-
8/13/2019 Pa to Log i of Central Nervous St Stem
1/20
Disorders of the central nervoussystem
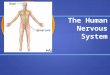
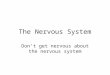
Common pathological featuresIntracranial herniationIntracranial
herniation is the movement of part of the
brain from one space to another with resultant damage.It usually
occurs following a critical increase in
intracranial pressure caused by an expanding lesion,e.g. tumour
or haematoma. However, it may be
inadvertently precipitated by withdrawing
cerebrospinal fluid (CSF) at lumbar puncture.Fig. 5.1 shows a
diagrammatical representation of
the sites of intracranial herniation.
Cerebral oedemaThis is an abnormal accumulation of fluid in
the
cerebral parenchyma. It is usually the result ofbreakdown of the
bloodbrain barrier, and it may
occur following damage initiated by several different
causes: Ischaemia, e.g. from infarction. Trauma, e.g. from head
injury.
Inflammation encephalitis or meningitis.
Cerebral tumours (primary or secondary). Metabolic disturbances,
e.g. hyponatraemia or
hypoglycaemia.
The condition results in cerebral swelling, and it is
associated with raised intracranial pressure.Treatment is by
minimizing the formation of
oedema by use of osmotic agents or steroids.
HydrocephalusHydrocephalus is an increase in the volume of
CSF
within the brain resulting in the expansion of thecerebral
ventricles. It can occur by one of threemechanisms:
Obstruction to flow of CSF (commonest form). Impaired absorption
of CSF at arachnoid villi
(rare). Overproduction of CSF by choroid plexus
neoplasms (very rare).
Obstructive hydrocephalus is either congenital or
acquired.
Congenital hydrocephalusThis occurs in 1 per 1000 births. The
principal causes
are congenital malformations, for example:
41
5. Pathology of the NervousSystem
falx cerebri
midbrain
ponscerebellum
medulla
dura
skull
tentoriumcerebelli
herniation of cingulate gyrusbeneath falx cerebri
collapse ofventricle
herniation of medialpart of temporal lobeover
tentoriumcerebelli
herniation of lower partof cerebellum throughforamen magnum
expandinglesion
herniation ofswollen brainthrough any
defect in duraand skull
C
B
DA
A
B
C
D
lateralventricle
Fig. 5.1 Sites of intracranialherniation. (A) Herniation of
thecingulate gyrus beneath the falxcerebri. (B) Herniation of
themedial part of the temporal lobeover the tentorium cerebelli.(C)
Herniation of the lower part of
the cerebellum through the foramenmagnum. (D) Herniation of
swollenbrain through any defect in thedura and skull.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
2/20
Pathology of the Nervous System
42
ArnoldChiari malformation (see p. 43). Congenital stenosis of
the cerebral aqueduct. Atresia of the foramina of Magendie and
Luschka
(DandyWalker syndrome). Some genetic causes associated with
X-linked
inheritance.
Acquired hydrocephalus
This may result from any lesion that obstructs theCSF pathway
such as: Tumoursespecially if located in the posterior
fossa, as the fourth ventricle aqueducts are
easilyobstructed.
Scarringpostinflammatory fibrosis of themeninges at exit
foramina, following meningitis orsubarachnoid haemorrhage.
Haemorrhageintraventricular or in the posteriorfossa.
Diagnosis
Severe forms of congenital hydrocephalus may bediagnosed
antenatally via ultrasound. Less severe
forms may present with considerably enlarged headsat birth.
In acquired hydrocephalus, enlargement of the headis prevented
by the inability of the skull to expand, butthis leads to massive
dilatation of the ventriclesresulting in increased intracranial
pressure.
Associated features are dementia with gaitdisturbances and
incontinence.
Treatment and management
A ventricular shunt with one-way valve system can
be inserted to drain CSF into the peritoneum.
Prognosis
Untreated patients may suffer irreversible braindamage, and the
condition is often fatal.
Special types of hydrocephalusSecondary or compensatory
hydrocephalus
Here, an increase in CSF occurs as a compensatorymeasure
following loss of brain tissue, e.g. due toinfarction or atrophy.
There is no associated increase
in CSF pressure.
Normal pressure hydrocephalus (intermittent
pressure hydrocephalus)
This is a rare condition of progressive dementiaassociated with
ventricular dilatation. Randomsampling shows normal CSF pressure,
butcontinuous monitoring reveals intermittentincreases.
Malformations, developmental
disease, and perinatal injuryNeural tube defects and posterior
fossaabnormalitiesThe aetiology of central nervous system
(CNS)malformations includes genetic factors, maternalinfections,
toxicity, metabolic factors, and irradiation
in utero. Neural tube defects are the commonestcongenital
abnormalities of the CNS, and they arecaused by defective closure
of the midline structuresover the neural tube. Screening for neural
tubedefects can be performed with ultrasound or bymeasurement of
-fetoprotein in the maternal serumor amniotic fluid. This is raised
in 90% of cases.Posterior fossa abnormalities are the second
mostcommon development abnormality of the CNS. Fig.5.2 illustrates
the types of congenital abnormalities.
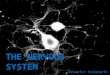
Syringomyelia and hydromyeliaSyringomyelia is a rare condition
in which a cyst(syrinx) develops within the spinal cord,
usuallyposterior to the central canal (Fig. 5.3). The cavity is
lined by gliosis (astrocytes). It is most common in thecervical
spinal cord, but it may extend into themedulla (syringobulbia).
Hydromyelia is the term used to denote cases inwhich the
dilatated central canal contains CSF, and islined by ependyma.
The causes of these conditions are either: Acquired (majority of
cases)secondary to
trauma or ischaemia, or occurring in associationwith tumours of
the spinal cord.
Congenitalmay be associated withmaldevelopment of the cord or
otherdevelopmental abnormalities of thecraniocervical junction,
especially inArnoldChiari syndrome.
Obstructive hydrocephalus isby far the most commonform of
hydrocephalus. Itis commonly subdivided
into: Non-communicating hydro-
cephalusobstruction within theventricular system leading
toblockage of CSF flow from theventricles to the subarachnoid
space.
Communicating hydrocephalusextraventricular obstruction
withinsubarachnoid space.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
3/20
Disorders of the Central Nervous System
43
The clinical manifestations are muscle weakness
and atrophy in the upper limbs due to compressionof the anterior
horn cells. There is loss of the
sensations of pain and temperature, butpreservation of those of
position and vibration, due
to damage to nerve fibres crossing the cord in the
lateral spinothalamic tracts.Surgery may arrest or alleviate
symptoms by
decompression or by draining the fluid in the cystic
cavity.
