Embed Size (px)
Citation preview

Proceedings of the NASS 20th Annual Meeting / The Spine Journal 5 (2005) 1S–189S 115S
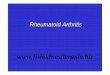
Fig. 1. 3D micro-CT reconstruction of vertebral body from Lrp5 null and WT mice.
STUDY DESIGN/SETTING: Skeletal genetic study using mutant mice.STUDY SAMPLE: The fifth lumbar vertebra (L5) was harvested fromeach mouse at 18 weeks of age.OUTCOME MEASURES: Lrp5 null mice were compared with age andgender-matched wild-type control (WT) mice.METHODS: In vivo BMD of the spine (L1-L5) was evaluated usingperipheral DXA (pDXA) every 4th week for 4 months in both Lrp5 nulland WT mice. Mice were euthanized at 18 weeks of age. Vertebral bodysize and cortical shell thickness of the L5 mid-vertebral body were evaluatedusing micro-computed tomography (micro-CT) and Scion Image software.Trabecular bone microarchitecture of the L5 vertebral body was evaluatedusing 3D micro-CT. Mechanical properties of the L5 vertebral body weretested by axial compression test.RESULTS: Longitudinal in vivo pDXA scans of the spine from Lrp5 nullmice showed significantly less BMD from a 4-week-old compared withage-matched WT mice (Fig. 1). Peak BMD in the spine from Lrp5 nullmice was 20% lower than WT mice. L5 cross-sectional area (CSA) fromLrp5 null mice was 14.5% lower. However, there was no significant differ-ence in cortical shell thickness. Trabecular bone microarchitecture fromLrp5 null mice revealed significantly lower bone volume fraction (�43%),trabecular number (�31%), and trabecular thickness (�16%). Ultimateforce from Lrp5 null mice was 51% lower in compression test. Parametersmost strongly related to ultimate force were BM D and trabecular number.CONCLUSIONS: These results suggest that Lrp5 gene governs mechani-cal strength of the vertebral body by regulating bone mass and trabecularbone microarchitecture.DISCLOSURES: No disclosures.CONFLICT OF INTEREST: No conflicts.
doi: 10.1016/j.spinee.2005.05.226
P12. Nonsurgical resource utilization in adult spinal deformitySteven Glassman, MD1, Sigurd Berven, MD2, John P. Kostuik, MD3,John Dimar, II, MD1, William Horton, MD4, Keith Bridwell, MD5;1Leatherman Spine Center, Louisville, KY, USA; 2University ofCalifornia, San Francisco, CA, USA; 3Department of OrthopaedicSurgery, Baltimore, MD, USA; 4Emory University, Atlanta, GA, USA;5Washington University in St. Louis, Saint Louis, MO, USA
BACKGROUND CONTEXT: Limited data exists with regard to theutilization or effectiveness of nonsurgical treatment modalities for adultspinal deformity.
PURPOSE: The purpose of this study is to quantify and analyze the useof nonsurgical resources in a large group of patients with adult spinaldeformity.STUDY DESIGN/SETTING: We reviewed the initial enrollment data fora group of 1061 patients entered into a prospective multi-center study ofadult spinal deformity between January 2002 and June 2004.PATIENT SAMPLE: Enrollment criteria were patients older than 18 yearswith scoliosis greater than 30 degrees, significant sagittal plane deformity,or history of scoliosis surgery greater than 18 months prior to enrollment.OUTCOME MEASURES: Health status measures were the SF-12, SRS-29 and ODI.METHODS: Demographic data, surgical history, symptom assessment andnonsurgical treatment regimen were reviewed. Resource utilization wasassessed based upon both patient and physician questionnaire responses.Three subgroups were identified: a surgical group (n�476), a high symptomnonsurgical group (n�335) and a low symptom nonsurgical group (n�250)based on age-adjusted ODI, validated by multiple regression analysis. Levelof resource utilization was compared across subgroups within the study.RESULTS: All the subgroups were similar with regard to age, genderand history of prior scoliosis surgery. The two nonsurgical subgroupsdiffered significantly on all reported health status measures (p�.0001).Quantifying resource utilization, the low symptom group used exercise(33%), analgesics or NSAIDS (24%), and pain management (22%) mostoften. The high symptom group used pain management (55%), with exerciseand analgesics or nonsteroidals reported equally (38%). The high symptomgroup used significantly greater resources in terms of narcotics, epiduralblocks and physical agent modalities (p�.001), analgesics (p�.01), painmanagement referral and