Embed Size (px)
Citation preview
Drug allergy
Dean TeyPaediatric Allergist & Immunologist
Monday 17 May 2010
Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs
Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs
Background: Adverse drug ireactions
• WHO 1966 definition1WHO 1966 definition– An adverse drug reaction is any noxious,
unintended undesired effect of a drugunintended, undesired effect of a drug– Occurring at doses used in humans for
prevention, diagnosis or treatmentprevention, diagnosis or treatment
World Health Organization. International drug monitoring: the role of the hospital. Geneva: The Organization; 1966.

Adverse drug reaction: incidence
H it li dHospitalised patients Outpatients
• 15.1% of patients• Nearly half being
i i t 1
• 17-25% of patientsM th h lfserious in nature1
• Fatal ADRs in 0.32%
• More than half being serious in nature2,30.32% nature ,
1. Lazarou et al. JAMA 1998;279:1200-52. Gandhi et al. J Gen Intern Med 2000;15:149-54;3. Gandhi et al. N Engl J Med 2003;348:1556-64
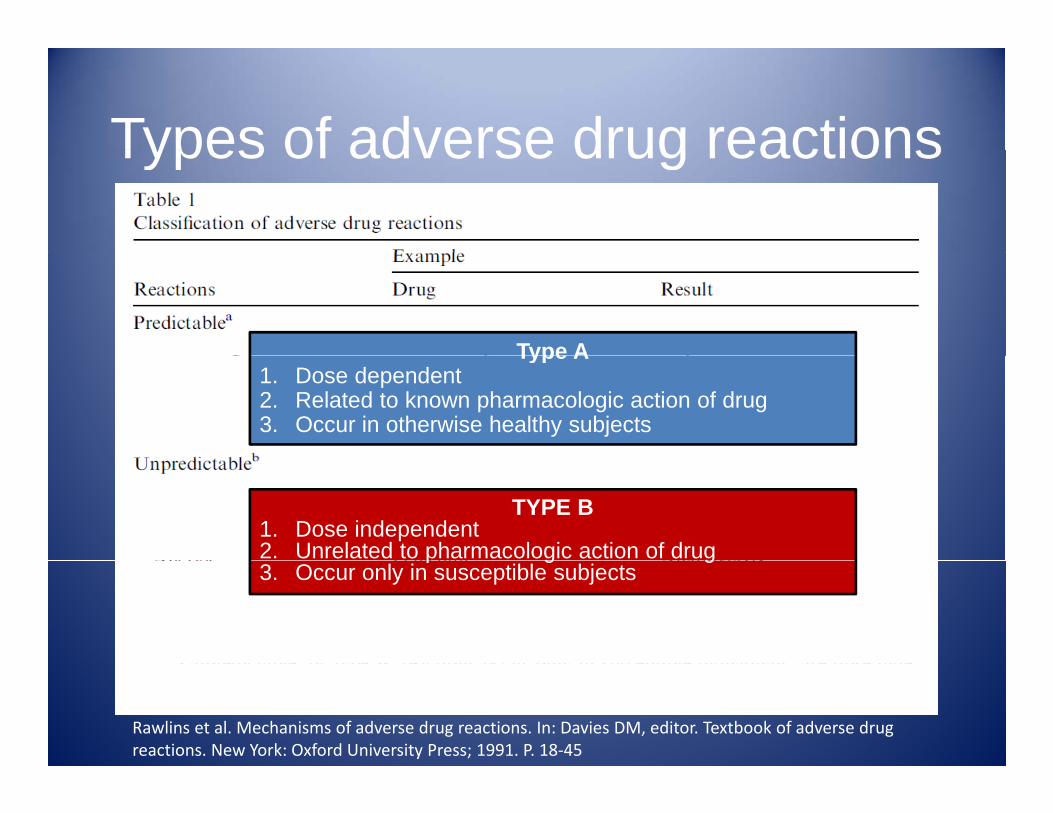
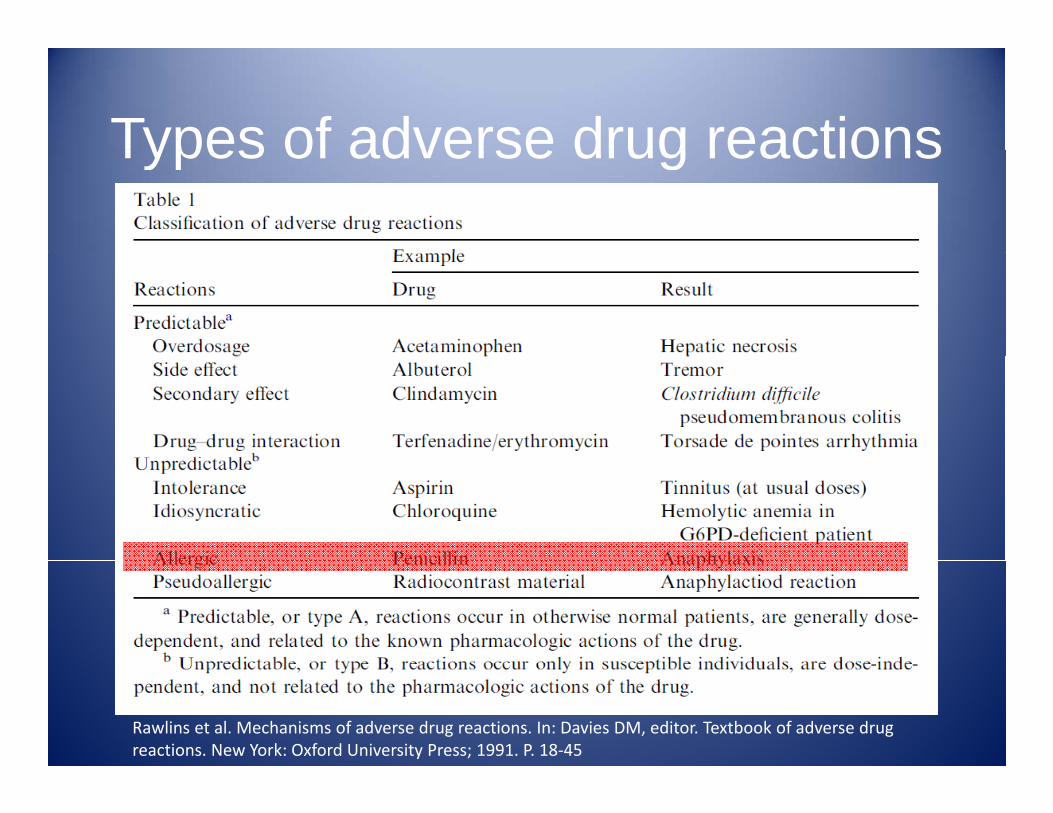
Types of adverse drug reactionsTypes of adverse drug reactions
Type AType A1. Dose dependent2. Related to known pharmacologic action of drug3. Occur in otherwise healthy subjects
TYPE B1. Dose independent2. Unrelated to pharmacologic action of drugp g g3. Occur only in susceptible subjects
Rawlins et al. Mechanisms of adverse drug reactions. In: Davies DM, editor. Textbook of adverse drug reactions. New York: Oxford University Press; 1991. P. 18‐45
Types of adverse drug reactionsTypes of adverse drug reactions
Rawlins et al. Mechanisms of adverse drug reactions. In: Davies DM, editor. Textbook of adverse drug reactions. New York: Oxford University Press; 1991. P. 18‐45
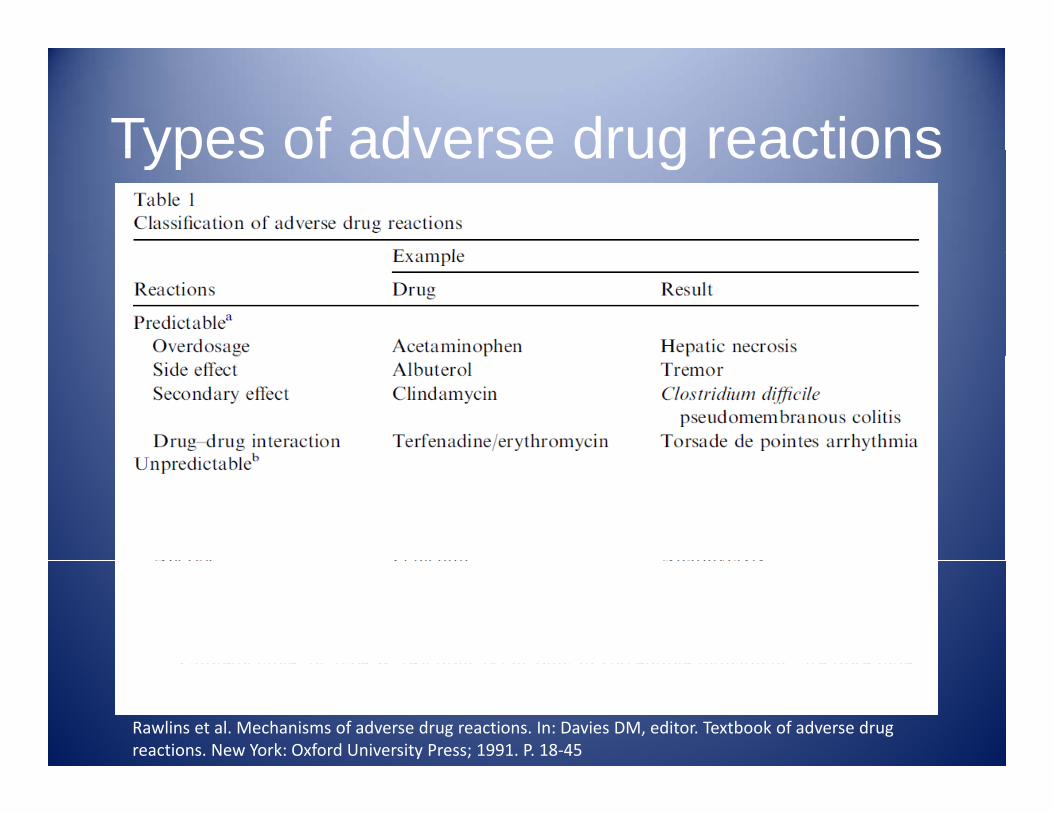
Types of adverse drug reactionsTypes of adverse drug reactions
