Embed Size (px)
Citation preview
PARATESTICULARPARATESTICULARTUMORSTUMORS
Dr. Vainrib, Urology Department
Meir Hospital
TESTICULAR TUMORSTESTICULAR TUMORS
UNCOMMON (1-2% of all UNCOMMON (1-2% of all pediatric solid tu)pediatric solid tu)
Benign>Malignant in childrenBenign>Malignant in children Incidence peaks at age 2yrs, Incidence peaks at age 2yrs,
tapers after 4yrs and rises tapers after 4yrs and rises again at pubertyagain at puberty
Rare in Asian children and Rare in Asian children and blackblack
Testicular Cancer – one of Testicular Cancer – one of the most curable solid the most curable solid neoplasmsneoplasms
TUMORS OF TESTICULAR ADNEXATUMORS OF TESTICULAR ADNEXA
PARATESTICULAR TUMORS: Rhabdomyosarcoma Leiomyosarcoma Miscellaneous Mesenchymal Tu of the Spermatic
Cord ADENOMATOID TUMORS:
Mesothelioma Cystadenoma
EPITHELIAL TUMORS
PARATESTICULAR TUMORSPARATESTICULAR TUMORS
7-10% among Primary Genitourinary Tu Occasional reports of purely testicular
mesenchymal tumor ~40% of all paratesticular tu – juvenile form of
rhabdomyosarcoma followed by leiomyosarcoma
PARATESTICULAR PARATESTICULAR RHABDOMYOSARCOMA (RMS)RHABDOMYOSARCOMA (RMS)
Peak age of presentation: 1-5yrs Location: distal portion of cord, may invade testis Clinical presentation: unilateral, painless scrotal
swelling/mass above scrotum Physical examination: firm mass, usually distinct
