Embed Size (px)
Citation preview
Parapneumonic Effusions and Empyema
Parapneumonic Effusions and Empyema
Journal Club
Preethi Yeturu and Navneesh Sharma
February 18, 2009
Journal Club
Preethi Yeturu and Navneesh Sharma
February 18, 2009
Pleural EffusionsPleural Effusions
Abnormal accumulation of fluid in the pleural space due to a disruption of the equilibrium across pleural membranes
Normal pleural fluid clear ultrafiltrate of plasma pH 7.6 - 7.64 Protein content <2%, WBC <1000 LDH <50% of plasma LDH
Two types Transudate Exudate
Abnormal accumulation of fluid in the pleural space due to a disruption of the equilibrium across pleural membranes
Normal pleural fluid clear ultrafiltrate of plasma pH 7.6 - 7.64 Protein content <2%, WBC <1000 LDH <50% of plasma LDH
Two types Transudate Exudate
TransudateTransudate
Increased capillary hydrostatic pressure or decreased colloid oncotic pressure Pleural membranes intact Permiability of capillary membranes normal
Fluid is an ultrafiltrate of plasma Causes
CHF Cirrhosis Nephritic syndrome
Increased capillary hydrostatic pressure or decreased colloid oncotic pressure Pleural membranes intact Permiability of capillary membranes normal
Fluid is an ultrafiltrate of plasma Causes
CHF Cirrhosis Nephritic syndrome
ExudateExudate Altered permeability of pleural membranes
and capillaries or obstruction of lymphatic drainage of pleural space
Light’s criteria: one or more of following must be present Pleural fluid/serum protein >0.5 Pleural fluid/serum LDH>0.6 Pleural fluid specific gravity >1.018
Causes Parapneumonic TB Malignancy PE
Altered permeability of pleural membranes and capillaries or obstruction of lymphatic drainage of pleural space
