Embed Size (px)
Citation preview

The Importance of Reporting Adverse Drug Reactions and Creating a Culture of Safety
Kristy Malacos
Magruder Hospital
Pharmacy Systems Inc
Objectives
bull Describe Adverse Drug Reactions (ADR)and the importance of reporting for patient safety
bull Illustrate the benefit of successful reporting and how to implement a reporting system and utilize reporting tools
bull Explain the importance of a successful ADR reporting program within the hospital to help create a culture of safety
What is an ADR
bull Harmful unintended reaction to medication that occurs at doses normally used for treatment
ndash World Health Organization
ADR (ASHP)
bull Undesirable experience associated with the use of a medication that may result inndash discontinuing the drugndash changing the drug therapyndash modifying the dosendash necessitates admission to a hospital or prolongs stayndash necessitates supportive treatmentndash significantly complicates diagnosisndash negatively affects prognosisndash results in temporary or permanent harm disability or
death
Side Effects
bull Expected well-documented reactions
bull Results in little or no change in patient management
Reporting of Medication Events
Adverse Drug Events
bull Medication error
bull Medication administration error
bull Inappropriate dose reductionincrease
Adverse Drug Reactions
bull Harm caused by drug therapy at normal clinical dose and during normal use
ndash Includes allergic reactions
ndash Includes drug product and vaccine issues
Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
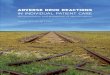
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
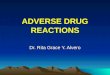
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Objectives
bull Describe Adverse Drug Reactions (ADR)and the importance of reporting for patient safety
bull Illustrate the benefit of successful reporting and how to implement a reporting system and utilize reporting tools
bull Explain the importance of a successful ADR reporting program within the hospital to help create a culture of safety
What is an ADR
bull Harmful unintended reaction to medication that occurs at doses normally used for treatment
ndash World Health Organization
ADR (ASHP)
bull Undesirable experience associated with the use of a medication that may result inndash discontinuing the drugndash changing the drug therapyndash modifying the dosendash necessitates admission to a hospital or prolongs stayndash necessitates supportive treatmentndash significantly complicates diagnosisndash negatively affects prognosisndash results in temporary or permanent harm disability or
death
Side Effects
bull Expected well-documented reactions
bull Results in little or no change in patient management
Reporting of Medication Events
Adverse Drug Events
bull Medication error
bull Medication administration error
bull Inappropriate dose reductionincrease
Adverse Drug Reactions
bull Harm caused by drug therapy at normal clinical dose and during normal use
ndash Includes allergic reactions
ndash Includes drug product and vaccine issues
Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

What is an ADR
bull Harmful unintended reaction to medication that occurs at doses normally used for treatment
ndash World Health Organization
ADR (ASHP)
bull Undesirable experience associated with the use of a medication that may result inndash discontinuing the drugndash changing the drug therapyndash modifying the dosendash necessitates admission to a hospital or prolongs stayndash necessitates supportive treatmentndash significantly complicates diagnosisndash negatively affects prognosisndash results in temporary or permanent harm disability or
death
Side Effects
bull Expected well-documented reactions
bull Results in little or no change in patient management
Reporting of Medication Events
Adverse Drug Events
bull Medication error
bull Medication administration error
bull Inappropriate dose reductionincrease
Adverse Drug Reactions
bull Harm caused by drug therapy at normal clinical dose and during normal use
ndash Includes allergic reactions
ndash Includes drug product and vaccine issues
Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

ADR (ASHP)
bull Undesirable experience associated with the use of a medication that may result inndash discontinuing the drugndash changing the drug therapyndash modifying the dosendash necessitates admission to a hospital or prolongs stayndash necessitates supportive treatmentndash significantly complicates diagnosisndash negatively affects prognosisndash results in temporary or permanent harm disability or
death
Side Effects
bull Expected well-documented reactions
bull Results in little or no change in patient management
Reporting of Medication Events
Adverse Drug Events
bull Medication error
bull Medication administration error
bull Inappropriate dose reductionincrease
Adverse Drug Reactions
bull Harm caused by drug therapy at normal clinical dose and during normal use
ndash Includes allergic reactions
ndash Includes drug product and vaccine issues
Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Side Effects
bull Expected well-documented reactions
bull Results in little or no change in patient management
Reporting of Medication Events
Adverse Drug Events
bull Medication error
bull Medication administration error
bull Inappropriate dose reductionincrease
Adverse Drug Reactions
bull Harm caused by drug therapy at normal clinical dose and during normal use
ndash Includes allergic reactions
ndash Includes drug product and vaccine issues
Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Reporting of Medication Events
Adverse Drug Events
bull Medication error
bull Medication administration error
bull Inappropriate dose reductionincrease
Adverse Drug Reactions
bull Harm caused by drug therapy at normal clinical dose and during normal use
ndash Includes allergic reactions
ndash Includes drug product and vaccine issues
Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Steps to Implementing an ADR Reporting Program
EducateMonitor and Investigate
Communicate
Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Part 1 - Education
bull Do our nursesstaff understand what an ADR looks like and when to report
bull Do our nursesstaff understand the value in reporting ADRs
bull Do our nursesstaff know wherehow to report an ADR
Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Why Arenrsquot ADRs Reported
bull Lack of knowledge about the reporting systems or perceived difficulty
bull Uncertainty about whether or not a drug is the cause of an adverse eventndash Concern about medical liability or professional disciplinary
action
bull Lack of time or high workload
bull Lack of understanding about why it is important to report
bull Complacency (believing that serious ADRs are well documented when the drug is released in the market)
Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Are ADRs Always Preventable
bull Majority of preventable ADRs occur at prescribing and monitoring stages
Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Who is most at risk for ADRs
bull Elderly
bull Patients taking multiple medications
bull Patients taking medications from specific classes
ndash Antidiabetics and hypoglycemic agents
ndash Cardiovascular drugs
ndash Psychotropics
ndash Anticonvulsants
ndash Antineoplastics
ndash Corticosteroids
What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