from the testis At Dx: 60% of paratesticular RMS – Stage I >90% of paratesticular RMS – embryonal
hystology (good prognosis)
PARATESTICULAR PARATESTICULAR RHABDOMYOSARCOMA (RMS)RHABDOMYOSARCOMA (RMS)
Evaluation: CT to evaluate retroperitoneum for node MTX
(FN rate of CT = 14%)
*** - up to 30% of patients have extension to lymph nodes
PARATESTICULAR PARATESTICULAR RHABDOMYOSARCOMARHABDOMYOSARCOMA
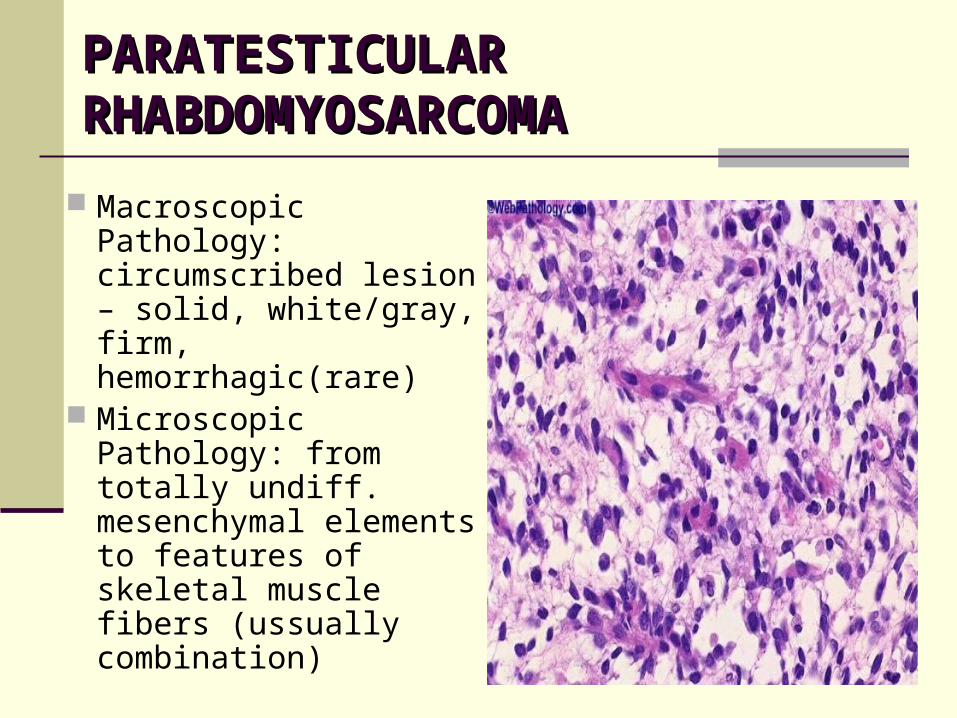
Macroscopic Pathology: circumscribed lesion – solid, white/gray, firm, hemorrhagic(rare)
Microscopic Pathology: from totally undiff. mesenchymal elements to features of skeletal muscle fibers (ussually combination)
PARATESTICULAR PARATESTICULAR RHABDOMYOSARCOMA TXRHABDOMYOSARCOMA TX Should be removed by ingiunal orchiectomy +/– RPLND Adjuvant TX:
RADIATION TX – 4000-6000cGy 5-8wks CHEMOTHERAPY:
Vincristine, Cyclophosphamide, Dactinomycin <10yrs + clinically LN-: CHEMOTHERAPY ALONE >10yrs: RPLND before CHEMOTHERAPY (50% chance
of LN involvement) and if LN+ >>> RADIATION TX Survival:
Stage I: 91% Stage II: 86% Stage III: 35% Stage IV: 5.2%
PARATESTICULAR PARATESTICULAR RHABDOMYOSARCOMARHABDOMYOSARCOMA
RPLND: controversial RPLND+:
Staging of the disease before radiation tx for involved area
AGAINST: Grossly involved LN are seen in CT Significant morbidity associated with surgery
