Embed Size (px)
Citation preview

443In Practice October 2014 | Volume 36 | 443-452
Companion AnimalsCompanion Animals
Paraneoplastic syndromes (PNSs) can be described as the indirect effects of tumours, typically due to tumour production and release of biologically active substances such as hormones, growth factors and cytokines. PNSs are sometimes the first evidence of a neoplastic disease; therefore, knowledge of these syndromes and their associated tumour types can help in early diagnosis. PNSs should resolve with treatment of the underlying tumour and, conversely, may return with recurrence of the underlying tumour. In some cases, they cause more significant morbidity than the tumour itself, so they must be clinically addressed for proper treatment or palliation. A further issue is that signs caused by PNSs may mimic side effects of treatment such as chemotherapy, complicating clinical decision making. This article discusses the different types of PNSs and treatment options for each case.
Endocrine paraneoplastic syndromes
Hypercalcaemia of malignancyThe most common cause of hypercalcaemia in dogs is an underlying malignancy, whereas non-neoplastic causes predominate in cats. The primary mechanism is the promotion of bone resorption by osteoclasts, resulting in release of calcium into the bloodstream. The mechanism includes elaborating substances such as parathyroid hormone–related peptide (PTHrP), which shares structural homology with parathyroid hormone (PTH). PTHrP binds to the PTH receptor with an affinity equal to that of PTH, resulting in similar biological effects. Other substances that can cause hypercalcaemia of malignancy (HM) include interleukin-1β (IL-1β), transforming growth factor-β (TGF-β), and the receptor activator of nuclear factor κ-B ligand (RANκL). In dogs, HM is most commonly associated with lymphoma, apocrine gland anal sac adenocarcinoma, multiple myeloma and thymoma, but other tumour types may cause hypercalcaemia. Dogs with T cell lymphoma, and in particular those with cranial mediastinal masses (which are usually T-cell types), are most likely to develop HM. The HM associated with canine multiple myeloma is believed to be caused by increased bone resorption in the immediate proximity of neoplastic foci due to widespread, polyostotic bone lesions. HM is less common in cats, but has been associated with lymphoma and a variety of carcinomas.
HM can have significant deleterious effects on the kidneys, due to altered renal blood flow and mineralisation. The distal tubules become less responsive to antidiuretic hormone (ADH), leading to polyuria and polydipsia (PUPD). Dogs with HM are far more frequently azotaemic than those with primary hyperparathyroidism.
PUPD is one of the most overt and important clinical indicators of hypercalcaemia. Other common signs of hypercalcaemia include inappetence or anorexia, weight
loss, weakness and vomiting. Bradycardia, obtundation, twitching and shaking can occur with severe and persistent calcium elevations. Cats experience less PUPD and gastrointestinal signs than dogs and about 25 per cent of cats with hypercalcaemia show signs associated with calcium oxalate urolithiasis. Diagnostic evaluation should include assaying serum-ionised calcium concentrations, as this is the biologically active fraction. This can be done using routinely available ‘bedside’ analysers, such as the iSTAT. If the ionised calcium is increased, serum may then be submitted for measurement of phosphorus, PTH, and PTHrP concentrations. Typically, dogs and cats with HM have increased serum-ionised calcium, normal or low serum phosphorus, low PTH, and increased PTHrP concentrations. Useful diagnostic steps include a thorough physical examination that includes rectal palpation (to identify anal sac masses), a complete blood count (to identify cytopenias and atypical circulating lymphoma or leukaemic cells), serum biochemical profile, urinalysis, and imaging of the thorax and abdomen. Thoracic radiographs are paramount given that a very large proportion of animals with HM will have mediastinal lymphoma, and they are also used to identify thymomas. Abdominal ultrasound is required as opposed to plain radiography because of the low sensitivity of the latter for detection of lesions, specifically lymphoma.
If an animal with hypercalcaemia is unwell, then imaging should be performed as a priority rather than waiting for analysis of ionised calcium (if not readily available in the practice), and PTH and PTHrP, as HM is a more likely differential in these cases. Also, analysis of PTH and PTHrP takes time, which may be of major clinical significance, particularly in lymphoma patients where time is of the essence.
