Embed Size (px)
Citation preview
P
Proton Magnetic Resonance Spectroscopic Imaging and Magnetic Resonance Imaging
Volumetry in the Lateralization of Temporal Lobe Epilepsy: A Series of 100 Patiekts
Fernando Cendes, MD, PhD,* Zografos Caramanos, MA, Frederick Andermann, MD, FranGois Dubeau, MD, and Douglas L. Arnold, MD
Surgery is a safe and effective treatment for drug-resistant temporal lobe epilepsy (TLE). However, bilateral electroen- cephalographic (EEG) abnormalities are frequently present, making presurgical lateralization difficult. New magnetic resonance (MR) techniques can help; proton magnetic resonance spectroscopic imaging (MRSI) can detect and quantify focal neuronal damage or dysfunction based on reduced signals from the neuronal marker N-acetylaspartate, and mag- netic resonance imaging (MRI)-based measurements of amygdala-hippocampal volumes (MRIVol) can improve the de- tection of atrophy of these structures. We performed proton MRSI and MRIVol in 100 consecutive patients with med- ically intractable TLE to determine how well these techniques agreed with the lateralization by extensive EEG investigation. We found that the EEG, MRSI, and MRIVol findings were highly concordant. The MRSI was abnormal in 99 of 100 patients (bilateral in 54%). The MRIVol was abnormal in 86 of 98 patients (bilateral in 28%). We obtained lateralization in 83% of patients using MRIVol alone, in 86% using MRSI alone, and in 90% by combining MRSI and MRIVol (vs 93% lateralization by EEG). MRSI was abnormal in 12 patients with normal MRIVol. The combination of proton MRSI and MRIVol can lateralize TLE accurately and noninvasively in the great majority of patients. By reducing reliance on EEG, these imaging techniques could reduce prolonged presurgical evaluation and make seizure surgery available to more patients.
Cendes F, Caramanos Z, Andermann F, Dubeau F, Arnold DL. Proton magnetic resonance spectroscopic imaging and magnetic resonance imaging volumetry in the lateralization of temporal lobe epilepsy:
a series of 100 patients. Ann Neurol 1997;42:737-746
In recent years there has been an extraordinary increase in interest in the surgical treatment of temporal lobe epilepsy (TLE). Surgical removal of epileptogenic brain tissue is safe and capable of eliminating or greatly re- ducing seizures in 80 to 90% of patients with TLE who fail to respond to medical treatment [l-31. The presurgical assessment of refractory epilepsy has tradi- tionally depended on analysis of clinical seizure pat- terns and a thorough electroencephalographic (EEG) investigation. EEG recording of several of the patient's habitual seizures is usually necessary for seizure-onset localization [4]. Radiological and neuropsychological studies are also important in the presurgical evaluation [4]. When the results of these investigations are not congruent or when scalp EEG recordings are not con- clusive, monitoring with intracranial electrodes may be
From Montreal Neurological Institute, McGill University, Mon- treal, Quebec, Canada.
*Present address: Department of Neurology, University of Campi- nas, UNICAMP, Campinas, SSo Paulo, Brazil.
required [4, 51. The morbidity associated with the im- plantation of intracranial electrodes is low but compa- rable with that of surgery for resection of epileptogenic tissue. The limited availability of these complex inves- tigations and their cost reduce the number of patients who can benefit from surgery [3 , 51.
TLE is usually associated with mesial temporal scle- rosis (MTS) [6-81. Recent advances in magnetic reso- nance imaging (MRT) have enabled the detection of structural abnormalities in most patients with intracta- ble TLE. MRI abnormalities in MTS include atrophy or abnormal T2-weighted signals in the hippocampus, amygdala, or both [9-201. MRI volumetric analysis (MRIVol) of temporal lobe structures in patients with TLE has been accurate in detecting volume reduction of mesial structures in most patients with MTS, as
Received Jan 10, 1997, and in revised form Mar 19 and JuI 15. Accepted for publication Jul 17, 1997.
Address correspondence to Dr Arnold, Montreal Neurological Hos- pital and Institute, 3801 University St, Montreal, Quebec, Canada H3A 284.
Copyright 0 1997 by the American Neurological Association 737

demonstrated by subsequent histopathology [9-12, 16, 17, 2 11. However, there remains a significant propor- tion of patients with TLE in whom no MRI changes can be detected.
Unlike conventional M R I , which provides structural information based on signals from water, proton mag- netic resonance spectroscopic imaging (MRSI) provides spatially encoded chemical information, thus enabling the noninvasive assay of regional chemical composition [22-251. Proton magnetic resonance spectra of normal human brain reveal a major resonance at 2.0 parts per million (ppm), from N-acetyl groups that originate largely from N-acetylaspartate (NAA), a compound lo- calized exclusively in neurons a n d neuronal processes [26, 271. Recent proton MRS studies have shown re- duced signals from NAA, reflecting focal neuronal loss or damage i n most patients with TLE [23, 28-35]. Thus, proton MRSI has promise for becoming a n im- portant part of the study of TLE.
We studied a large series of patients with TLE being evaluated for seizure surgery, t o determine how lateral- ization based on proton MRSI and MRIVol alone o r in combination would concur with lateralization by EEG.
Patients and Methods We studied 100 consecutive epileptic patients being evalu- ated for medically refractory TLE who had no mass lesions on conventional MRI. Accurate identification of the type and localization of the seizures was determined by a compre- hensive evaluation including a detailed history and neurolog- ical examination, serial EEGs with sphenoidal electrodes, and intensive video-EEG telemetry for recording of seizures [2, 41.
Informed consent was obtained from all subjects. This study is part of a research project approved by the Ethics Review Committee of the Montreal Neurological Institute and Hospital.
Electroencephalographic Investigation Prolonged EEG recordings, using the International 10-20 system including sphenoidal electrodes, and long-term video- EEG monitoring were performed initially to record at least three habitual seizures in all patients. If discrepancies arose between the localization of ictal and interictal abnormalities, if EEG seizure discharges could not be localized due to movement or muscle artifacts, or if ictal behavioral manifes- tations strongly indicated a possible seizure generator in ex- tratemporal structures (for example, elementary visual hallu- cinations), patients underwent intracranial EEG recordings with stereotaxically implanted depth electrodes (SEEG). In these patients, the lateralization was defined according to the ictal onsets during SEEG investigation. Twenty patients un- derwent SEEG investigation because the extracranial EEG recordings did not provide clear localization or lateralization of seizure onset. All these patients had SEEG seizure onsets in the temporal lobe regions.
Patients were classified according to the localization of
EEG seizure onsets preceding the first clinical manifestations as (1) unilateral Left (L) or Right (R), if more than 90% of ictal onsets were unilateral or clearly lateralized to the left or right side, respectively; (2) L > R or R > L, if more than 70% of ictal onsets lateralized to the left or right side, re- spectively; or (3) bilateral (L = R), if less than 70% of ictal onsets lateralized to one side.
