Embed Size (px)
Citation preview
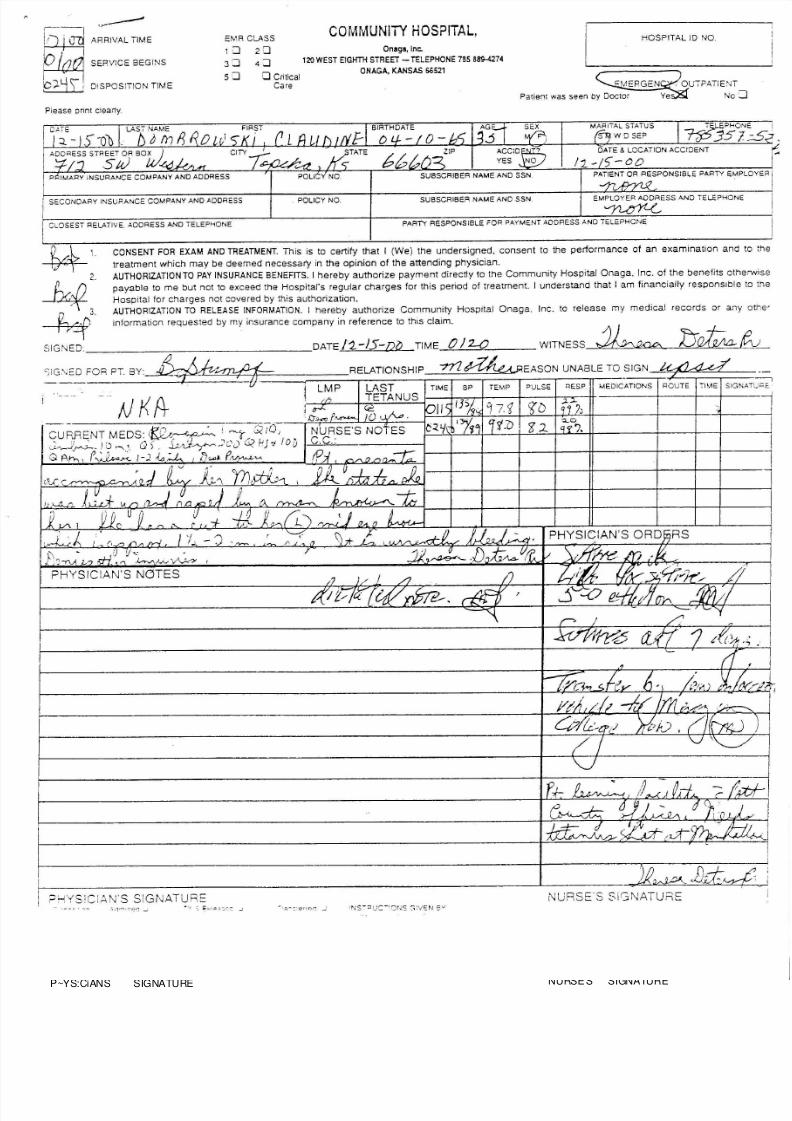
8/8/2019 Part 2 Rape 2001 Med Records_1
http://slidepdf.com/reader/full/part-2-rape-2001-med-records1 1/2
ARRIVAL TIME
SERVICE BEGINS
DISPOSITION TIME
EMR CLASS
1 : :J 2 : :J3 : :J 4 : :J5 ::J ::JCritical
Care
C O M M U N IT Y H O S P IT A L,
Onaga, Inc .
1 2 0 W E S T E I G H TH S T R EE T - T E LE P H ON E 7 8 5 8 8S - 42 7 4
O N A G A, K A N SA S 5 6 52 1
HOSPITAL 10 NO.
, OUTPATIENT
No:J
Please pnnt clearly.
I SECONDARY INSUf'ANCE COMPANY AND ADDRESS POLICY NO. SUBSCR~ERNAMEANDSSN
- r i ' ?3501~I •
DATE & LOCATION ACCIDENT ~
/1- )-00 I
PATIENT OR RESPONSIBLE PARTY EMPLOYER I
EMPLOYER ADDRESS AND TELEPHONE I
~ I
CLOSEST RELATIVE. ADDRESS AND TELEPHONE PARTY RESPONSIBLE FOR PAYMENT ADDRESS AND TELEPHONE
---,SIGNATlJPE,IMEROUTE
Q . . , . . l 1 . C ON S EN T F OR E XA M A N D T R EA T ME N T. This is to certify that I (We) the undersigned, consent to the performance of an examination and to the
---fff- treatment which may be deemed necessary in the opinion of the attending physician.
