-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
1/12
http://ajs.sagepub.com/ Medicine
The American Journal of Sports
http://ajs.sagepub.com/content/29/1/72The online version
of this article can be found at:
2001 29: 72Am J Sports Med
Joanna Kvist and Jan GillquistChain Exercises in Anterior
Cruciate Ligament-Deficient Patients and Control Subjects
Sagittal Plane Knee Translation and Electromyographic Activity
During Closed and Open Kinetic
Published by:
http://www.sagepublications.com
On behalf of:
American Orthopaedic Society for Sports Medicine
can be found at:The American Journal of Sports
Medicine Additional services and information for
http://ajs.sagepub.com/cgi/alertsEmail Alerts:
http://ajs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
at CAPES on May 4, 2011ajs.sagepub.comDownloaded from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/content/29/1/72http://ajs.sagepub.com/content/29/1/72http://ajs.sagepub.com/content/29/1/72http://www.sagepublications.com/http://www.sagepublications.com/http://www.aossm.org/http://ajs.sagepub.com/cgi/alertshttp://ajs.sagepub.com/cgi/alertshttp://ajs.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsPermissions.navhttp://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://ajs.sagepub.com/subscriptionshttp://ajs.sagepub.com/cgi/alertshttp://www.aossm.org/http://www.sagepublications.com/http://ajs.sagepub.com/content/29/1/72http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
2/12
Sagittal Plane Knee Translation and
Electromyographic Activity During Closedand Open Kinetic Chain
Exercises inAnterior Cruciate Ligament-DeficientPatients and
Control Subjects
Joanna Kvist,*†‡ RPT, PhD, and Jan Gillquist,* MD, PhD
From the Divisions of *Sports Medicine and † Physical Therapy,
Department of Neuroscience and Locomotion, Faculty of Health
Science, Linköping University, Linköping, Sweden
ABSTRACT
Using electrogoniometry and electromyography, wemeasured tibial
translation and muscle activation in 12patients with unilateral
anterior cruciate ligament injuryand in 12 control subjects.
Measurements were madeduring an active extension exercise with 0-,
4-, and8-kg weights and during squats on two legs and on oneleg
where the projection of the center of gravity wasplaced over,
behind, and in front the feet. In the unin-
jured subjects, tibial translation increased with
increas-ing load except during the squat with the center ofgravity
behind the feet, which produced the smallesttranslation. For the
active extension exercises, trans-lation was greater during
eccentric activity. In the an-terior cruciate ligament-injured
knees, all squats re-sulted in similar translation, which was
smaller thanthat during the active extension exercise. The
highestmuscle activation was seen during squats. Hamstringmuscle
activity was low. Increased static laxity in theanterior cruciate
ligament-deficient knee can be con-trolled during closed but not
during open kinetic chain
exercises. Coactivation of the quadriceps and gastroc-nemius
muscles seems to be important for knee sta-bility, whereas
hamstring muscle coactivation was in-significant. To minimize
sagittal translation duringnonoperative management of anterior
cruciate liga-ment-deficient knees, closed kinetic chain
exercises
are preferable to open kinetic chain exercises, andimportance
should be attached to the spontaneouscoactivation of the quadriceps
and gastrocnemiusmuscles.
Closed kinetic chain exercises have become increasinglypopular
and strongly recommended for rehabilitation af-
ter an ACL injury because they are believed to be saferthan
other exercises.6,12,23,28,30,40 In spite of this, Bynumet al.6
found only minor differences in instrumented kneelaxity
measurements between patients who used openkinetic chain and closed
kinetic chain exercises after ACLreconstruction, with the closed
kinetic chain group having slightly less laxity.
The factors of importance to characterize an exercise asmore or
less harmful for the injured knee are the musclecoactivation, shear
forces, tibial translation, and ACLstrain associated with it.
Coactivation of the lower limbmuscles is supposed to improve
stability of the knee joint.2,15,22,28,32,38 It is accepted
that closed kinetic chain
exercises lead to more quadriceps/hamstring muscle coac-tivation
than do open kinetic chain exercises,23,38 but theresults regarding
the amount of coactivation during openkinetic chain exercises are
contradictory.9,15,19,27,31,32
Closed kinetic chain exercises seem to produce smalleranterior
shear forces in healthy subjects and less anteriortibial
translation in ACL-injured knees than do open ki-netic chain
exercises.23,38,40 High anterior shear forcesand increased anterior
tibial translation could be harmfulto the injured or reconstructed
knee because the second-ary restraints or the ligament graft will
be stretched. Inthe early phase of rehabilitation after an ACL
reconstruc-tion, graft strain should be carefully controlled to
promote
‡ Address correspondence and reprint requests to Joanna Kvist,
RPT,PhD, Sports Medicine and Physical Therapy, Department of
Neuroscience andLocomotion, Faculty of Health Sciences, Linköping
University, SE-581 85Linköping, Sweden.
No author or related institution has received any financial
benefit fromresearch in this study. See “Acknowledgments” for
funding information.
0363-5465/101/2929-0072$02.00/0THE A MERICAN JOURNAL
OF SPORTS MEDICINE, Vol. 29, No. 1
© 2001 American Orthopaedic Society for Sports
Medicine
72
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
3/12
healing because too little strain does not stimulate
healing and too much strain leads to graft failure.39 Beynnon
etal.4 have shown in normal knees that the ACL strain issimilar
during open and closed kinetic chain exercises, butthere is no
information about the effect of these exerciseson ACL-deficient
knees. We have previously shown thatanterior tibial translation
during an open kinetic chainexercise with maximal effort remains
within the limits of translation seen during a 90-N Lachman
test, both inuninjured and ACL-injured knees.1,18,19 Therefore,
thereis no clear consensus about the effects of closed or
openkinetic chain exercises on the ACL-deficient or recon-structed
knee.
The purpose of this study was to investigate the
tibialtranslation and EMG activity of the quadriceps, ham-string,
and gastrocnemius muscles during an open kineticchain exercise
(active knee extension) and three differentclosed kinetic chain
exercises (squats where the projectionof the center of gravity was
placed over, behind, and infront of the feet), in persons with
unilateral ACL defi-ciency and uninjured control subjects. The
specific aimswere to investigate the maximal tibial translation
differ-ences 1) during exercises between injured and uninjuredlegs,
2) during four exercises performed with differentloads, and 3)
between the four different exercises. In ad-dition, the tibial
translation during the exercises was in-
vestigated in relation to the static laxity defined from
the90-N Lachman test and at different flexion angles.