Intestinal obstruction Ejaculatory dysfunction Edema of lower extremity
Microscopic LN disease effectively treated by chemotherapy
Diagnostic Laparoscopy - ???
CASE REPORTCASE REPORT
History: 5yrs old, healthy Occasional finding of painless lt scrotal mass Tumor markers: AFP, BHCG – negative,
LDH=mild elevation Physical examination:
Paratesticular mass in lt hemiscrotum US: paratesticular mass, w/o involvement of
testis Operation: Lt inguinal orchiectomy
CASE REPORTCASE REPORT
Pathology: Rhabdomyosarcoma Follow up: by CT of chest+abdomen
Enlarged lymph node in ext iliac LN, susp enlarged LN in subcarinal region
Referral to pediatric oncologist Mediastinal Bx: negative Chemotherapy F/U by CT: LN -
LEIOMYOSARCOMALEIOMYOSARCOMA
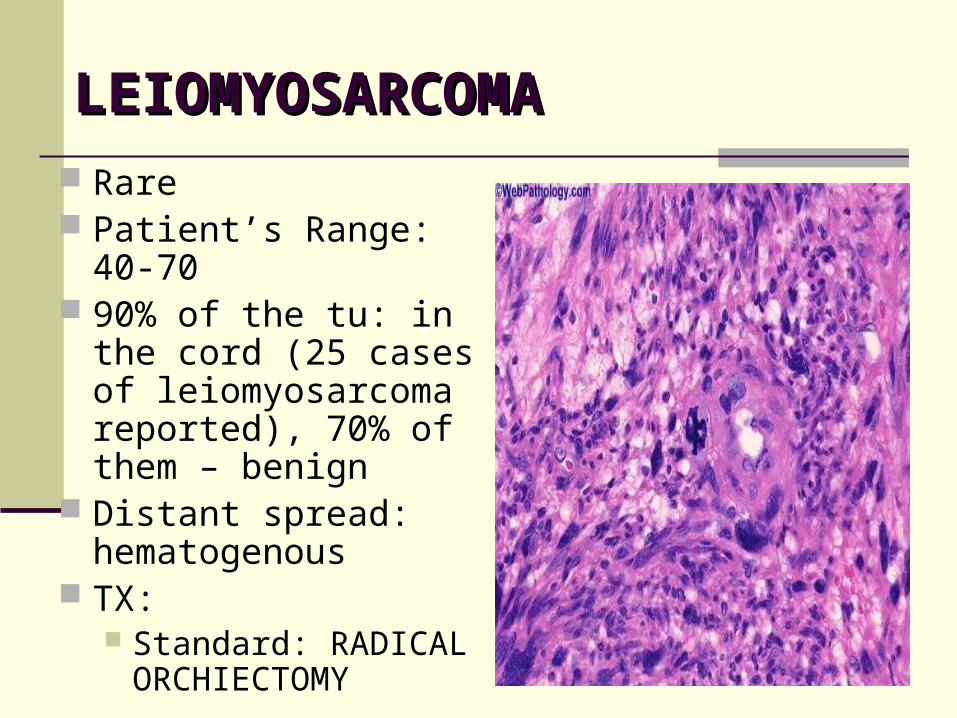
Rare Patient’s Range: 40-70 90% of the tu: in the
cord (25 cases of leiomyosarcoma reported), 70% of them – benign
Distant spread: hematogenous
TX: Standard: RADICAL
ORCHIECTOMY
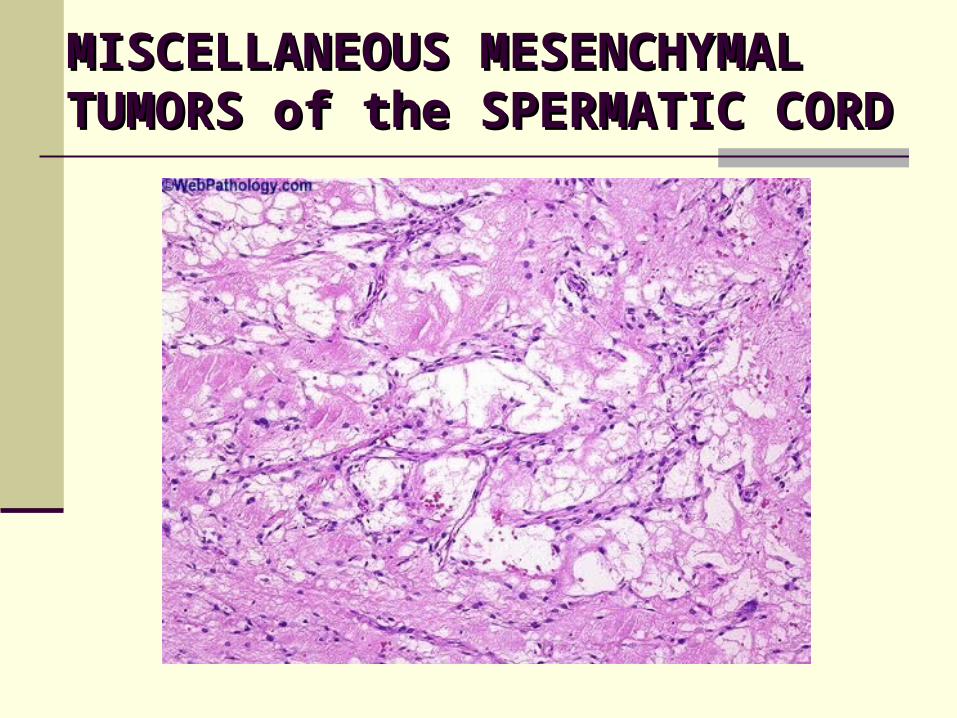
MISCELLANEOUS MISCELLANEOUS MESENCHYMAL TUMORS of the MESENCHYMAL TUMORS of the SPERMATIC CORDSPERMATIC CORD
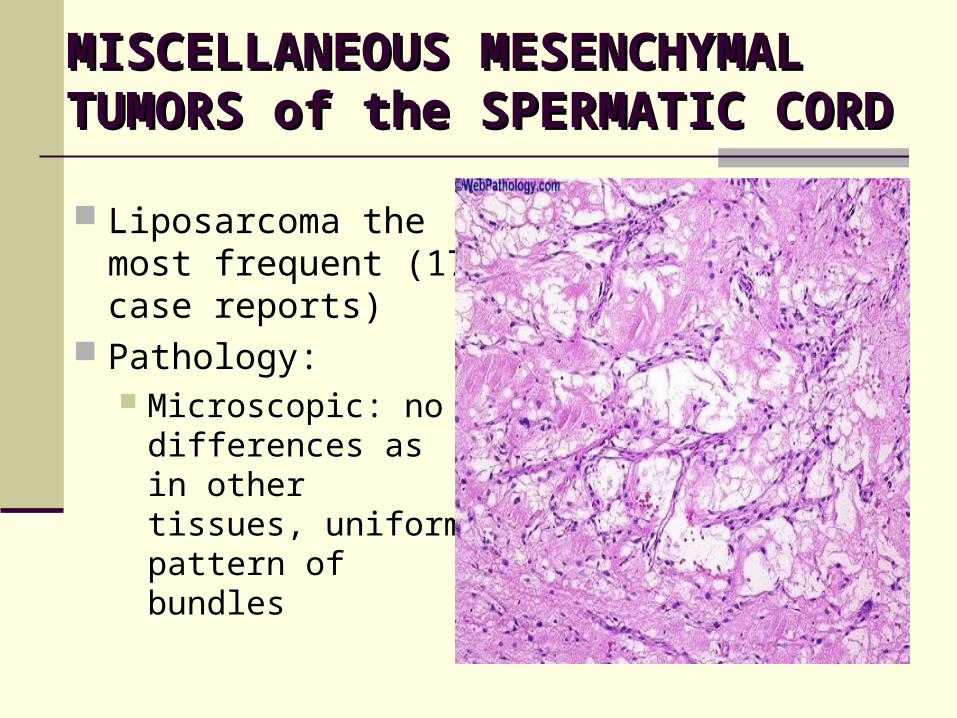
MISCELLANEOUS MISCELLANEOUS MESENCHYMAL TUMORS of the MESENCHYMAL TUMORS of the SPERMATIC CORDSPERMATIC CORD
Liposarcoma the most frequent (17 case reports)
Pathology: Microscopic: no
differences as in other tissues, uniform pattern of bundles