Light’s criteria: one or more of following must be present Pleural fluid/serum protein >0.5 Pleural fluid/serum LDH>0.6 Pleural fluid specific gravity >1.018
Causes Parapneumonic TB Malignancy PE
Parapneumonic EffusionsParapneumonic Effusions
Any pleural effusion associated with bacterial pneumonia, lung abscess or bronchiectasis
Most common cause of exudative pleural effusions in US 40-60% of bacterial pneumonias result in pleural
effusions Three types
Uncomplicated parapneumonic effusion Complicated parapneumonic effusion Empyema
Any pleural effusion associated with bacterial pneumonia, lung abscess or bronchiectasis
Most common cause of exudative pleural effusions in US 40-60% of bacterial pneumonias result in pleural
effusions Three types
Uncomplicated parapneumonic effusion Complicated parapneumonic effusion Empyema
Uncomplicated EffusionsUncomplicated Effusions
Parenchymal infection leads to increased interstitial fluid that causes accumulation of sterile pleural effusion
Pleural fluid is often small (<10mm) sterile w/ small amount of PMNs glucose and pH wnl
Resolve with resolution of pneumonia and treatment w/ antibiotics
Parenchymal infection leads to increased interstitial fluid that causes accumulation of sterile pleural effusion
Pleural fluid is often small (<10mm) sterile w/ small amount of PMNs glucose and pH wnl
Resolve with resolution of pneumonia and treatment w/ antibiotics
Complicated EffusionsComplicated Effusions
Persistent bacterial infection of previously sterile pleural fluid
Pleural fluid Many PMNs, bacteria and cell debris Acidosis - pH and glucose decrease LDH increases
Possible deposition of fibrin on pleura - formation of multiple locules
Persistent bacterial infection of previously sterile pleural fluid