Rawlins et al. Mechanisms of adverse drug reactions. In: Davies DM, editor. Textbook of adverse drug reactions. New York: Oxford University Press; 1991. P. 18‐45
Types of adverse drug reactionsTypes of adverse drug reactions
Rawlins et al. Mechanisms of adverse drug reactions. In: Davies DM, editor. Textbook of adverse drug reactions. New York: Oxford University Press; 1991. P. 18‐45
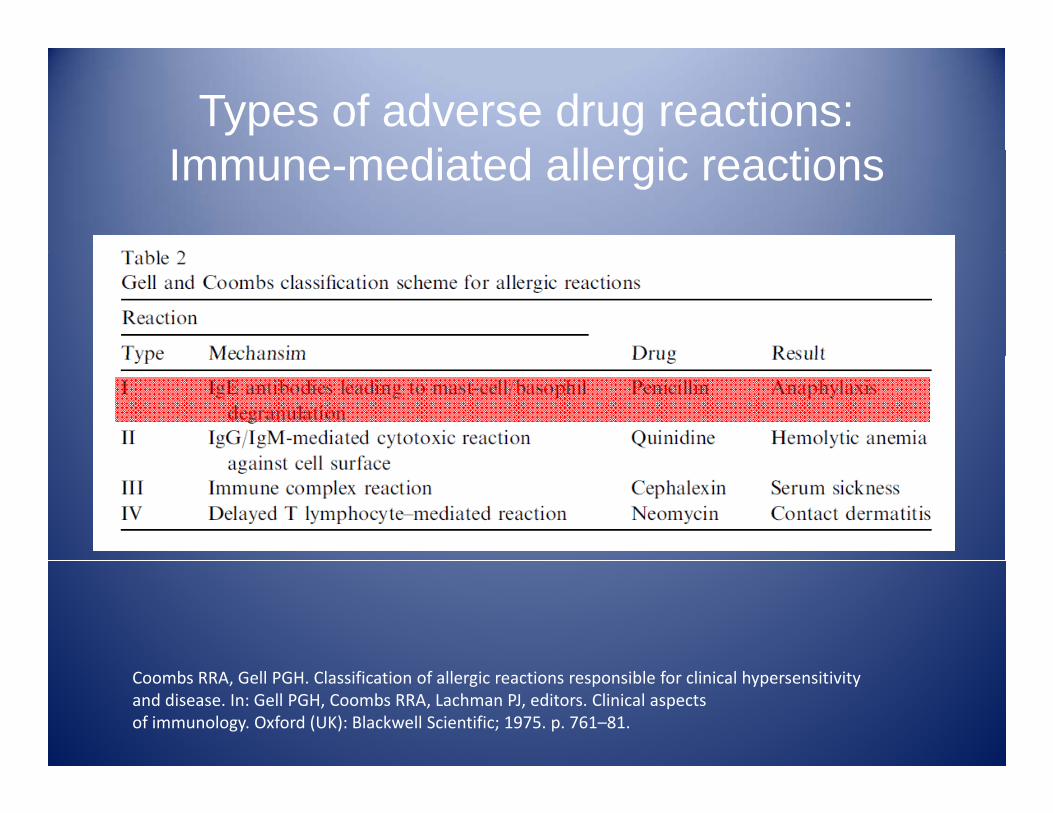
Types of adverse drug reactions:I di t d ll i tiImmune-mediated allergic reactions
Coombs RRA, Gell PGH. Classification of allergic reactions responsible for clinical hypersensitivityand disease. In: Gell PGH, Coombs RRA, Lachman PJ, editors. Clinical aspectsof immunology. Oxford (UK): Blackwell Scientific; 1975. p. 761–81.
SCARsS t d tiSevere cutaneous adverse reactions
• Comprises of:Comprises of:1. Stevens-Johnson syndrome (SJS) and toxic
epidermal necrolysis (TEN)epidermal necrolysis (TEN)2. Acute generalised exanthematous pustulosis
(AGEP)(AGEP)3. Hypersensitivity syndrome (HSS)
• Drug reaction with eosinophilia and systemic ug eac o eos op a a d sys e csymptoms (DRESS)
• Drug-induced hypersensitivity syndrome (DiHS)Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ , editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.
SCARsS t d tiSevere cutaneous adverse reactions
• Comprises of:Comprises of:1. Stevens-Johnson syndrome (SJS) and toxic
epidermal necrolysis (TEN)epidermal necrolysis (TEN)2. Acute generalised exanthematous pustulosis
(AGEP)(AGEP)3. Hypersensitivity syndrome (HSS)
• Drug reaction with eosinophilia and systemic ug eac o eos op a a d sys e csymptoms (DRESS)
• Drug-induced hypersensitivity syndrome (DiHS)Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ , editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.
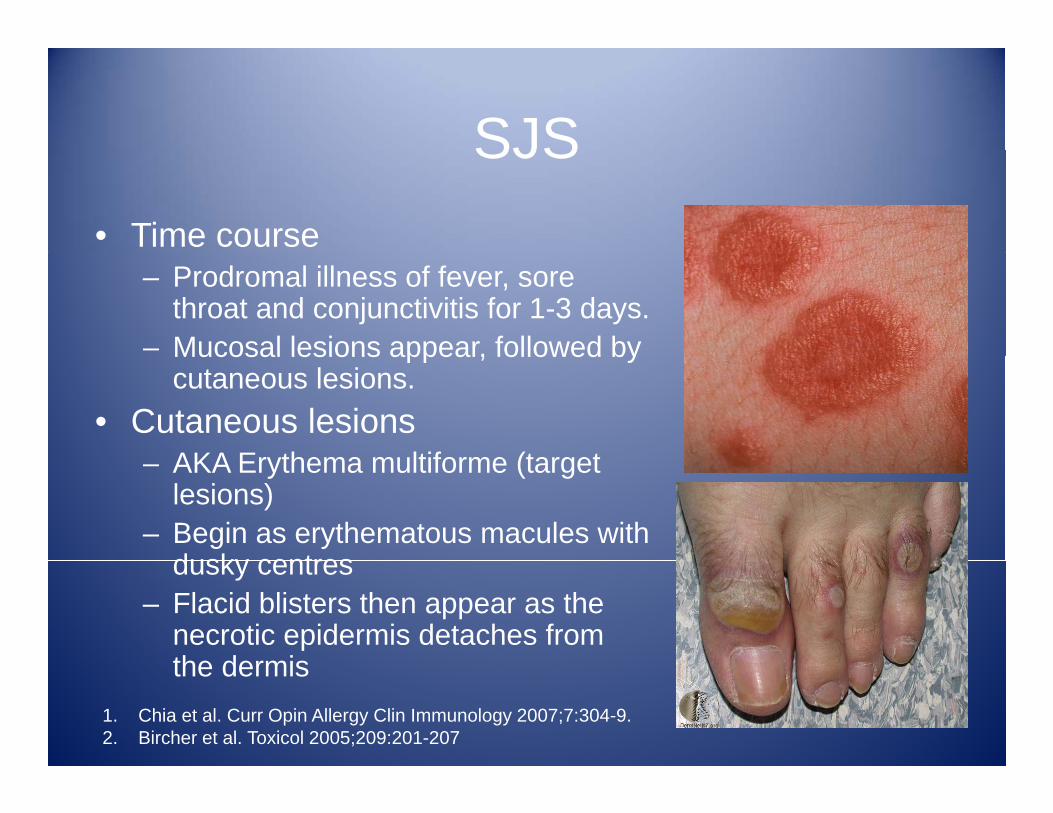
SJSSJS• Time course
– Prodromal illness of fever, sore throat and conjunctivitis for 1-3 days.
– Mucosal lesions appear, followed byMucosal lesions appear, followed by cutaneous lesions.
