consider different methods (e.g. wipes, toilet “wands” with disposable ends)

5/22/2017
7
Cleaning and Disinfecting Products
• “Do you have examples of products with low toxicity but still effective to kill broad range of microbes with low contact time?”
• Advanced hydrogen peroxide products
• Peracetic acid products
• Citric acid with silver ion products
• Newer bleach formulations
• Ultraviolet
CDC: EVS Recommendations
• Joint infection prevention / EVS team effort
• Base on Facility Assessment
• Responsibilities for cleaning high touch surfaces (e.g., nursing, activities, culinary surfaces) must be clearly defined
• Training and competency must be maintained
• Quality assessment and assurance (QAA) / quality assurance and performance improvement (QAPI) processes should be ongoing
Guh & Carling, 2010 https://www.cdc.gov/hai/toolkits/evaluating-environmental-cleaning.htmlLink accessed 5/22/17

5/22/2017
8
Source: https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilitiesLink accessed 5/22/17
Centers for Medicare and Medicaid Services (CMS)
“Mega Rule” Reform of Requirements
• Phase I November 28, 2016
– Basic Infection Prevention and Control Program (IPCP)
• Phase II November 28, 2017
– IPCP linked to Facility Assessment
– Antibiotic Stewardship Program
• Phase III November 28, 2019
– Trained Infection Preventionist (IP)
– IP participation in Quality Assurance
5/22/2017
9
Facility-wide Assessment by November 28, 2017
• Determine necessary resources to competently care for residents
• All hazards approach
• Review
– As necessary
– At least annually
– At any significant change
17
Source: Federal Register Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Final Rule: 10/4/16. https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilitiesLink accessed 5/22/17Image: Pixabay_P. Marco
Residents
• The facility’s resident population
• The care required for resident population:
– Types of diseases, conditions, physical and cognitive disabilities
– Overall acuity
– Other pertinent facts that arepresent within that population
• Ethnic, cultural or religious factors
18
Pixabay
Pixabay

5/22/2017
10
Personnel
• Staff competencies for level and types of care needed
• Ethnic, cultural, or religious factors
• All personnel, including managers, facility staff, volunteers, and contract employees
19
Infection Prevention Training and Competency
• Goal: staff comply with infection control practices
• Initial and ongoing infection control education
– when policies and procedures are revised
– when there is a special circumstance (e.g. outbreak)
– When there is required modification or replacement of current practices
20
SciencePhoto
Link Accessed 5/22/17
5/22/2017
11
Training and Competency
• Specific infection control training with follow-up competency evaluations
• Monitoring
• Environmental cleaning and disinfecting ARE infection prevention and control activities
21
Stock Unlimited
Link Accessed 5/22/17
CMS and CDC focus on nursing homes
• Residents frequently colonized with multi drug-resistant organisms (MDRO) (e.g. MRSA, Clostridium difficile, VRE, CRE, KPC)
• 30%-50% of frail, elderly long-term care residents with asymptomatic bacteriuria
• Skilled nursing = reservoir for MDRO
• Poor inter-facility and intra-facility communication• Infection related hospitalizations and deaths among
nursing home residents and patientsSource: CDC: https://www.cdc.gov/getsmart/healthcare/learn-from-others/factsheets/nursing-homes.html#needLink accessed 5/22/17
Pixabay

5/22/2017
12
QAPI Element 1: Design and Scope
• Maintain ongoing and comprehensive written plans (evidence-based goals)
• Include full range of services
• Address all systems of care and management practices
• Emphasize safety and high quality care
• Emphasize autonomy and choice
https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/downloads/qapifiveelements.pdfSource:

5/22/2017
13
QAPI Element 2: Governance and Leadership
• Foster culture where QAPI is a priority
• Seek input from entire Interdisciplinary Team (IDT)
• Assure adequate resources for QAPI safety, quality, rights, choice and respect
• Balance resident rights and safety
• Make person(s) accountable for QAPI: Leadership and facility-wide training
Source: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/downloads/qapifiveelements.pdf
QAPI Element 3:Feedback, Data Systems & Monitoring
• Monitor care and services
• Actively incorporate input from IDT
• Monitor processes and outcomes
• Review findings against benchmarks
• Track, investigate and monitor adverse events
• Develop action plans to prevent recurrences
https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/downloads/qapifiveelements.pdfSource:

5/22/2017
14
QAPI Element 4: Performance Improvement Projects
(PIPs)
• Concentrate efforts on particular problem(s)
• Gather information systematically
• Clarify issues or problems
• Intervene to improve
https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/downloads/qapifiveelements.pdfSource:
QAPI Element 5:Systematic Analysis & Systemic Action
• Analyze and understand the problem, causes and implications of change
• Identify how problems are occurring with consistent processes (e.g. root cause analysis)
• Take systemic actions look across all involved systems
• Develop policies and procedures and demonstrate proficiency
• Promote sustained improvement to prevent future events
https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/downloads/qapifiveelements.pdfSource:

5/22/2017
15
Quality Assessment and Assurance (QAA)
• November 28, 2016
• Management process
• Ongoing, multi-level
• All managerial, administrative, clinical and environmental services
• Performance of outside (contracted or arranged) providers and suppliers of care and services
• Purpose is continuous evaluation of facility systems
Source: CMS Mega Rule State Operations Manual 3/6/2017
Quality Assessment and Assurance (QAA)
• Continuous evaluation of facility systems
• Keep systems functioning consistently
• Maintain current practice standards
• Prevent deviation from care processes
• Identify and correct issues and concerns (“inappropriate care processes”) 5.17
Source: CMS Mega Rule State Operations Manual 3/6/2017