The electroencephalographers were unaware of the MRSI and MRIVol results before they reported the EEG findings.
Proton Magnetic Resonance Spectroscopic Imaging Conventional MRI scans, as well as two-dimensional proton MRSI scans, were acquired by using either a 1.5-T ACS I1 or 111 imaging/spectroscopy system (Philips Medical Systems, Best, The Netherlands).
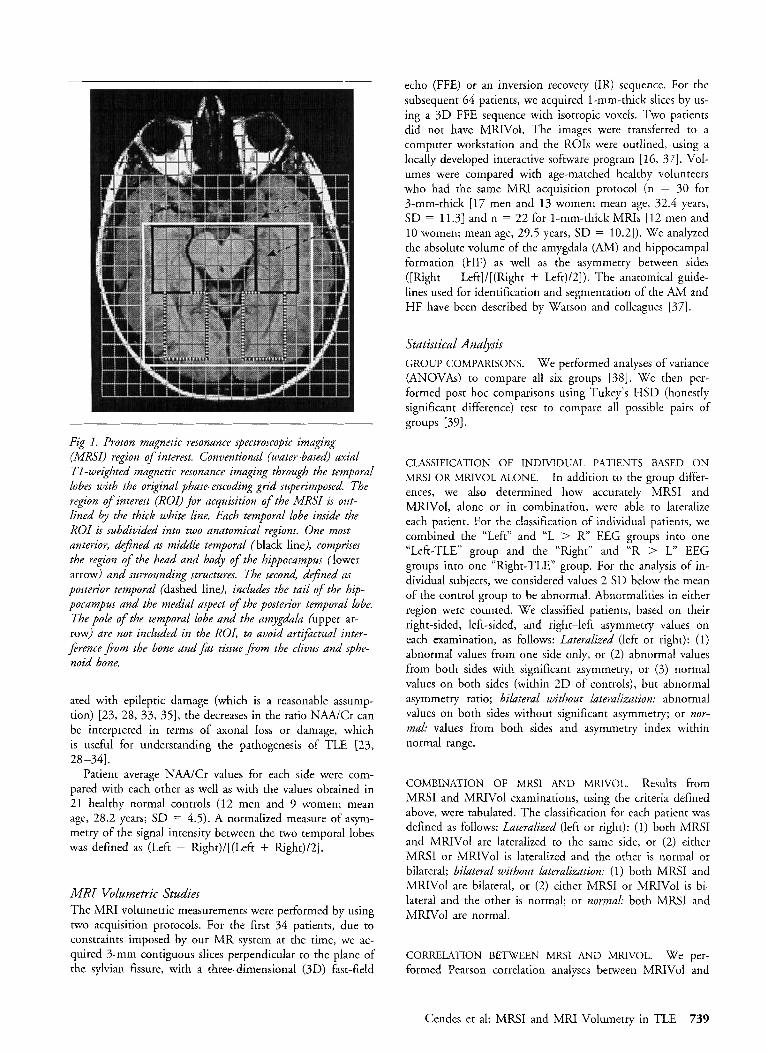
After scout images in axial and sagittal planes, multislice spin echo MRIs (repetition time [TR] 2,000 msec, echo time [TE] 30 msec) were obtained in the transverse plane along the axis of the temporal lobes and in the coronal plane per- pendicular to the axis of the sylvian fissure. A large region of interest (ROI) behind the clivus, including both temporal lobes and excluding bone, was defined for selective excitation before phase encoding for the proton MRSI. The ROI was oriented in a similar position for all examinations to cover the entire extension of both hippocampi (85-100 mm left- right X 75-95 mm anteroposterior X 20-mm thickness) (Fig 1). A water-suppressed proton MRSI was obtained from that ROI by using a 90"-180"-180" pulse sequence with a 2-second interpulse delay (TR 2,000 msec, T E 272, 250 X 250-mm field of view [FOV], 32 X 32 phase-encoding steps), followed by a proton MRSI without water suppres- sion (TR 850, T E 272, 250 X 250-mm FOV, 16 X 16 phase-encoding steps). After zero-filling the latter to 32 X 32 profiles, the water-suppressed MRSI was divided by the non- water suppressed MRSI to correct for artifacts resulting from magnetic field inhomogeneity. The resulting time domain signal was left shifted and subtracted from itself to improve water suppression [36]. This reduces the amplitude of creat- inine (Cr) as well as water and results in relatively high ratios of NAA/Cr; however, this is consistent for all the control data and patient data. To enhance the resolution of the spec- tral peaks, a Lorenzian-to-Gaussian transformation was ap- plied before Fourier transformation in three dimensions. The nominal voxel size in plane was approximately 8 X 8 mm and 12 X 12 mm after K-space filtering.
Resonance intensities on MRSIs were determined from peak areas by integration, using locally developed software. The values for NAA, choline (Cho), Cr, and NAA/Cr were determined for the middle (Mid) and posterior (Post) regions of each temporal lobe by averaging 12 i 3 spectra in each region (Figs 1 and 2). We divided the temporal lobes into two anatomical regions, to avoid averaging too many voxels and to increase the likelihood of detecting more focal abnor- malities. Spectra were excluded from the analyses if they were artifactually broadened (ie, full width at half maximum > 10 Hz) or if the Cho and Cr peaks were not resolved.
The intensity ratio NAA/Cr was used to simplify quanti- tation across patients. The observations do not depend on Cr being a stable internal reference. However, if Cr is assumed to be stable or only slightly changed in brain regions associ-
738 Annals of Neurology Vol 42 No 5 November 1997
echo (FFE) or an inversion recovery (IR) sequence. For the subsequent 64 patients, we acquired 1-mm-thick slices by us- ing a 3D FFE sequence with isotropic voxels. Two patients did not have MRIVol. The images were transferred to a computer workstation and the ROIs were outlined, using a locally developed interactive software program [ 16, 371. Vol- umes were compared with age-matched healthy volunteers who had the same MRI acquisition protocol (n = 30 for 3-mm-thick [17 men and 13 women; mean age, 32.4 years, SD = 11.31 and n = 22 for 1-mm-thick MRIs [ l a men and 10 women; mean age, 29.5 years, SD = 10.21). We analyzed the absolute volume of the amygdala (AM) and hippocampal formation (HF) as well as the asymmetry between sides ([Right - Left]/[(Right + Left)/2]). The anatomical guide- lines used for identification and segmentation of the AM and HF have been described by Watson and colleagues [37].