Perinatal injuryCerebral palsyCerebral palsy describes brain
malformation ordamage affecting motor areas of the brain. It is
the
leading cause of crippling handicap in children,affecting 2 per
1000 live births. Damage may occur
during fetal life, may be birth related, or may occur
postnatally (Fig. 5.4).The different types of cerebral palsy are
outlined
in Fig. 5.5.
Fig. 5.2 Types of congenitalabnormality.
Condition
Neural tube defects with cranial involvement
Anencephaly
Encephalocoele
Neural tube defects with spinal involvement
Spina bifida occulta
Spina bifida cystica
Posterior fossa abnormalities
ArnoldChiari malformation
DandyWalker malformation
Types of congenital abnormality
Features
Absence of the cranial vault and failure in the development
ofthe cerebral hemispheres
Ossification defects in the bones of the skull results
inherniation of the brain and meninges. Most common form
isoccipital
Abnormal development of the vertebral arches but the cordand
meninges are normal. Usually asymptomatic
Presents as either meningomyelocoele (90% of cases)
ormeningocoele (10% of cases). Abnormal development of the
vertebral arches results in cystic outpouching
Prolongation of the cerebellum downwards through theforamen
magnum often resulting in obstructivehydrocephalus
Obstruction of the foramina of Luschka and Magendie (exit ofthe
fourth ventricle) results in the formation of a cyst-likestructure
between the cerebellar hemispheres
early late
A B
Fig. 5.3 Syringomyelia. (A) Early effects: damage to the
decussating sensory fibres, with loss of temperature andtouch in
local segments. (B) Late effects: destruction ofgrey matter and
gradual affection of long tracts with lossof local reflexes, severe
sensory loss, and spastic paralysis.
Cerebral malformationCerebrovascular
accidentHypoglycaemiaHypoxiaInfectionKernicterus (bilirubin-induced
brain damage)PoisoningToxinsTrauma (peri- and postnatal)
Causes of cerebral palsy
Fig. 5.4 Types of cerebral palsy and their
associatedcharacteristics.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
4/20
Ischaemia and hypoxia
Ischaemia and hypoxia are major causes of severeperinatal brain
damage. Perinatal hypoxia is usuallydue to asphyxiation associated
with the trauma ofbirth, whereas perinatal ischaemia is
commonlycaused by intracranial haemorrhages.
Premature infants are highly susceptible todeveloping
intracranial haemorrhages because ofdisturbances in the cerebral
circulation possiblycaused by in-utero hypoxia/ischaemia.
In full-term infants, intracranial haemorrhageswith the
formation of small haematomas mayoccur during difficult deliveries,
although this isless common now because of improved
obstetriccare.
Mortality is high; one third of survivors maydevelop cerebral
palsy, epilepsy, or mentalretardation.
Traumatic injuries to the central
nervous systemSkull fracturesSkull fractures occur in
approximately 80% of fatalcases of head injuries. The most common
are linearfractures of the vault of the skull (62%); suchfractures
may extend into the base of the skullcausing cranial nerve
laceration.
The other types of skull fracture are: Penetratingincreased risk
of infection due to
tearing of the dura. Compoundincreased risk of infection due
to laceration of the scalp and tearing of the dura.
Depressedincreased incidence of epilepsy. Comminuted
(fragmented)increased incidence
of massive brain damage.
Parenchymal damageConcussion
This is an abrupt transient loss of consciousness dueto temporal
neuronal dysfunction following arelatively slight impact. It is
caused by an enormous,
but short-lived, increase in pressure within thecranium at time
of impact. Full recovery usuallyensues, although repeated
concussion may result inpermanent brain damage.
Contusions and lacerations
A contusion is a bruise with extravasation of bloodbut with the
pia-arachnoid intact. A laceration iswhere the pia-arachnoid is
torn.
Both are focal types of brain damage occurring at themoment of
injury, caused by striking the brain against
adjacent bone. They are most common at the frontaland occipital
poles and mainly affect the crests of gyri.Both lesions are
characteristically haemorrhagic.
Types of contusion: Fracture contusionoccurs at the site of
fracture. Coup contusionoccurs at point of impact in
absence of fracture. Contrecoup contusionoccurs
diametrically
opposite to the site of impact. Herniation contusionoccurs when
the
hippocampi or cerebellar tonsils (or both)
are impacted and bruised by the free edge of thetentorium and
foramen magnum, respectively.
Gliding contusionoccurs at the superior marginsof the cerebral
hemispheres; usually caused byinterference of the dura with a
rotationalmovement of the brain.
Diffuse axonal injury
The condition is produced as a result of rotationalmovements of
the brain within the skull during angularacceleration or
deceleration. It often occurs in the
absence of any skull fracture or cerebral contusions.There are
two main features:
Small haemorrhagic lesions in the corpus callosumand the
dorso-lateral quadrant of brainstem(macroscopic).
Widespread tearing of axons (microscopic).
This type of injury occurs in almost 50% of patientswith a
severe head injury, and in almost all fatal headinjuries. It is
associated with head injuries involvingvehicular accidents.
Traumatic vascular injuryBleeding from craniocerebral trauma is
oftenassociated with high mortality, and it may take place
Pathology of the Nervous System
44
Type
Spastic cerebral palsy (70%)
Dystonic (athetoid) cerebralpalsy (10%)
Ataxic cerebral palsy (10%)
Mixed cerebral palsy (10%)
Types of cerebral palsy and their associated characteristics
Characteristics
Hypertonia, ankle clonus and
extensor plantar response
Irregular, involuntary musclemovements
Hypotonia, weakness,uncoordinated movementsand intention
tremor
Fig. 5.5 Causes of cerebral palsy.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
5/20
in one or more of the potential spaces surrounding
the brain, e.g. extradural and subdural.
Extradural (epidural) haemorrhageThis type occurs in 2% of all
head injuries and in 15%
of fatal cases. Haemorrhage occurs between the skulland dura,
and gradually stripping dura from boneforming a large,
saucer-shaped haematoma (Fig. 5.6).
This injury is almost always the result of skullfracture,
usually a linear fracture of the thin
squamous part of the temporal bone, which contains
the middle meningeal artery (a branch of themaxillary
artery).
It is associated with a post-traumatic lucid intervalof several
hours followed by a rapid increase in
intracranial pressure.
Subdural haemorrhageHaemorrhage occurs between the dura and the
outersurface of the arachnoid membrane. It is usually
caused by a rupture of the small bridging veins or thevenous
sinuses. The resulting haematoma is often
extensive because of the loose attachment of the
dura and arachnoid membranes.Subdural haemorrhage may be acute
or chronic.