2 A U TH O R IZ A TI ON T O P A Y I NS U RA N C E B EN E F IT S . I hereby authorize payment directly to the Community Hospital Onaga, Inc. of the benefits otherwise
h/. (). payable to me but not to exceed the Hospital's regular charges for this period of treatment. I understand that I am financially responsible to the
--- 'A T Hospital for charges not covered by this authorization.
C , /".J.) 3 . A U TH O R IZ A TI ON T O R E L EA S E I N F OR M A TIO N . I hereby authorize Community Hospital Onaga, Inc. to release my medical records or any othe'
~ i nformatio n req ue sted b y my in suran ce co mp any i n referen ce to this c la im.
SIGNED.. DATE11.-15-D~ TIME OJ 1-0 WITNESS k A 1 0 . J:J~ tvC;!G'-;E_DFOR PT. BY~~~~----<.-.-------RELATIONSHIP -n1~EASON UNABLE TO SIGN
LM P TIME BP TEMP PULSE RESP MEDICATIONS
P~YS:CiANS SIGNATURE
~~1Jd:~ NURSE'S SIGNATURE
8/8/2019 Part 2 Rape 2001 Med Records_1
http://slidepdf.com/reader/full/part-2-rape-2001-med-records1 2/2
I Date Patient Na ! I ' r . . .cal Record Nwnber
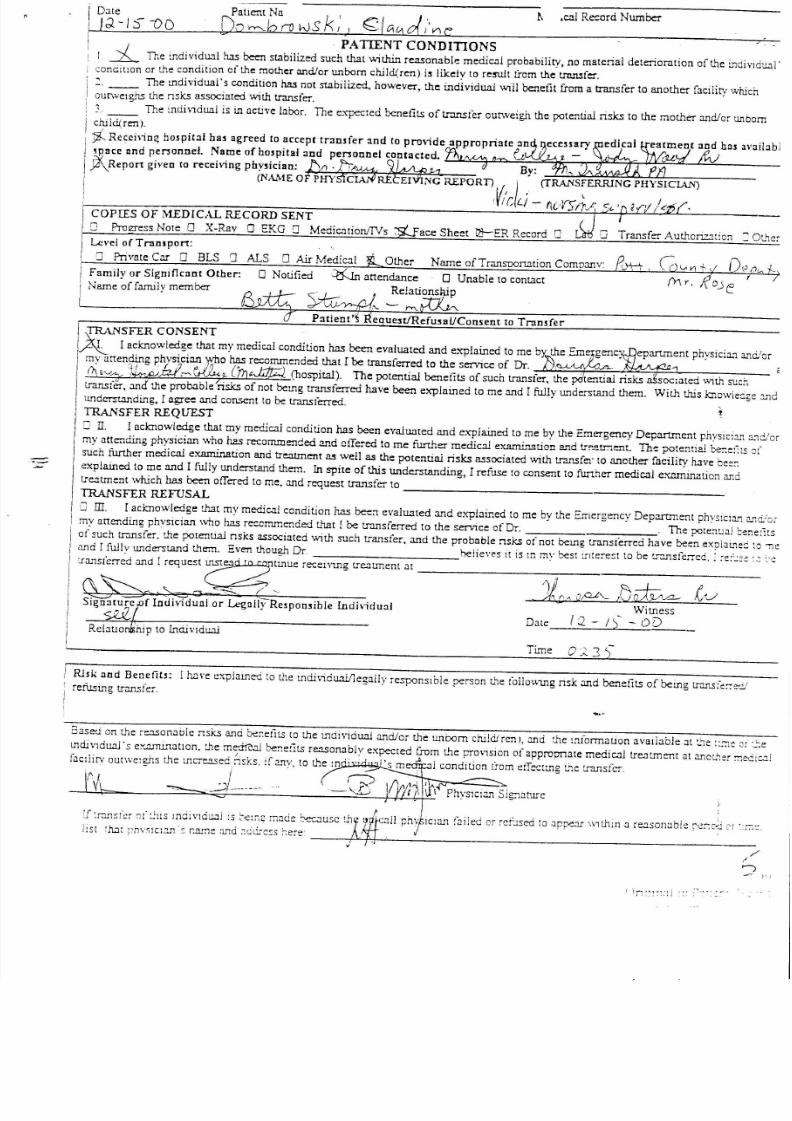
I };)-15""OO Do~bnJvJskl) E ; ! C i & 1 O f , 'n c ., PATIENT CONDITIONS ..
I ~ The individU.'l1!us been stabilized such that \.\Iithinreasonable medical probability, no material deteriorntion of L1elJldiYlCU.'ll'concitlOn or the condition of the mother llIld/or W1bornchild{ren) is likely to re:ru.ltfrom the tnutsfc:r.