bedrest (p�.02), strength training, nerve rootblocks and stabilization exercises (p�.05). Following study enrollment, thelow symptom group had a decrease in the use of pain management from22% to 8.4% (p�.001) and a decrease in the use of analgesics from 24%to 16% (p�.02). There was an increase in the use of exercise from 33% to66% (p�.001). For the high symptom nonsurgical group, there was adecrease in the use of no treatment from 37% to 19% (p�.001), exercisefrom 55% to 43% (p�.01), and bracing from 5% to 2% (p�.02). The highsymptom group had an increase in the use of bedrest from 15% to 27%,analgesics from 38% to 62%, and pain management from 17% to 39%(p�.001).CONCLUSIONS: This study demonstrates that within the population ofadult deformity patients, distinct high and low symptom subgroups exist, andcan be clearly identified. While there is a major difference in both typeand extent of intervention selected by patients with significant symptoms,even those patients with apparently limited clinical complaints utilized

Proceedings of the NASS 20th Annual Meeting / The Spine Journal 5 (2005) 1S–189S116S
transverse processes and achieve fusion equivalent to that seen with osteoge-nic autograft. The biocompatible silicate substituted calcium-phosphate ma-terial stimulated robust fusion and active cellular response throughout theosteoconductive matrix. Histological observations suggest the AP matrixresorbed through both cell-mediated and dissolution mechanisms. The APmatrix is a promising scaffold for posterior lateral fusion due to its initialmechanical support, interconnected porous structure, and silicate-initiatedosteostimulatory properties.DISCLOSURES: FDA device/drug: Pore-Si. Status: Not approved forthis indication.CONFLICT OF INTEREST: Author (DW) Consultant: ApaTech Lim-ited; Author (DW) Grant Research Support: ApaTech Limited #037281.
doi: 10.1016/j.spinee.2005.05.228
substantial nonsurgical treatment resources. Additional evaluation is neces-sary to determine the effectiveness of these nonsurgical treatments. It willbe important to assess the impact of each nonsurgical treatment regimen bothin terms of symptomatic improvement based on health status measures andupon the need for subsequent nonsurgical resource utilization or surgicalintervention.DISCLOSURES: No disclosures.CONFLICT OF INTEREST: Authors (SG, JDI) Consultant: Consultantfor Medtronic Sofamor Danek; Authors (SG, JDI) Other: Royalties receivedfrom Medtronic Sofamor Danek; Authors (SG, JDI, WH, KB) Grant Re-search Support: Medtronic Sofamor Danek; Author (SB) Consultant: Med-tronic Sofamor Danek, DePuy Spine; Author (SB) Grant Research Support:Medtronic Sofamor Danek, Kyphon.
doi: 10.1016/j.spinee.2005.05.227
P13. Posterior lateral lumbar spine fusion with silicate substitutedcalcium-phosphateDonna Wheeler, PhD1, Jason Marini1, Matthew Kovach1,Tatiana Motta1, Amy Lyons1, A. Turner, DVM1, Howard B. Seim, III,DVM, DRDES1, Louis Jenis, MD2*; 1Colorado State University, FortCollins, CO, USA; 2Boston Spine Group, Boston, MA, USA
BACKGROUND CONTEXT: Autograft has proven fusion efficacy overbone graft substitutes due to its cellularity and biological activity. Thesynthetic silicate substituted calcium-phosphate (Pore-Si, ApaTech) hasincreased bioactivity compared with pure hydroxyapatite.PURPOSE: To compare Pore-Si (AP) (without bone marrow supplementa-tion) with iliac crest autograft (AG) in an ovine single-level instrumentedlumbar dorsolateral intertransverse fusion.STUDY DESIGN/SETTING: Sheep underwent fusion with either AP orAG and healed for 2 (n�3/grp) or 6 months (n�6/grp).PATIENT SAMPLE: Skeletally mature ewes (50–80 kg).OUTCOME MEASURES: Plain radiographs, peripheral quantitativecomputed tomography (pQCT), biomechanics, histopathology, and histo-morphometry.METHODS: Anesthesized sheep (n�18) underwent decortication of L3and L4 transverse processes, L3-L4 facetectomies to induce instability, andgrafting with either AP or AG. Stabilization was accomplished with bilateraltranspedicular fixation. After 2 or 6 months of healing, spines were har-vested, plain radiographs acquired and films scored for fusion efficacy.pQCT scans were acquired at 2 and 4 months and at euthanasia (n�3/grp)and evaluated for fusion volume and fusion mass density. Lumbar segmentswere prepared and subjected to 5 