What Costs are Associated with ADRs
bull Ambulatory-setting cost impact of drug-related problems estimated at $766 billion in 1995
bull Cost estimated at $1774 billion in 2000
ndash New prescriptions
ndash Doctors visits
ndash Admission to hospital
ndash ED visit
ndash LTC admission
Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Why are there so Many
bull 75 of patient visits result in a prescription
bull Medicare Patients
ndash 89 take a prescription medicine daily
ndash 46 take greater than 5 prescriptions chronically
ndash 54 take meds prescribed by 2 or more doctors
ndash 5 obtain an Rx from CanadaMexico ƒ
bull ADRs increase exponentially with greater than 4 prescriptions
CDC Fast Stats
How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

How Do We Report an ADR
Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Part 2 ndash Monitor and Investigate
bull Monitor reporting and evaluate for ADRs
ndash Provide follow up to reporter
bull Investigate potential trends using medication-use evaluation (MUE)
bull Identify unreported ADRs through Trigger Tool
Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Reporting Increase
0
5
10
15
20
25
2014 2015
ADR Events Reported
Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Investigate Trends
Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Investigate through MUE
bull A process focused on evaluating and improving the usage of a medication with the goal of improving patient outcomes
bull Analyze prescribing trends
ndash Examine guidelines treatment protocols and standards of care for specific medication and medication-use processes based on data from recent literature
bull Collect data and evaluate usage
Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Indications an MUE is Needed
bull Increase in ADRs or medication errors
bull Multiple occurrences of treatment failure
bull Pharmacy intervention consistently necessary
bull Expensive medication
Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Interpreting the Data
bull Develop and implement plans for improvement of the medication- use process based on MUE findings (if indicated)
bull Recommend changes (if any) or suggest alternatives to current prescribing
bull After changes implemented continue to collect data
Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Ciprofloxacin MUE
bull By August of 2015 14 ADRs reported
ndash 6 related to infusion of Ciprofloxacin
bullCiprofloxacin is being infused over 60 minutes in the ED but infusion time appears to be increased in MedSurg and ICU to 90-120 minutes
Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Ciprofloxacin MUE
Total Ciprofloxacin Doses in 2014 175
Patients Given in ED and Admitted 99
Patients Given in ED and Discharged 43
Patients Given Ciprofloxacin in MedSurg 20
Patients Given in Surgery 2
Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Ciprofloxacin MUE
Cost of Levaquin (levofloxacin) Cost of Cipro (ciprofloxacin)
250mg50mL bag $204 200mg100mL $125
500mg100mL bag $298 400mg200mL $215
750mg150mL bag $2676
bullNo Levaquin ADRs have been reported
bullGiving Levaquin for all 175 doses of Cipro dispensed in 2014 would create a cost increase of $1027 for ciprofloxacin 200mg and $13446 for 400mg = total increase of $14473
Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Ciprofloxacin MUE
bull Can increase infusion time with no disruption in efficacy
bull Antibiogram shows greater susceptibility to Levaquin then Ciprofloxacin for all areas except pseudomonas
bull Diagnoses most prevalent (UTI and divertulitis) also indicated with Levaquin
MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

