Embed Size (px)
Citation preview

Oxidative Stress and Risk of Cardiovascular Disease Associated with Low- and High-Monounsaturated Fat
Portfolio Diets
By
Laura Chiavaroli
A thesis submitted in conformity with the requirements for the degree of Master of Science
Graduate Department of Nutritional Sciences University of Toronto
© Copyright by Laura Chiavaroli (2010)

ii
Oxidative Stress and Risk of Cardiovascular Disease Associated with Low- and High-Monounsaturated Fat
Portfolio Diets
Laura Chiavaroli Master of Science
Department of Nutritional Sciences University of Toronto
2010
Abstract
The objective was to assess the effect of a high-monounsaturated fat (MUFA) dietary
portfolio of cholesterol-lowering foods on oxidative stress and cardiovascular risk. Twenty-
four hyperlipidemic subjects followed a very low-saturated-fat therapeutic control diet for 4
weeks after which they were randomized to receive the dietary portfolio, consisting of soy
protein (20g/1000kcal), viscous fibre (10.3g/1000kcal), plant sterols (2-3g) and almonds
(21.5g/1000kcal), in combination with high- or low-MUFA (25.9% and 12.9% MUFA,
respectively) for the next 4 weeks, where MUFA replaced 13.0% of dietary carbohydrate.
On high-MUFA, there were significantly greater increases in HDL-C and apoA1 and
significantly greater reductions in total:high-density lipoprotein cholesterol (total:HDL-C)
ratio and high-sensitivity C-reactive protein (hs-CRP) compared to the low-MUFA dietary
portfolio. In all diets there were significant increases in protein thiols and reductions in
conjugated dienes and thiobarbituric acid reactive substances (TBARS) measured in the
LDL-fraction, however no difference between the high- and low-MUFA diets.
Abstract Word Count: 149

iii
Table of Contents
Chapter Title Page Abstract.............…………………....……………………………...…………….ii
Table of Contents……………………………………………..….…..………iii-v
List of Abbreviations………………………………….…….…….…..…..…vi-vii
List of Figures…………………………....……………….….….…..………...viii
List of Tables………………………………………………..….……………….ix
1 Introduction…………....…………………………………….……………….1-3 2 Literature Review………………………………….………...….………..……4
2.1 Cardiovascular Disease Risk Factors..….……….………………5
2.1.1 Hyperlipidemia……………..……….…….……….……5-6
2.1.2 Oxidative Stress………...…..………….………………6-7
2.1.2.1 Measures of Oxidative Stress….……….…..7-9
2.1.2.2 Supplemental Use of Antioxidants.…..…..9-10
2.1.3 HDL-C…………………………………......…………10-12
2.2 Foods with cholesterol-lowering and anti-oxidative potential...12
2.2.1 Nuts……………………………………………...……12-13
2.2.2 Soy Protein…………………………………………..13-14
2.2.3. Viscous Fibre………………………………………..14-15
2.2.4 Plant sterols and stanols…………………………….…16
2.2.5 The Dietary Portfolio..............................................17-18
2.2.6 Monounsaturated Fatty Acids…………………...…18-20
3 Hypothesis, Objectives & Rationale……………………………..………..21
3.1 Hypothesis………………………………………………………..………..22
3.2 Objectives………………………………………………………..…...……22
3.3 Rationale……………………………………………………………..…22-23
4 The Effect of Adding Monounsaturated Fat to a Dietary Portfolio of Cholesterol-Lowering Foods in Hypercholesterolemia…………...…..24 4.1 Abstract……………………………………………………………………..25
4.2 Introduction…………………………………………………………………26

iv
4.3 Methods…………………………………………………………………….26
4.3.1 Participants………………………………….……………….26-27
4.3.2 Study Protocol……………………………….………………27-28
4.3.3 Diets…………………………………………..………………28-29
4.3.4 Analyses………………………………………...……………29-30
4.3.5 Statistical Analysis…………………………………...………....30
4.4 Results………………………………………………………............……..30
4.4.1 Participants……………………………………………….….30-31
4.4.2 Blood Lipids and C-reactive Protein………………………31-32
4.4.3 Blood Pressure…………………………………………...……..32
4.4.4 Drop Outs and Adverse Events……………………............…32
4.5 Discussion……………………………………………………………...32-36
4.5.1 Figures …………………………………………………………..…..37-39
4.5.2 Tables……………………………………………....……………..…40-45
5 The Effect on Oxidative Stress of Adding Monounsaturated Fat to a Dietary Portfolio of Cholesterol-Lowering Foods.................................46
5.1 Abstract…………………………………………………………………..…47
5.2 Introduction………………………………………………………………...48
5.3 Methods………………………………………………………….….……..48
5.3.1 Participants……………………………………………....…..48-49
5.3.2 Study Protocol………………………………………….……49-50
5.3.3 Diets…………………………………………………...……..50-51
5.3.4 Analyses………………………………………………..….…51-52
5.3.5 Statistical Analysis…………………………………..….……...52
5.4 Results………………………………………………………………….….52
5.4.1 Participants……………………………………...………………52
5.4.2 Markers of Oxidation…..........…………………….………..52-53
5.4.3 Drop Outs and Adverse Events……………………….…........53
5.5 Discussion………………………………………………..……....…….53-55
5.5.1 Figures……………………………………………………………56
5.5.2 Tables…………………………………………………………….57

v
6 Overall Discussion, Limitations and Future Research…..….……….58 6.1 Overall Discussion………………………………………….…………59-62
6.2 Limitations………………………………………………………..…….62-63
6.3 Future Research………………………………………………….……63-64
7 Summary……………………………………………………………………….65
7. Summary………………………………………………………………….…66 8 References……………………………………………..…...........……….67-85