• Cutaneous lesionsAKA Erythema multiforme (target– AKA Erythema multiforme (target lesions)
– Begin as erythematous macules with dusky centresdusky centres
– Flacid blisters then appear as the necrotic epidermis detaches from the dermisthe dermis
1. Chia et al. Curr Opin Allergy Clin Immunology 2007;7:304-9.2. Bircher et al. Toxicol 2005;209:201-207
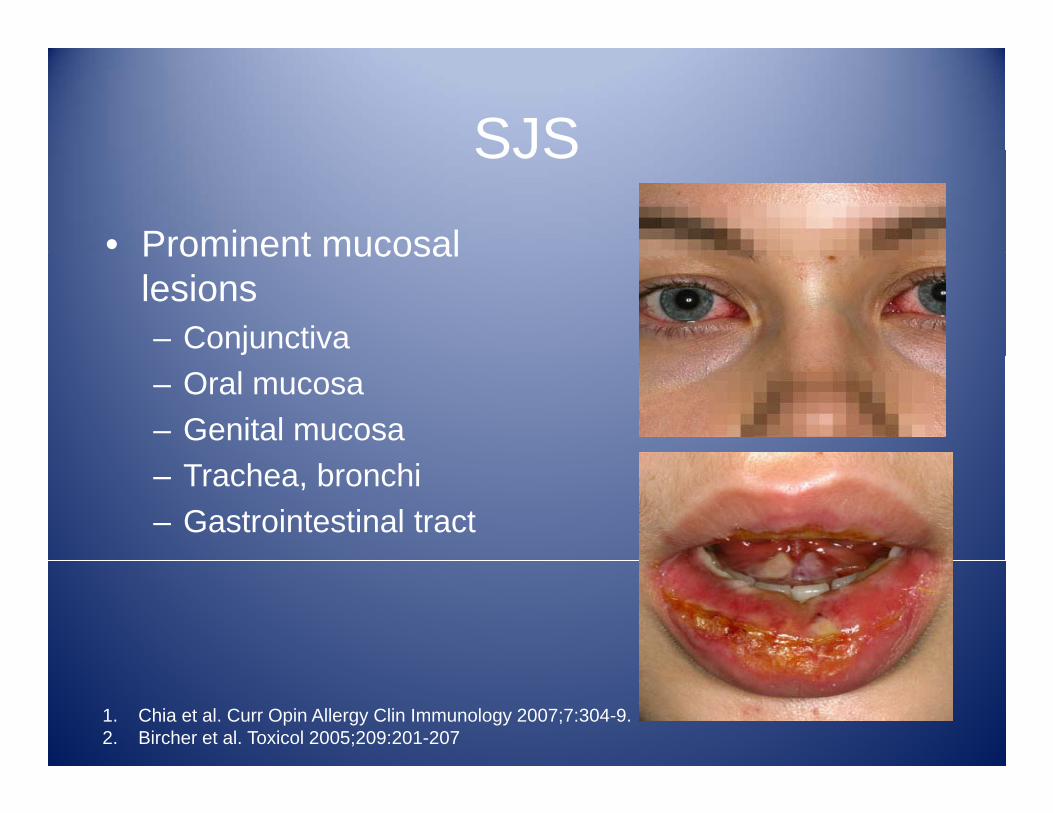
SJSSJS
• Prominent mucosalProminent mucosal lesions– Conjunctiva– Oral mucosa– Genital mucosa– Trachea, bronchi– Gastrointestinal tract
1. Chia et al. Curr Opin Allergy Clin Immunology 2007;7:304-9.2. Bircher et al. Toxicol 2005;209:201-207
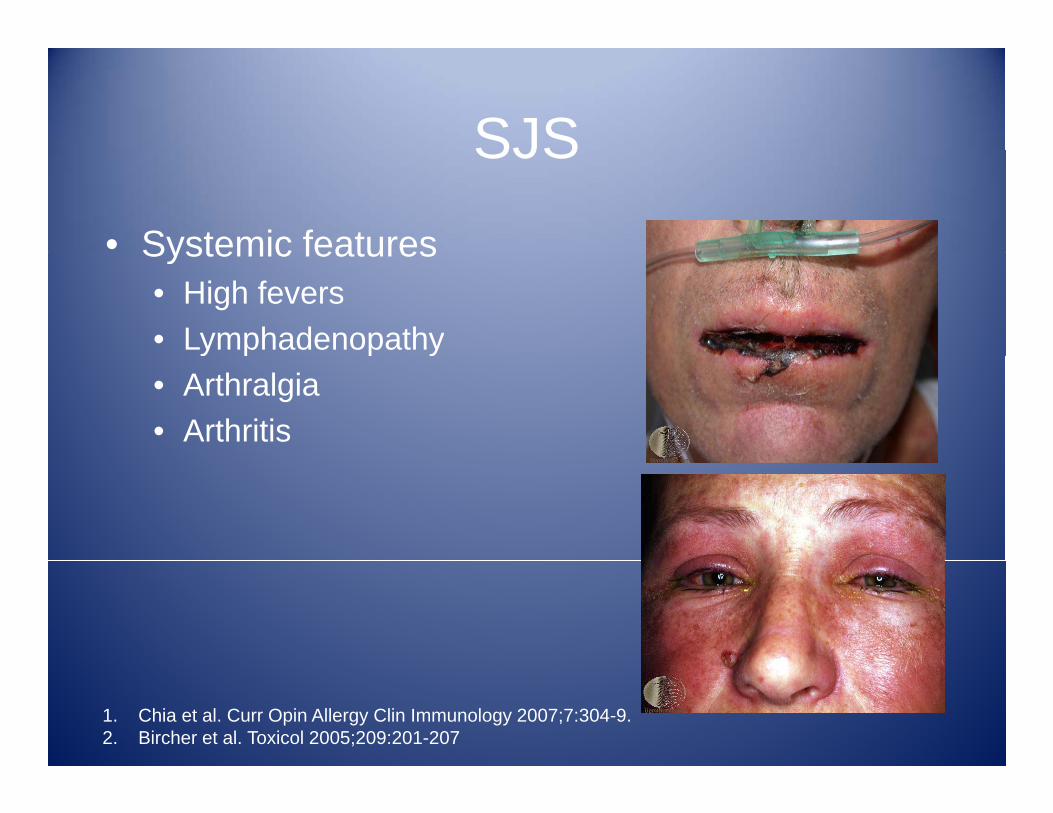
SJSSJS
• Systemic featuresSystemic features• High fevers• Lymphadenopathyy p p y• Arthralgia• Arthritis
1. Chia et al. Curr Opin Allergy Clin Immunology 2007;7:304-9.2. Bircher et al. Toxicol 2005;209:201-207
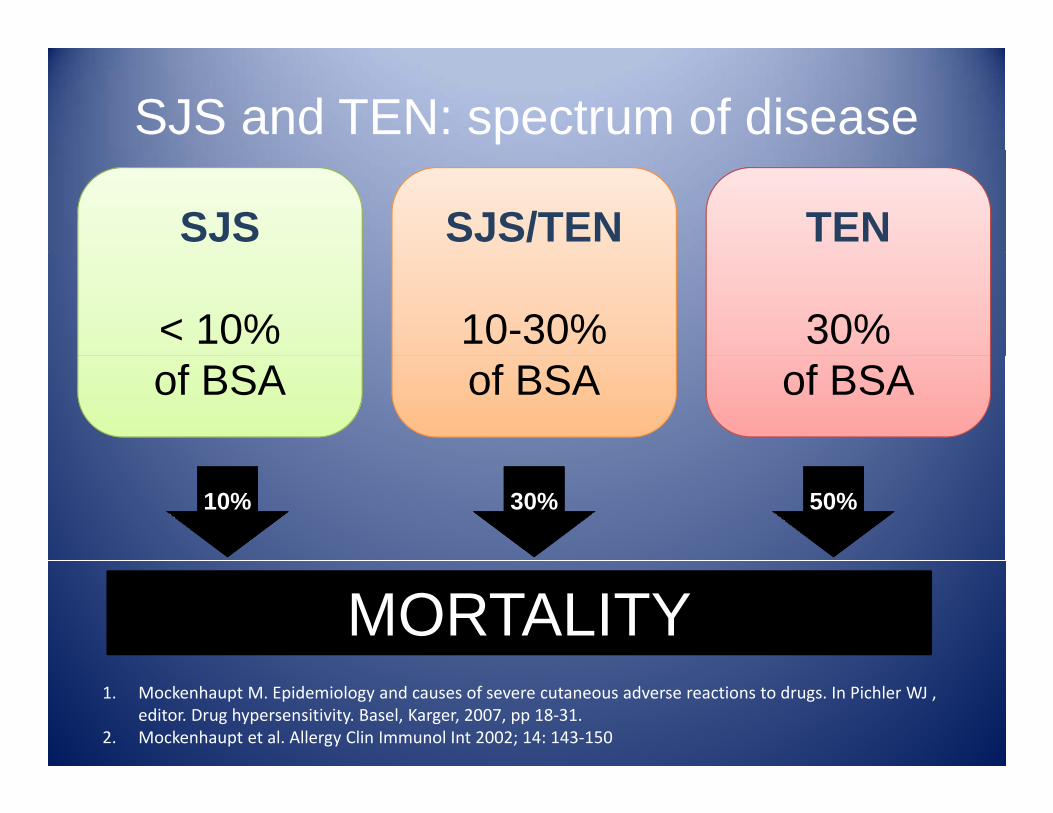
SJS and TEN: spectrum of disease
SJS SJS/TEN TEN
< 10% 10-30% 30% of BSA of BSA of BSA
10% 30% 50%
MORTALITY1. Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ ,
editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.2. Mockenhaupt et al. Allergy Clin Immunol Int 2002; 14: 143‐150
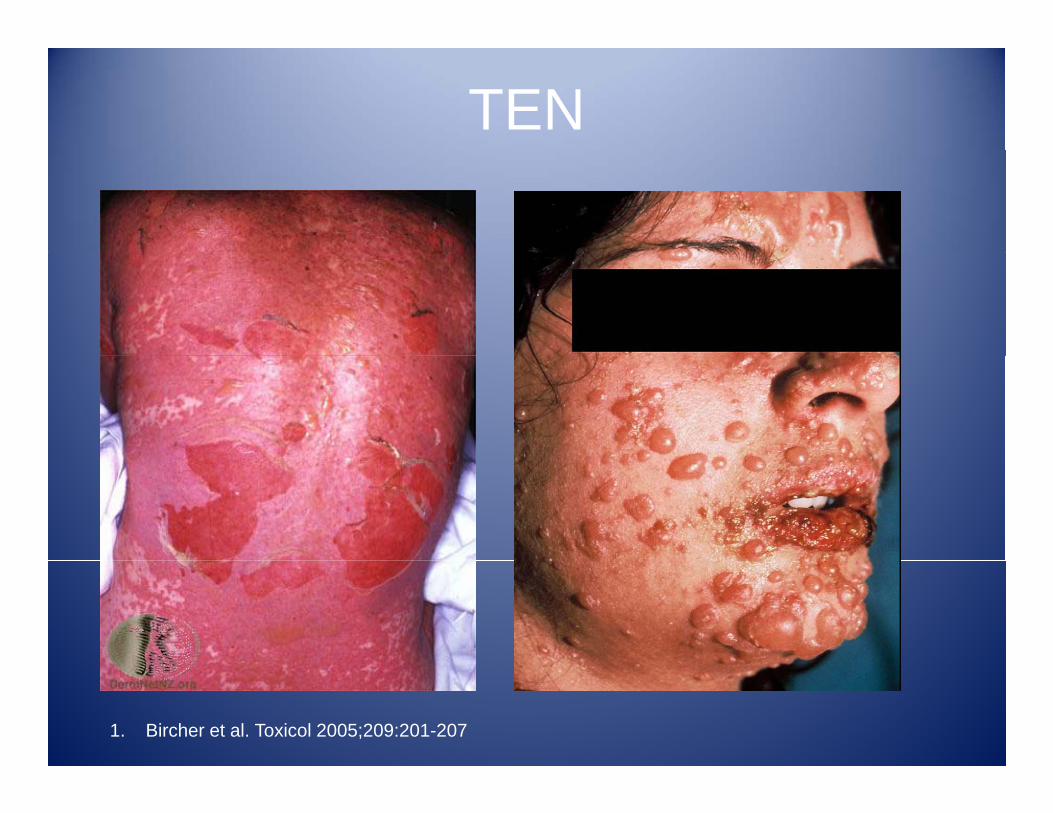
TEN
1. Bircher et al. Toxicol 2005;209:201-207
SJS and TENSJS and TEN• Onset
–Usually occurs 1-3 weeks after drug-introduction
• Culprit ‘high-risk’ drugs1. Anti-infective sulphonamides:
• Not associated with1. Beta-blockers2 ACE i hibitcotrimoxazole, sulfasalazine,
sulfadiazine, sulfadioxine, sulfafurazole
2 Allopurinol
2. ACE inhibitors3. Calcium channel
blockers4. Sulphonamide-relate 2. Allopurinol
3. Antiepileptics: carbamazepine, lamotrigine, phenytoin, phenobarbital
4 Oxicam-NSAIDs: meloxicam
Su p o a de e atediuretics
5. Sulfonylurea anti-diabetics
6 Insulin4. Oxicam-NSAIDs: meloxicam, piroxicam, tenoxicam
5. Nevirapine
6. Insulin7. Propionic acid NSAIDs
Mockenhaupt, M., C. Viboud, et al. (2008). "Stevens‐Johnson syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR‐study." Journal of Investigative Dermatology 128(1): 35‐44.
