Embed Size (px)
Citation preview

PAPRSB IHS
UBD
PeriOperative Nursing
18th Jan 2011

Objectives
Describe the issues that effect safety in
the OR
Discuss the process for creating an OR
safety program
Identify barriers to the implementation of
a safety program

What Are Adverse Events?
Pt incidents such as:
Patient falls
Medication errors
Surgical / Medical errors
Close calls (intercepted or resulted in no harm)

What Is A Sentinel Event?
-Death or permanent loss of function resulting from a medication or other Rx error
-Surgery on the wrong patient or body part
-Unintended retained surgical object
-Hemolytic transfusion reaction
-Unanticipated death resulting from an health care-acquired infection

What Is An Intentional Unsafe Act?
An adverse event that results from: criminal act purposefully unsafe act alcohol or substance abuse impaired provider/staff alleged patient abuse
Intentional unsafe acts should be reported to the In Charge & Management immediately
Intentional Unsafe Acts are investigated by administration

Safe Site Surgery
Performance of:
The correct procedure;On the correct patient;On the correct side;At the correct site

Safe Site Surgery Wrong site surgery:
rare but devastating occurrenceIt occurs when there is no:
○ Easy○ Systematic○ Redundant○ Fail safe
procedure for ensuring that the correct site is being treated

8
Wrong Side Surgery: Contributing Factors
Inadequate pt assessment Incomplete medical record review Poor handwriting Reliance on surgeon alone to identify site Poor communication among OR team Multiple procedures performed on same patient Time pressure Lack of clear policies
Vincent C, et al. BMJ. 2000;320:777-81.
Safe Site Surgery
Pt identification:
Methods needed to ensure the right pt is being treated
Pt identity is confirmed & communicated at each transfer
Good oral communication between HCWs

Safe Site Surgery
Procedure & site verification:
Discussion with pt
Consult notes
Consent
Imaging studies
Other relevant documentation
Correct implant if applicable

Site Marking:
Universal process
Involves a member of the surgical team who will be operating
Occurs generally prior to transfer to Operating room
Exceptions
Safe Site Surgery

The “Surgical Pause” or “Time Out”
ALL members in the room verbally agree to the procedure being done
Anyone can challenge prior to the procedure starting
Method in place to review case if there is not consensus
Safe Site Surgery
Marking Should be done prior to the OR
Marked on skin (not removable with prep, no stick-on marking)
Surgeon should sign the site
No extraneous marks
Pt involved

Marking (Exceptions)
Laparoscopic surgery
Midline Surgery
Single orifice surgery
Where decision is made intraop
Spinal Level (intraop marking)




Reduce Healthcare Acquired Infections (HAIs / HCAIs)
• Comply with current CDC Hand Hygiene Guidelines.
• Manage unanticipated death or major permanent loss of function associated with a HAIs as a sentinel event.
Hand Hygiene Is…
The #1 way to STOP transmission of infection!

Prevent Flu & Pneumonia
Protect yourself…..get immunized!
Protect your patients….
DID YOU KNOW….. With flu you are contagious 24 hours before you even know you are sick!
DID YOU KNOW….Hospitals with high employee flu vaccination rates have lower patient mortality!
Protect your families… don’t take germs home!
Why me?

Reduce Risk of Harm From Falls
Assess Fall Risk on admission, each reassessment, & after a fall
Use a Falling Leaf to indicate a patient is a high fall risk
Implement fall prevention devices, alarms & equipment
Correct spills or wet surfaces
Dispose of trash appropriately
Remove or report any trip hazards & environmental hazards immediately
Examine for injury before moving the pt after a fall
Complete incidence report & notify next of kin
Implement additional fall precautions as indicated
Points to Remember about Aseptic Technique
Adherence to the Principles of Aseptic Technique
Reflects One's Surgical Conscience.
1. The patient is the center of the sterile field.
2. Only sterile items are used within the sterile field.
A. Examples of items used.B. How do we know they are sterile? (Wrapping, label, storage)
3. Sterile persons are gowned & gloved.•
A. Keep hands at waist level & in sight at all times.
B. Keep hands away from the face.
C. Never fold hands under arms.
D. Gowns are considered sterile in front from chest to level
of sterile field, & the sleeves from above the elbow to cuffs.
Gloves are sterile.
E. Sit only if sitting for entire procedure.