vi
List of Abbreviations
8-OHdG – 8-Hydroxyeoxyguanosine
ABC transporter – ATP-binding Cassette Transporter
AHA – American Heart Association
apoA1 – apolipoprotein A1
apoB – apolipoprotein B
BMI – Body Mass Index
CD – Conjugated Dienes
CE – Cholesterol Ester
CETP - Cholesterol-Ester Transfer Protein
CHD – Coronary Heart Disease
CV – Coefficient of Variance
CVD – Cardiovascular Disease
DASH – Dietary Approaches to Stop Hypertension
DNA – Deoxyribonucleic Acid
DTNB – 5,5’-Dithio-bis 2-Nitrobenzoic Acid
FDA – Food and Drug Administration
HDL – High-Density Lipoprotein
HDL-C – High-Density Lipoprotein Cholesterol
HL – Hepatic Lipase
hs-CRP – high-sensitivity-C-Reactive Protein
IVUS – Intravascular Ultrasound
IL-6 – Interleukin-6
LCAT – Lecithin Cholesterol Acyltransferase
LDL – Low- Density Lipoprotein
LDL-C – Low- Density Lipoprotein Cholesterol
LPL – Lipoprotein Lipase
LRC-CPP – Lipid Research Clinic Coronary Primary Prevention
MDA – Malondialdehyde
MET – Metabolic Equivalent of Tasks

vii
MUFA – Monounsaturated Fatty Acid
NCEP – National Cholesterol Education Program
NCEP ATP III – National Cholesterol Education Program Adult Treatment Panel III
Ox-LDL – Oxidized Low-Density Lipoprotein
PAF-AH – Platelet-Activating Factor Acetylhydrolase
PON1 – Paraoxonase 1
PUFA – Polyunsaturated Fatty Acid
RCT – Reverse Cholesterol Transport
ROS – Reactive Oxygen Species
S-S – Disulfide Bond
SAS – Statistical Analysis System
SEM – Standard Error Mean
SFA – Saturated Fatty Acid
-SH – Thiol Group
TBARS – Thiobarbituric Acid Reactive Substances
Total-C – Total Cholesterol
TG – Triglycerides
TNF-α – Tumor Necrosis Factor - Alpha
USDA – United States Department of Agriculture
VLDL-C – Very Low-Density Lipoprotein Cholesterol

viii
List of Figures
Chapter 2 Figure 1. The development of atherosclerosis.
Figure 2. Oxidative modification of cellular macromolecules.
Figure 3: Reaction of a thiol group from a sulphur-containing amino acid with DTNB as a
measurement of the amount of unoxidized proteins.
Figure 4: Design of the proposed mechanism of HDL-C lowering.
Chapter 4 Figure 1: Patient flow diagram.
Figure 2: Mean (SE) percentage change from baseline for both treatments for HDL-C,
apoA1, total:HDL-C ratio and apoB:apoA1 ratio.
Figure 3. Mean (SE) percentage change from baseline for both treatments for total-C,
LDL-C, apoB and TG.
Chapter 5 Figure 1. Means of oxidative stress markers on high- and low-MUFA diets.

ix
List of Tables
Chapter 4 Table 1. Baseline characteristics of randomized study participants.
Table 2: Macronutrient Composition of the Participants' Habitual Diet
Table 3: Macronutrient Composition of the Study Diets
Table 4: Example Menuplan of Diets for 2000kcal
Table 5. Effect of Control, Very Low-Saturated-Fat, Diet on Blood Lipids, C-Reactive
Protein, and Blood Pressure in High- vs. Low-MUFA Groups
Table 6. Effect of High-MUFA and Low-MUFA Dietary Portfolio Treatments on Blood
Lipids, C-Reactive Protein, and Blood Pressure
Chapter 5 Table 1. Effect of Control, Very Low-Saturated-Fat, Diet on Oxidative Markers in High-
vs. Low-MUFA Groups
Table 2. Effect of Low-MUFA and High-MUFA Dietary Portfolio Treatments on Oxidative
Markers

1
1. Introduction

2
1. Introduction Cardiovascular disease (CVD) is the leading cause of death in Canada,
accounting for approximately one-third of all deaths, and is the largest economic
burden of disease (1). For prevention and treatment of CVD, attention to diet
and lifestyle has been continuously growing as Canadians are being encouraged
to follow what has been termed a “heart-healthy diet” (2, 3). Essentially this
means limiting intake of saturated fat, choosing leaner meats, low-fat dairy, and
increasing consumption of fruits, vegetables and whole grains as is
recommended by many organizations, including the American Heart Association
(AHA) and the Heart and Stroke Foundation of Canada (4, 5).
Over the past few decades, specific foods have been looked at for their
potential roles in reducing the risk of CVD by targeting one or more of the
associated risk factors. Elevated blood cholesterol is one such risk factor. It is
estimated that about 40% of Canadians have high blood cholesterol levels (6).
The National Institutes of Health in their Third Report of the Expert Panel on
Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult
Treatment Panel, ATP, III Final Report) encourages the use of therapeutic
dietary options for enhanced reduction of low-density lipoprotein cholesterol
(LDL-C), such as plant sterols and viscous (soluble) fibres (7). These dietary
options have been previously combined with other foods, including almonds and
soy protein, which have also demonstrated cholesterol reduction, into a dietary
intervention termed the dietary portfolio, which has been shown to effectively
reduce cholesterol levels to a similar extent as the therapeutic dose of first-
generation statins (28.6% vs. 30.9%, respectively) compared to a low-fat control
diet (8.0%) (8).
Another risk factor for CVD which has been given much attention is
oxidative stress. Many studies have been conducted on the effects of varying
dietary antioxidants on oxidative stress levels and risk of CVD with conflicting
results, indicating the need for further investigation (9). However, it is possible
that through the consumption of whole foods and the interactions between
vitamins and nutrients that a greater benefit may be observed. Dietary portfolio