SCARsS t d tiSevere cutaneous adverse reactions
• Comprises of:Comprises of:1. Stevens-Johnson syndrome (SJS) and toxic
epidermal necrolysis (TEN)epidermal necrolysis (TEN)2. Acute generalised exanthematous pustulosis
(AGEP)(AGEP)3. Hypersensitivity syndrome (HSS)
• Drug reaction with eosinophilia and systemic ug eac o eos op a a d sys e csymptoms (DRESS)
• Drug-induced hypersensitivity syndrome (DiHS)Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ , editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.
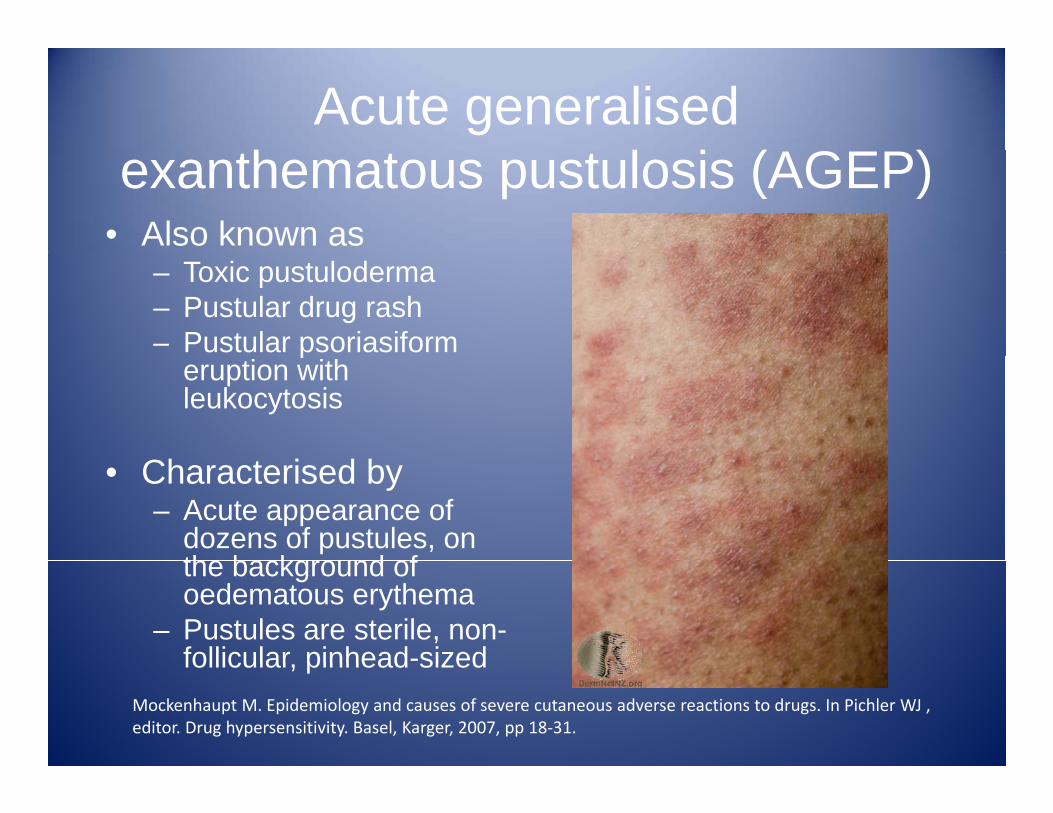
Acute generalised h l i (AGEP)exanthematous pustulosis (AGEP)
• Also known as – Toxic pustuloderma– Pustular drug rash– Pustular psoriasiformp
eruption with leukocytosis
• Characterised by– Acute appearance of
dozens of pustules, on th b k d fthe background of oedematous erythema
– Pustules are sterile, non-follicular pinhead-sizedfollicular, pinhead sized
Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ , editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.
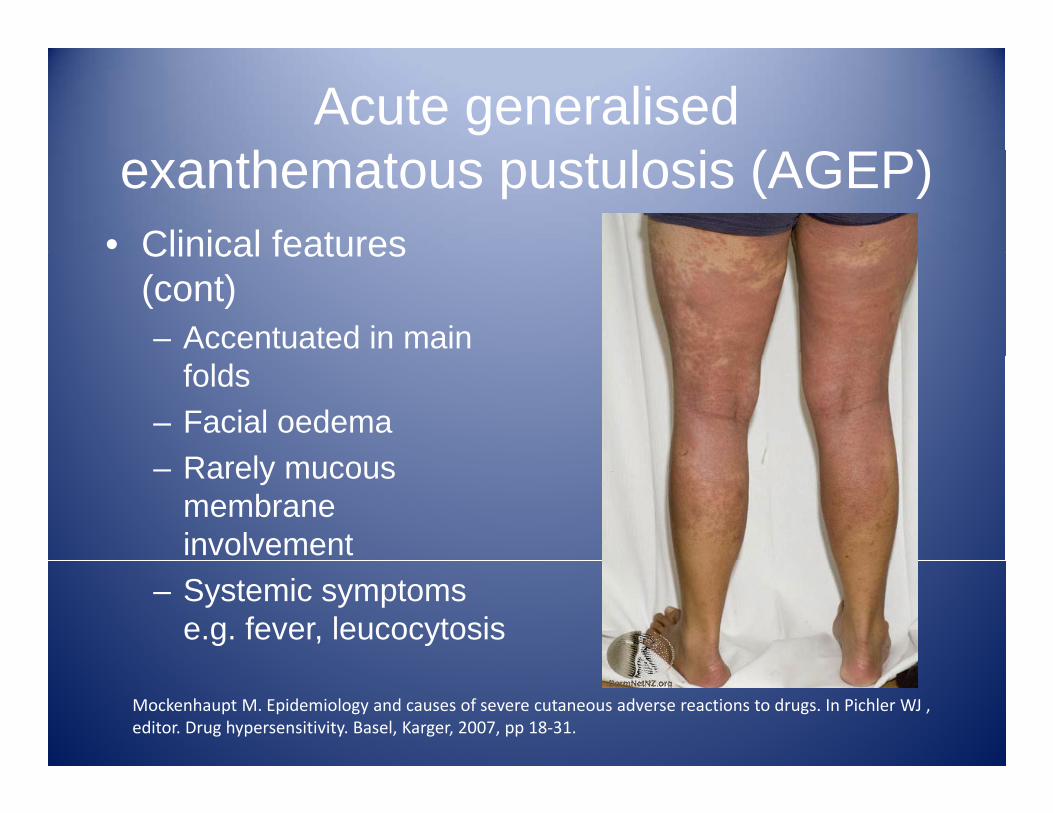
Acute generalised h l i (AGEP)exanthematous pustulosis (AGEP)
• Clinical featuresClinical features (cont)– Accentuated in main
folds– Facial oedema
R l– Rarely mucous membrane involvement
– Systemic symptoms e.g. fever, leucocytosis
Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ , editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.
