Embed Size (px)
Citation preview


Pain: Why treat it?Pain: Why treat it?
HumanitarianHumanitarian
JCAHO (2001)JCAHO (2001)
Blunt autonomic and somatic response to painBlunt autonomic and somatic response to pain
- Elevated metabolic rate- Elevated metabolic rate
- Elevated O2 consumption- Elevated O2 consumption
- Hypercoagulability- Hypercoagulability
- Altered immune status- Altered immune status
- Development of chronic pain- Development of chronic pain

Pain: Why Don’t We Treat It Well?Pain: Why Don’t We Treat It Well?
Lack of concern/caringLack of concern/caring Lack of knowledgeLack of knowledge Uniform prescribing practicesUniform prescribing practices Fear of side effectsFear of side effects Fear of addictionFear of addiction

ArmamentariumArmamentarium
Guided imagery (!)Guided imagery (!) Patient educationPatient education NarcoticsNarcotics NSAIDsNSAIDs Gaba agonistsGaba agonists Local/regional anestheticsLocal/regional anesthetics ““Preemptive” treatmentPreemptive” treatment ““Procedure specific” – Prospect websiteProcedure specific” – Prospect website

Local anestheticsLocal anesthetics
Dose-dependent blockage of sodium Dose-dependent blockage of sodium channels in neuronschannels in neurons
Amides and esters (amides less allergenic)Amides and esters (amides less allergenic)
Amides:Lidocaine, bupivacaine, prilocaineAmides:Lidocaine, bupivacaine, prilocaine
Esters: NovocaineEsters: Novocaine
Lidocaine dosing: 5 mg/kg without epiLidocaine dosing: 5 mg/kg without epi
7 mg with epi7 mg with epi

NSAIDSNSAIDS
Conventional Cox inhibitorsConventional Cox inhibitors Cox 2 inhibitorsCox 2 inhibitors
Decreased incidence of GI bleedingDecreased incidence of GI bleeding
Didn’t inhibit platelet aggregationDidn’t inhibit platelet aggregation
Initial data on side effects was on usage for Initial data on side effects was on usage for greater than 1-2 yearsgreater than 1-2 years
Now some data on side effects as Now some data on side effects as analgesics for CABG patientsanalgesics for CABG patients

Gabapentin/PregabalinGabapentin/Pregabalin
How do they work?How do they work? Who knows?Who knows?
Presynaptic binding to calcium channels in Presynaptic binding to calcium channels in brainbrain
Decrease excitatory transmissionDecrease excitatory transmission

NarcoticsNarcotics
MorphineMorphine FentanylFentanyl HydromorphoneHydromorphone All work on mu receptorsAll work on mu receptors
Decrease responsiveness of resp center to CO2Decrease responsiveness of resp center to CO2 Stimulate medullary chemoreceptor trigger zone Stimulate medullary chemoreceptor trigger zone Increase sphincter tone and decrease peristalsisIncrease sphincter tone and decrease peristalsis

Opiate Analgesic Options: Fentanyl, Opiate Analgesic Options: Fentanyl, Morphine, HydromorphoneMorphine, Hydromorphone
FentanylFentanyl HydromorphoneHydromorphone MorphineMorphine
Rapid onsetRapid onset XX
Rapid offsetRapid offset X*X*
Avoid in renal diseaseAvoid in renal disease X**X**
Preload reductionPreload reduction XX
Avoid in hemodynamic Avoid in hemodynamic instabilityinstability
XX
Equivalent dosesEquivalent doses 100 mcg100 mcg 1.5 mg1.5 mg 10 mg10 mg
* Offset prolonged after long-term use
** Active metabolite accumulation causes excessive narcosis

Rescue/Bolus DosesRescue/Bolus Doses
MSO4 0.1 mg-0.3 mg/kg IV (70 kg – 7-21 MSO4 0.1 mg-0.3 mg/kg IV (70 kg – 7-21 mg IV!!!) – I give 5mg IV!!!) – I give 5
Fentanyl 25-200 mg IVFentanyl 25-200 mg IV Dilaudid 0.01-0.03 mg/kg IV (70 kg – .7-Dilaudid 0.01-0.03 mg/kg IV (70 kg – .7-
2.1 mg IV)2.1 mg IV)

PCAPCA
MSO4 MSO4 Dose 1.5 mgDose 1.5 mg Lockout 7 minLockout 7 min 4 hr limit 30 4 hr limit 30 How do you adjust?How do you adjust?