Therapy for HM should be focused on re-establishing normal calcium levels and treating the underlying malignancy.
James Elliott qualified from the University of Edinburgh. After a period in general practice, he became an intern and then a resident in oncology at the University of Liverpool, where he subsequently became a lecturer. He is an European and RCVS recognised specialist in veterinary oncology. He currently works as an oncologist at Willows Referral Service.
Paraneoplastic syndromes in dogs and cats
James Elliott
doi:10.1136/inp.g5826
Elliott .indd 443 02/10/2014 16:36
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from

444 In Practice October 2014 | Volume 36 | 443-452
Companion AnimalsCompanion Animals
Treating hypercalcaemia due to lymphoma or aggressive lymphoid cancersThe majority of animals that require acute or emergency treatment of HM, including those that are feeling unwell, typically have a lymphoproliferative disease, such as lymphoma (almost always T-cell) or leukaemia. Animals with azotaemia, significant clinical illness related to their hypercalcaemia, or those with a marked increase in calcium should be hospitalised and treated with aggressive fluid diuresis (eg, three times the maintenance levels, unless there are contraindications), preferably using a calcium-free intravenous fluid such as 0.9 per cent saline, but Hartmann’s solution is also acceptable. Salmon calcitonin injections can be useful and the author has found this very useful for helping to reduce serum calcium levels in lymphoma patients in the short term. Furosemide can be used to promote calciuresis once hydration is re-established, but this is probably best avoided for the initial 12 to 24 hours. Prednisone will decrease serum calcium, but should be reserved for cases in which the diagnosis has been established, to avoid masking the diagnosis and potentially reducing the efficacy of future chemotherapy. Induction chemotherapy should be started as soon as a diagnosis is achieved, which is why ill patients with hypercalcaemia should be diagnostically evaluated as soon as possible.
Treating hyperglycaemia due to anal sac apocrine gland carcinoma or other solid tumoursPatients with hyperglycaemia associated with anal sac apocrine gland carcinomas or other solid tumours tend to be less of an emergency and, in the author’s experience, are often clinically well, unless very advanced or metastatic disease is present. These patients can therefore typically be managed as outpatients, unless their clinical status dictates otherwise. As with other cases of HM, treatment of the underlying cause is the initial treatment of choice. This may involve, for example, surgical removal of the primary perianal mass and any metastatic sublumbar lymph nodes. Masses that are surgically excisable should be removed and this may reverse the HM. Recurrence of HM typically signifies a return of the tumour and/or metastasis. A significant number of dogs with anal sac carcinoma have metastatic lymph nodes (usually medial iliac) at initial presentation, and these should be evaluated before surgical removal of the primary tumour, otherwise there may not be restoration of normocalcaemia.
In some cases where owners decline surgery or the disease is too advanced or inoperable, medical therapy of HM may be required, either as the sole therapy or in addition to palliative anti-cancer therapy. This can still be successful for a meaningful period in patients with anal sac carcinoma as, in many cases, the tumour itself progresses slowly. In this context, the author’s first line treatment of HM is prednisolone, and this appears to be safe in conjunction with chemotherapy or tyrosine kinase inhibitors. Doses typically start at 1 to 2 mg/kg (or 20 to 40 mg/m2, depending on the size of dog and the severity of corticosteroid adverse effects), reducing to the lowest effective dose as maintenance. Doses may need to be periodically increased as the tumour may secrete more PTHrP or other HM-promoting factors as it progresses. In cases that are corticosteroid-refractory, that require steroid-sparing measures or are intolerant to corticosteroids, then the author has had some success with the bisphosphonate pamidronate (Aredia; Ciba) at a dose of 1 to 2 mg/kg, administered intravenously in 0.9 per cent saline (not calcium-containing fluids) over two hours every two to three weeks. Zoledronate may also be
used. While oral bisphosphonates are available, they have a very low oral bioavailability and are significantly less potent. They can also cause more gastrointestinal upset (eg, oesophagitis). However, they may be worth trying in cases where alternatives are not possible for financial or logistical reasons.
Ultimately, effective treatment of the underlying malignancy is essential for sustained resolution of HM.
