Embed Size (px)
Citation preview

1
Pain Management: Interventional Strategies 101

2
Objectives
¨ Pharmacist ¤ Identify patients that may benefit from interventional management
¤ Evaluate the role of intrathecal pumps and nerve blocks for pain management
¤ Examine the considerations required when a patient with an intrathecal pump is hospitalized.
¨ Pharmacy technician ¤ Recognize agents that can be utilized for a nerve block ¤ List drugs used to prepare intrathecal nerve blocks
¤ Describe the preparation of a intrathecal pain pumps

Pain Management: Why Care?
¨ Pain is one of the most common reasons for seeking care
¨ In the United States, 20 to 30% of the general population experience chronic or recurring pain (3). ¤ Approximately, 2/3 of these people have had pain for
more than 5 years (4).
¨ 67% of patients with metastatic cancer report pain (5)
¨ “War on Opioids”
3

Pain Assessment Is Complex
¨ No single approach to pain assessment is appropriate for all patients or in all settings.
¨ Pain is subjective, so no satisfactory objective measures of pain exist.
¨ Pain is multidimensional, the clinician must consider multiple aspects (sensory, affective, cognitive) of the pain experience.
¨ Pain assessments may vary with respect to purpose, setting, patient population.

Pain History
¨ Significant previous and/or ongoing instances of pain and its effect on the patient. ¨ Previously used methods for pain control that have been either helpful or unhelpful. ¨ The patient's attitude toward use of opioids or other medications, including any history of
substance abuse. ¨ The patient's typical coping response for stress or pain, including the presence or absence of
psychiatric disorders such as depression, anxiety, or psychosis. ¨ Family expectations and beliefs concerning pain, stress, and postoperative course. ¨ Ways the patient describes or shows pain. ¨ The patient's knowledge of, expectations about, and preferences for pain management methods
and for receiving information about pain management.

Acute vs. chronic pain
¨ Acute pain might be mild and last just a moment, or it might be severe and last for weeks or months. ¤ In most cases, acute pain does not last longer than six
months ¤ Underlying cause of pain has been treated or has
healed.
¨ Chronic pain persists despite the fact that the injury has healed. Pain signals remain active in the nervous system for weeks, months, or years.

7
Pathophysiology of Pain
K+ = Potassium; PG = Prostaglandins; H+ = Hydrogen ions; BK = bradykinin; H= Histamine; SP= Substance P; 5HT = Serotonin
Harrison’s Principles of Internal Medicine, 2008

Noxius Stimuli Activate Pain Pathway 8
Impulse transmitted to
Peripheral Nerve
Synapse with Spinothalamic
tract
Travels to anterior
cingulate, frontal insular,
& somatosensory
cortex in thalamus
Activation of spinal pain transmission
Harrison’s Principles of Internal Medicine, 2008

Management Modalities
¨ Non-pharmacological ¤ Acupuncture, massage, aromatherapy, physical therapy,
etc.
¨ Pharmacological ¤ Topical, transdermal ¤ Oral, rectal ¤ Intramuscular, intravenous
¨ Interventional ¤ Procedure +/- pharmacologic
9

10
Interventional Management
¨ Surgery ¨ Radiation ¨ Radiofrequency ablation
¤ Electrical Stimulation directed towards a tumor ¨ Peripheral Nerve Blocks
¨ Intraspinal drug therapy ¤ Relieve pain by instilling small doses of morphine or
other drugs directly to cerebrospinal fluid
Brogan S, Junkins S. Interventional therapies for the management of cancer pain. J Support Oncol. 2010 Mar-Apr;8(2):52-9.

Neuraxial Pain Management
¨ Encompasses both spinal and epidural anesthesia ¨ performed as the sole anesthetic (with or without
sedation) ¨ combined with general anesthesia to decrease
anesthetic requirements ¨ postoperative analgesia
11

Nerve Blocks: Indications
¨ No specific indications for nerve blocks ¨ Typically used to avoid the effects of alternative
methods ¤ Side effects and complications of general anesthesia ¤ Minimizing opioid use
¨ Widely-used for surgical anesthesia ¨ Post-operative pain management ¨ Chronic pain management
12

Common Locations for Nerve Blocks 13

Sympathetic Nerve Block
¨ sympathetic nerves come together outside your spine area in thick networks of nerves called ganglions.
¨ Targets a series of nerves that spread out from your spine to your body to help control several involuntary body functions ¤ Blood flow, digestion, and sweating
¨ stellate ganglion block: pain in the upper part of your body.
¨ Lumbar sympathetic block: pain in the lower part of your body, a ganglion near the lower spine
14

