Embed Size (px)
Citation preview
P06 STROKE DETECTIONSimulation using magneticinduction tomography
P07 SILICONE OIL PROTECTSRadiation damage protection ofthe eyes using silicone oil
P07 CHILDHOOD CANCERInvestigating the link followingfoetal radiation exposure
SCOPERemote patient
monitoringTo improve patient
care on general wards
Simulatorsystems
For carrying outepicardial procedures
INSTITUTE OF PHYSICS AND ENGINEERING IN MEDICINE | www.ipem.ac.uk | Volume 19 Issue 4 | DECEMBER 2010
Special deliveriesSending radon and radium by post


PRESIDENT’S LETTER | SCOPE
have been reflecting on theattributes of a high-qualityscientific meeting, in the lightof another successful and wellattended IPEM Medical Physicsand Engineering Conference.
The quality of the scientificpresentations has to be top of the list,closely followed by the range ofopportunities for teaching andtraining. MPEC 2010 in Nottinghamcertainly provided all of those, andour thanks and congratulations go tothe organising committee and allmembers of the IPEM SIGs whocreated a programme which was bothdiverse and detailed. However,necessary as those attributes are, theyare not sufficient to ensure asuccessful conference.Accommodation, timetables, food,travel arrangements, exhibitioncontent and social events allcontribute to the experience of thedelegates, and create a framework forscientific and professionalinteractions which are at the heart ofa successful conference. All thoseinvolved in organising a conferencewant it to run smoothly, but in factthe scientific and professional successof any meeting is conditional onhaving the right environment inwhich to meet. Our thanks are due tothe organisers and to the IPEM officefor ensuring that once again,delegates were able to focus on thescientific and teaching sessions, in apleasant and stimulating setting.
OVERSEAS PARTNERSHIPMPEC 2010 and BioEngineering 2010was a jointly organised meeting withthe Bioengineering Society, and wecan look forward to an even widerpartnership arrangement next year.For some time the IPEM Trusteeshave been considering the possibilityof holding our annual conference at asuitable overseas venue, and MPEC2011 will be held at Trinity CollegeDublin, from 1st to 3rd September2011, as part of the European MedicalPhysics and Engineering Conference(EMPEC) 2011. More details can befound at http://www.empec.ie/, andinformation will also be circulatedvia the IPEM newsletter and website.The partner organisations will be the
IChris GibsonPresident
HARD WORK IS REWARDEDwinners, and countless otherscientists and engineers, are examplesof individuals who have foundsolutions to some of these problems,bringing to bear all the admirablehuman qualities of inspiration,imagination and ingenuity thatdemonstrate creativity. Progress is notjust a matter of doing yesterday’stasks better (although there is plentyof scope for that, and plenty ofbenefits too); it is also aboutidentifying tomorrow’s tasks.Scientist and engineers must be opento the possibilities of beingrevolutionary, at least in theirprofessional lives. The very use of theterm ‘revolution’ to denoteoverwhelming change was partlyinspired by ‘De RevolutionibusOrbium Coelestium’ by Copernicus,published in 1543, in which a newand elegant idea overthrew aprevious complex system. We tooshould be looking for those newideas, or new applications, or newprocesses, which by-pass our currentproblems with wholly novelsolutions. Whatever our role, allmembers of the Institute can engagewith this creative endeavour, and theIPEM prizes and awards are one wayin which we pay tribute to thosewhose successes are particularlyevident.
I wish you all a happy Christmas,and a creative, maybe evenrevolutionary, New Year.
Irish Association of Physicists inMedicine (the hosts) and also theEuropean Federation of Organisationsfor Medical Physics (EFOMP). I wouldlike to encourage all IPEM members toparticipate in this meeting, which willprovide an opportunity for you topresent your science in a Europeandimension. I am confident that theconference environment in Dublin,and the social dimension, will also beoutstanding!
AWARDS AND REWARDSOne of the many pleasures of beingIPEM President is the opportunity tomeet our award winners, and I hadthe privilege of presenting severalawards at the conference dinner inNottingham. Equally a pleasure, butperhaps a little more challenging, isthe traditional President’s after-dinnerspeech. With only a moderate degreeof ingenuity these two things canreadily be linked, giving the Presidenta ready-made subject for a speech, andnow a letter. I have no time for thosewho would divide academic andprofessional activities into the‘creative’ arts and the ‘mechanical’sciences, associating ‘inspiration’ withone and ‘perspiration’ with the other.Scientific work is all about solving thepuzzles set for us by the externalworld, and in healthcare there are aninfinite number of challenging andinteresting puzzles waiting for us toidentify and address. Our award
SCOPE | DECEMBER 2010 | 03
Creativity can grow fromseeds of inspiration
04 | DECEMBER 2010 | SCOPE
THIS ISSUE
COVER FEATURE51
08
26
40
RADON BY POSTSending radon by postduring World War II andwhat happened whenformerly radioactivecaves wererediscovered
08 MONITORINGRemote patient monitoring and the use of wireless technology to improvepatient care on general hospital wards
12 TRIALS AND TOOLS FOR TRAINEE TECHNOLOGISTS TO HELP LEARNIdeas for some simple and practical activities to gain knowledge and skills,leading to a great training experience
16 SIMULATOR SYSTEMSAn anthropomorphic simulator for epicardial procedures, useful fortraining and testing equipment
23 STATISTICAL PARADOXES: WHEN MATHS AND LOGIC COLLIDEParadoxes related to conditional probability and the implications they haveon data analysis in research
48 RADIUM BY POSTDocumentation from 1921 and the 1950s on the use of radium, and how it wassent through the post during wartime
03 PRESIDENT’S LETTER Hard work is rewarded05 EDITORIAL Christmas post06 NEWS Stories making headlines in the news40 INTERNATIONAL NEWS International conferences and useful web resources43 MEMBERS’ NEWS Congratulations to those who have passed exams45 BOOK REVIEWS New medical physics books and lots of new reports54 OBITUARY Sad news about Dr Jack Rowan
REGULARS
HISTORICAL FEATURE
26 10TH INTERNATIONAL WORKSHOP ON DIGITAL MAMMOGRAPHYJenny Diffey
31 5TH ANNUAL SENSE ABOUT SCIENCE LECTUREAlan McWilliam, Rosemary Eaton, Matt Ward and Neil Davis
35 RADIATION PROTECTION ADVISERS (RPA) UPDATE MEETING 2010Elizabeth Larkin
38 PER AORDUA AD ASTRACatherine Kendall
MEETING REPORTS
SCOPE | CONTENTS
16
ICov
er m
age
© G
etty
Imag
es

COMMENT | SCOPE
SCOPE | DECEMBER 2010 | 05
MARC E. MIQUEL EDITOR-IN-CHIEF
Scope is the quarterlymagazine of the Institute ofPhysics and Engineering inMedicineIPEM Fairmount House, 230 Tadcaster Road, York, YO24 1EST 01904 610821F 01904 612279E [email protected] www.ipem.ac.ukW www.scopeonline.co.uk
EDITOR-IN-CHIEFMarc E. MiquelDepartment of ClinicalPhysics, The Royal LondonHospital, 56–76 AshfieldStreet, London, E1 2BLT +44 (0)203 465 6771F +44 (0)207 377 7100E [email protected]
ASSISTANT EDITORGemma WhitelawRadiotherapy Physics,Basement, New KGVBuilding, St Bartholomew'sHospital, West Smithfield,London, EC1A 7BEE gemma.whitelaw@barts
andthelondon.nhs.uk
MEETING REPORTSEDITORAngela CottonHead of Non-IonisingRadiation Support, Medical Physics &Bioengineering,Southampton GeneralHospital, Southampton,SO16 3DRE angela.cotton@suht.
swest.nhs.uk
NEWS EDITORChristie McCombMRI/SPECT, Institute ofNeurological Science,Southern General Hospital,1345 Govan Road, Glasgow, G51 4TFT 0141 201 2120E [email protected]
BOOK REVIEW EDITORSMarium NaeemDepartment of RadiotherapyPhysics, St Thomas'Hospital, London, SE1 7EHE marium.naeem@
gstt.nhs.ukUsman I. LulaDepartment ofRadiotherapy, PooleHospital, Longfleet Road,Poole, BH15 2JBE [email protected]
ENGINEERING &ACADEMIC EDITORDr Constantinos ZervidesIntercollege Larnaca6019 Larnaca, CyprusE c.zervides@intercollege-
larnaca.comT 00357-24-747500/559F 00357-24-652213
MEMBERS’ NEWS EDITORMatt GwilliamCancer Research UKClinical MR ResearchGroup, Institute of CancerResearch and RoyalMarsden NHS FoundationTrust, Sutton, SM2 5PTE [email protected]
INTERNATIONAL EDITOR(Developing countries)Andrew GammieClinical Engineer, Bristol Urological Institute,BS10 5NBT +44(0)117 950 5050
extension 2448 or 5184E [email protected]
INTERNATIONAL EDITOR(North America)Richard A. Amos Department of RadiationPhysics, The University ofTexas M.D. AndersonCancer Center, 1840 Old
Spanish Trail,Houston,Texas 77054, U.S.A.T + 1 713 563 6894F + 1 713 563 1521E richamos@mdanderson.
org
INTERNATIONAL EDITORRyan D. LewisDepartment of MedicalPhysics and ClinicalEngineering, Abertawe BroMorgannwg University NHS Trust, SingletonHospital, Swansea, Wales, SA2 8QAT +44(0)179 220 5666
extension 6438E ryan.lewis@swansea-
tr.wales.nhs.uk
ONLINE EDITORDr Damian JJ Farnell Health MethodologyResearch Group, School ofCommunity-BasedMedicine, Jean McFarlaneBuilding, University PlaceUniversity of Manchester,Manchester M13 9PLT +44 (0)161 30 67329F +44 (0)161 275 5205E [email protected] http://www.medicine.manchester.ac.uk/staff/dfarnell
Published on behalf of the Institute of Physics and Engineering inMedicine byCENTURY ONEPUBLISHING LTD.Alban Row, 27–31 VerulamRoad, St Albans, Herts, AL3 4DGT 01727 893 894F 01727 893 895E enquiries@centuryone
publishing.ltd.ukW www.centuryone
publishing.ltd.uk
CHIEF EXECUTIVENick SimpsonT 01727 893 894E nick@centuryone
publishing.ltd.uk
ADVERTISING SALESBhupinder RanT 01727 739 182E bhupinder@centuryone
publishing.ltd.uk
SUB EDITORKaren MclarenE karen@centuryone
publishing.ltd.uk
DESIGN & PRODUCTIONHeena GudkaE studio@centuryone
publishing.ltd.uk
PRINTED BY Century One Publishing Ltd
Scope is publishedquarterly by the Institute ofPhysics and Engineering inMedicine but the viewsexpressed are notnecessarily the officialviews of the Institute.Authors instructions andcopyright agreement canbe found on the IPEMwebsite. Articles should besent to the appropriatemember of the editorialteam. By submitting toScope, you agree totransfer copyright to IPEM.We reserve the right to edityour article. Proofs are notsent to contributors. Theintegrity of advertisingmaterial cannot beguaranteed.
CopyrightReproduction in whole orpart by any means withoutwritten permission of thepublisher is strictlyforbidden. © IPEM 2010ISSN 0964-9565
inal issue of the year,Christmas fast approaching,and the Scope stocking isbursting at the seams,overflowing with features.
Like the Institute’smembership, the selection of
features is very diverse both through itsauthors and its subjects. Azzam Taktaklooks at the lighter side of statistics, whileLeanne Moore reflects on her trainingexperience. Our engineering editor,Constantinos, has been busy chasing copyand has provided us with two features. Thefirst by Anh Bui and colleagues looks atsimulator systems for epicardial procedures,while the second, by Reza Sahandi, GelarehRoushan and Vanessa Heaslip, focuses onremote patient monitoring.
With such a variety, I could nearlyparaphrase Forrest Gump and claim that:‘Scope is like a box of (Christmas) chocolates;you never know what you’re gonna getinside’.
Obviously, this is strictly speaking nottrue; as always, our other editors have alsobeen hard at work to bring us our regularmeetings, book reviews and news sections.
To close this issue, we celebrate the returnof historical features and, as we never dothings by half, we included two! DavidMurnaghan and Alan Jennings bring usback to a not-so-distant time where the postwas not only carrying our letters to Santabut also radium and radon. Alan’s featurealso has a Time Team flavour to it, but Iwill let you discover why.
Unfortunately, this profusion offeatures meant that we had to delay the
publication of our new members listwhich will now appear in the
March 2011issue.
To finish,I’d like tothank all of
those whocontributed to
Scope this year andall the members of the
editorial team for theirdedication.
Hope you enjoy this issue.
FCHRISTMAS POST
The selection offeatures is verydiverse boththrough its authorsand its subjects
”“
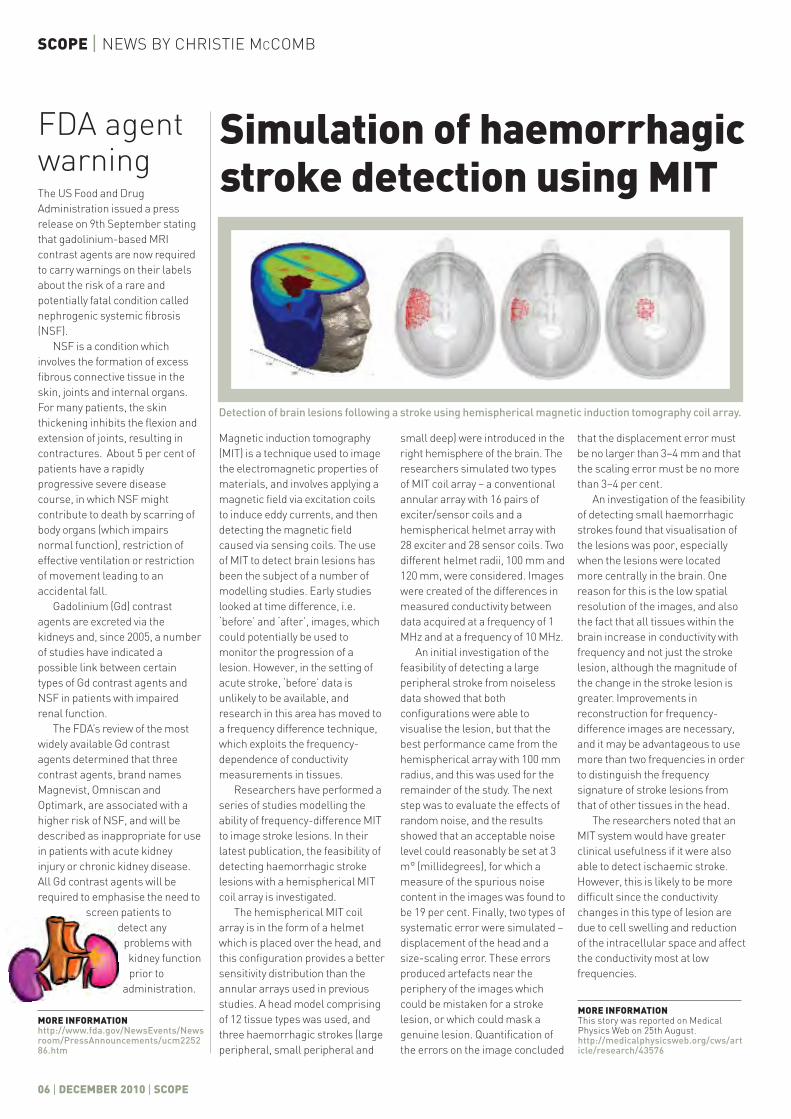
Magnetic induction tomography
(MIT) is a technique used to image
the electromagnetic properties of
materials, and involves applying a
magnetic field via excitation coils
to induce eddy currents, and then
detecting the magnetic field
caused via sensing coils. The use
of MIT to detect brain lesions has
been the subject of a number of
modelling studies. Early studies
looked at time difference, i.e.
‘before’ and ‘after’, images, which
could potentially be used to
monitor the progression of a
lesion. However, in the setting of
acute stroke, ‘before’ data is
unlikely to be available, and
research in this area has moved to
a frequency difference technique,
which exploits the frequency-
dependence of conductivity
measurements in tissues.
Researchers have performed a
series of studies modelling the
ability of frequency-difference MIT
to image stroke lesions. In their
latest publication, the feasibility of
detecting haemorrhagic stroke
lesions with a hemispherical MIT
coil array is investigated.
The hemispherical MIT coil
array is in the form of a helmet
which is placed over the head, and
this configuration provides a better
sensitivity distribution than the
annular arrays used in previous
studies. A head model comprising
of 12 tissue types was used, and
three haemorrhagic strokes (large
peripheral, small peripheral and
small deep) were introduced in the
right hemisphere of the brain. The
researchers simulated two types
of MIT coil array – a conventional
annular array with 16 pairs of
exciter/sensor coils and a
hemispherical helmet array with
28 exciter and 28 sensor coils. Two
different helmet radii, 100 mm and
120 mm, were considered. Images
were created of the differences in
measured conductivity between
data acquired at a frequency of 1
MHz and at a frequency of 10 MHz.
An initial investigation of the
feasibility of detecting a large
peripheral stroke from noiseless
data showed that both
configurations were able to
visualise the lesion, but that the
best performance came from the
hemispherical array with 100 mm
radius, and this was used for the
remainder of the study. The next
step was to evaluate the effects of
random noise, and the results
showed that an acceptable noise
level could reasonably be set at 3
m° (millidegrees), for which a
measure of the spurious noise
content in the images was found to
be 19 per cent. Finally, two types of
systematic error were simulated –
displacement of the head and a
size-scaling error. These errors
produced artefacts near the
periphery of the images which
could be mistaken for a stroke
lesion, or which could mask a
genuine lesion. Quantification of
the errors on the image concluded
that the displacement error must
be no larger than 3–4 mm and that
the scaling error must be no more
than 3–4 per cent.
An investigation of the feasibility
of detecting small haemorrhagic
strokes found that visualisation of
the lesions was poor, especially
when the lesions were located
more centrally in the brain. One
reason for this is the low spatial
resolution of the images, and also
the fact that all tissues within the
brain increase in conductivity with
frequency and not just the stroke
lesion, although the magnitude of
the change in the stroke lesion is
greater. Improvements in
reconstruction for frequency-
difference images are necessary,
and it may be advantageous to use
more than two frequencies in order
to distinguish the frequency
signature of stroke lesions from
that of other tissues in the head.
The researchers noted that an
MIT system would have greater
clinical usefulness if it were also
able to detect ischaemic stroke.
However, this is likely to be more
difficult since the conductivity
changes in this type of lesion are
due to cell swelling and reduction
of the intracellular space and affect
the conductivity most at low
frequencies.
FDA agentwarning
Simulation of haemorrhagicstroke detection using MIT
SCOPE | NEWS BY CHRISTIE MCCOMB
06 | DECEMBER 2010 | SCOPE
Detection of brain lesions following a stroke using hemispherical magnetic induction tomography coil array.
MORE INFORMATIONhttp://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm225286.htm
MORE INFORMATIONThis story was reported on MedicalPhysics Web on 25th August.http://medicalphysicsweb.org/cws/article/research/43576
The US Food and Drug
Administration issued a press
release on 9th September stating
that gadolinium-based MRI
contrast agents are now required
to carry warnings on their labels
about the risk of a rare and
potentially fatal condition called
nephrogenic systemic fibrosis
(NSF).
NSF is a condition which
involves the formation of excess
fibrous connective tissue in the
skin, joints and internal organs.
For many patients, the skin
thickening inhibits the flexion and
extension of joints, resulting in
contractures. About 5 per cent of
patients have a rapidly
progressive severe disease
course, in which NSF might
contribute to death by scarring of
body organs (which impairs
normal function), restriction of
effective ventilation or restriction
of movement leading to an
accidental fall.
Gadolinium (Gd) contrast
agents are excreted via the
kidneys and, since 2005, a number
of studies have indicated a
possible link between certain
types of Gd contrast agents and
NSF in patients with impaired
renal function.
The FDA’s review of the most
widely available Gd contrast
agents determined that three
contrast agents, brand names
Magnevist, Omniscan and
Optimark, are associated with a
higher risk of NSF, and will be
described as inappropriate for use
in patients with acute kidney
injury or chronic kidney disease.
All Gd contrast agents will be
required to emphasise the need to
screen patients to
detect any
problems with
kidney function
prior to
administration.
IN BRIEF
WARNINGS ONMRI AGENTSGadolinium-based MRIcontrast agents must nowcarry warnings on theirlabels about the risk of arare skin thickeningcondition callednephrogenic systemicfibrosis, which isparticularly dangerous inthe case of patients withkidney impairments.
MIT STROKEDETECTIONHaemorrhagic strokelesions in the brain havebeen investigated usingmagnetic inductiontomography (MIT) coilarrays. This involvedapplying a magnetic fieldvia excitation coils, andthen detecting it viasensing coils. However,visualisation of thelesions was poor soimprovements inreconstruction arenecessary.
SILICONE OILPROTECTS EYESThe use of silicone oil inthe eye has been found toprotect delicate tissuesfrom damage duringiodine-125 brachytherapytreatment for intraocularcancer. Following successin a porcine model andlive study, and theresearchers hope to begina human trial in the nearfuture.
CHILDHOODCANCER RISKA large study has beencarried out to investigatethe link between in uteroexposure to ionisingradiation and childhoodcancer. There was nostatistically significantrisk, but the possibility ofexposure to ionisingradiation throughdiagnostic imaging beingcarcinogenic has not beenruled out.
NEWS BY CHRISTIE MCCOMB | SCOPE
SCOPE | DECEMBER 2010 | 07
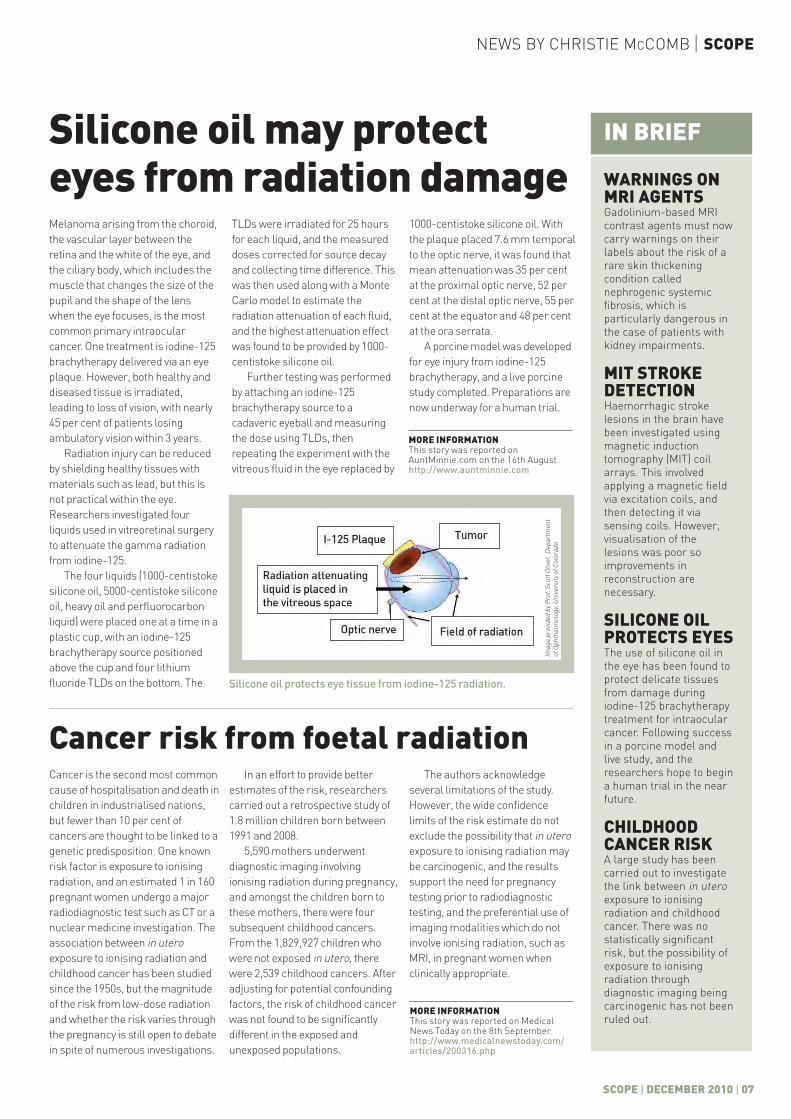
TLDs were irradiated for 25 hoursfor each liquid, and the measureddoses corrected for source decayand collecting time difference. Thiswas then used along with a MonteCarlo model to estimate theradiation attenuation of each fluid,and the highest attenuation effectwas found to be provided by 1000-centistoke silicone oil.
Further testing was performedby attaching an iodine-125brachytherapy source to acadaveric eyeball and measuringthe dose using TLDs, thenrepeating the experiment with thevitreous fluid in the eye replaced by
1000-centistoke silicone oil. Withthe plaque placed 7.6 mm temporalto the optic nerve, it was found thatmean attenuation was 35 per centat the proximal optic nerve, 52 percent at the distal optic nerve, 55 percent at the equator and 48 per centat the ora serrata.
A porcine model was developedfor eye injury from iodine-125brachytherapy, and a live porcinestudy completed. Preparations arenow underway for a human trial.
Cancer risk from foetal radiationCancer is the second most commoncause of hospitalisation and death inchildren in industrialised nations,but fewer than 10 per cent ofcancers are thought to be linked to agenetic predisposition. One knownrisk factor is exposure to ionisingradiation, and an estimated 1 in 160pregnant women undergo a majorradiodiagnostic test such as CT or anuclear medicine investigation. Theassociation between in uteroexposure to ionising radiation andchildhood cancer has been studiedsince the 1950s, but the magnitudeof the risk from low-dose radiationand whether the risk varies throughthe pregnancy is still open to debatein spite of numerous investigations.
In an effort to provide betterestimates of the risk, researcherscarried out a retrospective study of1.8 million children born between1991 and 2008.
5,590 mothers underwentdiagnostic imaging involvingionising radiation during pregnancy,and amongst the children born tothese mothers, there were foursubsequent childhood cancers.From the 1,829,927 children whowere not exposed in utero, therewere 2,539 childhood cancers. Afteradjusting for potential confoundingfactors, the risk of childhood cancerwas not found to be significantlydifferent in the exposed andunexposed populations.
Silicone oil may protecteyes from radiation damage
The authors acknowledgeseveral limitations of the study.However, the wide confidencelimits of the risk estimate do notexclude the possibility that in uteroexposure to ionising radiation maybe carcinogenic, and the resultssupport the need for pregnancytesting prior to radiodiagnostictesting, and the preferential use ofimaging modalities which do notinvolve ionising radiation, such asMRI, in pregnant women whenclinically appropriate.
Silicone oil protects eye tissue from iodine-125 radiation.
Melanoma arising from the choroid,the vascular layer between theretina and the white of the eye, andthe ciliary body, which includes themuscle that changes the size of thepupil and the shape of the lenswhen the eye focuses, is the mostcommon primary intraocularcancer. One treatment is iodine-125brachytherapy delivered via an eyeplaque. However, both healthy anddiseased tissue is irradiated,leading to loss of vision, with nearly45 per cent of patients losingambulatory vision within 3 years.
Radiation injury can be reducedby shielding healthy tissues withmaterials such as lead, but this isnot practical within the eye.Researchers investigated fourliquids used in vitreoretinal surgeryto attenuate the gamma radiationfrom iodine-125.
The four liquids (1000-centistokesilicone oil, 5000-centistoke siliconeoil, heavy oil and perfluorocarbonliquid) were placed one at a time in aplastic cup, with an iodine-125brachytherapy source positionedabove the cup and four lithiumfluoride TLDs on the bottom. The
MORE INFORMATIONThis story was reported onAuntMinnie.com on the 16th August.http://www.auntminnie.com
MORE INFORMATIONThis story was reported on MedicalNews Today on the 8th September.http://www.medicalnewstoday.com/articles/200316.php
Imag
e pr
ovid
ed b
y Pro
f. Sc
ott O
liver
, Dep
artm
ent
of O
phth
alm
olog
y, U
nive
rsity
of C
olor
ado