Fig 1. Proton magnetic resonance spectroscopic imaging (MRSI) region of interest. Conventional (water-based) axial TI-weighted magnetic resonance imaging through the temporal lobes with the original phase-encoding grid superimposed. The region o f interest ( R o d for acquisition of the MRSI is out- lined by the thick white line. Each temporal lobe inside the ROI is subdivided into two anatomical regions. One most anterior, defined as middle temporal (black line), comprises the region uf the head and body of the hippocampus (lower arrow) and surrounding structures. The second, defined as posterior temporal (dashed line), includes the tail of the hip- pocampus and the medial aspect of the posterior temporal lobe. The pole o f the temporal lobe and the amygdala (upper ar- row) are not included in the ROI, to avoid artifctual inter- ference f;om the bone and fat tissue from the clivus and sphe- noid bone.
ated with epileptic damage (which is a reasonable assump- tion) [23, 28, 33, 351, the decreases in the ratio NAAlCr can be interpreted in terms of axonal loss or damage, which is useful for understanding the pathogenesis of TLE [23, 28 -341.
Patient average NAA/Cr values for each side were com- pared with each other as well as with the values obtained in 21 healthy normal controls (12 men and 9 women; mean age, 28.2 years; SD = 4.5). A normalized measure of asym- metry of the signal intensity between the two temporal lobes was defined as (Left - Right)/[(Lefi + Right)/2].
Statistical Analysis GROUP COMPARISONS. We performed analyses of variance (ANOVAs) to compare all six groups [38]. We then per- formed post hoc comparisons using Tukey’s HSD (honestly significant difference) test to compare all possible pairs of groups [391.
CLASSIFICATION OF INDIVIDUAL PATIENTS BASED O N MRSI OR MRIVOL ALONE. In addition to the group differ- ences, we also determined how accurately MRSI and MRIVol, alone or in combination, were able to lateralize each patient. For the classification of individual patients, we combined the “Left” and “L > R EEG groups into one “Left-TLE” group and the “Right” and “R > L” EEG groups into one “Right-TLE” group. For the analysis of in- dividual subjects, we considered values 2 SD below the mean of the control group to be abnormal. Abnormalities in either region were counted. We classified patients, based on their right-sided, left-sided, and right-left asymmetry values on each examination, as follows: Lateralized (left or right): (1) abnormal values from one side only, or (2) abnormal values from both sides with significant asymmetry, or (3) normal values on both sides (within 2 D of controls), but abnormal asymmetry ratio; bilateral without lateralization: abnormal values on both sides without significant asymmetry; or nor- mal: values from both sides and asymmetry index within normal range.
COMBINATION OF MRSI AND MRIVOL. Results from MRSI and MRIVol examinations, using the criteria defined above, were tabulated. The classification for each patient was defined as follows: Lateralized (left or right): (1) both MRSI and MRIVol are lateralized to the same side, or (2) either MRSI or MRIVol is lateralized and the other is normal or bilateral; bilateral without lateralization: ( 1) both MRSI and MRIVol are bilateral, or (2) either MRSI or MRIVol is bi- lateral and the other is normal; or normal: both MRSI and MRIVol are normal,
MRI Volumetric Studies The MRI volumetric measurements were performed by using two acquisition protocols. For the first 34 patients, due to constraints imposed by our M R system at the time, we ac- quired 3-mm contiguous slices perpendicular to the plane of the sylvian fissure, with a three-dimensional (3D) fast-field
CORRELATION BETWEEN MRSI AND MRIVOL. We per- formed Pearson correlation analyses between MRIVol and
Cendes et al: MRSI and MRI Volumetry in TLE 739
Normal control Patient with Left TLE
hgh t Mid TL Left Mid TL Right Mid TL Left Mid TL ~ ~
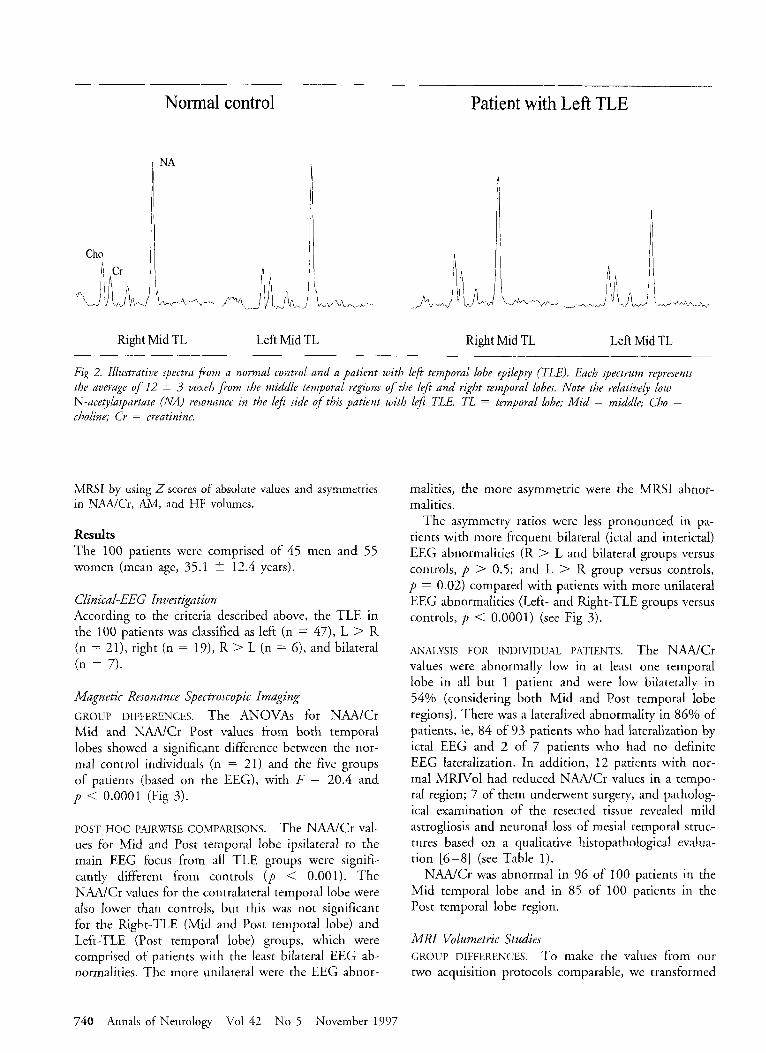
Fig 2. Illustrative spectra fFom a normal control and a patient with left temporal lobe epi1ep.y (TLE). Each spectrum represents the average of 12 5 3 voxels fiom the middle temporal regions of the leJt and right temporal lobes. Note the relatively low N-acetylaspartate (NA) resonance in the lefi side o f this patient with lefi TLE. TL = temporal lobe; Mid = middLe; Cho = choline; Cr = creatinine.
MRSI by using 2 scores of absolute values and asymmetries in N M C r , AM, and HF volumes.
Results The 100 patients were comprised of 45 men and 5 5 women (mean age, 35.1 i 12.4 years).
Clinical-EEG i'kvestigation According to the criteria described above, the TLE in the 100 patients was classified as left (n = 47), L > R (n = 21), right (n = 19), R > L (n = 6 ) , and bilateral (n = 7).