Facet Joint Block
¨ Facet joints are the small joints located between each vertebra that provide the spine with both stability and flexibility
¨ Facet syndrome occurs when one or more of these joints become inflamed or irritated
¨ Combines a local anesthetic and a corticosteroid anti-inflammatory medication
15

Splanchnic/Celiac/Hypogastric Plexus Blocks
¨ Dense cluster of nerve cells and supporting tissue, located behind the stomach, in the region of the celiac artery just below the diaphragm.
¨ Nerve signals to the majority of abdominal organs flow through the celiac plexus and the splanchnic nerves. ¤ Pancreas, liver, gallbladder, stomach, small intestine, and the parts of
the colon.
¨ Abdominal pain that may be caused by irritation, compression or entrapment of the nerve bundles within various abdominal organs ¤ Tumor invasion, fibrosis, or chronic inflammation
16

Splanchnic/Celiac/Hypogastric Plexus Blocks
¨ A local anesthetic, steroid or ethyl-alcohol administered ¨ The use of alcohol, called a neurolytic block, because it
destroys the nerves, can provide sustained pain relief in conditions where medications alone are not effective.
¨ A trial block is initially done with local anesthetic as a test to ensure there is pain relief. If substantial pain relief is acquired, a neurolytic block is performed.
17

Regional Anesthesia: Adverse Effects
¨ Toxicity of local anesthetics (with epidural techniques)
¨ Transient or chronic paresthesia ¨ Nerve damage ¨ Intra-arterial injection, seizures, or cardiac arrest ¨ Block failure and the need to supplement or convert
to general anesthesia ¨ Intra-arterial injection, seizures, or cardiac arrest ¨ Infection
18

Pharmacologic Agents
¨ Local Anesthetics
¨ Opiates ¤ Opioids can enhance analgesia, with the degree of side effects largely
related to lipid solubility. n Morphine (hydrophilic/lipophobic) injected epidurally stay in place or spread
rostrally
n Fentanyl (hydrophobic/liphophilic) rapidly absorbed
¨ Adjuncts ¤ Epinephrine (1:200,000 i.e., 5 ucg/mL) can prolong an epidural,
especially if chlorprocaine or lidocaine is used ¤ Sodium bicarbonate favors the non-ionized form of local anesthetics and
promotes more rapid onset of epidural anesthesia.
19

Local Anesthetics 20

Intrathecal Pain Management 21

Background
¨ Used in the control of pain and spasticity ¨ Allows for reduced medication doses that can
decrease the side effects typically associated with oral or parenteral drug delivery
¨ Data for pain relief, adverse effect reduction, and cost-effectiveness with cancer pain control are compelling
22

23
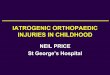
Implantable Drug Delivery Systems (IDDS)
http://www.spinesurgeon.co.uk/media/intrathecal-pump-implant.jpg

24
Implantable Drug Delivery Systems (IDDS)

Potential Candidates for IDDS
¨ Chronic pain ¨ Recalcitrant pain despite aggressive titration on
standard treatment modalities ¨ Patients unable to tolerate adverse effects of
standard treatment modalities
25

Where is therapy administered?
http://www.mayfieldclinic.com/PE-PUMP.htm

IDDS Trial Period
¨ Screening period which determines whether a patient will benefit from an IDDS ¤ Determine the response ¤ Prevention of ineffective pump
n About 95% of patients have a successful treatment of pain
27
Knight et al. Implantable intrathecal pumps for chronic pain: highlights and updates. Croat Med J. 2007

IDDS Trial Procedure 28

29
Intrathecal Pain Pumps: Benefits
¨ Provides effective pain control for patients who have failed other treatment modalities
¨ Less Systemic Side Effects
Ghafoor, Intrathecal drug therapy for long-term pain management. Am J Health-Syst Pharm 2007

- Postoperative subarachnoid hemorrhage - Back Pain, Loss of sensation, Lower extremity weakness
- Catheter tip inflammatory masses - Loss of drug effect with long-term therapy - New-onset radicular pain & spinal cord neurologic
deficits
- Invasive Infections: Bacterial Meningitis
30
Intrathecal Pain Pumps: Adverse Effects

IDDS Medications
Types of Medications Used
Opioids Morphine Hydromorphone
Fentanyl Local Anesthetic Bupivacaine
Adjunct Medications Ziconotide Clonidine Baclofen
31