08 | DECEMBER 10 | SCOPE
PATIENT MONITORINGHistorically, a general ward was anon-specialist hospital unit offering arange of treatments to a variety ofpatients. However, advances inmedical technology have led topatients living with much morecomplex health issues, leading to anincrease in the numbers of critically illpatients being managed within thegeneral ward setting.8, 9 Therefore,some patients require frequentattention whilst others who are instable conditions require less.
The interval for visiting patients bynurses to measure physiological datacan vary depending on the severity ofthe patient’s condition. NICE clinicalguidelines2 state that as a minimum,heart rate, respiratory rate, systolicblood pressure, level of consciousness,oxygen saturation and temperatureshould be recorded at the initialassessment and as part of routinemonitoring.
The practice has been that,typically, a nurse or healthcareassistant visits a patient to observevital signs and compare them with thedata taken previously. The frequencyof visits may relate to a suggestedschedule which will depend on theseverity of patient’s condition and thenurse’s judgment, which can besubjective. However, it is argued thatmonitoring vital signs is typicallyviewed as a mundane aspect of
INTRODUCTIONThe Commission for Healthcare Auditand Inspection1 indicated that thereare inefficiencies in patientmonitoring, particularly on generalhospital wards. This is supported bythe National Institute for Health andClinical Excellence (NICE) clinicalguidance,2 which indicated thatpatients on general wards within theUK believed there was insufficientmonitoring. This report identified thatsome patients felt ‘abandoned’, whilstothers experienced being leftunattended for varying lengths oftime. The Commission for HealthcareAudit and Inspection highlights twomajor concerns within healthcare inthe UK, which are poor care ofpatients within general wards andinequalities.1 The recent publication ofthe Darzi report3 further endorsed theneed to continuously improve thequality of care within the NationalHealth Service (NHS).
Nurses are fundamental to highquality healthcare,4 as they have thegreatest contact with patients. Part ofthis role within the hospital is themonitoring of patients, including thegathering of physiological data suchas blood pressure, temperature, pulseand respiration rates. The frequency ofcontact by nurses is dependent uponthe patients’ needs, based upon theseverity of their condition, which canbe subjective.
The application of remote patientmonitoring (RPM) would free nurses’time, enabling them to provideenhanced personal care to patients.Indeed there is recognition that qualityreviews must include the personalaspect of the clinical experience as wellas the clinical outcome,3, 4 yet theConfidence in Caring report5 identifiedthat patients feel the NHS is very goodat caring for them but not necessarilyabout them. It is indicated thatadopting RPM technologies couldimprove the healthcare services, byfreeing nurses up to provide morepersonalised care by reducing visits forroutine monitoring by 30–50 per cent.6
Thus, the use of RPM would providethe opportunity for nurses to focusupon the holistic needs of patients.Obviously RPM systems cannotreplace the functions of nurses;however, they can complement theirrole, further improving patient care. AnRPM system can provide convenienceand be more cost effective compared totraditional institutional care, since itenables healthcare organisations tomonitor and manage patients remotelywhilst being cared for professionally.7
Furthermore, early detection ofabnormalities of patients’physiological data could improverecovery and reduce mortality ratesduring hospitalisation. This articlediscusses wireless technology in thecontext of RPM systems.
Remotepatientmonitoring hasthe potential toimprovehealthcareservices.
�
Reza Sahandi, Gelareh Roushan and Vanessa Heaslip (Bournemouth University)explain the potential benefits of remote patient monitoring on a general ward
MONITORING To improve patient care on general hospital wards

FEATURE | SCOPE
SCOPE | DECEMBER 10 | 09
nursing care which is frequentlydelegated to healthcare assistants,whose varying levels of trainingprovokes concern regarding accuracyand interpretation of data.10
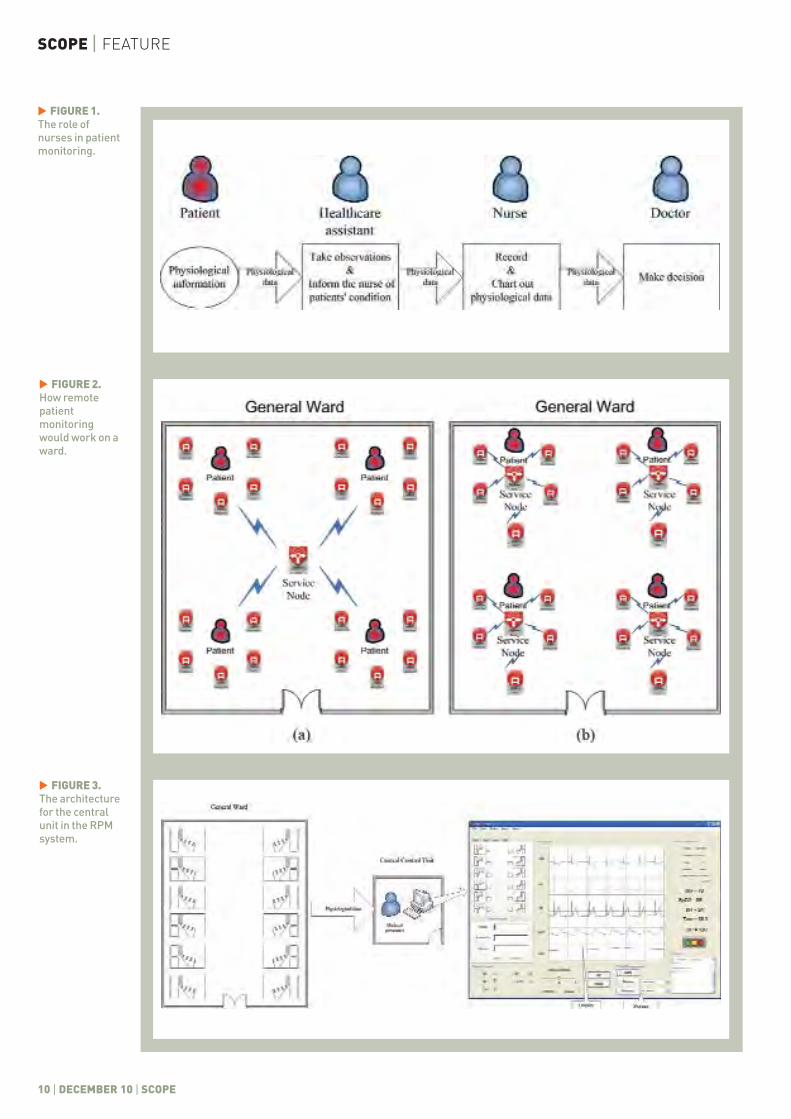
When a nurse realises that apatient’s condition is deteriorating, itis most likely that the frequency of thevisits will increase. This will onlyhappen if the patient is monitoredfrequently and effectively. Figure 1shows the role of nurses in this context.
Patient monitoring is a labour-intensive activity, and humanresources are the most important inputinto this provision.11 However, it isrecognised that there is a potential linkbetween increased medical errors anda cognitive overload of healthcareprofessionals.12 Therefore, it is arguedthat one major issue in patientmonitoring is the number of patientsper healthcare professional and thepotential cognitive overload that mayoccur with frequent messages frompatient monitoring systems.
To improve patient care on generalwards, early warning scores (EWS)have been introduced in manyhospitals. The mission of the EWSsystem is to ensure timelyidentification of patients withpotential or established critical illnessand to ensure early detection ofpatient deterioration and attendanceby appropriately skilled staff.13 Theinitial EWS systems were paper-basedand there were problems associatedwith them, for example diagnoseswritten illegibly on paper and doctorsnot having easy access to patientinformation14; however, this ismigrating to electronic-based systems.
RPM SYSTEM DEVELOPMENTMany approaches have been adoptedto improve the processes of recordingand disseminating patient’sphysiological data to healthcarepractitioners. The paper-basedpractice of keeping a patient’sphysiological data record at thebedside is gradually being replaced byelectronic recording and transmission.Various PDA-based systems for semi-automated recording and transmissionof vital signs have been introduced invarious hospitals. At Cedars-Sinaihospital in California, wirelesslyconnected PDAs were used to accessclinical information from patientrecords.15 Further, in the UK, a pilotstudy of a pen-based PDA system, torecord clinical data, concluded that thesystem presented a viable alternative
PDA-basedsystems recorddata.
�
to a paper-based one.16 In such asystem, medical staff carry PDAs toinput data, which is then transmittedthrough a wireless network to adatabase in the hospital. Further, toimplement data acquisition andtransmission in real-time, a dataacquisition module was integratedwith a PDA.17 The main functions ofthe PDA were to display patients’physiological data and transmit it to acontrol unit.
An integrated patient monitoringand physiological data recordingsystem based on PDAs wasdeveloped.18 The system relied ontimely collection and recording ofphysiological data in PDAs byhealthcare staff when visiting patients.By comparison with the traditionalpaper-based method, this speeded upvital signs recording and improvedaccurate decision making.19
Although the application of PDA-based systems is an improvement topaper-based systems, they cannotprovide real-time patient monitoring.Nurse visits are still an essential partof monitoring patients and gatheringphysiological data.
Interests in the application ofwireless sensor networks have grownconsiderably.20 If wireless sensors areused, they can provide flexibility andfacilitate better mobility for patients,which may possibly improve theirspeed of recovery.
It should be mentioned thatvarious remote patient monitoringsystems have already beendeveloped. However, they are moresuitable for applications such as inhome care,21 during patienttransportation intra-hospital22 and foremergency aid.23 These systems havemany limitations and they are notsuitable for general wards. Forexample, they are wired and theycannot support multiple patients ormultiple parameters.18
An automated remote patientmonitoring system would
provide further improvementand equal care to patients ongeneral wards. If wirelesssensors are used, the systemcan provide enhanced mobility
and comfort to the patients.Physiological data
gathered from eachpatient can betransmitted to acontrol unit in realtime for recordingand analysis.
ZigBee is a technology which canbe used for wireless sensors for suchan RPM system. Its low powerconsumption and reasonabletransmission range makes it moresuitable for long-term patientmonitoring.24
Khan et al. proposed a systembased on a single ZigBee sensornetwork,20 which could only supportRPM for a few patients on a ward.Figure 2a shows such a system. Inthis system, a service node gathersphysiological data from the sensorsattached to patients on a generalward and transmits it to a controlunit. However, some general wardsare large and the number of patientson them could rise to around 30. Inthese wards, a single ZigBee sensornetwork using a service node will beunable to support all of the sensors.An alternative approach wasproposed,25 which considers a ZigBeesensor network for each patient.Figure 2b illustrates this approach.
There is a possibility ofinterference between ZigBee andother wireless systems. In Sahandiand Liu,26 the interference betweenZigBee and WiFi systems wereinvestigated and it was concludedthat it is negligible, particularly if thelatest WiFi standard (IEEE 802.11n) isused. However, further researchwould be necessary to investigate theeffect of interference from otherwireless systems on ZigBee signals.
Due to the nature of generalwards, patients may require differentlevels of medical care and attention.Some patients may require frequentmonitoring, whilst others may needless. The RPM for general wardsshould, therefore, have the facility toenable the transmission interval to beadjusted. This is necessary aspatients’ conditions may change,resulting in more intensivemonitoring being required.
The control unit is the centre fordata processing, analysis and visualdisplay. Figure 3 illustrates thearchitecture for the central unit in theRPM system. Patient’s physiologicaldata received from the service nodescan be displayed graphically onlinefor real-time monitoring. The datacan be analysed for a pattern ofchange to identify abnormalities,possibly preventing furtherdeterioration of a patient’s condition,especially as these could beinterlinked with the EWS. An alarmmay be raised when an abnormality �
SCOPE | FEATURE
10 | DECEMBER 10 | SCOPE
FIGURE 1.The role ofnurses in patientmonitoring.
�
FIGURE 2.How remotepatientmonitoringwould work on award.
�
FIGURE 3.The architecturefor the centralunit in the RPMsystem.
�

SCOPE | DECEMBER 10 | 11
FEATURE | SCOPE
is identified, which would enable atimely assessment and management ofa patient’s needs. In addition, anothermajor benefit of this would be theability to monitor patients and observechanges to their conditions much moreunobtrusively, especially at night toavoid disturbing sleep. Doctors willalso be able to access this informationremotely through the Internet, whichwould reduce the time taken formedics to review patients, especially ifthey are away from them. Access topatients’ medical history may also beavailable through a web link.
It may be possible to implement adetection system based onidentification of sudden changes tovital signs, which may be used as aninitial trigger in an automated RPMsystem. Further, physiological datacan also be stored for future use at thecentral control unit. Data of a largepopulation of patients stored over aperiod of time may be used to studypossible patterns of change in patients’conditions, facilitating identification ofgeneric health problems of one ormore groups of patients.
The issue of security and dataintegrity also requires attention due topotential detrimental consequences.
Accordingly adoption of wirelesstechnologies for transmitting medicaldata signifies greater need forsecurity. Data transmitted throughwireless networks should beencrypted to increase security andany physiological data should beaccompanied by the patient’sidentification (PID), avoidingmisrepresentation. Access to recordedand live data should go throughauthentication processes, to avoidunauthorised access.
Finally, it should be noted thatsome aspects of RPM systems havealready been developed. Althoughmuch progress has been made, a fullyautomated RPM system on generalhospital wards with the capability ofmonitoring a large number of patientsand identifying patient abnormalitiesis yet to be developed.
CONCLUSION Patients on general wards are oftenmonitored by healthcare personnelaccording to the severity of theirconditions; however this is oftenbased upon the nurses’ judgmentwhich is subjective. In addition, thislabour-intensive task is oftendelegated to non-qualified
practitioners, and it is prone to error.Insufficient medical and nursing staffin some hospitals may result inpatients not receiving the expectedcare and attention.
Progression in patient monitoringin many hospitals has resulted in theintroduction of EWS to ensure timelyand appropriate responses are takenfor treatment. Furthermore, in recentyears, some hospitals haveimplemented PDA-based systems forsemi-automated recording andtransmission of vital signs.
An automated wireless RPMsystem providing flexibility, mobility,comfort and real-time monitoringcould go some way towardsimproving patient care on generalwards. The RPM can provide equalcare and attention to all patients on award, enabling speedy identificationof the deterioration of a patient’scondition, especially as these could beinterlinked with the EWS. Doctorsmay also have remote access to thisinformation through the Internet.Finally, RPM systems cannot replacethe role of nurses, but it will free theirtime to provide enhanced personalcare to patients and focus upon theirholistic needs. �
1 Commission for Healthcare Audit and Inspection. Are WeChoosing Health? The Impact of Policy on the Delivery ofHealth Improvement Programmes and Services. Concordatgateway number 137. London, 2008.
2 National Institute for Health and Clinical Excellence.Acutely Ill Patients in Hospital: Recognition of andResponse to Acute Illness in Adults in Hospital. NICEclinical guideline 50. London, 2007.
3 Department of Health. High Quality Care for All. London,2008.
4 Department of Health. Framing the Nursing and MidwiferyContribution: Driving Up the Quality of Care. London, 2008.
5 Department of Health. Confidence in Caring. London, 2008,1–37.
6 Kuraitis V. Five Lingering Questions Holding Back RemotePatient Monitoring (RPM) Adoption. http://e-caremanagement.com/five-lingering-questions-holding-back-remote-patient-monitoring-rpm-adoption/ (accessed18th April 2008).
7 Barlow J et al. Meeting government objectives for telecarein moving from local implementation to mainstreamservices. J Telemed Telecare 2005; 11: 49–51.
8 Gordon AC et al. Incidence and outcome of critical illness
amongst hospitalized patients with hematologicalmalignancy: a prospective observational study of ward andintensive care unit based care. Anaesthesia 2005; 60: 340–7.
9 Johnstone C, Rattray J, Myers L. Physiological risk factors,early warning scoring systems and organizational changes.Nurs Crit Care 2007; 12: 219–24.
10 Davidson K, Barber V. Electronic monitoring of patient ingeneral wards. Nurs Stand 2004; 18: 42–6.
11 Bloor K, Maynar A. Planning Human Resources in HealthCare: Towards an Economic Approach, An InternationalComparative Review.http://www.fcrss.ca/final_research/commissioned_research/programs/pdf/bloor_report.pdf (accessed 6 April 2008).
12 Varshney U. Enhancing Wireless Patient Monitoring byIntegrating Stored and Live Patient Information. Paperpresented at the 19th International Symposium on IEEEComputer-Based Medical Systems, Washington DC, USA,2006.
13 Department of Health and NHS Modernisation Agency. TheNational Outreach Report. London, 2003.
14 Meingast M, Roosta T, Sastry S. Security and Privacy Issueswith Health Care Information Technology. Paper presentedat the 28th Annual International Conference on IEEE
REFERENCES
�
SCOPE | FEATURE
12 | DECEMBER 10 | SCOPE
Engineering in Medicine and Biology Society, New York,USA, 2006.
15 Corman R. Cedars-Sinai uses Pal0000m VIIs to AccessClinical Information: A News Item Reported.http://www.handheldmed.com (accessed 12 May 2008).
16 Gardner M, Sage M, Gray P. Data capture for clinicalanaesthesia on a pen-based PDA: is it a viable alternative topaper? Proc HCI01 Conf People Comp XV 2001; 439–56.
17 Gao H et al. Systematic review and evaluation ofphysiological track and trigger warning systems foridentifying at-risk patients on the ward. Intens Care Med2007; 33: 667–79.
18 Smith G et al. Hospital wide physiological surveillance: anew approach to the early identification and management ofthe sick patient. Resuscitation 2006; 71: 19–28.
19 Prytherch D, Smith GB, Schmidt P. Calculating earlywarning scores-a classroom comparison of pen and paperand hand-held computer methods. Resuscitation 2006; 70:173–8.
20 Khan JY, Yuce MR, Karami F. Performance Evaluation of aWireless Body Area Sensor Network for Remote PatientMonitoring. Paper presented at the 30th Annual
International Conference on IEEE Engineering in Medicineand Biology Society, Vancouver, Canada, 2008.
21 Clarke M et al. Providing remote patient monitoringservices in residential care homes. Curr PerspectHealthcare Comput 2004; 114–22.
22 Lin YH et al. A wireless PDA-based physiological monitoringsystem for patient transport. IEEE T Inf Technol B 2004; 8:439–47.
23 Kumar S et al. Ubiquitous computing for remote cardiacpatient monitoring: a survey. Int J Telemed App 2008; 4:1–19.
24 Farahani G. ZigBee Wireless Network and Transceivers.Oxford: Elsevier, 2008.
25 Sahandi R et al. Wireless technology in the evolution ofpatient monitoring on general hospital wards. J Med EngTechnol 2010; 34: 51–63.
26 Sahandi R, Liu Y. Channel overlap problems of ZigBeenetworks for remote patient monitoring on general hospitalwards. IEEE Proceedings, International Conference onCommunications and Mobile Computing (CMC 2010),Shenzhen, China, 2010.
REFERENCES CONTINUED
Activitiesneed to bestructuredin aproductivemanner
“”
INTRODUCTIONAfter attending MPEC 2010 and receiving such positivefeedback on my presentation, Gaining Confidence in theMould Room, I feel there is a need for collaboration onhow to create a positive learning experience for traineetechnologists. As a second year trainee technologistspecialising in radiotherapy physics I would like toshare my training experience and inspire others tomaximise the opportunities we have.
I became involved with MPEC after an ATENrepresentative promoted the event. What reallyinterested me were the specific trainee sessions, as I feltit would be a great way to meet other trainees; howeverthis was not to be! I was one of two trainee technologiststo attend and this is such a shame as I gained so muchfrom going. I would like to reassure all traineetechnologists that physicists are not as scary as youthink, the content was quite accessible and theatmosphere was great. I found many of thepresentations interesting and it helped to link aspects of
my academic training with practical work scenarios. I amconcerned that if more interest is not expressed in thefuture technologists could be missing out on a fantasticlearning resource.
In this article I would like to summarise thepresentation I gave and to share my ideas of what makesfor a great training experience.
OVERVIEWThe aim of the presentation was to identify areas wheretrainees may require extra support and suggest practicalskills and strategies for trainees and training supervisorsto facilitate a more enriched training experience. Theexamples discussed relate directly to the mould room.The mould room is responsible for immobilisationdevices, treatment accessories and clinical impressions toaid radiotherapy treatment. However, activities aretransferable across all disciplines with the overall focus ofbuilding confidence. The presentation was split into foursections:
Leanne Moore (Plymouth Hospitals NHS Trust, Devon) shares her ideas on how toget the most out of training with some simple, practical activities
Successful trials and toolsfor trainee technologists
�
FEATURE | SCOPE
SCOPE | DECEMBER 10 | 13
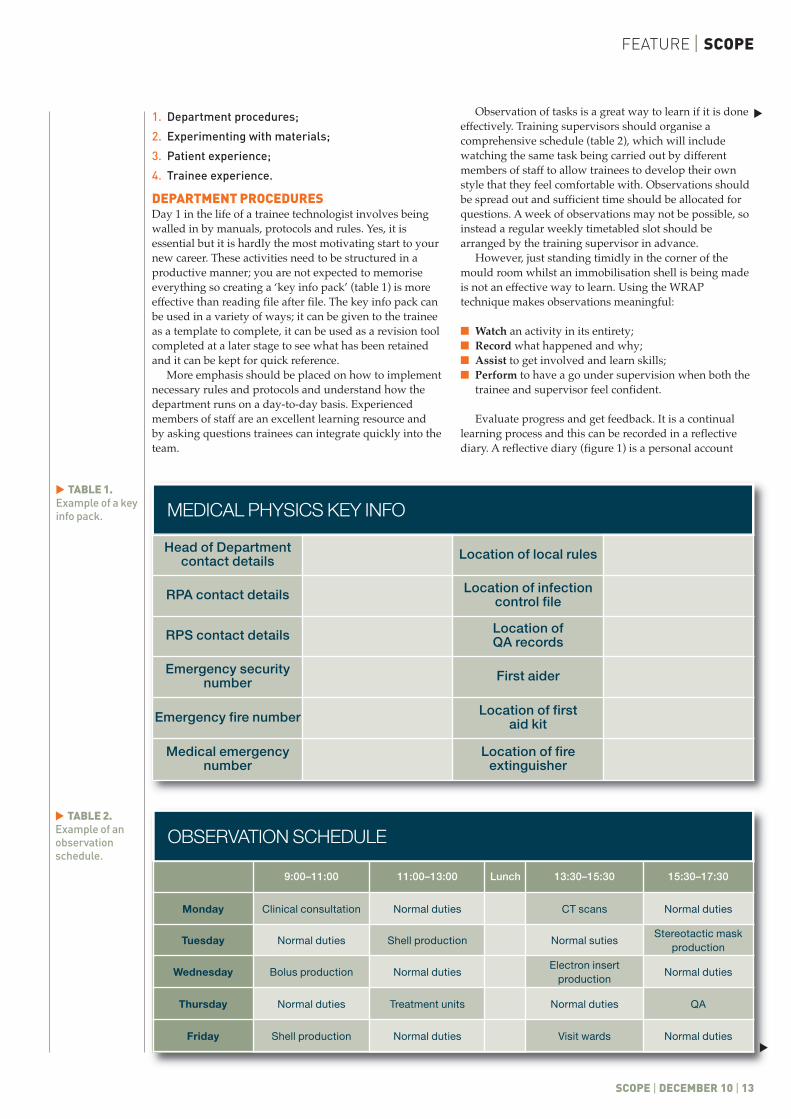
OBSERVATION SCHEDULE
9:00–11:00 11:00–13:00 Lunch 13:30–15:30 15:30–17:30
Monday Clinical consultation Normal duties CT scans Normal duties
Tuesday Normal duties Shell production Normal sutiesStereotactic mask
production
Wednesday Bolus production Normal dutiesElectron insert
productionNormal duties
Thursday Normal duties Treatment units Normal duties QA
Friday Shell production Normal duties Visit wards Normal duties
MEDICAL PHYSICS KEY INFO
Head of Departmentcontact details Location of local rules
RPA contact details Location of infectioncontrol file
RPS contact details Location of QA records
Emergency securitynumber First aider
Emergency fire number Location of first aid kit
Medical emergencynumber
Location of fireextinguisher
1. Department procedures;
2. Experimenting with materials;
3. Patient experience;
4. Trainee experience.
DEPARTMENT PROCEDURESDay 1 in the life of a trainee technologist involves beingwalled in by manuals, protocols and rules. Yes, it isessential but it is hardly the most motivating start to yournew career. These activities need to be structured in aproductive manner; you are not expected to memoriseeverything so creating a ‘key info pack’ (table 1) is moreeffective than reading file after file. The key info pack canbe used in a variety of ways; it can be given to the traineeas a template to complete, it can be used as a revision toolcompleted at a later stage to see what has been retainedand it can be kept for quick reference.
More emphasis should be placed on how to implementnecessary rules and protocols and understand how thedepartment runs on a day-to-day basis. Experiencedmembers of staff are an excellent learning resource andby asking questions trainees can integrate quickly into theteam.
Observation of tasks is a great way to learn if it is doneeffectively. Training supervisors should organise acomprehensive schedule (table 2), which will includewatching the same task being carried out by differentmembers of staff to allow trainees to develop their ownstyle that they feel comfortable with. Observations shouldbe spread out and sufficient time should be allocated forquestions. A week of observations may not be possible, soinstead a regular weekly timetabled slot should bearranged by the training supervisor in advance.
However, just standing timidly in the corner of themould room whilst an immobilisation shell is being madeis not an effective way to learn. Using the WRAPtechnique makes observations meaningful:
� Watch an activity in its entirety; � Record what happened and why;� Assist to get involved and learn skills;� Perform to have a go under supervision when both the
trainee and supervisor feel confident.
Evaluate progress and get feedback. It is a continuallearning process and this can be recorded in a reflectivediary. A reflective diary (figure 1) is a personal account
TABLE 1.Example of a keyinfo pack.
�
TABLE 2.Example of anobservationschedule.
�
��
SCOPE | FEATURE
14 | DECEMBER 10 | SCOPE
and not a technical step-by-step guide; it should focus onhow you felt, and be honest as it will show how you havedeveloped. Entries can be scored or colour-coded so thatprogress can be identified quickly.
EXPERIMENTING WITH MATERIALSThe mould room can be a daunting place for a trainee, withso many things you can spill or break and the addedpressure of dealing with a real-life patient. Being able topractice and become familiar with the properties ofdifferent materials removes some of this pressure.
Mistakes are an essential part of learning, as long as theyare allowed to happen away from patients. Being able todeal with unexpected events is a desirable skill which willbe developed over time. Control experiments with smallamounts of material help trainees understand how tomanage the materials. The knowledge of how differentmaterials respond allows trainees to develop their ownstyle. For example, what happens if cold water is added toalginate? What happens if hot water is added? Individualswill prefer different techniques but the aim is to apply itsafely to the patient without half of it ending up on thefloor. It is true that practice makes perfect, so get stuck inand make some mess!
PATIENT EXPERIENCEAs healthcare professionals it is our responsibility to makesure that patients are comfortable both physically andmentally. When patients arrive for a mould roomappointment they often have many preconceptions andfear of the unknown. If trainees understand the patientpathway and know how they have ended up in the mouldroom it will help you to pre-empt any questions. Byexperiencing the techniques first hand you will be able toempathise with the patients, so volunteer to be a dummyfor others to practice on you. Personally as a trainee I dreadthe thought of being asked a question which I can’t answer.Ask colleagues what type of questions they get asked andhow they respond, practice to help you think on the spotand if you don’t know the answer know-how can help.
TRAINEEEXPERIENCEIt is quite easy fortrainees to feelinvisible or a bitof a spare part,but trainees must takeresponsibility for their ownlearning experience and beproactive. If you show willing and seek out opportunitiescolleagues will be more willing to help you succeed.There are fantastic things already in place (I mentionedright at the start of the article how much I got out ofattending the MPEC), so use the publications andwebsites and talk to other trainees and learn from eachother.
One of the tools I have found most useful in mytraining is having regular weekly progress meetings withmy training supervisor. This is a guaranteed timetabledslot which allows me to air any concerns and get feedbackon my progress. It also makes the training moremanageable as competencies are broken down intoweekly targets and it means that my training is tailored tomy personal needs.
SUMMARYThere are lots of simple, practical activities which canhelp boost trainees’ confidence (table 3). Given the rightknowledge and skills a successful trainee technologistwill emerge, as a result of a partnership between traineeand training supervisor.
CONCLUSIONA successful training programme must provide all of therelevant information and develop skills. Therefore, thereneeds to be a balance between academic theory andpractical experience. Confidence is derived from practice.Trainee technologists are missing a trick if they don’tmake the most of the infrastructure in place – so come ontechies, get involved! �
FIGURE 1.Examples ofreflective diaryaccounts.
�
TABLE 3.Activities to helplearn.
�
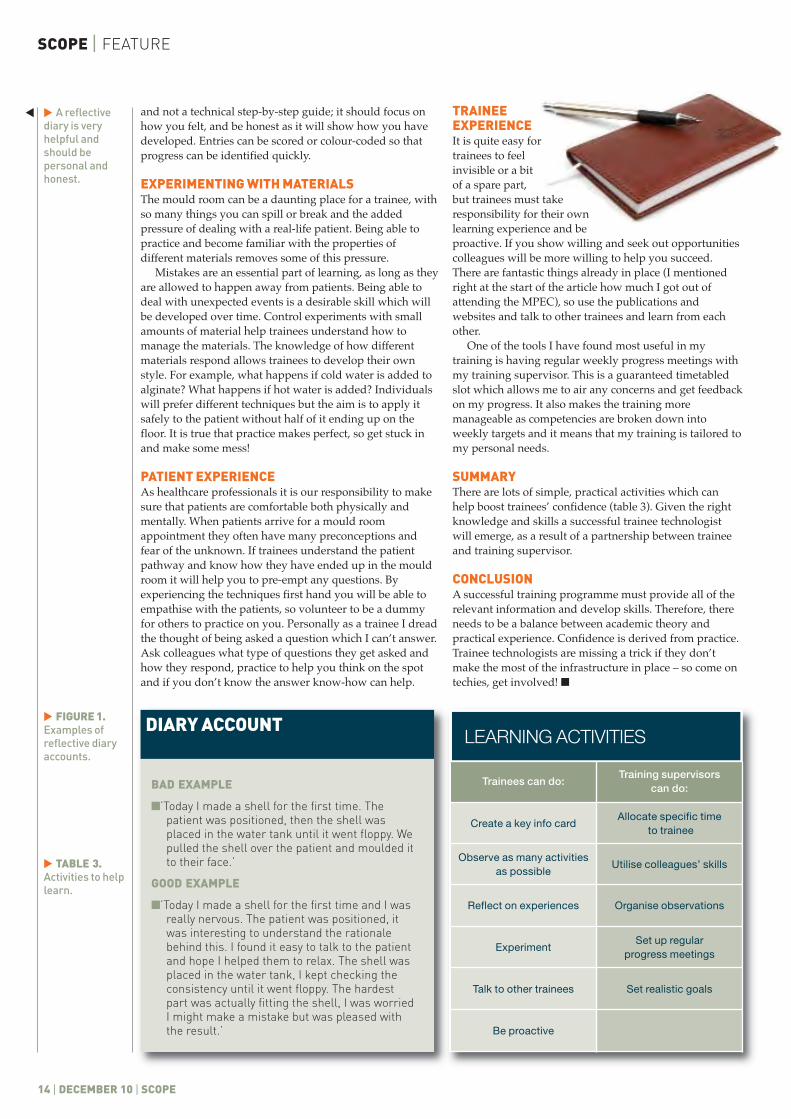
LEARNING ACTIVITIES
Trainees can do:Training supervisors
can do:
Create a key info cardAllocate specific time
to trainee
Observe as many activitiesas possible
Utilise colleagues’ skills
Reflect on experiences Organise observations
ExperimentSet up regular
progress meetings
Talk to other trainees Set realistic goals
Be proactive
DIARY ACCOUNT
BAD EXAMPLE
�’Today I made a shell for the first time. Thepatient was positioned, then the shell wasplaced in the water tank until it went floppy. Wepulled the shell over the patient and moulded itto their face.’
GOOD EXAMPLE
�’Today I made a shell for the first time and I wasreally nervous. The patient was positioned, itwas interesting to understand the rationalebehind this. I found it easy to talk to the patientand hope I helped them to relax. The shell wasplaced in the water tank, I kept checking theconsistency until it went floppy. The hardestpart was actually fitting the shell, I was worriedI might make a mistake but was pleased withthe result.’
A reflectivediary is veryhelpful andshould bepersonal andhonest.
�
�

SCOPE | DECEMBER 10 | 15
SCOPE | FEATURE
16 | DECEMBER 2010 | SCOPE
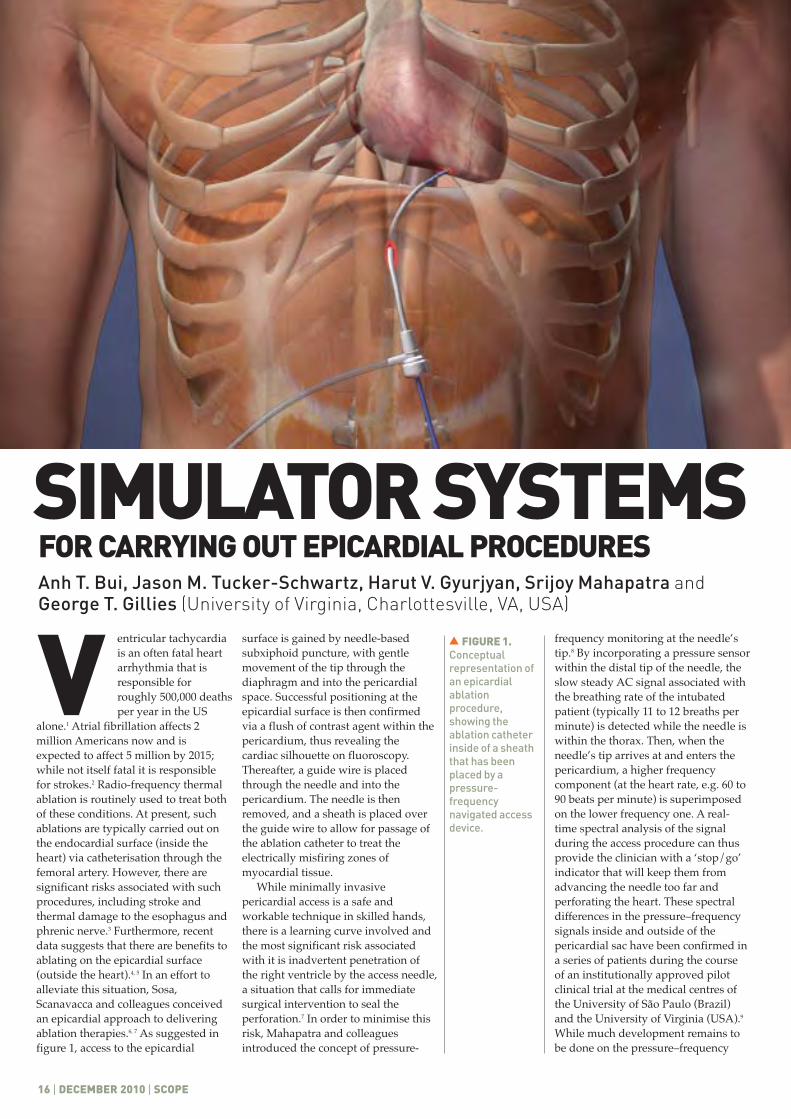
entricular tachycardiais an often fatal heartarrhythmia that isresponsible forroughly 500,000 deathsper year in the US
alone.1 Atrial fibrillation affects 2million Americans now and isexpected to affect 5 million by 2015;while not itself fatal it is responsiblefor strokes.2 Radio-frequency thermalablation is routinely used to treat bothof these conditions. At present, suchablations are typically carried out onthe endocardial surface (inside theheart) via catheterisation through thefemoral artery. However, there aresignificant risks associated with suchprocedures, including stroke andthermal damage to the esophagus andphrenic nerve.3 Furthermore, recentdata suggests that there are benefits toablating on the epicardial surface(outside the heart).4, 5 In an effort toalleviate this situation, Sosa,Scanavacca and colleagues conceivedan epicardial approach to deliveringablation therapies.6, 7 As suggested infigure 1, access to the epicardial
surface is gained by needle-basedsubxiphoid puncture, with gentlemovement of the tip through thediaphragm and into the pericardialspace. Successful positioning at theepicardial surface is then confirmedvia a flush of contrast agent within thepericardium, thus revealing thecardiac silhouette on fluoroscopy.Thereafter, a guide wire is placedthrough the needle and into thepericardium. The needle is thenremoved, and a sheath is placed overthe guide wire to allow for passage ofthe ablation catheter to treat theelectrically misfiring zones ofmyocardial tissue.
While minimally invasivepericardial access is a safe andworkable technique in skilled hands,there is a learning curve involved andthe most significant risk associatedwith it is inadvertent penetration ofthe right ventricle by the access needle,a situation that calls for immediatesurgical intervention to seal theperforation.7 In order to minimise thisrisk, Mahapatra and colleaguesintroduced the concept of pressure-
frequency monitoring at the needle’stip.8 By incorporating a pressure sensorwithin the distal tip of the needle, theslow steady AC signal associated withthe breathing rate of the intubatedpatient (typically 11 to 12 breaths perminute) is detected while the needle iswithin the thorax. Then, when theneedle’s tip arrives at and enters thepericardium, a higher frequencycomponent (at the heart rate, e.g. 60 to90 beats per minute) is superimposedon the lower frequency one. A real-time spectral analysis of the signalduring the access procedure can thusprovide the clinician with a ‘stop/go’indicator that will keep them fromadvancing the needle too far andperforating the heart. These spectraldifferences in the pressure–frequencysignals inside and outside of thepericardial sac have been confirmed ina series of patients during the courseof an institutionally approved pilotclinical trial at the medical centres ofthe University of São Paulo (Brazil)and the University of Virginia (USA).9
While much development remains tobe done on the pressure–frequency
Anh T. Bui, Jason M. Tucker-Schwartz, Harut V. Gyurjyan, Srijoy Mahapatra andGeorge T. Gillies (University of Virginia, Charlottesville, VA, USA)
V
SIMULATOR SYSTEMSFOR CARRYING OUT EPICARDIAL PROCEDURES
FIGURE 1.Conceptualrepresentation ofan epicardialablationprocedure,showing theablation catheterinside of a sheaththat has beenplaced by apressure-frequencynavigated accessdevice.
�

FEATURE | SCOPE
SCOPE | DECEMBER 2010 | 17
technique for subxiphoid access, themethod at present holds the promiseof replacing the existing qualitativeapproach to needle navigation with adecidedly quantitative one, thusmaking it possible forelectrophysiologists to do thisprocedure routinely in the clinicalelectrophysiology (EP) lab.
In order to minimise the need forand costs of in vivo experimentationto test access needle prototypes,validate pressure–frequency analysisalgorithms and train physicians inthis approach, we are developinganthropomorphic simulators forepicardial procedures. Althoughthere are a wide variety ofmannequin-type simulators used inmedical education and trainingprogrammes today10, 11, 12 none of themare optimised for the practice ofaccess techniques for epicardialprocedures.
THE FIRST PROTOTYPEEPICARDIAL SIMULATORThe earliest, bench-top version of oursystem is shown in figure 2. It wasdesigned to the scale of an adulthuman chest, and incorporated twomoulded balloons that served as air-inflated lungs and a moulded water-pumped heart. The lungs werepumped by a stepper motor-drivenbellows, so that the breathing rateand type of inhalation waveformsused in cardiac anaesthesiology couldbe mimicked. In this exploratoryversion of the system, the heart pumpwas driven at a constant rate of onebeat per minute by a high-torque gearmotor. The heart was surrounded bya thin-walled rubber balloon tosimulate the pericardial sac, and theresulting very narrow gap betweenthe outer wall of the moulded heartand the inner surface of thepericardial balloon was filled withwater. (This approach provided onlya rough approximation of thephysiological characteristics of theparietal pericardium, but our intentin this first prototype was only todemonstrate feasibility withoutseeking to mimic all of the differenttissue parameters.) Access procedurescould be practiced by passing apressure-sensing needle through thelatex ‘skin’ of the mannequin’ssubxiphoid region, then through alayer of moulded rubber that servedas a surrogate for the diaphragm, andfinally into the pericardium. Thechest cavity was sealed and the
FIGURE 2. Photograph of the original prototype of the epicardial simulator as positioned on amobile cart and including the host computer.
�
FIGURE 3. An exploded view of some of the components of the improved epicardial simulator. Thechest containment box is on the left, housing the lungs and the heart mould. The covering mannequinis in the middle along with the moulded heart. The heart replica used to create the pericardial sac is onthe right. Also shown there is one of the stepping motors used to drive the simulator’s pumps.
�
�
SCOPE | FEATURE
18 | DECEMBER 2010 | SCOPE
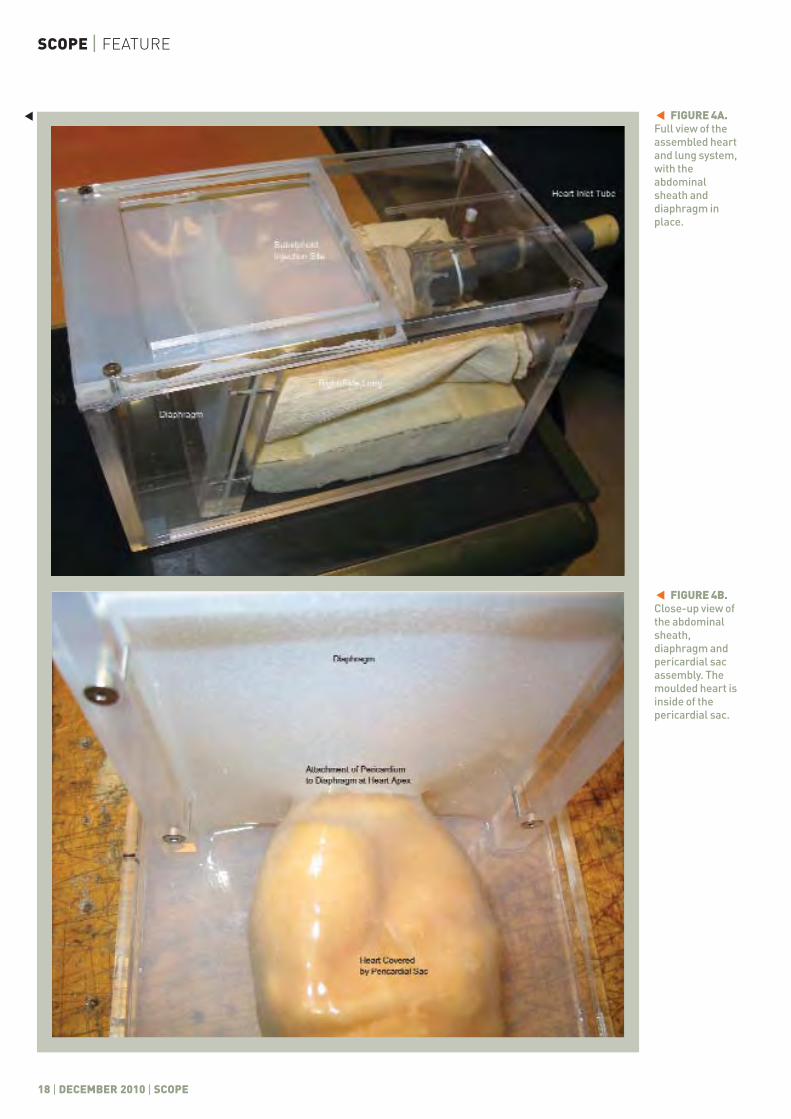
FIGURE 4B.Close-up view ofthe abdominalsheath,diaphragm andpericardial sacassembly. Themoulded heart isinside of thepericardial sac.
�
FIGURE 4A.Full view of theassembled heartand lung system,with theabdominalsheath anddiaphragm inplace.
��

slightly smaller heart volume, weconserved materials but still kept theheart size large enough to be a verysatisfactory training tool.) The actualmoulded heart itself is shown forscale relative to the Lucite®mannequin, which could be placedon top of the chest container duringuse. Also shown in the figure, to theright of the mannequin, is a secondreplica of a heart, created via rapidprototyping from an open-sourceSolidWorks™ (Dassault Systems,Vélizy-Villacoublay, France) design.This second replica was slightlyoversized compared to the one in thechest case, so that when a thin layerof Dragon Skin® silicone rubber(Easton, Pennsylvania, USA) was caston it the resulting pericardium couldbe slipped over the latex-mouldedheart without tearing. (Dragon Skin®is used routinely in industry tosimulate biological tissues.) Thecompliance of this surrogatepericardial sac allowed for the virtualspace between it and the outer wall ofthe heart to be converted to an actualphysical space by the injection ofwater to mimic the pericardial fluid.Also shown in figure 3 is one of thestepping motors used in thesimulator. In this improved version ofthe system, both the heart and lungpumps were driven by computer-controlled stepping motors. Thisallowed us to not only simulate anyanaesthesia waveforms that might beneeded, but also to simulate variableheart rates and arrhythmias.Moreover, any given heart or lungpumping profile could thus be easilydocumented, archived and repeatedas necessary for practice purposes. Inan interesting change relative to ourfirst system, the lungs were nowwater pumped and the heart was airpumped. This was carried outbecause the breathing component ofthe pressure wave in the surrogatepericardial space produced by thenow smaller lungs was significantlyless than that due to the relativelyheavy water-pumped heart.Therefore, switching to a lighter air-pumped heart and to higher-inertiawater-pumped lungs ensured that amore physiological ratio of thesepressure components was obtained.
There are several novel featuresincorporated into the redesignedsystem. In figure 4a, a full view of theassembled chest box is shown. A 1 cmthick layer of Dragon Skin® siliconerubber functions as the abdominal
skin and muscle sheath of the model.Another such layer of the rubberserves as the diaphragm. The twolayers are bonded together to form a‘T’ shape, as shown in the figure. Bothbranches of this ‘T’ are fixed onto thechest box by Lucite® frames, and thejoints are made leak-free with siliconesealant. The surface area of thesubxiphoid injection site is largeenough to permit a grazing-incidenceapproach to the right ventricle of themodel heart, in imitation of the actualclinical access procedure. Uponinflation, the lungs expand within thechest cavity, thus applying cyclicalpressure to the pericardium anddiaphragm. Figure 4b shows furtherdetails of this arrangement. As shownthere, the frames holding thediaphragm and subxiphoid injectionsite have been removed from thechest cavity and placed upside downonto a table to reveal the internalstructures. The interesting things tonote are the close, full-organ fit of thepericardial sac to the heart and theattachment of the pericardium to thediaphragm at the apex of the heart.The close fit of the pericardium ismeant to provide the trainee with arealistic clinical test, such asattempting to snag the thinpericardial membrane at grazingincidence (in order to minimise therisk of perforating the heart) with andwithout pressure–frequency guidanceduring the training session. By usingtransparent Lucite® as theconstruction material for thesimulator’s chest the trainee can dothe procedure with and withoutvisual feedback (i.e. with and withoutthe mannequin draped) in order topractice the procedure moreeffectively. The attachment of thepericardium to the diaphragm at theapex of the heart provides a keymeasure of physiological fidelity byhelping to hold the heart in placewithin the chest while the lungs workagainst it during inhalation, thusensuring that the mock pericardialfluid is hydrodynamically influencedby the pumping of both the heart andthe lungs. Perhaps most significantly,since the abdominal muscle sheath,diaphragm and pericardial sacsurrogates are all bonded together toform one continuous unit, it is easy toconceive this assembly being madeavailable as a single integratedreplacement part from amanufacturer marketing it. This is animportant point, since this assembly
thoracic pressure was monitored by astrain gauge sensor. A laboratorycomputer was used to acquire thethoracic pressures and thepressure–frequency signals in theaccess needle (the latter as in theclinical case). The inspiration andexpiration of the lungs not onlymimicked the intubated state of ananaesthetised patient, but alsoattempted to replicate the lifting forceapplied to the heart during thebreathing cycle. As described in ourpaper on the subject in the Journal ofMedical Engineering & Technology,13
this system allowed us todemonstrate the feasibility ofassembling and operating anepicardial access simulator, to thepoint where we were able to generatepressure–frequency signals in thesurrogate pericardial space that weresimilar to those found in the humanbody.9 Through extensive testing, weclarified a number of design andperformance parameters that haveenabled us to develop an improvedversion that brings us closer to thegoal of commissioning such a systemfor use in clinical trainingprogrammes.
AN IMPROVED EPICARDIALSIMULATORAn exploded view of the centralfeatures of the new apparatus thathas evolved from the originalsimulator is shown in figure 3. In anactual training exercise, the overlyingmannequin would be covered with asurgical drape to simulate thepatient’s situation in the EP lab. As aresult, the model chest and most of itsinternal components need only beanthropomorphic in function and notnecessarily in form. In practice, thismeant that we were able to redesignthe chest and its contents and makeeverything more modular for ease ofassembly and use. The centralelements of the redesigned system areshown left-to-right in figure 3. ALucite® chest box of 16.5 × 16.5 × 30cm served to hold the two latex-moulded lungs that had a combinedvolume of 1020 cm3. The heart seenresting on the lungs in figure 3 was anear life-like replica (Model CH7,Anatomical Chart Co., Hagerstown,MD, USA), upon which the latex-moulded model heart was cast. (Therelaxed-state volume of the mouldedheart is 220 cm3, which is about 20 percent less than the average adult heartvolume of 280 cm3. By employing a
Theoverlyingmannequinwould becoveredwith asurgicaldrape tosimulatethepatient’ssituation
“
”
SCOPE | DECEMBER 2010 | 19
FEATURE | SCOPE
�
SCOPE | FEATURE
20 | DECEMBER 2010 | SCOPE
of moulded parts will eventuallyrequire either repair or replacementafter a sufficiently large number ofpractice access procedures have beenperformed on it.
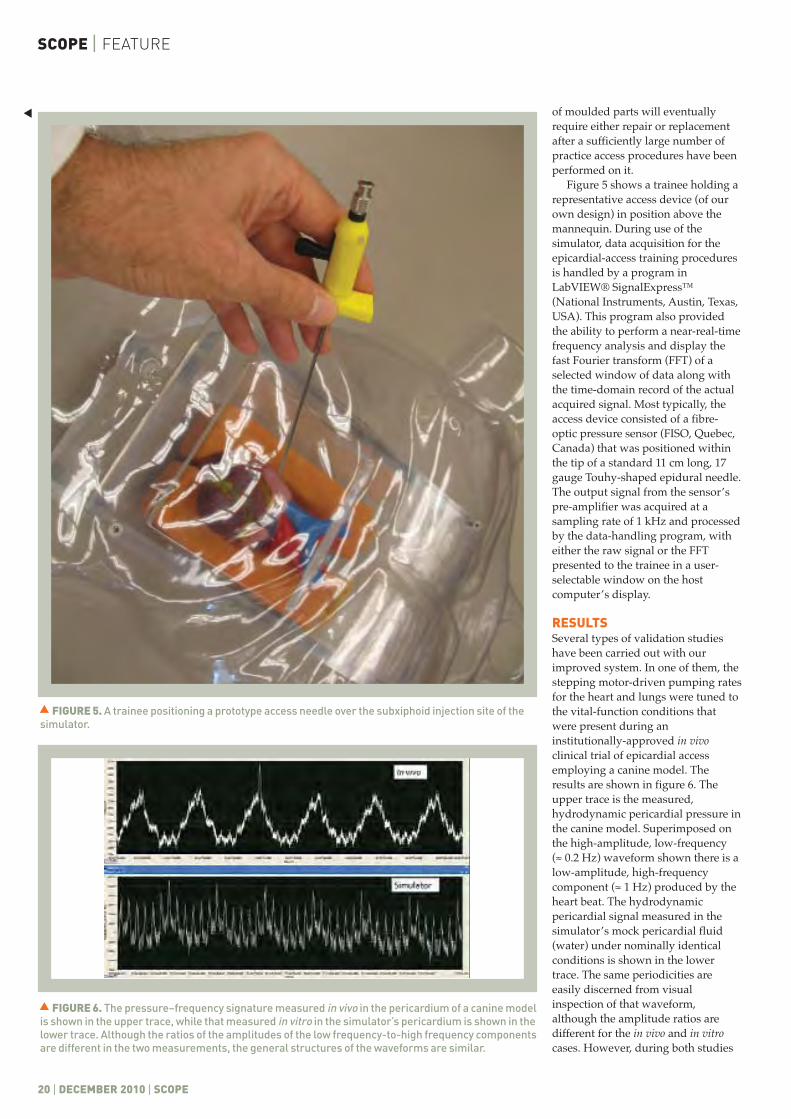
Figure 5 shows a trainee holding arepresentative access device (of ourown design) in position above themannequin. During use of thesimulator, data acquisition for theepicardial-access training proceduresis handled by a program inLabVIEW® SignalExpress™(National Instruments, Austin, Texas,USA). This program also providedthe ability to perform a near-real-timefrequency analysis and display thefast Fourier transform (FFT) of aselected window of data along withthe time-domain record of the actualacquired signal. Most typically, theaccess device consisted of a fibre-optic pressure sensor (FISO, Quebec,Canada) that was positioned withinthe tip of a standard 11 cm long, 17gauge Touhy-shaped epidural needle.The output signal from the sensor’spre-amplifier was acquired at asampling rate of 1 kHz and processedby the data-handling program, witheither the raw signal or the FFTpresented to the trainee in a user-selectable window on the hostcomputer’s display.
RESULTSSeveral types of validation studieshave been carried out with ourimproved system. In one of them, thestepping motor-driven pumping ratesfor the heart and lungs were tuned tothe vital-function conditions thatwere present during aninstitutionally-approved in vivoclinical trial of epicardial accessemploying a canine model. Theresults are shown in figure 6. Theupper trace is the measured,hydrodynamic pericardial pressure inthe canine model. Superimposed onthe high-amplitude, low-frequency (≈ 0.2 Hz) waveform shown there is alow-amplitude, high-frequencycomponent (≈ 1 Hz) produced by theheart beat. The hydrodynamicpericardial signal measured in thesimulator’s mock pericardial fluid(water) under nominally identicalconditions is shown in the lowertrace. The same periodicities areeasily discerned from visualinspection of that waveform,although the amplitude ratios aredifferent for the in vivo and in vitrocases. However, during both studies
�
FIGURE 5. A trainee positioning a prototype access needle over the subxiphoid injection site of thesimulator.
�
FIGURE 6. The pressure–frequency signature measured in vivo in the pericardium of a canine modelis shown in the upper trace, while that measured in vitro in the simulator’s pericardium is shown in thelower trace. Although the ratios of the amplitudes of the low frequency-to-high frequency componentsare different in the two measurements, the general structures of the waveforms are similar.
�
we noted that the cardiac componentof the waveform was not presenteither before the tip of the accessneedle had initially entered thepericardium or after it had beenwithdrawn from the pericardial sac,thus confirming the simulator’sability to credibly represent theclinical situation. Some further detailsof our design, construction andtesting efforts are presentedelsewhere.14
DIRECTIONS OF FUTURE WORKFrom the engineer’s perspective, oneis always either tempted orchallenged to incorporate additionalrefinements and improvements intosuch a system, in order to make itever more lifelike (albeit at theexpense of further complexity). Forinstance, it would not beunreasonable to introduce a versionof the system in which the pericardialsac was fixed to the moulded heart atseveral locations. This wouldreplicate the effect of post-surgicaladhesions, which in practice reducethe amount of fluid in the pericardialspace and thus decrease the strengthof the associated pressure–frequency
signal. Furthermore, these patientspresent the highest risk accessprocedures,9 hence focussed trainingon this problem would be beneficial. Itwould also be possible to introduce amotional artifact in the mannequinitself, to mimic the movement of thechest walls during the respirationcycle. Lastly, a significant materials-related improvement would beachieved through the use of asubstance that was more fully self-healing than the silicone rubberpresently employed for the abdominalsheath, diaphragm and pericardial sacassembly. Even when using very smallgauge needles in the access device,that assembly eventually developspericardial fluid leaks that are largeenough to require either manualsealing of the penetration holes orreplacement of it altogether.
We envisage using this system notonly as a training tool forelectrophysiologists interested indoing epicardial procedures, but alsoas a research tool for testing newepicardial technologies. For instance,the existing endocardial ablationcatheters are not properly configuredfor epicardial use. In particular they
have the lengths and curvaturesinappropriate for epicardialapplications. The simulator couldserve as a useful intermediate tool fortesting specially designed epicardialablation catheters and optimisingtheir construction and performanceprior to undertaking costly in vivotrials for clinical commissioning. Asimilar situation holds for the testingof custom-designed epicardial pacingleads as well. �
SCOPE | DECEMBER 2010 | 21
ACKNOWLEDGMENTSWe thank Ms Pamela Bunes, President,EpiEP, Inc., for permission to use figure1. We thank Mr Sammy Peppers and MrDan Hendrickson of Medical SimulationCorporation for several usefuldiscussions and for advice on technicalissues and details of construction of thesimulator systems. Mr B. H. Kent of theMachine Shop of the University ofVirginia’s Department of Physicsconstructed several of the criticalcomponents. This work has been fundedin part by the University of Virginia PatentFoundation Royalty Distribution Programand by EpiEP, Inc.The University ofVirginia Patent Foundation has licensedthe intellectual property for thesimulator systems to EpiEP, Inc. forcommercial development. The authorsare equity shareholders in EpiEP, Inc.and will also receive royalties from theUniversity of Virginia Patent Foundation.
REFERENCES
1 Uyguanco ER et al. Management of high defibrillationthreshold. Expert Rev Cardiovasc Ther 2008; 6: 1237–48.
2 Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as anindependent risk factor for stroke: the Framingham study.Stroke 1991; 22: 983–8.
3 Aupperle H et al. Ablation of atrial fibrillation andesophageal injury: effects of energy source and ablationtechnique. J Thorac Cardiov Sur 2005; 130: 1549–54.
4 Pak HN et al. Hybrid epicardial and endocardial ablation ofpersistent or permanent atrial fibrillation: a new approachfor difficult cases. J Cardiovasc Electr 2007; 18: 917–23.
5 Sacher FMP et al. Prevalence of epicardial scar in patientsreferred for ventricular tachycardia ablation. Heart Rhythm2009; 9: S175.
6 Sosa E et al. Endocardial and epicardial ablation guided bynonsurgical transthoracic epicardial mapping to treatrecurrent ventricular tachycardia. J Cardiovasc Electr 1998;9: 229–39.
7 Sosa E et al. Nonsurgical transthoracic epicardial catheterablation to treat recurrent ventricular tachycardiaoccurring late after myocardial infarction. J Am CollCardiol 2000; 35: 1442–9.
8 Tucker-Schwartz J et al. Pressure–frequency sensingsubxiphoid access system for use in percutaneous cardiacelectrophysiology: prototype design and pilot study results.IEEE T Bio-med Eng 2009; 56: 1160–8.
9 Mahapatra S et al. Pressure frequency characteristics ofthe pericardial space and thorax during subxiphoid accessfor epicardial ventricular tachycardia ablation. HeartRhythm 2010; 7: 604–9.
10 Bradley, P. The history of simulation in medical educationand possible future directions. Med Educ 2006; 40: 254–62.
11Cooper JB, Taqueti VR. A brief history of the developmentof mannequin simulators for clinical education andtraining. Postgrad Med J 2008; 84: 563–70.
12 Rosen KR. The history of medical simulation. J Crit Care2008; 23: 157–66.
13 Gyurjyan HV et al. Anthropomorphic simulator forminimally invasive epicardial access procedures. J Med EngTechnol 2010; 34; 134–40.
14 Bui AT. An Improved Simulator for Epicardial AccessProcedure. BSc Thesis, School of Engineering and AppliedScience, University of Virginia, 2010.
Thesimulatorcouldserve as auseful toolfor testingspeciallydesignedepicardialablationcatheters
“
”
FEATURE | SCOPE
22 | DECEMBER 10 | SCOPE
FEATURE | SCOPE
Byswappingto door 2,youactuallydoubleyourchances ofwinning
“
”
he world of statistics is full of paradoxeswhich have generated a lot of interest anddebate for many years.1 One of the mainthemes that these paradoxes take arerelated to the topic of probability and, morespecifically, conditional probability. These
paradoxes demonstrate quirks which have significantimplications on data analysis in research. The literature isfull of examples were researchers fell foul of the pitfallsthat these p aradoxes illustrate. Ben Goldacre’s BadScience book2 is an excellent reference highlighting howsuch pitfalls can lead to wrong, or simply dubious,conclusions. I have picked out a few examples herewhich make excellent party material for sad physicistsand engineers like myself (I am available for weddings,christenings and other occasions). I have linked theseexamples to some real-world medical applications.
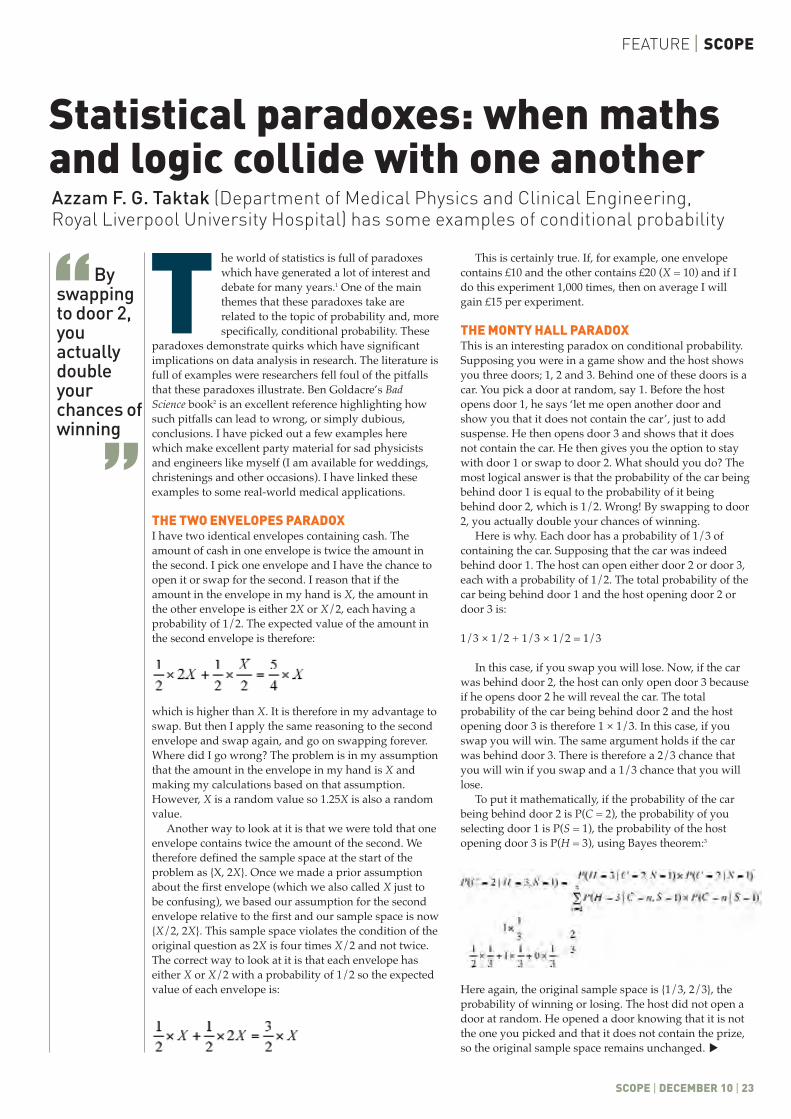
THE TWO ENVELOPES PARADOXI have two identical envelopes containing cash. Theamount of cash in one envelope is twice the amount inthe second. I pick one envelope and I have the chance toopen it or swap for the second. I reason that if theamount in the envelope in my hand is X, the amount inthe other envelope is either 2X or X/2, each having aprobability of 1/2. The expected value of the amount inthe second envelope is therefore:
which is higher than X. It is therefore in my advantage toswap. But then I apply the same reasoning to the secondenvelope and swap again, and go on swapping forever.Where did I go wrong? The problem is in my assumptionthat the amount in the envelope in my hand is X andmaking my calculations based on that assumption.However, X is a random value so 1.25X is also a randomvalue.
Another way to look at it is that we were told that oneenvelope contains twice the amount of the second. Wetherefore defined the sample space at the start of theproblem as {X, 2X}. Once we made a prior assumptionabout the first envelope (which we also called X just tobe confusing), we based our assumption for the secondenvelope relative to the first and our sample space is now{X/2, 2X}. This sample space violates the condition of theoriginal question as 2X is four times X/2 and not twice.The correct way to look at it is that each envelope haseither X or X/2 with a probability of 1/2 so the expectedvalue of each envelope is:
This is certainly true. If, for example, one envelopecontains £10 and the other contains £20 (X = 10) and if Ido this experiment 1,000 times, then on average I willgain £15 per experiment.
THE MONTY HALL PARADOXThis is an interesting paradox on conditional probability.Supposing you were in a game show and the host showsyou three doors; 1, 2 and 3. Behind one of these doors is acar. You pick a door at random, say 1. Before the hostopens door 1, he says ‘let me open another door andshow you that it does not contain the car’, just to addsuspense. He then opens door 3 and shows that it doesnot contain the car. He then gives you the option to staywith door 1 or swap to door 2. What should you do? Themost logical answer is that the probability of the car beingbehind door 1 is equal to the probability of it beingbehind door 2, which is 1/2. Wrong! By swapping to door2, you actually double your chances of winning.
Here is why. Each door has a probability of 1/3 ofcontaining the car. Supposing that the car was indeedbehind door 1. The host can open either door 2 or door 3,each with a probability of 1/2. The total probability of thecar being behind door 1 and the host opening door 2 ordoor 3 is:
1/3 × 1/2 + 1/3 × 1/2 = 1/3
In this case, if you swap you will lose. Now, if the carwas behind door 2, the host can only open door 3 becauseif he opens door 2 he will reveal the car. The totalprobability of the car being behind door 2 and the hostopening door 3 is therefore 1 × 1/3. In this case, if youswap you will win. The same argument holds if the carwas behind door 3. There is therefore a 2/3 chance thatyou will win if you swap and a 1/3 chance that you willlose.
To put it mathematically, if the probability of the carbeing behind door 2 is P(C = 2), the probability of youselecting door 1 is P(S = 1), the probability of the hostopening door 3 is P(H = 3), using Bayes theorem:3
Here again, the original sample space is {1/3, 2/3}, theprobability of winning or losing. The host did not open adoor at random. He opened a door knowing that it is notthe one you picked and that it does not contain the prize,so the original sample space remains unchanged.
Azzam F. G. Taktak (Department of Medical Physics and Clinical Engineering,Royal Liverpool University Hospital) has some examples of conditional probability
T
Statistical paradoxes: when mathsand logic collide with one another
SCOPE | DECEMBER 10 | 23
�
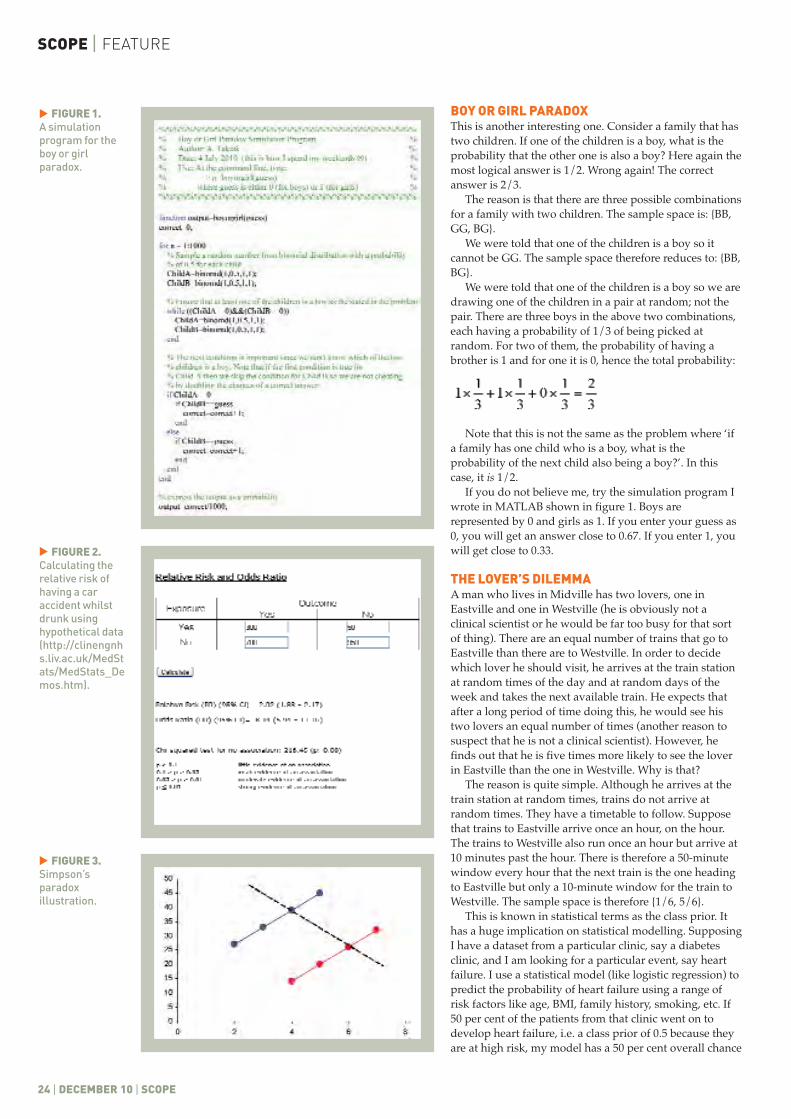
BOY OR GIRL PARADOXThis is another interesting one. Consider a family that hastwo children. If one of the children is a boy, what is theprobability that the other one is also a boy? Here again themost logical answer is 1/2. Wrong again! The correctanswer is 2/3.
The reason is that there are three possible combinationsfor a family with two children. The sample space is: {BB,GG, BG}.
We were told that one of the children is a boy so itcannot be GG. The sample space therefore reduces to: {BB,BG}.
We were told that one of the children is a boy so we aredrawing one of the children in a pair at random; not thepair. There are three boys in the above two combinations,each having a probability of 1/3 of being picked atrandom. For two of them, the probability of having abrother is 1 and for one it is 0, hence the total probability:
Note that this is not the same as the problem where ‘ifa family has one child who is a boy, what is theprobability of the next child also being a boy?’. In thiscase, it is 1/2.
If you do not believe me, try the simulation program Iwrote in MATLAB shown in figure 1. Boys arerepresented by 0 and girls as 1. If you enter your guess as0, you will get an answer close to 0.67. If you enter 1, youwill get close to 0.33.
THE LOVER’S DILEMMA A man who lives in Midville has two lovers, one inEastville and one in Westville (he is obviously not aclinical scientist or he would be far too busy for that sortof thing). There are an equal number of trains that go toEastville than there are to Westville. In order to decidewhich lover he should visit, he arrives at the train stationat random times of the day and at random days of theweek and takes the next available train. He expects thatafter a long period of time doing this, he would see histwo lovers an equal number of times (another reason tosuspect that he is not a clinical scientist). However, hefinds out that he is five times more likely to see the loverin Eastville than the one in Westville. Why is that?
The reason is quite simple. Although he arrives at thetrain station at random times, trains do not arrive atrandom times. They have a timetable to follow. Supposethat trains to Eastville arrive once an hour, on the hour.The trains to Westville also run once an hour but arrive at10 minutes past the hour. There is therefore a 50-minutewindow every hour that the next train is the one headingto Eastville but only a 10-minute window for the train toWestville. The sample space is therefore {1/6, 5/6}.
This is known in statistical terms as the class prior. Ithas a huge implication on statistical modelling. SupposingI have a dataset from a particular clinic, say a diabetesclinic, and I am looking for a particular event, say heartfailure. I use a statistical model (like logistic regression) topredict the probability of heart failure using a range ofrisk factors like age, BMI, family history, smoking, etc. If50 per cent of the patients from that clinic went on todevelop heart failure, i.e. a class prior of 0.5 because theyare at high risk, my model has a 50 per cent overall chance
SCOPE | FEATURE
24 | DECEMBER 10 | SCOPE
FIGURE 1.A simulationprogram for theboy or girlparadox.
FIGURE 2.Calculating therelative risk ofhaving a caraccident whilstdrunk usinghypothetical data(http://clinengnhs.liv.ac.uk/MedStats/MedStats_Demos.htm).
��
FIGURE 3.Simpson’sparadoxillustration.
�

of predicting heart failure. It would be wrong of me thento use the same model on a random person off the streetsince the class prior for the general public (also knownas prevalence) is a lot less than 0.5.
A TOMMY COOPER JOKELast Christmas, I got a Tommy Cooper joke book frommy wife which I thoroughly enjoyed. One joke ofparticular relevance to the topic here is as follows. It issaid that three out of every ten car accidents are causedby drunk drivers. That means that seven out of ten arecaused by sober drivers so if everyone gets drunk, therewould be fewer car accidents. At the risk of killing thejoke, I will try to show the flaw in this argument.
If we represent the event of being drunk as D, theevent of being sober as S and the event of having a caraccident as A, then:
P(D|A) = 0.3P(S|A) = 0.7i.e. P(D|A) < P(S|A).
This is not the same as:
P(A|D) < P(A|S)
which is what the joke implies. This is known as thetransposition of conditioning fallacy. The only way totest the inequality is by doing a controlled trial wherewe choose 100 drunk drivers and 100 sober drivers,send them out on a long journey and see how many ofthem make it home safely. Clearly not feasible. The otheroption is to use observational data (more about this inthe next section). If we assume that the above statisticscame from a sample of 1,000 car accident records, wesend out anonymous questionnaires to 1,000 drivers atrandom who have not been involved in car accidentsand ask them if they have ever been under the influenceof alcohol whilst on the wheel. Suppose that 95 per centof respondents said no (I think it is safe to assume thatat least 95 per cent of drivers on the road are sober).That means the relative risk of having a car accidentwhilst drunk is about 2 (figure 2). That is, there is 100per cent more risk of being involved in a car accidentwhilst drunk than if you were sober. Sorry Mr Cooper!
SIMPSON’S PARADOXSimpson’s paradox is a phenomenon that occurs whenstudying correlation between two variables fromobservational data without taking the effect ofconfounders into consideration. Edward H. Simpsonfirst described this phenomenon in a technical paper in1951.4 This effect can be best illustrated in figure 3.Suppose variable Y has a positive linear relationshipwith variable X. The slope of the best fit line is constantbut the intercept depends on the level of a binaryvariable C so that when C = 0, the correlation isdescribed by the blue line and when it is 1, it isdescribed by the red line. Now if we did not take C intoaccount, we might do an experiment which results inthe dashed black line which has a negative slope so wemight wrongly conclude that X and Y have an inverserelationship.
In observational (non-randomised) studiescomparing treatments, it is likely that the initial choice
FEATURE | SCOPE
SCOPE | DECEMBER 10 | 25
REFERENCES
1 http://en.wikipedia.org/wiki/List_of_paradoxes
2 Goldacre B. Bad Science.London: Fourth Estate Ltd,2008.
3 Gill J. Bayesian Methods.Boca Raton, FL, USA: CRCPress, 2002.
4 Simpson EH. Theinterpretation of interaction incontingency tables. J R StatSoc B 1951; 13: 238–41.
5 Julious SA, Mullee MA.Confounding and Simpson'sparadox. Brit Med J 1994;309(6967): 1480–1.
6 Smith GC, Pell JP. Parachuteuse to prevent death andmajor trauma related togravitational challenge:systematic review ofrandomised controlled trials.Brit Med J 2003; 327(7429):1459–61.
of treatment would have been influenced by patients’characteristics such as age or severity of condition, soany difference between treatments could be accountedfor by these original factors. To take a real-worldexample, Charig et al. undertook a historicalcomparison of success rates in removing kidney stones.5
He showed that open surgery had a success rate of 78per cent (273/350) while keyhole surgery had a successrate of 83 per cent (289/350). The study concluded thatkeyhole surgery improves the chances of a successfuloutcome. However, when stone diameter was takeninto account, this showed that, for stones < 2 cmdiameter, 93 per cent (81/87) of cases with open surgerywere successful compared with just 87 per cent(234/270) of cases with keyhole surgery. One wouldnaturally assume that for larger stones, keyhole surgerymust perform much better than open surgery in orderto make up the difference. In fact it was observed thatfor stones of > 2 cm, success rates were 73 per cent(192/263) for open surgery and 69 per cent (55/80) forkeyhole surgery. The main reason that the success ratereversed is because the choice of surgery depends onthe diameter of the stones.
Although randomised-controlled trials are morescientifically rigorous than observational studies, it isnot always feasible to do randomised trials for a varietyof reasons. The section on alcohol and car accidentsabove is one example. Another ‘tongue-in-cheek’example is the use of a parachute as an intervention toprevent death or serious injury after jumping out of anaeroplane.6 The authors point out in a highly articulateand extremely witty way that we must not always jump(pun not intended) to conclusions when assessingevidence of interventions resulting from observationaldata. In the discussion, the authors make the followingpoint related to selection bias: ‘individuals jumpingfrom aircraft without the help of a parachute are likelyto have a high prevalence of pre-existing psychiatricmorbidity’. If you have not come across this article yet,I strongly recommend that you get a copy.
I hope you enjoyed reading this article and it servedto educate rather than to confuse. I would like to leaveyou with this famous Aaron Levenstein quote:‘Statistics are like bikinis. What they reveal issuggestive, but what they conceal is vital’. �
Statisticsare likebikinis.What theyreveal issuggestive,but whattheyconceal isvital
“
”

SCOPE | MEETING REPORTS
26 | DECEMBER 2010 | SCOPE
10TH INTERNATIONAL WORKSHOP ONDIGITAL MAMMOGRAPHY
GIRONA, CATALONIA, SPAIN 16th–18th June 2010
JENNY DIFFEY Department of Cancer and Enabling Science, University of Manchester /Department of Medical Physics, Westmead Hospital, Sydney, Australia
THE INTERNATIONAL WORKSHOP ON DigitalMammography (IWDM) brings together a diverse set ofresearchers (physicists, mathematicians, computerscientists, engineers, radiologists) and representatives ofindustry who are jointly committed to developingtechnology to support clinicians in the early detectionand subsequent patient management of breast cancer. Ihave spent the last 5 years carrying out a part-time PhDin breast density and breast cancer risk, whilst workingas an imaging medical physicist specialising inmammography, and have found IWDM to be afascinating conference and an excellent venue (figures 1,2 and 3) to learn about emerging technologies in breastimaging. I am very grateful to IPEM for the opportunityto attend.
DAY 1The opening session was on CAD (computer-aideddetection). Paul Taylor (University College London)presented the ‘Impact of CAD with full field digitalmammography (FFDM) on workflow and cost’. CADhas not been widely adopted in the UK partly due toconcerns regarding its sensitivity and specificity,although a recent New England Journal of Medicine studyfound that single reading plus CAD was as effective asdouble reading in terms of detection rate. However, thecost-effectiveness of CAD was not considered.Calculations were based on the balance of cost ofradiologist time saved or spent in screening and post-screening assessment by using CAD with single readinginstead of double reading and the cost of CADworkstations. The conclusions were that CAD has thepotential to save radiologist time and costs, althoughthis is dependent on the relative increase in recall rateand the time taken per patient at assessment. Thisdiffered from the study carried out by the Centre forEvidence-based Purchasing which came to morepessimistic conclusions, but did make a number ofdifferent assumptions and was based on digitised filmmammograms rather than digital mammograms. Anadditional conclusion was that the most cost-effectivesolution may be to use more radiographer advancedpractitioners in the film-reading role.
The talk by Elodia B. Cole (University of NorthCarolina, USA) was a retrospective study of digital casesfrom the DMIST trial, aiming to assess if radiologistperformance would have been improved with CAD.Two CAD systems were employed (iCAD and R2) andresults were the same for both. A slight improvement insensitivity but a slight decrease in specificity wereobserved; neither result was significant. The impact onrecall rate was not considered. The conclusion was thatCAD would not have improved the performance ofFFDM as the radiologists were rarely influenced by the
CAD prompts. However, an audience member queriedwhether the fact that this was a retrospective study, withthe clinical decision already having been made, mighthave had some bearing on the results.
Other talks in the session included an evaluation ofthe performance of triple modality (FFDM, ultrasoundand DCE-MRI) CADx on breast cancer detectionclassification. A method for image registration of x-raymammograms with MRI breast images was alsopresented; this is very challenging due to differencesbetween the two modalities such as breast deformation,dimensionality and resolution and the fact that yourequire a 2D to 3D registration framework. However, itwould certainly have many clinical applications such asstaging and surgical planning.
The session on image processing and analysisincluded an interesting talk by Fabian Zohrer(Fraunhofer MEVIS, Germany) on ‘Interactive multi-scale contrast enhancement of previously processeddigital mammograms’. The aim of the technique was toachieve homogeneity of images, regardless of thesystem they had been acquired on. Post-processing ofimages is vendor-specific and has a huge impact on theappearance of the image to the extent that it can bedifficult to detect changes in the breast between thecurrent and prior images, if they have been acquired ondifferent mammography units. A reader preferencestudy revealed that it was preferable to modify the priorto look like the current image. The technique is nowbeing adapted so that it can be used to improve thevisualisation of fine structure in dense background.
The medical physics community was well-represented in the afternoon session on breast imagingphysics. There were three talks on mean glandular dose(MGD) surveys for FFDM: one on clinical breast dosesby Niall Phelan (Breastcheck, Dublin), one on phantomdoses by Kristen Pedersen (Norwegian RadiationProtection Authority, Norway) and one comparingcalculated MGD to that indicated by the vendor fromJames McCullagh (Breastcheck, Cork). There were somecommon conclusions; most notably that MGD is lowerfor FFDM compared to film-screen systems and therehas been a significant change in the selected beamquality. kVs are generally higher and harder target/filter combinations are being employed, such as W/Rh.Even on units with a molybdenum target, Mo/Mo isalmost never selected. MGD surveys should becomeless time consuming for FFDM equipment as theexposure factors can be downloaded from the DICOMheader. It is still recommended that the MGD iscalculated, rather than relying on the indicated value, asthere was found to be some discrepancy between thetwo. In the majority of cases, this was less than 15 percent but it was vendor-specific. �

SCOPE | DECEMBER 2010 | 27
SCOPE | MEETING REPORTS
28 |DECEMBER 2010 | SCOPE
DAY 2The second day started with an interesting session onclinical experiences. Nick Marshall (University HospitalsLeuven, Belgium) presented the tests required for technicalevaluation of digital breast tomosynthesis (DBT) systems.These could form the basis for a QA programme and couldalso be used to compare systems, in the absence of clinicaltrials data. The tests presented included focal spotdimensions, detector lag, detector response, MTF, NNPSand DQE. These were assessed from projection images. Afuture challenge is how to evaluate results for thereconstruction planes. Yan Chen (LoughboroughUniversity) discussed the possibility of using low-costdisplay devices for mammographic interpretation trainingof radiologists, who may have limited time and limitedaccess to 5MP workstations for training purposes. Otherdevices included standard PC monitors (LCD) and even aniPhone! For a set of training mammograms, participantswere asked to report features, rate their confidence onabnormality presence and classify the case. As expected,performance on the iPhone was poor but interestingly, theresults for PC monitors using post-processingmanipulation tools were comparable to those for the 5MPmonitors and although their lower resolution makes themunsuitable for diagnosis, they could have a role to play intraining. Jenny Oduko (National Coordinating Centre forthe Physics of Mammography, Guildford) presented theresults of a UK digital mammography dose survey from2007–9 with some similar conclusions to those discussedabove. The MGD to the standard breast has decreased byan average of 25 per cent for integrated digital detectorscompared to film-screen, but remains the same for CR. A
talk by Koen Michielsen (University Hospitals Leuven,Belgium) raised the interesting question of whether thefrequency of some medical physics quality control checkscould be reduced, on the basis that radiographer daily QCchecks produce extremely consistent results. Althoughmedical physicists would have to closely review the resultsof daily tests, this would potentially allow them more timefor research and optimisation.
The next session was breast density. Both Mona Jeffries(University of Bristol) and I presented on the relationshipbetween volumetric breast density with other risk factors forbreast cancer. Common conclusions were that percentagebreast density showed strong negative correlations withweight and body mass index; I observed the samerelationship with absolute glandular volume but to a lesserextent. Use of HRT is found to increase breast density.Further research is needed to demonstrate how changes inbreast density relate to breast cancer risk. Mona Jeffries andDespina Kontos (University of Pennsylvania, USA)presented comparisons of volumetric density techniques(known as Volpara™ and Quantra™, respectively) to thearea-based technique, Cumulus, currently considered to bethe gold standard. As expected, percentage breast densitymeasures by volume are lower than those by area but thetwo were generally found to be closely associated,suggesting that volumetric breast density measures couldaid breast cancer risk measurement.
The afternoon session on digital breast tomosynthesisincluded some fascinating talks on new technologyincluding high-resolution CT of the breast (Willi Kalendar,University of Erlangen, Germany), a novel CMOS(complementary metal-oxide semiconductor) flat panel
FIGURE 1.The canalthrough thevillage of Girona.
�
�
MEETING REPORTS | SCOPE
SCOPE | DECEMBER 2010 | 29
FIGURE 2. GironaCathedral.
�
FIGURE 3. Delegatesviewing theposters.
�
�

SCOPE | MEETING REPORTS
30 | DECEMBER 2010 | SCOPE
digital detector (Steve Naday, Dexela Ltd, London) and adual modality scanner combining x-ray breasttomosynthesis with molecular breast imaging (MarkWilliams, University of Virginia, USA) to obtain co-registered structural and functional images. The pilot studyshowed that the dual modality technique is feasible andprovides improved specificity and PPV compared to x-raybreast tomosynthesis alone.
DAY 3The first session of the final half-day was lesion detection.Simulation methods for micro-calcifications, speculatedlesions and architectural distortions were presented. Thesemethods can be used to generate images with abnormalpathology for observer performance experiments. They canalso have applications in the development of CAD software.The simulation models can account for changes in exposuresettings, breast thickness and composition, system MTF andpixel size, or different reconstruction techniques in DBT.
The second session was registration and was heavilyrepresented by the Centre for Medical Image Computing atUniversity College London. Registration techniques areused to warp one medical image of the breast to matchanother, where the images have been acquired in differentorientations, or more commonly on different modalities. Itpresents many challenges in breast imaging, such asmapping 2D to 3D data, accounting for tissue deformationand applying motion correction.
KEYNOTE SPEAKERSMelcior Sentis (Sabadell, Spain) and Cristina Romero(Toledo, Spain) spoke about the ‘Transition to digitalmammography: challenges and future trends’. Thisincluded the challenges associated with becoming filmlessand paperless; a RIS system was introduced and a decisionwas made to only report from softcopy in order to useFFDM to its full advantage. They are also usingteleradiology, and radiologists have been provided with5MP monitors at home!
Ingvar Andersson (Malmo University Hospital, Sweden)presented ‘Breast tomosynthesis: mammography of the
future?’. 2D mammography inevitably suffers fromlimitations, particularly noise; anatomic noise is thought tobe a more significant factor than quantum noise.Tomosynthesis was first described in 1997 so its transitionto use in clinical practice has obviously taken some time,mainly due to the inadequacy of available detectortechnology. Tomosynthesis has shown some promisingimprovements over 2D imaging, most notably in moreaccurate tumour measurement and staging, bettersensitivity in thicker breasts and reduced compressionforce. Dr Andersson stated that calcification detection is notdecreased; they are still there but radiologists requireadditional training to detect them. Although it should bepossible to use tomosynthesis as an alternative to 2Dmammography, there are still some barriers to overcomesuch as increased examination and reading time. Fasterworkstations are required as well as development of CADsoftware.
Professor Sir Michael Brady (University of Oxford) hashad an extensive career in mammography and imageprocessing, having authored over 580 papers. He chose tospeak on ‘Information from breast images’ (figure 4). Thistalk focussed particularly on the development of avolumetric breast density technique. He co-authored thebook Mammographic Image Analysis in 1999 with RalphHighnam, in which a standard representation of the breastwas presented, enabling composition analysis. The methodwas known as ‘hint’ where this refers to the thickness of‘interesting’ (i.e. non-fat) tissue at any point within thebreast. Further developments to the method resulted inSMF (standard mammographic form), Quantra™ andVolpara™, the latter two of which are commerciallyavailable and are being used around the world toinvestigate the relationship between volumetric breastdensity and breast cancer risk. �
�
FIGURE 4.Professor SirMichael Bradyspeaking at theconference.
�
ACKNOWLEDGEMENTSI would like to thank IPEM for the travel bursary. Many thanks go to theconference organisers, Dr Joan Marti and his team from the Universityof Girona, for putting together an excellent programme and fantasticevening entertainment, including a visit to the Dali Museum and dinnerat a three Michelin-starred restaurant!
MEETING REPORTS | SCOPE
SCOPE | DECEMBER 2010 | 31
IT’S TIME TO STAND UP FOR SCIENCE ONCE MORESense About Science (SAS) is an independent charitabletrust. It responds to the misrepresentation of science andscientific evidence on issues that matter to society, fromscares about plastic bottles, fluoride and the MMR vaccineto controversies about genetic modification, stem cellresearch and radiation. SAS works with scientists and civicgroups to promote evidence and scientific reasoning inpublic discussion.
The annual Sense about Science lecture 2010, of whichIPEM was one of the principal sponsors, was held in theRoyal Society for Medicine in London, entitled ‘It’s time tostand up for science once more’, and given by FionaGodlee (Editor-in-Chief of the British Medical Journal (BMJ),figure 1). In order to manage such a large, high-profileevent Sense about Science required several volunteers. Anemail request had been sent to the Medical Physicsmailbase in the hope of persuading a few IPEM membersto help out. A fantastic response was received with nineyoung scientists and engineers agreeing to give up theirevening for the event. With the addition of three volunteersfrom the APEN panel, IPEM representatives made up themajority of the volunteer force. Below is a summary of the
lecture, followed by accounts from some of the volunteers.
THE LECTUREDuring her time as editor of the BMJ, Dr Godlee haschampioned evidence-based medicine, openness inresearch, peer review and editors’ responsibilities. She hasalso played an active role in the current high-profile SenseAbout Science campaign against libel laws, in particularagainst libel in publishing. The lecture focussed on DrGodlee’s area of expertise, medicine, but the themes andideas can easily be applied across science.
One of the first, and most famous, editors of the BMJwas Earnest Heart. He led an investigative journal articleinto the practice of baby farming during the industrialrevolution where parents of children, many illegitimate,paid for someone to take their children away to look after,often only for them to be neglected or killed. This piece ofjournalism led to the reform and legislation of childwelfare and shows the power that journals can have insociety – something that Dr Godlee believes should still bethe case.
As she wrote the lecture she found it turning into a pleafor greater independence in science and medicine. The
5TH ANNUAL SENSEABOUT SCIENCE LECTURE
ROYAL SOCIETY OF MEDICINE, LONDON 21st June 2010
ALAN MCWILLIAM (APEN panel), ROSEMARY EATON (APEN panel), MATT WARD(Integrated Radiological Services, Liverpool), NEIL DAVIS (East and NorthHertfordshire NHS Trust)
FIGURE 1.Dr Fiona Godleedelivering thelecture.
�
�
SCOPE | MEETING REPORTS
32 | DECEMBER 2010 | SCOPE
same phrases kept turning up: conflict of interests,reporting bias, manipulation of evidence, ghost/guestwriting, opinion leaders, disclosure and peer review.Countless examples were given to show the effect thesehave on science, more than enough to fill an entire issueof Scope, and this was just the tip of the iceberg. Thelecture finished with examples from America and Italy,where improvements are already being implemented,and with Dr Godlee’s recipe for change.
The extent of some of these influences was quicklyhighlighted with some recent examples. Out of 56recent papers on anti-inflammatory drugs, nonepresented an unfavourable conclusion. This isstatistically unlikely. However, the authors were foundto have ties with the pharmaceutical industry and eventhough the results might have been unfavourable theconclusions had been spun to be more positive. In fact,studies have shown that trials funded by a company arefour times more likely to show favourable conclusionsthan independent trials. At times the same studies havebeen re-written and published by separate authors tohighlight results while negative trails are buried anddon’t get published.
Journals themselves are also potential culprits,especially those who gain the majority of their revenuefrom advertising. During Dr Godlee’s time as editor, ontwo occasions the journal’s advertising revenue hasdropped dramatically owing to negative articlespublished about a company’s drugs. It is not unheardof for editors to be fired for this reason. True editorialfreedom and independence cannot exist under thesefinancial pressures.
One recent example that we were all exposed to wasthe recent flu pandemic. Tamiflu was the drug of choiceand was stockpiled in countries around the world. The
Cochrane Collaboration (an independent, not-for-profitorganisation promoting systematic reviews ofhealthcare) found that the pharmaceutical companymanufacturing the drug, Roche, had not published eightout of ten trials involving more than 3,000 people. Rocherefused to share this data. The BMJ and Channel 4became involved in a piece of investigative journalism;some further data was released but still not everything.Of the trials published some had been ghost written,where the company itself conducts the trial and analysisand writes the paper. The company pays to get an‘opinion lead’ to attach their name to the article, thislending weight, prestige and the appearance ofindependence. This also means the evidence is still heldby the company and not in the public domain. DrGodlee described the process of ghost writing as, whatthey call in the trade, fraud.
To deal with the flu pandemic the WHO set up a 16member advisory committee. They set in place thecontracts for countries to stockpile Tamiflu and decidedwhen to begin this process. They also changed thedefinition of a pandemic so it depended solely ongeographical coverage and not a combination of thisand severity, therefore allowing the term pandemic to beapplicable. Investigations revealed that at least three ofthe 16 members of this committee were linked directlyto companies who would profit from the flu pandemic.At no stage was this conflict of interest declared, nor theinfluence this may have had on their decisionsconsidered.
Vioxx is a controversial drug created by Merck usedto treat osteoarthritis. It elevates the risk of myocardialinfarctions in at-risk patients and this has led to a seriesof court cases in the USA. The initial trials did notconsider heart attacks in individuals, and the trial board
FIGURE 2.Rosemary Eaton,Steven Keevil andAlan McWilliam atthe IPEM standwith an interestedattendee.
�
�

MEETING REPORTS | SCOPE
SCOPE | DECEMBER 2010 | 33
did not include a cardiologist. The large-scale trialconcentrated on gastrointestinal effects to show thedrug’s benefit over the current commonly prescribedmedication. The published trial results, as is now clearfrom the lawsuits, were intermediate results while thefinal conclusions were not yet clear. But on the basis ofthis the pharmaceutical company went ahead andmarketed the drug. It also turned out that the head of thetrial board had been given a two-year consultancycontract with Merck and had family shares worth$70,000 in the company. This conflict of interest wasnever declared. Independent trials went on to show amuch higher risk of myocardial infarctions over 3 yearsagainst a placebo, leading to the court cases in America.
This did raise the question during the lecture, and inthe discussions afterwards, about patient choice. Vioxxwas a very good drug; patients on it were extremelypleased with the increase in quality of life. Was this anopportunity for openness in medicine where doctorscould engage in a grown-up discussion with theirpatient about the benefits and risks to them fromprescribing this drug? Should this be part of the futurehealthcare model?
The Institute of Medicine in the USA has asked thequestion: is disclosure enough? Do we then leave thereader to make their own judgement or should we gofurther and use this as a bar to involvement in a panel,research or authorship? They have taken the latter viewand, with the help of Senator Grassley, are pushinglegislation, the ‘Sunshine Act’, through the Senate for thecreation of a database of conflicts of interest. They havealso made the statement ‘researchers should not conductresearch if they have a financial interest in the outcome’.This is a statement that Dr Godlee applauds.
Italy is another country taking steps in this area. Alaw has been passed that requires drug companies topay into an independent pot of money. This is then usedto fund research into drugs trials, the results of which arepublished in a fair and independent manner.
Dr Godlee’s recipe for change follows four points.Number one: stop drugs companies running their owntrials. Follow Italy’s system by creating a pot of money,into which companies would pay 5 per cent of theirbudget, for truly independent trials. Number two:independent experts cannot exist if they are paid bydrug companies. The pot of money should also be usedto pay for their expertise. Number three: the entire trialdata set should be published (especially with theunlimited online space journals can access) including allthe meta-level data; decisions, panel minutes, etc.Number four: a return to investigative journalism. Keepsubjects before the public until questions have beenanswered or reform begun (as in the history of the BMJ).As Dr Godlee pointed out, where is the Private Eye formedicine? It has been said that ‘news is what someonewants to suppress, all else is advertising’.
The lecture finished with a statement, one we shouldall perhaps take to heart, not just in our own work butwhen evaluating the evidence we use everyday:‘independence is not a privilege, it’s a duty’.Alan McWilliam
VIEW FROM THE FRONT LINEBefore and after the lecture there was plenty of time fornetworking with eminent scientists, journalists andpoliticians over a glass of wine. APEN volunteers ran anexhibition stand to promote IPEM and medical physics ingeneral. Aided by an eye-catching poster and a colourfulrange of leaflets, brochures and the ubiquitous IPEM pen,we attracted a number of visitors (figure 2). Although mostof those we spoke to were not familiar with medicalphysics, all had some connection with the field: from afriend undergoing radiotherapy to tales of an interestingmedical device. We were struck by how ready the publicwere to engage with us and how interested they were inboth established and emerging technologies. Overall thiswas a very productive opportunity to raise the profile ofour profession in the wider scientific community.
On behalf of the APEN panel I’d like to thank all of theAPEN members who volunteered at the lecture: KirstyBlythe, Neil Davis, David Eaton, Joanna Findlay, Matt Grey,Elizabeth Howell, Matthew Lee, Philip Rixham, Matt Ward,Alan McWilliam and Jonathan Taylor. We hope that youenjoyed the evening and will consider participating in anyfuture collaborations between IPEM and SAS. Rosemary Eaton
VOLUNTEERING AT THE EVENTAs some of you may know, the Medical-Physics-Engineeringmailbase is awash with information. Sitting in the office oneafternoon, I was pleased to have enough time to catch theinvitation circulated on the mailbase to volunteer and attendthe fifth annual SAS lecture before a million other emailsbegan screaming for my attention. I was due to be in Londonfor the RPA Update on 22nd June – the SAS lecture tookplace on the 21st, so it was win–win all round for yourstruly, travelling down from the grimy North.
As a member of IPEM, but currently on the fringes of anyformal or informal trainee network, taking a ‘route B’ path toclinical scientist training, it was useful to meet up with thelocal SAS team, APEN volunteers and the SAS Voice ofYoung Science (VoYS) scientists from other areas of research,including healthcare, academia, politics and journalism.
The volunteer work itself was easy enough – we werestrong in numbers! Meeting and greeting the main body ofSAS attendees, including Chris Gibson representing IPEM atthe highest level, ushering them through the pleasantarchitecture of the Royal Society of Medicine’s WimpoleStreet building, I hope we set an amiable mood amongst allthe arrivals, and that was certainly the feeling amongst theAPEN contingent.
A crystal clear yet passionate opening speech from ChairTracy Brown reminded the delegation of the difficulties ofcommunicating objective, sensible scientific facts in the faceof commercial, populistic and politically pressurisedenvirons. We’re probably all used to de-bunking the oddmyth or two in our day jobs, no matter how large or smallour departmental teams. I’m sure I wasn’t alone amongst theattendees considering how many health and safetymisnomers and radiation ‘facts’ (scares!) I have contested,formally or informally.
As a volunteer activity, it was a pleasure to representIPEM in a small way and be privy to the impact that we canall make in a larger scientific and medical arena. I’drecommend volunteering in any small way to anyonereading this – hopefully I’ll be there again next year.Matt Ward
MORE INFORMATIONMore details on the lecture, including a podcast of the event, areavailable from the Sense About Science website:www.senseaboutscience.org.uk �

SCOPE | MEETING REPORTS
34 | DECEMBER 2010 | SCOPE
MEETING AND GREETINGOn the 21st June I volunteered at Sense About Science’s5th Annual Lecture, held at the Royal Society of Medicine.I arrived and was introduced to the staff and othervolunteers helping to run the event. Along with anothervolunteer I was put to work straight away manning theRoyal Society of Medicine stand in the atrium (figure 3).As a physicist and a psychologist, neither of us knew agreat deal about the Royal Society of Medicine, butenjoyed finding out. After a while it was time for thelecture to begin, and we helped usher people into theirseats in the lecture theatre (figure 4). The lecture was wellreceived, and invited much discussion from the floor, so
we sprang back into action, carrying microphones topeople asking questions. Afterwards at the drinksreception I had the chance to mingle with the othervolunteers and enjoyed hearing about the range ofdifferent research people were involved in, and theircareer aspirations. I talked with scientists of all ages andspecialties, as well as bloggers and journalists, each withtheir own interesting points of view. There were also oneor two famous faces in attendance (figure 5), and for meone of the highlights of the evening was shaking handswith Ben Goldacre, author of the Guardian’s Bad Sciencecolumn. I eagerly await next year’s lecture!Neil Davis �
FIGURE 3. [TOP LEFT]Neil Davis at theRoyal Society ofMedicine standswith an attendee.
FIGURE 4. [TOP RIGHT]Attendeeswaiting for thelecture.
FIGURE 5. [BOTTOM]Science writerSimon Singh.
��
�
�
MEETING REPORTS | SCOPE
SCOPE | DECEMBER 2010 | 35
�
RADIATION PROTECTION ADVISERS(RPA) UPDATE MEETING 2010
UCL INSTITUTE OF CHILD HEALTH, LONDON 22nd June 2010
ELIZABETH LARKIN Queen Elizabeth Hospital, Birmingham
THE ANNUAL RPA UPDATE MEETING, organised by theInstitute of Physics in Engineering and Medicine (IPEM)Radiation Protection Special Interest Group, was held on22 June at UCL Institute of Child Health in London. EddyRafiqi (Queen Elizabeth Hospital, Birmingham) openedthe day by welcoming everyone to London. He handedover to Penny Allisy-Roberts, who was chairing the firstsession.
DEVELOPING THE EC BASIC SAFETY STANDARDSGareth Thomas (Health & Safety Executive, Cardiff) gavea comprehensive overview of the process leading to newregulation, concentrating on the two Basic Safety Standards(BSS) currently under revision; the Euratom BSS Directive(mandatory in EU member states) and the InternationalBSS (highly influential, but not strictly mandatory). TheHealth and Safety Executive is the UK lead, whilst the UKgovernment lead for EC negotiation is the Department ofEnergy and Climate Change. The UK has three negotiatinggoals: to improve by simplifying and achieving better
regulation, to retain flexibility and to avoid new burdensthat offer no radiation protection improvement.
The draft Euratom BSS showed some harmonisationwith International Standards (using ICRP103 terminology),integration of natural and artificial sources, betterdefinition of medical/non-medical exposures, a gradedapproach to regulatory control, enhanced role of thecompetent authorities and existing exposure situations.
Two of the eight steps have been completed for theEuratom BSS; transportation into national legislation isexpected within the next 3–4 years. Version 3.0 of theInternational BSS was issued in May and the InternationalAtomic Energy Agency hope to get agreement from theRadiation Safety Standards Committee in December 2010.
USEFUL WEB LINKS INCLUDE: http://www.hse.gov.uk/radiation/rpnewshttp://www.hse.gov.uk/aboutus/europe/euronews/dossiers/radiationprotect.htmhttp://www.ec.europe.eu/energy/nuclear/radiation_protection/article_31_en.htmhttp://www.iaea.org
SCOPE | MEETING REPORTS
36 | DECEMBER2010 | SCOPE
NEW BRACHYTHERAPY AND RADIOTHERAPYTECHNIQUES: RADIATION PROTECTION ISSUESWet age-related macular degeneration (AMD) is the mostcommon cause of blindness in the UK. Standard treatmentinvolves regular eye injections with a drug called Lucentis.In his presentation, John Saunderson (Hull & EastYorkshire Hospitals) talked about the radiation protectionissues surrounding epiretinal brachytherapy where a 24 Gydose of beta-radiation is delivered to the small area of theeye affected by wet AMD in a single fraction (delivered in3–4 minutes). He outlined the legislative considerations forradiation protection, i.e. those relating to RSA93/EPR10,M(ARS), IRR99, IR(ME)R2000 and CDG2009. Typical staffdoses are: 265 μSv to the surgeon’s fingers per patient and6 μSv to the physicist’s body per patient. If 566 patientswere treated in a year, doses to the surgeon’s fingers andthe physicist’s body would be 150 mSv (i.e. 3/10th of thedose limit) and 3.4 mSv, respectively. John also lookedbriefly at radiation protection issues surroundingcyberknife and tomotherapy treatments, intraoperativeradiotherapy and kilovoltage stereotactic radiosurgery.
IODINE RESTRICTIONSBill Thomson (Sandwell & West Birmingham HospitalsNHS Trust) discussed the issues and problems followingoutpatient administration of a 600 MBq dose of 131Iodine.As much of the material presented was taken frompublications, the appropriate references have beenincluded. In summary, there needs to be an awareness ofthe appropriate dose constraints, comforters and carersneed to be identified, calculations may need to be carriedout for individual situations, the correct dose rate modelneeds to be applied, there may be travel restrictions, therewill be pregnancy restrictions and there can be flexibleinterpretation for difficult cases.
RADIATION PROTECTION IN PET/CTThe design of the facility is important because patients canbe in the department for up to 2 hours each; there can bemultiple patients resting and space is always less thanideal. 18Fluorine emits a 511 keV gamma, thus increasingthe shielding requirements for storage and preparation …and then there is the CT! Radiation protection in PET is amultidisciplinary issue from the regulators to the patients.
Debbie Peet (Royal Surrey County Hospital, Guildford)discussed other issues for consideration, i.e. riskassessments, training requirements, systems of work, staffdose and pregnancy, contingency plans, contaminationmonitoring, licenses under RSA93/EPR10 and ARSACcertification.
HSE: AN UPDATEGillian Rodaks (Health & Safety Executive) highlightedthe outcome of a review of 31 radiation inspections over a10-year period. The inspections showed varying standards;there were areas of non-compliance and areas of significantimprovement. There were recommendations relating tolocal rules (20 inspections), co-operation betweenemployers (18 inspections), risk assessments (13inspections), training of staff (11 inspections), doseassessment and recording (10 inspections) and exposuresnot being ALARP (10 inspections). However, bettercompliance was observed in the implementation of QAprogrammes, greater management commitment andhandover arrangements for equipment.
OUTCOME OF THE COMARE 12 CONSULTATIONIn December 2007, the COMARE 12 report was published.COMARE made nine recommendations; the Department ofHealth (DH) carried out a consultation and Ian Chell(Department of Health, London) provided feedback. Theconclusion was that whilst COMARE’s recommendationsstood undiminished, the practice of self-referredasymptomatic individuals needed to be brought within UKregulations. Appropriate changes will be made to theIonising Radiation (Medical Exposure) Regulations 2000(IR(ME)R) to ensure that the CT scanning of self-referredasymptomatic imaging is included. These changes willmean that individual health assessments (IHA) are clearlybrought within the regulatory regime. The clinical referralguidance has the potential to protect the health of thosepatients who may choose to have IHA CT screening. Insummary, a balanced way forward has been achieved thatis based on the globally accepted system of justification.
The Health & Social Care Act 2008 came into force on 1stApril 2009. This Act has changed how health and socialcare services in England are regulated and all providers ofa ‘regulated’ activity are required to register with the CareQuality Commission (CQC) in order to be able to continueto lawfully carry on a regulated activity.
UPDATE FROM THE ENVIRONMENT AGENCYThe Environmental Permitting Regulations 2010 (EPR 2010)came into force on 6th April 2010 and have largely replacedthe Radioactive Substances Act 1993 (RSA 93) in Englandand Wales; RSA 93 is still active in Scotland and NorthernIreland. Kate Griffith (Environment Agency) advised thatRSA93 authorisations and registrations automaticallybecame ‘environmental permits’ and that there were nomajor changes in the scope or nature of the radioactivesubstances legislation. Whilst there are no regulatorchanges, changes in the scope of regulation or standards forenvironmental protection, the following changes will occur:full or partial transfer of an environmental permit is nowallowed, the process for new applications is subject topublic consultation, a site plan is required for applications
�
USEFUL REFERENCES INCLUDE:Cyberknife:NCRP Report 151, 2005http://www.accuray.com/services/site_planning.aspxhttp://www.aapm.org/meetings/07ss/documents/RodgersCyberKnifeShieldingpostmeeting.pdfTomotherapy:Wu C et al. Phys Med Biol 2006; 51: N389–92Intraoperative radiotherapy:Parry J et al. Radiother Oncol 2005; 76, Suppl 2: S202–3Joseph DJ et al. ANZ J Surg 2004; 74: 1043–8Daves JL et al. J Appl Clin Med Phys 2001; 2: 165–73Kilovoltage stereotactic radiosurgery:Chell E et al. AAPM, 2009http://www.orayainc.com/articles.asp for this and papers
USEFUL REFERENCES INCLUDE:Approved Code of Practice, paragraphs 126–33http://www.hse.gov.uk/research/rrhtm/rr155.htmNuclear Medicine Communications: Hilditch TE et al. 1991; 12: 485; Thomson WH, Harding LK 1995; 16:879; Thomson WH et al. 1996; 17: 300; Gunasekara R et al. 1997; 18:333; Greaves CD, Tindale WB 1999; 20: 179European Journal of Nuclear Medicine: Barrington SF et al. 1999; 26: 686–92; Pauwels EKJ et al. 1999; 26:1453; Barrington SF et al. 2008; 35: 2097–104ICRP Publications 88 and 95
FOR FURTHER INFORMATION: http://www.cqc.org.uk
MEETING REPORTS | SCOPE
SCOPE | DECEMBER 2010 | 37
and the requirement to display sealed source certificates isno longer required. The key benefits include consistentregulatory approach across environmental regulation,improved procedural arrangements, e.g. inter-site transfersand staged regulation for repositories.
The principal aims of RSA 93 Exemption Order revieware to rationalise and standardise, to reduce burden onusers and regulators, to achieve a risk informed basis forexemption, to align with the BSS Directive and ECguidance and to be flexible enough to deal with change.
SURVEYING DOSE LEVELSThere remains a general feeling that while set-up,technique and doses in computed radiography (CR) mayvary, there is limited published evidence. Jonathan Cole(King’s College Hospital, London) presented the results ofa project initiated by the Department of Health. Datacollected for PA chest and AP abdomen examinations fromparticipating departments included local standardoperating protocols (SOPs), entrance surface air kerma(ESAK) measured ‘free in air’ with an ionisation chamberand detector dose measured using an Unfors mult-o-meterin a modified cassette and corrected for ratio of ESAKs;distances, half value layers, kVp and measured data wereused to calculate effective dose (E) using the Monte Carloprogramme PCXMX. The results show that the wide rangeof SOPs, detector air kerma (DAK) and E obtainedsuggested substantially different optimisation methods;DAK varied from 2.4 to 7.8 μGy and from 4.6 to 19 μGy forAP abdomen and PA chest examinations, respectively. Noevidence has been found for differences between CRsupplier or technique.
E-IR(ME)RSteve Evans (Northampton General Hospital) described e-IR(ME)R as a joint project between IPEM and e-Learningfor Healthcare (Department of Health). It uses an e-learning approach to satisfy the core training requiredunder the Ionising Radiation (Medical Exposure)Regulations 2000 (amended 2006) (IR(ME)R). The principalgroups requiring this training are referrers, practitionerand operators who are involved in the use of ionisingradiation for the diagnosis and treatment of patients. Eachmodule contains a number of e-learning training sessionsthat are designed to be engaging, validate prior knowledgeand deliver relevant content that the learner is expected toremember; each session contains interactive content thatwill deliver the educational objectives using a variety oftechniques such as animation and video.
IS THE INSTANTANEOUS DOSE RATE RELEVANTAS A DETERMINANT OF SHIELDING THICKNESS?Philip Mayles (Clatterbridge Centre for Oncology, Wirral)indicated that dose rates from modern linear accelerators
can be as high as 30 Gy/min. This makes primary barriers,designed to instantaneous dose rates (IDR) of 7.5 μSv/h,unnecessarily large. A realistic assessment of the TADR2000could be around 0.1 mSv, even with an IDR of 20 μSv/h,because the total dose to the isocentre may not be affectedby the peak dose rate. The ACOP suggests that if the IDRexceeds 7.5 μSv/h in an area accessible to workers, the areashould be controlled, whereas the Medical and DentalGuidance Notes suggest that TADR2000 is more important.NB. IRR Regulations 8 and 16 – there is nothing in theregulations regarding IDR.
ISSUES REGARDING THE DEREGULATION OFSOME COSMETIC LASER USERSOn 1st October 2010 the Health and Social Care Act 2008(Regulated Activities) Regulations 2010 come into force.Stan Batchelor (Guys’ & St Thomas’ NHS FoundationTrust, London) reported that many cosmetic laser users willno longer come under the regulation enforced by the CareQuality Commission (CQC), i.e. they will no longer have tobe registered with them. Users may choose not to employthe services of a certificated Laser Protection Adviser (LPA)and may well cut out the LPA service altogether. Whilstusers still need to comply with the Health and Safety atWork Act, there will not be the same degree ofmonitoring/inspection process which would help maintainstandards and assure public safety. A group has met with the Department of Health in anendeavour to remediate this potentially disastrous situation.The group hopes to put regulation back in the hands of localauthorities who will licence premises as some used to priorto NCSC/HC/CQC days. Councils without these existingstatutes will not be in a position to do this by 1st October.
UPDATE ON THE GUIDANCE DOCUMENT FOR RADI-ATION EMERGENCY PREPAREDNESSIan Chell reported that the latest version of the radiationguidance for the NHS should be published this summer,once the new minister has agreed publication. Theambulance guidance was published earlier in the year androlled out to ambulance trusts; the Health ProtectionAgency (HPA) are now providing a 24/7 radiationprotection advisory service for on-duty trust supervisorsand a comprehensive training programme.
PFI CONTRACTS AND THE HOSPITAL RPAFor a traditional hospital build, the appointed RadiationProtection Adviser (RPA) takes full responsibility forspecification of radiation protection and critical examinationof the finished facility. In a private finance initiative (PFI)contract, there may be other parties involved. For example,the PFI contractor may appoint a RPA to specify radiationprotection requirements. Ultimately, the hospital RPAassures statutory compliance and takes responsibility for thedesign. It is possible that the two RPAs disagree on thespecification. There may be a question over who is legallyresponsible if there is a problem with the protection. MarkKnight (Maidstone & Tunbridge Wells NHS Trust) advisedRPAs to check their contractual obligations prior to signingany contract. �
FOR FURTHER INFORMATION: http://www.defra.gov.uk/environmental/policy/permits/guidance.htmhttp://www.environment-agency.gov.uk/business/sectors/32481.aspxhttp//:www.decc.gov.uk/en/content/cms/what_we_do/uk_supply/energy_mix/nuclear/radioactivity/radioactivity.aspx
FOR FURTHER INFORMATION: http://www.kcare.co.uk
FOR FURTHER INFORMATION: http://www.e-IRMER.org.uk
SPONSORSThe meeting was sponsored by e-Learning for Healthcare, ImagingEquipment, MediScientific, Mirion Technologies, Panasonic IndustrialEurope, PTW-UK Ltd, Qados and Wardray Premise Ltd.

SCOPE | MEETING REPORTS
38 | DECEMBER 2010 | SCOPE
PER AORDUA AD ASTRA: ENHANCING THESCIENCE OF ARTIFICIAL OPTICAL RADIATION
UNIVERSITY OF READING 27th–28th July 2010
CATHERINE KENDALL Gloucestershire Hospitals NHS Foundation Trust)
THE BIANNUAL LPA UPDATE MEETING was held at theUniversity of Reading. Michael Lynn (Royal BerkshireHospital, Reading, UNIRSIG Chair) welcomed everyone tothe meeting and explained that one of the aims of themeeting was to look at the challenges and opportunitiespresented by the new Artificial Optical Radiation (AOR)Regulations which came into force in April 2010.
Day 1 started with an overview, by David Taylor(Gloucestershire Hospitals NHS Foundation Trust), of theupdate to IPEM Report 76 ‘Phototherapy physics:principles, sources, dosimetry and safety’ which is eagerlyawaited and expected to be published late in 2010. SinceReport 76 was first published in 1997 the therapeuticapplications of light have developed although the scienceremains the same. Broadband UVB has almost disappearedfrom clinical use being replaced by narrowband UVB, andphotodynamic therapy (PDT) is now widely used;therefore a chapter has been devoted to this topic in thenew edition (it wasn’t mentioned previously). The revisedreport reflects that we now have a better understanding ofneonatal jaundice, Crigler-Najjar syndrome and how bluelight can be used to treat these conditions. David Grimes(Dublin City University) then presented an entertaininglook at a dosimetry model for UV phototherapy withplenty of maths to make sure all the delegates were kept ontheir toes. Lynn Gaynor (Mater Misericordiae UniversityHospital, Dublin) then discussed her work, demonstratingthe spectral shifts that are seen in UV spectral output fromcabins with protective perspex sheeting in place withimplications for many who use UV cabins (figure 1). Aftercoffee Donald Allan (North Western Medical Physics,Christie Hospital, Manchester) presented results from astudy using interstitial PDT for the treatment of BCCs inpatients with Gorlins syndrome.
The focus then moved to the practical implementation ofthe new AOR regulations with examples of hazardassessment for various light sources in the hospitalenvironment, such as IPLs presented by Colin Swift(Coventry & Warwickshire NHS Trust, Coventry) and avariety of other sources presented by Fiametta Fedele(Guy’s and St Thomas NHS Foundation Trust, London)(figure 2). Neil Haigh (Luminanz Ltd, Bolton) thendemonstrated software developed in conjunction with NPLfor the assessment of optical radiation sources. JohnO’Hagan (Health Protection Agency, Didcot) provided apractical introduction to undertaking a hazard assessmentof a ubiquitous optical source: office lighting. After anintroduction to units and solid angles, delegates wereencouraged to find the correct limits to apply. Thisintroduction then led to three workshops, during whichparticipants got to grips with practical demonstrations ofmeasurements on various sources likely to be encounteredin the hospital: red LED array used for PDT, white lightinspection lamp and blue light sources used to treatneonatal jaundice and UV tubes (figure 3). It wasacknowledged that many medical physics departments do
not have the resources available to use a spectroradiometerfor measurements but that a radiometer can provide usefulinformation if the spectral output of the source is known.
Day 2 started with insight into Salisbury’s experience oflaser quality assurance (QA). Tom Lister (Wessex SpecialistLaser Centre, Salisbury) shared his experience ofimplementing a quality control system run by nurses usingthe lasers. Reuben Lowson (Wessex Specialist LaserCentre) continued the theme with information on a systemfor remote monitoring of QA records. After coffee SheonaBrowne (Care Quality Commission (CQC), London)explained the scope of CQC registration required withrespect to laser use from October 2010. The CQC is theindependent regulator of all health and adult social care inEngland. From October 2010 the non-surgical use of class3B and 4 lasers and intense-pulsed light equipment will bederegulated. Sheona said that the public have the freedomto choose which services they use and that the consumerhas responsibility for making sure that a laser clinic is safe.However the consensus of those attending the meeting feltthis was not an acceptable approach to the safetymanagement of cosmetic lasers. The CQC position is athttp://www.cqc.org.uk/_db/_documents/Lasers_Lights.pdf. Stanley Batchelor (Guy’s and St Thomas NHSFoundation Trust, London) concluded the morning withresults from an audit of laser safety in universities andhospitals. Several photos of interesting items in laser labs,including bikes and cardboard boxes, illustrated that insome instances academia can be rather more relaxed withrespect to laser safety than clinical settings (figure 4).
The afternoon of day 2 was mainly devoted toimplementation of the AOR regulations, picking up on theworkshops and worked examples presented on day 1.Steve Walker (Health and Safety Executive, Bootle) gavean overview of the regulations and the HSE’s expectationswith regard to implementation. Catherine Kendall(Gloucestershire Hospitals NHS Foundation Trust)presented work being undertaken by a UNIRSIG workingparty to prepare a practical guide on implementation ofAOR regulations which will be published as an IPEMreport. Ian Negus (University Hospital of Bristol)presented ways of acquiring the required data to informhazard and risk assessments for implementation of AOR,e.g. manufacturer’s data and source spectral database.Karen McBride (Scottish Health Boards) then shared theexperience of an interdepartmental approach toimplementation of AOR north of the border. It wasencouraging to see various groups using similarapproaches to the new legislation.
After tea Luke Price (Health Protection Agency, Didcot)gave the final presentation of the meeting with anintroduction to his interesting research project on thebeneficial effects of light on human health and how he isgoing to assess and measure these effects in care homes.
The meeting concluded with a lively discussion, chairedby Philip Wright (Wessex Specialist Laser Centre),

MEETING REPORTS | SCOPE
SCOPE | DECEMBER 2010 | 39
focussing on the following topics raised during themeeting.
John O’Hagan kicked off by asking ‘What do laser andIPL standards provide?’, and indicated that theclassification scheme for lasers may be restructured. Theaudience felt the standards provide a helpful frameworkbut that a requirement for manufacturers to provide moreinformation on products such as nominal ocular hazarddistance and spectral output would be helpful. It waspointed out that existing legislation does requiremanufacturers to provide such information; however, aspurchasers, we should be asking more questions at thepre-procurement stage. John also indicated there is avacancy for an IPEM representative on the BSI committee.
‘What is the appropriate tolerance for laser QA?’ wasdiscussed next. The standard states +/− 20 per cent. Theneed for clinical repeatability was felt to be moreimportant than absolute output, but there is also a need forcomparison between centres for which the output needs tobe measured accurately. There was some discussion aboutwhere the best place is to make measurements at theoutput of the laser itself or at the handpiece. This questionalso raised the issue of meter calibration.
‘Laser de-regulation: what does it mean for me?’ raisedrelated questions about patient/public safety followingderegulation and alternative regulation schemes beingproposed by Independent Healthcare Advisory Services.
This led nicely onto the next question: ‘Is there any pointin being an accredited Laser Protection Adviser (LPA)?’
Employers are responsible for gaining expert adviceand an LPA certificate is proof of this. However, this is notclear-cut until CQC takes action against someone for pooradvice from an uncertificated LPA (an unprotected title inUK). It should be remembered that healthcare is only onesector which uses lasers; there are also lots of LPAs inacademia and industry who will continue. Whether theaccreditation schemes for LPAs in heath will continue wasalso raised.
The final question related to local implementation ofAOR and discussion of the various approaches that havebeen adopted by trusts around the country depending ontheir existing health and safety and radiation safetymanagement structures.
Finally, everyone was invited to the British MedicalLaser Association annual scientific meeting to be held atWoburn Abbey on 19th–20th May 2011. This is a jointmeeting with the British Skin Laser Study Group and theUK PDPDT Interest Group, and a great opportunity tonetwork with the principal academic and commerciallaser community from the NHS and private centres andhear from at least two eminent international speakers.
Thanks to the exhibitors, Bentham Instruments Ltd andLaser Physics UK Ltd, who supported this informativeand interesting meeting which was well attended. �
FIGURE 2.(BOTTOM RIGHT)Example of a riskassessment of aknown sourcepresented byFiametta Fedele.
FIGURE 3.(TOP RIGHT) Hands-onworkshopsdemonstratingmeasurement ofartificial opticalradiation sources;red LED array forPDT, UV sourcesand blue lightsources forneonatalphototherapy.
FIGURE 4. (BOTTOM LEFT)Example of hownot to manageyour laser lab withrespect to lasersafety.
��
�
FIGURE 1.(TOP LEFT) Spectroradiometerand handheldradiometercharacterisationof ultravioletphototherapycabin output.
�

SCOPE | INTERNATIONAL NEWS
40 | DECEMBER 2010 | SCOPE
� to share knowledge on available
resources: guidelines, tools,
strategies, policies and best
practices at national and
regional levels and determine
the needs;
� to bring together policy makers,
organisations, funding
agencies and key stakeholders
to foster interdisciplinary
partnerships and cultivate the
aim of reaching a common
goal of having accessible
medical devices.
As a starting point of the
forum, the report ‘Medical
Devices: Managing the Mismatch’
summarised the results of the
Priority Medical Devices Project.
This was established to
determine whether medical
devices currently on the global
market meet the needs of health
care providers and patients
throughout the world and if not,
propose remedial action based on
sound research. Their
investigation evaluated the ‘four
A's’ in the context of available
means to fight the health hazards,
which are: availability,
accessibility, appropriateness and
affordability. As the title shows,
they found a mismatch between
what is available on the market
and what is needed in the field to
combat the main health
problems.
Also during the forum,
sessions discussed the outcome
of the ‘call for innovative
technologies to address global
health concerns’.
Commercialised devices selected
include an LED phototherapy unit,
fluorescence visualisation for
cancer screening and a reusable
neonatal suction system. Some
devices selected that are
currently under development are
a simplified anaesthesia unit and
a transcutaneous anaemia
Around 350 participants from every
corner of the globe were present
when the forum was formally
opened by the WHO Director-
General Margaret Chan, showing
the interest at the highest level of
the WHO in medical technology.
The goals were stated as being:
� to demonstrate evidence on the
need for appropriate evaluation,
prioritisation, regulation,
assessment, management
and research strategies on
medical devices;
monitor. More information is
available on the WHO website.
Other presentations were
given by a range of speakers
from the World Bank, NICE, UN
agencies and also from a wide
variety of country health
ministries. Summaries of future
trends, appropriate technologies
and device regulation issues
showed the way forward in a
number of problem areas. After
the closing session, four
workshops were held on ‘Health
Technology Assessment’,
‘Medical Devices Management’,
‘Medical Devices Regulation’ and
‘e-Health’, enabling industry,
practitioners and health
ministries to have the rare
chance to discuss these
important topics together.
Follow-up and copies of the
presentations are available on:
www.who.int/medical_devices/
Also recommended is the
video commissioned by WHO and
launched at the conference on
‘The Power and Potential of
Medical Devices’. This is
available online at
http://www.rockhopper.tv/progra
mmes/450 and will be a useful
resource in communicating the
vital role medical devices play in
healthcare.
(Edited by Andrew Gammie from
IFMBE report by Marc Nyssen)
First Global Forum on Medical Devices
WEB RESOURCES
This is a great resource. Visit www.learningradiology.com. It is directed to radiology residents but is a great resource for medicalphysicists.It includes a museum with great pictures (use them for teaching,presentations, etc.), and there is a section for medical students which
includes ‘Recognizing’ and ‘Must See’ sections. The images are useful as they present basic anatomy and pathology. The site was put together by William Herring, MD, Vice Chair andResidency Program Director at Albert Einstein Medical Center inPhiladelphia.
Visit http://e-radiography.net/ for a file of hundreds, if notthousands, of pictures associated with radiology and medicalphysics. There are hundreds of x-ray images such as lumbar spine,
CT, MRI, etc.Click on x-ray tubes to find severalhundred pictures of x-ray tubes.
LEARNING RADIOLOGY
XRAY2000 NICK’S WEBSITE
Bangkok, Thailand, 9th–11th September 2010
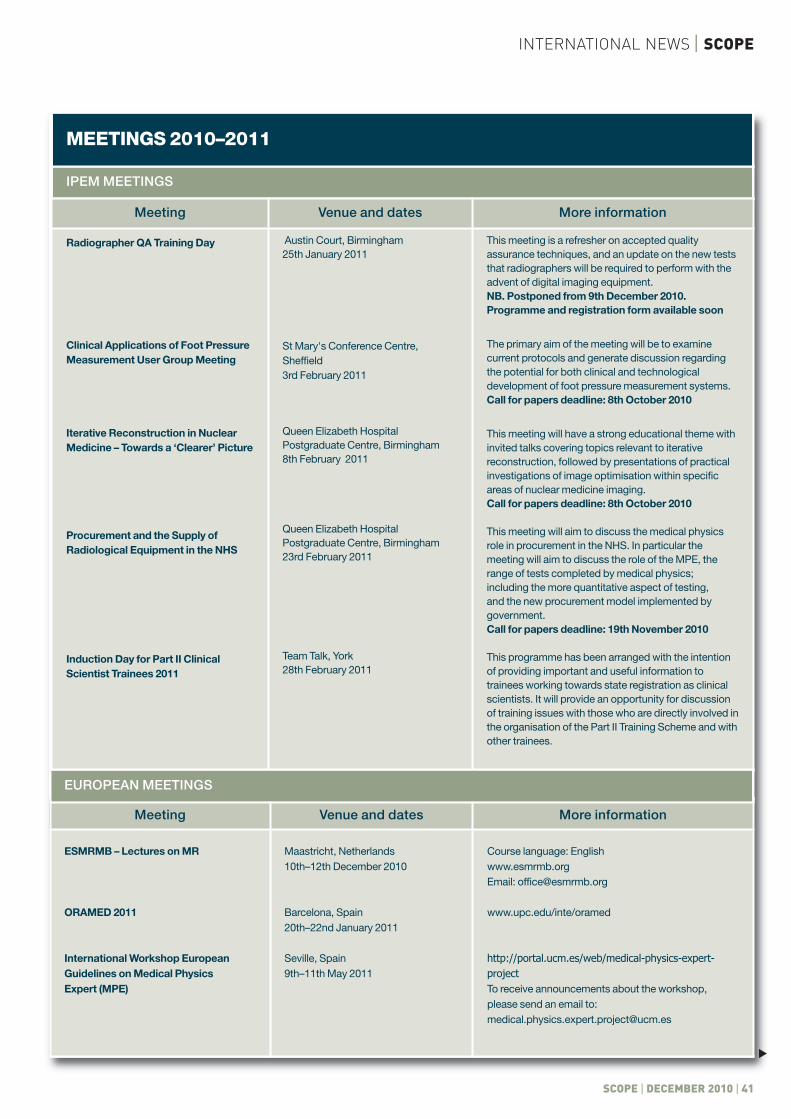
SCOPE | DECEMBER 2010 | 41
INTERNATIONAL NEWS | SCOPE
MEETINGS 2010–2011
IPEM MEETINGS
Meeting Venue and dates More information
Radiographer QA Training Day
Clinical Applications of Foot PressureMeasurement User Group Meeting
Iterative Reconstruction in NuclearMedicine – Towards a ‘Clearer’ Picture
Procurement and the Supply ofRadiological Equipment in the NHS
Induction Day for Part II ClinicalScientist Trainees 2011
Austin Court, Birmingham 25th January 2011
St Mary's Conference Centre,Sheffield3rd February 2011
Queen Elizabeth HospitalPostgraduate Centre, Birmingham8th February 2011
Queen Elizabeth HospitalPostgraduate Centre, Birmingham23rd February 2011
Team Talk, York28th February 2011
This meeting is a refresher on accepted qualityassurance techniques, and an update on the new teststhat radiographers will be required to perform with theadvent of digital imaging equipment.NB. Postponed from 9th December 2010.Programme and registration form available soon
The primary aim of the meeting will be to examinecurrent protocols and generate discussion regardingthe potential for both clinical and technologicaldevelopment of foot pressure measurement systems. Call for papers deadline: 8th October 2010
This meeting will have a strong educational theme with invited talks covering topics relevant to iterativereconstruction, followed by presentations of practicalinvestigations of image optimisation within specificareas of nuclear medicine imaging.Call for papers deadline: 8th October 2010
This meeting will aim to discuss the medical physicsrole in procurement in the NHS. In particular themeeting will aim to discuss the role of the MPE, therange of tests completed by medical physics;including the more quantitative aspect of testing,and the new procurement model implemented bygovernment.Call for papers deadline: 19th November 2010
This programme has been arranged with the intention of providing important and useful information totrainees working towards state registration as clinicalscientists. It will provide an opportunity for discussionof training issues with those who are directly involved inthe organisation of the Part II Training Scheme and withother trainees.
Meeting Venue and dates More information
ESMRMB – Lectures on MR
ORAMED 2011
International Workshop EuropeanGuidelines on Medical Physics Expert (MPE)
Maastricht, Netherlands10th–12th December 2010
Barcelona, Spain20th–22nd January 2011
Seville, Spain9th–11th May 2011
Course language: Englishwww.esmrmb.org Email: [email protected]
www.upc.edu/inte/oramed
http://portal.ucm.es/web/medical-physics-expert-projectTo receive announcements about the workshop,please send an email to:[email protected]
EUROPEAN MEETINGS
�

MEETINGS 2011
NORTH AMERICAN MEETINGS
Meeting Venue and dates More information
Society of Nuclear Medicine Mid-Winter Meeting
2nd Annual COMP Winter SchoolQuality and Safety in Radiation Oncology
SPIE Medical Imaging Conference
55th Annual Meeting of the BiophysicalSociety
2011 ABS Winter School:Quality Management inLDR and HDR Brachytherapy
2011 American Brachytherapy Society(ABS) Annual Conference
5th International IEEE EMBS Neural Engineering Conference
Cancer Imaging and Radiation TherapySymposium
ACMP Annual Meeting
Conference of Radiation Control ProgramDirectors (CRCPD) Annual Meeting
Society for Imaging Informatics inMedicine (SIIM) Annual Meeting
AAPM+COMP Annual Meeting American Association of Physicists inMedicine and the Canadian Organizationof Medical Physicists
Asian Oncology Summit 2011
18th International Conference on MedicalPhysics: Science and Technology forHealth for All (ICMP 2011)
Palm Springs, CA20th–23rd January 2011
Mont Tremblant, Canada30th January–3rd February 2011
Lake Buena Vista, FL 12th–17th February 2011
Baltimore, MD5th–9th March 2011
Palm Beach, FL11th–12th March 2011
San Diego, CA14th–16th April 2011
Cancun, Mexico27th April–1st May 2011
Atlanta, GA29th–30th April 2011
Chattanooga, TN30th April–3rd May 2011
Austin, TX16th–19th May 2011
Washington, DC2nd–5th June 2011
Vancouver, Canada31st July–4th August 2011
Hong Kong8th–10th April 2011
Porto Alegre, Brazil17th–20th April 2011
www.snm.org/mwm2011
http://www.medphys.ca/
http://spie.org/x12166.xml
http://www.biophysics.org/Default.aspx?alias=www.biophysics.org/2011meeting
http://www.americanbrachytherapy.org/meetings/2011_winterschoolpromoflyer.pdf
http://www.americanbrachytherapy.org/meetings/2011_callforabstracts.pdf
http://ne2011.embs.org/
http://www.cancerimagingandrtsymposium.org/
http://acmp.org/
http://www.crcpd.org/meetings.aspx
http://www.siimweb.org/index.cfm?id=6934
http://www.aapm.orghttp://www.medphys.ca/
http://www.asianoncologysummit.com/
http://www.pucrs.br/fisica/icmp2011/
REST OF THE WORLD
42 | DECEMBER 2010 | SCOPE
SCOPE | INTERNATIONAL NEWS
�
IPEM EXAM RESULTS CLINICAL TECHNOLOGISTS
Congratulations to the following who have recently been successful in the IPEM Viva Voce examinations for the Clinical Technologist Certificate andDiploma of IPEM DipIPEM(T)
IPEM EXAM RESULTS
Name Training centre Result Examination
Jenna BankheadSarah-Louise BlackDavid Blane Michelle BradfordCaoimhghin CampfieldRoss ChildsVictoria CookeUrsula DalyGemma DavisDavid DonovanStephanie GoddardMatt GoslingAlexandra Hallett Anthony HartleyKirsty LeePaul McDonaldKimberley MouldAlexander NealeCatherine NelsonAlexandra ParryClaire PuzeyMichelle SatterthwaiteHesham SaudAndrew ScottLaura SmythLianne YouleHelen FarrowAdrian McNairn
Royal Victoria HospitalNICC Belfast City HospitalGartnavel General HospitalNew Cross HospitalRoyal Victoria HospitalGlenfield HospitalFreeman HospitalNICC Belfast City HospitalUniversity Hospital North StaffordshireAddenbrookes HospitalAddenbrookes HospitalDerriford HospitalSingleton HospitalAddenbrookes HospitalUniversity Hospitals Coventry & WarwickshireInverclyde Royal HospitalDiana Princess of Wales HospitalCity Hospital NHS TrustNICC Belfast City HospitalBristol Haematology and Oncology CentreRoyal Shrewsbury HospitalSouthampton General HospitalCastle Hill Hospital, CottinghamRotherham District General HospitalNICC Belfast City HospitalRoyal Hallamshire Hospital Castle Hill Hospital, CottinghamDumfries & Galloway Royal Infirmary
Pass with MeritPass with DistinctionPassPassPass with MeritPass with MeritPassPass with DistinctionPass with MeritPassPass with MeritPass with DistinctionPassPassPass with DistinctionPassPass with DistinctionPass with DistinctionPass with DistinctionPass with MeritPass with MeritPass Pass with DistinctionPass with DistinctionPass with DistinctionPass with DistinctionPass with MeritPass
DiplomaDiplomaDiplomaCertificateDiplomaCertificateDiplomaDiplomaCertificateDiplomaCertificateCertificateDiplomaCertificateCertificateDiplomaCertificateDiplomaDiplomaCertificateDiplomaCertificateDiplomaCertificateDiplomaCertificateDiplomaDiploma
To advertise in Scopecall Bhupinder on
01727 739 182
or email [email protected]
SCOPE | DECEMBER 2010 | 43
MEMBERS’ NEWS | SCOPE
�
SCOPE | MEMBERS’ NEWS
44 | DECEMBER 2010 | SCOPE
Congratulations to the following who have recently been successful in the IPEM Viva Voce examinations for the Clinical Science Diploma of IPEMDipIPEM(S)
IPEM EXAM RESULTS
Name Training centre Grade
Nafisa Ajmal
Clare Antoine
John Archer
Christopher Baker
Gary Barfield
David Broadbent
Patrick Conaghan
Helen Davies
Christine Denby
Benjamin Earner
Katie Edmunds
Mark Edwards
Katie Eyre
Amanda Fender
Matthew Firth
Clare Francis
Alastair Gemmell
Catherine Heyward
Sarah Higgins
Kirsten Hodgson
Nick Holtom
Holly Jenkins
Emily Joel
Daniel Johnson
Adam Jones
Sarah Kilfeather
Robert Lievesley
Arkadiusz Mazurek
Matthew Memmott
Jill Merrett
Leila Nichol
Jonathan Noble
Aidan O’Brien
Jim O’Doherty
Joanne Page
Philip Parsons
Craig Paterson
David Paynter
Laura Perry
Wojciech Polak
John Powell
David Randall
Maxwell Robinson
Martin Rojas Fisher
Katie Sanders
Hayley Snelling
Richard Speight
Elizabeth Tunnicliffe
Ceri Williams
Elaine Woods
Royal Berkshire NHS Foundation Trust
Walsgrave Hospital NHS Trust
The Christie NHS Foundation Trust
Royal Free Hospital
Lincoln County Hospital
Leeds General Infirmary
King’s College Hospital NHS Foundation Trust
Walsgrave Hospital NHS Trust
Royal Liverpool University Hospital
Royal Free Hospital
St George’s Hospital
Singleton Hospital
Addenbrooke’s Hospital NHS Trust
Leeds General Infirmary
Royal Hallamshire Hospital
University of Aberdeen
University Hospital of Aberdeen
Singleton Hospital
Walsgrave Hospital NHS Trust
Southampton General Hospital
Gloucestershire Royal Hospital
United Hospital of Wales
King’s College Hospital NHS Foundation Trust
The Christie NHS Foundation Trust
Royal Free Hospital
Queen Mary’s Hospital
Royal Berkshire NHS Foundation Trust
United Hospital of Wales
Lincoln County Hospital
Queen Alexandra Hospital
University Hospital of Aberdeen
King’s College Hospital NHS Foundation Trust
University Hospital of Aberdeen
Royal Surrey County Hospital
Royal Free Hospital
United Hospital of Wales
University Hospital of Aberdeen
Leeds General Infirmary
Royal Free Hospital
Royal Surrey County Hospital
Royal Free Hospital
Royal Hallamshire Hospital
Royal Berkshire NHS Foundation Trust
Royal Free Hospital
Royal Liverpool University Hospital
Royal Sussex County Hospital
Leeds General Infirmary
Addenbrooke’s Hospital NHS Trust
The Christie NHS Foundation Trust
Royal Free Hospital
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass
Pass with Merit
Pass
Pass
Pass
Pass
Pass with Merit
Pass
Pass with Merit
Pass
Pass
Pass
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass with Merit
Pass with Merit
Pass
Pass
Pass with Merit
Pass
Pass with Merit
Pass
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass with Merit
Pass with Merit
Pass
Pass with Merit
Pass with Merit
Pass
Pass with Merit
IPEM EXAM RESULTS CLINICAL SCIENTISTS
�

BOOK REVIEWS | SCOPE
SCOPE | DECEMBER 2010 | 45
elcome toanother editionof Scope. In thisissue, we bringyou somereviews fromthe medical
physics genre and and an update on newreports.
After the introduction of our newsection listing ‘New Reports’ in the lastissue, we present you with a review fromSarah Cade of the IAEA Human HealthSeries No. 6: Quality Assurance forSPECT Systems, which members of thenuclear medicine community may finduseful. Marc Miquel uncovers themysteries of sport science with hisreview of Gold Medal Physics – TheScience of Sport. James Stirrup exploresIntroduction to Physics in ModernMedicine, whilst Angela Newing unveilsPhysics of the Human Body.
The ‘Just Published!’ and ‘NewReports’ sections detail recently or soonto be published books and reports,covering medical physics andengineering subjects. If you would liketo review any of the titles (or any othersthat you may have in mind), pleasecontact the joint book review editors.
With our increasing success andgrowing community on theSCOPEBookReviews Ubidesk onlineworkspace, we would like to encouragereaders to join. The workspace lists allbooks and reports available for review(prior to publication in Scope) andallows you to request books of interest.To join, please drop us an email and wewill send the relevant details for joining.The joint book review editors lookforward to welcoming you to the onlinecommunity.
Last but not least, a big ‘thank you’ toall reviewers who have submittedreviews to Scope in the recent past.Please keep up the good work!
Usman I. Lula([email protected] [email protected])Marium Naeem([email protected])
W
IAEA HUMAN HEALTH SERIES NO. 6: QUALITYASSURANCE FOR SPECT SYSTEMSPublisher: International Atomic Energy Agency(IAEA)ISBN: 978-92-0-103709-1Pages: 249
IAEA Human HealthSeries No. 6: QualityAssurance for SPECTSystemsThis book presents the recommendations ofthe International Atomic Energy Agency forroutine and acceptance testing of gammacameras. The tests are divided intoconvenient sections which cover basicgamma camera tests, whole body imaging,SPECT systems and multi-head systems aswell as the computer system used to controlthe camera and the display system. Theinitial chapter of the book is used to discussarrangements for quality control as well asgeneral care and preventative maintenance.
Each section begins by describing thebasic principles of the imaging techniqueand the relevant components of the camerasystem. This provides a useful introductionwhich would be essential reading formedical physics trainees and other membersof staff who are new to gamma cameratesting as it links the key performancecharacteristics measured to the effect onimage quality and describes the most likelymechanisms for reduction in function.Figures are included which give examples ofthe appearance of some of the defects thatcan be observed; the clarity of figures withsubtle image effects is improved whenviewing the electronic version of the report.
Tables of the recommended tests aregiven with suggested test frequencies andare followed by detailed instructions of howto perform and analyse the tests. Theprocedures for each of the tests are easy tofollow with clear diagrams to enhance thedescription of the set-up where appropriate.The list of tests is very comprehensiveincluding all those recommended by IPEMReport 86 (2003) and the more recent EANMGuidelines (2010), as well as a number oftests not mentioned in these reports. As aguide for acceptance testing this is anexcellent resource covering all the tests thatare likely to be required. However, forroutine testing it is likely to represent asomewhat unrealistic demand on cameraand staff time in many departments. Audits
of current practice for quality assurancetesting in the UK have shown significantvariation in the tests performed at differentcentres; this situation is unlikely to be alteredby this report as departments select the teststhey feel are most relevant to them.
This book is free to download from theIAEA website (http://www-pub.iaea.org/MTCD/publications/PDF/Pub1394_web.pdf), making it a very usefulresource for any nuclear medicinedepartment and an essential reference foranyone preparing to acceptance test a newgamma camera. Medical physicists andtechnologists training in nuclear medicinewould also benefit from review of this text toincrease their understanding of theimportance of quality assurance tests and thepotential impact of sub-optimal performance.
Sarah CadeRoyal United Hospital, Bath
�
Gold Medal Physics –The Science of SportsAdmit it; just like me, you often wonderedwhat all those Sport Science students weredoing and studying. I was hoping to shedsome light on the mystery when I decided toread and review Gold Medal Physics – TheScience of Sports by J. E. Goff, AssociateProfessor of Physics at Lynchburg College.Do I now know more on the subject(s) youmight ask? No; but I did learn a good lesson:nowadays not only shouldn’t you judge abook by its cover (a diver in this case), youshould also not assume too much from a titleand sub-title either. Gold Medal Physics is not atreaty on sport science but more a series ofsport-illustrated mechanics problems with acouple of chapters thrown in at the end onthermodynamics/metabolism andprobabilities/betting, maybe just anafterthought or maybe a good editor’sdecision to justify a more appealing subtitle.
Last but not least, abig ‘thank you’ to allreviewers who havesubmitted reviews toScope in the recent past
”“