3
studies have also shown significant reductions in high-sensitivity C-reactive
protein (hs-CRP) and increases in protein thiols, demonstrating the potential to
improve oxidative and inflammatory status (10-12). In addition to antioxidant-rich
foods, the lipid factor high-density lipoprotein cholesterol (HDL-C) has been
associated with improvements in lipid oxidation, as well as anti-inflammatory and
antithrombotic activity. High HDL-C levels have been associated with reduced
oxidative stress and conversely, low HDL-C has been associated with increases
in oxidation (13-15). Methods known to increase HDL-C levels include increased
dietary fat intake, as well as exercise, smoking cessation and moderate alcohol
intake (16, 17). As a result of recommended dietary restrictions on saturated fatty
acid (SFA) and polyunsaturated fatty acid (PUFA) intake, monounsaturated fatty
acid (MUFA) intake is recommended as the dietary method of increasing HDL-C,
which can be achieved through increased consumption of foods rich in MUFA
such as avocados, high-MUFA oils including olive and canola oil, as well as nuts
and seeds.
In the present study, MUFA was added to an effective dietary portfolio of
cholesterol-lowering foods to determine if further reductions could be made in
CVD risk, particularly by targeting the oxidative and lipid risk factors.

4
2. Literature Review

5
2.1 CVD Risk Factors 2.1.1 Hyperlipidemia Cardiovascular disease (CVD) is a leading cause of death in North America.
Although rates of death due to heart disease have declined by 25% in the past decade,
it still accounts for approximately one third of all deaths in both Canada and America
and is expected to rise due to increasing rates of obesity and diabetes, which are known
risk factors for CVD (6, 18). Other risk factors include hypertension, smoking, oxidative
stress and inflammation, and high blood cholesterol, especially elevated LDL-C. Due to
the prevalence of CVD, organizations exist to continuously evaluate scientific evidence
in order to present clinical guidelines on how best to prevent and treat risk factors. The
National Cholesterol Education Program Expert Panel and the Canadian Cardiovascular
Society have developed treatment recommendations, which are updated regularly with
evidence from emerging trials, in order to control hyperlipidemia and reduce the risk of
heart disease. Their recommendations are based on risk of developing coronary heart
disease (CHD), which is calculated, for example, from an equation developed as a
result of a large epidemiological study, the Framingham Heart Study. The Framingham
predictive risk equation is used to predict 10-year risk of CHD and includes the risk
factors age, total cholesterol (total-C), HDL-C , systolic blood pressure, and cigarette
smoking (19). LDL-C remains the primary lipid target because many studies over the
past 3 decades have demonstrated that through the use of statins, LDL-C levels could
be reduced with a corresponding reduction in risk of CVD (20, 21). One meta-analysis
found that for every 1.0mmol/L decrease in LDL-C, there is a corresponding reduction of
21% and 12% in major cardiovascular disease events and all-cause mortality,
respectively (20). However, not only the quantity, but the quality of the LDL-C plays a
very important role in the risk of CVD since when coupled with an increased oxidative
and inflammatory environment, can result in the development of atherosclerosis, which
is one of the most prevalent forms of CVD (22). Research focused on reducing oxidative
stress has been inconsistent, unlike the majority of research on the other risk factors.
For example, blood pressure reduction has been demonstrated in the successful DASH
(Dietary Approaches to Stop Hypertension) trial and can also be controlled through

6
pharmaceuticals (23). Also, there are many methods available for smoking cessation
and exercise can reduce obesity, which coupled with avoiding excess carbohydrate,
especially simple sugars or choosing foods with low glycemic index (GI), can help in the
management or prevention of diabetes (24, 25). Research, however, on reducing
oxidative stress, including the trials on antioxidant supplementation, is still very
controversial, therefore requires further investigation.
2.1.2 Oxidative Stress Oxidative stress occurs when there is an imbalance between the production of reactive
oxygen species (ROS), which occurs naturally from oxidative metabolism, and
antioxidant defences (26). ROS are unstable molecules, such as superoxide, hydroxyl
and hydroperoxyl radicals, with an unpaired electron which can readily extract electrons
from other molecules, thus behaving as oxidants (27). They can act beneficially by
killing pathogens through phagocytes in the immune system, but can also elicit cytotoxic
effects (28). When the amount of ROS rises above normal levels, which has been
associated with many chronic disease states including hypercholesterolemia and
atherosclerosis, the antioxidant system of the body is overwhelmed, resulting in the
oxidation of particles such as proteins and lipids (29). The oxidation of the lipid particle
LDL-C is known to increase its atherogenicity since oxidized LDL (ox-LDL) is
recognized by macrophages and taken up via scavenger receptors. The macrophages
are then thought to become foam cells which form plaque in the arteries and thus, the
development of atherosclerosis (22, 30, 31) (Figure 1). Therefore, the oxidative
modification of LDL-associated lipids is directly involved in the initiation process of
atherosclerosis (32).

7
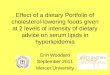
Figure 1. The development of atherosclerosis (33). Abbreviations: LDL, Low-density
lipoprotein; MM-LDL, minimally modified low-density lipoprotein; ox-LDL, oxidized-low-
density lipoprotein; ROS, reactive oxygen species; SR-A, scavenger receptor A.
2.1.2.1 Measures of Oxidative Stress Due to the very short half-lives of ROS, damage is measured via causally
associated molecules such as those resulting from protein and lipid oxidation (34-37)
(Figure 2).