Pleural fluid Many PMNs, bacteria and cell debris Acidosis - pH and glucose decrease LDH increases
Possible deposition of fibrin on pleura - formation of multiple locules
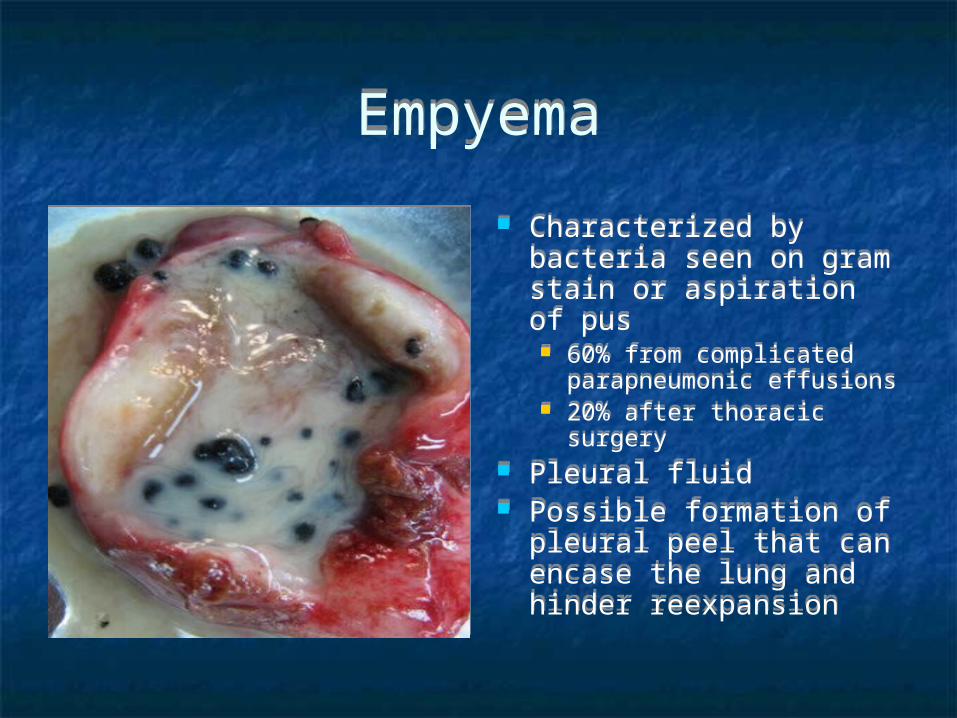
EmpyemaEmpyema
Characterized by bacteria seen on gram stain or aspiration of pus 60% from complicated
parapneumonic effusions 20% after thoracic surgery
Pleural fluid Possible formation of
pleural peel that can encase the lung and hinder reexpansion
Characterized by bacteria seen on gram stain or aspiration of pus 60% from complicated
parapneumonic effusions 20% after thoracic surgery
Pleural fluid Possible formation of
pleural peel that can encase the lung and hinder reexpansion
Clinical ManifestationsClinical Manifestations History
Acute febrile episode Dyspnea Cough - w/ purulent sputum Pleuritic chest pain Weight loss
Physical exam Dullness to percussion Diminished breath sounds in affected hemithorax Decreased tactile fremitus Egophony Pleuritic friction rub
History Acute febrile episode Dyspnea Cough - w/ purulent sputum Pleuritic chest pain Weight loss
Physical exam Dullness to percussion Diminished breath sounds in affected hemithorax Decreased tactile fremitus Egophony Pleuritic friction rub
Diagnosis - ImagingDiagnosis - Imaging
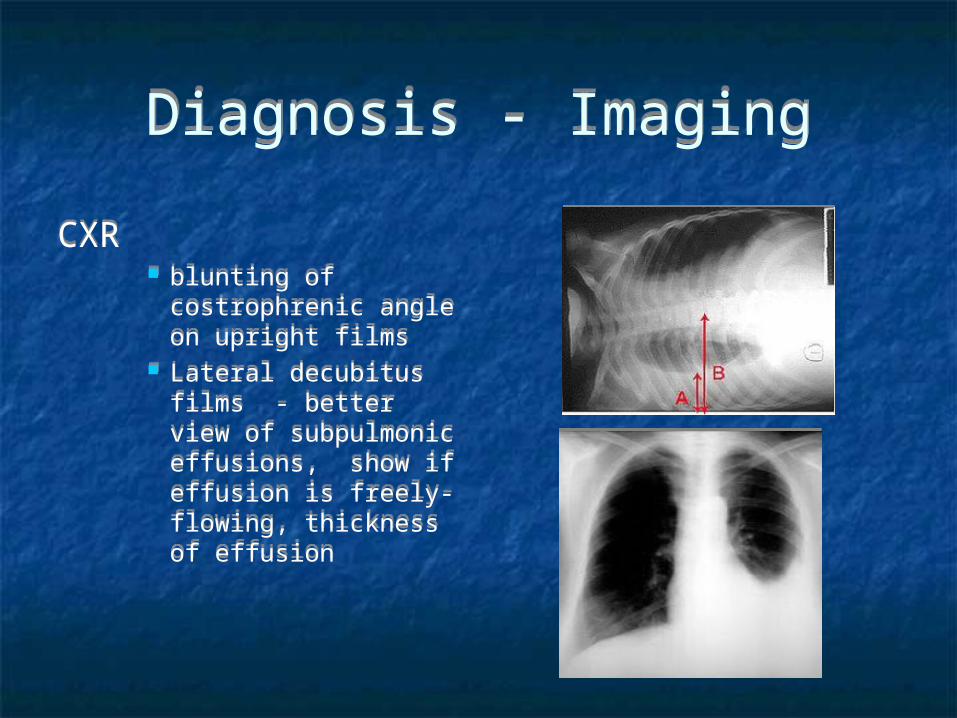
CXR blunting of
costrophrenic angle on upright films
Lateral decubitus films - better view of subpulmonic effusions, show if effusion is freely-flowing, thickness of effusion
CXR blunting of
costrophrenic angle on upright films
Lateral decubitus films - better view of subpulmonic effusions, show if effusion is freely-flowing, thickness of effusion
Diagnosis - ImagingDiagnosis - Imaging
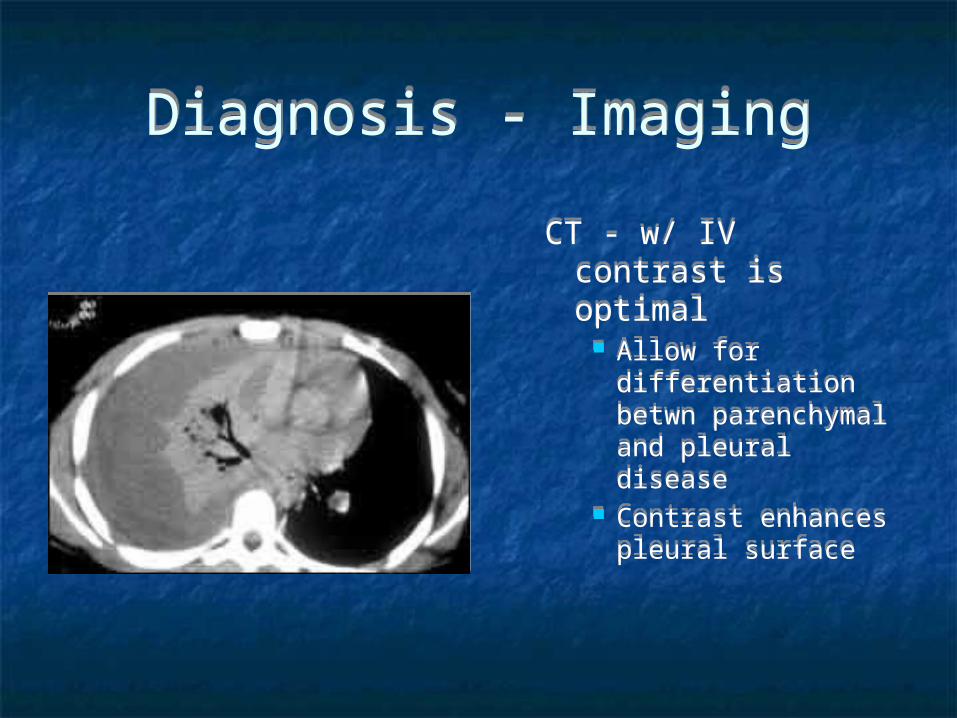
CT - w/ IV contrast is optimal