Elec-tromyographic analysis was used in the ACL-deficientgroup to
help explain differences in tibial translation.
MATERIALS AND METHODS
The study groups included 12 patients (4 women and 8men) with
unilateral ACL injury verified by arthroscopicexamination or MRI,
and 12 volunteers (6 women and 6men) without any knee joint injury.
The mean age of the ACL-deficient patients was 28 years
(range, 18 to 38) andthe mean age of the control subjects was 29
years (range,
18 to 35). The individual characteristics of all participantsare
shown in Tables 1 and 2.
Measurements
Tibial Translation. A computerized goniometer
linkage(CA-4000, OSI Inc., Hayward, California) was used to
meas-ure the flexion angle and sagittal tibial translation.
Thegoniometer has been described before.1,18,19,24,34–37,40
Thesystem is composed of three parts: the femoral and tibialframes
and a rotation module. Three potentiometers in therotation module
measure the relative rotations between thefemur and tibia. The
potentiometer for sagittal motion,
mounted in the tibial frame, registers the difference in
posi-tion between a spring-loaded patellar pad and the
fixationpoint on the tibial tuberosity during knee motion. The
sag-ittal plane direction is perpendicular to the tibial frame.
Thepotentiometer registering knee extension-flexion wasaligned with
an approximate knee flexion axis in the centerof the lateral
femoral epicondyle and the alignment waschecked repeatedly during
the examination. The flexion an-gle from the CA-4000 corresponds
well with that measuredwith other equipment (unpublished data from
our laborato-
TABLE 1Individual Characteristics of the ACL-Deficient Group
Sex Age Weight
(kg)Height
(cm)Injured
leg Examination
methodaConcominant
injuriesb Surgeryc
Time totest
(months)
Tegner level
Lysholmscore
Lachman (mm)
Preinjury At
exam-ination
ACL-deficient /uninjured
F 22 44 153 L ACI MCL partial, LM 34 3 6 85 11/10
M 24 75 180 L ACI MM MM 22 7 7 60 9/12M 32 88 187 L ACI LM LM 26
9 3 83 7/8M 30 77 181 L ACI 27 7 7 95 9/10M 31 73 170 L ACI 33 9 5
71 7/9M 25 70 183 R ACI LM 35 9 3 59 10/15M 38 61 164 R ACI 24 7 7
95 12/17M 27 87 170 R MRI 20 9 3 100 5/9M 37 81 179 R ACI MM, LM LM
24 9 6 99 7/14F 23 90 173 R MRI 17 9 3 90 8/14F 34 59 160 R ACI MM
MM 35 3 3 73 9/13F 18 62 179 R MRI LM 21 9 2 100 8/12
a ACI, arthroscopy; MRI, magnetic resonance imaging.b MCL,
medial collateral ligament; MM, medial meniscus; LM, lateral
meniscus.c Surgery consisted of partial meniscectomy of the medial
or lateral meniscus.
TABLE 2Individual Characteristics of the Control Group
Sex Age Weight
(kg)Length
(cm)Tegner
levelLachman (mm)
Right Left
M 34 70 183 4 8 8M 31 69 185 4 4 7M 28 68 183 4 5 7M 31 84 183 5
8 12F 29 63 175 5 7 9M 35 64 171 3 7 9F 29 58 167 4 11 10F 25 70
176 3 5 8F 23 64 170 4 8 10F 30 61 174 5 8 10F 18 51 160 10 9 12M
29 75 183 4 8 6
Vol. 29, No. 1, 2001 Translation and EMG Activity During Closed
and Open Kinetic Chain Exercises 73
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
4/12
ry). The system was zeroed at the beginning of each test withthe
subject lying on the examination table and the kneerelaxed in full
extension. Data were sampled from the fourpotentiometers by a
computer at a rate of 100 Hz per chan-nel. In this study, only the
sagittal plane translation (in
millimeters) and the knee flexion angle (in degrees)
wereanalyzed. The accuracy of the measurement system through-out a
range of motion has been shown to be good comparedwith
fluoroscopy.35
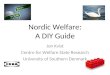
The tibial translation was calculated by subtracting thetibial
position values during a passive extension (de-scribed under
experimental protocol) from the position values during motion
(Fig. 1). During passive extension,the tibia follows the path
determined by joint geometry,including the femoral roll back, and
falls back to theposterior limit of a passive envelope of knee
motion due tothe gravity vector.5
EMG. The EMG activity of the vastus medialis,
vastus
lateralis, hamstring, and gastrocnemius lateralis muscleswas
recorded by surface electrodes. The muscles werelocated by
palpation during a submaximal isometric con-traction, and the most
prominent part of the muscle wasused for the placement of the
electrodes. The electrodeplacement was verified through functional
testing whileobserving the recording on the computer screen. The
skin
was first dry shaved and then cleaned with 70% alcohol.On the
skin above each muscle, two recording pregelledsilver-chloride
electrodes (Blue sensor, M-00-S, Medi-cotest, Denmark; diameter of
active part, 10 mm) wereplaced within 2 cm of each other
(center-to-center dis-tance) and one ground electrode with
amplifier was placedabout 10 cm from the measuring area. Signals
were sam-pled at 2000 Hz by an MESPEC 4000 EMG unit system(MEGA
Electronics Ltd., Kuopio, Finland). All signalswere amplified and
analog-to-digital converted with 12-bitaccuracy in the signal range
of 5000 V. An averagedEMG signal was
formed by rectifying the raw signal andtaking the average of 12
signal readings taken at 1-msecintervals.
Data from the CA-4000 (knee flexion angle, tibial posi-tion in
relation to the patella and femur, and anterior-posterior load from
a force handle) and the four EMGchannels were acquired
simultaneously in a personal com-puter. The output frequency of all
signals was 83 Hz.