nondestructive load cycles ranging from–5.0 N-m to 5.0 N-m in flexion/extension, lateral bending and torsion whilevertebral body motion was monitored with an optical tracking system.Stiffness and range of motion were quantified at the fusion site. The fusedmotion segments were trimmed and processed for undecalcified histology.Histopathology scores for graft integration, bone remodeling, cellular activ-ity, and inflammatory cells were made. Histomorphometric measurementsof total reactive area of fusion, bone and graft within fusion mass, andconnectivity characterized fusion.RESULTS: Plain radiographs revealed a strong trend for improved fusionscores in the AP group compared with AG. Similarly, trends towards greaterfusion volume in the AP group were seen using pQCT analysis. Densitycharacterization showed AP treated animals had denser fusion masses thanAG animals. Biomechanically, the AP and AG treatment groups had equiva-lent stiffness and range of motion in flexion/extension and lateral bending.Both AP and AG treatments showed similar progression of healing from 2to 6 months with equivalent bone remodeling, osteoblast activity, osteoclastactivity scores and minimal or no inflammatory cells. Both AP and AGgrafts were well integrated into the new bone matrix. The reactive area(fusion mass) was significantly greater for AP compared with AG animalswith equal percentages of bone and graft within the fusion. The connectivity(bone between transverse processes) was equivalent for AP and AG.CONCLUSIONS: This unique synthetic silicate substituted calcium-phos-phate material proved to successfully stimulate bone bridging between
P14. Piriformis syndrome: a controversial and undertreated causeof sciaticaKingsley R. Chin1, Ashraf Ragab, MD2, Jeffrey Roh, MD3,Henry H. Bohlman, MD4; 1University of Pennsylvania, Philadelphia,PA, USA; 2University of Mississippi, Jackson, MS, USA; 3CornellUniversity Medical College, New York, NY, USA; 4Case WesternReserve University, Cleveland, OH, USA
BACKGROUND CONTEXT: Spine specialists continue to view pirifor-mis syndrome as a controversial diagnosis and as such many patientsare undertreated.PURPOSE: We assessed outcome after surgical decompression of thesciatic nerve to treat piriformis syndrome.STUDY DESIGN/SETTING: Retrospective Clinical.PATIENT SAMPLE: 34 consecutive patients.OUTCOME MEASURES: Hip Score.METHODS: We evaluated 34 of 38 consecutive patients diagnosed byexclusion of spinal or pelvic pathology as a cause of sciatica, pelvic MRIof a potential source of sciatic nerve compression, and relief of symptomsimmediately after an injection of 1% Lidocaine and Triamcinolone aroundthe sciatic nerve in some patients. The mean duration of preoperativesymptoms was 47 months and 5 patients had a history of preceeding trauma.15 patients had a previous lumbar operation. Outcome was based on painrelief and patient satisfaction. Potential compressive structures and thepiriformis muscle were excised using a posterolateral approach.RESULTS: MRI detected potential unilateral compressive lesions in 31patients and bilateral in 4 patients. 12 patients reported some relief withlocal anesthetic injection versus 8 patients with no relief. Fibrous bandsor a leash of vessels was found directly compressing the sciatic nerve in30 patients, a split sciatic nerve in 5 patients, and an anomalous piriformismuscle splitting the nerve in 2 patients. 24 patients reported complete reliefof symptoms immediately after surgery. 3 patients reported partial relief, and7 patients reported no relief. 2 patients were re-explored for recurrentsymptoms at 10 and 16 months after the indexed procedure.CONCLUSIONS: Surgical decompression effectively treated piriformissyndrome provided strict patient selection criteria to rule out spinal orpelvic causes of sciatica.DISCLOSURES: No disclosures.CONFLICT OF INTEREST: No conflicts.
doi: 10.1016/j.spinee.2005.05.229
P15. Assessment of the accuracy of in vivo placement of artificialdiscs in the lumbar intervertebral space using computedtomography along with its radiographic and clinical consequencesVikas V Patel, MA, MD1*, Ben B Pradhan, MD, MSE2, Carol Andrews,MD2, Hyun W Bae, MD2, Linda E A Kanim, MS2, Rick B Delamarter,MD2; 1University of Colorado, Denver, CO, USA; 2The Spine Instituteat Saint John’s Health Center, Santa Monica, CA, USA