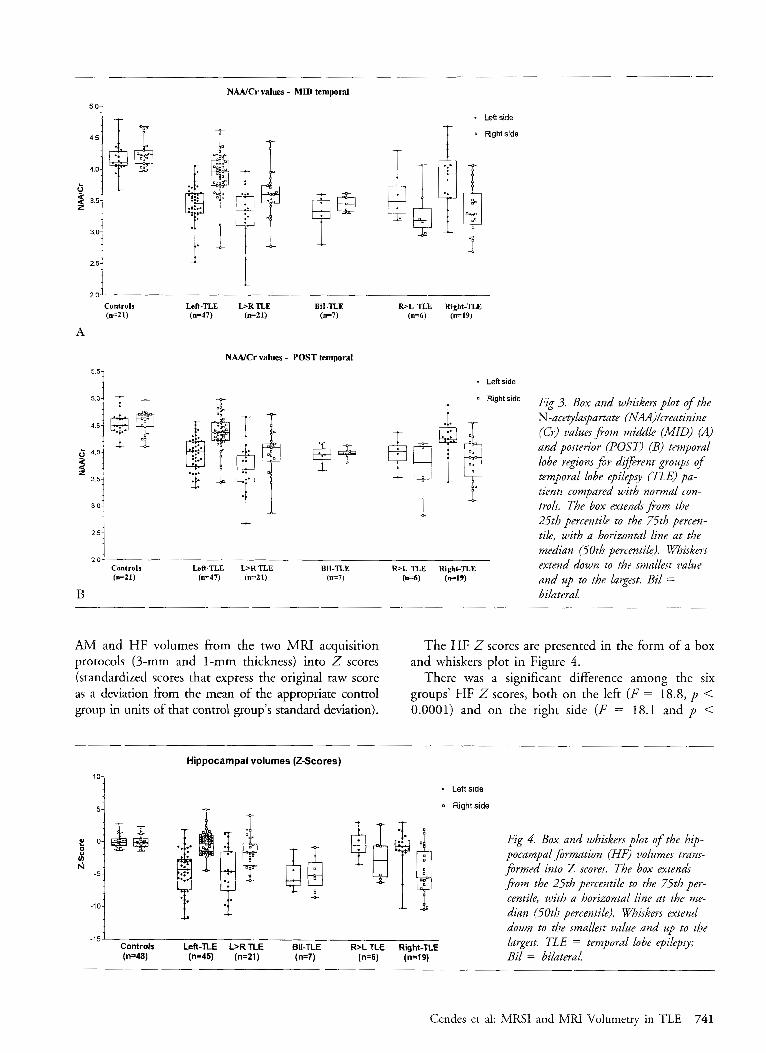
Magnetic Resonance Spectroscopic Imaging GROUP DIFFERENCES. The ANOVAs for NAA/Cr Mid and NAA/Cr Post values from both temporal lobes showed a significant difference between the nor- mal control individuals (n = 21) and the five groups of patients (based on the EEG), with F = 20.4 and p < 0.0001 (Fig 3 ) .
POST HOC PAIRWISE COMPARISONS. The N M C r Val- ues for Mid and Post temporal lobe ipsilateral to the main EEG focus from all TLE groups were signifi- cantly different from controls ( p < 0.001). The NAA/Cr values for the contralateral temporal lobe were also lower than controls, but this was not significant for the Right-TLE (Mid and Post temporal lobe) and Left-TLE (Post temporal lobe) groups, which were comprised of patients with the least bilateral EEG ab- normalities. The more unilateral were the EEG abnor-
malities, the more asymmetric were the MRSI abnor- malities.
The asymmetry ratios were less pronounced in pa- tients with more frequent bilateral (ictal and interictal) EEG abnormalities (R > L and bilateral groups versus controls, p > 0.5; and L > R group versus controls, p = 0.02) compared with patients with more unilateral EEG abnormalities (Left- and Right-TLE groups versus controls, p < 0.0001) (see Fig 3 ) .
ANALYSIS FOR INDIVIDUAL PATIENTS. The N M C r values were abnormally low in at least one temporal lobe in all but 1 patient and were low bilaterally in 54% (considering both Mid and Post temporal lobe regions). There was a lateralized abnormality in 86% of patients, ie, 84 of 93 patients who had lateralization by ictal EEG and 2 of 7 patients who had no definite EEG lateralization. In addition, I2 patients with nor- mal MRIVol had reduced N M C r values in a tempo- ral region; 7 of them underwent surgery, and patholog- ical examination of the resected tissue revealed mild astrogliosis and neuronal loss of mesial temporal struc- tures based on a qualitative histopathological evalua- tion [6-81 (see Table 1).
NAA/Cr was abnormal in 96 of 100 patients in the Mid temporal lobe and in 85 of 100 patients in the Post temporal lobe region.
MRI Volumetric Studies GROUP DIFFERENCES. To make the values from our two acquisition protocols comparable, we transformed
740 Annals of Neurology Vol 42 No 5 November 1997
NAAlCr values - MID temporal
5 0-
4 5-
0' 4.0-
z 3 5-
1 :
3 0-
2 5-
2 0
4.5;
4 0- 4
;E$
2 o i Controls (n=Zl)
0
I f .
-5-
? 0
r 4 .
-10-
A
Fig 4. Box and whiskers plot o f the hip- pocampal formation (HF) volumes trans- firmed into Z scores. The box extends porn the 25th percentile to the 75th per- centile, with a horizontal line at the me- dian (50th percentile). Whiskers extend down to the smallest value and up to the
;& ..-"'
51
f 0
1
* Left side
0 Rght side
Left-TLE b R T L E BiI-TLE (n=47) (IF21) (n=7)
N M C r values - POST temporal
R>L TLE Right-TLE (14) ( ~ 1 9 )
* Left side
Fig 3. Box and whiskers plot o f the N-aceqlaspartate (NAA)/creatinine (Cr) valuesfiom middle (MID) (A) and posterior (POST) (B) temporal lobe regions for different groups of temporal lobe epilepsy (TLE) pa- tients compared with normal con- trols. The box extendsfiom the 25th percentile to the 75th percen- tile, with a horizontal line at the median (50th percentile). Whiskers extend down to the smallest value and up to the largest. Bil = bilateral.
AM and HF volumes from the two MRI acquisition protocols (3-mm and 1-mm thickness) into 2 scores (standardized scores that express the original raw score as a deviation from the mean of the appropriate control group in units of that control group's standard deviation).
The HF 2 scores are presented in the form of a box and whiskers plot in Figure 4.
There was a significant difference among the six groups' HF 2 scores, both on the left (F = 18.8, p < 0.0001) and on the right side ( F = 18.1 and p <
Hippocampal volumes (2-Scores)
t &
- Left side
0 Rightside
Cendes et al: MRSI and MRI Volumetry in TLE 741

0.OOOI). The six groups also differed in their left AM 2 scores (F = 9.6, p < 0.0001) but not in their right AM Z scores (F = 2.0, p = 0.08).