32
Agents Utilized for IDDS

33
Recommended Starting Doses for Intrathecal Therapy

Comparison of Opioid Characteristics
Characteristic Morphine Sulfate
Hydromoprhone Hydrochloride
Fentanyl
Solubility Hydrophilic Hydrophilic Lipophilic
Degree of spread in cerebrospinal fluid
High Intermediate Low
34
Ghafoor, Intrathecal drug therapy for long-term pain management. Am J Health-Syst Pharm 2007

Comparison of Opioid Equianalgesic Potency
35
Equianalgesic Potency (mg)
Morphine Sulfate
Hydromoprhone Hydrochloride
Fentanyl
Oral 300 60 2
Parenteral 100 20 1
Epidural 10 2 0.1
Intrathecal 1 0.25 0.01
Ghafoor, Intrathecal drug therapy for long-term pain management. Am J Health-Syst Pharm 2007

Evidence Supporting Use IT Opioids in Non-Cancer Pain
¨ Morphine effeciacy has been documented in case studies, retrospective studies, and prospective studies since 1980 ¤ Efficacy Stuides documented
at least a 30- 50% improvement in Visual analog scores
¨ Hydromorphone IT infusions offer therapeutic alternative to IT morphine for patients with intractable pain not alleviated by morphine
¨ Retrospective studies and case reports have documented improvement in pain scores with minimum increase in adverse side effects
Morphine Hydromorphone
36
Njee et al. Neuromodulation 2004;7:249–259

Local Anesthetics - Bupivacaine
¨ Co-administration of bupivacaine and morphine has been shown to provide synergistic pain relief, resulting in reduction in morphine dosage
¨ Common Adverse Effects: ¤ Parasthesia, motor and sensory blockade, arterial
hypotension, diarrhea, and urinary retention
37

Adjunct Analgesic: Ziconotide
¨ Only administered intrathecally to maximize antinoceptive effectiveness and minimize sympatholysis
¨ Patients with chronic pain received an average reduction of 43% in their Visual Analog Scale of Pain Intensity (VASPI) score.
¨ Common Adverse Effects: ¤ Dizziness, nystagmus, confusion, abnormal gait,
somnolence
38

Adjunct Analgesic: Clonidine
¨ Antinoceptive effects of clonidine are mediated via inhibitory interactions with pre-synaptic and postsynaptic afferent fibers in the dorsal horn of the spinal cord
¨ Combination of clonidine and morphine has been shown to be more effective than morphine alone
¨ Common Adverse Effects: ¤ Sedation, hypotension, dry mouth, and bradycardia
39

Adjunct Analgesic: Baclofen
¨ Used to treat spinal cord spasticity ¨ Combination therapy with an opioid has been
studied in chronic nociceptive or sympathetic pain syndromes
¨ Common Adverse Effects: ¤ Weakness, hypotonia, sedation, constipation,
respiratory depression
40

PUBLISHED LITERATURE REVIEW

42
EFFICACY RESULTS AFTER 1 MONTH OF EPIDURAL MORPHINE INFUSION
Measure Baseline At One Month P
Avg Oral Equalanalgesic Morphine Use
77.7± 19.1 mg/day 16.1 ± 3.6 mg/day <0.001
Pain Analog Scale 8.6 ± 0.3 3.8 ± 0.4 <0.001
Hassenbusch, J Neurosurg 73: 405-409, 1990
STUDY DESIGN Observational Study
PATIENT POPULATION
69 Patients Enrolled with 41 being studied
OBJECTIVE • Demonstrate that the epidural route is effective with minimal complications • Screening with temporary epidural catheter infusions results in high rate of subsequent pain relief
COMMON COMPLICATIONS & SIDE EFFECTS EXPERIENCED INCIDENCE
Superficial Wound Infections 3
Skin necrosis 1
Catheter Migration 4
Voiding Disturabances 3

43
Randomized Clinical Trial of an Implantable Drug Delivery System Compared with
Comprehensive Medical Management for Refractory Cancer Pain: Impact on Pain, Drug-
Related Toxicity, and Survival
J Clin Oncology. 2002 Oct; 20(19):4040-4049

44
The Cancer Pain Trial J Clin Oncology. 2002 Oct; 20(19):4040-4049
Purpose Evaluate the clinical success of intraspinal IDDS in patients with intractable cancer-associated pain.
Design Prospective, Multicenter, Randomized, Concealed, Clinical Trial
Objectives
Primary Objective: Evaluate the clinical success of each study arm at 4weeks • At least 20% reduction in Pain using Visual Analog Scores (VAS) • Equal pain scores with at least 20% reduction in symptom control based on National Cancer Institute’s common toxicity criteria Secondary Objective: • Differences in individual drug toxicities measured using the National Cancer Institute Common Toxicity Criteria (NCI CTC)