4. Tables are sterile only at table level.
A. Anything over the edge is considered unsterile,
such as a suture or the table drape.
B. Use non-perforating device to secure tubing &
cords to prevent them from sliding to the floor.

5. Sterile persons touch only sterile items or areas; unsterile persons touch only unsterile items or areas.
A. Sterile team members maintain contact with sterile field
by wearing gloves & gowns.
B. Supplies are brought to sterile team members by the
circulator, who opens wrappers on sterile packages. The
circulator ensures a sterile transfer to the sterile field. Only
sterile items touch sterile surfaces.

6. Unsterile persons avoid reaching over sterile field; sterile persons avoid leaning over unsterile area.
•
A. Scrub person sets basins to be filled at edge of table to fill
them.
B. Circulator pours with lip only over basin edge.
C. Scrub person drapes an unsterile table toward self first to
avoid leaning over an unsterile area. Cuff drapes over
gloved h&s.
D. Scrub person st&s back from the unsterile table when
draping it to avoid leaning over an unsterile area.
7. Edges of anything that encloses sterile contents are considered unsterile.
A. When opening sterile packages, open away from you first.
Secure flaps so they do not dangle.
B. The wrapper is considered sterile to within one inch of the
wrapper.
C. In peel-open packages, the edges where glued, are not
considered sterile.

8. Sterile field is created as close as possible to time of use.
A. Covering sterile tables is not recommended.
9. Sterile areas are continuously kept in view.
A. Sterility cannot be ensured without direct observation. An
unguarded sterile field should be considered contaminated.
10. Sterile persons keep well within sterile area.
A. Sterile persons pass each other back to back or front to
front.
B. Sterile person faces a sterile area to pass it.
C. Sterile persons stay within the sterile field. They do not
walk around or go outside the room.
D. Movement is kept to a minimum to avoid contamination of
sterile items or persons.

11. Unsterile persons avoid sterile areas.
• A. Unsterile persons maintain a distance of at least 1 foot from the
sterile field.
•
B. Unsterile persons face & observe a sterile area when passing it
to be sure they do not touch it.
•
C. Unsterile persons never walk between two sterile fields.
•
D. Circulator restricts to a minimum all activity near the sterile field.

12. Destruction of integrity of microbial barriers results in contamination.•
A. Strike through is the soaking through of barrier from sterile to non-
sterile or vice versa.
•
B. Sterility is event related.
• 13. Microorganisms must be kept to irreducible minimum.
•
A. Perfect asepsis is an idea. All microorganisms cannot be eliminated.
Skin cannot be sterilized. Air is contaminated by droplets.

HAZARDS IN THE SURGICAL SUITE
• Electrical
• Cautery Units, Defibrillators, OR Beds, numerous pieces of equipment
All equipment must be checked for electrical safety before use!!
• Anesthetic Waste
• Radiation
• Leaded aprons & shields available for use during procedures.

Laser Safety
• Protective eyewear for pt & OR team.
• Doors remain closed with sign - "Danger, Laser in Use."
• Sterile water available in the room & on sterile field.
• Smoke evacuation system is to be employed when applicable.
• Surgery high filtration masks should be worn during procedures that
produce a plume.

General Safety
• Apply good body mechanics at all times when transferring pts.
•
OR beds & gurneys will be locked before pt transfer.
Operating safety belts will be used for all pts.
• Never disconnect or connect electrical equipment with wet or moist
hands.
• Discard all needles, razors, scalpel blades & broken glass into special
identified containers.

UNIVERSAL PRECAUTIONS SUMMARY• Although the risk of contracting HIV in the healthcare setting is extremely low,
there are other bloodborne pathogens which pose a much more significant risk.
• Precautions should be followed to reduce the risk of exposure to bloodborne
pathogens.
• Each healthcare worker should assess their possible risks & take precautions to
reduce these risks.
• Universal Precautions are designed to protect healthcare workers from
occupational exposure & should be followed when potential for exposure might
occur.

Universal blood & or body fluid precautions
should be consistently used for ALL pts.
Fundamental to the concept of Universal
Precautions is treating all blood & or body
fluids as if they were infected with
bloodborne pathogens & taking appropriate
protective measures, including the following:

• 1) Gloves should be worn for touching blood & or body fluids, mucous membranes, non-intact skin, or items/surfaces soiled with blood & or body fluids.
• Gloves should be changed after contact with each pt & h&s washed after glove removal.
• Though gloves reduce the incidence of contamination, they cannot prevent penetrating injuries from needles & other sharp instruments.

