Embed Size (px)
Citation preview

CASE PRESENTATIO
N

LYCEUM OF THE PHILIPPINES UNIVERSITY- BATANGASCapitol Site, Batangas City
PANCREATIC PSEUDOCYSTPANCREATIC PSEUDOCYSTPrepared By:
Florendo, Rachael Ann G.Florendo, Rachael Ann G.BSN III-5BSN III-5Group CGroup C
Submitted to:Submitted to:Dra. Annabelle IturraldeDra. Annabelle Iturralde
INTRODUCTION
Pseudocyts is applied to a collection of fluid that arises from loculation of inflammatory processes, necroses or hemorrhages. This type represents the overwhelming majority of clinically important cyst and is almost always associated with pancreatitis. Pseudocyts may also follow traumatic injury to the abdomen with direct damage and hemorrhage in the pancreas. Acute pancreatitis or trauma precedes the clinical discovery of a pseudocyst in nine of ten cases.
These cyst are usually solitary and most measure 5-10 cm in diameter. They may be situated with in the pancreatic substance, but more often they are found adjacent to the pancreas, particularly in the region of the tail of the pancreas. The cyst walls may be thin or thick and fibrous. Characteristically, they do not have an epithelial lining and have no connection of communication with surrounding ductal systems. There may have a marked inflammatory reaction in the fibrous capsule and often organizing blood clot, old blood pigment, precipitates of calcium and cholesterol crystals. The cyst fluid is usually serons and turbid .
Pseudocyst produce abdominal pair and intraperitoneal hemorrhage and if infected, may cause generalized peritonitis. However, their clinical significance lies in their being discovered as an abdominal mass in a location that strongly suggest a primary intra abdominal malignancy. The diagnosis is made by ultrasonography or CT sacnning with the ultrasound, pseudocysts are evident as sonolucent areas with re;atively smooth, well outlines. They are usually unilocular, multi-loculation suggests a neoplastic cyst. CT scanning adds specificity by ultrasound in this settting.
Pancreatitis in children is uncommon and represents a diagnostic challenge for clinicians. Although most adult cases of pancreatitis are caused by alcohol abuse or gallstone disease, the etiology for pancreatitis in children is diverse. The predominant causes include abdominal trauma (23%), anomalies of the pancreaticobiliary system (15%), multisystem disease (14%), drugs and toxins (12%), viral infections (10%), hereditary disorders (2%), and metabolic disorders (2%). In the United States, trauma is responsible for 15-37% of cases.1
In general, the prognosis of children with acute pancreatitis is excellent, although pseudocysts have been reported to complicate 10-23% of acute episodes. In addition, when associated with abdominal trauma, the frequency rate of pseudocyst identification is higher than 50%. Approximately 60% of pancreatic pseudocysts that are caused by blunt trauma require surgical intervention.
In children, however, the presenting signs and symptoms can be quite varied. So I choose this case for further understanding these disease and to know the prevention and management.
In this case study, I want to learn, know and understand better the disease. It has been chosen, since it is now fastly increasing in our morbidity rates among diseases. It is better for us to be educated with its causative factors as well as the prevention and management whenever Pancraetic Pseudocyst occurs.
OBJECTIVE
GENERAL OBJECTIVES:
At the end of the case presentation I will be enhanced with the knowledge ,equipped with the skills and acquire positive attitude about pancreatic pseudocyst its effect to the individual as well as to their significant others, its manifestation and prevention, necessary treatment and appropriate nursing action.
SPECIFIC OBJECTIVES:
1)The patient condition. State the patient profile, past medical history, personal, social, and family as well as history of present illness.2) Asses the physical appearance of the patient and the recognizes the clinical manifestations of the disease.3) Identify, interpret and understand laboratory examination and diagnostic tests indicated and its significant finding.4) Understand the anatomical parts and explain the nature and identify the cause, disease process and manifestation of the disease.5)Utilize the nursing process in the delivery of cared based in the clients needs and concerns.6) Enumerate and analyze the drugs that have been administered to the patient.7) Provide information on the prognosis and discharged planning intended to the patient condition.
PATIENT’SPROFILE

• NAME: Child X• AGE: 16 years old• SEX: Female• DATE OF BIRTH: January 19, 1992• CIVIL STATUS: Teen• ADDRESS: Brgy. Look Balete Batangas • NATIONALITY: Filipino• RELIGION: Roman Catholic• DATE OF ADMISSION: December 5, 2008• PHYSICIAN: Dr. Arellano,Dr. Gonzales and Dr. Reyes• CHIEF COMPLAINT: Abdominal pain• ADMITTING DIAGNOSIS. Pancreatic Pseudocyst s/s explore by acute
hemorrhologic pancreatitis.• FINAL DIAGNOSIS: Pancreatic Pseudocyst

CLINICALAPPRAISAL

A. Past Health History
Ms. X have completed the childhood immunization. She was operated for acute hemorrhologic pancreatitis on October 1, 2008. She stayed in the hospital for 10 days and was discharged improved. However she came back about a week later with symptoms of obstruction. An ultrasound was taken which showed a pancreatic pseudocyst. Alimentation was advised. A few days ago, a request ultrasound showed an increase of the size of the mass. She is coherent to undergo a CT scan of the abdomen often with note surgery to drain the pseudocyst is contemplated.
B. Family History
Her father is a security guard and her mother is a plain housewife. She has 2 brothers and 3 sisters. They have a history of disease hypertension, hypotension and cancer of the bone in mother side.
C. Personal History
Ms. X is a 16 year old who finished a high school degree only. Before her hospitalization, she has been working in a small store as a cashier.
According to her she’s fun of eating sour and salty foods, she added that she even drink the vinegar after eating the snacks. She also loves drinking soft drinks.
When Ms. X was high school, she was a honor student. Therefore she sleep for 4-5 hours only because she studied her lesson well.
D. Social History
Their house are made of cement and woods. They have only four neighbors. They welcomed all persons on their house especially their relatives. They believe in “anting-anting” for them to have a healthy life.