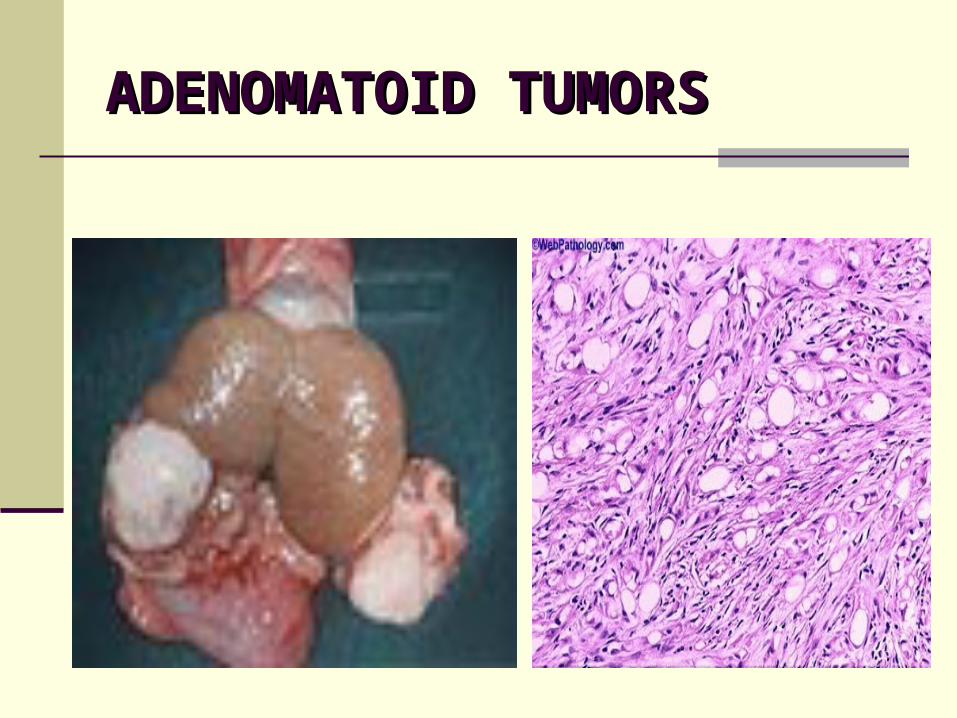
ADENOMATOID TUMORSADENOMATOID TUMORS Most common tu of paratesticular tissues (PTT) 30% of all PTT Distribution: epididymis>>tunicae>>cord Max occurance: 20-30 years old (range 20-80) Clinical appearance: small, solid, asymptomatic Occasional appearance: mild pain, discomfort The tumors ussualy attached to the tunicae Macroscopic Pathology: white, yellow or tan with
fibrous apparence Microscopic Pathology: epithelium-like cells,
fibrous stroma
ADENOMATOID TUMORSADENOMATOID TUMORS
ADENOMATOID TUMORSADENOMATOID TUMORS
Tumor origin – Unknown Tumor behavior: benign, none of the cases with
MTX, sometimes – local invasion TREATMENT: SURGICAL EXCISION
MESOTHELIOMAMESOTHELIOMA
More common in older, but maybe seen in children Clinical Presentation: firm, painless scrotal mass +/-
hydrocele (sometimes gradual enlargement of hydrocele)
15% MTX to inguinal LN or abdominal structures Macroscopic Patholoogy: poorly demarcated,
wite/yellow, intermittent firm, friable mass Microscopic Pathology: papillary&solid structures +
dense fibroconnective tissue, no mitotic activity, sometimes psammoma bodies are seen
TREATMENT: Surgical Exsicion+/- local bx if MTX are suspected
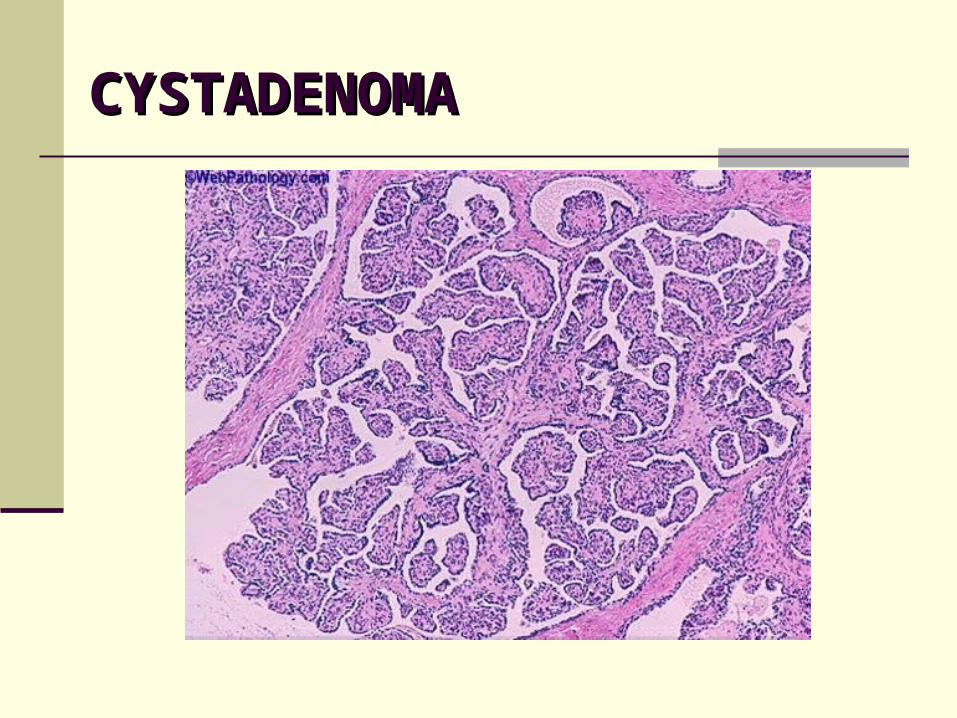
CYSTADENOMACYSTADENOMA
CYSTADENOMACYSTADENOMA Cysadenoma of the epididymis – benign epithelial