8
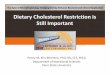
Figure 2. Oxidative modification of cellular macromolecules (36).
Protein oxidation is measured by the oxidation of side chains. The DTNB [5’, 5’-
dithio-bis(2-nitrobenzoic acid)] assay is a common method used to measure the

9
oxidation of sulphur containing amino acid side chains (cysteine and methionine)
because the DTNB molecule reacts with the thiol groups (-SH) (Figure 3). When there is
increased protein oxidation, less thiol groups will be detected since they will be already
oxidized into disulfide bonds (S-S).
Figure 3: Reaction of a thiol group from a sulphur-containing amino acid with
DTNB as a measurement of the amount of unoxidized proteins (38).
For lipids, the oxidation of LDL is of great interest because of its association with
the development of atherosclerosis. There are multiple ways of measuring oxidized
LDL, two of which include via conjugated dienes (CD) and thiobarbituric acid reactive
substances (TBARS) in LDL extracts precipitated from serum. In the former, the amount
of CD is measured directly by spectrophotometric determination of CDs in the extracted
LDL lipids (39). In the latter, the lipid peroxidation product malondialdehyde (MDA) is
measured through its reaction with thiobarbituric acid, which is added to the serum, and
also read spectrophotometrically (40). Considering the association between ox-LDL and
disease states including hypercholesterolemia, diabetes and the development of
cardiovascular disease (41, 42), many studies have investigated the role of antioxidants
in minimizing oxidative damage and reducing the risk of CVD.
2.1.2.2 Supplemental Use of Antioxidants Studies investigating the supplemental use of antioxidants have demonstrated
conflicting results. Some studies have demonstrated reductions in oxidative damage
resulting from antioxidant use, such as a reduction in ox-LDL with high doses of vitamin
E supplementation (43-46). However, most large trials conducted with antioxidant
supplementation have found no effect, such as the MRC/BHF (Medical Research
Council and British Heart Foundation) Heart Protection Study which assessed long term
supplementation of vitamin E, C and beta-carotene daily in subjects at high risk of CHD
(47). Other studies have demonstrated harmful effects, such as the increased risk of

10
lung cancer and cardiovascular disease in smokers supplemented with b-carotene (48),
or the HOPE (Heart Outcomes Prevention Evaluation) Study which found an increase in
heart failure in high risk subjects given 400IU of vitamin E daily for a mean of 7 years
(49). It must be questioned, however, whether these studies were targeting the
oxidative stress risk factor in the appropriate way. It is known that antioxidants may
become pro-oxidants in an oxidative environment, therefore, instead of giving single
vitamin supplements to high risk subjects who are under high oxidative stress, it may be
more effective to target the environment itself as a whole. This may be accomplished by
consumption of foods rich in vitamins in their whole form as it may be through the
interaction of all food components where protection seen in epidemiological studies may
be attained. Some support for this idea includes the results of the DASH trial which
tested a diet rich in fruit, vegetables, whole grains and low-fat dairy and not only
demonstrated significant reductions in blood pressure, but in further analyses, found
significant reductions in markers of oxidative damage (23, 50, 51). Additionally, the main
sources of many vitamins are plant foods, as well as nuts, seeds, and vegetable oils for
vitamin E, therefore, the benefits noted in epidemiological studies may be the result of
multiple vitamins working together or in combination with other nutrients present, such
as phytochemicals, fibre, or polyunsaturated and monounsaturated fats (52). Thus,
further investigation into the consumption of whole foods rich in vitamins and nutrients is
required to allow for possible synergistic activity and the potential promotion of a less
oxidative environment and ultimately, reduction in CVD risk.
2.1.3 HDL-C
Risk factors other than LDL-C are increasingly receiving attention due to the
residual risk for CVD that remains once LDL-C has been effectively lowered. This
includes the growing area of research on low HDL-C and risk of CVD independent of
LDL-C, total-C and TG. Many studies have found that for every 0.026mmol/L increase in
HDL-C, there is a corresponding 1-3% reduction in CVD risk and that even when LDL is
reduced or total-C levels are low, those with lower HDL-C are at a much greater risk of
developing CVD (53-61). As a result of the inverse correlation between HDL-C levels
and risk for CVD, the activities of HDL-C have been investigated. HDL-C is known for its

11
facilitating role in reverse cholesterol transport (RCT) whereby excess cholesterol from
the peripheral tissues is transferred from the plasma to the liver where it is either
recycled or excreted from the body through bile (62). Additionally, HDL-C has many
effects on the endothelium and antithrombotic actions (63, 64). However, its ability to
inhibit the oxidative modification of LDL via its potential antioxidative activity may be of
greater interest since oxidized LDL plays a central role in the initiation and propagation
of atherosclerosis (65-67). Mechanistically, there are many possible pathways by which
HDL-C may inhibit LDL oxidation, such as through the HDL-associated proteins
paraoxonase 1 (PON1) (14, 68) and platelet-activating factor acetylhydrolase (PAF-AH)
(69). The former protects against LDL oxidation, reverses biological effects of oxidized
LDL, inhibits the oxidation of HDL thereby preserving its function, and has been
associated with reduced risk of CVD (13, 70-75). The later attenuates proinflammatory
activity of PAF and functions as an antioxidant by hydrolyzing oxidized phospholipids
which result from the oxidation of LDL (76-78).
Another important component of HDL-C is its associated apolipoprotein, apoA1.
ApoA1 is a useful clinical measure because it can be measured directly with little error
and is a reflection of the anti-atherogenic HDL-C. It plays a central role in RCT, as it is
responsible for its initiation by picking up cholesterol from the periphery and delivering it
to the liver in HDL particles, and it has also been shown to have anti inflammatory and
antioxidant effects (79). Recently, apoA1, as well as the apolipoprotein associated with
LDL-C, apoB, have been called more informative risk indicators than their lipoproteins
or other lipids (79, 80). Two very large epidemiological studies, the AMORIS
(Apolipoprotein Mortality RISk) and INTERHEART studies (A Global Study of Risk
Factors for Acute Myocardial Infarction) found that there was a very strong direct
relation between the apoB:A1 ratio and fatal or acute myocardial infarction and that it
was the strongest lipid ratio predictor of CVD risk (81, 82). Interest in apoA1 began in
the early 1980s when it was discovered that a small group of people in Italy carried a
mutation of the apoA1 gene that resulted in low HDL-C and apoA1 and high TG but low
rates of CVD, which they termed apoA1Milano (83, 84). Studies began in the 1990s with
the recombinant version of apoA1 and those in animals demonstrated regression of
atheroma volume and promotion of more stable plaques (85-87). A few studies have