E. Psychological History
Her major stressor is the duration of her hospitalization. She felt bored in the hospital. She wants someone to talk.
For her to cope up her stressor, she talks to every person that she met. Like the other patient in the hospital and also a student nurse like me.
F. History of Present Illness
Three months PTA Ms. X developed abdominal pain vomiting, fever, anorexia, persistent of abdominal pain is prompted consults.
Second months PTA , she had an operation at BRH, after one week of discharged from the hospital she had dehydration and was returned to the hospital.
GENERALSURVEY
As the assessement revealed for the general appearance the findings was she has a poor body coordination and it is abnormal that affects body movement and posture. Her body becomes either very floppy or very stiff because of her condition. The body and breath odors I found out that she is having a foul mouth odor that can result from poor oral hygiene, or suffer from different tooth problem. About the psychological presence, she was clean and neat and dress properly. When I talked to her she’s so cooperative that she’s the one who wants to talked everything about her life. But she’s distress when we talked about her operation.
The vital sign was taken, temperature 36.1, 36.6, 36.1, blood pressure 90/70, 100/70, 100/60, pulse rate 74, 76, 69, respiratory rate 25, 27, 25 and her height is 153 and weight is 24.8 kg.
PHYSICAL ASSESSMENT
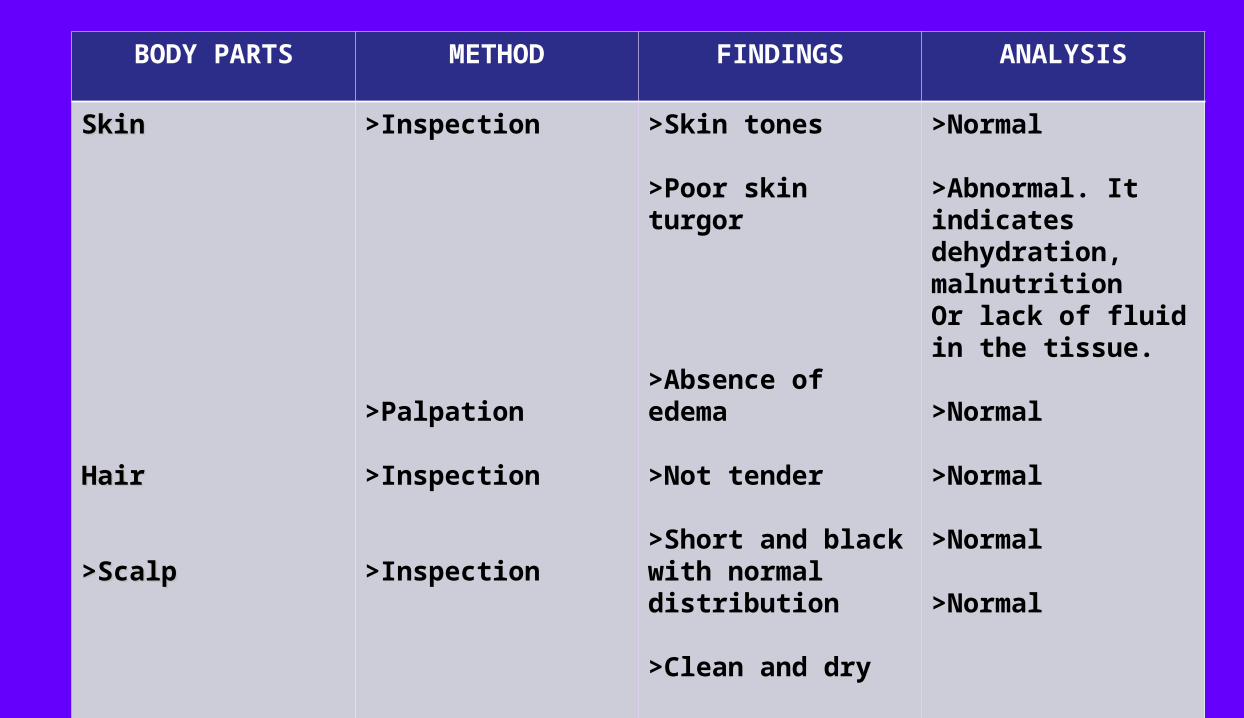
BODY PARTS METHOD FINDINGS ANALYSIS
SkinSkin
HairHair
>Scalp>Scalp
>Inspection
>Palpation
>Inspection
>Inspection
>Skin tones
>Poor skin turgor
>Absence of edema
>Not tender
>Short and black with normal distribution
>Clean and dry
>Normal
>Abnormal. It indicates dehydration, malnutritionOr lack of fluid in the tissue.
>Normal
>Normal
>Normal
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
Nails
Head
>Inspection
>Inspection
>Palpation
>No abrasion
>Pink tones
>Long and dirty nails
>Symmetrical
>Absence of masses or nodules
>Normal
>Normal
>Abnormal. Dirty, broken or jagged fingernails may be seen poor hygiene. They may also result from clients hobby or occupation.
>Normal
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
Face
Neck
Shoulders
Thyroid Gland
>Inspection
>Inspection & Palpation
>Inspection
>Inspection & Palpation
>Facial features & facial movements are symmetrical
>No enlargements of lymph nodes
>Does not use muscles when breathing
>No enlargement of the thyroid gland
>Normal
>Normal
>Normal
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
Eyes
>Eyebrow
>Eyelashes
>Conjunctiva
>Inspection
>Inspection
>Inspection
>Symmetrically aligned
>Equal movements
>Hair evenly distributed
>Normal distribution
>Bulbar conjunctiva
>Normal
>Normal
>Normal
>Normal
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
>Pupillary reaction
Ear
>Inspection
>Inspection
>Constricting & dilating
>Auricles are mobile, firm & not tender
>Symmetrically aligned
>Color of the auricles is same as the face
>Normal
>Normal
>Normal
>Normal
BODY PARTS METHOD FINDINGS ANALYSIS
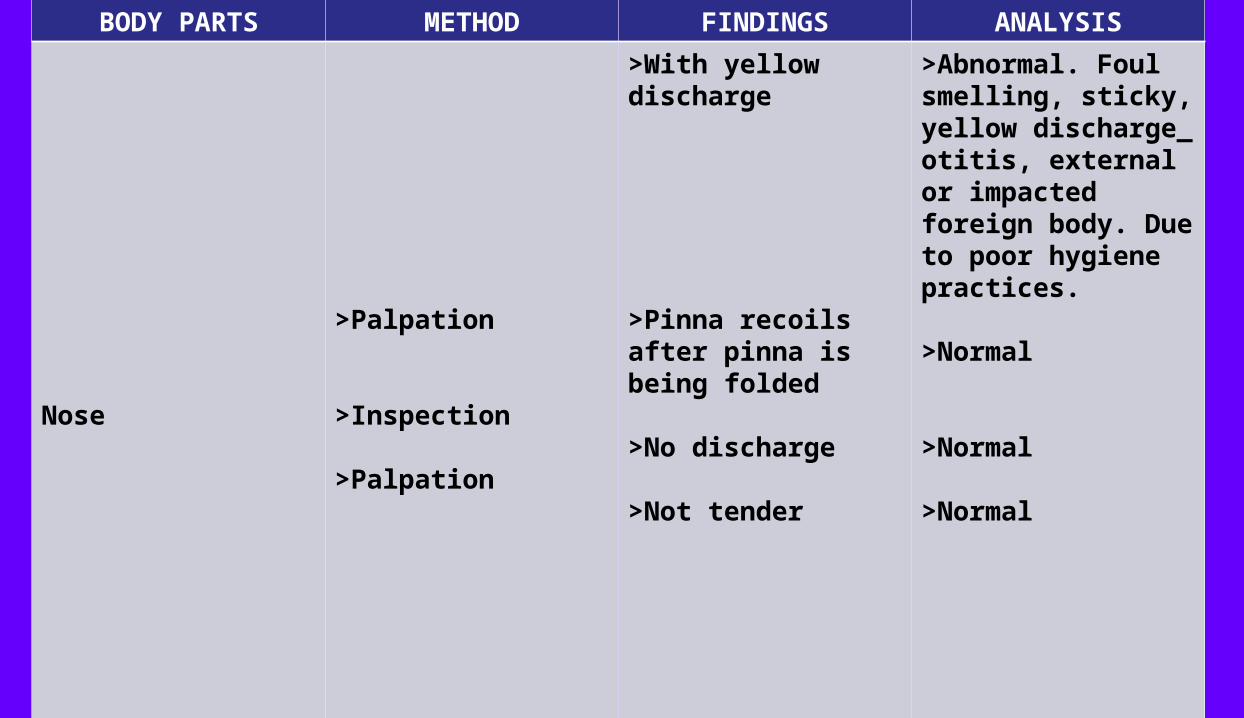
Nose
>Palpation
>Inspection
>Palpation
>With yellow discharge
>Pinna recoils after pinna is being folded
>No discharge
>Not tender
>Abnormal. Foul smelling, sticky, yellow discharge_ otitis, external or impacted foreign body. Due to poor hygiene practices.
>Normal
>Normal
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
Sinuses
Mouth
>Lips
>Teeth
>Tongue
>Palpation
>Inspection
>Inspection
>Inspection
>Frontal & maxillary sinuses are not tender
>Dry with cracks
>With yellow cavities
>Dry
>Moves freely
>Normal
>Abnormal. Dry lips indicates dehydration.
>Abnormal. Due to oral hygiene practices.
>Abnormal. It indicates dehydration.
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
>Uvula
Chest & Lungs
>Thorax
>Palpation
>Inspection
>Inspection & Auscultation
>Palpation
>Inspection
>Tongue at midline
>Not tender
>presence of uvula
>Does not use accessory muscles when breathing
>No tenderness or pain
>Normal chest configuration
>Normal
>Normal
>Normal
>Normal
>Normal
>Normal
BODY PARTS METHOD FINDINGS ANALYSIS
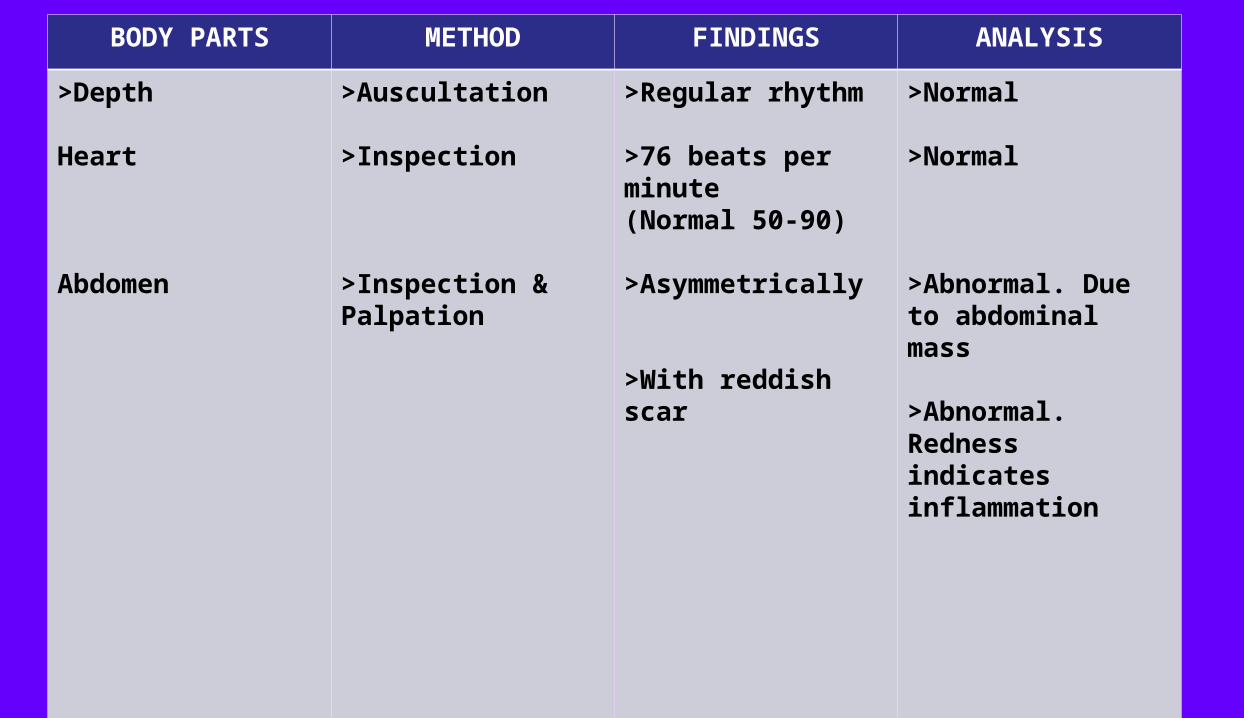
>Depth
Heart
Abdomen
>Auscultation
>Inspection
>Inspection & Palpation
>Regular rhythm
>76 beats per minute(Normal 50-90)
>Asymmetrically
>With reddish scar
>Normal
>Normal
>Abnormal. Due to abdominal mass
>Abnormal. Redness indicates inflammation
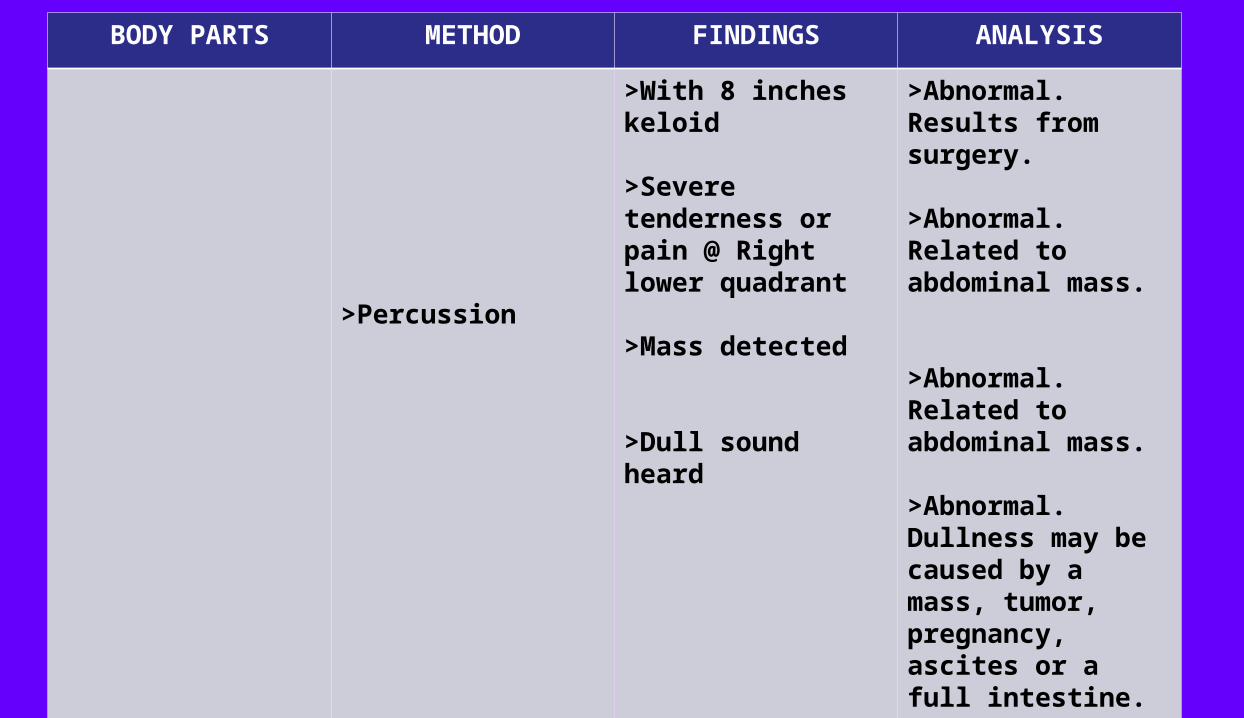
BODY PARTS METHOD FINDINGS ANALYSIS
>Percussion
>With 8 inches keloid
>Severe tenderness or pain @ Right lower quadrant
>Mass detected
>Dull sound heard
>Abnormal. Results from surgery.
>Abnormal. Related to abdominal mass.
>Abnormal. Related to abdominal mass.
>Abnormal. Dullness may be caused by a mass, tumor, pregnancy, ascites or a full intestine.
BODY PARTS METHOD FINDINGS ANALYSIS
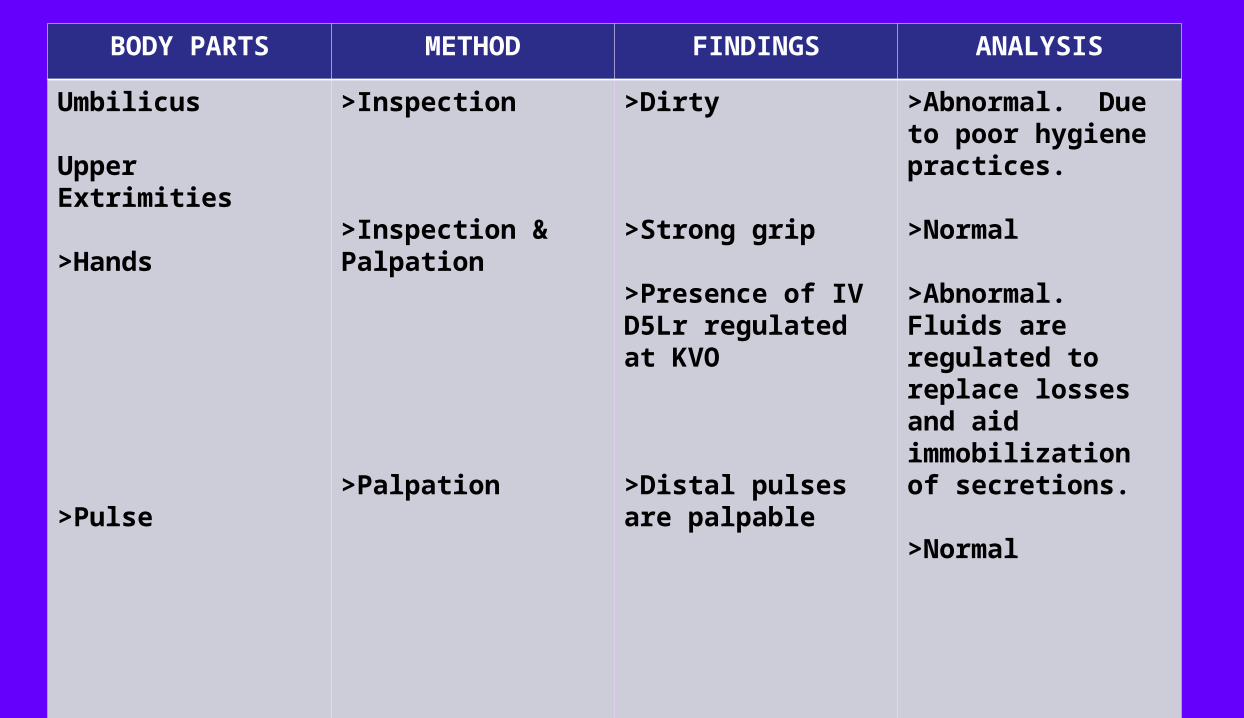
Umbilicus
Upper Extrimities
>Hands
>Pulse
>Inspection
>Inspection & Palpation
>Palpation
>Dirty
>Strong grip
>Presence of IV D5Lr regulated at KVO
>Distal pulses are palpable
>Abnormal. Due to poor hygiene practices.
>Normal
>Abnormal. Fluids are regulated to replace losses and aid immobilization of secretions.
>Normal

BODY PARTS METHOD FINDINGS ANALYSIS
>Nail beds
Lower Extremities
>Inspection
>Inspection & Palpation
>Pink tones
>Capillary refill every 2-3 seconds(Normal 2-3 seconds)
>No edema
>Normal
>Normal
>Normal
SUMMARY OF
PHYSICALASSESSMENT

Child X, the subject of the study is diagnosed with Pancreatic Pseudocyst. Physical Appearance of the patient was assessed through inspection, palpation, percussion and auscultation. This will serve as a baseline guide to recognize the signs and symptoms of the disease.
She has a poor skin turgor that indicates dehydration or malnutrition. She has a long and dirty nails that indicates poor hygiene may be result from her hobby.
Upon inspecting the ear she has a yellow discharge. Foul smelling, sticky, yellow discharge or otitis, external or impacted foreign body. Due to her poor hygiene practices. Her lips and tongue was dry indicates dehydration. She also have a yellow cavities due to her oral hygiene practices.
Upon inspecting and palpating the abdomen she has abdominal mass, with reddish scar that
redness indicates inflammation. She also have a 8 inches keloid from her last operation.
she suffer from severe tenderness or pain at right lower quadrant related to abdominal mass. When I percussed her abdomen I heard a dull sound that may be caused by her mass. Her umbilicus was also dirty due to poor hygiene practices.
Presence of D5ILR regulated at KVO was also noted to replace losses and aid to immobilization of secretions.