PCAPCA
FentanylFentanyl Dose 20 mcgDose 20 mcg Lockout 7 minLockout 7 min 4 hour dose 300 mcg4 hour dose 300 mcg When do you use it?When do you use it?

PCAPCA
DilaudidDilaudid Dose 0.2 mgDose 0.2 mg Lockout 7 mgLockout 7 mg 4 hr limit 3 mg4 hr limit 3 mg

Case 1Case 1
36 y.o morbidly obese woman with RUQ 36 y.o morbidly obese woman with RUQ pain at 20 hrs, RUQ tenderness, WBC 13, pain at 20 hrs, RUQ tenderness, WBC 13, US with stones, wall 5.0 mmUS with stones, wall 5.0 mm
What’s she got?What’s she got?
How will we manage her pain? What are How will we manage her pain? What are our Prospects?our Prospects?

Case 1Case 1

Case 2Case 2
65 y.o. man with COPD here for 65 y.o. man with COPD here for esophageal canceresophageal cancer
What operation is he going to get?What operation is he going to get?


Epidural AnesthesiaEpidural Anesthesia
What is good about it?What is good about it? Decreases risk of DVTDecreases risk of DVT Increases risk of graft thrombosisIncreases risk of graft thrombosis Decreases post op ileus in upper abd surgyDecreases post op ileus in upper abd surgy Decrease ICU days and vent days after abd Decrease ICU days and vent days after abd
vasc surgeryvasc surgery

Flavors of epiduralsFlavors of epidurals
NarcoticsNarcotics Narcotics + Local anestheticsNarcotics + Local anesthetics Complications:Complications:
Rostrol migration of morphine with respiratory Rostrol migration of morphine with respiratory depression up to 18 hrs after depression up to 18 hrs after
Hypotension from sympathectomyHypotension from sympathectomy

P.O. ConversionP.O. Conversion
Morphine 10 mg. = oxycodone 20 mgMorphine 10 mg. = oxycodone 20 mg

Case 3Case 3
20 y.o. man MCC intubated in field for 20 y.o. man MCC intubated in field for combativeness, open femur, SAH and L combativeness, open femur, SAH and L cerebral contusion, etoh 498cerebral contusion, etoh 498
What’s going to happen to him tonight?What’s going to happen to him tonight?

Case 3Case 3
Back from the ORBack from the OR Ex-fix, EVD with ICP 16Ex-fix, EVD with ICP 16 What meds will you write for? What do you What meds will you write for? What do you
have to treat?have to treat?

Sedation Options: PropofolSedation Options: PropofolPharmacology: GABA agonistPharmacology: GABA agonist
Pharmacokinetics/dynamics: onset 1 - 2 minutes, terminal half-Pharmacokinetics/dynamics: onset 1 - 2 minutes, terminal half-life 6 hours, duration 10 minutes, hepatic metabolismlife 6 hours, duration 10 minutes, hepatic metabolism
BenefitsBenefits• Rapid onset and offset and easily titratedRapid onset and offset and easily titrated• Hypnotic and antiemeticHypnotic and antiemetic• Can be used for intractable seizures and elevated intracranial pressureCan be used for intractable seizures and elevated intracranial pressure
RisksRisks• Not reliably amnestic, especially at low dosesNot reliably amnestic, especially at low doses• NO analgesia!NO analgesia!• HypotensionHypotension• Hypertriglyceridemia; lipid source (1.1 kcal/ml)Hypertriglyceridemia; lipid source (1.1 kcal/ml)• Respiratory depressionRespiratory depression• Propofol Infusion SyndromePropofol Infusion Syndrome
-- Cardiac failure, rhabdomyolysis, severe metabolic acidosis, and renal failureCardiac failure, rhabdomyolysis, severe metabolic acidosis, and renal failure
-- Caution should be exercised at doses > 80 mcg/kg/min for more than 48 hoursCaution should be exercised at doses > 80 mcg/kg/min for more than 48 hours
-- Particularly problematic when used simultaneously in patient receiving Particularly problematic when used simultaneously in patient receiving catecholamines and/or steroidscatecholamines and/or steroids