Allow for differentiation betwn parenchymal and pleural disease
Contrast enhances pleural surface
CT - w/ IV contrast is optimal
Allow for differentiation betwn parenchymal and pleural disease
Contrast enhances pleural surface
DiagnosisDiagnosis
Thoracentesis Sample if any of following are present
Free flowing but >10mm in lateral decubitus film Loculated Associated w/ thickened parietal pleura on CT - suggests
empyema Complications - pain, bleeding, pneumothorax,
puncture of liver or spleen
Thoracentesis Sample if any of following are present
Free flowing but >10mm in lateral decubitus film Loculated Associated w/ thickened parietal pleura on CT - suggests
empyema Complications - pain, bleeding, pneumothorax,
puncture of liver or spleen
Analysis of Pleural FluidAnalysis of Pleural Fluid
Gross examination for color, turbidity and odor
Microbiology - gram stain and cultures pH or glucose, LDH, protein CBC w/ differential
Gross examination for color, turbidity and odor
Microbiology - gram stain and cultures pH or glucose, LDH, protein CBC w/ differential
Analysis of Pleural FluidAnalysis of Pleural Fluid
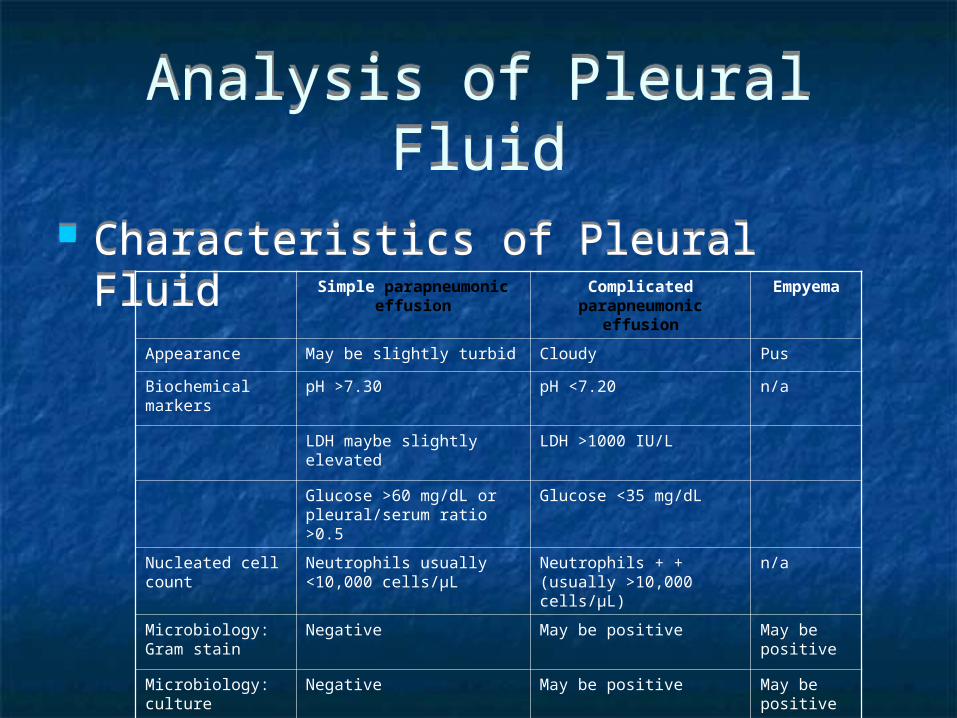
Characteristics of Pleural Fluid Characteristics of Pleural Fluid Simple parapneumonic
effusionComplicated parapneumonic
effusionEmpyema
Appearance May be slightly turbid Cloudy Pus
Biochemical markers pH >7.30 pH <7.20 n/a
LDH maybe slightly elevated LDH >1000 IU/L
Glucose >60 mg/dL or pleural/serum ratio >0.5
Glucose <35 mg/dL
Nucleated cell count Neutrophils usually <10,000 cells/μL
Neutrophils + + (usually >10,000 cells/μL)
n/a
Microbiology: Gram stain
Negative May be positive May be positive
Microbiology: culture Negative May be positive May be positive
Categories risk for poor outcomes
Categories risk for poor outcomes
