Embed Size (px)
Citation preview

Pages 965-1008
C h a p t e r
26
The Urinary System
PowerPoint® Lecture Slides prepared by John L. Wilson
Copyright © 2009 Pearson Education, Inc.,publishing as Pearson Benjamin Cummings

Elimination of metabolic wastesWastes mostly from catabolism of
moleculesThese molecules excreted by various
systems
Excretion Defined

Systems Involved in Excretion
Urinary system_____
Respiratory system____________
Digestive system_____
Integumentary system_____
Carbon dioxide
Feces
Sweat
Urine

Functions of the Urinary System
Excretion of metabolic wastes Regulates fluid and electrolyte balanceRegulates blood pH Produces hormones
Calcitriol (vitamin D) helps regulate calciumErythropoietin regulates RBC formation
Regulates blood pressure by enzyme renin

Nephron
Microscopic filtering units of kidneys composed of renal tubules and a blood supply
Called functional units – make most of urine
About 1.25 million per kidneyMostly in renal cortex with some tubules
extending into renal pyramids of medulla

Nephron Anatomy
Bowman’s CapsuleGlomerulusDistal Convoluted Tubule
(end of nephron)Proximal Convoluted Tubule
Collecting Duct
Descending limb of Henle Ascending limb of Henle
Papillary Duct
Renal Papilla

Renal Corpuscle Anatomy
Renal Corpuscle Glomerulus – the
capillaries beneath
the podocytes
PCT
Afferent arteriole
Efferent arterioleDCT
Capsular space
Bowman’s Capsule

Nephron Blood Supply
Afferent arteriole
Efferent arteriolePeritubular capillaries
Vasa Recta

Physiology of the Urinary System
2 31
•Three processes required for urine formation
1. Filtration from the glomerulus to Bowman's capsule
2. Tubular reabsorption from renal tubules to blood of peritubular capillaries
3. Tubular secretion from blood of peritubular capillaries into the renal tubules
Urine
Afferent arteriole
Efferent arteriole
peritubular capillaries
Glomerulus
Bowman’s capsuleRenal Tubules

Filtration
Water and many different solutes pass from glomerulus to the Bowman’s capsule
Resulting fluid in capsular space called filtrate
Filtrate contains Wastes such as urea and uric acid that must be
eliminated in the urine
Useful (vital) substances such as water, organic nutrients and electrolytes that must be kept

Filtrate Formation
High glomerular blood hydrostatic pressure forces water and solutes through filtration membrane into the capsular space, then into the PCT
Capsular space
Filtration membrane
PCT

Filtration Continued
Amount of blood flow through kidneys in one minute = renal blood flow (RBF) About 1200 mL/minute
Amount of filtrate formed in one minute = glomerular filtration rate (GFR)Between 105 and 125 mL/minute
So, around 10% of RBF becomes filtrate

Tubular Reabsorption
Most of the filtrate is taken back into the blood from the nephron tubules by various methods Most Water, organic nutrients and electrolytes are kept Wastes and some water remain in filtrate and become
urine Most reabsorption in proximal convoluted tubule
Blood of peritubular capillaries

Tubular Reabsorption Continued
Water reabsorbed by osmosisSolutes reabsorbed by diffusion,
active transport, cotransport, countertransport and pinocytosis

Reabsorption Continued
Most actively transported substances have a transport maximum (Tm)The Tm refers to how much of a substance
(in milligrams) the nephron tubules can reabsorb in a minute
When Tm is exceeded, substance shows up in urine

Reabsorption Continued
Renal threshold is the maximum blood concentration at which a substance begins to appears in the urine when transport maximum (Tm) is exceeded
Renal threshold for glucose 180 milligrams per 100 mL (deciliter), and above that amount, glucose will appear in the urine
Can you think of what might cause the RT of glucose to be exceeded?