MUE Recommendations
bull Increase infusion time from 60 minutes to 90 minutes
ndash ED patients being admitted 70 so will not need to worry about infusion time lengthening stay
bull Remove Ciprofloxacin from pre-built order sets for prescribers
ndash Propose utilizing Levaquin instead of Cipro for UTI diverticulitis and when appropriate
Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Monitor Results
bull Since implementing recommendations 1 ADR related to ciprofloxacin
ndash Utilized Smart Pump software to determine pre-programmed infusion rate was overridden and infused at 60 minutes
Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Increase Reporting
bull Use Smart Pump software for trends of infusion rates being consistently overridden
ndash Evaluate if any overrides created infusion-related ADRs
Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Increase Reporting
bull Examine patients who were given antidotes
bull Was this given as an antidote for an ADR
ndash Was it reportedTrigger Process identified
T1 Diphenhydramine Hypersensitivity reaction or drug effect
T2 Vitamin K Over-anticoagulation with warfarin
T3 Flumazenil Oversedation with benzodiazepine
T4 Droperidol Nauseaemesis related to drug use
T5 Naloxone Oversedation with narcotic
Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Increase Reporting
bull Create an ADR committee charged with increasing and monitoring ADR reporting
ndash Promotes interdisciplinary problem solving
bull Inservices held with all departments to educate (food always works)
Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Part 3 - Communication
bull Disseminate information from PampT Committee
bull Share data with nursing staff
ndash Value of reporting is realized when changes are implemented as a result
bull Communicate through meetingnewsletter
Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Internal Reporting Mechanism
Contrast Monitoring (Radiology)
Spontaneous Drug Product Issues
Pharmacist Review of Orders
Retrospective Identification in coding
Medication Use Evaluations
Retrospective Drug Monitoring
ADR Reporting Program
Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Creating a Culture of Safety
bull Just Culture addresses behavior and analyzes systems and workflows in place when evaluating errors
bull Encourages reporting of events and coaching at-risk behaviors non-punitive response
bull Open dialogue promotes discussion among departments
Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Reporting of Medication Events
0
20
40
60
80
100
120
140
Actual Near Miss ADR Total
2015 Total
2014 Total
2013 Total
35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

35
44
39
23
38
48
38
29
36
49
39
22
49
5759
32
60
65
68
48
44
5048
35
51
58
52
43
0
10
20
30
40
50
60
70
80
Composite Score Staff feel like theirmistakes are held against
them
When an event isreported it feels like theperson is being written
up not the problem
Staff worry that mistakesthey make are kept in
their personnel file
NONPUNITIVE RESPONSE TO ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

54
74
35
54
50
71
30
50
47
62
34
45
56
71
36
60
69
84
54
69
62
76
48
6365
79
50
67
0
10
20
30
40
50
60
70
80
90
Composite Score Staff will freely speak up ifthey see something that maynegatively affect patient care
Staff feel free to question thedecisions or actions of those
with more authority
Staff are afraid to askquestions when something
does not seem right
COMMUNICATION OPENNESS
2008 2010 2012 2014 2016 National 6-24 Beds
58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

58
45
62
68
52
42
53
60
49
38
51
5856
44
60
65
70
62
67
81
67
59
67
73
69
60
70
77
0
10
20
30
40
50
60
70
80
90
Composite Score We are given feedback aboutchanges put into place based
on event errors
We are informed abouterrors that happen in this unit
In this unit we discuss waysto prevent errors from
happening again
FEEDBACK AND COMMUNICATION REGARDING ERRORS
2008 2010 2012 2014 2016 National 6-24 Beds
Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

Conclusion
bull Reporting of ADRs is vital for patient safety
ndash Work to minimize preventable ADRs
bull Successful program can help identify problems and lead to positive change
References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf

References
bull Lancet 2000 Oct 7356(9237)1255-9 Adverse drug reactions definitions diagnosis and management Edwards IR1 Aronson JK
bull Adverse Drug Reactions by Joan B Tarloff PhD httpwwwmerckmanualscomprofessionalclinical-pharmacologyadverse-drug-reactionsadverse-drug-reactions
bull ASHP Guidelines on Adverse Drug Reaction Monitoring and Reportingbull httppharmacistslettertherapeuticresearchcomcececourseaspxpc=13-219 The Ins and Outs
of Adverse Event Recognition and ReportingVolume 2013 Course No 219bull Using Clinical Pharmacy Support Technicians to Optimize Pharmaceutical Care in the Intensive
Care Unit Can J Hosp Pharm 2010 Jan-Feb 63(1) 41ndash45bull Transitions of Care Pharmacy Technicians Role in Helping to Reduce Readmissionsbull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training Rachel Lutz
Published Online Thursday November 6 2014 See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull Pharmacists Underreport Adverse Drug Reactions Due to Inadequate Training - See more at httpwwwpharmacytimescomnewsPharmacists-Underreport-Adverse-Drug-Reactions-Due-to-Inadequate-TrainingsthashD6A2lZv1dpuf
bull httpswwwaccessdatafdagovscriptsmedwatchindexcfmaction=reportinghomebull httpwwwvagovmsprofessionalsmedicationsadverse_drug_reaction_faqpdf