hyperplasia 20 case reports up to date (1/3 as part of von Hippel-
Lindau dis) Most often in young people Clinical Presentation: partially cystic lesion with mild
discomfort/asymptomatic Macroscopic Pathology: multicystic, encapsulated or
circumscribed Microscopic Pathology: glands&papillary structures,
Glycogen-staining cytoplasm as in RCC (DD - RCC MTX) TX: Surgical excision
CASE REPORTCASE REPORT History:
15yrs old, Talassemia major, s/p BMT failure Urological f/u of bilateral simple epididymal cysts Tumor markers: negative
Physical Examination: 2 small testis in scrotum, epididymal cysts bilateral (lt>rt), lt varicocele
US: bilateral small testes, 2 lt epididymal cysts (previousle known), rt large (9mm) epididymal cyst
Operation: Lt Epididymal Cyst Excision+Lt Low ligation of spermatic Vein
CASE REPORTCASE REPORT
Pathology: Papillary Cystadenoma of Epididymis Follow up: no evidence of varicocele, no
inflammation in scrotum
EPITHELIAL TUMORSEPITHELIAL TUMORS
Rare Epididymis and paratesticular tissues maybe
involved by extensions from 1’ germinal cell testicular tu
OVARIAN-TYPE OVARIAN-TYPE EPITHELIAL TUMORSEPITHELIAL TUMORS
Rare Location: testicular tunics or parenchyma Tumor origin:
Mullerian metaplasia of mesothelium Mullerian structures