HypoglycaemiaHypoglycaemia, particularly severe and symptomatic, is most commonly associated with insulinoma. However, it can also occur secondary to intestinal smooth-muscle tumours, hepatocellular carcinoma and lymphoma. Tumour production of insulin, insulin-like growth factor 1 (IGF1) and insulin-like growth factor 2 (IGF2), and somatomedins have all been implicated. In addition, upregulation of insulin receptors, decreased glycogenolysis or gluconeogenesis, excess tumour utilisation of glucose, and binding of insulin by M proteins in myeloma may contribute to paraneoplastic hypoglycaemia.
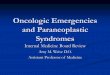
Ideally, hypoglycaemia is treated via surgical removal of the neoplasm; however, management before surgery may be necessary. In an emergency situation, intravenous glucose products may be required, but only in a strictly controlled hospitalised environment as there is a possible risk of rebound hypoglycaemia, particularly in insulinoma, where intravenous glucose can stimulate a surge of insulin release (Fig 1). If emergency management is needed at home, owners can apply honey or Glucogel to their pet’s gums and then follow this with solid food containing complex carbohydrates. In insulinoma cases, resolution of hypoglycaemia for a period of time is the norm with surgery, but it invariably recurs. When insulinomas are unresectable or the tumour recurs, medical management of hypoglycaemia with dietary and pharmacological intervention (eg, prednisone, diazoxide or glucagon) may reduce the severity of clinical signs.
Ectopic adrenocorticotropic hormone syndromeAlthough reported with a number of malignancies in people, ectopic production of adrenocorticotropic hormone (ACTH) is extremely rare in animals. It has been reported in patients with an abdominal neuroendocrine tumour, hepatic carcinoid tumours, and in dogs with primary lung tumours, but it has not, to the author’s knowledge, been reported in cats. Clinical signs can resolve with surgical removal of the primary tumour.
Syndrome of inappropriate ADH secretionSyndrome of inappropriate ADH secretion (SIADH) is characterised by hyponatraemia, serum hypo-osmolality, and urine hyper-osmolality in the absence of renal or adrenal dysfunction. Although widely recognised in humans, it has not been reported in animals. Symptoms in people relate to the effects of hyponatraemia on the CNS. Drug-related SIADH can also occur.
HyperoestrogenismThe most common neoplastic cause of hyperoestrogenism is the presence of a Sertoli cell tumour. As well as a possible mass, signs include non-pruritic symmetrical alopecia, hyperpigmentation, gynaecomastia, a pendulous prepuce, and a symmetrically enlarged prostate. Owners of male dogs with this condition have observed that their dog will attract intact male dogs and may start to squat to urinate. Hyperoestrogenism results in bone marrow suppression
Elliott .indd 444 02/10/2014 16:36
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from

447In Practice October 2014 | Volume 36 | 443-452
Companion AnimalsCompanion Animals
and resultant pancytopenia with subsequent signs of anaemia and/or neutropenia and/or thrombocytopenia. Haematology will demonstrate any cytopenias, and bone marrow biopsy reveals hypocellularity. Effective treatment relies on surgical excision of the tumour. Preoperative supportive care of animals with pancytopenia should include administration of broad-spectrum antibiotics for neutropenia and blood or red cell transfusions as required. There is a significant surgical risk due to bleeding diathesis and anaemia. Once surgically removed, bone marrow may take weeks to months to recover. In the author’s experience, clinical recovery from severe pancytopenia is rare and the prognosis is very poor.
Haematological paraneoplastic syndromesAnaemiaAnaemia is one of the most common PNSs in dogs and cats, occurring with a wide variety of tumours and mechanisms, such as blood loss and haemolysis.
For blood-loss anaemia to be considered paraneoplastic, it must occur distant from the primary tumour. Examples include blood loss due to gastrointestinal ulceration that occurs with mast cell tumours (due to histamine release) and gastrinomas (due to gastrin secretion). This type of anaemia is usually regenerative early in the course of the disease, but later becomes non-regenerative, microcytic, and hypochromic due to iron-deficiency. Treatment is by eradication of the primary tumour and supportive measures, including gastrointestinal protectants.