Acute subdural haemorrhage is associated with: Severe head
injury, subarachnoid haemorrhage,
and cerebral contusions. A rapid increase in intracranial
pressure.
Chronic subdural haemorrhage has the following
characteristics: More common in the very young and elderly.
Usually occurs as a result of minimal trauma, oras a result of
cerebral atrophy (in the elderly),
which causes a gradual widening of thesubdural space leading to
rupture of the bridging
veins. Blood typically accumulates slowly over a period
of days or weeks.
Presents with personality change, memory loss,and confusion.
Subarachnoid haemorrhageArterial rupture is usually secondary to
superficial
contusions or lacerations of the brain. Small amounts
of blood can be disposed of by arachnoid granulations.Larger
haemorrhages cause arachnoid fibrosis leading
to meningeal irritation and raised intracranial pressure.It can
also occur as a result of hypertension, aneurysms,
embolisms, or infarction.
Intracerebral haemorrhageThis is caused by direct rupture of the
intrinsiccerebral vessels at the time of injury.
Resulting haematomas are classified into three
types:
Solitaryoccur in association with corticalcontusions; common in
temporal and frontalpoles.
Multipleassociated with severe contrecouplesions; often
fatal.
Burst lobeintracerebral or intracerebellarhaematoma in
continuity with subdural
haematoma; most common in temporal andfrontal lobes; rapidly
fatal.
Spinal cord injuries
Most spinal injuries occur in males aged under 40years. Road
traffic accidents account for more than80% of such injuries.
There are two types of spinal cord injuriesopenand closed.
Open injuries
These are rare, and they are a result of direct traumato the
spinal cord and nerve roots. They can be either
perforating (i.e. with extensive disruption andhaemorrhage) or
penetrating (i.e. with incomplete
cord transectionBrownSquards syndrome).
Closed injuriesThese are in the majority, and they are
associated
with fracture or dislocation of the spinal column
Disorders of the Central Nervous System
45
scalp
skulldura
arachnoid
CSF
pia
brain
skullfracture middle
meningealartery
extradural
haematoma
Fig. 5.6 Extradural haemorrhage. (Redrawn with permissionfrom
Pathology by A Stevens and J Lowe, Mosby.)
-
8/13/2019 Pa to Log i of Central Nervous St Stem
6/20
causing compression of the cord by distortion of thespinal
canal.
Primary damage: Contusions. Nerve fibre transection.
Haemorrhagic necrosis.
Secondary damage: Extradural haematoma. Infarction. Infection.
Oedema.
The consequences depend mainly on the site andseverity of the
lesion. Cervical lesions result intetraplegia; lower thoracic
lesions result inparaplegia.
Cerebrovascular diseaseCerebrovascular disease is the third
leading cause ofdeath in the UK.
Stroke is a common outcome of cerebrovasculardisease, and it is
defined as a sudden event in which aneurological deficit occurs
over minutes or hours andlasts for longer than 24 hours.
If CNS disturbance lasts for less than 24 hours,
then the condition is termed a transient ischaemicattack.
The incidence is 1 or 2 per 1000 per year, but it ismuch higher
in the elderly, affecting males more thanfemales.
Causes of stroke are: Cerebral infarction (80%). Intracerebral
haemorrhage (10%). Subarachnoid haemorrhage (10%).
Pathological effects occur because of extensive
hypoxic neuronal damage. The area of brainaffected can be
readily localized since the bloodsupply of the brain has a fairly
constant anatomicdistribution. Fig. 5.7 shows the territories of
themajor arteries.
Pathology of the Nervous System
46
anterior cerebral artery
internal carotid artery
posterior communicating artery
superior cerebellar artery
vertebral artery
basilar artery
A B C
posterior cerebral artery
deep branches
superficial branches
middle cerebral artery
anterior communicating artery
key
anterior cerebral arterymiddle cerebral arteryposterior cerebral
artery
1
2
Fig. 5.7 Territories of the majorarteries. (1) Main cerebral
arteriesforming circle of Willis. (2) Their ter-ritories: (A)
Lateral view. (B) Inferiorview. (C) Medial view. (Reproducedwith
permission from AndersonsPathology, Damjanou, ed., Mosby.)
-
8/13/2019 Pa to Log i of Central Nervous St Stem
7/20
Disorders of the Central Nervous System
47
Clinical features of stroke depend on localization
and the nature of the lesion. Risk factors areatheroma, heart
disease, hypertension, and diabetes
mellitus.
Hypoxia, ischaemia and infarctionCerebral infarction is the
process whereby a focal
area of necrosis is produced in the brain in response
to a decreased supply of oxygen (and glucose) in theterritory of
a cerebral arterial branch.
There are two main causes of infarction: Hypoxiathe reduction of
oxygen supply to
tissues despite an adequate blood supply, e.g.following
respiratory arrest.
Ischaemiablood supply to tissues is absent, orseverely reduced,
usually as a result of
constriction or obstruction of a blood vessel.
Ischaemia accounts for the majority of cases ofcerebral
infarction.
Mechanisms of ischaemiaIschaemia may be caused by: Vascular
diseasee.g. thrombosis, embolic
occlusion or vasculitis. Cardiac diseasee.g. prolonged
hypotension or
cardiac embolism. Traumahead injury leading to vascular
occlusion, dissection, or rupture.
Infarcted tissue becomes swollen and soft with
the loss of definition between grey and white matter.The
infarcted tissue undergoes colliquative necrosis
and shows microglial macrophage infiltration.Eventually, the
necrotic tissue is completely
phagocytosed to leave a fluid-filled cystic cavity witha gliotic
wall. Fig. 5.8 shows the macroscopic and
microscopic pathological features of cerebral
infarction.Strokes caused by cerebral infarction clinically
present with slowly evolving signs and symptoms.
Atraumatic haemorrhageIntracerebral haemorrhageThe majority of
intracerebral haemorrhages are
thought to arise from CharcotBouchardmicroaneurysms associated
with hypertension and
diabetic vascular disease. These haemorrhages occurmost
frequently in the basal ganglia (80%),
brainstem, cerebellum, and cerebral cortex.The resulting
haematoma acts as a space-
occupying lesion leading to increased intracranialpressure and
herniation. The clinical picture is
often indistinguishable from a cerebral infarction,but the
raised intracranial pressure commonly
gives rise to sudden headache, vomiting, andimpairment of
consciousness. Mortality is about
80%.
Subarachnoid haemorrhageThis can occur at any age, but it is an
important cause
of death and disability in the 2040 year age group.The majority
of subarachnoid haemorrhages are
caused by saccular berry aneurysms, which develop
at proximal branch points in the major cerebralvessels on the
circle of Willis (Fig. 5.9).