The lIldividual's condition has not stabilized., how~ver, the individual wIll benefit from a transfer to another facility whichoutweIghs the nsks associated \.\lithtransfer.
- The :ndiV1dllillis lIlllctive labor. The expected benefits oftr.lnsfer outweigh the potential risks to the mother and/or unbornchiici(ren).
-; t Rccci\io~ h05pital ha5 agreed to accept transfer and to provide appropriate :10
'pace and penonne!. Name of hospital :md penonnel contacted. G9\Report given to recehing phY5ician: J : j f l .ljA-1M,,31.A.e &1 By:'
(NM1E OF PHYSfCIAXiREtEIVING REPORn , I , I .(TRANS~ERRING PHYSICIAN)
'V l r ; L . / - flc , YS/"r/' COPII.S OF MEDICAL RECORD SENT
[] ProI2reSSNote 0 X-Rav 0 EKG [] Medicatiorv1Vs ace Sheet ~ER Record I] Transfer Authori.z:!tion :::OtherLevel of Transport:
D Private Car 0 BLS 0 ALS 0 Air Medical Other Name ofTransoortation ComDanv:
Family or Significllnt Other: 0 Notified .~ attendance 0 Unable to contact
Name of family member fJ rfii;: 5 * u / y > - t J - 1 , ~e~~
=--'7 Patient4ifequestJRefusuUConsent to Transfer
ITRANSFER CONSENT
XIacknowledge that my medical condition has been evaluated and explained to me by'the Em
my anen9ing phvslClan '1 '0 0 has recommended that I be transferred to the ServIce of Dr. .4-C '-'A-- '1
C \ "'VA? ~ •.•.•.~ '- Crn~ (hospital). The potential benefits of such transfer, the pOtential risks 'soclated Wlthsuc~,
transtcr. and the probable "risks of not belIlg transferred have been explained to me and r fully W1derstand them. With this knowie"....ge:1.1undcrstanding, I agree and consent to be transferred. t
TRANSFER REQUEST
J II. Iaclcnowledge that my medical condition has been evaluated and explained to me by the Emergency Department phvslcian a."1cJo
my attending physician v .n o has recommended and offe:-ed to me further medicnl eXIiIT'i.!lationand tr~-'.:tr.;ent. The pote:llia! ber:e::lSoj
such further medical examination ancitreatment as well as the potential risks associated \.\lithtransfer to another facility have bee::
explained to me and I fully understand them. In spite of this W1derstanding, I refuse to consent to further medical examination an d
tre:Itment which has been offered to me, and request transfer to _
TRANSFER REFUSAL
'J ill. Iacknowledge ch2tmy medical condition has been evaluated and explained to me by the Emergency Department phvsiclan : : .n o .!: : ;,
my attending physician who !us reccmmended that !be transferred to the service of Dr. The potenuai cene:its
of such transfer. the potenu.al nsks associated \.\lithsuch transfer. and the probable nsks of not belIlg trnnsferred have been expiaulec to 'TIC
ClIldI fully understand them. Even though Dr heiieves It is m mv best lIlte:-est to be tr:lnsferred. : ,e:'~:e :2 :.'clrClIlsCerredand I request ~llIlue retel\'U1g treaunent at
~~~'>"GO S G'- k ~ Q / Q t " - /J~ tvSjgn;~.u,'Ire f IndhiduaJ or Legally Re5poo5ible Indhidual Witness
~ Date 1 : 2 - / ')~ - 0DReiauo hip to IndivldUJ..l
! Rl5k llnd Beoefit3: !have t:xplarned to the lIldividu.all1egally responsIble person L'1efoilov,1ng nsk and benefits of being trarufe:-:-e-"J! refusmg transfe:.
'[ :r:msfcr e;f ~lIS mdi vldu.:Jirs ~err,2 made t- er.. ,,:lUSC th> (j t, II phv IClan railed or re!~sed to Jppe.'1I \'.1thm a reasonClb!e ,\::r-:c-jCI :"' ::.
J I S t r h 1 r pn\'SlC:~ 's r.arne md :;c.idIcss he:-e"
Based on t.he re.1.Sonablensks and ber.efits to the mdividuaJ and/or the W1bom childirenl, and the !nformauon available at :.'1e::.le or :",",e
lIldivlduaJ's e:'..J.ffilI1atlon.che m~ber.e:its reasonably expected from L~eprOV1Slonof approunale medical treatment at anoL'1er:i"1eere..:(ac:iirv outWC1gJJSthe lIlCTea.sednsks. lfanv, to the:n . , "s m ,A i condition from t:tTetllIlg L'1e:ransfer.
~ l - - - - - - _ ( ~
,/
)'.)
I ):i":::.' II ," .