LABORATOTY RESULTS

Ultrasound Nov. 26 2008Examination RequestedWhole abdomen UTS
Report
Follow whole abdominal ultrasound since Oct. 19, 2008.
Liver is normal in size. Parenchymal echo pattern is homogenous. No facial mass is seen. Intrahepatic ducts isnot dilated.
Gall bladder is normal in size and wall thickness. No intraluminal echoes seen. Proximal common ducts is notdilated and measures 0.3 cm.
There are two wall defined a necrosis structures seen at the mid upper abdomen which are intimate to theanterior surface of the pancreas measuring approximately 4.4 x 4.9 x 4.8 cm.
Medium level echoes and some septations, are seen with in the cystic structures.
Spleen is normal in size and echopattern with no focal solid or cystic nodule seen.
Both kidneys are normal in size and echopattern. The right kidney measures 7.1x2.3 cm
withcortical thickness of 0.78 cm, while the left kidney measures 10.6x4.5 cm with cortical
thickness of 1.7 cm. No stone mass or hydronephrosis seen.
Uterus is anteverted normal in size measuring 4.7 x 2.2 cm. Myocardial echopattern is
homogenous. No focal mass is seen. Endometrial lining is not thickened and measures 0.7 cm.

The abdominal aorta is not dilated and measures 0.76 cm in its widest diameter.
Urinary bladder is well distended it’s wall is not thickened. There is no stone or mass seen.
There is a well defined cystic structure at the left adnexa which measures 3.8x3.0x3.o cm. Leveling fluid and hyperechoic structure is seen with in the cyst probably fat fluid density.
IMPRESSION
Two anechoic structures detected at upper mid abdomen intimate to the anterioir surface of the pancreas. This may relate to pseudocyst of the pancreas, differential diagnosis is marked distended stomach and duodenum bulb. Correlation with abdominal CT scan with oral contrast is suggested.
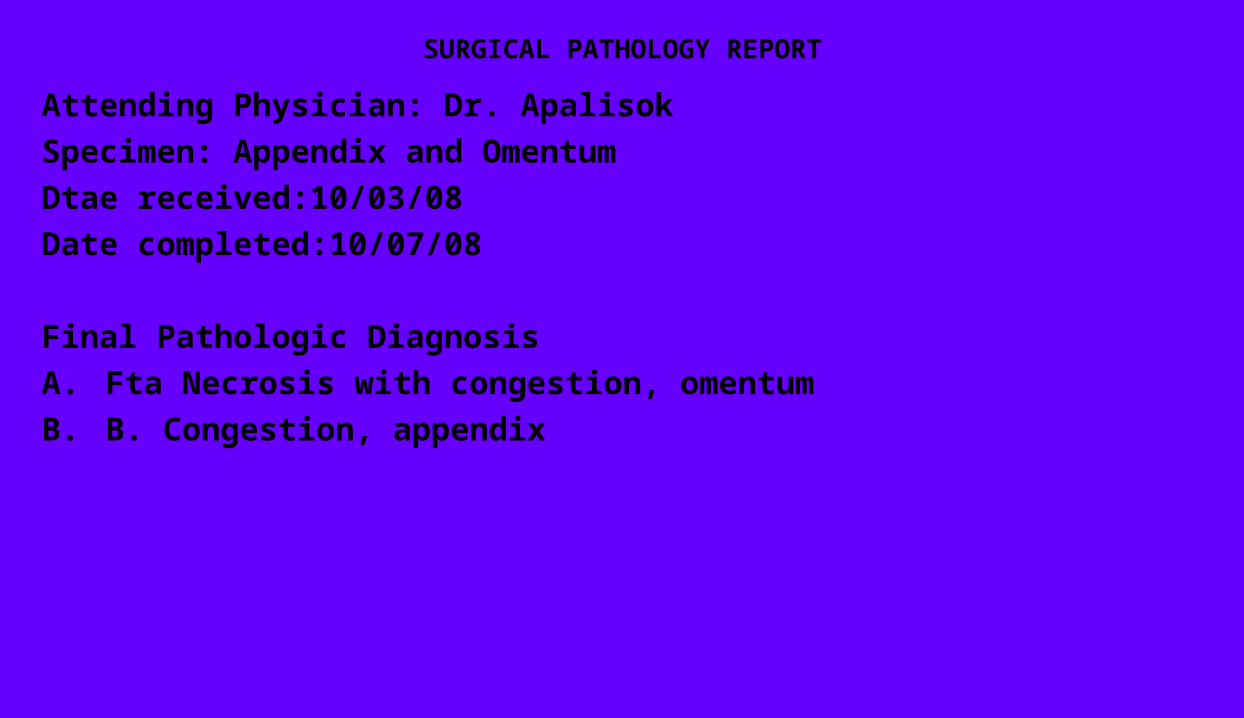
SURGICAL PATHOLOGY REPORT
Attending Physician: Dr. Apalisok
Specimen: Appendix and Omentum
Dtae received:10/03/08
Date completed:10/07/08
Final Pathologic Diagnosis
A. Fta Necrosis with congestion, omentum
B. B. Congestion, appendix
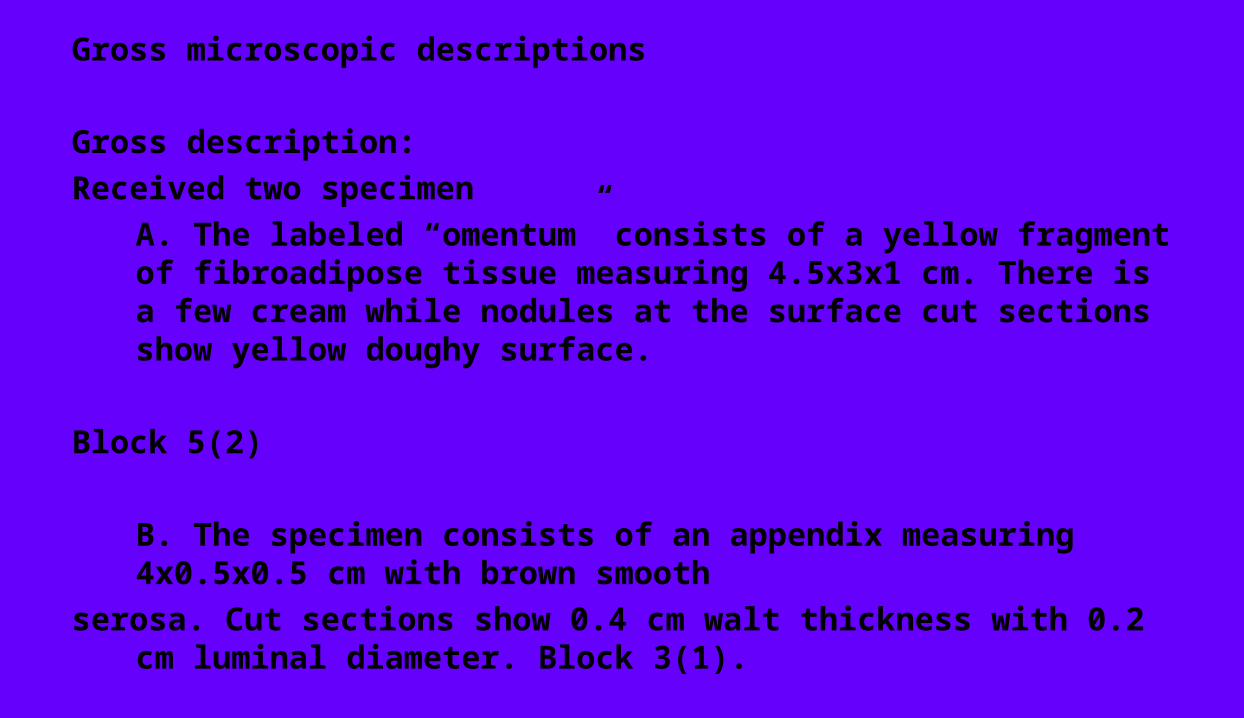
Gross microscopic descriptions
Gross description:
Received two specimen
A. The labeled “omentum” consists of a yellow fragment of fibroadipose tissue measuring 4.5x3x1 cm. There is a few cream while nodules at the surface cut sections show yellow doughy surface.
Block 5(2)
B. The specimen consists of an appendix measuring 4x0.5x0.5 cm with brown smooth
serosa. Cut sections show 0.4 cm walt thickness with 0.2 cm luminal diameter. Block 3(1).

Microscopic Description
A. Histological sections reveal mature adipocytes with dilated vessels. Focal fat necrosis is
noted.
B. Histological sections reveal appendix with dilated vessels at the serosal surfsce.

Dec. 9, 2008 HEMATOLOGY
TEST RESULTS NORMAL ANALYSIS
Erythrocytes
Hemoglobin
Hematocrit
Leukocyte
Neutropil
Eosinophils
Basophils
Lymphocytes
4.08 10 ^12L
120.5 g/L
0.364 %
5.78 10 ^9/L
0.339 %
0.087 %
0.003 %
0.492 %
Female: 4.2-5.4
Female: 120-140
Female: 0.38-0.47
4.5-11
50-70 %
0-O.7x10 9/L
0.5-1.0 %
25-35 %
Normal
Normal
Normal
Normal
Decrease. Folic acid deficiency
Eosinophilia
Decrease. Anemia plastic
Lymphopenia
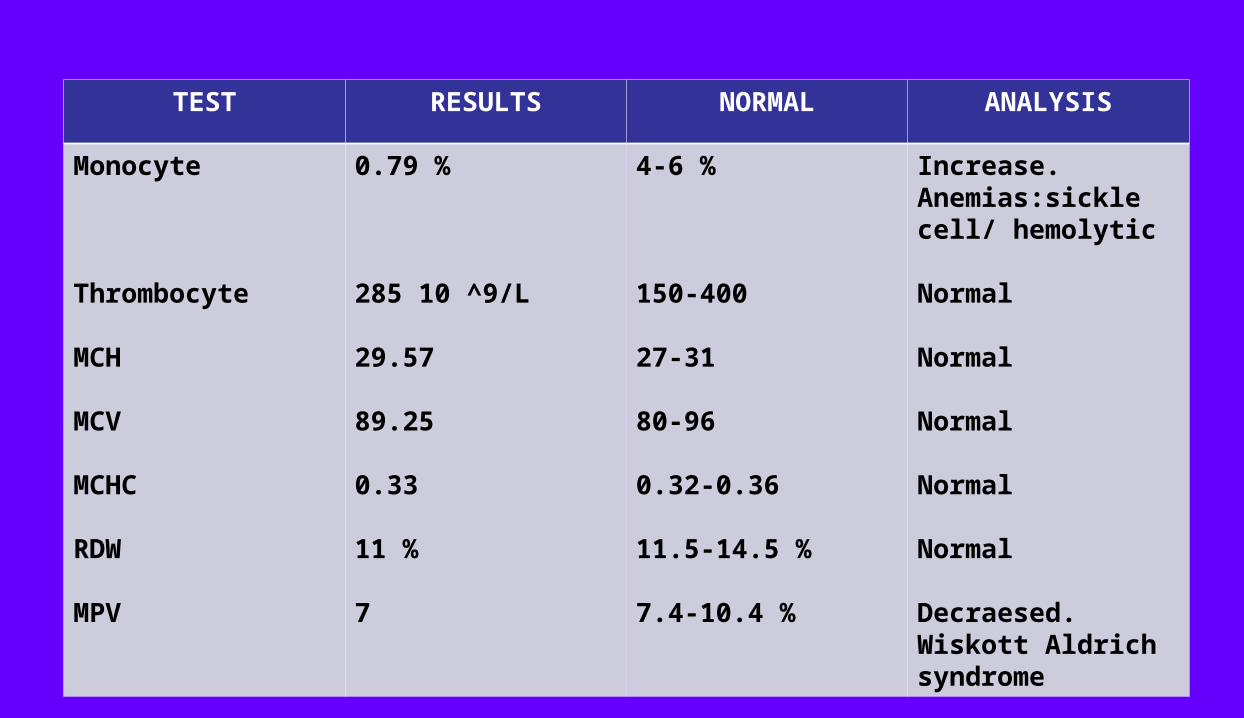
TEST RESULTS NORMAL ANALYSIS
Monocyte
Thrombocyte
MCH
MCV
MCHC
RDW
MPV
0.79 %
285 10 ^9/L
29.57
89.25
0.33
11 %
7
4-6 %
150-400
27-31
80-96
0.32-0.36
11.5-14.5 %
7.4-10.4 %
Increase. Anemias:sickle cell/ hemolytic
Normal
Normal
Normal
Normal
Normal
Decraesed. Wiskott Aldrich syndrome
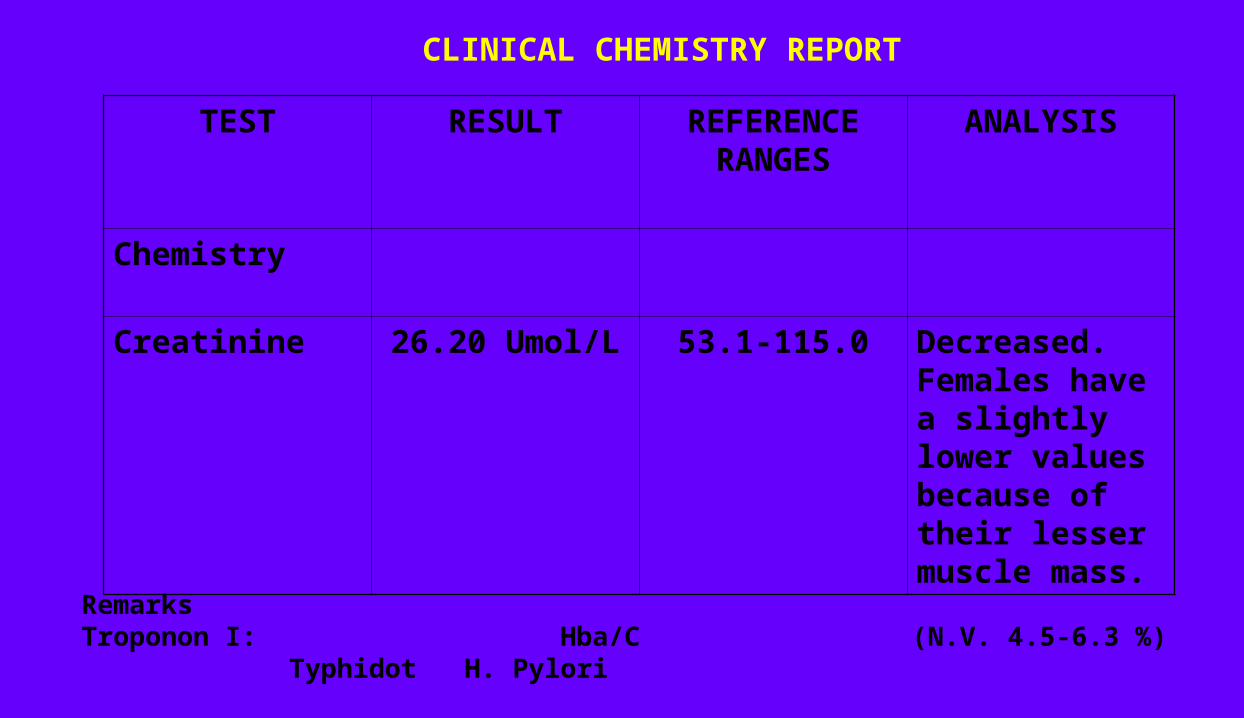
CLINICAL CHEMISTRY REPORT
TEST RESULT REFERENCE RANGES
ANALYSIS
Chemistry
Creatinine 26.20 Umol/L 53.1-115.0 Decreased. Females have a slightly lower values because of their lesser muscle mass.
RemarksTroponon I: Hba/C (N.V. 4.5-6.3 %) Typhidot H. Pylori