POST HOC PAIRWISE COMPARISONS. For all groups, ex- cept for the bilateral TLE group, HF 2 scores ipsilat- era1 to the main EEG focus were significantly lower than in controls ( p < 0.05). The HF 2 scores con- tralateral to the EEG focus, however, did not differ from controls ( p > 0.5). The bilateral TLE group had significantly lower 2 scores than controls for both the left and the right HF ( p < 0.003). HF asymmetry ra- tios were significantly different from controls in the Left-TLE and Right-TLE (both p < 0.0001) and L >R TLE ( p = 0.01) groups but not in the R > L TLE and bilateral TLE groups ( p > 0.5) (see Fig 4).
AM Z scores were significantly different from con- trols only for the ipsilateral temporal lobe in the Left- TLE ( p < 0.001), L > R TLE ( p < 0.001), and hght-TLE ( p = 0.02) groups. In a similar manner, the AM asymmetry ratios were significantly different from controls in only the Left-TLE ( p < 0.001), L > R TLE ( p = 0.02), and kght-TLE ( p < 0.01) groups.
In summary, the more unilateral the EEG abnormal- ities, the more asymmetric the MRIVol abnormalities were in both the AM and the HF.
ANALYSIS FOR INDIVIDUAL PATIENTS. The AM-HF volumes combined were abnormal in 86 of 98 (87.7%) patients. The AM-HF atrophy was bilateral in 27 (28%) patients; there was no lateralization in 5 of these patients. The AM-HF volumes were normal in 12 pa- tients; all these 12 patients had lateralized MRSI ab- normalities in agreement with the lateralization by EEG (Table 1).
The AM volumes alone were abnormal in 58 of 93 (62.4%) patients, and the HF volumes alone were ab- normal in 84 of 98 (85.7%) patients.
We found no significant difference for the MRIVol lateralization in the patients who had 3-mm-thick MRI slices (28 of 34, 82.4%, lateralized) versus the group with I-mm slices (53 of 64, 83%, lateralized). This
lack of a difference between the overall lateralization, using these two protocols, may reflect differences in the clinical characteristics of the two groups of patients, rather than the se tivity of measurements performed
creased sensitivity of thin slices is expected mainly in patients with subtle atrophy that would be missed with the use of 3-mm-thick slices. Proper comparison of the effect of slice thickness on sensitivity requires making both measurements in the same subjects. We have done this in a small group of patients and normal con- trols and found an increased sensitivity, using 1-mm- thick slices, that was greater for AM volumes than for HF volumes. This increase was due, at least in part, to less variation in the normal control data (data not shown here).
on 3-mm versus ?! mm-thick images in general. In-
Proton MRSI and MRIVoL Interrelationships 2 scores for absolute values and asymmetries in NAA/Cr and AM and HF volumes were highly inter- related and concordant (Table 2).
Combinution o f MRSI und MRIVoL All 98 patients (2 patients did not have MRIVol avail- able) were classified as abnormal, ie, 88 of 98 (90%) as unilateral and 10 of 98 (10%) as bilateral. Only 1 pa- tient was lateralized contralateral to the EEG classifica- tion (see Table 1).
Results in Disagreement with EEG There were 4 patients who had some imaging results in disagreement with the EEG investigation. One patient had both MRIVol and MRSI lateralization opposite to the EEG, 2 patients had only MRIVol, and another 1 had only MRSI lateralization contralateral to the EEG (see Table 1).
One patient had MRSI (both for Mid and Post tem- poral regions) and MRlVol (right HF atrophy and nor- mal AM volumes) lateralization to the right temporal lobe, whereas intracranial EEG investigation revealed a clear predominance of seizure onsets from the left me- sial temporal structures. This patient underwent a left
Table 1. ClassiJicationr Based on Normal Control Cutofi (Mean - 2 SO)
Bilateral on EEG Left on EEG Right on EEG Disagreement
MR Examination Bilat Left N1 k g h t Bilat Left NI Right Bilat Left NI Right Normal (%) Abnormal (9'0) Lateralization with EEG
MRIVol (n = 98) 1 2 1 3 3 54 6 3 1 0 5 19 12(12) 86(88) 81 (83) 3 MKSI (n = 100) 5 1 0 1 7 58 1 2 1 0 0 24 l ( 1 ) 99 (99) 86 (86) 2 MRIVol + MRSI 2 2 0 3 7 58 0 I 1 0 0 24 O(0) 98 (100) 88 (90) 1
(n = 98)
MR = magnetic resonance; EEG = electroencephalography; Bilat = bilateral; NI = normal; MRI = magnetic resonance imaging; MRIVol = MRI volumetric analysis; MRSI = proton magnetic resonance spectroscopic imaging.
742 Annals of Neurology Vol 42 No 5 November 1997
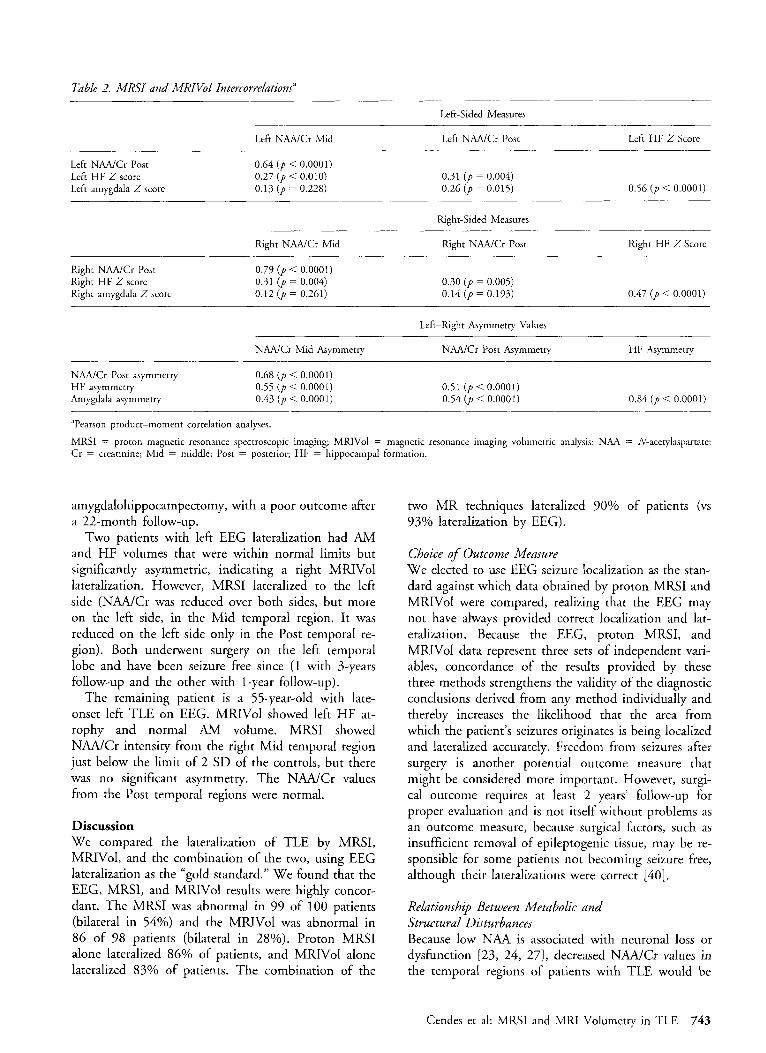
Table 2. MRSI and MRIVool Intercorrelations"
Left-Sided Measures
Left N M C r Mid Left N M C r Post Left HF 2 Score
Left N M C r Post Left HF 2 score Left amygdala 2 score
0.64 ( p < 0.0001) 0.27 ( p < 0.010) 0.13 ( p = 0.228)
0.31 ( p = 0.004) 0.26 ( p = 0.015) 0.56 ( p < 0.0001)
Right-Sided Measures
Right N M C r Mid Right NAA/Cr Post Right HF 2 Score
Right NAA/Cr Post Right HF 2 score Right amygdala Z score
0.79 ( p < 0.0001) 0.31 ( p = 0.004) 0.12 ( p = 0.261)
0.30 ( p = 0.005) 0.14 ( p = 0.193) 0.47 ( p < 0.0001)
Left-Right Asymmetry Values
NAAiCr Mid Asymmetry NAAiCr Post Asymmetry HF Asymmetry
N M C r Post asymmetry HF asymmetry Amygdala asymmetry
0.68 ( p < 0.0001) 0.55 ( p < 0.0001) 0.43 ( p < 0.0001)
0.51 ( p < 0.0001) 0.54 ( p < 0.0001) 0.84 ( p < 0.0001)
"Pearson product-moment correlation analyses.