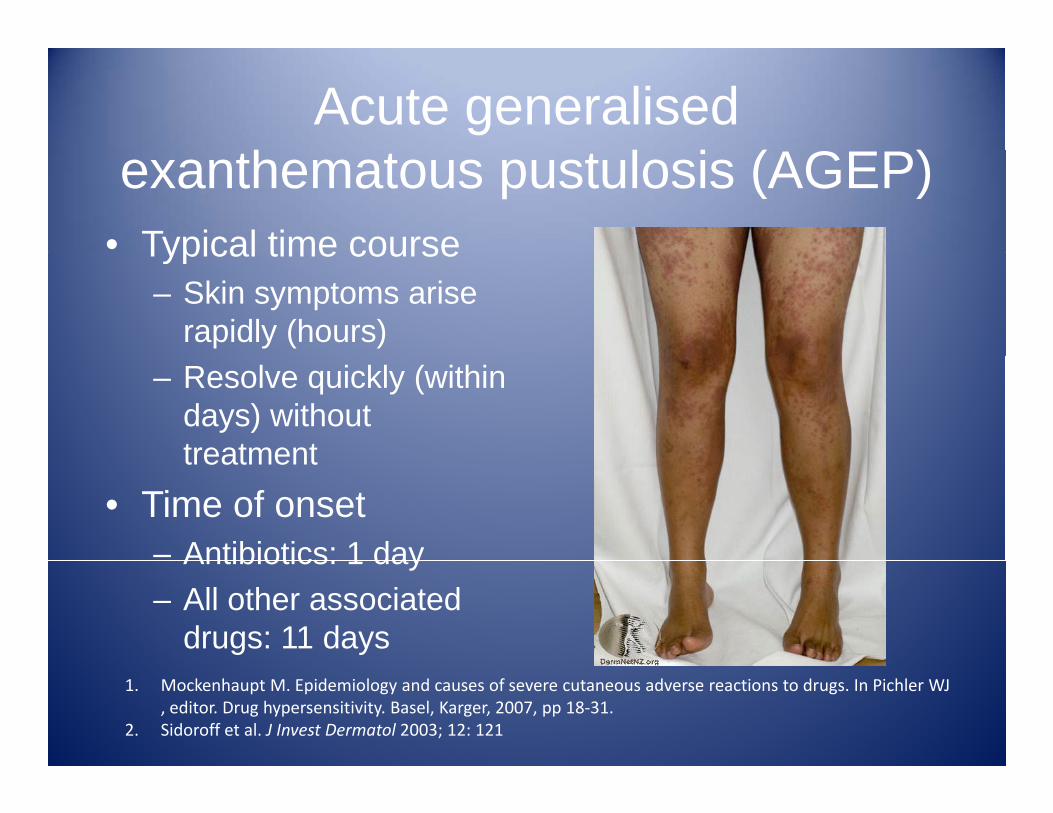
Acute generalised h l i (AGEP)exanthematous pustulosis (AGEP)
• Typical time courseTypical time course– Skin symptoms arise
rapidly (hours)– Resolve quickly (within
days) without treatmenttreatment
• Time of onset– Antibiotics: 1 dayAntibiotics: 1 day– All other associated
drugs: 11 days1. Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ
, editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.2. Sidoroff et al. J Invest Dermatol 2003; 12: 121
Acute generalised h l i (AGEP)exanthematous pustulosis (AGEP)
• Aetiologygy– Antimicrobials: pristinamycin, aminopenicillins,
quinolones, sulphonamides, terbinafineHyrdroxychloroquine– Hyrdroxychloroquine
– Diltiazem• ComplicationsComplications
– Rare– Usually in elderly or patients with poor medical
h lthhealth– Amongst 97 patients with validated cases of AGEP,
death rate was 4%1. Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ
, editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.2. Sidoroff et al. J Invest Dermatol 2003; 12: 121
SCARsS t d tiSevere cutaneous adverse reactions
• Comprises of:Comprises of:1. Stevens-Johnson syndrome (SJS) and toxic
epidermal necrolysis (TEN)epidermal necrolysis (TEN)2. Acute generalised exanthematous pustulosis
(AGEP)(AGEP)3. Hypersensitivity syndrome (HSS)
• Drug reaction with eosinophilia and systemic ug eac o eos op a a d sys e csymptoms (DRESS)
• Drug-induced hypersensitivity syndrome (DiHS)
Mockenhaupt M. Epidemiology and causes of severe cutaneous adverse reactions to drugs. In Pichler WJ , editor. Drug hypersensitivity. Basel, Karger, 2007, pp 18‐31.
HSS/DRESS/DiHSHSS/DRESS/DiHSHypersensitivity syndrome (HSS)yp y y ( )
• Traditionally used to summarise numerous severe drug reactions 1,2
• More recently, 2 other denominations were created 3,4
Drug rash with eosinophillia Drug induced and systemic symptoms
(DRESS)Hypersensitivity
Syndrome (DiHS)
1. Shear and Spielberg 1988; 2. Peyriere, Dereure et al. 2006; 3. Bocquet, Bagot et al. 1996; 4. Seishima, Yamanaka et al. 2006
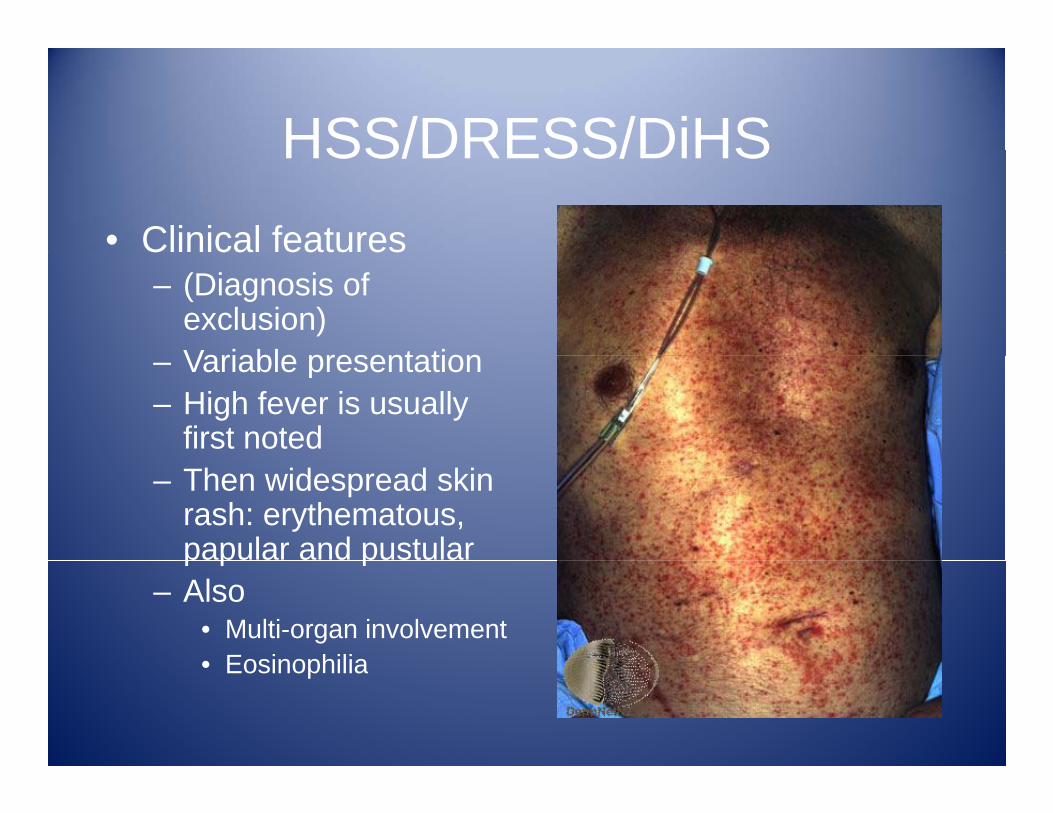
HSS/DRESS/DiHSHSS/DRESS/DiHS• Clinical features
– (Diagnosis of exclusion)Variable presentation– Variable presentation
– High fever is usually first noted
– Then widespread skin rash: erythematous, papular and pustularp p p
– Also• Multi-organ involvement• Eosinophilia• Eosinophilia
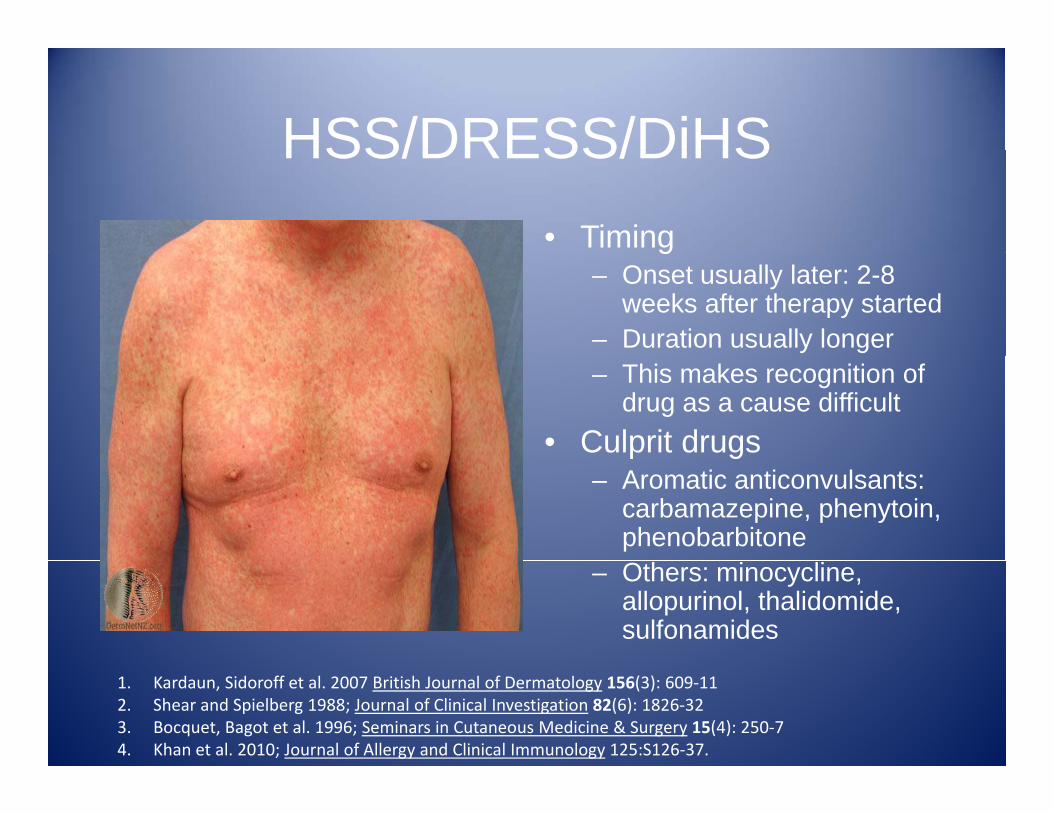
HSS/DRESS/DiHSHSS/DRESS/DiHS• Timingg
– Onset usually later: 2-8 weeks after therapy started
– Duration usually longer– This makes recognition of
drug as a cause difficult• Culprit drugsp g
– Aromatic anticonvulsants: carbamazepine, phenytoin, phenobarbitone
– Others: minocycline, allopurinol, thalidomide, sulfonamides
1. Kardaun, Sidoroff et al. 2007 British Journal of Dermatology 156(3): 609‐112. Shear and Spielberg 1988; Journal of Clinical Investigation 82(6): 1826‐323. Bocquet, Bagot et al. 1996; Seminars in Cutaneous Medicine & Surgery 15(4): 250‐74. Khan et al. 2010; Journal of Allergy and Clinical Immunology 125:S126‐37.