SUMMARYOF THE
LABORATORYRESULT

As the laboratory exam has been released I found some abnormalities in the blood. The neutrophil was decreased that may caused a folic deficiency. The eosinophil indicates eosinophilia and the basophil is decreased indicates anemia plastic. The lymphocytes indicates lymphopenia.
The monocytes is increased indicates anemias= sickle cell or hemolytic. The MPV is decraesed indicates Wiskott Aldrich syndrome.
The creatinine is decreased because females have a slightly lower values because of their lesser muscle mass.
ANATOMYAND
PHYSIOLOGY
The digestive tract (also known as the alimentary canal) is the system of organs within multicellular animals that takes in food, digests it to extract energy and nutrients, and expels the remaining waste. The major
functions of the GI tract are ingestion, digestion, absorption, and defecation. The picture to the right doesn't show the Jejunum. The GI tract
differs substantially from animal to animal. Some animals have multi-chambered stomachs, while some animals' stomachs contain a single
chamber. In a normal human adult male, the GI tract is approximately 6.5 meters (20 feet) long and consists of the upper and lower GI tracts. The
tract may also be divided into foregut, midgut, and hindgut, reflecting the embryological origin of each segment of the tract.
The first step in the digestive system can actually begin before the food is even in your mouth. When you smell or see something that you just
have to eat, you start to salivate in anticipation of eating, thus beginning the digestive process. Food is the body's source of fuel. Nutrients in food give the body's cells the energy they need to operate. Before food can be used it has to be broken down into tiny little pieces so it can be absorbed and used by the body. In humans, proteins need to be broken down into
amino acids, starches into sugars, and fats into fatty acidsand glycerol.
Pancreas
The pancreas is located posterior to the stomach and in close association with the duodenum. The pancreas is a 6-10 inch elongated organ in the abdomen located retro peritoneal. It is often described as
having three regions: a head, body and tail. The pancreatic head abuts the second part of the duodenum while the tail extends towards the spleen. The
pancreatic duct runs the length of the pancreas and empties into the second part of the duodenum at the ampulla of Vater. The common bile duct
commonly joins the pancreatic duct at or near the point.
The pancreas is supplied arterially by the pancreaticoduodenal arteries, themselves branches of the superior mesenteric artery of the hepatic artery (branch of celiac trunk from the abdominal aorta). The superior mesenteric
artery provides the inferior pancreaticoduodenal arteries while the gastroduodenal artery (one of the terminal branches of the hepatic artery) provides the superior pancreaticoduodenal artery. Venous drainage is via the pancreatic duodenal veins which end up in the portal vein. The splenic vein passed posterior to the pancreas but is said to not drain the pancreas
itself.
The portal vein is formed by the union of the superior mesenteric vein and splenic vein posterior to the body of the pancreas. In some
people (as many as 40%) the inferior mesenteric vein also joins with the splenic vein behind the pancreas in others it simply joins with the
superior mesenteric veininstead.
The function of the pancreas is to produce enzymes that break down all categories of digestible foods (exocrine pancreas) and secrete hormones that affect carbohydrates metabolism(endocrine pancreas).
The pancreas is near the liver, and is the main source of enzymes for digesting fats (lipids) and proteins - the intestinal walls have enzymes that will digest polysaccharides. Pancreatic secretions from ductal cells contain bicarbonate ions and are alkaline in order to neutralize the acidic chyme that the stomach churns out. Control of the exocrine function of the pancreas are via the hormone gastrin, cholecystokinin and secretin, which are hormones secreted by cells in the stomach and duodenum, in
response to distension and/or food and which causes secretion of pancreatic juice.

DIGESTIVE SYSTEMDIGESTIVE SYSTEM
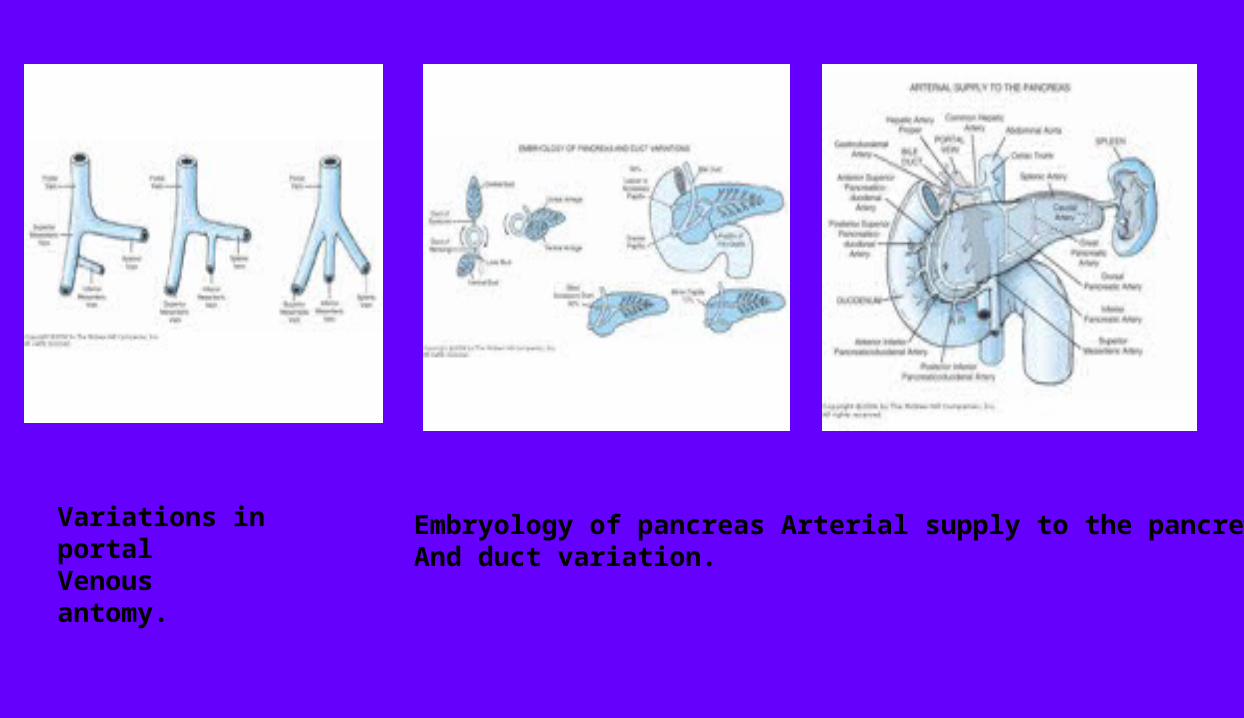
Variations in portalVenous antomy.
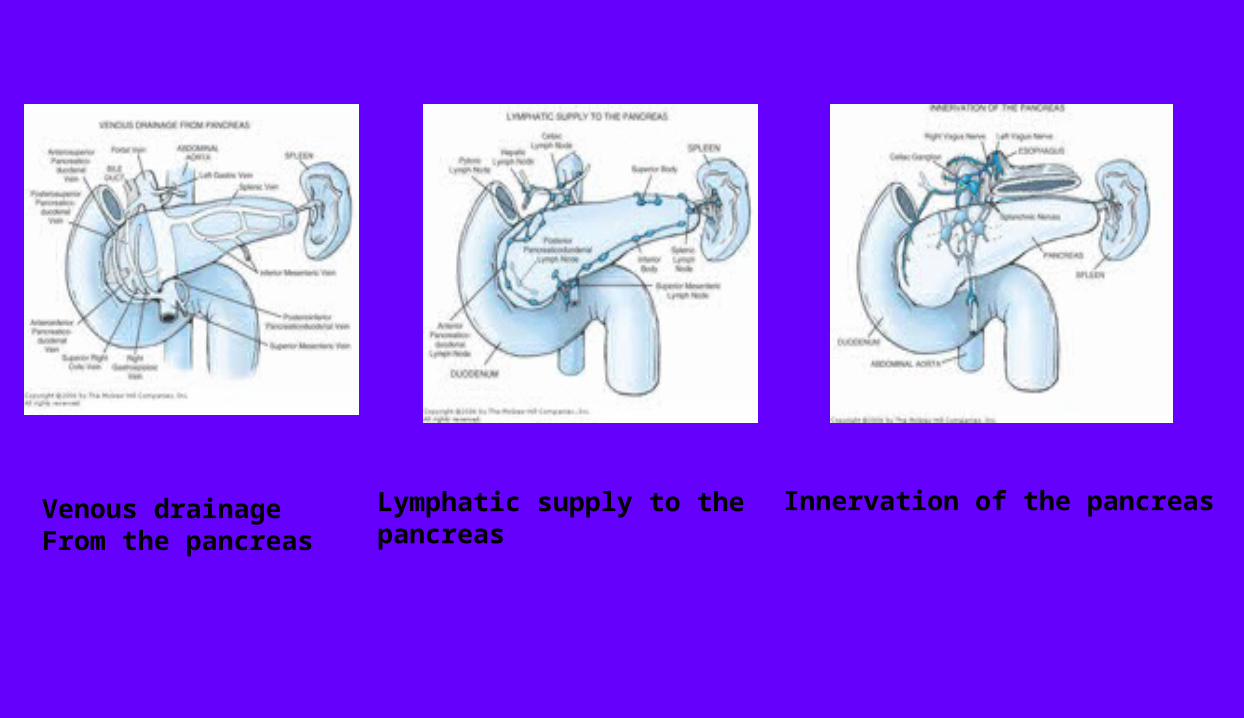
Embryology of pancreasAnd duct variation.
Arterial supply to the pancreas
Venous drainageFrom the pancreas
Lymphatic supply to thepancreas
Innervation of the pancreas
PATHOPHYSIOLOGY
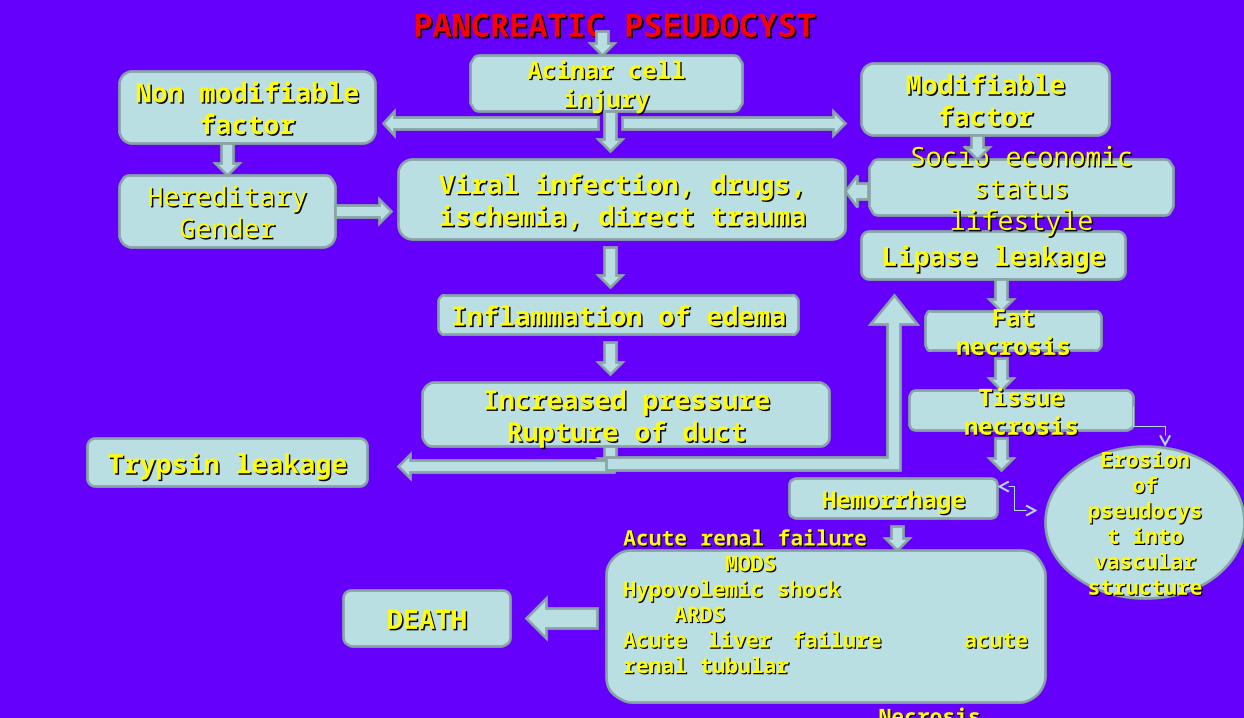
PANCREATIC PSEUDOCYSTPANCREATIC PSEUDOCYST
Acinar cell injuryAcinar cell injuryNon modifiable Non modifiable factorfactor
Modifiable factorModifiable factor
Viral infection, drugs, ischemia, Viral infection, drugs, ischemia, direct traumadirect trauma
Inflammation of edemaInflammation of edema
Increased pressureIncreased pressureRupture of ductRupture of duct
Trypsin leakageTrypsin leakage
Lipase leakageLipase leakage
Fat necrosisFat necrosis
Tissue necrosisTissue necrosis
HemorrhageHemorrhageErosion of Erosion of
pseudocyst pseudocyst into into
vascular vascular structurestructure
Acute renal failure MODSAcute renal failure MODSHypovolemic shock ARDSHypovolemic shock ARDSAcute liver failure acute renal tubularAcute liver failure acute renal tubular NecrosisNecrosis
DEATHDEATH
HereditaryHereditaryGenderGender
Socio economic statusSocio economic statuslifestylelifestyle