12
been conducted in humans also demonstrating significant regression of atherosclerosis
when given recombinant apoA1Milano complexed with phospholipids to mimic properties
of nascent HDL (85, 88). It appears that the mutation results in a form of apoA1 with
elevated performance of the activities of normal apoA1. Additionally, a number of
prospective cohort studies have concluded that HDL-C and apoA1 are strong predictors
of CVD risk, with some suggesting apoA1 is the stronger predictor (58, 89-95). As a
result, some countries have expanded their clinical guidelines for decreasing CVD risk
to include apoA1, including Sweden and Norway (96). Therefore, apoA1 and HDL-C
remain potential targets for anti-atherosclerotic therapeutic strategies. In order to test whether elevation in HDL-C can improve CVD risk, methods of
increasing HDL-C have been elucidated. Those that have demonstrated success
include exercise, smoking cessation, weight loss, moderate alcohol intake and
increased MUFA consumption (16, 17, 97-99) and they have also demonstrated the
potential to reduce CVD risk (100-104). From a dietary approach, MUFAs could be
easily incorporated into the diet as they are found naturally in oils, such as olive and
canola, as well as in nuts, seeds and avocados.
2.2 Foods with cholesterol-lowering and anti-oxidative potential 2.2.1 Nuts The many health benefits of nuts have fuelled investigations into their effects on
CVD risk with many having an associated decreased risk (105-109). Some studies
indicated that a CVD risk reduction of 35% or more may be obtained with increased nut
consumption (≥ 2-5 servings per week) (110-112). As a result, nuts have been permitted
a health claim for heart disease risk reduction by the FDA stating that as part of a diet
low in saturated fat and cholesterol, consumption of 42g (1½ oz) of almonds per day
may reduce the risk of heart disease (113). In addition to studies looking at the overall
effect of nut consumption on CVD risk, many studies have investigated potential ways
by which nuts target risk factors, including effects on lipids.
LDL-C has been shown to be significantly reduced by the consumption of nuts,
primarily almonds and walnuts (114, 115). Consumption of between 68 to 100g per day

13
of almonds has been shown to result in LDL-C reductions of 7 to 29% (116, 117). Even
consuming a handful (approximately 1 ounce) of almonds a day has demonstrated
reductions in LDL-C around 4-5% (118). Almonds are an excellent source of the anti-
oxidant vitamin E, phytochemicals, flavonoids, fibre, protein, and MUFA, however
exactly which part of the nut results in the lipid benefit is unknown. Some studies
comparing the effects of the whole nut to the oil from the nut have demonstrated similar
reductions in total- and LDL-C, therefore there is the potential for the effect to arise from
the type of fats found within the almond (115), most of which is MUFA. In addition to the
lipid lowering effects, almonds have associated with a reduction in oxidative damage.
The antioxidant activity of almonds has been demonstrated in reductions in LDL
oxidizability, inflammatory molecules and endothelial dysfunction (119). Acute studies
have demonstrated that whole almonds decreased the susceptibility of lipids to
oxidation and increased the total antioxidant capacity, and did so more than compared
to walnuts (120). Additionally, studies investigating the effects of the skins of almonds
have demonstrated that the variety of polyphenols within have anti-oxidant activity
against specific radicals (121, 122). Due to the fact that the different components of
almonds have potential antioxidant activity, greater oxidative reduction may result from
the consumption of whole almonds thereby targeting a larger variety of radical types
and the health conditions that may arise from each.
2.2.2 Soy Protein
The effect of soy protein on blood cholesterol has been of interest since the early
1900s when the idea emerged that animal protein had negative consequences in the
arteries and thus a search for a plant protein replacement began (123). Compared to
lean meat protein, some studies have demonstrated soy protein significantly reduced
LDL-C around 10% versus 5%, suggesting a specific effect of proteins on cholesterol
transport and metabolism (123, 124), whereas other studies have reported significant
reductions of only 5-6% (125-131). Studies comparing the effects of soy protein to
casein protein express similar results where soy protein effective reduced LDL-C 16%
more than did the casein protein treatment (132). A meta-analysis conducted in 1995
indicated a 12.5% reduction in LDL-C as a result of an average 47g per day of soy

14
protein whereas subsequent studies did not support as great a reduction (126, 133-
135). However, in an article by Sirtori in 2007, who conducted many of the early studies
expressing the beneficial effects of soy protein, he re-evaluated the more recent studies
using a ‘nomogram’ prepared on the basis of initial cholesterol concentrations in the
1995 meta-analysis and concluded that the studies done in the past 10 years are in
agreement with the conclusion of that meta-analysis (136). Additionally, a recent meta-
analysis by Harland concluded that modest soy protein intakes of around 25g per day,
almost half as much as the 1995 meta-analysis, resulted in highly significant reductions
in LDL-C of 6%, which supports the previous meta-analysis (131).
There has been much debate over the effectiveness of soy protein versus soy
isoflavones, and over the effectiveness of highly processed soy products. However, soy
isoflavones have not acquired as much support for their cholesterol-lowering effects and
there are many studies indicating the greater the processing of soy products, the less
effective in cholesterol reduction (133-135, 137, 138). Therefore, the most effective
method of cholesterol-reduction with soy foods is by using whole soy foods which are
least processed.
Soy protein also has potential for reducing lipid oxidation. Many studies done in
animals (139-144) and in humans (145, 146) have reported significant antioxidant
activity resulting from soy protein consumption, possibly by up-regulating LDL-receptor
machinery in the liver, resulting in decreased LDL levels and LDL oxidation. Studies
have demonstrated about a 9-16% reduction in conjugated dienes in the LDL fraction
with intakes of soy foods of around 33g/d (147, 148) Again, there is debate whether it is
the soy isoflavones that contribute the antioxidant properties, however in this respect,
there is more evidence supporting its role (149, 150) in addition to those on whole soy
foods (147, 148). Overall, epidemiological studies suggest the soy consumption is
associated with a reduced risk of CVD (151).
2.2.3 Viscous Fibre
Dietary fibres can be classified based on their solubility. The insoluble fibres include
lignins and cellulose, whereas soluble fibres, also known as viscous fibres, include
natural gel-forming fibres such as pectins, gums and mucilages. Overall, dietary fibre is