These aneurysms occur in 12% of the population,but they are more
common in the elderly and
hypertensives.The clinical picture is one of sudden onset of
severe headache accompanied by neck pain/stiffnessand vomiting.
Only 3040% survive for a few hours;
among those who survive longer, there is a 30%mortality rate
within the first month.
Time
Before 24 h
After 24 h
After a few days
After weeks/months
Macroscopic
No naked eye abnormalities
Softening and swelling (oedema) of affected tissue
Necrotic tissue
Fluid-filled cystic cavity with gliotic wall
Pathological features of cerebral infarction
Microscopic
Some neuronal damage
Line of demarcation between normal and abnormal myelinin white
matter
Infiltrating macrophagesProliferating astrocytes and
capillaries
Necrotic tissue removedThickened capillary wallsOnly astrocytes
remain
Fig. 5.8 Pathological features of cerebral infarction.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
8/20
Hypertensive cerebrovascular diseaseSystemic hypertension can
affect the CNS resultingin neurological dysfunction, thus:
Atheroma of the larger cerebral vessels leads to aloss of
autoregulation of cerebral blood flow.
Aneurysms, both saccular and microaneurysms,may cause
spontaneous intracerebralhaemorrhage.
Encephalopathypathogenesis is uncertain butdamage to the
bloodbrain barrier leads to forcedcerebral hyperperfusion.
Infections of the central nervoussystemBacterial
meningitisMeningitis refers to inflammation of the meninges.There
are two classes: leptomeningitis withinflammation centred on the
subarachnoid space,and pachymeningitis with inflammation centred
onthe dura.
Acute pyogenic (bacterial) meningitisThis is infection of the
leptomeningespia andarachnoid materand the CSF, which
diffuselyaffects the whole meninges and subarachnoid
space.Organisms that typically cause this condition vary
between age groups (Fig. 5.10).The clinical features are
headache, drowsiness,
vomiting, fever, petechial rash, and neck stiffness.The
complications are:
Ventriculitis. Intracerebral abscess (see below). Cerebral
infarction. Subdural empyema. Epilepsy. Disseminated intravascular
coagulation (DIC). Adrenal haemorrhage.
Diagnosis and managementThe CSF is cloudy dueto increased
numbers of neutrophils (>1000cells/mm3). CSF protein levels
increase and glucoseconcentrations fall. Treatment is with
vigorousantibiotic therapy.
Pathology of the Nervous System
48
90% of total
10% of total
middlecerebral
artery
posteriorcerebral
artery
anteriorcerebral
artery
basilarartery
30% occurhere
30%occur here
10% occurhere
30% occurhere
Fig. 5.9 Berry aneurysmsapproximate frequency anddistribution.
The dotted line separates anterior fromposterior circulation.
(Redrawn with permission fromAndersons Pathology, Damjanou, ed.,
Mosby.)
There are four possiblemechanisms of meningealinfection: Direct
spreadfrom
penetrating trauma (e.g.compound skull fractures) oradjacent
focus of infection(e.g. sinusitis, middle ear ormastoid
infection).
Blood-borne spreadfromsepticaemia or septic emboli fromother
infections such as bacterialendocarditis.
Iatrogenic infectionfollowing the
introduction of organisms into CSFat lumbar puncture. Congenital
abnormalities, e.g.
meningomyelocoeles.
Neonates
Escherichia coliGroup B StreptococcusListeria monocytogenes
Infants
Neisseria meningitidisHaemophilus influenzae
Streptococcus pneumoniae
Meningitis-causing bacteria
Young adults
N. meningitidisS. pneumoniae
Elderly
S. pneumoniaeN. meningitidisL. monocytogenes
Fig. 5.10 Meningitis-causingbacteria.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
9/20
Disorders of the Central Nervous System
49
PrognosisMortality ranges from 3% for
Haemophilus influenzae to 60% for Streptococcuspneumoniae, and
it is highest in the very young and
the elderly.
Aseptic (viral) meningitisThis is the commonest cause of
meningitis. It is abenign and self-limiting illness, usually less
severe than
bacterial meningitis. It may occur as a complication ofviral
infection, e.g. mumps or measles.
Common causative organisms
The common causative organisms are enteroviruses(e.g.
echoviruses, coxsackie viruses, and polioviruses)
and mumps virus.The illness clinically presents with acute onset
of
headache, irritability, and rapid development ofmeningeal
irritation.
Diagnosis and managementThe CSF is clear andcolourless. It
contains excess lymphocytes but
normal glucose and protein. Treatment involves
control of symptoms only.PrognosisComplete recovery usually
occurs
without specific therapy.
Brain abscessA brain abscess is a severe focal infection of the
brain
and is typically 12 cm across. It starts as an area
ofcerebritisinflammation of the brain parenchyma
and develops into a pus-filled cavity walled off by
gliosis and surrounded by cerebral oedema. It oftenresults in
raised intracranial pressure.
The aetiology of brain abscesses is as follows: Middle ear
infection (60%)temporal lobe and
cerebellar abscesses. Frontal sinusitis (20%)frontal lobe
abscess.
Bacteraemia/septicaemia (10%)usually frontallobe abscess.
Penetrating skull trauma. Secondary to meningitis.
Unknown causes.
Common causative organisms are Streptococcus
vividans, Staphylococcus aureus, andKlebsiella, butit may also
be caused by fungal infection.
The clinical presentation is similar to that of acute
bacterial meningitis but focal neurological signs,epilepsy, and
fever are common manifestations.
Complications include: Meningitis.
Intracranial herniation. Focal neurological deficit.
Epilepsy.
Treatment is with antibiotic therapy at an early
stage, with surgical aspiration or excision of thecapsule.
PrognosisOverall mortality is about 10%.
Subdural empyemaThis is a collection of pus in the subdural
space and itis relatively uncommon. In adults it usually
results
from frontal sinusitis, whereas in infants it is
usuallysecondary to meningitis.
Clinically, patients with subdural empyema areusually very ill.
The pus spreads rapidly on the
surface of a hemisphere, producing hemiparesis,
raised intracranial pressure, fits, and meningism.
Chronic meningoencephalitisTuberculous meningitis
This is meningitis due to infection byMycobacteriumtuberculosis.
It is rare in the UK but a major problem
in developing countries.The disorder is almost always secondary
to
tuberculosis elsewhere in the body; infection usuallyreaches the
CNS via the bloodstream.
PathogenesisGranulomatous inflammationaffects the basal
meninges, large arteries and cranial
nerves.