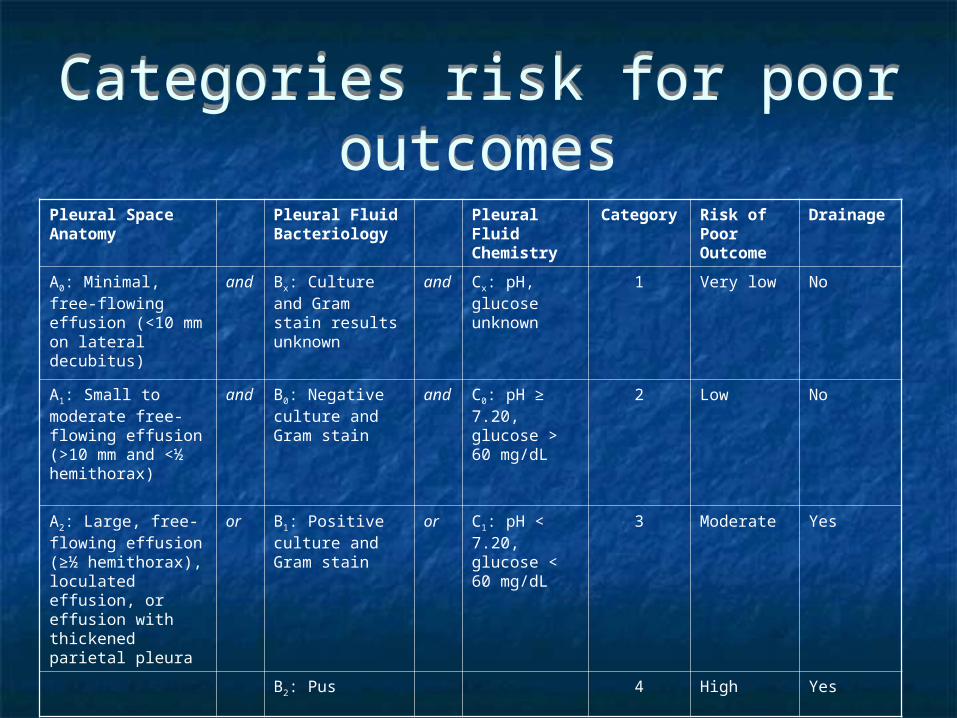
Pleural Space Anatomy
Pleural Fluid Bacteriology
Pleural Fluid Chemistry
Category Risk of Poor Outcome
Drainage
A0: Minimal, free-flowing effusion (<10 mm on lateral decubitus)
and Bx: Culture and Gram stain results unknown
and Cx: pH, glucose unknown
1 Very low No
A1: Small to moderate free-flowing effusion (>10 mm and <½ hemithorax)
and B0: Negative culture and Gram stain
and C0: pH ≥ 7.20, glucose > 60 mg/dL
2 Low No
A2: Large, free-flowing effusion (≥½ hemithorax), loculated effusion, or effusion with thickened parietal pleura
or B1: Positive culture and Gram stain
or C1: pH < 7.20, glucose < 60 mg/dL
3 Moderate Yes
B2: Pus 4 High Yes
TreatmentTreatment Depends on type and category of effusion
Uncomplicated - category 1 or 2 Resolves w/ antibiotic treatment alone Does not need drainage
Complicated - category 3 Variable response to antibiotics alone - thus often treated like
empyema Empyema - category 4
Requires complete drainage Goal of therapy:
Sterilization of cavity - antibiotics for 4-6 weeks Complete drainage as evidenced by minimal chest tube output
and CT documentation that no residual loculations persist Obliteration of empyema cavity w/ adequate lung expansion
Depends on type and category of effusion Uncomplicated - category 1 or 2
Resolves w/ antibiotic treatment alone Does not need drainage
Complicated - category 3 Variable response to antibiotics alone - thus often treated like
empyema Empyema - category 4
Requires complete drainage Goal of therapy:
Sterilization of cavity - antibiotics for 4-6 weeks Complete drainage as evidenced by minimal chest tube output
and CT documentation that no residual loculations persist Obliteration of empyema cavity w/ adequate lung expansion