Bone marrow infiltration and myelophthisis (eg, with lymphoma, leukaemia, myeloma and histiocytic sarcoma) can lead to decreased red blood cell production and resultant anaemia, but some clinicians do not consider this truly paraneoplastic. However, cytopenias are not just the result of ‘over-crowding’ of normal haematopoietic tissue, and neoplastic cells can release cytokines which suppress myelopoiesis.
Anaemia of chronic disease (ACD) occurs with many different neoplastic diseases. It is typically very mild, and is characterised as normocytic, normochromic and non-regenerative. The exact cause is unknown, but it may be partly due to abnormal iron metabolism. Resolution can be anticipated once the primary tumour is addressed, although ACD may persist if aggressive treatment such as chemotherapy is undertaken.
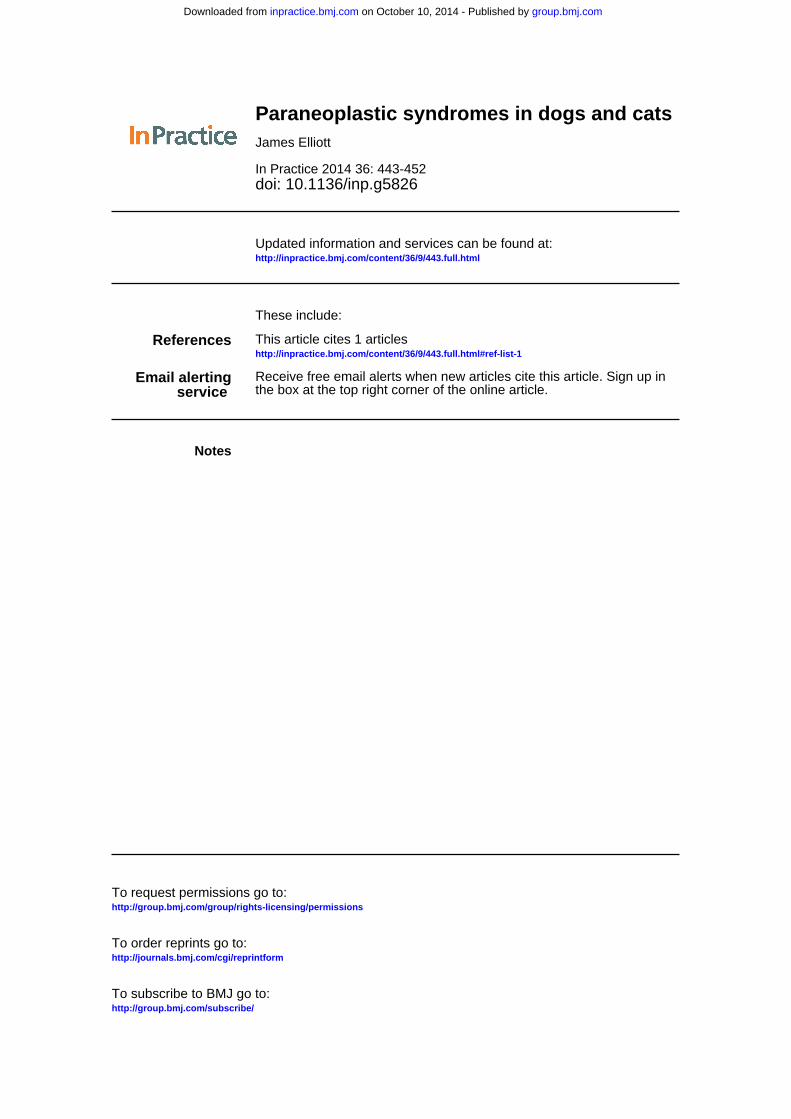
Immune-mediated haemolytic anaemia (IMHA) can occur as a PNS associated with haematopoietic and (rarely) solid tumours. It is a secondary IMHA, in which antibodies directed against tumour-associated antigens cross-react with erythrocytes. The anaemia can be acute or chronic, mild or severe. Clinical signs include lethargy, weakness, tachycardia, pallor, icterus, hepatosplenomegaly, haemoglobinuria and anorexia, depending on the severity of the anaemia and how acutely haemolysis occurs. Diagnostic tests may include identification of spherocytes (Fig 2), other signs of haemolysis, or a positive Coombs’ test. Drugs used in the treatment of primary IMHA, including corticosteroids, azathioprine, ciclosporin, mycophenolate, intravenous γ-globulin and liposome-encapsulated clodronate, have not been fully assessed for their value in treating secondary IMHA. Optimal therapy requires elimination of the underlying malignancy as the most important factor, although specific treatment with one or more of the above agents may be necessary.
