-
8/7/2019 Pancreatic Injuries
1/42
PANCREATIC INJURIESPANCREATIC INJURIES
-
8/7/2019 Pancreatic Injuries
2/42
Pancreatic traumaPancreatic trauma
Pancreatic trauma can occur after directPancreatic trauma can
occur after direct
abdominal traumaabdominal trauma
Incidence 2Incidence 2--10% in major trauma10% in major
trauma
Seen in 20Seen in 20--30% penetrating abdominal wounds30%
penetrating abdominal wounds
Stabbing from back can cause itStabbing from back can cause
it
-
8/7/2019 Pancreatic Injuries
3/42
Pancreatic traumaPancreatic trauma
High mortality and morbidityHigh mortality and morbidity
Mortality 12Mortality 12--23%23% Mortality rises dramatically
with shock and otherMortality rises dramatically with shock and
other
organs traumaorgans trauma
-
8/7/2019 Pancreatic Injuries
4/42
Pancreatic traumaPancreatic trauma
Morbidity 30Morbidity 30 49%49%
Necrosis, hemorrhage, abscess, fistula,Necrosis, hemorrhage,
abscess, fistula,
pseudocystpseudocyst
Endocrine 20%Endocrine 20%
Morbidity >60% when diagnosis is delayedMorbidity >60%
when diagnosis is delayed
Main pancreatic duct rupture seen in 1.6% bluntMain pancreatic
duct rupture seen in 1.6% blunt
traumatrauma
-
8/7/2019 Pancreatic Injuries
5/42
Associated injuriesAssociated injuries
9090--9595% have other injuries% have other injuries Liver
42Liver 42--32%32%
Spleen 25Spleen 25--40%40%
Stomach 20Stomach 20--40%40% Major vessel 25Major vessel
25--35%35%
Thorax 22Thorax 22--31%31%
Bowel 10Bowel 10--29%29%
CNS 25%CNS 25%
Duodenum 18%Duodenum 18%
-
8/7/2019 Pancreatic Injuries
6/42
ANATOMYANATOMY
-
8/7/2019 Pancreatic Injuries
7/42
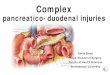
Blood supplyBlood supply
ARTERIALARTERIALMultiple branches from celiac nd
S.M.ArteryMultiple branches from celiac nd S.M.Artery
Pancreaticoduodenal arteriesPancreaticoduodenal arteries
Branches from Splenic arteryBranches from Splenic
arteryVENOUSVENOUS
--Direct into PORTAL veinDirect into PORTAL vein
--pancreaticoduodenal vein join
gastroepiploicpancreaticoduodenal vein join gastroepiploicvein to
form common venous trunk TO SMVvein to form common venous trunk TO
SMV
--Body and tail drain into splenic veinBody and tail drain into
splenic vein
--Inferior arcade to IMVInferior arcade to IMV
-
8/7/2019 Pancreatic Injuries
8/42
Pancreas with accessory pancreatic ductPancreas with accessory
pancreatic duct
-
8/7/2019 Pancreatic Injuries
9/42
-
8/7/2019 Pancreatic Injuries
10/42
ImagingImaging
CTCT
USUS
MRCPMRCP ERCPERCP
Serum amylase elevated in 73Serum amylase elevated in
73--82%82%
Amylase also elevated with bowel injury andAmylase also elevated
with bowel injury andrenal failurerenal failure
-
8/7/2019 Pancreatic Injuries
11/42
Acute CT findingsAcute CT findings
Direct findingsDirect findingsPancreatic enlargementPancreatic
enlargement
LacerationLaceration
Inhomogeneous enhancementInhomogeneous enhancement Secondary
findingsSecondary findings
Peripancreatic strandingPeripancreatic stranding
Peripancreatic fluid collectionPeripancreatic fluid
collectionFluid between splenic vein and pancreasFluid between
splenic vein and pancreas
HaemorrhageHaemorrhage
-
8/7/2019 Pancreatic Injuries
12/42
Acute CT findingsAcute CT findings
Pancreatic duct disruption often not appreciatedPancreatic duct
disruption often not appreciated
Sensitivity 40Sensitivity 40--69%69%
Other injury may obscure pancreatic findingsOther injury may
obscure pancreatic findings
-
8/7/2019 Pancreatic Injuries
13/42
GRADE-I Contusion Superficial laceration not involving duct
-
8/7/2019 Pancreatic Injuries
14/42
GRADE - I
-
8/7/2019 Pancreatic Injuries
15/42
GRADEGRADE -- II
-
8/7/2019 Pancreatic Injuries
16/42
GRADE - II Laceration disrupting the main ductin the body or
tail
-
8/7/2019 Pancreatic Injuries
17/42
GRADE - II
-
8/7/2019 Pancreatic Injuries
18/42
GRADE - III
Crushing or transection of the head Duodenum intact
-
8/7/2019 Pancreatic Injuries
19/42
GRADEGRADE -- IIIIII
-
8/7/2019 Pancreatic Injuries
20/42
GRADEGRADE -- IIIIII
-
8/7/2019 Pancreatic Injuries
21/42
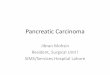