• 2) Gowns or aprons should be worn during procedures that are likely to generate splashes of blood & or body fluids onto clothing or exposed skin.
• 3) Masks & protective eyewear should be worn during procedures that are likely to generate droplets of blood & or body fluids into the mucous membranes of the mouth, nose, or eyes.

• 4) Needles & sharps should be placed directly into a puncture-resistant leakproof container which should be as close as possible to the point of use. Needles should not be recapped, bent, broken, or manipulated by hand.
• 5) Hands & skin surfaces should be washed after contact with blood &/or body fluids, after removing gloves, & between pt contact.

• 6) Gloves should be worn to cleanup blood spills. Blood spills should be wiped up & then an EPA registered tuberculocidal disinfectant applied to the area. The disinfectant should have a one minute contact time & the area rinsed with tap water. If glass is involved, wear double gloves or heavy gloves. Pick up the glass with broom & dust pan, tongs, or a mechanical device.
• 7) Healthcare workers with exudative lesions or weeping dermatitis should not perform direct patient care until the condition resolves.

8) Disposable resuscitation devices should be used in an emergency.
9) Occupational Exposures: Definition
- Puncture wounds- Needlesticks/Cuts- Splashes into the eyes, mouth, or nose- Contamination of an open wound

10) Occupational Exposures:
- Wash the area immediately with soap & water
- If splashed in the eyes mouth or nose have
them properly flooded or irrigated with water
- Notify supervisor as soon as possible
- Call infection control unit for information
regarding blood &/or body fluid exposure
management

General safety – cuts & sticks, lifting, falls,
radiation, burns, hand/foot injuries
Biohazards
Fire Hazards
Laser Hazards

Compressed Gases
Trace Gases
Electrical Hazards
Substances
Operational hazards

Safety Issues in OR

Safety Issues in OR

Safety issues in OR

Safety Issues in OR

Electrical hazards are the cause of numerous workplace fires each year. Faulty electrical equipment or misuse of equipment produces heat & sparks that serve as ignition sources in the presence of flammable & combustible materials.
Egs of common ignition hazards:overloading circuitsuse of unapproved electrical devicesdamaged or worn wiring
Fire Safety-Electrical Electrical IssuesIssues

Anaesthetic Machine / Gas

Fire in the OR

Barker, S. J. et al. Anesth Analg 2001;93:960-965
Electrosurgical unit application

Fire in the OR

LASERS
Retained instruments & sponges

U/sound features of missed pack & The pack is soaked with altered blood &
purulent exudate (arrow)

Gossypiboma: Retained gauze
Retained surgical sponge: an unusual cause of malabsorption.

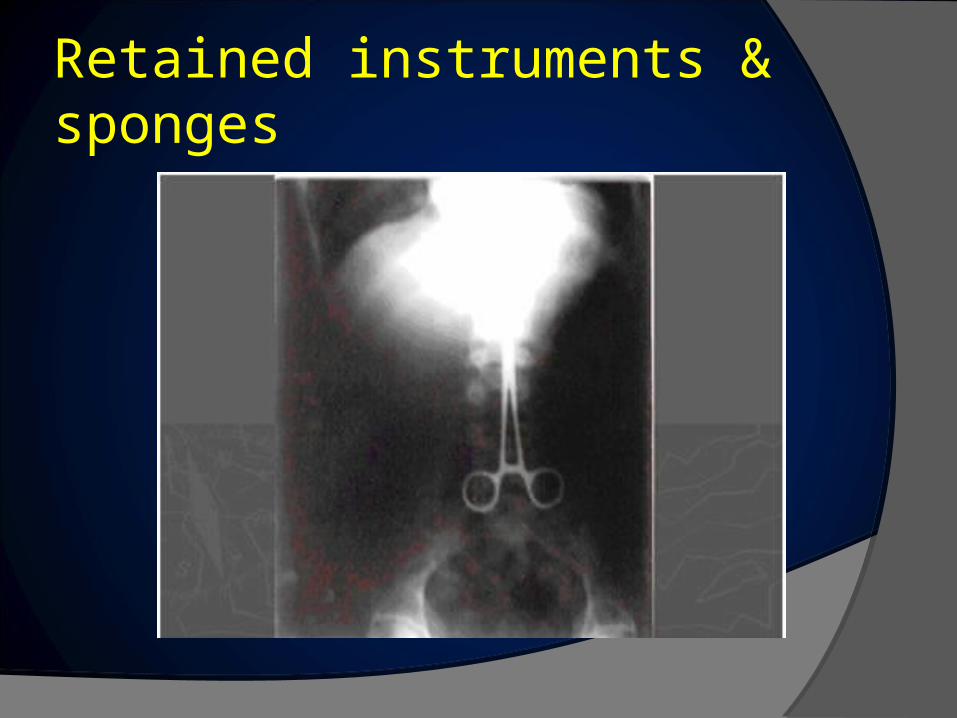
Retained instruments & sponges
X-ray of a surgical scissor blade that broke off that the surgical team didn’t notice.
X-ray of a retained clamp that the surgical team forgot to remove.