45
Patient Selection
Patient Inclusion Criteria
• Documented Cancer • VAS pain scores consistently ≥5/10 • Opiate doses ≥ 200 mg of oral morphine or equivalent • Opiate doses ≤ 200 mg with unacceptable side effects • Life expectancy ≥ 3 months
Study Design
• Patients were Randomized to CMM or IDDS • Data Recorded: Every other week (2-12 weeks) then Monthly until 6 months • Data collected at visits included
• Comparison of VAS • Composite Drug Toxicity score
• Sum of 15 individual drug toxicity scores (0-4) Of Note: Patients assigned to intrathecal morphine group needed to undergo a trial of intraspinal morphine

202 Randomized
99 CMM
15 Died 6 Withdrew consent
1 Lost to Follow-Up
5 Implanted
70 Not Implanted
75
4- week Follow- Up
101 IDDS
8 Died 8 Withdrew Consent
12 Missed Visits
22 Not Implanted
51 Implanted
73
4-week Follow-Up
46

47
Results: Baseline Characteristics of Patients
Characteristic CMM Group (n = 99)
IDDS Group (n = 101)
Age, years 57.8 ± 13.7 56.2 ± 13.2
Type of Pain, %
Neuropathic 14.3 12.9
Nociceptive 25.5 25.7
Mixed 60.2 61.4
Baseline Medication Use, %
Opioids alone 39.8 41.6
Nonopiod adjunctive alone 2.0 2.0
Both 58.2 56.4
Morphine Oral Equivalent dose, mg/d 280 260
Baseline VAS 7.57 ± 1.97 7.44 ± 1.97
Baseline Composite Toxicity Score 6.65 ± 5.58 6.95 ± 4.91

48
Reduction in Pain and Drug Toxicity from Baseline to 4 Weeks CMM Group IDDS Group
Variabe n Baseline 4 Weeks n Baseline 4 Weeks P
Median Daily MOEDs
272 mg 290 mg 250 mg 50 mg
VAS Pain Score 72 7.81±1.63 -3.05 ± 3.16 71 7.57 ± 1.79 -3.90 ± 3.42 .055
Common Toxicity Criteria
75 6.36 ± 5.65 -1.09 ± 5.57 73 7.22 ± 5.00 -3.63 ± 5.43 .004
Results: VAS and Toxicity Scores
MOEDs = Morphine Oral Equivalent Doses

49
Results: Clinical Success Results
Clinical Success and Failure
CMM Group IDDS Group
Criteria n % n % P
VAS Pain Reduced by ≥ 20% regardless of increseased toxicity, or
equal VAS with ≥ 20% reduction in toxicity
51/72 70.8 60/71 84.5 .05
Both pain and toxicity reduced by ≥ 20% 27/72 37.5 41/71 57.5 .02
Neither pain nor toxicity reduced by ≥ 20% 17/72 23.6 8/71 11.3 .05

50
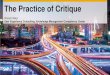
Results: Drug Side Effects
KEY
██ CMM ██ IDDS

Results: Adverse Events seen in IDDS
Event CMM N= 98
IDDS N=101
Total
IDDS-related SAE 5 22 27
Lumbar Site _ 5 5
Catheter Problems _ 5 5
Infections 1 1 2
Hematoma _ 2 2
Inflammation _ 2 2
Wound dehiscence _ 2 2
CSF leak _ 1 1
Nerve irritation _ 1 1
¨ Total Serious Adverse Events = 194 ¤ CMM = 95 (49%) ¤ IDDS = 99 (51%)
51

Discussion
¨ Patients with refractory cancer pain are more effectively treated with IDDS than CMM ¤ Increase pain relief ¤ Fewer side effects due to opioids ¤ Improved survival
¨ Limitations: ¤ Did not mention how medication was titrated to effect ¤ Survival analysis was not powered
52

53
Who would benefit?
¨ Patients with estimated life expectancy ≥ 3 months ¨ Patients with Moderate – Severe Pain Scores despite:
¤ Using ≥ 200 mg morphine/day without any symptomatic relief
¤ Using ≤ 200 mg morphine/day suffering from opioid related side effects
¨ Patients with no contraindications to intraspinal or epidural use ¤ Active infection, spinal cord obstruction, coagulopathy,
anticoagulants due to hematoma risk
Smith TJ, et al. Curr Oncol Rep. 2004 Jul;6(4):291-6.