Experimental Protocol
The testing protocol was similar in the two groups, exceptthat
the EMG measurements were performed on both legsin the
ACL-deficient group only. In the control group, theright or left
leg was tested first in a random order; in the ACL-deficient
group, the uninjured leg was always tested
first.The subjects in the ACL-deficient group began with
three maximum isometric voluntary contractions each forknee
extension, knee flexion, and ankle plantar flexion.For knee
extension and flexion, the subjects were seatedwith the knee
positioned and restrained by a strap at 40°and 130° of knee
flexion, respectively. For ankle plantarflexion, the subjects were
standing on one leg in an up-right position with balance support
and instructed to riseon their toes as high as possible. The mean
value during the period of 252 msec with the highest signal
values foreach muscle was used to normalize the EMG values dur-ing
the exercises.
In all subjects, an instrumented Lachman test was per-formed
with the subject strapped to a special seat with theknee flexed to
20°. Tibial translation was recorded when aperpendicular,
posterior-anterior directed load of morethan 140 N was applied by a
force handle to a point 9 cmbelow the medial joint line. The total
translation at 90 Nof force is reported.
To identify a reference line for the calculation of trans-lation
during activity, a passive extension motion wasperformed from 100°
to 0° of knee flexion with the subjectsitting on an examination
table and his or her back sup-ported in a start position of 110° of
hip flexion and 90° of knee flexion. The subjects relaxed and,
with the heel sup-
Figure 1. Calculation of translation during the active
exer-
cises. A, the filled circles represent the position of the
tibia
relative to the patella/femur during the active exercise and
the open circles represents the same position during the
passive extension test (one mark for each fifth degree of
knee flexion angle). B, each marker represents the sagittal
tibial translation during the active exercise (subtracted
value
of the tibial position during the passive extension from the
position values during active exercise). Negative
translation
values imply posterior translation.
74 Kvist and Gillquist American Journal of Sports
Medicine
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
5/12
ported by the examiner, the knee joint was first passivelyflexed
to 100° and then extended to full extension, whileavoiding axial
rotation of the tibia. The passive extensiontest has a good
repeatability. The mean difference be-tween seven repetitions
during a 1.5-hour long test ses-sion, with two to four other
exercises in between, is 0.06 0.09 mm.17
The subjects then performed four repetitions of the
fourexercises in a random order (Fig. 2). In the open kineticchain
exercise (active knee extension), the start positionwas the same as
for the passive extension test. The exer-cise was performed with
0-, 4-, and 8-kg weights appliedon the distal tibia.
Three closed kinetic chain exercises (squats) were done:1) a
squat where the projection of the center of gravity
wasapproximately over the feet, 2) a squat with the backresting
against a wall and the feet 40 cm from the wall(the center of
gravity in this exercise was behind the feet),and 3) a squat with
the hands on a wall and the feet 1meter from the wall (the center
of gravity in this exercisewas in front the feet). The load during
the closed kineticchain exercises was varied by doing the exercises
on one orboth legs.
Repeatability
The repeatability of the tibial translation
measurementsthroughout a range of motion (0° to 90° to 0° at 5°
intervalsfor a total of 37 angles compared) for the squat with
centerof gravity over the feet was tested. Six subjects in
thecontrol group (three right and three left legs) were ran-domly
chosen to do the test on 2 different days. Using analysis of
variance for repeated measures, we found no
significant differences between the measurements fromthe 2 days.
The mean difference between days throughoutthe range of motion was
0.73 0.41 mm, with a mean 95%confidence interval at the different
flexion angles between0.51 and 1.97.
The repeatability of the maximal translation betweenthe four
repetitions in the right knee was analyzed in thecontrol group.
Using analysis of variance for repeatedmeasures, we found no
significant differences. The meandifference in the exercises
between the four repetitionswas 0.07 0.08 mm ( N 9),
with a mean individual 95%confidence interval between 0.29 and
0.43.
Data Analysis
The mean values from the four repetitions were used infurther
calculations. The translation measurements at 20°of knee flexion in
all exercises were normalized to thetranslation during a 90-N
Lachman test for the same leg.In the ACL-deficient group, the
translation at 20° of flex-ion in the injured leg was also
normalized to the transla-tion of the uninjured knee during the
90-N Lachman test.
The EMG signals were normalized to signals during themaximum
voluntary contraction test for the same leg. TheEMG activity of
quadriceps muscle was calculated as themean of the vastus medialis
and vastus lateralis muscles.
Statistics
A two-way analysis of variance for repeated measureswith
contrast analysis was used for differences in maxi-mal translation
and the flexion angle where the maximaltranslation occurred between
the uninjured and injuredleg in the ACL-deficient group and between
right and leftlegs in the control group. A two-way analysis of
variance(2 10) between group design with contrast analysis wasused
for differences in maximal translation and the flex-ion angle where
the maximal translation occurred be-tween the control group and the
uninjured leg in the ACL-deficient group.
Analysis of variance for repeated measures and Stu-dent’s
t-test for dependent variables with Bonferroni cor-rection
for multiple tests was used for comparisons be-tween the exercise
subsets in the ACL-deficient group,regarding maximal translation
and translation at 20° of knee flexion.
A three-way analysis of variance (4 2 11), betweenthe 4
exercises, within the 2 legs, and at 11 angles (10°,
20°, 30°, 50°, 70°, 90°, 70°, 50°, 30°, 20°, 10°), and
theStudent’s t-test for dependent variables with
Bonferronicorrection for multiple tests were used for
comparisonbetween the four exercises regarding translation in
thedifferent flexion angles in the ACL-deficient group.
The EMG data were analyzed at a range of motionbetween 10° and
90° of knee flexion. Analysis of variancefor repeated measures was
done for differences in EMGbetween the legs and between the flexion
angles, 10° to45°, 50° to 85°, 85° to 50°, and 45° to 10°, and
between thedifferent exercises within the same leg.
Statistics were calculated using commercially availablesoftware
(Statistica 4.3, StatSoft, Inc., Tulsa, Oklahoma).
RESULTS
Control Group
Maximal Translation. The translation recorded
during the 90-N Lachman test (1.7 1.6 mm) was 19% greater
inthe left leg than in the right. For the active exercises,
nosignificant difference existed between the two legs. Themean
values for the right and left legs were used in fur-ther
statistical analysis.
In terms of the different loads used, in the open kineticchain
exercise, the maximal translation increased 16%
between the 0-kg and the 4-kg load and 11% from the 4-kg to
8-kg load ( P 0.005). In the closed kinetic chain exer-cises,
for squats with the center of gravity over the feet orin front of
the feet, the increase in translation comparedwith that during
active extension was similar (17% and22%, respectively), but there
was no change in translationduring the squat with the center of
gravity behind the feet(Table 3 and Fig. 3).