Microangiopathic haemolytic anaemia is erythrocyte fragmentation resulting from intravascular fibrin formed in disseminated intravascular coagulation (DIC). It may be a result of other causes, such as abnormal vascularity within a tumour. It is most often associated with the vascular splenic haemangiosarcoma (HSA), but can occur with any tumour that leads to DIC. Resolution of the underlying malignancy is considered the only effective treatment.
ThrombocytopeniaThrombocytopenia occurs as a PNS with a wide range of tumours, most commonly lymphoma, HSA and melanoma. Mechanisms include increased platelet utilisation, platelet destruction, or decreased platelet production. Platelet counts are significantly lower in dogs with HSA that present with a splenic mass and haemoabdomen, compared to dogs with non-HSA. As with anaemia, immune-mediated destruction of platelets can be seen with lymphoma or multiple myeloma, and decreased platelet production can occur secondary to myelophthisis induced by marrow-infiltrating malignancies. Clinical signs are typically not evident until platelet counts decrease below 30 x 109/litre, when findings may include petechiation and haemorrhage. Interestingly, however, with severe thrombocytopenia in canine lymphoma patients, spontaneous haemorrhage appears to be unusual. Treatment varies depending upon the severity of the thrombocytopenia and the underlying cause, although resolution of the primary tumour is the ideal outcome. Fresh whole blood may be indicated before surgery, or red cell transfusion may be required if secondary significant anaemia has ensued. In the case of immune-mediated thrombocytopenia (ITP), immunosuppressive drugs may be required along with chemotherapy to treat the tumour.
ErythrocytosisErythrocytosis (or polycythaemia) is an uncommon PNS that is most often associated with renal cancer, although various other neoplasms have been implicated. It is a form of secondary erythrocytosis in which the underlying mechanism is an increased level of erythropoietin (EPO),
Fig 1: Intravenous glucose products may be required in the treatment of hypoglycaemia associated with a tumour. These should only be given in a strictly controlled hospital environment, as there is a risk of rebound hypoglycaemia
Elliott .indd 447 02/10/2014 16:37
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from

448 In Practice October 2014 | Volume 36 | 443-452
Companion AnimalsCompanion Animals
rather than a bone marrow disorder. EPO may be produced ectopically by the tumour itself, or it may be produced in excess by the kidney, either in direct response to renal hypoxia caused by tumour compression or through the action of hypoxia-inducible transcription factors, which stimulate EPO production.
Clinical findings include erythema of the mucous membranes, polydipsia, and neurologic signs such as disorientation, ataxia, and seizures secondary to hyperviscosity or hypervolaemia. Polycythaemia is readily apparent on haematology. Subsequent diagnostics include chemistry profile, thoracic radiographs and abdominal ultrasound, arterial blood gas, echocardiography and possibly measurement of serum EPO concentrations. As primary and secondary polycythaemias are principally classified based on EPO levels, it would appear that measurement of serum EPO concentration may be helpful, but only an increased EPO value is helpful clinically. Although an increased serum EPO level is diagnostic for secondary polycythaemia, a low or normal serum EPO value can also be found in animals with secondary polycythaemia. Contrary to popular belief, examination of bone marrow aspirates and core biopsy cannot distinguish causes of primary and secondary polycythaemia, and hence is generally not helpful. In either case, erythroid hyperplasia with complete maturation is observed.
The presence of a renal mass with concurrent erythrocytosis is, in the author’s opinion, sufficient evidence of paraneoplastic polycythaemia, such that additional diagnostics are rarely necessary, other than staging of the tumour. Nephrectomy is generally effective in resolving paraneoplastic polycythaemia related to renal neoplasia, provided that metastasis has not yet occurred, although medical management may be required initially. For other aetiologies, hydroxyurea, phlebotomy and treatment of the underlying cause are the cornerstones of therapy.