15
associated with reduced risks for many diseases including many cardiovascular
diseases (152, 153). However, much of the attention on fibres is on the soluble fibres
including oats, pectins, guars and psyllium and their LDL-C lowering abilities. Common
foods high in viscous fibre include whole oats, barley, psyllium powder, oat bran,
eggplant, and okra. Many studies have demonstrated reductions of 7-9% in LDL-C and
that intakes of only 3g of soluble fibre can have significant reductions in LDL-C of
0.13mmol/L (154) and the consumption of fibre from 3 apples or 3 bowls (28g) of
oatmeal can result in total-C reductions of 2% (154, 155). There are a few possible
mechanisms of effect including increased bile acid output resulting in less reabsorption
of cholesterol and greater usage of cholesterol for hepatic bile acid synthesis (156,
157), inhibition of hepatic fatty acid synthesis by products of fermentation (158), and
changes in intestinal motility (159). Studies of soluble fibre have also shown reductions
in small LDL subfractions which are associated with more atherogenic conditions (160).
In addition to the cholesterol-lowering effect of viscous fibres, other
cardiovascular benefits include reductions in the inflammatory marker CRP (161, 162)
and blood pressure (163, 164) and some studies have demonstrated the potential for
antioxidant activity. Animal studies have demonstrated guar gum can increase
antioxidant protein expression and therefore decrease oxidative stress-induced arterial
injury (165). Also, since oxidative stress can result from inflammation, the anti-
inflammatory potential of fibre is also of interest. In the Iowa Women’s Health Study,
whole grain consumption was associated with a reduced risk of death attributed to
inflammatory diseases which were noncardiovascular of >35% for those who reported
the highest intake (≥ 22.5 servings per week) and since whole grains are an excellent
source of fibre, there is potential for fibre to play a role in reducing inflammation (166).
The same group analyzed the total antioxidant capacity in over 1000 food samples
obtained from the US Department of Agricultural National Food and Nutrient Analysis
Program and found that several whole grain products were at the top of the ranked list
(166). This may be the result of increased enterlactone concentrations associated with
whole grain intake, as a product of lignin precursors within whole grains, which have
anti-oxidative activity (166).

16
Overall, the multifactorial effects of viscous fibre and its large range availability
make it an attractive addition to obtain greater cardiovascular health.
2.2.4 Plant Sterols and Stanols Plant sterols and stanols are structurally similar to cholesterol with sterols being
found naturally in plant foods such as vegetable oils, nuts and seeds, and stanols being
commercially available hydrogenated sterols (167). They are believed to exert their
cholesterol-lowering abilities by decreasing the absorption of dietary and biliary
cholesterol, thus increasing cholesterol synthesis and the activity of LDL-receptors and
ultimately reducing serum LDL-C concentrations (167, 168). Studies have
demonstrated these effects over the past 40 years with plant sterols/stanols enriched in
vehicles such as margarines, dairy products and orange juice and have shown that for
consumption of 3.4g of esterified plant sterol/stanol (or 2.1g plant sterol/stanol)
reductions in LDL-C range from 5 to 16% (169-172), with margarines, the more
common vehicle, averaging about 11% reduction (169). As a result, the United States
Food and Drug Administration (FDA) granted plant sterols health claim status for CHD
risk reduction (113) and NCEP ATP III recommends them for cholesterol reduction (19).
Although there have been some studies questioning the safety of plant sterols (173-
177), many studies have alleviated those concerns (178-182) and a recent review
assessing their efficacy and safety concluded that they are important for cholesterol-
lowering and good heart health (183).
There is also some evidence for potential anti inflammatory and antioxidative
effects of plant sterols. Some studies have shown they may inhibit the secretion of
inflammatory mediators, such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-
α), although most of these studies have been done in animals (184). The studies on
their antioxidative effects have been done in humans and demonstrate a reduction in
ox-LDL with 2-3g plant sterol consumption, thus suggesting the potential to protect LDL
from oxidation (185, 186). However, some studies have shown no effect (187).
As a result of their cholesterol-lowering ability and the potential for anti
inflammatory and antioxidative activity, plant sterols may contribute to reducing CVD
risk.

17
2.2.5 The Dietary Portfolio
In the late 1990s with the growing interest in diet in the management of elevated
blood lipids and the many studies investigating the cholesterol-lowering effects of
particular foods, many organizations began recognizing key foods which had
demonstrated effectiveness in cholesterol reduction. The NCEP ATP was
recommending 2g/d of plant sterols and 10-25g/d of viscous fibre (19) and the AHA was
encouraging the consumption of soy proteins (188) for the management of elevated
cholesterol. The FDA had also approved health claims for plant sterols (113), viscous
fibres (189) and soy protein (190). Mechanistically, studies had shown that viscous
fibres increased bile acid losses (191-193), plant sterols increased fecal cholesterol
losses (194, 195) and soy proteins decreased hepatic cholesterol synthesis and
increased LDL-receptor-mediated cholesterol uptake (196, 197). With this information,
Dr. David Jenkins saw the potential for greater cholesterol reduction through dietary
means and therefore combined these foods into what he termed the “dietary portfolio”.
In a preliminary study combining 1.2g/1000kcal plant sterols, 8.3g/1000kcal viscous
fibres, and 16.2g/1000kcal soy protein, as well as 2.9g/1000kcal of almonds as an
added source of vegetable protein and because it also had previously demonstrated the
potential for cholesterol reduction (114), Dr. Jenkins found this dietary portfolio had an
additive effect in lowering LDL-C by 29% (198). With these results, and an FDA health
claim for nuts which encouraged an increase in the contribution of almonds to
16.2g/1000kcal in the dietary portfolio, a series of studies assessing the many benefits
of this dietary portfolio began (8). When tested alongside a first generation statin, the
dietary portfolio demonstrated LDL-C reductions of a similar magnitude (30.9% and
28.6%, respectively), as well as reductions in hs-CRP (33.3% and 28.2%, respectively)
(10). When assessed for long-term effects under real-world conditions, as opposed to
metabolically controlled, 14% and 12% reductions in LDL-C were seen at 3 months and
1 year, respectively, with >30% of subjects maintaining a reduction >20% (199).
Additionally, significant reductions in blood pressure (200), haematological indicies