SUMMARY OF
PATOPHYSIOLOGY

The specific inciting factors causing pancreatitis remain to be elucidated. Pancreatitis may be induced by primary acinar cell injury as a result of viral infections, drugs, ischemia, and direct trauma.
Pancreatitis may originate from a disruption of the ductal system and subsequent excretion of digestive enzymes from the acinar cells of the pancreas. Normally these cells release inactive enzymes into collecting ducts, which then drain into the main or accessory pancreatic ducts emptying directly into the duodenal lumen. If obstruction or disruption of these ducts occurs, the pancreatic secretions are activated within the parenchyma of the pancreas and initiate autodigestion of the pancreatic tissue.
Interstitial edema is an early finding. Exacerbation of pancreatitis may result in pancreatic necrosis, blood vessel occlusion or disruption inciting hemorrhage, and systemic inflammatory response syndrome with multiorgan failure. Collections of pancreatic secretions often become walled off by granulation tissue to form a pseudocyst either within or adjacent to the pancreas. Predominantly, the pseudocyst is localized in the lesser sac behind the stomach. The stomach, duodenum, colon, small bowel, or omentum may abut or form part of the pseudocyst capsule.

NURSING CARE PLAN
ASSESSMENT NURSING DIAGNOSIS
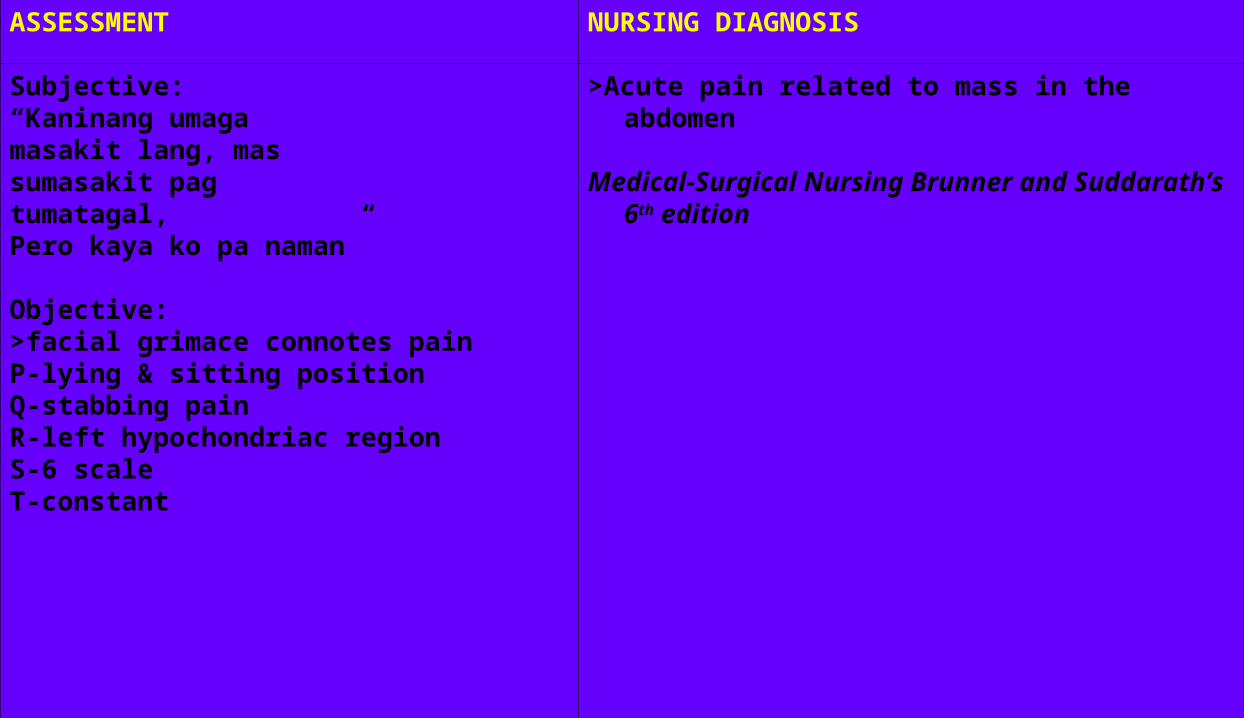
Subjective:“Kaninang umagamasakit lang, massumasakit pagtumatagal,Pero kaya ko pa naman”
Objective:>facial grimace connotes painP-lying & sitting positionQ-stabbing painR-left hypochondriac regionS-6 scaleT-constant
>Acute pain related to mass in the abdomen
Medical-Surgical Nursing Brunner and Suddarath’s 6th edition
SCIENTIFIC EXPLANATION PLANNING
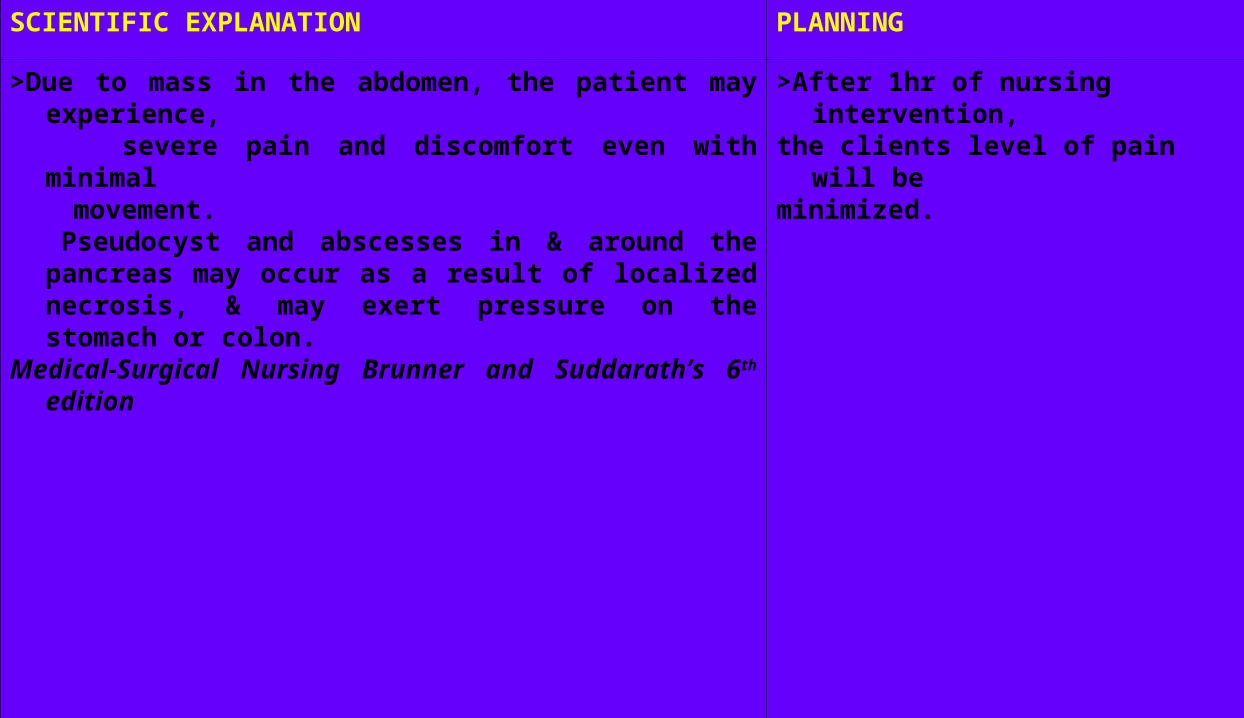
>Due to mass in the abdomen, the patient may experience, severe pain and discomfort even with minimal movement. Pseudocyst and abscesses in & around the pancreas
may occur as a result of localized necrosis, & may exert pressure on the stomach or colon.
Medical-Surgical Nursing Brunner and Suddarath’s 6th edition
>After 1hr of nursing intervention,the clients level of pain will beminimized.
INTERVENTION RATIONALE EVALUATION
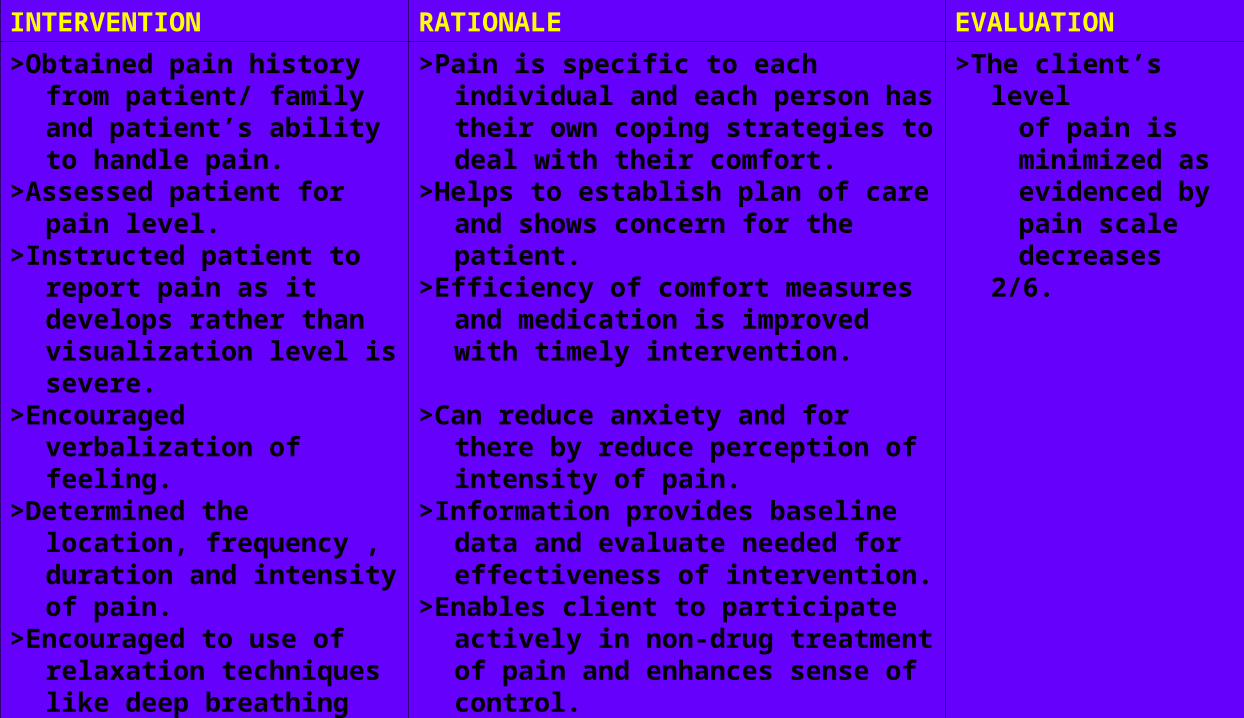
>Obtained pain history from patient/ family and patient’s ability to handle pain.
>Assessed patient for pain level.
>Instructed patient to report pain as it develops rather than visualization level is severe.
>Encouraged verbalization of feeling.
>Determined the location, frequency , duration and intensity of pain.
>Encouraged to use of relaxation techniques like deep breathing exercise.
>Performed palliative measures (e.g. repositioning)
>Pain is specific to each individual and each person has their own coping strategies to deal with their comfort.
>Helps to establish plan of care and shows concern for the patient.
>Efficiency of comfort measures and medication is improved with timely intervention.
>Can reduce anxiety and for there by reduce perception of intensity of pain.
>Information provides baseline data and evaluate needed for effectiveness of intervention.
>Enables client to participate actively in non-drug treatment of pain and enhances sense of control.
>May relieve pain and enhance circulation.
>The client’s level of pain is minimized as evidenced by pain scale decreases 2/6.
INTERVENTION RATIONALE
>Provided accurate, concrete information about what is being done. E.g. sensation the expect, usual procedures under taken.
>Provided calm, quite environment.
>Helps reduce fears of going through a frightening experience alone. Provide opportunity for so to express feelings/concerns.
>Involves in a patient plan of care and decreases unnecessary anxiety about unknown.
>Removing patient from outside stressors promotes relaxation may enhance coping skills.
>Encourage significant other patient as able.>respond to call signal promptly, use touch and eye
contact as appropriates.>Helps go to deal with own anxiety that can be
transmitted to patient. Promotes a supportive attitude that can facilitate recovery.
Nursing Care Plan Guidelines for Individualizing Client Care Across Lifespan
ASSESSMENT NURSING DIAGNOSIS
Subjective:
“Gusto ko ng umuwi nakakainip”
Ojective:
>restless
>irritable
>unsuccessful social interaction behavior
Boredom related to long hospital stay
SCIENTIFIC EXPLANATION PLANNING
It is always a factor that trigger the mood of a person. After 2 hours of nursing intervention the patient will be able to cope with her present condition.
INTERVENTION RATIONALE EVALUATION
>Provide structured environment with daily routines.
>Encouraged verbalization of concerns. Assist patient in experiencing feelings by Active Listening.
>Provided frequent rest periods and decreases sensory stimuli.
>Determined coping mechanism used.
>Observed interactions with others.
>Provides continuity of care
>Establishes a therapeutic relationship. Assist patient in dealing with feelings, and provides opportunity to clarify misconception. Acknowledge that this is a fearful situation and that others have expressed similar fears.
>Fatigue and sensory overload increases confusion.
>To note how these behaviors affect current situation.
>To note difficulties or ability to establish satisfactory relationship.
The patient was able to cope her present condition as verbalized by successful social interaction.
INTERVENTION RATIONALE
>Conveyed attitude of acceptance and respect.
>Encouraged control in all situation possible, include client in decision and planning.
>Instructed family to assist with reorientation as needed.
>Encouraged client to learn relaxation techniques, use guided imagery an positive affirmation of self.
>To avoid threatening client’s self-concept, preserve existing self-esteem.
>To preserve autonomy.
>Involves family in care. Patient may be more trusting of family members.
>In order to incorporate and practice new behavior.
NANDA
Nursing Care Plan Guidelines for Individualizing Client Care Across Lifespan
ASSESSMENT NURSING DIAGNOSIS
Subjective:
“Sa 18 na ang opera ko, dito na ako magpapasko”
Objective:
>happy
>calm
>relax
>sitting comfortably
Readiness for enhanced self-concept related to the acceptance of the condition