It presents clinically with slow-onset, subacutemeningitis. It
may be accompanied by isolated cranial
nerve palsies.Hydrocephalus may result from impaired
reabsorption of CSF or obstruction of CSF outflowfrom the fourth
ventricle.
CSF shows an initial increase in polymorphs, thenan increase in
lymphocytes.
PrognosisUntreated, the disease is usually fatal.Intensive
treatment with antituberculous drugs
lowers mortality to 1520%.Chronic meningitisThis is a rare
condition, which usually occurs in the
middle-aged and elderly.Neisseria meningitidis isthe most common
cause. The patient can be unwell
for weeks or even months with recurrent fever,sweating, joint
pains, and transient rash.
NeurosyphilisThis is caused by invasion of the CNS by
Treponema
pallidum weeks, months, or years after initialinfection.
Meningitic illness occurs in only
approximately 25% of cases of syphilis. It is usuallymild or
even asymptomatic, but it may be severe
with transient cranial nerve palsies and convulsions.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
10/20
Lyme disease
This disorder is caused by the tick-borne spirochaete
Borrelia burgdorferi. It is a systemic illnesscharacterized by
skin lesions and neurological features.
Viral encephalitisThis is a virally induced diffuse inflammation
ofthe brain, which is usually concomitant withinflammation of the
meninges. It is a commoncomplication of many viral illnesses.
Commoncausative viruses are: Arboviruses. Herpes simplex virus I
and II. Measles. Cytomegalovirus. Polio and enterovirus. Rabies.
Human immunodeficiency virus (HIV).
Most cases are mild and self-limiting. However, somecases (e.g.
those involving herpes simplex virus type Iand rabies) result in
extensive tissue destruction andmay be fatal.
Mortality for the more severe type is 50%, and themajority of
survivors have severe, permanent braindamage.
Fungal infectionsThese are relatively rare and occur mainly in
theimmunosuppressed (e.g. associated withchemotherapy, steroid
treatment, acquired immunedeficiency syndromeAIDS), but some
organisms,e.g. Cryptococcus neoformans, can produce disease inthe
absence of immunosuppression.
The spread can be haematogenous (e.g. fromthe lungs, which is
the most common) or direct
(e.g. from the nose and paranasal sinuses, which
israre).Causative organisms are:
Cryptococcus neoformansfungal meningitis. Aspergillus
fumigatusfungal abscesses usually
accompanied by pulmonary infection. Candida albicansfungal
abscesses. Phycomycosisthrombosis and associated
infarction; commonly affects uncontrolleddiabetics.
Protozoal infectionToxoplasmosis
This is caused by infection with Toxoplasmagondii. It may be
acquired by eating poorly-
cooked infected meat or food contaminated withfeline faeces. It
has two forms: congenital andacquired.
The incidence of congenital toxoplasmosis showsgeographical
variation, e.g. 1 per 4000 births in the
US; 1 per 100 births in France. The organism istransmitted to
the fetus through the placenta duringmaternal infection.
The infection can cause: Abortion or stillbirth. Severe brain
damage leading to early death. Moderate brain damage and
chorioretinitis;
compatible with life but with permanentdisability.
Acquired toxoplasmosis is the commonestopportunistic infection
of the CNS in adults withAIDS. It results in: Necrotizing
cerebritis. Chronic abscesses. Meningoencephalitis.
However, in healthy subjects, it rarely causescerebral
symptoms.
Other protozoan organisms that may causeinfection of the CNS
are:
Amoebae. Plasmodium falciparum. Trypanosomes.
Progressive multifocal leucoencephalopathyMultifocal destruction
of oligodendrocytes results indemyelination with minimal
inflammation andminimal damage to axons. It is caused by the DNAJC
papovavirus, and it occurs in association withunderlying diseases
such as AIDS, chroniclymphocytic leukaemia, carcinoma, and
systemic
lupus erythematosus.Patients present with progressive dementia.
The
disease is progressive and death usually occurs withina few
months.
Subacute sclerosing panencephalopathyThis subacute encephalitis
occurring in children isdue to persistent measles infection. It
presents withprogressive neurological dementia, and death
usuallyoccurs within two years of onset.
Spongiform encephalitis (CreutzfeldtJakobdisease)This is rapidly
progressive dementia, ataxia, andmyoclonus, and it is rare in the
UK (at 1 per 1 000 000
Pathology of the Nervous System
50
-
8/13/2019 Pa to Log i of Central Nervous St Stem
11/20
Disorders of the Central Nervous System
51
per year). The infectious agent is not precisely
known, but it is most likely to be non-nucleic acidtransmission
by prion (or proteinaceous infectious
agent) protein (see page 33). The condition has anincubation
period of up to 30 years but it is always
fatal, usually within 6 months.A recently described variant
appears to be the
human manifestation of bovine spongiform
encephalopathy.
Demyelination and degenerationDemyelinating diseasesThis group
of diseases has a common factor ofprimary damage to myelin of
nerves while the axons
and nerve cells remain relatively intact.
Multiple sclerosisMultiple sclerosis (MS) is the commonest
demyelinating disorder of the CNS affecting 50 per100 000 in the
UK. Peak incidence is between 20
and 40 years with a slight female predominance.MS is
characterized by relapsing and remitting
episodes of immunologically mediateddemyelination within the
CNS. Recovery from each
episode of demyelination is usually incomplete,leading to
progressive deterioration. There is an
association between the disease and certain HLA
antigens (A3, B7, DR2 & DQ1). However theaetiology is
unknown but current theories are: Myelin abnormality. Autoimmune
disorder.
Toxin damage. Viral infection of the CNS, e.g. measles.
PathogenesisAcute demyelination occurs in the
central white matter in discrete areas known asplaques.
Abnormalities are confined to the CNS; the
peripheral nervous system (PNS) is usually spared.Common sites
are the optic nerve, brainstem,
cerebellum, periventricular regions, and cervical
spinal cord.Fig. 5.11 gives a list of the clinical
manifestations
of MS and their causes.Diagnosis and managementClinical
evaluation
and computed tomography (CT) and magneticresonance imaging (MRI)
scans can show areas ofdemyelination within the brain. CSF
examination
shows increased lymphoid cells and oligoclonalbands of IgG.
There is no specific treatment
but corticosteroids may accelerate remission inrelapse.
Beta-interferon has also been used to some
success.The diseases progress is variable. In about 5% of
patients, the disease is rapidly progressive and fatalwithin 5
years. However, others may survive for
more than 20 years with only minor disability.
Degenerative disordersCorticalAlzheimers disease
This is the most common cause of dementia inWestern countries.