54
Conclusions
¨ Intrathecal drug delivery systems have been shown to effectively decrease pain and drug toxicity
¨ Intrathecal drug delivery systems have many serious
adverse side effects that will need to be considered prior to treatment

Pumps: Practical Considerations for Hospitalized Patients
¨ Identifying patients with implanted pump devices ¨ Interrogating the pump
¤ Verification of contents and pump settings
¤ Typically limited to specialty services
¨ Communication ¤ Medication administration record
¨ Refilling pumps ¤ Double check process
¤ Products prepared externally can have a variety of different formulations, concentrations, etc.
¨ Accounting for patients’ complete pain needs
55

Refilling IDDS
¨ Review pump contains with provider refilling pump ¨ Ensure double check process in place at critical
points ¤ Calculations for preparation ¤ Review of product selection prior to compounding
initiation n REMEMBER: PRESERVATIVE FREE PRODUCTS ONLY
¤ Real-time verification of compounding
¨ Complete preparation in clean room
56

Role of Pharmacists
¨ Medication Safety ¤ Standard concentrations and preparations ¤ Preservative free products ¤ Product sterility
¨ Optimize the use of opioids ¨ Transitioning patients to hospice
57

References
¨ Brull R, MacFarlane AJR, Chan VWS. Spinal, epidural, and caudal anesthesia. In: Miller RD, ed. Miller's Anesthesia. 8th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 56.
¨ Sherwood ER, Williams CG, Prough DS. Anesthesiology principles, pain management, and conscious sedation. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 19th ed. Philadelphia, PA: Elsevier Saunders; 2012:chap 16.
¨ Kleinman, W. & Mikhail, M. (2006). Spinal, epidural, & caudal blocks. In G.E. Morgan et al Clinical Anesthesiology, 4th edition. New York: Lange Medical Books.
¨ Morgan, G.E., Mikhail, M.S., Murray, M.J. (2006). Peripheral nerve blocks. In G.E. Morgan et al Clinical Anesthesiology, 4th edition. New York: Lange Medical Books.
¨ Warren, D.T. & Liu, S.S. (2008). Neuraxial anesthesia. In D.E. Longnecker et al (eds) Anesthesiology. New York: McGraw-Hill Medical.
¨ Staal C, Arends A, Ho S.A self-report of quality of life of patients receiving intrathecal baclofen therapy. Rehabil Nurs. 2003 Sep-Oct;28(5):159-63.
¨ Ackerman LL, Follett KA, Rosenquist RW. Long-term outcomes during treatment of chronic pain with intrathecal clonidine or clonidine/opioid combinations. J Pain Symptom Manage. 2003 Jul;26 (1):668-77.
58

References
¨ Angel IF, Gould HJ Jr, Carey ME. Intrathecal morphine pump as a treatment option in chronic pain of nonmalignant origin. Surg Neurol. 1998;49:92-98.
¨ Paice JA, Penn RD, Shott S. Intraspinal morphine for chronic pain: a retrospective, multicenter study. J Pain Symptom Manage. 1996;11:71-80.
¨ Winkelmuller M, Winkelmuller W. Long-term effects of continuous intrathecal opioid treatment in chronic pain of nonmalignant etiology. J Neurosurg. 1996;85:458-467.
¨ Bedder MD. Epidural opioid therapy for chronic nonmalignant pain: critique of current experience. J Pain Symptom Manage. 1996;11:353-356.
¨ Brown J, Klapow J, Doleys D, et al. Disease-specific and generic health outcomes: a model for the evaluation of long-term intrathecal opioid therapy in noncancer low back pain patients. Clin J Pain. 1999;15:122-131
¨ Dahm P, Nitescu P, Appelgren L, Curelaru I. Efficacy and technical complications of long-term continuous intraspinal infusions of opioid and/or bupivacaine in refractory nonmalignant pain: a comparison between the epidural and the intrathecal approach with externalized or implanted catheters and infusion pumps. Clin J Pain. 1998;14:4-16.
¨ Valentino L, Pillay KV, Walker J. Managing chronic nonmalignant pain with continuous intrathecal morphine. J Neurosci Nurs. 1998;30:233-239.
¨ Anderson VC, Burchiel KJ. A prospective study of long term intrathecal morphine in the management of chronic nonmalignant pain. Neurosurgery. 1999;44:289 - 300.
59