SCIENTIFIC EXPLANATION PLANNING
Acceptance of the condition may help for fast recovery
After 2 hours of nursing intervention the patient will verbalized the understanding of own sense of self-concept.
INTERVENTION RATIONALE EVALUATION
>Determined current status of individual’s belief about self.
>Determined availability or quality of family support.
>Noted willingness to seek assistance, motivation for change.
>Developed therapeutic relationship.
>Self-concept consists of the physical self, personal identity and self-esteem, and information about client’s current thinking about self provides as beginning for making changes to improve self.
>Presence of supportive people who reflect positive attitudes regarding the individual promotes a positive sense of self.
>Individuals who have a sense of their self-image and are willing to look at
themselves realistically will be able to progress in the desire to improve.
>Promotes trusting situation in which client is free to be open and honest with self and others.
The patient verbalized sense of self-concept, as verbalized by “handa naman ako sa operasyon”
INTERVENTION RATIONALE
>Accepted client’s perception or view of current status.
>Discussed what behavior does foe client.
>Given reinforcement for progress note.
>Allowed client to progress at own rate.
>Emphasized importance of grooming and personal hygiene.
>Prepared patient and family members for the operation.
>Avoids threatening existing self-esteem and provides opportunity for client to develop realistic plan for improving self-concept.
>Encouraged thinking about what inner motivations are and what actions can be taken to enhance self-esteem.
>Positive words of encouragement support development of effective coping behaviors.
>Adaptation to a change in self-concept depends on it’s significance to the individual and disruption to lifestyle.
>Looking your best improves sense of self-esteem and presenting a positive appearance enhances how others see you.
>Operation are required and family must be prepared.
NANDA
Nursing Care Plan Guidelines for Individualizing Client Care Across Lifespan
DRUG STUDY
NAME OF DRUGMECHANISM OF
ACTIONINDICATION CONTRAINDICATION
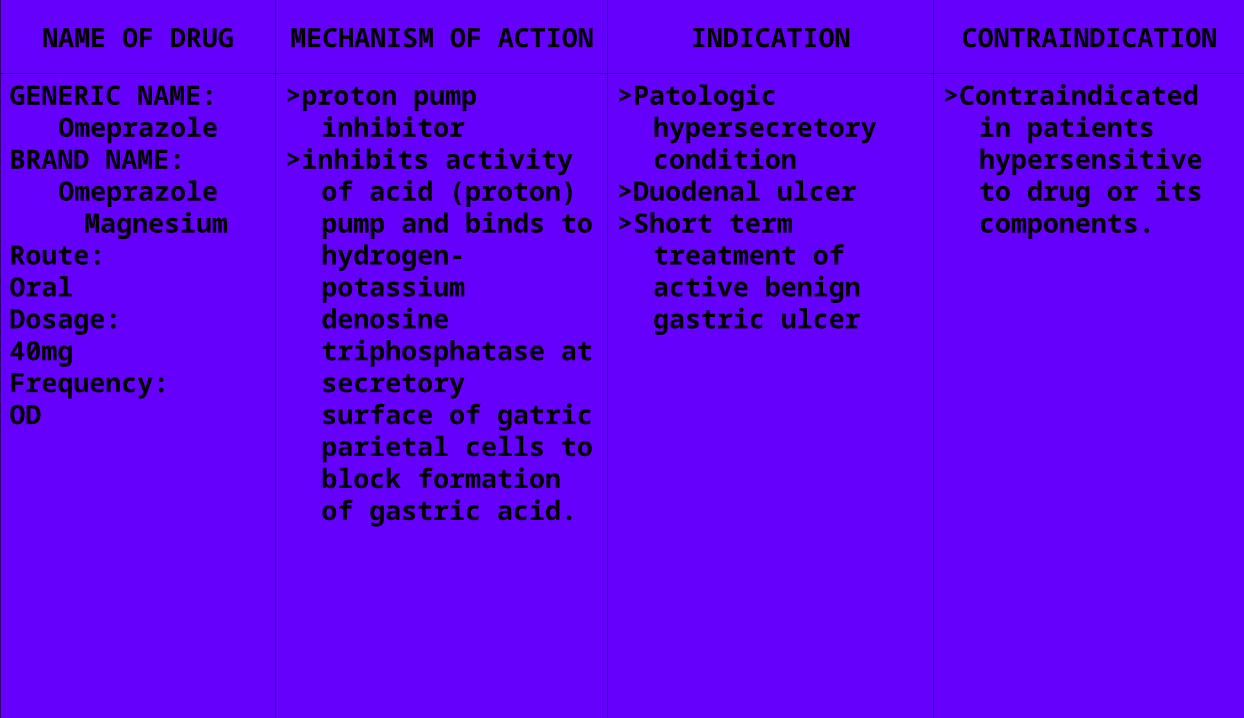
GENERIC NAME: Omeprazole
BRAND NAME:Omeprazole
MagnesiumRoute:OralDosage:40mgFrequency:OD
>proton pump inhibitor>inhibits activity of acid
(proton) pump and binds to hydrogen-potassium denosine triphosphatase at secretory surface of gatric parietal cells to block formation of gastric acid.
>Patologic hypersecretory condition
>Duodenal ulcer>Short term treatment
of active benign gastric ulcer
>Contraindicated in patients hypersensitive to drug or its components.
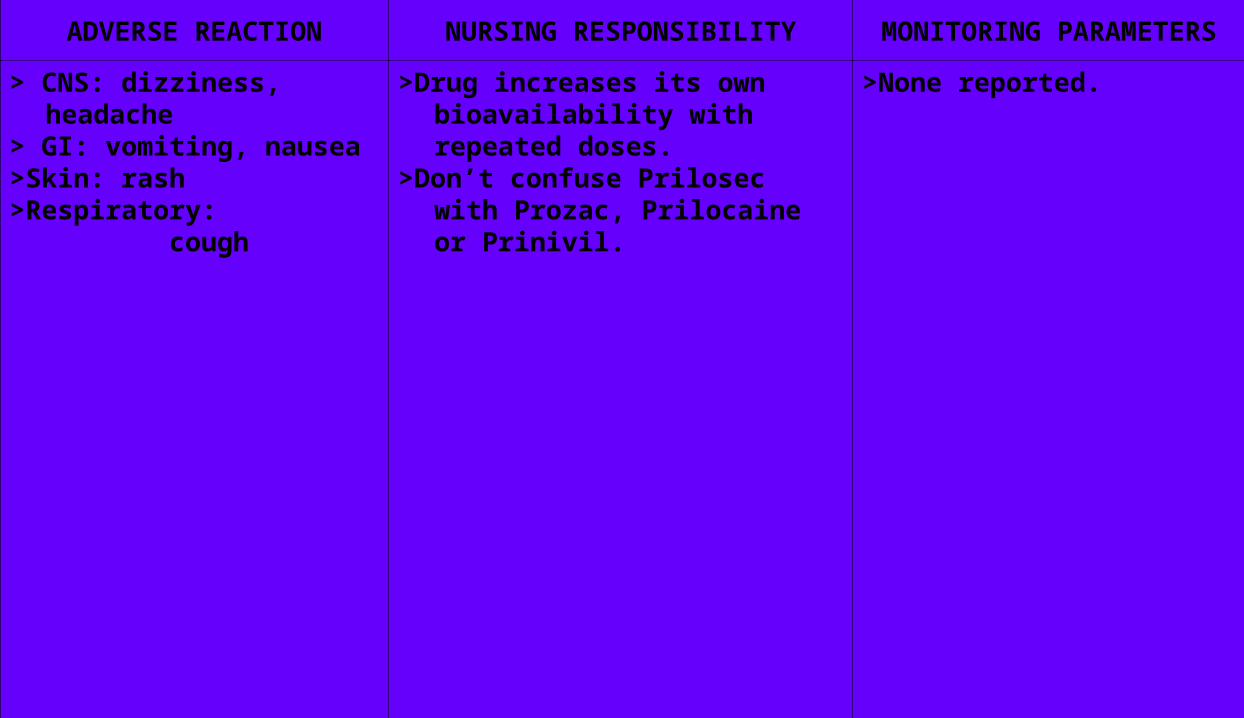
ADVERSE REACTION NURSING RESPONSIBILITY MONITORING PARAMETERS
> CNS: dizziness, headache> GI: vomiting, nausea>Skin: rash>Respiratory: cough
>Drug increases its own bioavailability with repeated doses.
>Don’t confuse Prilosec with Prozac, Prilocaine or Prinivil.
>None reported.
NAME OF DRUGMECHANISM OF
ACTIONINDICATION CONTRAINDICATION
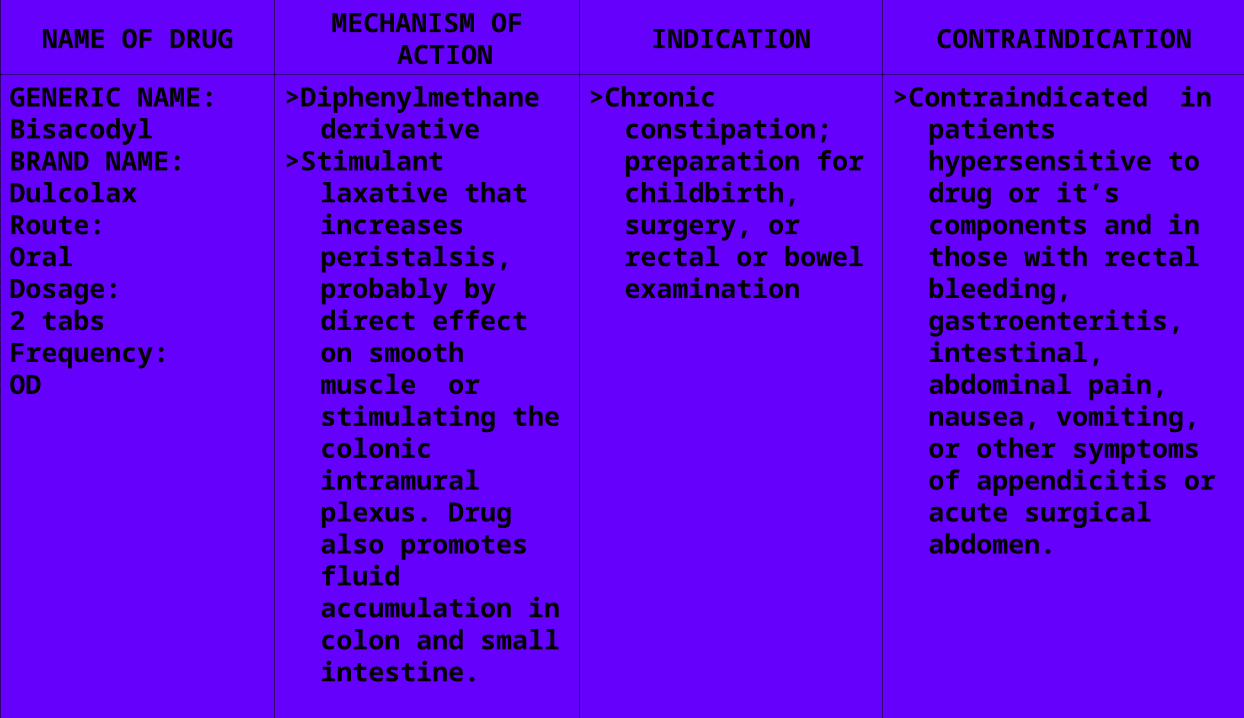
GENERIC NAME: BisacodylBRAND NAME:DulcolaxRoute:OralDosage:2 tabsFrequency:OD
>Diphenylmethane derivative
>Stimulant laxative that increases peristalsis, probably by direct effect on smooth muscle or stimulating the colonic intramural plexus. Drug also promotes fluid accumulation in colon and small intestine.
>Chronic constipation; preparation for childbirth, surgery, or rectal or bowel examination
>Contraindicated in patients hypersensitive to drug or it’s components and in those with rectal bleeding, gastroenteritis, intestinal, abdominal pain, nausea, vomiting, or other symptoms of appendicitis or acute surgical abdomen.
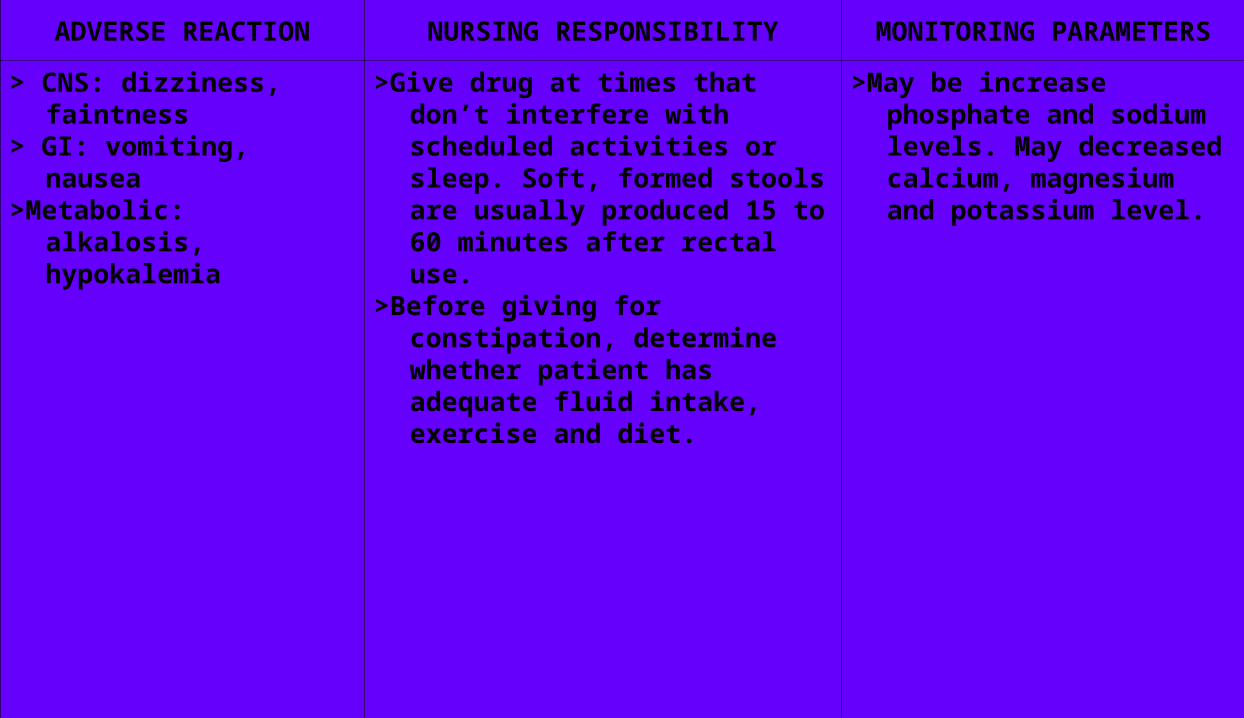
ADVERSE REACTION NURSING RESPONSIBILITY MONITORING PARAMETERS
> CNS: dizziness, faintness
> GI: vomiting, nausea>Metabolic: alkalosis,
hypokalemia
>Give drug at times that don’t interfere with scheduled activities or sleep. Soft, formed stools are usually produced 15 to 60 minutes after rectal use.
>Before giving for constipation, determine whether patient has adequate fluid intake, exercise and diet.
>May be increase phosphate and sodium levels. May decreased calcium, magnesium and potassium level.
NAME OF DRUGMECHANISM OF
ACTIONINDICATION CONTRAINDICATION
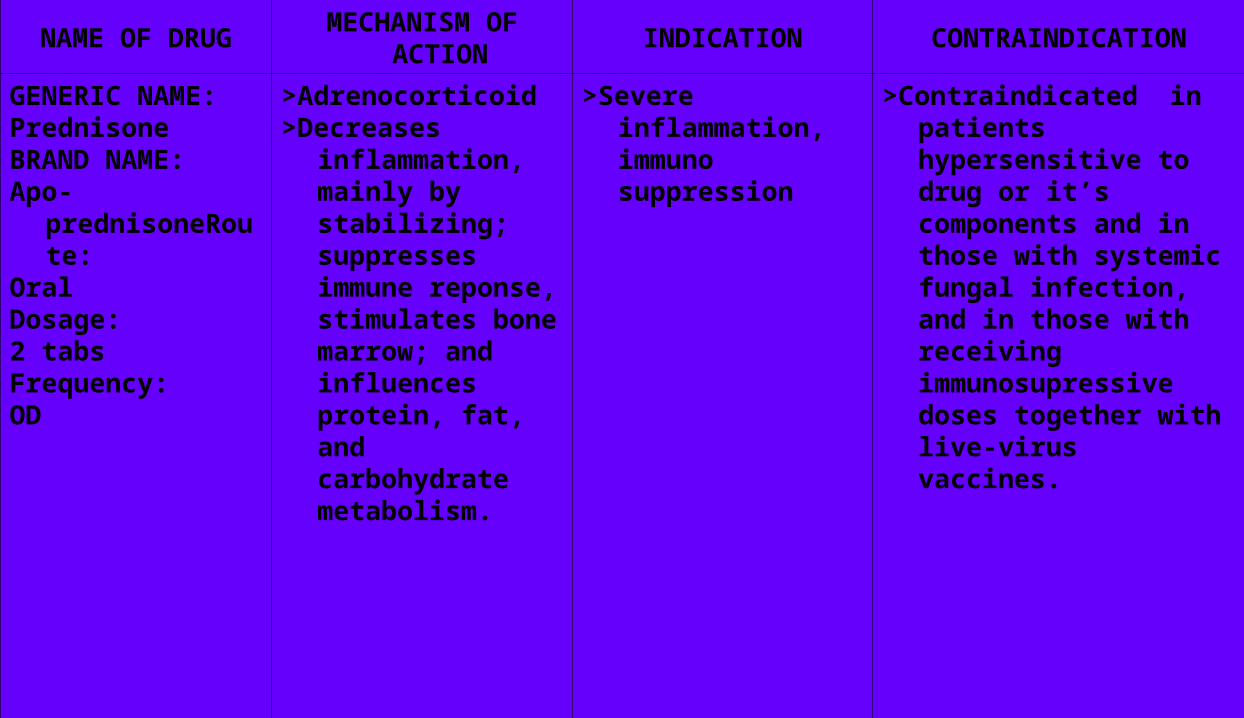
GENERIC NAME: PrednisoneBRAND NAME:Apo-
prednisoneRoute:
OralDosage:2 tabsFrequency:OD
>Adrenocorticoid>Decreases
inflammation, mainly by stabilizing; suppresses immune reponse, stimulates bone marrow; and influences protein, fat, and carbohydrate metabolism.
>Severe inflammation, immuno suppression
>Contraindicated in patients hypersensitive to drug or it’s components and in those with systemic fungal infection, and in those with receiving immunosupressive doses together with live-virus vaccines.
ADVERSE REACTION NURSING RESPONSIBILITY MONITORING PARAMETERS
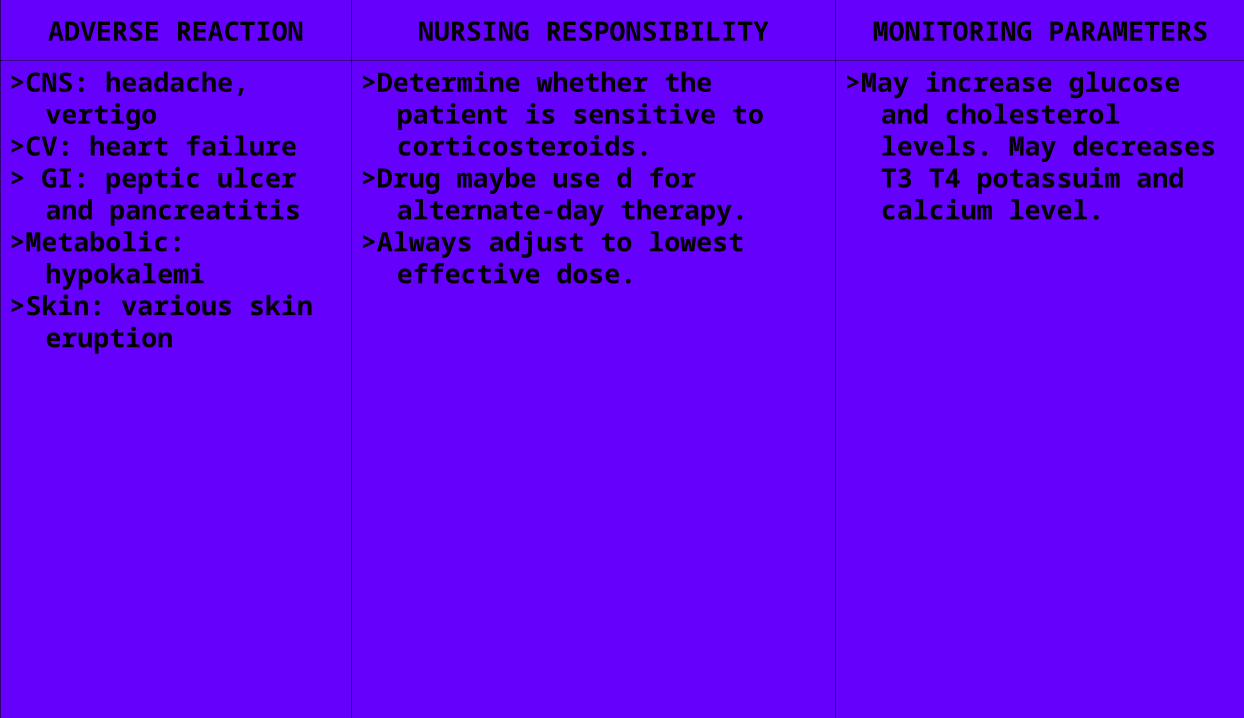
>CNS: headache, vertigo>CV: heart failure> GI: peptic ulcer and
pancreatitis>Metabolic: hypokalemi>Skin: various skin
eruption
>Determine whether the patient is sensitive to corticosteroids.
>Drug maybe use d for alternate-day therapy.
>Always adjust to lowest effective dose.
>May increase glucose and cholesterol levels. May decreases T3 T4 potassuim and calcium level.
PROGNOSIS
The prognosis is good because the surgery was successful and
the patient was able to do some of her activities in daily living.
Because of the continuous care that is given to the client, Child X’s condition has improved.