Sedation Options: Benzodiazepines Sedation Options: Benzodiazepines (Midazolam and Lorazepam)(Midazolam and Lorazepam)
Pharmacokinetics/dynamicsPharmacokinetics/dynamics• Lorazepam: onset 5 - 10 minutes, half-life 10 hours, glucuronidatedLorazepam: onset 5 - 10 minutes, half-life 10 hours, glucuronidated• Midazolam: onset 1 - 2 minutes, half-life 3 hours, metabolized by cytochrome P450, Midazolam: onset 1 - 2 minutes, half-life 3 hours, metabolized by cytochrome P450,
active metabolite (1-OH) accumulates in renal diseaseactive metabolite (1-OH) accumulates in renal disease
BenefitsBenefits• AnxiolyticAnxiolytic• AmnesticAmnestic• SedatingSedating
RisksRisks• DeliriumDelirium• NO analgesiaNO analgesia• Excessive sedation: especially after long-term sustained useExcessive sedation: especially after long-term sustained use• Propylene glycol toxicity (parenteral lorazepam): significance uncertain Propylene glycol toxicity (parenteral lorazepam): significance uncertain
-- Evaluate when a patient has unexplained acidosisEvaluate when a patient has unexplained acidosis
-- Particularly problematic in alcoholics (due to doses used) and renal failureParticularly problematic in alcoholics (due to doses used) and renal failure• Respiratory failure (especially with concurrent opiate use)Respiratory failure (especially with concurrent opiate use)• WithdrawalWithdrawal

Case 3Case 3
Continuous infusionContinuous infusion Fentanyl 1 mcg/kg/hrFentanyl 1 mcg/kg/hr MS04 1-5 mg/hrMS04 1-5 mg/hr MidazolamMidazolam 1-4 mg/hr1-4 mg/hr LorazepamLorazepam 1-4 mg/hr1-4 mg/hr Propofol – 30-120 mcg/kg/min (packaged at Propofol – 30-120 mcg/kg/min (packaged at
10mg/cc; approx 10-40 cc/hr for 70 kg pt)10mg/cc; approx 10-40 cc/hr for 70 kg pt)

Overview of SCCM AlgorithmOverview of SCCM Algorithm
Yes
Reassess goal daily,Titrate and taper therapy to maintain goal,Consider daily wake-up,Taper if > 1 week high-dose therapy & monitorfor withdrawal
No
Set Goalfor
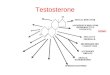
Analgesia
Hemodynamically UnstableFentanyl 25 - 100 mcg IVP Q 5-15 min, orHydromorphone 0.25 - 0.75 mg IVP Q 5 - 15 min
Hemodynamically stableMorphine 2 - 5 mg IVP Q 5 - 15 min
Repeat until pain controlled, then scheduled doses + prn
Set Goalfor
Sedation
Acute Agitation #
Midazolam 2 - 5 mg IVP Q 5 - 15 min untilacute event controlled
Ongoing Sedation #
Lorazepam 1 - 4 mg IVP Q 10-20 min untilat goal then Q 2 - 6 hr scheduled + prn , orPropofol start 5 mcg/kg/min, titrate Q 5 minuntil at goal
Set Goalfor Controlof Delirium
Haloperidol 2 - 10 mg IVP Q 20 - 30 min,then 25% of loading dose Q 6hr x 2-3 days,then taper
IVP Dosesmore often than Q
2hr?
Consider continuousinfusion opiate or
sedative
> 3 Days Propofol?(except neuro pt.)
Convert toLorazepam
Yes
Benzodiazepine or Opioid:Taper Infusion Rate by
10-25% Per Day
Yes
Dosesapproximate for
70kg adult
Rule out and Correct Reversible Causes
Use Non-pharmacologic Treament,Optimize the Environment
ALGORITHM FOR SEDATION AND ANALGESIA OF MECHANICALLY VENTILATED PATIENTS
Use Pain Scale * toAssess for Pain
Use Sedation Scale **
to Assess forAgitation/Anxiety
Use Delirium Scale *** toAssess for Delirium
Is the Patient Comfortable & at Goal?
Lorazepam viainfusion?
Use a low rate and IVPloading doses
1
2
3
4
Jacobi J, Fraser GL, Coursin D, et al. Crit Care Med. 2002;30:119-141.