5/22/2017
16
Question (yes/no)
1. I am included in the product-selection process
2. I am involved with training staff to use a new product
3. The IP is required to assist with EVS monitoring
4. The IP is required to be a part of the QAPI process
5. I know what a GPO is (before this webinar!)
Performance Improvement Project (PIP)
• Concentrate on a particular problem in one area of the facility or facility wide
• Gather information systematically
• Use team approach to identify the cause of a problem
• Fix problems that are important and meaningful for the specific type and scope of services
Source: Appendix B QAPI Definitions: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/Downloads/QAPIAtaGlance.pdfLink accessed 5/22/17

5/22/2017
17
Sample Case Study
Why is a QAPI PIP needed?
• Your facility assessment reveals that increasing numbers of patients and residents are colonized with multi drug-resistant organisms (MDRO) such as carbapenem-resistant Enterobacteriaceae (CRE)
• IP does not work with EVS to select cleaning/disinfecting products
• Product selection is a corporate decision
• Cleaning and disinfecting is not routinely monitored
5/22/2017
18
The Business Case
• Combine what you have to do with what you need to do!
• Group Purchasing Organizations (GPO)
• Interdisciplinary Purchasing Committees
• QAPI Performance Improvement Project (PIP)
• PIP Team = Interdisciplinary Purchasing Committees
PIP Team
• Form PIP team for product selection and system change
• PIP team consists of those who use, purchase and pay for the cleaning disinfecting chemicals
• Front-line personnel
• Managers and supervisors
• Materials Management and Purchasing
• CEO, CFO, Owners may need to be part of the team

5/22/2017
19
Root Cause Analysis
• Chemicals are purchased based on cost rather than on efficacy/effectiveness and ease of use
• No consistent process to ensure cleaning and disinfecting chemicals are at point of care
• No competency-based training
• No routine monitoring of cleaning/disinfecting
• Punitive approach
• Emphasis is working quickly
Root Cause Analysis continued
• No permanent EVS supervisors
• The last supervisor left 6 months ago
• The corporate supervisor rounds once a month
• Supply company for cleaning and disinfecting chemicals specializes in janitorial and food service
• No healthcare expertise or support
• The disinfectants (when available) require a 10 minute wet contact time
• The EVS housekeepers speak very little English. The corporate supervisor does not speak Spanish, Polish or Vietnamese
5/22/2017
20
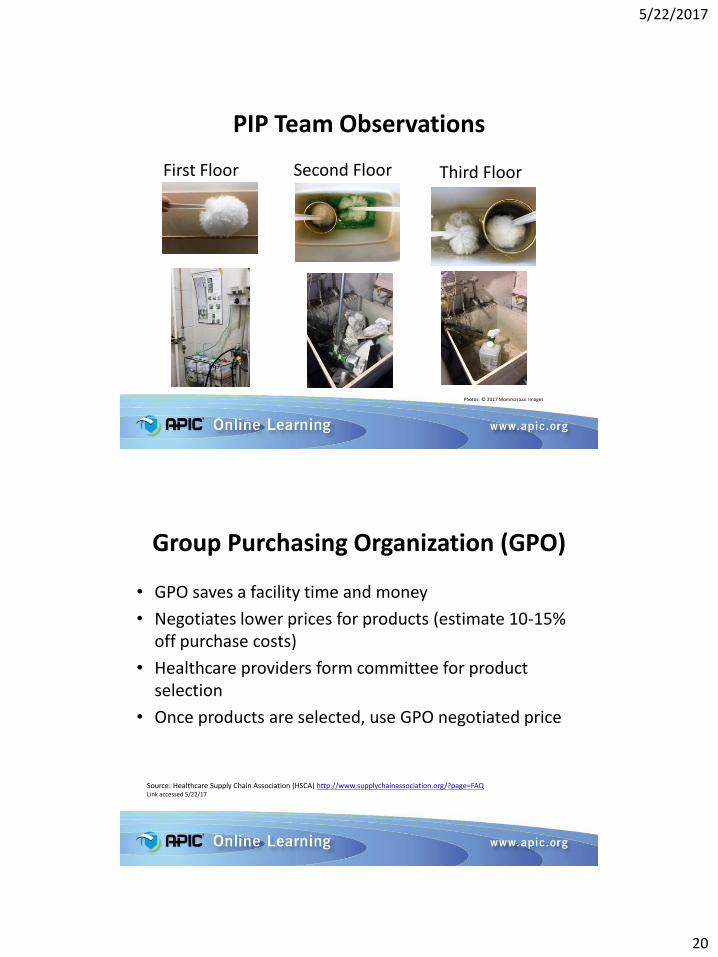
First Floor Second Floor Third Floor
PIP Team Observations
Photos: © 2017 Mommarazzi Images
Group Purchasing Organization (GPO)
• GPO saves a facility time and money
• Negotiates lower prices for products (estimate 10-15% off purchase costs)
• Healthcare providers form committee for product selection
• Once products are selected, use GPO negotiated price
Source: Healthcare Supply Chain Association (HSCA) http://www.supplychainassociation.org/?page=FAQLink accessed 5/22/17

5/22/2017
21
Cleaning and Disinfecting Products
• Select products with the assistance of the PIP Team, GPO representation and company with healthcare expertise
• Shortest contact time to kill the most organisms with lowest human toxicity– Advanced hydrogen peroxide products
– Peracetic acid products
– Citric acid with silver ion products
– Newer bleach formulations
• Healthcare EVS companies can provide support and training as part of the contract
Pilot
• Pilot the environmental services program on selected unit(s) or facilities
• PIP team collect data on environmental cleaning, and staff and patient/resident response
• Potentially compare other infection prevention indicators (e.g. readmission rates, infection rates)
• Modify and expand
• Document and take credit for a QAPI PIP!!






