Neutrophilic leukocytosisAn increase in the number of mature neutrophils in the absence of infection or leukaemia and has been reported in various histologies. The underlying aetiology is tumour
production of colony-stimulating factors (CSFs). It is usually an incidental finding and should resolve with successful treatment of the underlying tumour. The elevation in neutrophil count can be very marked.
EosinophiliaParaneoplastic eosinophilia is a rare manifestation of cancer, but seems to primarily occur in cases of T-cell lymphoma and mast cell tumours (MCTs), due to tumour production of IL-5. However, it is insensitive and non-specific for the diagnosis of neoplasia.
ThrombocytosisThrombocytosis may be an incidental finding in dogs and cats with neoplastic disease, but it is rarely of clinical concern, and the aetiology is unknown. Although thrombocytosis theoretically puts animals at risk of thrombotic events, these appear to be extremely rare. The diagnosis is one of exclusion, once other causes have been excluded. Treatment is generally not necessary, although resolution of the underlying malignancy can be expected to cause a normalisation of the platelet count.
Platelet hyperactivity and hypercoagulabilityChanges in platelet function have been demonstrated in dogs with cancer. Mechanisms may include an increase in serum factors that induce platelet aggregation, a change in the lipid composition of plasma membranes, and an increase in the number of newer platelets that have a higher activity. It is of clinical relevance in that it may predispose affected animals to thromboembolism.
Disseminated intravascular coagulationDIC is a clinical alteration of coagulation frequently seen in dogs and cats with cancer. The cancers most often implicated are HSA, mammary carcinoma and lung carcinoma, but various others have been implicated. Interestingly, the incidence of DIC in dogs with haematopoietic malignancies appears to be less than that seen in people, with DIC predominating in solid canine malignancies. Animals with paraneoplastic DIC have a poor prognosis, unless the underlying tumour can be completely eradicated.
HyperglobulinaemiaHyperglobulinaemia occurs most commonly in association with multiple myeloma, although other neoplastic diseases (typically lymphoid), including lymphoma, chronic lymphocytic leukaemia and plasmacytoma are also reported causes. The mechanism is excess production of monoclonal (or, rarely, bi- or oligoclonal) immunoglobulins by plasma cells or neoplastic lymphocytes. Most animals with multiple myeloma have an IgG or IgA monoclonal gammopathy. Production of normal immunoglobulins may be inhibited, leading to infections (so called ‘immune cripples’). Other significant clinical sequelae may include hyperviscosity syndrome and associated hypertension and tissue hypoxia. Related clinical findings, such as cardiomegaly, renal failure, ocular disorders including retinopathies and papilloedema, and various neurologic abnormalities may develop, and these are the primary concern of owners. Bleeding tendencies are also common with hyperglobulinaemia and relate to decreased adhesion of platelets to damaged endothelial surfaces, coating of platelets with immunoglobulins, and release of platelet factor 3. Confirmation of paraneoplastic hyperglobulinaemia is via serum or urine electrophoresis, where a monoclonal gammopathy indicates a likely neoplastic cause and a polyclonal gammopathy indicates
Fig 2: Identification of spherocytes can be used as a diagnostic test of immune-mediated haemolytic anaemia
Elliott .indd 448 02/10/2014 16:37
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from

451In Practice October 2014 | Volume 36 | 443-452
Companion AnimalsCompanion Animals
a likely infectious or inflammatory cause. Successful treatment relies on resolution of the underlying tumour, usually with chemotherapy in the case of myeloma or lymphoma. Plasmapheresis may be necessary for patients with serum hyperviscosity.
Cutaneous paraneoplastic syndromesFeline paraneoplastic alopeciaA unique PNS of alopecia occurs in some cats with pancreatic and biliary carcinoma. The underlying mechanism is unclear, but an association with Malassezia species yeast has been suggested and leads to pruritus. Acute, progressive, non-pruritic symmetrical alopecia occurs, with lesions characterised by easily epilated hair and underlying smooth, shiny skin. Resolution has been reported after removal of the primary pancreatic mass, with recurrence coinciding with developing metastases.