When comparing the different exercises at maximalload, the squat
with the center of gravity over or in frontof the feet resulted in
the same translation as the activeextension exercise, whereas the
squat with the center of gravity behind the feet produced a
24% smaller transla-
Vol. 29, No. 1, 2001 Translation and EMG Activity During Closed
and Open Kinetic Chain Exercises 75
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
6/12
tion ( P 0.005) than the other exercises (Table 3, Fig.
4).The squat with the center of gravity in front the feetproduced
the largest translation of the closed chain exer-
cises ( P 0.005). Normalized Translation. All
the exercise subsets pro-
duced translations within the limits seen during a 90-NLachman
test (Table 3).
Flexion Angle Where Maximal Translation Occurred. In
the open chain exercises, the maximal translation oc-curred
between 16° and 19° of knee flexion. In the three
Figure 2. The four active exercises. A, active knee
extension. B, squat where the projection of the center of gravity
was
approximately over the feet. C, squat where the projection of
the center of gravity was approximately behind the feet. D,
squat
where the projection of the center of gravity was approximately
in front the feet.
76 Kvist and Gillquist American Journal of Sports
Medicine
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
7/12
closed kinetic chain exercises, the maximal translationoccurred
at significantly higher angles (23° to 40°) com-pared with the open
kinetic chain exercises, but therewere no significant differences
between the three closedkinetic chain exercises.
Differences in Translation at Different Flexion Angles.In
the open kinetic chain exercise, the translation washigher during
the eccentric phase than during the con-centric phase. Between 40°
and 10° of knee flexion, thetranslation was always smaller in the
closed kineticchain exercises than in the open kinetic chain
exercises. At 40° to 70°, a shift occurred so that at flexion
anglesover 70°, the translation was larger in the closed
kinetic
chain exercises, especially during the concentric phaseof the
motion. The difference in the translation behaviorduring flexion
and extension between the types of exer-cise was significant
( P 0.0007). During the closedkinetic chain
exercises, the change in translation be-tween 30° and 90° of knee
flexion was only half thatduring the open kinetic chain exercise (a
change of 1.3mm per 20° interval during the closed kinetic
chainexercise and 2.6 mm during the open kinetic
chainexercise).
Figure 3. Maximal translation during the four exercises
with
the different loads (mean SD). Open circles are for
the
lowest load (0 kg in the active extension test and squat
performed on two legs in the squat tests), open squares are
for the intermediate load (4 kg in the active extension
test),
and filled circles are for the highest load (8 kg in the
active
extension test and squat performed on one leg in the squat
tests). C, control group; U, uninjured leg; I, injured leg;
CG,
center of gravity. Asterisks indicate significant
differences.
Figure 4. Maximal translation with maximal load for the
fourexercises (mean SD): active extension with an 8-kg
load
(filled circle), squat with the projection of the center of
gravity
over the feet on 1 leg (open squares), squat with the
projec-
tion of the center of gravity behind the feet on 1 leg
(horizon-
tal line), and squat with the projection of the center of
gravity
in front of the feet on 1 leg (open circles). Comparison
within
groups for the control subjects, the uninjured leg in the
ACL-
deficient subjects, and the injured leg in the ACL-deficient
subjects. a, significantly different from active extension with
8
kg; b, significantly different from squat with the center of
gravity over the feet; c, significantly different from squat
with
the center of gravity behind the feet; d, significantly
different
from squat with the center of gravity in front the feet.
TABLE 3Maximal Translation (in Millimeters) in the Control Group
and the Uninjured and Injured Legs in the ACL-Deficient Group
(Mean and SD)
Exercise Control ACL-deficient group P
Value
Uninjured leg Injured leg Difference ACLa C-ACLb
Lachman 8.2 1.7 8.4 1.9 11.9 2.8 3.5 2.3 0.0000
0.8754 Active extension
0 kg 5.6 1.9 7.9 3.5 10.1 3.1 2.2 1.9 0.0002 0.05904 kg 6.7 1.8
9.0 3.1 11.6 3.5 2.6 1.2 0.0000 0.04688 kg 7.5 2.0 10.3 3.5 12.4
3.4 2.1 2.2 0.0003 0.0140
SquatCenter of gravity over the feet
2 legs 5.9 2.1 7.1 3.6 8.9 2.9 1.8 1.6 0.0023 0.26261 leg 7.1
2.1 8.1 3.7 9.1 2.5 0.9 2.0 0.1059 0.3446
Center of gravity behind feet2 legs 5.8 1.5 6.8 3.3 9.0 2.7 2.1
1.6 0.0003 0.35521 leg 5.7 1.8 7.2 3.1 8.5 2.9 1.2 1.4 0.0276
0.1863
Center of gravity in front of feet2 legs 6.6 2.3 6.7 3.9 7.5 3.1
0.9 1.3 0.1300 0.98731 leg 8.5 2.1 8.8 4.1 9.8 3.0 1.1 1.8 0.0557
0.8174
a P value for difference between uninjured and
injured leg in the ACL-deficient group.b P value for the
difference between the control group and the uninjured leg in the
ACL-deficient group.
Vol. 29, No. 1, 2001 Translation and EMG Activity During Closed
and Open Kinetic Chain Exercises 77
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
8/12
ACL-Deficient Group
Maximal Translation. The translation in the
uninjured
leg of the ACL-deficient patients was similar to that in
thecontrol group in all exercises except during the activeextension
tests performed with 4- and 8-kg loads, where it
was 27% larger ( P 0.05). In the ACL-injured
leg, the
translation seen during the 90-N Lachman test (3.5
2.3mm) was 29% greater than that in the uninjured leg.During the
active exercises, the maximal translation inthe injured legs was
15% to 24% greater ( P 0.05) than in
the uninjured legs in all but three exercise subsets (squatswith
the center of gravity over the feet on one leg and
squats with the center of gravity in front of the feet onboth
one and two legs).
In terms of the effect of different loads, the uninjured
leg
had the same motion pattern as the control group in allexercises
(Table 3, Fig. 3). The injured leg followed the
same pattern as the uninjured leg, with similar
relativeincreases in translation with increased load, except
during
the squats with the center of gravity behind and over thefeet,
where translation did not increase with load.