SCARsS t d tiSevere cutaneous adverse reactions
• Take home pointsTake home points1. Important to recognise these conditions2 High morbidity and mortality2. High morbidity and mortality3. Presents as a contraindication to skin testing
and drug provocation testingand drug provocation testing
Drug allergy: talk outlineDrug allergy: talk outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs
Epidemiology I E di t d d llIgE mediated drug allergy
• Penicillin allergy– Self-reported versus post-assessment
• Rate of self-reported penicillin allergy is 10% 1• Following evaluation > 90% are able to tolerate drug 2,3Following evaluation > 90% are able to tolerate drug
– Possible explanations?• Mislabelled as allergic due to other cause e.g. viral-induced
Loss of penicillin specific IgE antibodies o er time• Loss of penicillin-specific IgE antibodies over time– Why bother?
• Patients incorrectly labelled as penicillin-allergic more likely t b t t d ith i b d t tibi ti 4to be treated with expensive, broad-spectrum antibiotics 4
• This can lead to development and spread of multi-drug resistant bacteria
1. Solensky, R. (2003). Clinical Reviews in Allergy & Immunology 24(3): 201‐20.2. Sogn, D. D., R. Evans, 3rd, et al. (1992). Archives of Internal Medicine 152(5): 1025‐32.3. Gadde, J., M. Spence, et al. (1993). JAMA 270(20): 2456‐63.4. Solensky, R., H. S. Earl, et al. (2000). Annals of Allergy, Asthma, & Immunology 84(3): 329‐33
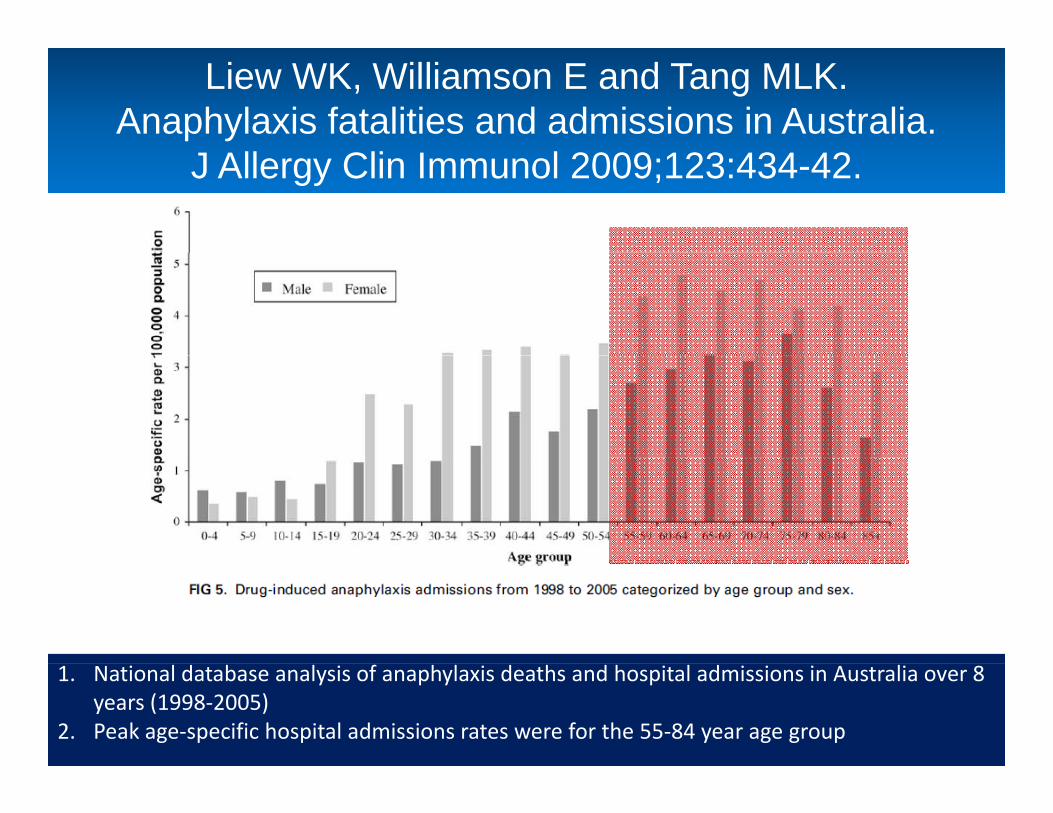
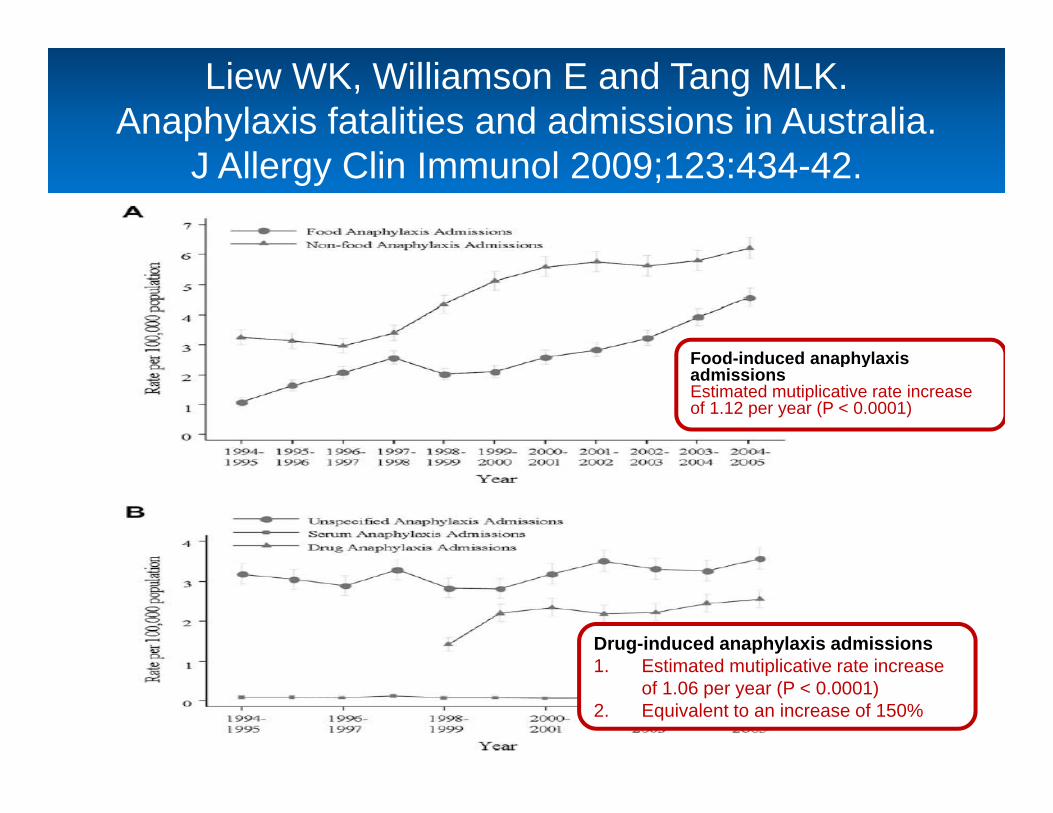
Liew WK, Williamson E and Tang MLK. Anaphylaxis fatalities and admissions in Australia.
J Allergy Clin Immunol 2009;123:434-42.