DISCHARGE PLANNING
M
Instructed the significant others to give home medications that the physician will prescribe upon discharge.
>Omeprazole 40 mg OD
>Dulcolax 2 tabs OD
>Prednisone 2 tabs OD
E
Avoid strenuous activities due to surgery. Emphasized the importance of quiet and healthy environment.
T
Encouraged the patient to take the medicine on time and take the medicine after meal.
H
>Advised the patient and the mother to provide good hygiene like cleaning the nails and ears.
>Advised the significant others to provide good personal hygiene of the client.
O
Encouraged to have a follow-up check-up after one week to Dr. Arellano, Dr. Gonzales and Dr. Reyes.
D
Advised the patient to eat foods rich in protein , carbohydrates and calcium. Avoid eating sour and salty foods. Avoid also too much soft drinks and increase fluid intake.
S
Advised whole family to keep their faith in GOD and never forget to ask guidance and support from our Lord.
ACKNOWLEDGEMENTACKNOWLEDGEMENT
I would like to extend my heartfelt thanks to the following people that with their presence, the accomplishment of this case study and presentation will not be possible.
To the Almighty One for giving me the strength, knowledge and power.
To my parents and friend for continuously supporting me financially and emotionally.
To my clinical instructor Mrs. Iturralde for professionally guiding us throughout the accomplishment study and for spending time and ideas with us.
To the staff of the IMC for letting me, lend books and assisting me in all I needs without hesitations.
To my classmate for their cooperation and for giving extra information even in the smallest thing that they know.