Drainage of EffusionDrainage of Effusion Theurapeutic thoracentesis Tube thoracotomy
Often left until rate of drainage <50mL/day and cavity is closed W/ fibrinolytics - intrapleural administration was suggested for
loculated effusions Reported data does not demonstrate benefit in most pts
Thoracoscopy Alternative treatment for multiloculated empyema
Open thoracostomy Open drainage at inferior border of empyema cavity w/ chest
tube Preferred in pts who cannot tolerate thoracotomy
Theurapeutic thoracentesis Tube thoracotomy
Often left until rate of drainage <50mL/day and cavity is closed W/ fibrinolytics - intrapleural administration was suggested for
loculated effusions Reported data does not demonstrate benefit in most pts
Thoracoscopy Alternative treatment for multiloculated empyema
Open thoracostomy Open drainage at inferior border of empyema cavity w/ chest
tube Preferred in pts who cannot tolerate thoracotomy
Drainage of EffusionDrainage of Effusion
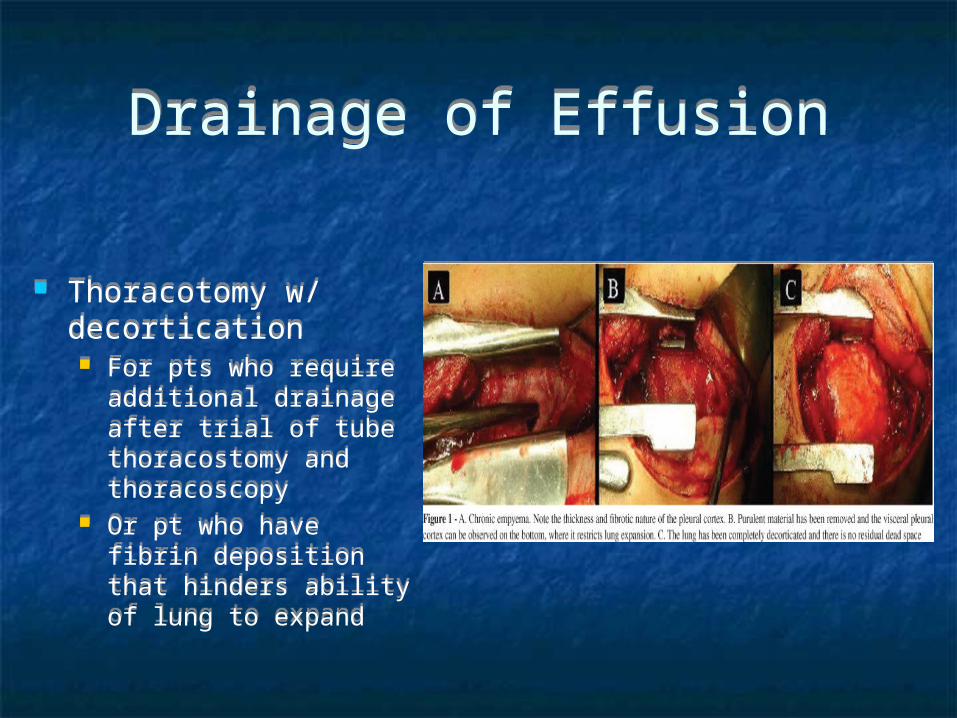
Thoracotomy w/ decortication For pts who require
additional drainage after trial of tube thoracostomy and thoracoscopy
Or pt who have fibrin deposition that hinders ability of lung to expand
Thoracotomy w/ decortication For pts who require
additional drainage after trial of tube thoracostomy and thoracoscopy
Or pt who have fibrin deposition that hinders ability of lung to expand
Thank you!!Thank you!!








![Arnab Bhadra arXiv:2003.08149v2 [q-bio.BM] 27 Jul 2020 · 2020. 7. 28. · Arnab Bhadra Computer Science and Engineering IIT Tirupati India, 517506 cs18s501@iittp.ac.in Kalidas Yeturu](https://img.pdfslide.us/doc/110x75/60b34e186326ed06121b3e77/arnab-bhadra-arxiv200308149v2-q-biobm-27-jul-2020-2020-7-28-arnab-bhadra.jpg)