In the UK it affects 5% of
people over 65 years, and 15% of people over 80years; females
more than males. Also of significance
is the subgroup of early onset patients (4060years). Genetic
studies have shown that there is an
increase in incidence of sporadic cases in individualswith
ApoEe4 genotype on chromosome 19. The
amyloid precursor protein (APP) gene onchromosome 21 has been
implicated in the familial
cases.However, the aetiology and pathogenesis are
unknown; some cases (5%) are familial but most
(95%) are sporadic. Current theories involve: Infectious
agents.
Toxins, e.g. aluminium. Traumatic injury.
Manifestations
Early clinical symptoms. blurring of vision. incoordination.
abnormal sensation
Late stages. blindness, paraplegia and incontinence. ataxia.
intellectual dysfunction
Clinical manifestations of MS and their causes
Causes
Optic nerve diseaseCerebellar peduncle diseaseDisease of long
ascending sensory tracts
Spinal tract involvementSpinal and cerebellar involvementLoss of
hemispheric white matter
Fig. 5.11 Clinical manifestations ofmultiple sclerosis (MS) and
theircauses.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
12/20
-
8/13/2019 Pa to Log i of Central Nervous St Stem
13/20
Disorders of the Central Nervous System
53
Metabolic disorders and toxinsVitamin deficienciesVitamin B1
(thiamine) deficiencyThis is common in chronic alcoholics,
resulting in:
Wernickes encephalopathy: memory impairment,
ataxia, visual disturbances, and peripheralneuropathy.
Korsakoff s psychosis: confused state, memory
loss, and confabulation.
If both occur, it is known as WernickeKorsakoff
syndrome.
Vitamin B12 (cyanocobalamin) deficiencyThis produces weakness
and paraesthesia in the
lower limbs resulting from subacute combined
degeneration of the spinal cord (Fig. 5.13).Replacement therapy
at an early stage reverses thedegenerative process, but
long-standing cases show
irreversible axonal damage with reactive gliosis.
Iodine deficiencySevere iodine deficiency causes hypothyroidism;
it is
the most important endocrine disorder to affect theCNS in
children. In the fetus, severe iodine deficiency
causes cretinism characterized by dwarfism, mentaldefect, and
spastic diplegia. This can be prevented by
iodine supplements during pregnancy.
ToxinsCarbon monoxideCarbon monoxide (CO) binds irreversibly
to
haemoglobin, rendering erythrocytes incapable ofoxygen
transport. CO poisoning, therefore, results in
brain damage due to hypoxia. This poisoning may beaccidental or
associated with attempted suicide.
The amount of carbon monoxide-boundhaemoglobin (HbCO) with
corresponding clinical
symptoms are as follows:
>20%Dyspnoea and slight headache.
30%Severe headache, fatigue, and impairedjudgement.
6070%Loss of consciousness. >70%Rapidly fatal.
PathogenesisHypoxia results in neuronal necrosis
with a predilection for globus pallidus. Other
selectively vulnerable regions are the hippocampus,and cerebral
and cerebellar cortices.
MethanolMethanol is highly toxic to the CNS. It is lipid
soluble, so it readily diffuses into the CSF andaqueous humour
in concentrations higher than in
plasma.
Methanol is metabolized into formic acid andformaldehyde. It is
the formaldehyde that is thoughtto be the mediator of toxic
effects. There are two
types of methanol poisoning: Acutesudden death with multiple
haemorrhagic
lesions in the cerebral hemispheres. Chronicatrophy of retinal
ganglion cells with
secondary degeneration of the optic nerve.
EthanolThe consequences of excessive ethanol intake on the
CNS are manifold (Fig. 5.14).
Neoplasms of the central nervoussystemGliomasGliomas are tumours
that arise from glial supportive
tissue of brain. They are the most common primarybrain tumours,
accounting for 50% of all CNS
tumours.
Astrocytoma
This is a glioma derived from astrocytes, and it ismore common
in children, usually occurring in thecerebellum. It accounts for
10% of all primary
tumours in adults, usually in the cerebralhemispheres.
Common types of astrocytomas and theircorresponding tumour
grading:
Benign juvenile pilocytic astrocytoma (grade I). Astrocytoma
(grade I/II).
Anaplastic astrocytoma (grade III).
Glioblastoma multiforme (grade IV).
Prognosis depends on the degree of tumourdifferentiation and the
size of the neoplasm. For
example:
Degeneration of:posterior columnsandcorticospinal tracts
Fig. 5.13 Subacute combined degeneration of the spinalcord.
Degeneration of posterior columns leads to sensoryloss (vibration
and proprioception) causing ataxia.Degeneration of corticospinal
tracts leads to upper motorneuron damage causing spastic
paralysis.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
14/20
Grade I: survival times of 2030 years are possible. Grade IV:
20% survive for 1 year.
Oligodendrogliomas
These ill-defined, slow-growing tumours arise
fromoligodendrocytes in the white matter of the
cerebralhemispheres, especially the temporal lobe. Theyaccount for
5% of all primary CNS neoplasms in
adults, but they are rare in children.The prognosis is
relatively good.
Ependymoma
These tumours arise from the ependymal cells liningthe ventricle
and central canal of the spinal cord.Ependymoma is the most common
tumour of the spinalcord, accounting for 5% of all primary CNS
neoplasms.It is common in children and young adults.
Medulloblastoma
This tumour of primitive neuroepithelial cells arisesin the
cerebellum in children, in whom it is the mostcommon CNS tumour. It
is malignant, with a rapidgrowth rate; obstruction of the fourth
ventricleresults in hydrocephalus.
Other tumoursPrimary brain lymphomas
Associated with immunosuppression, especiallyAIDS, most primary
brain lymphomas are highgrade, non-Hodgkins lymphomas of B cell
type with
a poor prognosis.
Germ cell tumours
These rare tumours are seen mainly in children;males more than
females. Most arise near the
pineal gland, and they behave as malignantteratomas.
Meningiomas
These account for approximately 15% of adultintracranial
tumours; females more than males.Tumours arise from the arachnoid
mater, and theyare usually benign but may invade adjacent bone
resulting in erosion and hyperosteosis. Meningiomasproduce
symptoms by compression of brain tissuerather than by invasion.
Metastatic tumours
The CNS is a common site for metastasis, andtumours are usually
multiple. They may arise fromhaematogenous or direct spread. The
cerebellum isthe preferred site but they can affect any part of
thebrain as well as other intracranial structures,especially
meninges (hence malignant meningitis).
Metastases often occur at the boundary betweengrey and white
matter.The most common neoplasms to metastasize to
the CNS are: Breast carcinomas. Bronchus carcinomas. Kidney
carcinomas. Colon carcinomas. Malignant melanoma.