MRSI = proton magnetic resonance spectroscopic imaging; MRIVol = magnetic resonance imaging volumetric analysis: NAA = N-acetylasparrate; Cr = creatinine; Mid = middle; Post = posterior; HF = hippocampal formation.
amygdalohippocampectomy, with a poor outcome after a 22-month follow-up.
Two patients with left EEG lateralization had AM and HF volumes that were within normal limits but significantly asymmetric, indicating a right MRIVol lateralization. However, MRSI lateralized to the left side (NAA/Cr was reduced over both sides, but more on the left side, in the Mid temporal region. It was reduced on the left side only in the Post temporal re- gion). Both underwent surgery on the left temporal lobe and have been seizure free since (1 with 3-years follow-up and the other with 1-year follow-up).
The remaining patient is a 55-year-old with late- onset left TLE on EEG. MRIVol showed left HF at- rophy and normal AM volume. MRSI showed NAA/Cr intensity from the right Mid temporal region just below the limit of 2 SD of the controls, but there was no significant asymmetry. The N M C r values from the Post temporal regions were normal.
Discussion We compared the lateralization of TLE by MRSI, MRIVol, and the combination of the two, using EEG lateralization as the "gold standard." We found that the EEG, MRSI, and MRIVol results were highly concor- dant. The MRSI was abnormal in 99 of 100 patients (bilateral in 54%) and the MRIVol was abnormal in 86 of 98 patients (bilateral in 28%). Proton MRSI alone lateralized 86% of patients, and MRIVol alone lateralized 83% of patients. The combination of the
two MR techniques lateralized 90% of patients (vs 93% lateralization by EEG).
Choice of Outcome Measure We elected to use EEG seizure localization as the stan- dard against which data obtained by proton MRSI and MRIVol were compared, realizing that the EEG may not have always provided correct localization and lat- eralization. Because the EEG, proton MRSI, and MRIVol data represent three sets of independent vari- ables, concordance of the results provided by these three methods strengthens the validity of the diagnostic conclusions derived from any method individually and thereby increases the likelihood that the area from which the patient's seizures originates is being localized and lateralized accurately. Freedom from seizures after surgery is another potential outcome measure that might be considered more important. However, surgi- cal outcome requires at least 2 years' follow-up for proper evaluation and is not itself without problems as an outcome measure, because surgical factors, such as insufficient removal of epileptogenic tissue, may be re- sponsible for some patients not becoming seizure free, although their lateralizations were correct [40].
Relationship Between Metabolic and Structural Disturbances Because low NAA is associated with neuronal loss or dysfunction [23, 24, 271, decreased NAAJCr values in the temporal regions of patients with TLE would be
Cendes et al: MRSI and MFU Volumetry in TLE 743
expected to be associated with medial temporal lobe atrophy. In accordance with this, we found that the NAA/Cr values correlated well with volume loss on MRIVol in our patients (see Table 2). However, 12 patients with normal MRI had reduced N M C r values in the temporal region; 7 of these patients underwent surgery. Qualitative histopathological examination of the resected tissue revealed mild astrogliosis and neu- ronal loss of mesial temporal structures 16-81. Four of these patients are seizure free, or have auras only, after surgery [I], with a follow up of at least 1 year. The remaining 3 patients have undergone surgery recently and the outcomes are not yet available. These data im- ply that proton MRS evidence of neuronal damage is detectable in vivo before structural changes are seen by conventional MRI [41].
Consistent with this, we found that proton MRSI demonstrated more diffuse abnormalities within the temporal lobes than did MRI. The presence of bilateral proton MRSI abnormalities may preclude lateralization by MRSI in some patients. MRIVol provides lateral- ization in some of these patients, at least some of whom can still benefit from surgery. The significance of bilateral proton MRSI abnormalities and their rela- tionship to postoperative outcome in TLE must be in- vestigated further.
Patients with bilateral ictal EEG abnormalities had more severe bilateral proton MRSI and MRIVol abnor- malities than patients with all or more than 90% of their seizures originating from one temporal lobe. Us- ing NAA/Cr values from the Mid and Post temporal regions together allowed us to lateralize more patients than using each one of these regions separately. To a lesser extent the same was true for the AM and the HF volumes.
We obtained lateralization in 83% of patients by us- ing MRIVol alone and in 86% of patients by using proton MRSI alone. By combining MRSI and MRIVol results all patients could be classified as having tempo- ral lobe abnormalities, and 90% of patients could be lateralized. EEG investigation lateralized 93% of patients. Thus, combining data sources resulted in clas- sification of more patients with a higher degree of accuracy.
Relationship of Metabolic and Structural Disturbances to EEG Findings The side of maximal proton MRSI and MRIVol ab- normalities correlated with the side from which most seizures originated, according to the EEG investigation, in all but 4 patients. However, when MRSI and MRIVol findings were combined, only 1 patient had lateralization on the side opposite to the most frequent EEG seizure onsets. The reason for the incongruent proton MRSI and MRIVol in this patient remains un- clear. She has undergone surgery on the side of pre-
dominant intracranial EEG seizure onsets, opposite to the side of greater atrophy and NAA/Cr decrease, and has had a poor outcome after a 22-month follow-up. It is not clear whether the EEG lateralization was mis- leading in this patient, or whether the poor outcome was related to bitemporal seizure onsets or to other factors such as the amount of epileptogenic tissue resected.