Tubular Secretion
Some solutes move from the blood of the nephron capillaries into the filtratePotassium, ammonium, hydrogen and
bicarbonate ions are secreted into filtrateHelps regulate acid-base balance and
electrolyte concentrationsBlood of peritubular capillaries

Water Reabsorption
Each day we lose about as much water as we gain
If loss exceeds gain, become dehydrated If gain exceeds loss, become over-
hydratedControlled by reabsorption of varying
amounts of water

Water Reabsorption Continued
Each day, between 150-180 L of filtrateEach day, 1-2 L of urine What does this tell you?

Types of Water Reabsorption
Obligatory water reabsorption In PCT and descending LOH More constant
Facultative water reabsorption In DCT and CDVariable, depending on degree of hydrationThis reabsorption controlled by hormones,
particularly the antidiuretic hormone (ADH)

Amounts of H2O Reabsorbed
65% in proximal convoluted tubules15% in descending limbs of HenleNone in ascending limb of Henle10-15% in distal convoluted tubulesRemainder in collecting ductsNext slide illustrates these amounts

Water Reabsorption Drawing
H2O-65%
H2O-15% from descending LOH
ISF and Blood
More salt and urea
Less salt and urea
Facultative Reabsorption-remainder of H2O reabsorptionis from the DCTand CD; variable, depending on water balance – mostly controlledby hormone ADH.
Obligatory Reabsorption – about 80 percent of H2Oreabsorbed at a more constant rate in PCT and descending LOH
No water reabsorbedby thick ascending LOH,it reabsorbs only salt(NaCl)
ISF and Blood

Concentration and Dilution of Urine
When water loss exceeds water gain, our kidneys can increase facultative water reabsorption Results in a smaller volume of a darker urine Our kidneys are thus concentrating our urine
When water gain exceeds water loss, our kidneys can decrease facultative water reabsorption Results in a larger volume of a lighter-colored
urine Our kidneys are thus diluting our urine

Steps in Concentration of Urine
1. As water loss exceeds gain, hypothalamus stimulates secretion of antidiuretic hormone (ADH) from the posterior pituitary
2. ADH makes the cells of the DCT and CD more permeable to water – adds water pores
3. More water leaves the DCT and CD and enters concentrated interstitial fluid and blood of the pyramid

Steps in Concentration of Urine
4. Concentrated interstitial fluid and blood take more water out of the filtrate and concentrate the urine
5. Result is less of a darker, concentrated urine Also, aldosterone from adrenal cortex
increases salt reabsorption from tubules and thus helps to concentrate urine How does this work?

Concentration of Urine-ADH Present
ADH
ADH
DCT and CD more permeable to water thus more water reabsorbed and urine is concentrated

Steps in Dilution of Urine
1. As water gain exceeds loss, hypothalamus stops secreting ADH
2. DCT and CD become less permeable to water – water pores decrease
3. Less water is reabsorbed
4. More water stays in filtrate and urine

Steps in Dilution of Urine
5. Results in more of a dilute urine
6. Adrenal cortex decreases aldosterone
secretion, thus less salt is reabsorbed
from tubules and this helps to dilute
urine

Dilution of Urine–ADH Absent
No ADH, so DCT and CD less permeable to water, thus less water reabsorbed and urine is diluted

Urine composition
95% H2O
5% solutes (solids) ElectrolytesNitrogenous wastes such as urea, creatinine
and uric acidUrea from __________________Creatinine from ________________Uric acid from ____________________
protein metabolism
muscle metabolism
nucleic acid metabolism

Characteristics of Urine
Color
Turbidity
Specific gravity
pH

Clinical Terms
Glomerulonephritis – page 1030
Acute and Chronic Renal failure – page 1030 Hemodialysis (kidney dialysis) –page 1022
Renal Calculi – page 1030

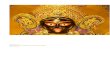
Polycystic Disease – page 1030&1031
Cyst-------------
Incurable, kidney disease in which cysts form in kidney, and destroy it. Cysts can be clearly seen in kidney below; it weighed 17 pounds.