Superficial necrolytic dermatitisSuperficial necrolytic dermatitis (SND) is a rare PNS mainly associated with glucagonoma in dogs and pancreatic carcinoma in cats, although it has been reported with insulinoma. SND caused by hepatopathy, often with a history of phenobarbital therapy is more common, hence the term hepatocutaneous syndrome. Other terms previously used to describe this disorder are necrolytic migratory erythema (NME), metabolic epidermal necrosis, and diabetic dermatopathy. Hypoaminoacidaemia is a characteristic feature and may be central to the aetiology. The cutaneous lesions are characterised by erythema, crusting, exudation, ulceration, and non-pruritic alopecia. Lesions affect the face, anogenital region, and pressure points on the trunk and extremities. The footpads are also often affected, with severe crusting, fissures, ulceration, and secondary infections with yeast, bacteria or dermatophytes. There are reported classical histological findings. Although not entirely understood, plasma amino acid concentrations are typically markedly decreased in affected dogs. Dogs and cats with paraneoplastic SND have a guarded to poor prognosis, depending on the severity of their underlying neoplastic disease. Surgical removal of pancreatic tumours has been associated with resolution of SND, as has administration of somatostatin analogues.
Nodular dermatofibrosisNodular dermatofibrosis is a rare cutaneous PNS affecting dogs, typically German shepherd dogs, that have bilateral renal cystadenocarcinoma. The genetic mutation associated with this disorder has been mapped to exon 7 of the Birt-Hogg-Dubé locus of canine chromosome 5. It is characterised by small, firm skin nodules located in the subcutaneous tissues of the limbs and head. The nodules are composed of well-differentiated, densely packed collagen. Uterine leiomyomas may occur in a large percentage of affected intact females. Given the progressive nature of the disease and the degree of renal impairment that can occur with bilateral disease, the overall prognosis for affected dogs is poor.
Gastrointestinal paraneoplastic syndromesCancer cachexiaCancer cachexia is a complex syndrome that includes weight loss and loss of lean body mass with or without anorexia. It is not very common in veterinary practice and, indeed canine cancer patients are more likely to be overweight than cachectic; however, cats may be more
affected. Cancer cachexia appears to be more often associated with lymphoma than with solid tumours in dogs and cats.
Metabolic alterations are complex with altered cytokine profiles, hyperlactataemia, and changes in responsiveness to insulin. Clinical signs include weight loss, reduced fat mass, and muscle wasting, often despite a good appetite. In addition to treatment of the underlying malignancy, aggressive nutritional support is necessary, via an enteral route if possible. Attention should be paid to conditions related to the primary tumour or its treatment which may affect food intake. In truly cachectic cancer patients, foods high in fat (including polyunsaturated omega-3 fatty acids) and low in carbohydrates have been recommended, although dietary modification must be tailored to each individual cancer patient.
Gastrointestinal ulcerationParaneoplastic gastrointestinal ulceration occurs indirectly as a result of an ulcerogenic substance being released from the primary tumour. Examples include release of histamine from an MCT and gastrin from a gastrinoma. Both substances bind to receptors on the parietal cells and stimulate increased gastric acid secretion and subsequent gastrointestinal ulceration. Therapy is aimed at resolution of the primary tumour and treatment for gastrointestinal ulceration with proton-pump inhibitors, H2-receptor blockers and sucralfate.
Neurological paraneoplastic syndromes Myasthenia gravisMyasthenia gravis (MG) is an uncommon PNS that most often occurs with thymoma, but has also been reported with other tumours. The cause of paraneoplastic MG is production of antibodies to the nicotinic acetylcholine receptors (AChRs) by the tumour. A rare disorder of MG development after thymectomy for thymoma has also been described. Clinical signs include muscle weakness, dysphagia, regurgitation, and aspiration pneumonia secondary to megaoesophagus. Diagnosis is aided by detection of circulating auto-antibodies against the AchR or by the edrophonium (tensilon) test and electromyography with repetitive nerve stimulation. Anticholinesterase agents such as pyridostigmine bromide may improve signs of muscle weakness. Use of immunosuppressive agents such as prednisone is controversial, and may be contraindicated if aspiration pneumonia is present. Elevating food and water bowls may decrease the risk of aspiration with megaoesophagus. When feasible, resection of the primary tumour is recommended and may eliminate clinical signs. However, owners must be forewarned that MG may not resolve and may require specific therapy longer term.