The relative merits of ictal EEG findings versus as- sociated structural or metabolic abnormalities in later- alizing the most epileptogenic area remains to be de- termined. The primary importance of the EEG in the diagnosis of epilepsy is self-evident because epileptic seizures are an electrical phenomenon. However, it is well known that seizures may appear to begin on both sides in many patients with TLE, and that the first recorded seizure may not originate from the main sei- zure generator [4, 51. The structural and, presumably, the metabolic abnormality in TLE may reflect the pathological substrate of the seizure generator. Thus, these image-based abnormalities may bear a sufficiently consistent relationship to the origin and severity of sei- zures to obviate the need to record multiple ictal events to determine the side from which most seizures origi- nate. We do not believe rhat EEG will ever be replaced by imaging alone. However, the results of the present study, together with previous publications [9-13, 16, 17, 20, 28, 29, 33-35, 42-45], support the preopera- tive strategy, proposed by Cascino and associates [45], that selected patients with a history and ictal semiology consistent with medial TLE may undergo surgery if in- terictal epileptiform discharges recorded during serial routine EEGs or long-term video-EEG monitoring consistently lateralize to one temporal lobe, in agree- ment with strong functional and structural imaging ev- idence of unilateral medial temporal lobe damage. Re- cording of ictal events by surface or intracranial EEG would still be imperative in those patients without abundant interictal abnormalities, in patients with nor- mal imaging studies, in patients with bilateral imaging or bilateral interictal EEG abnormalities, and in pa- tients with discordant preoperative studies [2, 4, 451.
The present series included only patients with TLE, and therefore, it is not suitable for assessment of the specificity of MRIVol or MRSI abnormalities. Our previous studies in patients with TLE and extratempo- ral epilepsy, however, indicated that abnormalities on both MRIVol 116, 441 and MRSI from the temporal lobes [46] can be specific for TLE in this setting. Be- cause specificity always depends on the patient popu- lation under study, the specificity we have found may not apply to other patient populations.
The use of proton MRSI for the presurgical evaha- tion of extratemporal epilepsies has potential [47, 481 but poses greater technical difficulties and must be evaluated further.
744 Annals of Neurology Vol 42 No 5 November 1997
Conclusions Although the improved sensitivity achieved by combin- ing MRSI and MRIVol is relatively small (83-90%), we believe that this is a worthwhile improvement for the following reasons: ( I ) In this series of difficult cases, 7 additional patients could be lateralized; (2) the use of these two MR examinations, which can be per- formed on an outpatient basis, increased our confi- dence of the lateralization of the seizure focus; and (3 ) the EEG lateralization in 20% of these patients re- quired invasive intracranial recordings after long-term extracranial EEG investigations had failed to provide lateralization. It is possible that intracranial recordings could be avoided by use of multimodal MR examina- tions.
One could question whether patients with TLE must have both of these MR examinations in addition to an extensive EEG investigation. Although the differ- ent examinations may agree on lateralization, they pro- vide different kinds of information, namely, electro- physiological, structural, and functional information, that are helpful in understanding the significance of abnormalities in individual patients and making deci- sions regarding the use of surgical therapy in difficult cases.
Our results suggest that proton MRSI and MRIVol represent powerful new tools for the noninvasive pre- surgical lateralization of TLE.
This study was supported by a grant from the Medical Research Council of Canada and from the Savoy Foundation for Epilepsy Research, Montreal, Quebec, Canada.
References 1. Engel J Jr, Van Ness PC, Rasmussen T, Ojemann LM. Out-
come with respect to epileptic seizures. In: Engel J Jr, ed. Sur- gical treatment of the epilepsies. 2nd ed. New York: Raven Press, 1993:609-621
2. Wieser H, Engel JJ, Williamson PD, et al. Surgically remedia- ble temporal lobe syndromes. In: Engel JJ, ed. Surgical treat- ment of the epilepsies. 2nd ed. New York: Raven Press, 1993:
3. Gumnit RJ. Cost, accessibility, and quality-of-life issues in sur- gery for epilepsy. In: Luders H, ed. Epilepsy surgery. New York: Raven Press, 1991:47-49
4. Engel J Jr. Approaches to localization of the epileptogenic le- sion. In: Engel J Jr, ed. Surgical treatment of the epilepsies. New York: Raven Press, 1987:75-95
5. Olivier A, Marchand E, Peters T, Tyler J. Depth electrode im- plantation at the Montreal Neurological Institute and Hospital. In: Engel J Jr, ed. Surgical treatment of the epilepsies. New York: Raven Press, 1987:595-601
6. Babb TL, Brown WJ. Pathological findings in epilepsy. In: En- gel J Jr, ed. Surgical treatment of the epilepsies. New York: Raven Press, 1987:511-540
7. Gloor P. Mesial temporal sclerosis: historical background and an overview from a modern perspective. In: Luders H , ed. Ep- ilepsy surgery. New York: Raven Press, 1991:689-703
8. Meencke HJ, Veith G. Hippocampal sclerosis in epilepsy. In:
49 - 63
Luders H, ed. Epilepsy surgery. New York: Raven Press, 1991:
9. Berkovic SF, McIntosh AM, Kalnins RM, et al. Preoperative MRI predicts outcome of temporal lobectomy: an actuarial analysis. Neurology 1995;45: 1358 -1 363
10. Cascino GD, Jack CR, Parisi JE, et al. Magnetic resonance imaging-based volume studies in temporal lobe epilepsy: patho- logical correlations. Ann Neurol 1991;30:31-36
1. Cook MJ, Fish DR, Shorvon SD, et al. Hippocampal volumet- ric and morphometric studies in frontal and temporal lobe ep- ilepsy. Brain 1992;115:1001-1015
2. Jack CR Jr, Trenerry MR, Cascino GD, et al. Bilaterally sym- metric hippocampi and surgical outcome. Neurology 1995;45:
3. Jackson GD, Connelly A, Duncan JS, et al. Detection of hip- pocampal pathology in intractable partial epilepsy: increased sensitivity with quantitative magnetic resonance T2 relaxom- etry. Neurology 1993;43:1793-1799