Disorders of the peripheralnervous system
Disorders of peripheral nerves are termedneuropathies, and they
can be predominantly
Pathology of the Nervous System
54
Disease
Fetal alcohol syndrome
Acute intoxication
Cerebral and cerebellar atrophy
Nutritional disorders
Hepatocerebral syndromes
Demyelinating disorders
Features
Cerebral malformations
Facial and somatic malformationsGrowth retardation
Cerebral oedemaPetechial haemorrhages
Neuronal loss
Wernicke s encephalophathy
Hepatic encephalopathyChronic hepatocerebral degeneration
Central pontine myelinolysis
Consequences of excess ethanol intake on the central nervous
system
Mechanism
Direct toxicity
Direct toxicity
Direct toxicity
Deficiency of vitamin B1
Hepatic toxicity with secondary effects on CNS
Electrolyte disturbances
Fig. 5.14 Consequences of excess ethanol intake on the CNS.
(Adapted from Underwood, 2000.)
-
8/13/2019 Pa to Log i of Central Nervous St Stem
15/20
sensory, predominantly motor, or mixed depending
on which nerves are affected.
Hereditary neuropathiesHereditary motor and sensory
neuropathies
(HMSN)Peroneal muscular atrophy (HMSN I+II;CharcotMarieTooth
disease)This disorder is characterized by pronounced atrophyof the
calf muscles with associated sensory deficits as
a result of slowly progressive symmetric neuropathy.It is the
commonest of the hereditary neuropathies,
and it is usually autosomal dominant. It impedesambulation and
causes foot deformities (pes cavus),
but it does not shorten the lifespan.
Fig. 5.15 provides a table of the different types
of peroneal muscular atrophy and theircharacteristics.
DejerineSottas disease (HMSN III)This severe, chronically
progressive symmetric
peripheral neuropathy is caused by hypertrophy ofperipheral
nerves, followed by gradual axon
degeneration. There is delayed onset of motor skills(e.g. in
walking) and gradual progression to
wheelchair confinement in young adult life.
Hereditary sensory and autonomicneuropathies (HSAN)This group of
autosomal inherited diseases produce
mainly sensory and autonomic neuropathies. Thereare three major
types as described in Fig. 5.16.
Traumatic neuropathiesLacerationsLaceration refers to a jagged
tear of the peripheral
nerve in which there is partial or complete loss of
continuity of the nerve. It occurs most commonly
from a penetrating injury such as a knife wound, or a
misplaced intramuscular injection, or from bone
fractures.
AvulsionThis is the tearing of nerve fibres from the surface
of
the spinal cord or from a muscle. It may be partial orcomplete
depending on whether all or only some of
the rootlets contributing to the spinal nerve areinvolved.
Nerve roots may be avulsed from the spinal cord
in two ways: Tensile stresses from cervical plexus
transmitted
centrally can stretch and finally avulse the nerveroots.
A spinal cord injury, such that displacement of thecord acts
directly on the nerve roots between their
attachment to the cord and their entry into theintravertebral
foramen.
Both laceration and avulsion injuries cause the
severed ends of the damaged nerve to retract and
then to undergo Wallerian degeneration forming a
Disorders of the Peripheral Nervous System
55
Note that: Disorders affecting many
peripheral nerves are termedpolyneuropathies, and they
usually cause symmetricaldeficits.
Disorders affecting only one(mononeuropathy) or a few(multiple
mononeuropathies)peripheral nerves typically causeasymmetrical
deficits.
Radiculopathies are disorders ofnerve roots.
Type of neuropathy
Relative occurrence
Type of axonal loss
Nerve conduction velocity
Time of onset
Effects
HMSN I
Demyelinating neuropathy
75%
Large calibre axons
Impaired (45 m/s)
Later (second decade)
Weakness and wasting less marked
Fig. 5.15 Different types ofperoneal muscular atrophy and
theircharacteristics.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
16/20
Pathology of the Nervous System
56
traumatic neuroma. Subsequently, the proximalportion of the
nerve develops neuritic sprouts which,if sited in proximity to the
severed distal nerve, mayreinnervate by regrowth along the nerve
sheath.
If continuity of the nerve is completelyinterrupted, basal
laminae sheaths no longer formcontinuous tubes to guide
regeneration sprouts andso the potential for recovery is
limited.
Compression/entrapment neuropathyCompressed nerves undergo
segmental
demyelination with decreased nerve conductionvelocity. If
compression is prolonged or severe,axonal degeneration may occur.
Symptoms of nervecompression are paraesthesia, anaesthesia, and
loss ofmuscle strength.
Carpal tunnel syndrome
This is a disorder in which the size of the carpaltunnel is
significantly reduced causing compression
of the median nerve. Causes include inflammationof the flexor
retinaculum, arthritic changes, etc.
Saturday night palsy
Radial nerve compression (in the middle of the arm),which may
result from improper positioning of theupper limb during sleeping,
especially in intoxicatedpersons.
Inflammatory neuropathiesGuillainBarr syndrome (acute
inflammatorydemyelinating polyradiculopathy)
This is the commonest form of acute neuropathycaused by
immune-mediated demyelination ofperipheral nerves, usually
occurring 24 weeks afterviral illness.
Affected patients develop motor neuropathy withlesser sensory
changes due to widespreaddemyelination of the peripheral nerves.
Recovery(i.e. remyelination) occurs over 34 months and isusually
complete.
Infectious neuropathiesLeprosy (Hansens disease)A chronic
granulomatous disease caused by
Mycobacterium leprae. It is the most common causeof peripheral
neuritis worldwide, affecting about 10million patients in
total.
The clinicopathological features of leprosy aredependent on the
hosts response to infection, with aspectrum of disease ranging from
tuberculoid tolepromatous form (Fig. 5.17).
Varicella-zoster virus (VZV)An invasion of cutaneous sensory
nerves duringprimary infection with VZV (chickenpox) leads
toinfection of the dorsal root ganglia where the virusenters a
latent state. Reactivation of VZV may occur
Clinical syndrome
Eponym
Inheritance
Affected neurons
HSAN II
Congenital sensory neuropathy
Giacci s
Autosomal recessive
Degeneration of large andsmall myelinated fibres
Types of hereditary sensory and autonomic neuropathies
(HSANs)
HSAN I
Ulcerative acropathy due to numbness
Morvan s
Autosomal dominant
Degeneration of large myelinated fibresof both peripheral nerves
andposterior columns of spinal cord
HSAN III
Familial dysautonomia
RileyDay
Autosomal recessive
Degeneration of non-myelinated fibreswith preservation of
myelinated fibres
Loss of neurons of autonomic ganglia
Fig. 5.16 Types of hereditary sensory and autonomic
neuropathy.