When comparing the translation during maximal load
in the different exercises, the uninjured knees behavedsimilar
to the control group (Table 3, Fig. 4). The closedkinetic chain
exercises produced the same translation as
the active extension exercise except for the squat with
thecenter of gravity behind the feet, where the translation
was 30% smaller ( P 0.05). In the injured leg, the
trans-lation produced during the closed kinetic chain exerciseswas
between 69% and 79% of that in the active extension
test ( P 0.005), with no differences between the
individ-ual exercises.
Normalized Translation. In the uninjured leg,
thetranslation limits were the same as those seen during the90-N
Lachman test (Table 3). In the injured knee, the
translation measured during squats with the center
of gravity over the feet on two legs, behind the feet on
bothtwo legs and one leg, and in front of the feet on two legs
was only 70% of that seen during the Lachman test. In theactive
extension exercises and the squats with the center
of gravity over and in front of the feet on one leg,
thetranslation limits were the same as those during the Lach-man
test. When comparing the translation during activity
in the injured knee with the 90-N Lachman test in theuninjured
leg, only the active extension with 8 kg ex-
ceeded the envelope by 20%. Flexion Angle Where Maximal
Translation Occurred. In
the uninjured leg, the maximal translation occurred at the
same flexion angles as in the control group. In the injuredleg
the maximal translation occurred at the same angle asin the
uninjured leg during the open kinetic chain exer-
cises but in significantly smaller angles (10°, P
0.05)during closed kinetic chain exercises except in
the squatwith the center of gravity behind the feet on one leg.
Differences in Translation at Different Flexion
Angles.
Both the uninjured and injured legs had the same motionpattern
as the control group (Fig. 5).
EMG in the ACL-Deficient Group (Fig. 6)
No muscle activation was found during the Lachman testor the
passive extension test.
Mean EMG Activity at 10°-90°-10° of Knee Flexion.
Inthe uninjured leg, the EMG activity of the quadricepsmuscles
increased (mean, 13% 2% units) with increasedload during all
exercises except the squat with the centerof gravity in front of
the feet. When comparing the exer-cises with the highest load in
the uninjured leg, the activeextension test had less quadriceps
muscle activity (mean,19% 17% maximal voluntary
contraction [MVC]) thanthe closed kinetic chain exercises. The
squats with thecenter of gravity over and behind the feet resulted
ingreater EMG activity of the quadriceps muscle (33% 20% and
32% 21% MVC, respectively) than the squatwith the
center of gravity in front of the feet (25% 23%MVC) ( P
0.05). The injured leg had the same EMGactivity pattern as
the uninjured leg.
In the uninjured leg, the hamstring muscle EMG activ-ity
increased with increased load (mean, 3% 3% units)
in all exercises except the squat with the center of gravityin
front of the feet. When comparing the exercises with thehighest
load in the uninjured leg, the activation of thehamstring muscles
increased from 3% 1% during activeextension to 8% 7% during the
squat with the center of gravity behind the feet and 9%
8% during the squatwith the center of gravity over the feet
( P 0.05). Thesquat with the center of gravity
in front of the feet was amean of 5% 6% units lower
in EMG activity than thesquat with the center of gravity over the
feet ( P 0.05). Inthe injured leg, the activation pattern was
the same as inthe uninjured leg except that the squat with the
center of gravity in front of the feet resulted in less EMG
activity
than did the other two squats ( P 0.05).In both legs, the
EMG activity of the gastrocnemius
Figure 5. Tibial translation in the injured leg (mean)
during
the range of motion between 0° and 90° of knee flexion
angle, in the four exercises with the highest load: active
extension with an 8-kg load (filled circles), squat with the
projection of the center of gravity over the feet on one leg
(open squares), squat with the projection of the center of
gravity behind the feet on one leg (plus), and squat with
the
projection of the center of gravity in front of the feet on
one
leg (open circles).
78 Kvist and Gillquist American Journal of Sports
Medicine
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
9/12
muscle remained the same with increased load during theopen
kinetic chain exercises, but it increased a mean of 10%
2% units with increased load during the closedkinetic chain
exercises. For the exercises with the highestload, in both legs the
EMG activity of the gastrocnemiusmuscle was lower in the active
extension exercise com-pared with all the closed kinetic chain
exercises ( P
0.05), with no difference between the three closed kineticchain
exercises.
EMG Activity at Flexion Angles of 10° to 45° and 50°
to
85° in Both Concentric and Eccentric Phase. In both
legs,in all exercises, the activation of the vastus medialis
and vastus lateralis muscles was always significantly
largerduring the concentric phase than during the eccentricphase.
During the active extension test, the activation waslarger at the
smaller knee flexion angles (10° to 45°); during the closed
kinetic chain exercises, the activation was largerat the higher
flexion angles (50° to 85°) ( P 0.05).
For the hamstring muscles, in both legs the activationlevel
during the active extension exercise was the same at
the different flexion angles. Only small differences (mean,2%
1% MVC) were found between the different kneeflexion
angles in the closed kinetic chain exercises, exceptin squats with
the center of gravity over the feet, wherethe activation was a mean
5% 1% units greater during the concentric phase than during
the eccentric phase( P 0.05).
The EMG activity of the gastrocnemius muscle during the
active extension test was not significantly different atthe
different flexion angles. During the closed kineticchain exercises,
the activation pattern of the gastrocne-mius muscle was the same as
for that of the quadricepsmuscles.
Summary of Results
•The injured legs produced greater tibial translationcompared
with the contralateral uninjured leg during allexercises except for
squats with the center of gravity overthe feet (on one leg) and in
front of the feet (on both twolegs and one leg).
•In the uninjured legs, tibial translation increased
withincreased load during the active extension and during thesquats
with the center of gravity over the feet and in frontof the feet
but remained the same during the squats withthe center of gravity
behind the feet. In the injured leg, thetibial translation
increased only during the active exten-sion and during the squat
with the center of gravity infront of the feet.
•In the uninjured legs, the different closed kinetic
chainexercises resulted in different amounts of tibial
transla-tion, and only the squat with the center of gravity
behindthe feet produced less translation than the other
exercises.In the injured legs, all the closed kinetic chain
exercises
produced similar translations, which were less than
thetranslation produced during the open kinetic chainexercise.