GRADE - IVCrushing or transection of Pancreatic head and
duodenum injury
-
8/7/2019 Pancreatic Injuries
22/42
GRADEGRADE -- IVIV
-
8/7/2019 Pancreatic Injuries
23/42
GRADEGRADE -- IVIV
-
8/7/2019 Pancreatic Injuries
24/42
GRADEGRADE -- IVIV
-
8/7/2019 Pancreatic Injuries
25/42
MANAGEMENT OFMANAGEMENT OF
PANCREATIC TRAUMAPANCREATIC TRAUMA
Depends upon location of injuryDepends upon location of injury[
BY CT ][ BY CT ]
Whether or not pancreatic duct is injuredWhether or not
pancreatic duct is injured
-
8/7/2019 Pancreatic Injuries
26/42
DIAGNOSING PANCREATICDIAGNOSING PANCREATIC
DUCT INJURYDUCT INJURY NO IDEAL METHOD EXISTS FORNO IDEAL METHOD
EXISTS FOR
IDENTIFYINGDUCCTAL INURIESIDENTIFYINGDUCCTAL INURIES
Operative pancreatography throughOperative pancreatography
through
duodenotomy or following resection of tail ofduodenotomy or
following resection of tail of
pancreaspancreas
Passing of Coronary artery dilator into duct viaPassing of
Coronary artery dilator into duct via
papillapapilla
ERPERP
-
8/7/2019 Pancreatic Injuries
27/42
LOCATION OF PANCREATICLOCATION OF PANCREATIC
INJURYINJURYTAILTAIL
BODYBODY
NECKNECK
HEADHEAD
-
8/7/2019 Pancreatic Injuries
28/42
TAIL,BODY AND NECK INJURIESTAIL,BODY AND NECK INJURIES
WITH DUCT TRANSECTEDWITH DUCT TRANSECTED
Distal pancreatectomy with splenectomyDistal pancreatectomy with
splenectomy
Distal pancreatectomy with spleen perservationDistal
pancreatectomy with spleen perservation
Conserving distal pancreas and spleen with RouxConserving distal
pancreas and spleen with Roux--enen--Y LimbY Limb
-
8/7/2019 Pancreatic Injuries
29/42
Pancreatic head andduct injuryPancreatic head andduct injury
-
8/7/2019 Pancreatic Injuries
30/42
RouxRoux--enen--YY panreatojejunostomypanreatojejunostomy
-
8/7/2019 Pancreatic Injuries
31/42
GRADEGRADE IV INJURYIV INJURY
HEAD OF PANCREAS AND DUODENALHEAD OF PANCREAS AND DUODENAL
INJURYINJURY
-
8/7/2019 Pancreatic Injuries
32/42
-
8/7/2019 Pancreatic Injuries
33/42
GASTROJEJUNOSTOMY WITHGASTROJEJUNOSTOMY WITH
DUODENUM REPAIR AND FEEDINGDUODENUM REPAIR AND FEEDING
JEJUNOSTOMYJEJUNOSTOMY
-
8/7/2019 Pancreatic Injuries
34/42
WHIPPLES PROCEEDUREWHIPPLES PROCEEDURE
INDICATIONS OF WHIPPLES ININDICATIONS OF WHIPPLES IN
PANCREA TIC TRAUMAPANCREA TIC TRAUMA
Injury to CBD and pancreatic duct in head ofInjury to CBD and
pancreatic duct in head of
pancreaspancreas
A
vulsion of papilla of vater from duodenumA
vulsion of papilla of vater from duodenum Destruction of entire
2Destruction of entire 2ndnd part of duodenumpart of duodenum
-
8/7/2019 Pancreatic Injuries
35/42
WHIPPLES PROCEEDUREWHIPPLES PROCEEDURE
INDICATIONS OF WHIPPLES ININDICATIONS OF WHIPPLES IN
MALIGNANCIESMALIGNANCIES
Malignant tumors affecting duodenumMalignant tumors affecting
duodenum
Head of pancreasHead of pancreasDistal part of bile ductDistal
part of bile duct
-
8/7/2019 Pancreatic Injuries
36/42
WHIPPLES PROCEEDUREWHIPPLES PROCEEDURE
-
8/7/2019 Pancreatic Injuries
37/42
WHIPPLE[ BEFORE ]WHIPPLE[ BEFORE ]
-
8/7/2019 Pancreatic Injuries
38/42
WHIPPLE [ AFTER ]WHIPPLE [ AFTER ]
-
8/7/2019 Pancreatic Injuries
39/42
COMLICATIONSCOMLICATIONS
NecrosisNecrosis
HaemorrhageHaemorrhage
AbscessAbscess PseudocystPseudocyst
FistulaFistula
Diabetes mellitusDiabetes mellitus Pancreatic
insufficiencyPancreatic insufficiency
PSEUDOCYSTPSEUDOCYST
-
8/7/2019 Pancreatic Injuries
40/42
PSEUDOCYSTPSEUDOCYST
WALLED OF COLLECTIONWALLED OF COLLECTIONOF SECRETIONSOF
SECRETIONS
-
8/7/2019 Pancreatic Injuries
41/42
CONCLUSIONCONCLUSION
Signs on admission CT may be easily overlookedSigns on admission
CT may be easily overlooked
CT tends to under stage pancreatic injuriesCT tends to under
stage pancreatic injuries Pancreatic duct disruption not well seen
on CTPancreatic duct disruption not well seen on CT
Delayed diagnosis has worse prognosisDelayed diagnosis has worse
prognosis
Surgery indicated for majorSurgery indicated for major splspl
pancreatic headpancreatic headtraumatrauma
MRCP and ERCP useful to assess ductMRCP and ERCP useful to
assess duct
-
8/7/2019 Pancreatic Injuries
42/42