Classification: Papillary serous tumor of low malignant potential (most) Serous carcinoma Endometrioid adenocarcinoma Benign/malignant mucinous tumors Benign/malignant Brenner tumors Clear cell carcinoma
OVARIAN-TYPE OVARIAN-TYPE EPITHELIAL TUMORSEPITHELIAL TUMORS
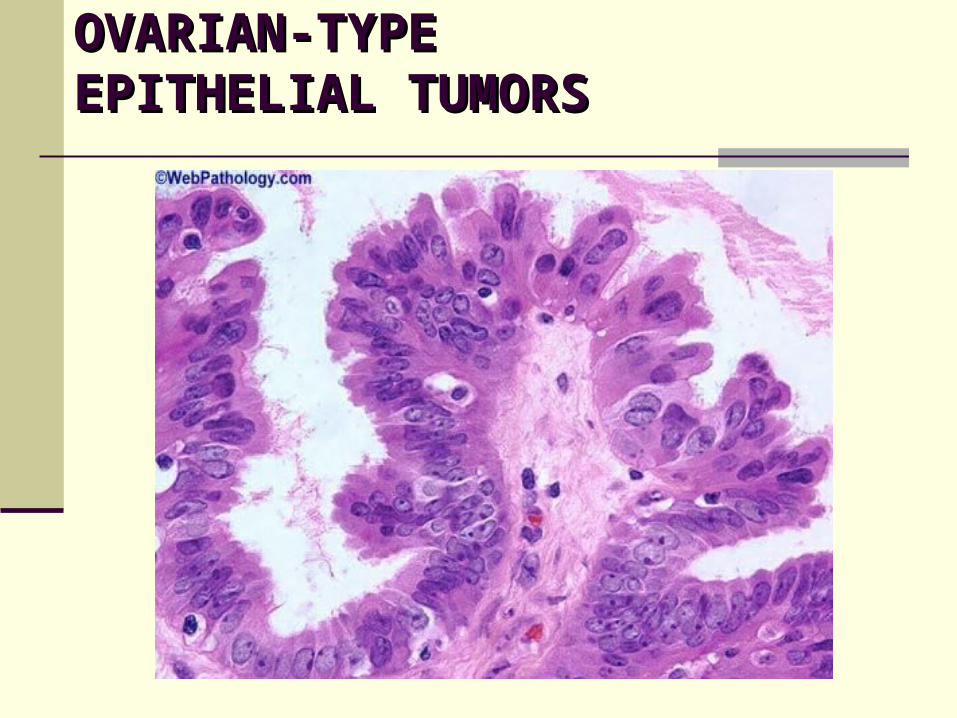
OVARIAN-TYPE OVARIAN-TYPE EPITHELIAL TUMORSEPITHELIAL TUMORS Papillary serous tumor of low malignant potential:
Paratesticular tu when involve tunica vaginalis are often accompanied by hydrocele
Pathology (DD of Mesothelioma): Single/multifocal, exophytic, papillary on tunica
vaginalis Like in ovary: arborizing pattern of epithelium,
detached buds of epithelium
Mucinous tu: same pathologic pattern as in ovary USUAL TX: RADICAL ORCHIECTOMY
CASE REPORTCASE REPORT
History: 12yrs old, usually healthy Main complaint: pain and swelling in LT testis
during 1mo prior admission to the ER Physical Examination:
Lt testis isn’t palpable because of Lt Hydrocele US in ER: Complicated Lt Hydrocele Negative markers
CASE REPORTCASE REPORT
US before Operation: Lt hydrocele with paratesticular cyst with solid papillary lesion of 10mm diameter in it
CASE REPORTCASE REPORT
Operation: Inguinal excision of paratesticular cystic lesion with hydrocele
Pathology: Papillary serous cystadenoma, borderline malignancy in tunica vaginalis
Elective admission for Radical orchiectomy Patient released after operation filling well Currently: follow up by abdominal CT