OverdoseOverdose
NalaxoneNalaxone flumazenilflumazenil


Address PainAddress Pain
Set G oalfor
Analgesia
Hem odynam ically UnstableFentanyl 25 - 100 m cg IVP Q 5-15 m in, orHydromorphone 0.25 - 0.75 m g IVP Q 5 - 15 m in
Hem odynam ically stableMorphine 2 - 5 m g IVP Q 5 - 15 m in
Repeat until pain controlled, then scheduled doses + prn
Use Pain Scale * toAssess for Pain
Reassess goal daily,T itrate and taper therapy to m aintain goal,Consider daily wake-up,Taper if > 1 week high-dose therapy & m onitorfor withdrawal
Is the Patient Com fortable & at Goal?

Atypical Antipsychotics: Quetiapine, Atypical Antipsychotics: Quetiapine, Olanzapine, Risperidone, ZiprasidoneOlanzapine, Risperidone, Ziprasidone
Mechanism of action unknownMechanism of action unknown
Less movement disorders than haloperidolLess movement disorders than haloperidol
Enhanced effects on both positive (agitation) and negative Enhanced effects on both positive (agitation) and negative (quiet) symptoms(quiet) symptoms
Efficacy = haloperidol?Efficacy = haloperidol?• One prospective randomized study showing equal efficacy of olanzapine One prospective randomized study showing equal efficacy of olanzapine
to haldol with less EPSto haldol with less EPS
IssuesIssues• Lack of available IV formulationLack of available IV formulation• Troublesome reports of CVAs, hyperglycemia, NMSTroublesome reports of CVAs, hyperglycemia, NMS• Titratability hamperedTitratability hampered
-- QTc prolongation with ziprasidone IMQTc prolongation with ziprasidone IM
-- Hypotension with olanzapine IMHypotension with olanzapine IM

HaloperidolHaloperidol
No prospective randomized controlled trials in ICU No prospective randomized controlled trials in ICU delirium delirium
> 700 published reports involving > 2,000 patients> 700 published reports involving > 2,000 patients
The good:The good:• Hemodynamic neutralityHemodynamic neutrality• No effect on respiratory driveNo effect on respiratory drive
The bad:The bad:• QTc prolongation and QTc prolongation and torsades de pointestorsades de pointes• Neuoroleptic malignant syndromeNeuoroleptic malignant syndrome - only three cases with IV - only three cases with IV
haloperidolhaloperidol• Extrapyramidal side effectsExtrapyramidal side effects - less common with IV than oral - less common with IV than oral
haloperidolhaloperidol


Opiate and Benzodiazepine WithdrawalOpiate and Benzodiazepine Withdrawal
Frequency related to dose and durationFrequency related to dose and duration• 32% if receiving high doses for longer than a week32% if receiving high doses for longer than a week
Onset depends on the half-lives of the parent drug and its active Onset depends on the half-lives of the parent drug and its active metabolites metabolites
Clinical signs and symptoms are common among agentsClinical signs and symptoms are common among agents• CNS activation: seizures, hallucinations, CNS activation: seizures, hallucinations, • GI disturbances: nausea, vomiting, diarrheaGI disturbances: nausea, vomiting, diarrhea• Sympathetic hyperactivity: tachycardia, hypertension, tachypnea, sweating, Sympathetic hyperactivity: tachycardia, hypertension, tachypnea, sweating,
feverfever
No prospectively evaluated weaning protocols availableNo prospectively evaluated weaning protocols available• 10 - 20% daily decrease in dose10 - 20% daily decrease in dose• 20 - 40% initial decrease in dose with additional daily reductions of 10 - 20%20 - 40% initial decrease in dose with additional daily reductions of 10 - 20%
Consider conversion to longer acting agent or transdermal Consider conversion to longer acting agent or transdermal delivery formdelivery form

Protocols and Assessment ToolsProtocols and Assessment Tools
SCCM practice guidelines can be used as a template for SCCM practice guidelines can be used as a template for institution-specific protocols.institution-specific protocols.
Titration of sedatives and analgesics guided by Titration of sedatives and analgesics guided by assessment tools:assessment tools:
• Validated sedation assessment tools (Ramsay Sedation Scale [RSS], Validated sedation assessment tools (Ramsay Sedation Scale [RSS], Sedation-Agitation Scale [SAS], Richmond Sedation-agitation Scale Sedation-Agitation Scale [SAS], Richmond Sedation-agitation Scale [RSAS], etc.)[RSAS], etc.)
-- No evidence that one is preferred over anotherNo evidence that one is preferred over another• Pain assessment tools - none validated in ICU (numeric rating scale Pain assessment tools - none validated in ICU (numeric rating scale
[NRS], visual analogue scale [VAS], etc.)[NRS], visual analogue scale [VAS], etc.)