1. National database analysis of anaphylaxis deaths and hospital admissions in Australia over 8 years (1998‐2005)
2. Peak age‐specific hospital admissions rates were for the 55‐84 year age group
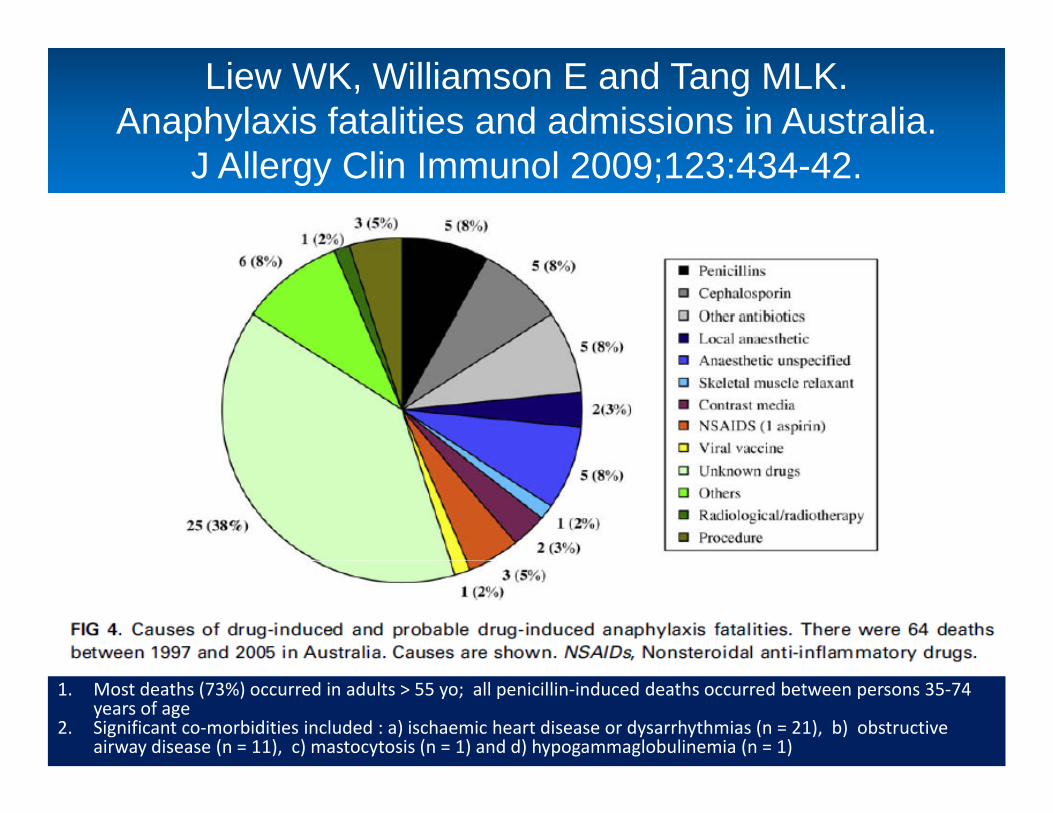
Liew WK, Williamson E and Tang MLK. Anaphylaxis fatalities and admissions in Australia.
J Allergy Clin Immunol 2009;123:434-42.
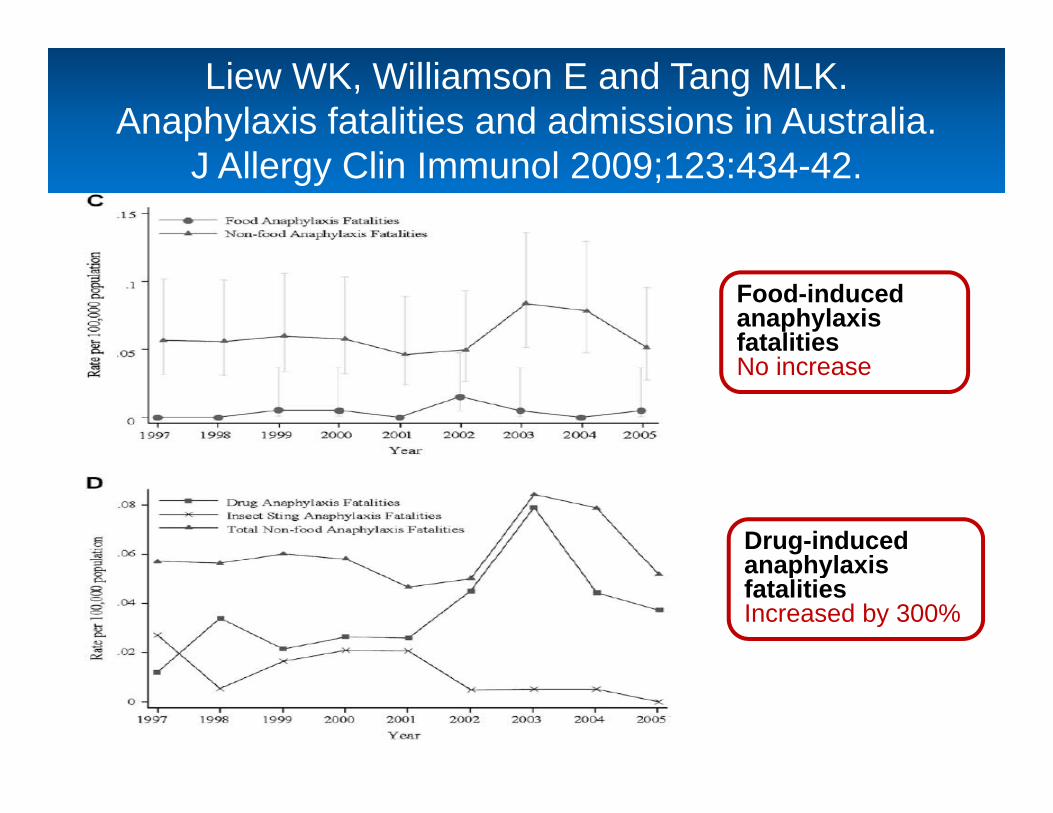
1. Most deaths (73%) occurred in adults > 55 yo; all penicillin‐induced deaths occurred between persons 35‐74 years of age
2. Significant co‐morbidities included : a) ischaemic heart disease or dysarrhythmias (n = 21), b) obstructive airway disease (n = 11), c) mastocytosis (n = 1) and d) hypogammaglobulinemia (n = 1)
Liew WK, Williamson E and Tang MLK. Anaphylaxis fatalities and admissions in Australia.
J Allergy Clin Immunol 2009;123:434-42.
Food induced anaphylaxisFood-induced anaphylaxis admissionsEstimated mutiplicative rate increase of 1.12 per year (P < 0.0001)
Drug-induced anaphylaxis admissions1 Estimated mutiplicative rate increase1. Estimated mutiplicative rate increase
of 1.06 per year (P < 0.0001)2. Equivalent to an increase of 150%
Liew WK, Williamson E and Tang MLK. Anaphylaxis fatalities and admissions in Australia.
J Allergy Clin Immunol 2009;123:434-42.
Food-induced anaphylaxis fatalitiesNo increase
Drug-induced anaphylaxisanaphylaxis fatalities Increased by 300%
Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs
Mechanism of actionMechanism of action
• HaptensHaptens– Most medications are small in size are not
able to elicit an immune response independently
– Drugs must first covalently bind to larger carrier molecules (e g tissue/serum proteins)carrier molecules (e.g. tissue/serum proteins) to act as complete multivalent antigens
– This process is haptenization with the drugThis process is haptenization, with the drug acting as a hapten
1. Park, B. K., J. W. Coleman, et al. (1987). "Drug disposition and drug hypersensitivity." Biochemical Pharmacology 36(5): 581‐90.
2. Solensky, R. (2006). "Drug hypersensitivity." Medical Clinics of North America 90(1): 233‐60.
Mechanism of actionMechanism of action
• Native versus active statesNative versus active states– Most drugs are chemically inert in native state1
• Most need to be enzymatically metabolized to y ychemically reactive intermediates then form covalent bonds with macromolecules to elicit an immune responseresponse
– Penicillin is an exception 2• Spontaneously degrades under physiologic conditions
to reactive intermediates capable of binding proteins
1. Park, B. K., J. W. Coleman, et al. (1987). "Drug disposition and drug hypersensitivity." Biochemical Pharmacology 36(5): 581‐90.
2. Solensky, R. (2003). "Hypersensitivity reactions to beta‐lactam antibiotics." Clinical Reviews in Allergy & Immunology 24(3): 201‐20.
Mechanism of actionMechanism of action
• StepsSteps1. Drug undergoes enzymatic metabolisation
into its active state2. Covalent bonding to macromolecules3. An immune response can be elicited via..
– Humoral pathway: with production of specific antibodies e.g. IgE, or
– Cellular pathway: generation of specific TCellular pathway: generation of specific T lymphocytes, or
– Both pathways
Solensky, R. (2006). "Drug hypersensitivity." Medical Clinics of North America 90(1): 233‐60.
Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs
Important points on historyImportant points on history• What was the name of the medication?
– Penicillin vs amoxycillin/augmentin– Frequently this is not accurately recalled,
becausebecause• Time elapsed since last reaction• Similar name with another medication
M ltiple dr g reactions s spected• Multiple drug reactions suspected• Time course and duration of symptoms
– How long ago did reaction occur?How long ago did reaction occur?• Important as some allergies wane over time
– When during the course did it occur?
1. Solensky, R. (2006). "Drug hypersensitivity." Medical Clinics of North America 90(1): 233‐60.2. Khan et al. (2010). “Drug allergy.” Journal of Allergy and Clinical Immunology 125:S126‐37.
Important points on historyImportant points on history• Which systems were involved?Which systems were involved?
– Cutaneous• Mucous membrane involvement?• Urticarial vs bullous vs exfoliative vs morbiliform?
– Other• Gastrointestinal respiratory arthropathy feverGastrointestinal, respiratory, arthropathy, fever
• What illness was the medication prescribed for?– E.g. Cellulitis versus viral upper respiratory tract
infection
1. Solensky, R. (2006). "Drug hypersensitivity." Medical Clinics of North America 90(1): 233‐60.2. Khan et al. (2010). “Drug allergy.” Journal of Allergy and Clinical Immunology 125:S126‐37.
Important points on historyImportant points on history
• Concurrent medications prescribed?Concurrent medications prescribed?– E.g. Narcotics, NSAIDs – may in fact be the
culprit medicationp• Previous course of same/similar medication?
– May suggest past sensitisationMay suggest past sensitisation• Previous episodes of similar symptoms in the
absence of drug treatment?absence of drug treatment?– Suggestive of idiopathic urticaria
1. Solensky, R. (2006). "Drug hypersensitivity." Medical Clinics of North America 90(1): 233‐60.2. Khan et al. (2010). “Drug allergy.” Journal of Allergy and Clinical Immunology 125:S126‐37.
Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs
InvestigationsInvestigations
• Commonly performedCommonly performed1. Skin prick test2 Intradermal test2. Intradermal test3. Drug provocation test (challenge)
L l d• Less commonly used1. Serum sIgE2. Basophil activation assay3. Patch testing
Less commonly used investigationsLess commonly used investigations
1 Serum sIgE1. Serum sIgE– Detects antigen-specific IgE antibodies in
subject’s serumsubject s serum– Most are not adequately validated– Unclear specificity and sensitivity– Unclear specificity and sensitivity– Difficult to bind drug allergens to solid-phase
matricesmatrices
Khan DA and Solensky R. Drug allergy. Journal of Allergy and Clinical Immunology 2010;125:s126-37.
Less commonly used investigationsLess commonly used investigations
2 Basophil activation test2. Basophil activation test– Uses flow cytometry to quantify the expression of
activation markers (CD63 or CD203C) on ( )basophils after stimulation with an allergen1
– Currently there is only limited data using this method to evaluate patients with possible drug allergies1
Diagnostic sensitivity and specificity is poor when– Diagnostic sensitivity and specificity is poor when directly compared to skin testing2
1. Khan DA and Solensky R. Drug allergy. JACI 2010;125:s126-37.2. Hamilton RG and Adkinson NF Jr. In vitro assays for the diagnosis of
IgE-mediated disorders. JACI 2004;114:213-225.
Less commonly used investigationsLess commonly used investigations
3. Drug patch testing1,23. Drug patch testing– Patches placed on the upper back– Read at 20 minutes, with delayed readings atRead at 20 minutes, with delayed readings at
48 hours, 96 hours and (if negative) 7 days.– Might be useful for presumed non-IgE
delayed cutaneous drug reactions e.g. maculopapular exanthems, AGEP, fixed drug eruptionseruptions
– Not helpful for SJS or urticarial reactions
1. Khan DA and Solensky R. Drug allergy. JACI 2010;125:s126-37.2. Barbaud A. Drug patch testing in systemic cutaneous drug allergy.
Toxicology 2005;209:209-16.
Commonly performed investigations
Skin prick test
Intradermalskin test
Drug challenge
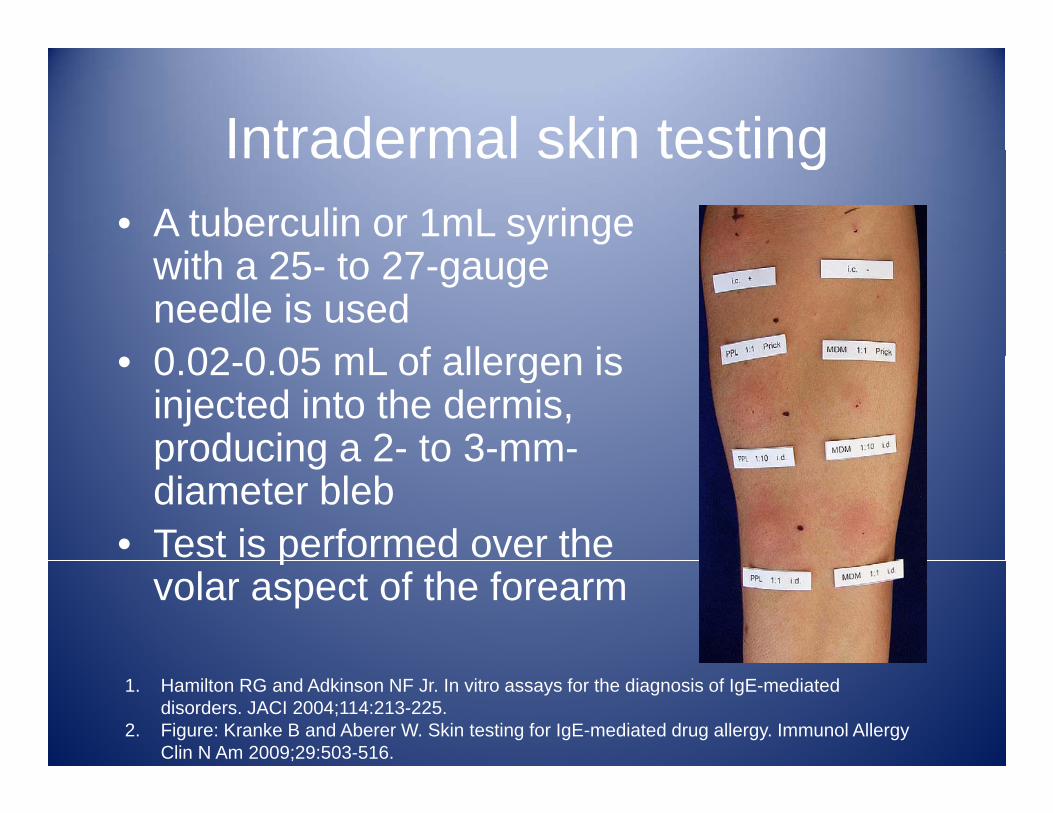
Intradermal skin testingIntradermal skin testing• A tuberculin or 1mL syringe
ith 25 t 27with a 25- to 27-gauge needle is used0 02 0 05 mL of allergen is• 0.02-0.05 mL of allergen is injected into the dermis, producing a 2- to 3-mm-producing a 2 to 3 mmdiameter bleb
• Test is performed over the pvolar aspect of the forearm
1. Hamilton RG and Adkinson NF Jr. In vitro assays for the diagnosis of IgE-mediated disorders. JACI 2004;114:213-225.
2. Figure: Kranke B and Aberer W. Skin testing for IgE-mediated drug allergy. Immunol Allergy Clin N Am 2009;29:503-516.
Intradermal skin testingIntradermal skin testing
• European Network for Drug AllergyEuropean Network for Drug Allergy (ENDA) position paper in 2003 outlines the following scoring method1following scoring method– Read at 15-20 minutes after performance of
testtest– Positive if wheal increased by > 3 mm with an
associated flare, when compared to initialassociated flare, when compared to initial wheal
Torres et al. Diagnosis of immediate allergic reactions to beta-lactamantibiotics. Allergy 2003; 58: 961-972.
Intradermal skin testingIntradermal skin testing
• However, studies following this scoringHowever, studies following this scoring system has been variable
• The other common scoring system isThe other common scoring system is– Positive intradermal test when any wheal
diameter is > 5 mm– This method has been used in a number of
European studies 1,2,3,4
• This needs to be noted when comparing results from different centres
1. Blanca‐Lopez et al. Allergy 2009: 64: 229‐233; 2. Romano et al. Allergy 2007: 62: 53‐58; 3. Romano et al. Ann Intern Med 2004; 141: 16‐22; 4. Mendelson et al. JACI 1984; 73: 76‐81.
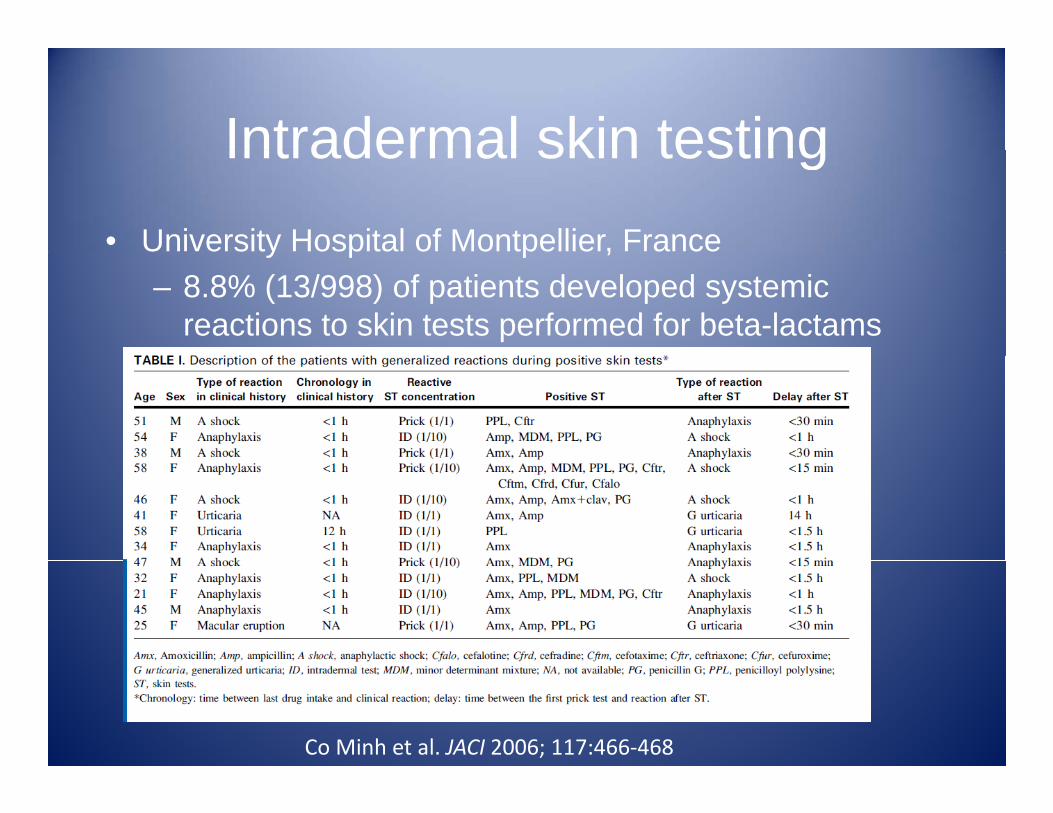
Intradermal skin testingIntradermal skin testing• University Hospital of Montpellier, Francey p p ,
– 8.8% (13/998) of patients developed systemic reactions to skin tests performed for beta-lactams b t 1996 2004between 1996-2004
Co Minh et al. JACI 2006; 117:466‐468