•In the uninjured legs, all exercises resulted in trans-lation
limits equal to those seen during the 90-N Lachmantest. In the
injured legs, the limits of translation during the squats
performed on two legs and during the squatwith the center of
gravity behind the feet on one leg wereonly 70% of that seen during
the Lachman test. The otherexercises resulted in translation equal
to that seen during the Lachman test.
•The uninjured and injured legs followed the same pat-tern of
tibial motion in the sagittal plane throughout the
Figure 6. Graph showing the EMG in the injured leg, of
the quadriceps (mean of vastus medialis and vastus lateralis),
the
gastrocnemius, and hamstring muscles during the open kinetic
chain (active extension) test with an 8-kg load (AE8) and theclosed
kinetic chain squat tests on one leg with the projection of the
center of gravity (CG) over the feet (CG01), behind the feet
(CGB1), and in front of the feet (CGF1). The hamstring muscle
activity is expressed as negative values. The four
columns/groups
represent the EMG activity at angles of 10°to 45°and 50°to 85°of
knee flexion (eccentric phase) and at angles of 85°to 50°
and 45°to 10°of knee flexion (concentric phase).
Vol. 29, No. 1, 2001 Translation and EMG Activity During Closed
and Open Kinetic Chain Exercises 79
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
10/12
range of motion. The translation was always less during the
closed kinetic chain exercises than during the openkinetic chain
exercises between 40° and 10° of knee flex-ion, and at flexion
angles over 70° the translations werelarger in the closed kinetic
chain exercises.
•Similar muscle activation patterns were found in theuninjured
and injured knees. The overall EMG activity
was higher during the closed kinetic chain exercises thanduring
the open kinetic chain exercises. The quadricepsand gastrocnemius
muscles acted simultaneously. The ac-tivity in the hamstring
muscles was generally low.
DISCUSSION
The main result of this study was that translation in-creased
with increasing load in the uninjured and normalknees except during
the squats with the center of gravitybehind the feet, where it
remained the same. The increasein translation indicates an
increased recruitment of therestraining mechanism with increased
load, in accordancewith other studies.1,18,19 Translation values
during theactive extension exercises were higher during the
eccen-tric phase than during the concentric phase, which is inline
with our previous results.19 The different closed ki-netic chain
exercises resulted in different amounts of tib-ial translation, and
the squat with the center of gravitybehind the feet produced less
translation than did theother exercises in all uninjured and normal
knees, indi-cating that the restraining mechanism is engaged
depend-ing on variations of the external load.
In the ACL-deficient knees, all closed kinetic chain ex-ercises
produced less translation than the open kineticchain exercise, and
there was no difference between theclosed kinetic chain exercises
when performed with the
highest load. Activation of the quadriceps and gastrocne-mius
muscles also increased with increasing load, exceptfor
insignificant gastrocnemius muscle activity during theopen kinetic
chain exercises and low quadriceps muscleactivation during the
squat with the center of gravity infront of the feet. The hamstring
muscle activation levelswere rather low, but increased with load
similar to thequadriceps muscle activation pattern. The highest
activa-tion levels for all muscles were seen during closed
kineticchain exercises.
The knee joint has six degrees of freedom, and all mo-tions are
combinations of rotations and translations. Lig-aments guide and
limit the combined motions, and an
ACL rupture will affect primarily the anterior tibial
trans-lation but also the axial rotation of the tibia.7 In
thepresent study, we analyzed only sagittal translation
anddescribed the motion pattern only two-dimensionally. Thismethod
of analyzing tibial translation has been found tohave good accuracy
and repeatability,1,17,18,34,35 but stan-dardized methods to
evaluate axial rotations are lacking.
The amount of anterior tibial translation in normalknees depends
on the muscle activation, joint compressionforces, geometry, and
ligament restraints, primarily the ACL.7 After an ACL
rupture, muscle activation and jointcompression forces become more
important as joint stabi-lizers. In the ACL-deficient knees we
found that closed
kinetic chain exercises caused less translation than didthe
other exercises, which confirms the findings by Yack etal.40 The
joint moments differed between the exercisesand, in spite of the
smaller translation during the closedkinetic chain exercises, the
largest quadriceps muscle ac-tivation was found during these
exercises and occurred atlarge flexion angles. In contrast, in the
open kinetic chain
exercises, the maximum quadriceps muscle activity oc-curred near
extension. During the closed kinetic chainexercises, the tibia
assumed an initial anterior positionand then remained within a
rather narrow range. In con-trast, during the open kinetic chain
exercises, the changein translation with change in knee flexion was
muchlarger. Here the neutral tibial position during passivemotion
was reached at 90° of flexion, when the quadricepsmuscle activity
was low. This anterior displacement of thestarting position with
compressive load on the joint isthought to be due to the joint
geometry, including theposterior tilt of the tibial plateau, and
has been describedbefore in vitro by Torzilli et al.33 and Li et
al.21
Knee extension moments cause anterior shear forces onthe tibia
at flexion angles between 0° and 70° during anopen kinetic chain
exercise.3,25,29,38 During closed kineticchain exercises, posterior
shear forces, which should pro-hibit anterior translation of the
tibia, have been recordedthroughout the whole range of motion.38
Our results agreewith findings of higher joint compression forces
that de-crease anteroposterior translation during a closed
kineticchain exercise compared with an open kinetic
chainexercise.38
Previous studies have analyzed the importance of ham-string
muscle coactivation for knee stability.2,15,22,28,32,38
In agreement with other studies, we found low levels
of hamstring muscle coactivation during the open kinetic
chain exercise but significantly more activation
during squats with the center of gravity over and behind
thefeet.19,23,38 Even so, the activation levels were generallylow,
and it has been questioned if these levels can coun-teract the
anterior shear forces generated by the quadri-ceps muscle.13
Torzilli et al.33 found in an in vitro exper-iment that not even a
100-N posterior force could reducethe anterior positioning that
occurred after sectioning of the ACL when the knee was under a
joint compressionload corresponding to weightbearing. In contrast
to ourresults, Kellis and Baltopoulos14,16 found 30% to
40%hamstring muscle coactivation during an isokinetic quad-riceps
muscle exercise. They calculated the hamstring mo-
ment to be about 29 Nm during concentric quadricepsmuscle action
and 43 Nm during eccentric quadricepsmuscle action,15 which is only
about 10% of the simulta-neous quadriceps moment. Other studies
have presentedwidely varying figures for hamstring muscle
coactivationduring open kinetic chain exercises, from 1.5%18 to
40%MVC,9,27,31,32 and during a squat it varies between 3%and
15%.10,11,13 Our registered hamstring muscle activa-tion was close
to what can be found as cross talk8 and is inthe lower end of the
range in other studies. It is thereforequestionable if this
activation had importance for jointstability.