Common sites of nervecompression are: Nerve roots in the
intervertebral foramina byprolapsed intervertebral discsor
osteophytes due toosteoarthritis of the spine.
Median nerve in carpal tunnel at thewrist.
Ulnar nerve in flexor carpal tunnelat medial epicondyle of
humerus.
Common peroneal nerve at theneck of the fibula.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
17/20
Disorders of the Peripheral Nervous System
57
years later causing shingles. The reason forreactivation is
unknown, but there is increased
incidence in the immunocompromised.In shingles, VZV migrates
down the nerves into
the skin and causes vesicular lesions identical to those
of chickenpox but confined to one or two adjacentdermatomes
usually on the trunk.
Metabolic and toxic neuropathiesPeripheral neuropathy of
diabetes mellitusThis occurs in both type I and II diabetes
mellituswith a prevalence of 1060% clinically, but up to
100% when evaluated by nerve conduction studies.
There is increased prevalence with increasedduration of the
disease.
PathogenesisVascular occlusion of the blood vessels supplying
the
nerves results in neuronal atrophy.There are four types:
Symmetrical and predominantly sensory
polyneuropathy. Autonomic neuropathy.
Proximal painful motor neuropathy. Cranial mononeuritis (mainly
CN III, IV
and VI).
Metabolic and nutritional causesUraemic neuropathy in renal
failureApproximately 60% of patients with chronic renalfailure have
symptoms of uraemic neuropathy at
onset of dialysis. It is expressed as pain andparaesthesia with
the lower extremities
preferentially involved. Dialysis usually improvessymptoms.
Thyroid dysfunctionMild chronic sensorimotor neuropathy is
sometimes
seen in both hypothyroidism (more commonly)
andhyperthyroidism.
Vitamin deficienciesVitamin deficiencies are important causes
of
peripheral neuropathies. Especially important aredeficiencies of
vitamins B1 (thiamine), B12, B6(pyridoxine), and E.
Toxic neuropathiesMany toxins cause damage to peripheral nerves.
Themost common toxins are: Drugsisoniazides, sulphonamides,
vinca
alkaloids, dapsone, and chloroquine. Alcoholin cases of chronic
abuse. Industrial toxinsacrylamide, hexane,
organophosphates, lead, arsenic, mercury.
Most toxins produce a dying back pattern of axonaldamage
resulting in a distal symmetric pattern of
sensorimotor involvement. There is a stockingglove distribution
at onset but continued exposure
to the toxin extends the deficit to the lower calvesand
forearms.
Immune mechanism
Spread of organisms
Distribution in nerves
Nerve enlargement and damage
Neurological deficit
Prognosis
Lepromatous
Minimal immune response (occurs in
patients with low cellular immunity)
Bacteraemia occurs in peripheral sites
Widely disseminated diffuse nerveinvolvement
Intense infiltration of nerves byvacuolated macrophages
Sensory and motor involvementPatchy loss of sensation
Progressive and lethal
Comparison of peripheral nerve damage by lepromatous and
tuberculoid forms of leprosy
Tuberculoid
Vigorous T cell mediated (delayed) hypersensitivity
Bacteraemia rare
One or a few sites (asymmetrical)
Hallmark of nerve involvement is discrete,
well-formedgranulomas
Sensory, motor and autonomic involvementPeripheral nerve
palsiesAnaesthetic areas prone to injury and secondary
infection
Progression slow, but immune response produces extensive
destruction of tissue resulting in severe
disfigurementEventually heals spontaneously
Fig. 5.17 Comparison of peripheral nerve damage by lepromatous
and tuberculoid forms of leprosy.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
18/20
-
8/13/2019 Pa to Log i of Central Nervous St Stem
19/20
Disorders of the Autonomic Nervous System
59
Beneficial effectsOf benefit is the reduction of acid and
pepsin
secretion by abolishing direct vagal drive (and
to a minor degree by reducing antral gastrin
secretion).
Harmful effectsImpairment of antral motility is caused by
abolishing
receptive relaxation in the gastric corpus, andreducing the
power of antral contractions.
The harmful effects of truncal vagotomy can nowbe largely
overcome by performing a selective
vagotomy instead, but this is less effective and it hasa higher
incidence of ulcer recurrence.
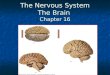
Fig. 5.18 Peripheral nervoussystem tumours.
superior
cervicalganglion
middlecervicalganglion
salivaryglands
eye
lungs
inferiorcervical
ganglion
olfactoryglands
Fig. 5.19 Sympathetic innervation to the eye and faceshowing the
relationship of the sympathetic trunk to theapex of the lungs.
Tumour
Schwannoma
Neurofibroma
Neurofibromatosis type I
Neurofibromatosis type II
Tuberous sclerosis
Von HippelLindau disease
Peripheral nervous system tumours
Features
Benign tumour of schwann cells of the nerve
sheaths. Most common site is the vestibular branch ofCN VIII
A tumour of the neural crest cells derived from theepineurium
and endoneurium
An autosomal dominant neurocutaneous syndrome.Characterized by
multiple neurofibromas
Autosomal dominant disorder affecting CN VIII
Autosomal dominant disease causing epilepsy andmental
retardation
Autosomal dominant disease characterized by
multiple haemangiomas
Truncal vagotomy means asection of the trunk of thevagus
nerve.
Selective vagotomy means
a vagotomy where onlythose vagal fibres that passto the body of
the stomachare divided, while thosesupplying the antrum,pylorus,
and otherabdominal viscera arespared.
-
8/13/2019 Pa to Log i of Central Nervous St Stem
20/20
Pathology of the Nervous System
Describe the common pathological features of the CNS. What are
the congenital malformations and developmental diseases of the CNS?
Give examples of types of traumatic injury that affect the CNS.
What is the pathogenesis of cerebrovascular disease? Name the
infections of the CNS. Describe CreutzfeldtJakob disease. Give
examples of diseases of demyelination and diseases of degeneration.
Name the vitamin deficiencies and toxins that damage the CNS. What
are the consequences of excess ethanol intake on the CNS? Name the
neoplasms of the CNS. Name the different types of hereditary
neuropathies. What are the causes and outcomes of traumatic
neuropathies? Outline the pathology of GuillainBarr syndrome
(inflammatory neuropathy). Name infections that can cause
neuropathies.
Give types of metabolic and toxic neuropathies. Name the
neoplasms of the peripheral nerves. What are the characteristics
and causes of Horners syndrome? Give indications for performing
sympathectomies and describe their effects. Describe the pathology
of phaeochromocytomas. What are the effects of vagotomies?