Peripheral neuropathyPeripheral neuropathy is associated with several tumour types in dogs, including lymphoma, multiple myeloma, insulinoma, and various carcinomas and sarcomas. The likely aetiology is production of antibodies targeting antigens that are shared between the tumour and the peripheral nerves. This PNS is characterised by focal or whole-body weakness. Electromyography and motor-nerve conduction studies are helpful in confirming the diagnosis. This may be difficult to distinguish from drug-induced neuropathy, a rare adverse effect associated with the use of some chemotherapeutic agents, such as vincristine.
Elliott .indd 451 02/10/2014 16:38
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from

452 In Practice October 2014 | Volume 36 | 443-452
Companion Animals
Renal paraneoplastic syndromesGlomerulonephritis and nephropathy Glomerular disorders may occur in cancer patients secondary to tumour-related immune complexes being deposited in the renal glomeruli. As such, neoplasia should be considered in the differential diagnosis list for dogs and cats that have protein-losing renal disease. Treatment involves elimination of the underlying tumour, with careful attention to fl uid and electrolyte needs and avoidance of drugs that may exacerbate renal damage. Therapy for proteinuria may involve ACE inhibitors.
Other paraneoplastic syndromesHypertrophic osteopathyHypertrophic osteopathy (HO) is a well-characterised PNS that is uncommon in dogs and is rarely seen in cats. It is most often associated with primary intrathoracic masses, although non-neoplastic space-occupying lesions within the thoracic or abdominal cavities, including abscesses and granulomas, foreign bodies and parasites, may induce HO. The disorder is characterised by progressive periosteal proliferation along the shafts of long bones of distal extremities and occasionally along other bones of the appendicular skeleton. The aetiology is not completely understood, but one mechanism is thought to involve stimulation of the vagus nerve, resulting in increased blood fl ow to the distal extremities. Resolution of signs in some patients following vagotomy supports this hypothesis. Presenting complaints include shifting leg lameness or reluctance to move, and affected limbs are typically warm and can be oedematous. Radiographs of the affected limbs
reveal a characteristic periosteal reaction. Successful treatment of the primary mass should lead to resolution of HO. When this is not feasible, pain management with anti-infl ammatory doses of steroids or NSAIDs is advised. Vagotomy may lead to resolution of HO, but is not commonly employed in the management of HO in dogs, because of the poor prognosis associated with an unresectable primary tumour.
FeverTrue paraneoplastic fever occurs secondary to release of pyrogenic cytokines, either by the tumour or by the host immune response to the tumour, which act as endogenous pyrogens on the thermoregulatory centre of the anterior hypothalamus. Therapy is dependent upon the underlying cause of the fever, although symptomatic therapy with NSAIDs or paracetamol may provide some palliation if the underlying cancer cannot be eliminated.
ConclusionUltimately, the recognition of PNSs may lead to the more timely diagnosis and treatment of neoplastic disorders and may help optimise therapy. An understanding of the aetiology and pathogenesis of these disorders can lead to an improved patient approach and better care of the whole patient.
Further readingBERGMAN, P. (2013) Paraneoplastic syndromes. In Withrow & MacEwen’s Small Animal Clinical Oncology. 5th edn. pp 83-92HENRY, C. (2010) Paraneoplastic syndromes. In Textbook of Veterinary Internal Medicine. 7th edn, vol 2. pp 2213-2218
Elliott .indd 452 02/10/2014 16:38
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from
doi: 10.1136/inp.g5826 2014 36: 443-452In Practice
James Elliott Paraneoplastic syndromes in dogs and cats
http://inpractice.bmj.com/content/36/9/443.full.htmlUpdated information and services can be found at:
These include:
References http://inpractice.bmj.com/content/36/9/443.full.html#ref-list-1
This article cites 1 articles
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 10, 2014 - Published by inpractice.bmj.comDownloaded from