46 | DECEMBER 2010 | SCOPE
SCOPE | BOOK REVIEWS
�
INTRODUCTION TO PHYSICS IN MODERNMEDICINES. A. KANEPublisher: Taylor & Francis LtdISBN 13: 978-1584889434Pages: 448
books on medical physics, I find that it canbe difficult sometimes to know exactlywhich to suggest – whilst many goodexamples exist, they can be, on occasion,rather dry. Here, then, is the book that I willnow recommend.
Now in its second edition, AnIntroduction to Physics in Modern Medicine byKane succeeds at the rather difficult task ofdescribing medical physics in plain English.The book, described as ‘a relatively non-mathematical introduction to … applied[medical] physics’, is a distillation of asingle-term course provided to students ofmedicine and professions allied to healthrequiring an elementary background inmedical physics. Interestingly, the firstedition of the book was also (unexpectedly)favoured by physics undergraduateslooking for a more descriptive text as acompanion to those with heaviermathematical content. Undoubtedly, theseare the groups who stand to benefit fromthis book.
The book is divided into chaptersdevoted to, respectively, fibre optics andendoscopy, lasers, ultrasound imaging, x-rays/CT, nuclear medicine, radiotherapyand magnetic resonance imaging. Eachdescribes the physical underpinnings ofthese techniques in simple terms using acombination of clear prose and excellentdiagrams. Equations are kept to a relativeminimum; those that are included areaccompanied by sample calculations forillustration. As the book focusespredominantly on physics, only a handfulof clinical applications are described,usually to highlight the pertinent physicalissues – those looking for details of specificclinical applications will need to lookelsewhere. Each chapter concludes with aset of questions and problems to attempt,although it should be noted that answersare not provided.
Perhaps the only criticism of thisotherwise excellent introductory textbook isthat the layout can be a little overwhelming.Some sections run as long tracts ofuninterrupted prose without any cleardemarcation of separate topic areas. Forinstance, SPECT and PET are covered in asingle section of prose that runs overapproximately 10 pages, with no sub-headings signposting discussions on thedistinct physical aspects of thesetechniques. This might be the result of theformat from which the book is derived, aseach section is written as it might be spokenin a lecture. Although this style is certainlyresponsible for the clarity with which thephysical principles are explained, it makesit rather difficult to pick out sub-topicswhen using the book as a reference.
This criticism aside, the book simplifies
relatively complex concepts forundergraduates and postgraduate non-specialists requiring a conciseunderstanding in medical physics.Although established medical physicstrainees are likely to derive little from thisbook, those considering a career in medicalphysics may wish to explore its contents toconfirm their aspirations. As anintroductory text, it is highlyrecommended.
James Stirrup National Heart and Lung Institute,Imperial College, London & RoyalBrompton and Harefield NHS Trust
The book has a definite American flavourand if like me you are not keen on baseball, itstarts quite badly (surely trying to explainShane Warne’s ball of the century would havebeen more instructive – at least to MikeGatting). It is also quite comical to read theauthor’s defence of David Beckham for onlyfinishing twice runner-up in the FIFA worldplayer award.
The chapter on (soccer) ball trajectories isnot bad in itself but it is easy to find longerand better treaties on the matter, plus thebook was written and published too early toexplain why the Jabulani has a mind of itsown. The book also feels quite cheap and thephotograph budget was only sufficient toinclude a couple of real sport stars, the gapinghole is plugged by the students of the college.
Overall, I cannot say it is a terribly badbook but it is far from being a page-turnerand if you really are into that sort of book youcan find dozens of better ones (fair play to theauthor, he even includes some in hisbibliography). It is probably not an opus foryour popular science library shelves but asChristmas is fast approaching, it could be agood present for a physics teacher trying toengage with male teenagers or a youngrelative who is into sports but cannot see thepoint of physics (he probably still won’t see itafterwards though). As for me, thanks toGoogle Earth, I at least learnt where leafyLynchburg is located but I am not going toreveal it to you, that would spoil one of themost interesting questions raised by thisbook.
Marc E. Miquel
Introduction toPhysics in ModernMedicineWhen I am asked by undergraduates (or,for that matter, by clinical colleagues)whether I know of any good introductory
GOLD MEDAL PHYSICS – THE SCIENCE OFSPORTSJOHN ERIC GOFFPublisher: The John Hopkins University PressISBN-13: 978-0801893223Pages: 232
Physics of the HumanBodyAn ambitious title for a volume with fewerthan 300 pages, but the basic physics ofmotion, circulation, hearing, sight etc. aredescribed with clear line diagrams. Theauthor is Professor of Physics at anAmerican College of Pharmacy, who statesthat the book is based upon his lectures totrainee pharmacists so, inevitably, it isslanted towards their needs rather thanbeing a rigorous treatment of the subject.
There is clear information about theworkings of the human eye and ear withuseful diagrams. I also liked the chapter‘Motion and balance’, with a goodexplanation of muscles and forces. Sometopics such as blood pressure and how itrelates to posture and the movements of theheart are treated in depth in the chapter‘Energy, work and metabolism’. We learnhow air gets into the lungs but not howoxygen gets into the blood (perhaps that ischemistry). In the ‘Drug delivery’ chapterthere is information on the routes by whichdrugs can be administered but, again, noexplanation of their absorption.
Just Published!Science Isn’t Everything: Memoirs of aScientist by Lloyd Kemp (Aspect Design) is acollection of memoirs by OBE-awardedscientist Lloyd Kemp. It is a fruitful journeythrough his life as a London-based hospitalphysicist and includes details of workcarried out at the National PhysicalLaboratory.
Practical MR Physics by Alexander C.Mamourian (Oxford University Press, USA)attempts to explain the basic principles ofMR, including the underlying physics. It canbe used as a helpful guide as it includestopics and clinical case studies such asimaging artifacts. The book would be bestsuited to those in the field of MR imaging orwho are looking to improve their MRknowledge.
Mathematical and Statistical Methods forBioengineering: Applications in MATLABby Michael R. King and Nipa A. Mody(Cambridge University Press) is aimed atbioengineers and is the first book of its kindthat uniquely integrates MATLAB-basednumerical methods with modellingconcepts. The book includes relevantexamples from clinical trials andbioinformatics as well asend of chapter problems.
Introduction to MedicalImaging: Physics,Engineering andClinicalApplications byNadine Barrie Smith and
New Reports� Radiation Safety of Gamma, Electron and
X-ray Irradiation Facilities Specific SafetyGuide. IAEA Safety Standards Series No.SSG-8; 2010.
� Schedules of Provision of the IAEARegulations for the Safe Transport ofRadioactive Material. IAEA SafetyStandard Series No. TS-G-1.6; 2010.
� Radiological Consequences Resultingfrom Accidents and Incidents Involvingthe Transport of Radioactive Materials inthe UK – 2009 Review. Report HPA –CRCE 003. HPA; 2010.
� Patient Safety in Radiotherapy SteeringGroup Activity (November 2007 – March2010), Patient Safety in RadiotherapySteering Group. Report HPA – CRCE 002.HPA; 2010.
� Individual Monitoring Conducted by theHealth Protection Agency in the LondonPolonium-210 Incident, M. R. Bailey et al.Report HPA RPD – 067. HPA; 2010.
� Cancer in the Offspring of FemaleRadiation Workers, Report HPA-RPD-063; 2010.
� Third Analysis of the National Registryfor Radiation Workers: OccupationalExposure to Ionising Radiation in
Relation to Mortality and CancerIncidence, Report HPA-RPD-062; 2010.
� DICOM Image and Data Managementfor Nuclear Medicine, PhysiologicalMeasurements, Radiotherapy andUltrasound, Report 99. IPEM; 2010.
� Guidance on the Measurement and Useof EMF and EMC, Report 98. IPEM; 2010.
� Measurement of the PerformanceCharacteristics of Diagnostic X-RaySystems: Digital Imaging Systems,Report 32, Part VII; 2010.
� Stereotactic Body Radiation Therapy: TheReport of AAPM Task Group 101. MedicalPhysics 2010, Volume 37, No. 8.
� QA for Helical Tomotherapy: Report ofthe AAPM Task Group 148. MedicalPhysics 2010, Volume 37, No. 9.
PHYSICS OF THE HUMAN BODYRICHARD P. MCCALLPublisher: Johns Hopkins University PressISBN-13: 978-0-8018-9456-5Pages: 290 + index
Andrew Webb (Cambridge University Press)covers the basics of all modern imagingtechniques available. The text, whichincludes over 130 end-of-chapter exercises,explores the basic theory, instrumentationand clinical applications of physics andengineering knowledge to medicine, whichmay prove useful to new medical physicistsand engineers.
Quality and Safety in Radiotherapy:Imaging in Medical Diagnosis andTherapy by Todd Pawlicki, Peter Dunscombe,Arno J. Mundt and Pierre Scalliet (Taylor &Francis Ltd) focuses on the safety and qualityaspects of radiotherapy. It is divided intoseven broad categories, which cover topicsincluding quality management andimprovement, and people and quality. Thebook provides an approach to improvingquality within your radiotherapy centre.
Radiopharmaceuticals: Introduction toDrug Evaluation and Dose Estimation byLawerence E. Williams (CRC Press) details thedevelopment process ofradiopharmaceuticals. The text examines thebenefits of these and covers the medicalinternal radiation dose (MIRD) dosimetrysystem. There are a number of examplesincluded, which also discuss topicsincluding PET/CT.
Research Methods for Science by Michael P.Marder (Cambridge University Press) is anintroductory text which covers topics suchas design, analysis and presentation ofscientific projects. This may be a useful textfor scientists and engineers at the beginningof their career as it includes guidelines foraccessing scientific papers as well asdescribing the importance of statistics andits applications.
What Are Gamma-Ray Bursts? by JoshuaBloom (Princeton University Press) comesunder the popular science genre. Forbudding astronomers amongst thephysicists and engineers, this book exploresthe phenomenon that is gamma-ray bursts.The author provides a concise overview ofthe bursts whilst tracing the history behindthe discovery of them.
Adaptive Radiation Therapy: Imaging inMedical Diagnosis and Therapy by X. Allen
Li (CRC Press) is focussed on evolvingareas of radiation therapy and the
optimisation of individual treatmentplans. It brings together contributions
from a number of scientists andincludes clinical examples, whichdemonstrate the application of
adaptive radiation arc therapy fora number of treatment sites.
One of the longer chapters entitled‘Biological effects of nuclear radiation’ offerscomprehensive data on the types of ionisingradiation and how they are produced, butthere is very little about their actual effect oncells or reasoning why cancer cells may bekilled while normal cells can recover, forinstance.
There is a good list of American furtherreading material at the end of the book anda fairly comprehensive index.
Despite my criticisms, here is a bookwhich draws together, in one volume, thevarious ways in which physics is at work inthe body. It provides an overview of thesubject which gives a good insight for A-level students and undergraduatescontemplating medical physics as a career.
Angela NewingGloucestershire NHS Foundation Trust(retired)
BOOK REVIEWS | SCOPE
SCOPE | DECEMBER 2010 | 47
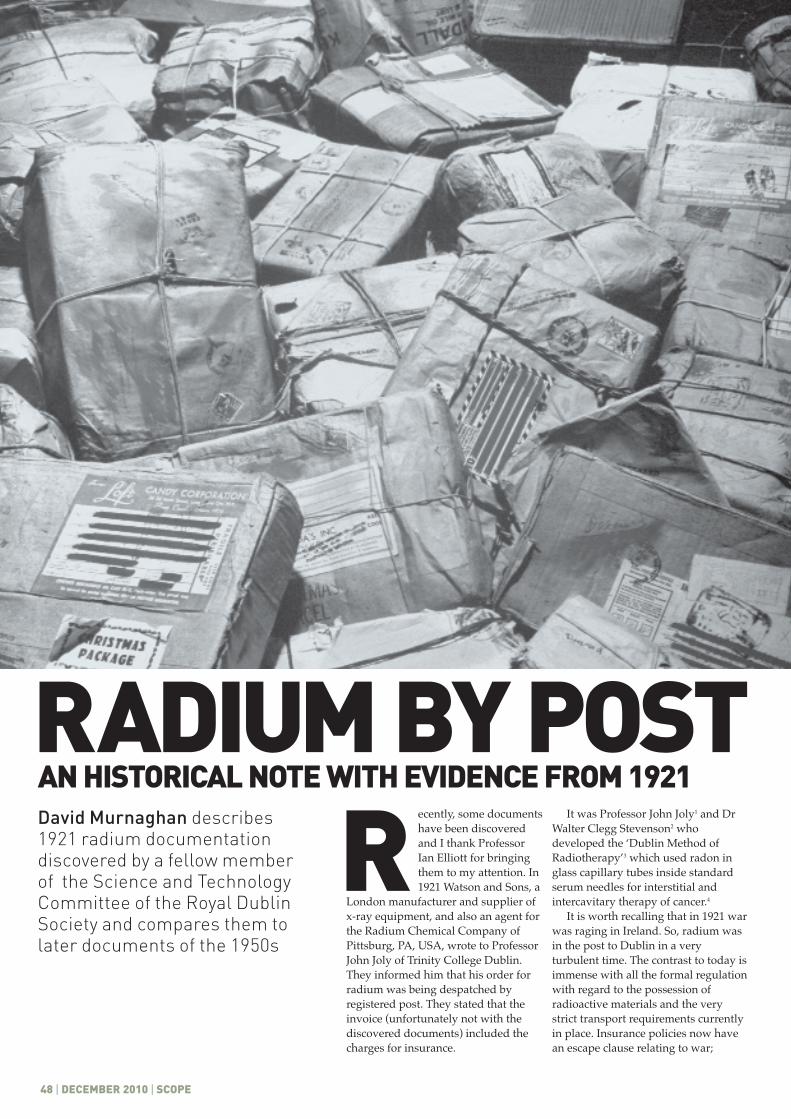
48 | DECEMBER 2010 | SCOPE
ecently, some documentshave been discoveredand I thank ProfessorIan Elliott for bringingthem to my attention. In1921 Watson and Sons, a
London manufacturer and supplier ofx-ray equipment, and also an agent forthe Radium Chemical Company ofPittsburg, PA, USA, wrote to ProfessorJohn Joly of Trinity College Dublin.They informed him that his order forradium was being despatched byregistered post. They stated that theinvoice (unfortunately not with thediscovered documents) included thecharges for insurance.
It was Professor John Joly1 and DrWalter Clegg Stevenson2 whodeveloped the ‘Dublin Method ofRadiotherapy’3 which used radon inglass capillary tubes inside standardserum needles for interstitial andintercavitary therapy of cancer.4
It is worth recalling that in 1921 warwas raging in Ireland. So, radium wasin the post to Dublin in a veryturbulent time. The contrast to today isimmense with all the formal regulationwith regard to the possession ofradioactive materials and the verystrict transport requirements currentlyin place. Insurance policies now havean escape clause relating to war;
David Murnaghan describes1921 radium documentationdiscovered by a fellow memberof the Science and TechnologyCommittee of the Royal DublinSociety and compares them tolater documents of the 1950s
RRADIUM BY POSTAN HISTORICAL NOTE WITH EVIDENCE FROM 1921
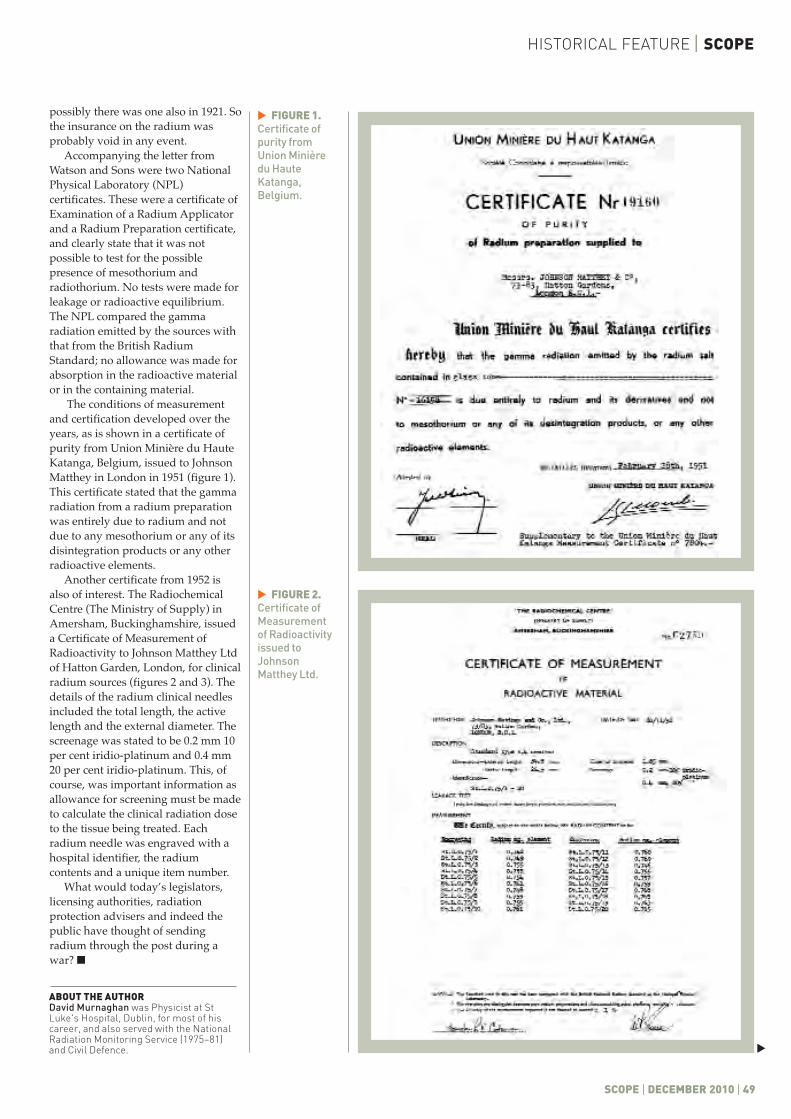
HISTORICAL FEATURE | SCOPE
SCOPE | DECEMBER 2010 | 49
possibly there was one also in 1921. Sothe insurance on the radium wasprobably void in any event.
Accompanying the letter fromWatson and Sons were two NationalPhysical Laboratory (NPL)certificates. These were a certificate ofExamination of a Radium Applicatorand a Radium Preparation certificate,and clearly state that it was notpossible to test for the possiblepresence of mesothorium andradiothorium. No tests were made forleakage or radioactive equilibrium.The NPL compared the gammaradiation emitted by the sources withthat from the British RadiumStandard; no allowance was made forabsorption in the radioactive materialor in the containing material.
The conditions of measurementand certification developed over theyears, as is shown in a certificate ofpurity from Union Minière du HauteKatanga, Belgium, issued to JohnsonMatthey in London in 1951 (figure 1).This certificate stated that the gammaradiation from a radium preparationwas entirely due to radium and notdue to any mesothorium or any of itsdisintegration products or any otherradioactive elements.
Another certificate from 1952 isalso of interest. The RadiochemicalCentre (The Ministry of Supply) inAmersham, Buckinghamshire, issueda Certificate of Measurement ofRadioactivity to Johnson Matthey Ltdof Hatton Garden, London, for clinicalradium sources (figures 2 and 3). Thedetails of the radium clinical needlesincluded the total length, the activelength and the external diameter. Thescreenage was stated to be 0.2 mm 10per cent iridio-platinum and 0.4 mm20 per cent iridio-platinum. This, ofcourse, was important information asallowance for screening must be madeto calculate the clinical radiation doseto the tissue being treated. Eachradium needle was engraved with ahospital identifier, the radiumcontents and a unique item number.
What would today’s legislators,licensing authorities, radiationprotection advisers and indeed thepublic have thought of sendingradium through the post during awar? �
ABOUT THE AUTHORDavid Murnaghan was Physicist at StLuke's Hospital, Dublin, for most of hiscareer, and also served with the NationalRadiation Monitoring Service (1975–81)and Civil Defence.
FIGURE 1.Certificate ofpurity fromUnion Minièredu HauteKatanga,Belgium.
�
FIGURE 2.Certificate ofMeasurementof Radioactivityissued toJohnsonMatthey Ltd.
�
�
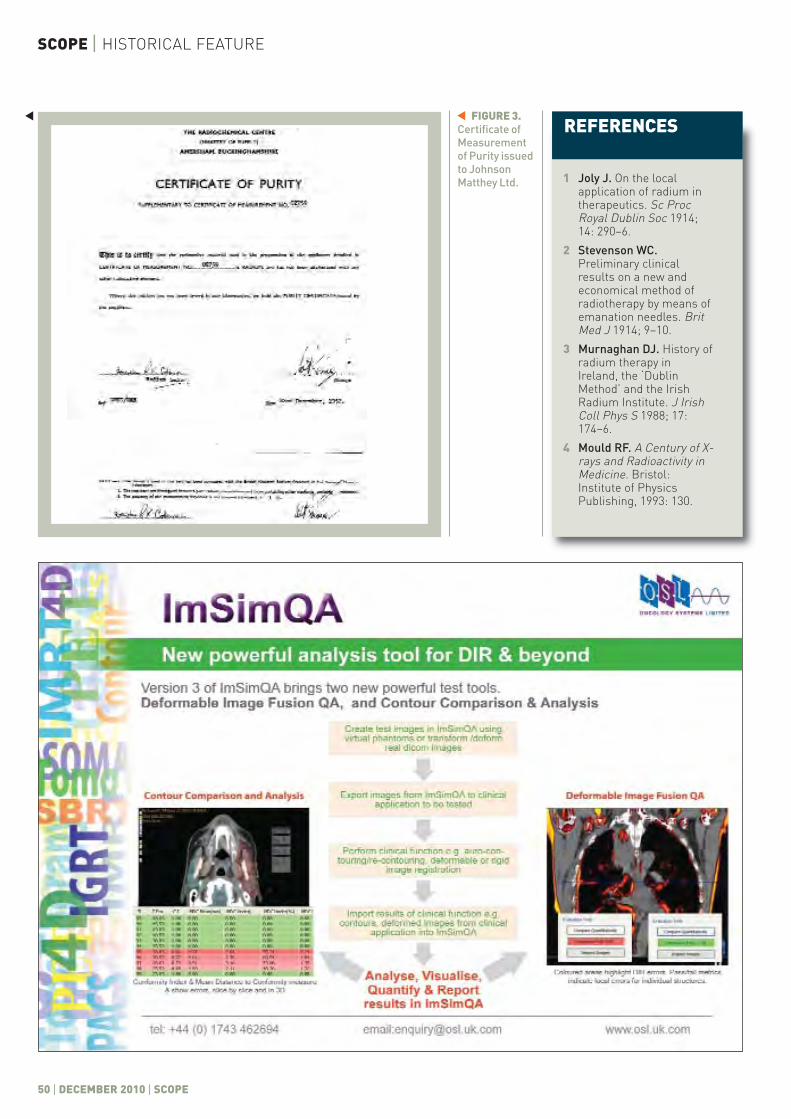
50 | DECEMBER 2010 | SCOPE
SCOPE | HISTORICAL FEATURE
REFERENCES
1 Joly J. On the localapplication of radium intherapeutics. Sc ProcRoyal Dublin Soc 1914;14: 290–6.
2 Stevenson WC.Preliminary clinicalresults on a new andeconomical method ofradiotherapy by means ofemanation needles. BritMed J 1914; 9–10.
3 Murnaghan DJ. History ofradium therapy inIreland, the ‘DublinMethod’ and the IrishRadium Institute. J IrishColl Phys S 1988; 17:174–6.
4 Mould RF. A Century of X-rays and Radioactivity inMedicine. Bristol:Institute of PhysicsPublishing, 1993: 130.
FIGURE 3.Certificate ofMeasurementof Purity issuedto JohnsonMatthey Ltd.
��
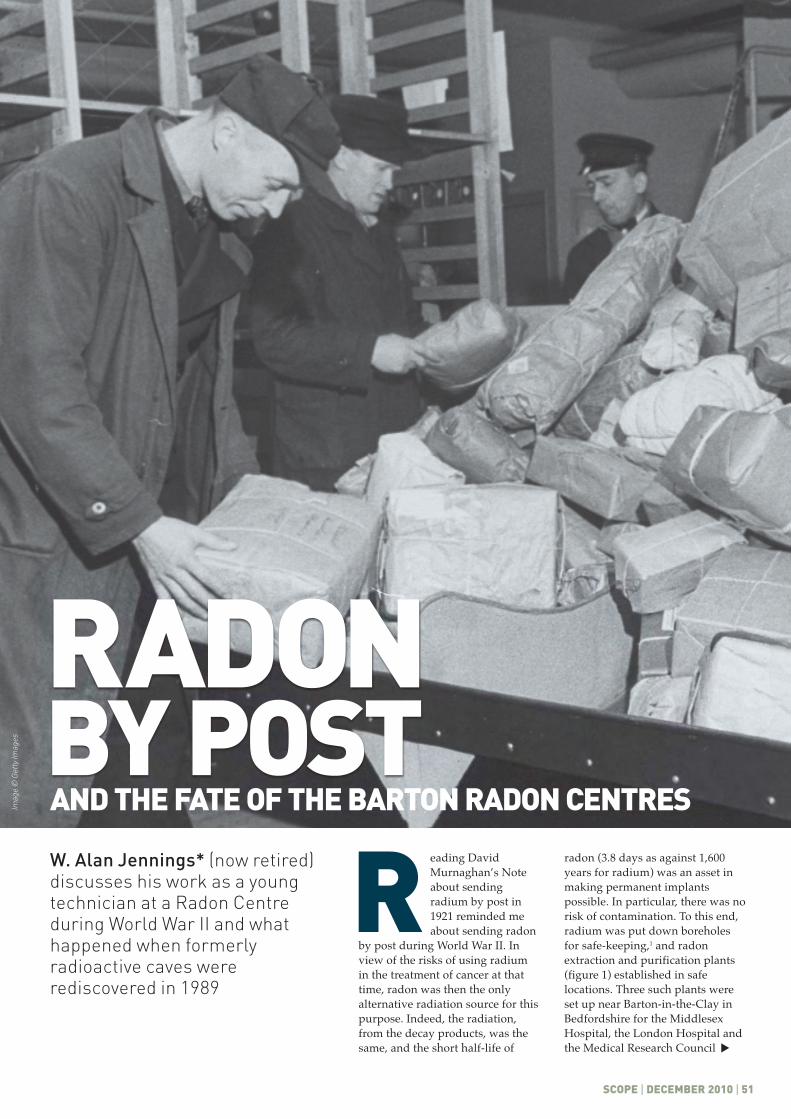
eading DavidMurnaghan’s Noteabout sendingradium by post in1921 reminded meabout sending radon
by post during World War II. Inview of the risks of using radiumin the treatment of cancer at thattime, radon was then the onlyalternative radiation source for thispurpose. Indeed, the radiation,from the decay products, was thesame, and the short half-life of
radon (3.8 days as against 1,600years for radium) was an asset inmaking permanent implantspossible. In particular, there was norisk of contamination. To this end,radium was put down boreholesfor safe-keeping,1 and radonextraction and purification plants(figure 1) established in safelocations. Three such plants wereset up near Barton-in-the-Clay inBedfordshire for the MiddlesexHospital, the London Hospital andthe Medical Research Council
W. Alan Jennings* (now retired)discusses his work as a youngtechnician at a Radon Centreduring World War II and whathappened when formerlyradioactive caves wererediscovered in 1989
R
RADONBY POST
SCOPE | DECEMBER 2010 | 51
AND THE FATE OF THE BARTON RADON CENTRES
�
Imag
e ©
Get
ty Im
ages
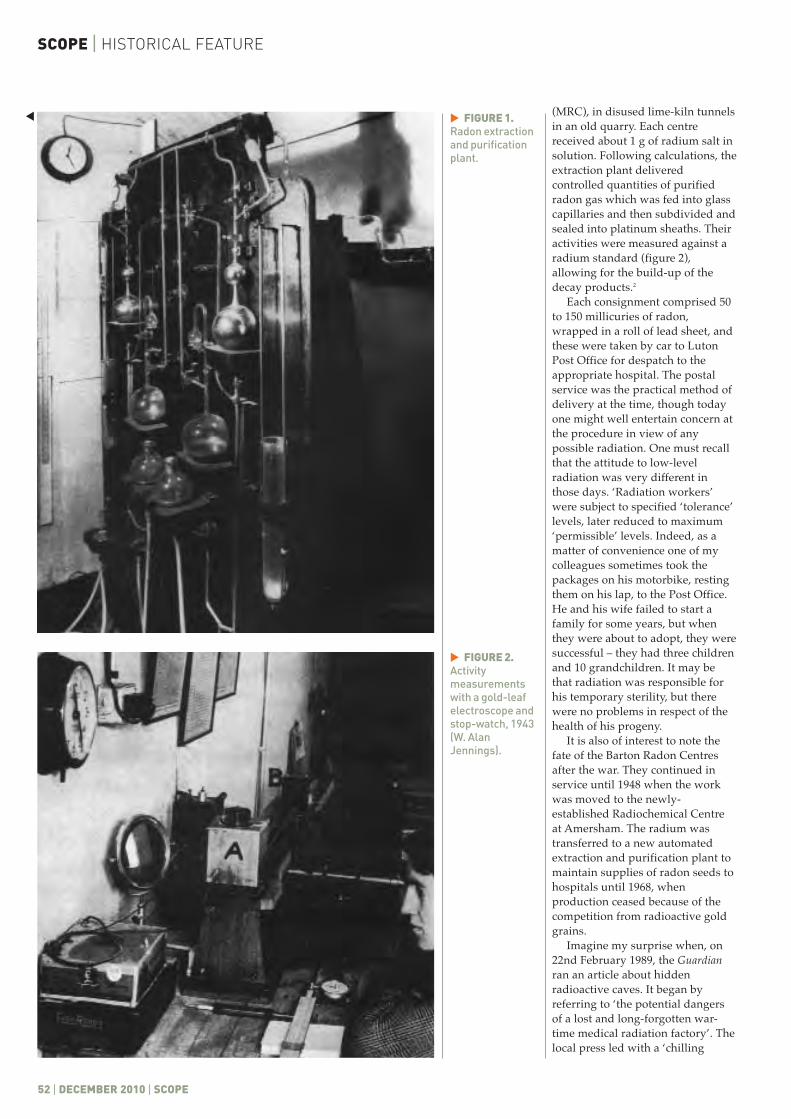
SCOPE | HISTORICAL FEATURE
52 | DECEMBER 2010 | SCOPE
FIGURE 1.Radon extractionand purificationplant.
�
FIGURE 2.Activitymeasurementswith a gold-leafelectroscope andstop-watch, 1943(W. AlanJennings).
�
(MRC), in disused lime-kiln tunnelsin an old quarry. Each centrereceived about 1 g of radium salt insolution. Following calculations, theextraction plant deliveredcontrolled quantities of purifiedradon gas which was fed into glasscapillaries and then subdivided andsealed into platinum sheaths. Theiractivities were measured against aradium standard (figure 2),allowing for the build-up of thedecay products.2
Each consignment comprised 50to 150 millicuries of radon,wrapped in a roll of lead sheet, andthese were taken by car to LutonPost Office for despatch to theappropriate hospital. The postalservice was the practical method ofdelivery at the time, though todayone might well entertain concern atthe procedure in view of anypossible radiation. One must recallthat the attitude to low-levelradiation was very different inthose days. ‘Radiation workers’were subject to specified ‘tolerance’levels, later reduced to maximum‘permissible’ levels. Indeed, as amatter of convenience one of mycolleagues sometimes took thepackages on his motorbike, restingthem on his lap, to the Post Office.He and his wife failed to start afamily for some years, but whenthey were about to adopt, they weresuccessful – they had three childrenand 10 grandchildren. It may bethat radiation was responsible forhis temporary sterility, but therewere no problems in respect of thehealth of his progeny.
It is also of interest to note thefate of the Barton Radon Centresafter the war. They continued inservice until 1948 when the workwas moved to the newly-established Radiochemical Centreat Amersham. The radium wastransferred to a new automatedextraction and purification plant tomaintain supplies of radon seeds tohospitals until 1968, whenproduction ceased because of thecompetition from radioactive goldgrains.
Imagine my surprise when, on22nd February 1989, the Guardianran an article about hiddenradioactive caves. It began byreferring to ‘the potential dangersof a lost and long-forgotten war-time medical radiation factory’. Thelocal press led with a ‘chilling
�
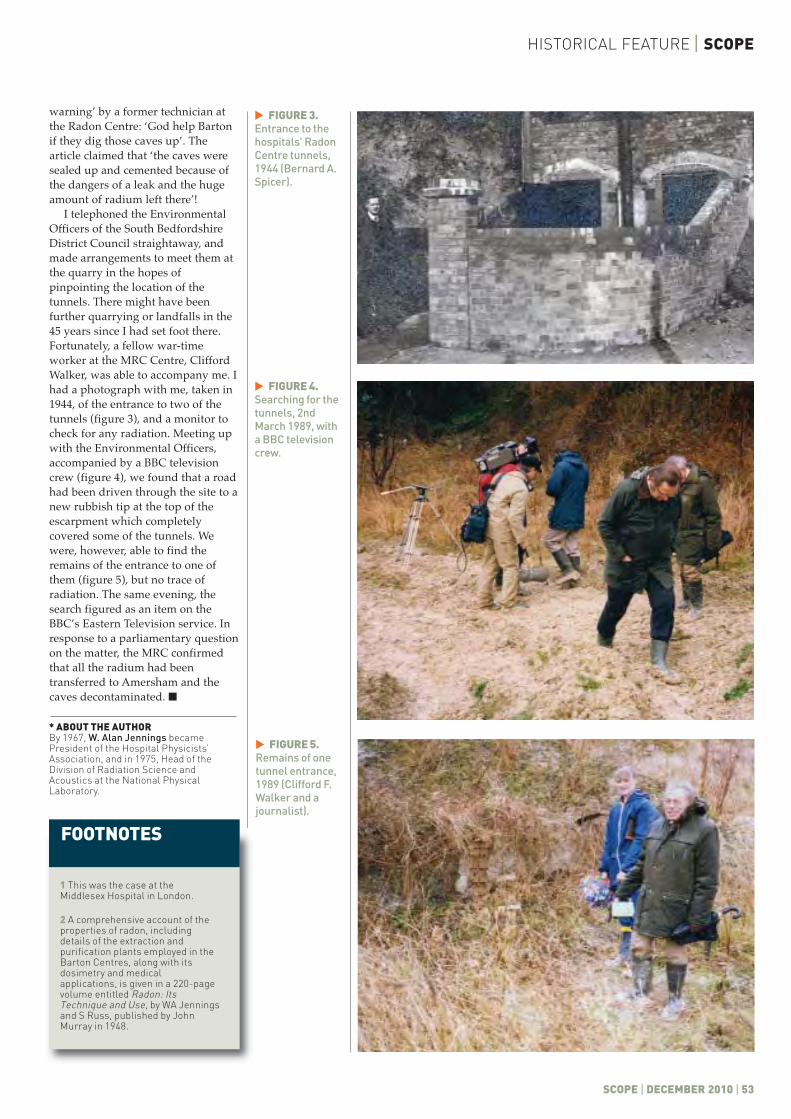
HISTORICAL FEATURE | SCOPE
SCOPE | DECEMBER 2010 | 53
warning’ by a former technician atthe Radon Centre: ‘God help Bartonif they dig those caves up’. Thearticle claimed that ‘the caves weresealed up and cemented because ofthe dangers of a leak and the hugeamount of radium left there’!
I telephoned the EnvironmentalOfficers of the South BedfordshireDistrict Council straightaway, andmade arrangements to meet them atthe quarry in the hopes ofpinpointing the location of thetunnels. There might have beenfurther quarrying or landfalls in the45 years since I had set foot there.Fortunately, a fellow war-timeworker at the MRC Centre, CliffordWalker, was able to accompany me. Ihad a photograph with me, taken in1944, of the entrance to two of thetunnels (figure 3), and a monitor tocheck for any radiation. Meeting upwith the Environmental Officers,accompanied by a BBC televisioncrew (figure 4), we found that a roadhad been driven through the site to anew rubbish tip at the top of theescarpment which completelycovered some of the tunnels. Wewere, however, able to find theremains of the entrance to one ofthem (figure 5), but no trace ofradiation. The same evening, thesearch figured as an item on theBBC’s Eastern Television service. Inresponse to a parliamentary questionon the matter, the MRC confirmedthat all the radium had beentransferred to Amersham and thecaves decontaminated. �
* ABOUT THE AUTHORBy 1967, W. Alan Jennings becamePresident of the Hospital Physicists’Association, and in 1975, Head of theDivision of Radiation Science andAcoustics at the National PhysicalLaboratory.
FIGURE 3.Entrance to thehospitals’ RadonCentre tunnels,1944 (Bernard A.Spicer).
�
FIGURE 4.Searching for thetunnels, 2ndMarch 1989, witha BBC televisioncrew.
�
FIGURE 5.Remains of onetunnel entrance,1989 (Clifford F.Walker and ajournalist).
�
FOOTNOTES
1 This was the case at theMiddlesex Hospital in London.
2 A comprehensive account of theproperties of radon, includingdetails of the extraction andpurification plants employed in theBarton Centres, along with itsdosimetry and medicalapplications, is given in a 220-pagevolume entitled Radon: ItsTechnique and Use, by WA Jenningsand S Russ, published by JohnMurray in 1948.

r Jack Rowan, formerPresident of theHospital Physicists’Association (HPA),died suddenly on 3rdSeptember 2010, aged74, after a very short
illness. He is remembered withadmiration and affection by hiscolleagues in the Department ofClinical Physics and Bioengineering inGlasgow. This department wasestablished by Professor John Lenihanin 1953. With the growing use oftechnologies in health care and withJohn’s drive and vision the departmentexpanded rapidly during the ensuingyears. Medical physics was afascinating field for physics graduatesand so John was able to cherry picksome of the brightest talent. One suchcherry was Jack Rowan, who joinedthe department in 1966, following 2years as an electronics engineer at Barrand Stroud and 3 years at the ScottishResearch Reactor Centre in EastKilbride.
Jack was appointed to lead theClinical Physics team at the Institute ofNeurological Sciences at the SouthernGeneral Hospital. At the time theUniversity of Glasgow was formingthree academic units: Neurosurgeryunder Professor Bryan Jennett,Neurology under Professor IanSimpson and Neuropathology underProfessor Hume Adams. Over the nextthree decades, the academic units andtheir NHS counterparts bonded intoone of the most productive centres inthe world. The glue was Jack’s ClinicalPhysics section; an NHS unitembedded in a university clinicalsetting.
One factor that made his leadershipso special was his ability to collaboratewith clinical academic colleagues. Thepivotal role of technologies in researchensured that Jack’s Clinical Physicssection was involved in a broad rangeof activity, including ICP, EEG, EMG,
imaging and cerebral blood flowmeasurement. The latter was based onthe 133Xenon washout technique, whichhad been pioneered by Niels Lassen inDenmark and Walter Obrist in theUSA. Jack and Bryan Jennett took thistechnique into the operating theatreand developed it for use during carotidartery ligation surgery. This is just oneillustration of a theme that was centralto Jack’s philosophy; the emphasis onclinical value.
Jack was a major player in the teamthat brought the first clinical CTscanner (the EMI scanner) and the firstcommercial MRI scanner to Scotland.Physics was certainly fun in thosedays, when devices could be modifiedby hospital-based staff. Jack built up ahappy, effective and internationallyrespected team. This included manyscientists and technologists who havethemselves gone on to developrewarding careers in medical physicsand who owe so much to Jack’stutorage. We perhaps didn’t know it atthe time, but he was the one who builtup the research funds to support ourearly development; he was the onewho instilled the ‘can do’ attitude; hewas the one who emphasised theimportance of scientific rigour, and hewas the one who set up the invaluableclinical collaborations that wereessential for our career development.The clinicians who worked closelywith Jack include Sir Graham Teasdale,Ian Bone, David Graham, DonaldHadley, Murray Harper, DouglasMiller and John Pickard. We are allindebted to Jack for his skill as ascientist and for his ability to organiseboth people and events.
In addition to his contribution asscientific leader, Jack also fulfilledseveral professional roles, includingbeing Honorary Treasurer of theScottish Branch of the Institute ofPhysics (1972–77), Honorary Secretaryof the HPA (1976–78), Vice-President(1980–82) and then President
SCOPE | OBITUARY
54 | DECEMBER 2010 | SCOPE
JACK ROWAN
DAVID WYPER
Former President of the Hospital Physicists’ Association withrespected research leadership will be sadly missed
D In thatsetting heworkedhonestlyandtirelesslyfor thedepartment
“
”
(1982–84). As Honorary Secretary hewas closely involved in theintroduction of the RegionalRepresentative System, which becamean important link between theMembership and the Council. One ofthe key roles Jack fulfilled as Presidentwas to present the views and interestsof the HPA in discussions with officialsof the Department of Health and theBritish Medical Association. He alsoheld meetings on matters of mutualinterest with many professional bodiesincluding the Royal College ofRadiologists, the College ofRadiographers, the British MedicalUltrasound Society, the BiologicalEngineering Society, the Society ofRadiological Protection and theAssociation of Clinical Biochemists. AsPresident he was Chairman of theEducation Sub-committee and amember of the ProfessionalCommittee. He was also on theeditorial boards of Physics in Medicineand Biology and Clinical Physics andPhysiological Measurement.
In his role as President of the HPAJack became a Director of the Instituteof Physical Sciences in Medicine. Thiswas formed when the HPA’sprofessional activities were separatedoff from other work that could becounted as a charity. Many newermembers of IPEM will be unaware ofthis very important milestone.
In 1992 Jack left to become DeputyDirector of the department, first underProfessor Joe McKie and then underProfessor Alex Elliott. In that setting heworked honestly and tirelessly for thedepartment, using his vast experienceto navigate the constant reorganisationwithin the Health Service.
Away from work Jack was alwaysgood company, remembered by all forhis outrageous laugh. We all knewwhen Jack was in the building. Oursympathies are with Jack’s wife Anne,daughters Irene and Joanne andgrandchildren Kirsty and Andrew.


MP3 Maxi MP3-M Standard MP3-T TomoTherapy®
MP3-XS Stereotaxy MP3-P Particle Therapy
Call us at +44 (0)147 6577503 or visit us at www.ptw-uk.com
IMRT QARelativeDosimetry
AbsoluteDosimetryLINAC QA
TomoTherapy is a registered trademark of TomoTherapy Inc.
Making the right choicecan be so easy.
MP3 Water PhantomsLargest variety of application-specific solutions and tank sizes in 1D, 2D and 3D
Fast TPS beam data acquisition with drag & drop task list
Calibration-free high-precision stepping motors without radiation-sensitive feedback
Unique, patented TRUFIX detector positioning system for utmost precision