Retained instruments & sponges
Surgical sponge that was left in a patient, identified by the radio-opaque thread inside the sponge.
Retained laparotomy pad, Mount Sinai Medical Center, New York, 1998. ‡

Positioning / Injury / Fall in OR

Positioning / Injury / Fall in OR

Sharps / Needle Stick Injuries in OR

AANA Position Statement 2.13Safe Practices for Needle and Syringe Use
www.aana.com


Sharps Safety In the Operating Room
Creating an Injury Prevention Program


Implementation Suggestions Use scalpel blades with safety blades
Reusable Disposable

Implementation Suggestions Alternative cutting methods Cautery Harmonic scalpel
Cautery
Harmonic Scalpel

Implementation Suggestions Use blunt suture needles, stapling devices or
steristrips
Blunt suture needle
Stapler
Steristrips

Implementation Suggestions Keep used needles on the sterile field in a
disposable puncture resistant needle container

Implementation Suggestions Adopt a hands-free technique of passing suture
needles & sharps between perioperative team members
Implementation Suggestions Use a one handed or instrument assisted
suturing technique to avoid finger contact with needles
Use “control-release” or “pop-off” needles

Implementation Suggestions Double glove during all surgical procedures

Implementation Suggestions
DO NOT bend, break or recap contaminated needles
If re-capping is absolutely required, use one-handed scoop technique: (1) Place needle cap on table
(2) Holding the syringe only, guide needle into cap
(3) Lift up syringe so cap is sitting on needle hub
(4) Secure needle cap into place

Sharps Disposal
Closable orange or red, leak-proof puncture
resistant containers
Located close to the point of use maintained
upright
Replaced routinely and not allowed to overfill
Wall / Floor mounted

Sharps Disposal: New Containers
Safety sharps containers
Goal: to Prevent Needlesticks
• Counter-balanced drop in prevents children’s fingers from getting in
• Automatically closes at ¾ full – prevents overfilling
Reusable sharps containers
Goal: to reduce landfill waste
• Outside contractor removes contaminated sharps, cleans container and returns it

Retained FB / Surgical Instrument

Retained surgical instruments
Foot-long surgical tool left in woman's abdomen

Diathermy – Burns / Electrocution

Iatrogenic skin burns due to spirit during laparotomy

IV Lines / Blood Transfusion

Employer Responsibilities
Comply with regulations
Create a safety-oriented culture
Encourage reporting
Analyze data
Provide training
Evaluate devices
Establish safe staffing patterns

Worker Responsibilities
Observe regulations
Comply with methods available
Use & Practice using safety devices
Actively participate in evaluation & safety
conversion process

Worker Responsibilities
Use appropriate PPE
Use appropriate sharps containers
Participate in education and follow
recommendations
Support others to follow the recommendations
Follow hospital exposure control policy

Worker Responsibilities
Report Exposures
Employers required by OSHA to document all staff exposures to blood / body fluids anonymously
○ Sharps Injury incidence reportLocation, job title, description of incident, type &
brand of sharps involved
Source testing, risk analysis & post-exposure prophylaxis if indicated

BARRIERS TO IMPLEMENTATION
Psychosocial & organizational factors
Attitude/Resistance to Change
Shortcomings associated with safety devices
Perceived cost associated with engineered
devices
Inadequate training
Time limitations

Overcoming Obstacles to Compliance
Frequent & multiple training methods
Multidisciplinary sharps injury prevention plan
Educate new employees & all HCWs
Multidisciplinary sharps safety committee
Network with other facilities
Involve front-line workers in evaluation & selection of
safety devices

Other Issues?
Drugs Preparation & Administration.
Substance Abuse (Drugs).





