On the other hand, the gastrocnemius muscle activation
80 Kvist and Gillquist American Journal of Sports
Medicine
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
11/12
coincided with and was about 50% of the quadriceps mus-cle
activation during the closed kinetic chain exercises andwas
generally higher in the ACL-deficient leg, as has beenseen in
another study.20 The gastrocnemius muscle hasbeen shown to pull the
femur backward on the tibia.26
Limbird et al.22 found subnormal gastrocnemius andquadriceps
muscle activation in the ACL-deficient knee,
which supports our suggestion of a parallel activation
of these muscles. In the present study, this parallel
activa-tion probably moved the tibia to a forward position,
whichcould also be observed at the start of the squatting motion.It
would also tend to increase joint compressive forces
and,accordingly, we found no increase in translation in
the ACL-deficient knees with increasing load in squats withthe
center of gravity over and behind the feet, when bothmuscles were
activated. Therefore, the simultaneous acti- vation of the
quadriceps and gastrocnemius musclesseems to represent an important
mechanism for stabiliza-tion of the unstable knee in contrast to
hamstring muscleactivation.
The results of this study indicate that patients cancontrol the
increased static laxity of the ACL-deficientknee during closed
kinetic chain exercises, as has beenreported in previous
studies,37,40 but not during openkinetic chain exercises,
especially not during the eccentricphase of the motion, in line
with our previous results.19
For nonoperative treatment after an ACL injury, it isimportant
to strengthen the spontaneous coactivation of quadriceps and
gastrocnemius muscles, which will help tomaintain a relatively
stable knee position because of theincreased joint compression
forces. It is still unknown howdifferent performance of the closed
kinetic chain exercisesinfluences knee kinematics after an ACL
reconstructionand what effect these exercises might have on
long-termknee stability.
CONCLUSIONS
1. Open kinetic chain exercises with increased load onthe knee
joint cause increasing anterior tibial translation.
2. Closed kinetic chain exercises cause less translationin the
ACL-injured knee than do open kinetic chainexercises.
3. In the ACL-deficient knee, the translation was thesame during
the three different closed kinetic chain exer-cises, in contrast to
the results in normal knees where thesquat with the center of
gravity behind the feet caused theleast translation.
4. Hamstring muscle coactivation was low during theopen kinetic
chain exercises but somewhat higher during the closed kinetic
chain exercises. In contrast, the gastroc-nemius muscle activation
was much higher, 50% of thequadriceps muscle activation, during the
closed kineticchain exercises.
5. Joint compression and simultaneous quadriceps
andgastrocnemius muscle activation seem to be importantmechanisms
to increase knee stability.
ACKNOWLEDGMENTS
The authors thank Peter Rockborn, MD, PhD,
Norrköping County Hospital, Sweden, for referring the
ACL-deficientpatients. This study was supported by grants from
TheSwedish Foundation for Health Care Sciences and AllergyResearch
“Vårdalsstriftelsen,” Stockholm; the SwedishMedical Research
Council (nr K1999–73x-012223– 03),Stockholm; the Swedish Centre for
Research in Sports (nr103/98), Stockholm; and the “Doctor
Svantessons Memo-rial Fund.”
REFERENCES
1. Antonopoulos J, Gillquist J: Anterior tibia translation
related to isokineticconcentric quadriceps torques. Isokin
Exerc Sci 6: 145–151, 1996
2. Baratta R, Solomonow M, Zhou B, et al: Muscular coactivation:
The role ofthe antagonistic musculature in maintaining knee
stability. Am J Sports Med 16: 113–122,
1988
3. Beynnon BD, Fleming BC, Johnson RJ, et al: Anterior cruciate
ligamentstrain behavior during rehabilitation exercises in vivo.
Am J Sports Med 23: 24–34, 1995
4. Beynnon BD, Johnson RJ, Fleming BC, et al: The strain
behavior of the
anterior cruciate ligament during squatting and active
flexion-extension. Acomparison of an open and closed kinetic chain
exercise. Am J Sports Med 25: 823–829,
1997
5. Blankevoort L, Huiskes R, de Lange A: The envelopment of
passive knee joint motion. J Biomech 21:
705–720, 1988
6. Bynum EB, Barrack RL, Alexander AH: Open versus closed chain
kineticexercises after anterior cruciate ligament reconstruction. A
prospectiverandomized study. Am J Sports Med
23: 401–406, 1995
7. Daniel DM, Akeson WH, O’Connor JJ: Knee Ligaments.
Structure, Func- tion, Injury, and Repair. New York,
Raven Press, 1990
8. De Luca CJ, Merletti R: Surface myoelectric signal cross-talk
amongmuscles of the leg. Electroencephalogr Clin
Neurophysiol 69: 568–575,1988
9. Draganich LF, Jaeger RJ, Kralj AR: Coactivation of the
hamstrings andquadriceps during extension of the knee. J Bone
Joint Surg 71A: 1075– 1081, 1989
10. Graham VL, Gehlsen GM, Edwards JA: Electromyographic
evaluation ofclosed and open kinetic chain knee rehabilitation
exercises. J Athletic
Training 28: 23–30, 199311. Gryzlo SM, Patek RM,
Pink M, et al: Electromyographic analysis of knee
rehabilitation exercises. J Orthop Sports Phys Ther
20: 36–43, 199412. Henning CE, Lynch MA, Glick KR Jr: An
in vivo strain gage study of
elongation of the anterior cruciate ligament. Am J Sports
Med 13: 22–26,1985
13. Isear JA, Erickson JC, Worrell TW: EMG analysis of lower
extremitymuscle recruitment patterns during an unloaded squat.