14. Kuzniecky RI, Jackson GD. Magnetic resonance in epilepsy. New York: Raven Press, 1995
15. Cendes F, Andermann F, Gloor P, et al. Atrophy of mesial structures in patients with temporal lobe epilepsy: cause or con- sequence of repeated seizures? Ann Neurol 1993;34:795-801
16. Cendes F, Andermann F, Gloor P, et al. MRI volumetric mea- surements of amygdala and hippocampus in temporal lobe ep- ilepsy. Neurology 1993;43:719-725
17. Lencz T, McCarthy G, Bronen RA, et al. Quantirative mag- netic resonance imaging in temporal lobe epilepsy: relationship to neuropathology and neuropsychological function. Ann Neu- rol 1992;31:629-637
18. Spencer SS, McCarthy G, Spencer DD. Diagnosis of medial temporal lobe seizure onset: relative specificity and sensitivity of quantitative MRI. Neurology 1993;43:2117-2124
19. Gilmore RL, Childress MD, Leonard C, et al. Hippocampal volumetrics differentiate patients with temporal lobe epilepsy and extratemporal lobe epilepsy. Arch Neurol 1995;52:819- 824
20. Murro AM, Park YD, King DW, et al. Seizure localization in temporal lobe epilepsy: a comparison of scalp-sphenoidal EEG and volumetric MRI. Neurology 1993;43:2531-2533
21. Jack CR, Sharbrough FW, Cascino GD, et al. Magnetic reso- nance image-based hippocampal volumetry: correlation with outcome after temporal lobectomy. Ann Neurol 1992;31:138- 146
22. Henriksen 0. In vivo quantitation of metabolite concentrations in the brain by means of proton MRS. NMR Biomed 1995;s: 139 -1 48 (Review)
23. Petroff OAC, Pleban LA, Spencer DD. Symbiosis between in vivo and in vitro NMR spectroscopy: the creatine, N- acetylaspartate, glutamate, and GABA content of the epileptic human brain. Magn Reson Imaging 1995;13:1197-1211
24. Arnold DL, Matthews PM. Practical aspects of clinical applica- tions of MRS in the brain. In: Young IR, Charles HC, eds. MR spectroscopy: clinical applications and techniques. London: Martin Dunitz, 1996:139-159
25. Preul MC, Caramanos Z, Collins DL, et al. Accurate, nonin- vasive diagnosis of human brain tumors by using proton mag- netic resonance spectroscopy. Nat Med 1996;2:323-325
26. Simmons ML, Frondoza CG, Coyle JT. Immunocytochernical localization of N-acetyl-aspartate with monoclonal antibodies. Neuroscience 199 1 ;45:37-45
27. Moffett JR, Namboodiri MAA, Cangro CB, Neale JH. Immu- nohistochemical localization of N-acetylaspartate in rat brain. Neuroreport 199 1;2: I3 1-1 34
28. Connelly A, Jackson GD, Duncan JS, et al. Magnetic resonance spectroscopy in temporal lobe epilepsy. Neurology 1994;44: 1411-1417
689-703
1353-1 358
Cendes et al: MRSI and MRI Volumetry in TLE 745
29. Hugg JW, Laxer KD, Matson GB, et al. Neuron loss localizes human temporal lobe epilepsy by in vivo proton magnetic res- onance spectroscopic imaging. Ann Neurol 1993;34:788 -794
30. Matthews PM, Andermann F, Arnold DL. A proton magnetic resonance spectroscopy study of focal epilepsy in humans. Neu- rology 1990;40:985-989
31. Petroff OA, Spencer DD, Alger JR, Prichard JW. High-field proton magnetic resonance spectroscopy of human cerebrum obtained during surgery for epilepsy. Neurology 1989;39: 1197- 1202
32. Cendes F, Andermann F, Preul M, Arnold DL. Lateralization of temporal lobe epilepsy based on regional metabolic abnor- malities in proton magnetic resonance spectroscopic images. Ann Neurol 1994;35:211-216
33. Hetherington H, Kuzniecky R, Pan J, et al. Proton nuclear magnetic resonance spectroscopic imaging of human temporal lobe epilepsy at 4.1 T. Ann Neurol 1995;38:396-404
34. Ng TC, Comair YG, Xue M , et al. Temporal lobe epilepsy: presurgical localization with proton chemical shift imaging. Ra- diology 1994;193:465-472
35. Cross JH, Connelly A, Jackson GD, et al. Proton magnetic res- onance spectroscopy in children with temporal lobe epilepsy. Ann Neurol 1996;39:107-113
36. Rorh K, Kimber BJ, Feeney J. Data shift accumulation and al- ternate delay accumulation techniques for overcoming dynamic range problems. J Magn Reson 1980;41:302
37. Watson C, Andermann F, Gloor P, et al. Anatomic basis of amygdaloid and hippocampal volume measurement by mag- netic resonance imaging. Neurology 1992;42: 1743-1750
38. Sokal RR, Rohlf FJ. Assumptions of analysis of variance. In: Sokal RR, Rohlf FJ, eds. Biometry. 2nd ed. New York: Free- man, 1981:400-560
39. Stoline MR. The status of multiple comparisons; simultaneous
estimations of all painvise comparisons in one-way ANOVA de- signs. Am Stat 1981;35:134-141
40. German0 IM, Poulin N , Olivier A. Reoperation for recurrent temporal lobe epilepsy. J Neurosurg 1994;81:31-36
41. Ebisu T, Rooney WD, Graham SH, et al. N-Acetylaspartate as an in vivo marker of neuronal viability in kainate-induced sta- tus epilepticus: 1 H magnetic resonance spectroscopic imaging. J Cereb Blood Flow Metab 1994;14:373-382
42. Arruda F, Cendes F, Andermann F, et al. Mesial atrophy and outcome after amygdalohippocanipectomy or temporal lobe re- moval. Ann Neurol 1996;40:446-450
43. Cendes F, Arruda F, Dubeau F, et al. Relationship between mesial temporal atrophy and ictal and interictal EEG findings: results in a series of 250 patients. Epilepsia 1995;36(suppl 4):23 (Abstract)
44. Cendes F, Dubeau F, Andermann F, et al. Significance of me- sial temporal atrophy in relation to intracranial ictal and inter- ictal stereo EEG abnormalities. Brain 1996;119:1317-1326
45. Cascino G D , Trenerry MR, So EL, et al. Routine EEG and temporal lobe epilepsy-relation to long-term EEG monitoring, quantitative MRI, and operative outcome. Epilepsia 1996;37: 651-656
46. Cendes F, Sranley JA, Dubeau F, et al. Proton magnetic reso- nance spectroscopic imaging for discrimination of absence and complex partial seizures. Ann Neurol 1997;41:74-81
47. Garcia PA, Laxer KD, van der Grond J, et al. Proton magnetic resonance spectroscopic imaging in patients with frontal lobe epilepsy. Ann Neurol 1995;37:279-281
48. Stanley JA, Cendes F, Dubeau F, et al. Decreased N-acetyl- aspartate in the epileprogeiiic region of patients with extratem- poral epilepsy via in vivo 1 H MRS. Proceedings of the Inter- national Society of Magnetic Resonance in Medicine 1996;l: 135 (Abstract)
746 Annals of Neurology Vol 42 No 5 November 1997