THANK YOU THANK YOU VERY MUCH VERY MUCH
AND GOD BLESSAND GOD BLESS

BIBLIOGRAPHYBIBLIOGRAPHY

Applying Nursing Process, Alfaro- Le Fevre Rosalinda, pg. 207
Current Diagnosis and treatment,Marcus A.Krupp and Milton J. Chatton
Delmar’s Pediatric Nursing Care Plans, 3rd edition,Luxner
Health Assesment & Physical Examination, Estes
Health Assesment in Nursing 3rd edition, Janet Weber & Jane Kelley
Human Anatomy and Physiology, Hole,Jr,et.al, 6th edition.
Ignatius, et.al.
Laboratory and diagnostic tests with nursing implications Seventh Edition,Joyce
Medical-surgical nursing, Smeltzer,et al.
Medical- Surgical Nursing Critical Thinking for collaborative care, vol.1,5th edition,
Medical-Surgical, 6th edition, Burner et al, pg 468-469
MIMS 107th edition 2006
Medical-Surgical Nursing, Brunner and Suddharts, Smeltzer,vol.1 & 2
Nursing Care Plan,7th edition, Doenges, et.al
Nurses’ Pocket Guide 11th edition, by Donges et. Al.
Nursing Care Plans; 6th edition, Donenges et. Al, pg. 130.
Nursing Care Plan, Meg Gulanck,et. Al, pg. 3
Pediatric Nursing Care Plan, Axton, et. Al, pg. 296-300

NURSINGPROCESS
The nursing process is an organized, systematic approach used by medical-surgical nurses to meet the individualized health care needs of their clients, families and communities. The term nursing process emerged in the mid-1960s. As nursing became more recognized and respected as a profession, there was a growing need to define more clearly what nurses do.
OBJECTIVE
Identify the steps of the nursing process
Nurses apply the Nursing Process as a competency when delivering care
This is a DYNAMIC, CONTINUOUS process which allows for a nurse to modify care as needed

PURPOSE
Purpose: A nurse follows the nursing process to organize and deliver nursing care
Use of the process allows the nurse to integrate elements of critical thinking to make judgments and take actions based on reason
The nursing process is a variation of scientific reasoning that allows nurses to organize and systematize nursing practice
STEPS STEPS OF THEOF THE
NURSING NURSING PROCESSPROCESS
STEPS
I. Assessment
II. Nursing diagnosis
III. Planning
IV. Implementation
V. Evaluation
ASSESSMENTASSESSMENT
ASSESSMENT
This is the first step of the nursing process. It involves the systematic and continuous collection, validation (evaluation) and selection of data. Data is collected from a variety of sources (clients, families, health records, physicians, nurses, and other healthcare professionals). Data collection guidelines reflect the CSUB Department of Nursing Conceptual Model. Activities include: (1) establishing the database (nursing history, physical assessment, review of the patient/client’s record and nursing literature, and consultation with patient/client’s support persons and healthcare professionals); (2) continuously updating the database; (3) validating data; and (4) communicating data.
TWO STEPS OF NURSING ASSESSMENT
1. Collection and verification of data from a primary source (client) and secondary sources (family, health professionals, medical record)
2. Analysis of all data as a basis for developing nursing diagnoses and an individualized plan of care for the client
Assessment • When beginning an assessment, it is helpful for the nurse to organize
the assessment process and determine which data must be collected• Assessment data must be descriptive, concise, and complete
Types of data: • – Subjective-client’s perceptions• – Objective-observations or measurements made by the data
collector
SOURCE OF DATA
• Subjective: from the client, family, significant others, health care team members, and health records
• Objective: physical examination, diagnostic and laboratory test results, pertinent nursing and medical literature
• Usually the client is the best source of information
Subjective-Client Interview
• Interview the client
• An interview is an organized conversation with the clients to obtain the client’s health history and information about the current illness

Phases of the interview-orientation, working, and termination
• Schedule interviews around interruptions if possible, and in a conducive atmosphere
• Use open-ended questions, back channeling, problem seeking interview techniques, and close ended questions for symptom clarification
Nursing Health History
• The nursing health history is data collected about the client’s current level of wellness, including a review of body systems, family and health history, socio-cultural history, spiritual health, and mental and emotional reactions to illness
• Obtained during an interview
NURSING HEALTH HISTORY-COMPONENTS
• Biographical Information
• Reason for Seeking Health Care
• Client Expectations
• Present Illness or Health Concerns
• Health History
• Family History
• Environmental History
• Psychosocial History
• Spiritual Health
• Review of Systems
PHYSICAL EXAM• Vital signs are taken
• Other objective measurements are taken
• (ht, wt, VS, general survey)
• All body systems are examined in a systematic manner
• head to toe physical examination of all body systems
• Assessment –Formulating Nursing Judgments
• The successful interpretation of assessment data requires critical thinking
• After gathering data, the nurse validates the collected information to ensure its accuracy
• After validating and interpreting assessment data, the nurse organizes the information into meaningful clusters, keeping in mind the client’s response to illness (a cluster is a set of signs or symptoms that are grouped together in a logical order)

NURSING DIAGNOSIS
NURSING DIAGNOSIS
From the assessment of functional health patterns human response patterns are identified and classified according to statements of actual, high risk and possible problems, and wellness diagnoses (Carpenito, 1993). It requires data analysis to identify the patient/client’s strengths and health problems that independent nursing interventions can resolve. Activities include: (1) interpreting and analyzing patient/client data; (2) identifying patient/client strengths and health problems; (3) formulating and validating nursing diagnoses; and (4) developing a prioritized list of nursing diagnoses.

PURPOSE OF NURSING DIAGNOSIS
• Nursing diagnoses offer a language to promote understanding between nurses about clients’ health problems to facilitate communication and care planning
• Nursing diagnoses distinguish the nurse’s role from that of the physician
• Nursing diagnoses help nurses to focus on the role of nursing in client care
• Diagnostic Process
_ Includes decision-making steps
– Gathering the assessment database
– Validating data
– Analyzing and interpreting data
– Identifying client needs
– Formulating the nursing diagnoses

FORMULATION OF THE NURSING DIAGNOSIS
• Actual nursing diagnosis: describes human responses to health conditions/life processes that exists in an individual, family, or community
• Risk nursing diagnosis: describes human responses to health conditions/life processes that may develop in a vulnerable individual, family, or community
• Wellness nursing diagnosis: describes human responses to levels of wellness in an individual, family, or community that have a readiness for enhancement

NURSING DIAGNOSIS-COMPONENTS
• Diagnostic label-name of the nursing diagnosis as approved by NANDA, often includes descriptors (nursing assessment data must support the diagnostic label)
• Related factors-causative or other contributing factors that have influenced the client’s actual or potential response to the health problem, and can be changed by nursing interventions (related factors must support the etiology)
• Definition-approved NANDA definition for each diagnosis following clinical use and testing; the definition describes the characteristics of the human response identified
• Risk Factors-environmental, physiological, psychological, genetic, or chemical elements that increase the vulnerability of an individual, family, or community to an unhealthful event
SOURCE OF DIAGNOSTIC ERRORS
• Errors in data collection
• Errors in interpretation and analysis of data
• Errors in data clustering
• Errors in the diagnostic statement
Avoiding and Correcting Errors
• Identify the client’s response, not the medical diagnosis
• Identify a NANDA Int. diagnostic statement rather than the symptom
• Identify a treatable etiology rather than a clinical sign or chronic problem
• Identify the problem caused by the treatment or diagnostic study rather than the treatment or study itself

MORE AVOIDING & CORRECTING ERRORS
• Identify the client response to the equipment rather then the equipment itself
• Identify the client’s problems rather than the nurse’s problems
• Identify the client problems rather than the nursing intervention
• Identify the client problem rather than the goal
• Make professional rather then prejudicial judgments
More Avoiding and Correcting Errors
• Avoid legally inadvisable statements
• Identify the problem and etiology
• Identify only one client problem in the diagnostic statement

PLANNINGPLANNING

PLANNING
Specification of client goals to promote health and/or prevent, reduce, or resolve the problems that are identified in the nursing diagnoses, and related nursing interventions. Implementation strategies address the patient/client’s health state and aim to facilitate attaining the desired outcomes. Implementation encompasses four levels of care: preventive, supportive, restorative and rehabilitative. Activities include: (1) establishing priorities; (2) writing goals and developing an evaluative strategy; (3) selecting nursing measures; (4) communicating the plan of nursing care.
PLANNING• Priorities are classified as high, intermediate, or low
• Goals: should be realistic and based on client needs and resources; client participation in goal setting is ideal
• A client-centered goal is a specific and measurable behavior or response that reflects a client’s highest possible level of wellness and independence in function
Planning
• Short term goal: an objective that is expected to be achieved within a short time frame, usually less than a week
• Long term goal: an objective that is expected to be achieved over a longer time frame, usually over weeks or months
• Expected outcome: specific measurable change in a client’s status that is expected to occur in response to nursing care
GUIDELINES FOR WRITING GOALS
• Client centered
• Singular goal or outcome
• Observable
• Measurable
• Time-limited
• Mutual factors
• Realistic

NURSING NURSING INTERVENTIONINTERVENTION

INTERVENTION
Implementing the plan of care. Activities include: (1) carrying out the plan of care; (2) continuing data collection and modifying the plan of care as needed; (3) documenting the care given.
TYPES OF INTERVENTION
Nursing interventions are any treatment or action, based upon clinical judgment and knowledge, that nurses perform to enhance clients’ outcomes
Three categories of nursing interventions:• – Nurse-initiated interventions• – Physician-initiated interventions• – Collaborative interventions

TYPES OF INTERVENTION• Nurse-initiated interventions are the independent response of the
nurse to the client’s health care needs and nursing diagnoses.
• Physician-initiated interventions are based on a physician’s response to treat or manage a medical diagnosis.
• Collaborative interventions are therapies that require the knowledge, skill, and expertise of multiple health care professionals.
Choosing interventions
• The nurse does not select interventions haphazardly. The nurse deliberates about six important factors:
1. characteristics of the nursing diagnosis
2. expected outcomes
3. research base, or nursing knowledge for interventions
4. feasibility of the intervention
5. acceptability to the client, and
6. competencies of the nurse
EVALUATIONEVALUATION
EVALUATION
Measures the extent to which the patient/client has achieved the goals specified in the plan of care, and identifies the factors that positively or negatively influenced goal achievement. The plan of care is revised as necessary. Activities include: (1) measuring how well the client has achieved the desired goals; (2) identifying factors that contributed to the client’s success or failure; (3) modifying the plan of care (if indicated).
NURSING CARE NURSING CARE PLANPLAN
NURSING CARE PLAN
• A nursing care plan is a guide for clinical care
• A written care plan is designed to direct clinical care and to decrease the risk of incomplete, incorrect, or inaccurate care
• It is organized so that any nurse can quickly identify the client’s nursing diagnoses, goals, and outcomes, and nursing interventions to be delivered
• It can help identify and coordinate resources used to deliver nursing care

STUDENT CARE PLAN
• Nursing students learn to write and use a nursing care plan as part of their education
• By using a nursing care plan, students can apply the knowledge gained from nursing and medical literature and the classroom to a practice situation
• The nurse enters a scientific rationale for a specific intervention
• Scientific rationale: the reason that, based on supporting literature, a specific nursing action was chosen
THANK YOU MAMTHANK YOU MAMGOD BLESSGOD BLESS

![Pancreatic endometrial cyst mimics mucinous cystic neoplasm of … · 2017. 4. 29. · The most common sites of endometriosis are the pelvic organs[5]; however, endometriosis of the](https://img.pdfslide.us/doc/110x75/6117aa33d0c6a51c5b69412a/pancreatic-endometrial-cyst-mimics-mucinous-cystic-neoplasm-of-2017-4-29-the.jpg)


