Med Sci Sports Exerc 29: 532–539, 1997
14. Kellis E, Baltzopoulos V: Muscle activation differences
between eccentricand concentric isokinetic exercise. Med Sci
Sports Exerc 30: 1616–1623,1998
15. Kellis E, Baltzopoulos V: The effects of antagonist moment
on the result-ant knee joint moment during isokinetic testing of
the knee extensors. Eur J Appl Physiol 76:
253–259, 1997
16. Kellis E, Baltzopoulos V: The effects of normalization
method on antag-onistic activity patterns during eccentric and
concentric isokinetic kneeextension and flexion. J
Electromyogr Kinesiol 6: 235–245, 1996
17. Kvist J: Knee motion pattern during activity, in individuals
with anteriorcruciate ligament injury and uninjured controls.
Doctoral Thesis, Faculty ofHealth Sciences, Linköping University,
Linköping, Sweden, 2000
18. Kvist J, Gillquist J: Anterior tibial translation during
eccentric, isokineticquadriceps work in healthy
subjects. Scand J Med Sci Sports
9: 189–194,1999
19. Kvist J, Karlberg C, Gerdle B, et al: Knee motion pattern
during differentisokinetic quadriceps torques in anterior cruciate
ligament deficient indi-viduals. J Orthop Sports Phys Ther
31: in press, 2001
20. Lass P, Kaalund S, leFrevre S, et al: Muscle coordination
following ruptureof the anterior cruciate ligament.
Electromyographic studies of 14 patients.Acta Orthop Scand
62: 9–14, 1991
21. Li G, Rudy TW, Allen C, et al: Effect of combined axial
compressive andanterior tibial loads on in situ forces in the
anterior cruciate ligament: Aporcine study. J Orthop Res
16: 122–127, 1998
22. Limbird TJ, Shiavi R, Frazer M, et al: EMG profiles of knee
joint muscu-lature during walking: Changes induced by anterior
cruciate ligamentdeficiency. J Orthop Res 6:
630–638, 1988
Vol. 29, No. 1, 2001 Translation and EMG Activity During Closed
and Open Kinetic Chain Exercises 81
at CAPES on May 4, 2011ajs.sagepub.comDownloaded
from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/
-
8/17/2019 Am J Sports Med 2001 Kvist 72 82
12/12
23. Lutz GE, Palmitier RA, An KN, et al: Comparison of
tibiofemoral jointforces during open-kinetic-chain and
closed-kinetic-chain exercises.J Bone Joint Surg 75A:
732–739, 1993
24. Lysholm M, Messner K: Sagittal plane translation of the
tibia in anterior
cruciate ligament-deficient knees during commonly used
rehabilitationexercises. Scand J Med Sci Sports
5: 49–56, 1995
25. Nisell R: Mechanics of the knee. A study of joint and muscle
loadwith clinical applications. Acta Orthop Scand (Suppl
216) 56: 4–42,1985
26. O’Connor J, Shercliff T, FitzPatrick D, et al: Mechanics of
the knee, inDaniel DM, Akeson WH, O’Connor JJ (eds): Knee
Ligaments. Struc- ture, Function, Injury, and Repair .
New York, Raven Press, 1990, pp
201–23727. Osternig LR, Caster BL, James CR: Contralateral
hamstrings (biceps
femoris) coactivation patterns and anterior cruciate ligament
dysfunction.Med Sci Sports Exerc 27: 805–808, 1995
28. Palmitier RA, An KN, Scott SG, et al: Kinetic chain exercise
in kneerehabilitation. Sports Med 11: 402–413,
1991
29. Renström P, Arms SW, Stanwyck TS, et al: Strain within the
anterior
cruciate ligament during hamstring and quadriceps activity.
Am J Sports Med 14: 83–87, 1986
30. Shelbourne KD, Nitz P: Accelerated rehabilitation after
anterior cruciateligament reconstruction. Am J Sports Med
18: 292–299, 1990
31. Snow C, Cooper J, Quanbury A, et al: Antagonist
cocontraction of kneeflexors during constant velocity muscle
shortening and lengthening. J Electromyogr Kinesiol
3: 78–86, 1993
32. Solomonow M, Baratta R, Zhou BH, et al: The synergistic
action of theanterior cruciate ligament and thigh muscles in
maintaining joint stability.Am J Sports Med 15:
207–213, 1987
33. Torzilli PA, Deng X, Warren RF: The effect of
joint-compressive load andquadriceps muscle force on knee motion in
the intact and anterior cruciateligament-sectioned knee. Am J
Sports Med 22: 105–112, 1994
34. Vergis A: Sagittal plane knee translation in healthy and ACL
deficientsubjects. A methodological study in vivo with clinical
implications. 1999Doctoral Thesis, Faculty of Health Sciences,
Linköping University, Linkö-ping, Sweden
35. Vergis A, Gillquist J: Fluoroscopic validation of
electroniometrically meas-ured femoral roll-glide motion in the
knees of healthy and ACL deficientsubjects. Trans Orthop Res
Soc 25: 486, 2000
36. Vergis A, Gillquist J: Sagittal plane translation of the
knee during stairwalking. Comparison of healthy and anterior
cruciate ligament-deficientsubjects. Am J Sports Med
26: 841–846, 1998
37. Vergis A, Hindriks M, Gillquist J: Sagittal plane
translations of the knee inanterior cruciate deficient subjects and
controls. Med Sci Sports Exerc 29: 1561–1566, 1997
38. Wilk KE, Escamilla RF, Fleisig GS, et al: A comparison of
tibiofemoral jointforces and electromyographic activity during open
and closed kineticchain exercises. Am J Sports Med
24: 518–527, 1996
39. Woo SL-Y, Chan SS, Yamaji T: Biomechanics of knee ligament
healing,repair and reconstruction. J Biomech
30: 431–439, 1997
40. Yack HJ, Collins CE, Whieldon TJ: Comparison of closed and
open kineticchain exercise in the anterior cruciate
ligament-deficient knee.Am J Sports Med 21: 49–54,
1993
82 Kvist and Gillquist American Journal of Sports
Medicine
at CAPES on May 4, 2011ajs.sagepub.comDownloaded from
http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/http://ajs.sagepub.com/



























![Green Club: Yes, we ‘can’! Contributors: Anna Pastwa | Gyan Prakash | Nichlas Kvist Jørgensen Simon Overgaard | Victoria Vic [Group 4]](https://img.pdfslide.us/doc/110x75/56649e7d5503460f94b80c2c/green-club-yes-we-can-contributors-anna-pastwa-gyan-prakash-nichlas.jpg)