18
(201) and reductions in the smallest and most atherogenic subclass of LDL-C (202)
have also been demonstrated over the years. Most recently, strawberries were added to
the dietary portfolio and demonstrated significantly improved palatability and reductions
in TBARS as a measure of oxidative stress, while maintaining reductions in blood lipids,
therefore suggesting that added berries may improve the overall utility of the diet (12). It
is thus of interest to continue to explore methods of improving this effective cholesterol-
lowering diet to further reduce the risk of CVD.
2.2.6 Monounsaturated Fatty Acids (MUFAs) With interest in determining the best replacement for SFA, many studies have
looked into the effect of MUFA compared to carbohydrates and PUFA. In terms of
effects on blood lipids, all three of the above food components are effective in
cholesterol reduction when compared to the average American diet (203, 204).
However, when looking into the relative effects on markers of oxidation, many studies
have demonstrated a significant difference with MUFA being the better choice.
MUFA consumption has been found to result in less oxidative modification of
LDL-C compared to when PUFAs are consumed (205), and additionally, when
carbohydrate is replaced by MUFA there are reductions in such measurements of
oxidation as LDL oxidation lag phase and TBARS (203, 206, 207). There are also many
studies which conclude that MUFAs are the preferred substitution due to a greater
potential risk reduction for CVD (203, 208). The AHA also indicates in its statement that
there are prospective observational studies which document that diets rich in MUFAs
are associated with a decreased risk of CHD (100).
MUFAs are most commonly found in oils such as olive and canola, as well as in
nuts, seeds and avocados. Many studies on olive oil on risk of CVD have demonstrated
reductions in markers of oxidative stress. One study which fed participants olive oil at
real-life doses (25mL/day), found a significant increase in the oleic/linoleic acid ratio in
LDL-C and that with every 1 unit increase in the ratio, there was an associated
decrease of 4.2ug/L in plasma isoprostanes, an in vivo measure of ox-LDL (209). Other
studies have also demonstrated how an increase in the amount of oleate in the diet can
reduce the susceptibility of LDL to oxidative modification (210).

19
There is also interest in MUFA because of the potential to raise HDL-C, which is a
risk factor for CVD when levels are low. Although some studies have found no effect of
increased MUFA consumption on HDL-C levels (211-214), there are many studies
which provide support for their potential (203, 215, 216). In the early 1970s when the
interest in HDL-C as a cardioprotective factor began and the search for a suitable
replacement for SFA was of interest, large quantities of PUFA (as much as 20 to 30% of
total calories) were demonstrated to result in great reductions in HDL-C along with LDL-
C, whereas MUFA replacements reduced LDL-C while preserving HDL-C (207, 217).
Studies trying to explain these results compared the different fatty acids to carbohydrate
and found that each had HDL-C raising effects relative to carbohydrate, with PUFAs
having the least and SFA having the greatest with MUFA closely following (218, 219).
Further investigations demonstrated that the decreases in HDL-C and apoA1 were
associated with increased fractional clearance of apoA1, which was later supported by
further evidence showing decreased HDL-C was associated with reduced apoA1
production in addition to increased apoA1 clearance (220, 221). Therefore it is possible
that MUFA may raise HDL-C by increasing secretion of apoA1 or reducing its clearance.
Investigation into the kinetics of HDL-C and apoA1 suggest possible mechanisms
by which these levels are affected. These began as a result of many negative
correlations observed clinically between plasma TG levels, HDL-TG content and fasting
plasma HDL-C and apoA1 concentrations (222-226). Studies have demonstrated that
the metabolism of HDL-C is affected by the interactions between TG-rich lipoproteins
and HDL-C in plasma in at least two ways; firstly, through the lipolytic enzyme
lipoprotein lipase (LPL) which breaks down TG-rich lipoproteins forming surface
materials transferred to HDL, impacting its maturation (227-229), and secondly, through
the cholesterol ester transfer protein (CETP) which transfers TGs from TG-rich
lipoproteins to HDL in exchange for cholesterol esters (CE) producing TG-rich, CE-poor
HDL which is more prone to catabolism (230-232). Kinetic studies in humans with
hypertriglyceridemia and low HDL-C have demonstrated that there is a significant
increase in the fractional catabolic rate of apoA1 but no reduction in apoA1 production
rates, therefore it is the enhanced clearance of HDL-C and apoA1 rather than a reduced
production of HDL-C resulting from LPL which may contribute to the reduced

20
concentration of HDL-C (233-237). However, authors of these studies note that the
CETP-mediated lipid exchange process itself can reduce plasma HDL-C but must be
coupled with additional processes in order to reduce apoA1 concentrations which
include the following: 1. TG-rich, CE-poor HDL are thermodynamically less stable and
have the apoA1 more loosely bound, 2. TG-rich, CE-poor HDL are more readily
lipolyzed by hepatic lipase (HL), which reduces HDL size and releases apoA1, 3.
smaller HDL are more readily cleared from circulation (Figure 4). Since CETP is highly
dependent on the concentration of TG-rich lipoproteins in the plasma, it is possible that
by decreasing the concentration of TG in the circulation through decreasing glucose or
carbohydrate intake by replacement of MUFA, HDL-C and apoA1 concentrations can be
preserved by the converse of this proposed mechanism.
Figure 4: Design of the proposed mechanism of HDL-C lowering (238).
Therefore, increased MUFA consumption by replacement of carbohydrate, may
decrease oxidative stress directly through free radical quenching as supported in
studies where less oxidation is observed when SFA is replaced by MUFA compared to
replacement by PUFA, or indirectly through reductions in glucose fluctuations and thus
TG production, potentially preserving HDL-C along with its antioxidative properties.