Daily Goal is Arousable, Daily Goal is Arousable, Comfortable SedationComfortable Sedation
Sedation needs to be protocolized and titrated to goal:Sedation needs to be protocolized and titrated to goal:• Lighten sedation to appropriate wakefulness daily.Lighten sedation to appropriate wakefulness daily.
Effect of this strategy on outcomes:Effect of this strategy on outcomes:• One- to seven-day reduction in length of sedation and mechanical One- to seven-day reduction in length of sedation and mechanical
ventilation needsventilation needs• 50% reduction in tracheostomies50% reduction in tracheostomies• Three-fold reduction in the need for diagnostic evaluation of CNSThree-fold reduction in the need for diagnostic evaluation of CNS

Appropriate Recall May be ImportantAppropriate Recall May be Important
Factual memories (even unpleasant ones) help to put Factual memories (even unpleasant ones) help to put ICU experience into perspective ICU experience into perspective
Delusional memories risk panic attacks and PTSDDelusional memories risk panic attacks and PTSD
The optimal level of sedation for most patients is that The optimal level of sedation for most patients is that which offers comfort while allowing for interaction with which offers comfort while allowing for interaction with the environment.the environment.

Recall in the ICURecall in the ICU
Some degree of recall occurs in up to 70% of ICU Some degree of recall occurs in up to 70% of ICU patients.patients.
• Anxiety, fear, pain, panic, agony, or nightmares reported in 90% of Anxiety, fear, pain, panic, agony, or nightmares reported in 90% of those who did have recall.those who did have recall.
Potentially cruel:Potentially cruel:• Up to 36% recalled some aspect of paralysis.Up to 36% recalled some aspect of paralysis.
Associated with PTSD in ARDS? Associated with PTSD in ARDS? • 41% risk of recall of two or more traumatic experiences.41% risk of recall of two or more traumatic experiences.
Associated with PTSD in cardiac surgeryAssociated with PTSD in cardiac surgery

What We Know About ICU What We Know About ICU Agitation/DiscomfortAgitation/Discomfort
PrevalencePrevalence• 50% incidence in those with length of stay > 24 hours50% incidence in those with length of stay > 24 hours
Primary causes: unrelieved pain, delirium, anxiety, sleep Primary causes: unrelieved pain, delirium, anxiety, sleep deprivation, etc.deprivation, etc.
Immediate sequelae: Immediate sequelae: • Patient-ventilator dyssynchronyPatient-ventilator dyssynchrony• Increased oxygen consumption Increased oxygen consumption • Self (and health care provider) injurySelf (and health care provider) injury• Family anxietyFamily anxiety
Long-term sequelae: chronic anxiety disorders and post-Long-term sequelae: chronic anxiety disorders and post-traumatic stress disorder (PTSD)traumatic stress disorder (PTSD)

OpiatesOpiates
BenefitsBenefits• Relieve pain or the sensibility to noxious stimuliRelieve pain or the sensibility to noxious stimuli• Sedation trending toward a change in sensorium, especially with more lipid Sedation trending toward a change in sensorium, especially with more lipid
soluble forms including morphine and hydromorphone.soluble forms including morphine and hydromorphone.
RisksRisks• Respiratory depressionRespiratory depression• NO amnesiaNO amnesia• PruritusPruritus• IleusIleus• Urinary retentionUrinary retention• Histamine release causing venodilation predominantly from morphineHistamine release causing venodilation predominantly from morphine• Morphine metabolites which accumulate in renal failure can be analgesic Morphine metabolites which accumulate in renal failure can be analgesic
and anti-analgesic.and anti-analgesic.• Meperidine should be avoided due to neurotoxic metabolites which Meperidine should be avoided due to neurotoxic metabolites which
accumulate, especially in renal failure, but also produces more sensorium accumulate, especially in renal failure, but also produces more sensorium changes and less analgesia than other opioids.changes and less analgesia than other opioids.