21
3. Hypothesis, Objectives, and Rationale

22
3.1 Hypothesis Increasing the dietary intake of MUFA will increase levels of HDL-C compared to
the lower fat, higher carbohydrate diet, and decrease oxidative stress through reduced
ox-LDL and increased protein thiols indicative of a protection of plasma proteins.
3.2 Objectives Overall Objective: To assess the effect on serum lipids and oxidative damage to
proteins and lipids of the replacement of carbohydrate with MUFA in
a cholesterol-lowering diet.
1. To determine the effect of a cholesterol-lowering dietary
portfolio combined with either high- or low-MUFA on HDL-C and
apoA1.
2. To determine the effect of a cholesterol-lowering dietary portfolio
in combination with either a high- or low-MUFA on oxidative
damage to protein and lipids, as assessed by protein thiols and
CD and TBARS in the LDL fraction, respectively.
3. To determine the effect of a cholesterol-lowering dietary portfolio
combined with either high- or low-MUFA on LDL-C and apoB.
4. To determine the effect of a cholesterol-lowering dietary portfolio
combined with either high- or low-MUFA on the total:HDL-C ratio
and the apoB:A1 ratio.
3.3 Rationale The dietary portfolio is a combination of foods which have been individually
researched as effective in blood lipid control and to have some antioxidant activity.
Previous dietary portfolio studies have consistently demonstrated significant reductions
in LDL-C (10, 198, 199, 239). Recently, there is increasing concern in the risk factors for
CVD other than LDL-C due to the residual risk that remains once LDL-C has been
effectively reduced. One such risk factor includes low HDL-C which is present in over a
third of adult men and women. Studies have suggested that for every 0.026mmol/L
increase in HDL-C, there is a corresponding 1-3% decrease in CVD risk (53-55, 97).

23
There is much evidence that both MUFA and HDL-C have antioxidative potential
and that the former may increase the later (13, 66, 71, 203, 218, 219, 240, 241). MUFAs
can easily be incorporated into the diet through the use of high-MUFA oils including
olive and canola oil, as well as avocados, nuts and seeds.
It therefore is appropriate to combine a high-MUFA background diet to an already
effective cholesterol-lowering diet to further reduce the risk of CVD.

24
4. Study: The Effect of Adding Monounsaturated Fat to a Dietary Portfolio of Cholesterol-Lowering
Foods in Hypercholesterolemia

25
The Effect of Adding Monounsaturated Fat to a Dietary Portfolio of Cholesterol-Lowering Foods in Hypercholesterolemia
4.1 Abstract
Background: Higher monounsaturated fat intakes may raise HDL-C without raising
LDL-C. We have therefore tested whether increasing the monounsaturated fat (MUFA)
content of an effective LDL-C lowering diet (dietary portfolio) both increases HDL-C and
further reduces the total:HDL-C ratio, two key risk factors for CVD.
Methods: Twenty-four hyperlipidemic participants took a very low-saturated-fat
therapeutic diet for one month and then were randomized to a low- or high-
monounsaturated-fat dietary portfolio for a further month. Food was provided for the 2
month period with calorie intake based on Harris-Benedict estimates for energy
requirement.
Results: On the high-MUFA dietary portfolio, HDL-C rose 13.1±3.6% (P=.004),
whereas on the low-MUFA dietary portfolio, HDL-C did not change (2.7±3.6%, P=.466)
(treatment difference, P=.004). The respective figures for the total:HDL-C ratio were -
24.5±2.1% (P<.001) on high-MUFA versus -17.6±3.0% (P<.001) on low-MUFA
(treatment difference, P=.006). These treatment differences were associated with
significantly higher apoA1 concentrations on high-MUFA dietary portfolio. CRP was also
significantly reduced on the high-MUFA dietary portfolio. No treatment difference was
seen in body weight although a mean weight loss was seen over both low-MUFA (-0.98
± 0.26kg) and high-MUFA (-0.78 ± 0.21kg) diets.
Conclusions: Monounsaturated fat increased the effectiveness of a cholesterol-
lowering dietary portfolio and may reduce cardiovascular risk through raising HDL-C,
further lowering the ratio of total:HDL-C and also by reducing CRP.

26
4.2 INTRODUCTION
Strategies that combine cholesterol-lowering foods or food components such as
viscous fibres and plant sterols have been recommended to enhance the effectiveness
of therapeutic diets low in saturated-fat and cholesterol (19, 242). Such dietary
combinations (dietary portfolio) have resulted in substantial reductions in LDL-C (10)
and its apolipoprotein, apoB, but the effects on HDL-C and its apolipoprotein, apoA1,
have been less apparent (199). Low plasma HDL-C and apoA1 concentrations and an
elevated ratio of total:HDL-C are recognized risk factors for CVD (243-247). Thus,
dietary strategies that both lower total and LDL-C and raise HDL-C should have broad
application. One method for increasing HDL-C appears to be the use of
monounsaturated fat (MUFA), particularly when MUFA replaces dietary carbohydrates
(248, 249). Furthermore, increased intakes of MUFA through increased nut
consumption and vegetable oil intake has been associated with a reduced incidence of
CVD in cohort studies (250, 251).
We have therefore compared the effect on serum lipids of substituting 13.0% of
total calories as carbohydrate for MUFA in a dietary portfolio that has been shown to be
effective under controlled conditions in lowering LDL-C by 28% and the total:HDL-C
ratio by 24% (10).
4.3 METHODS
4.3.1 Participants
Men and women with mild to moderate hypercholesterolemia were recruited from
the Clinical Nutrition and Risk Factor Modification Centre at St Michael’s Hospital,
Toronto, Ontario, and from newspaper advertisements. Only postmenopausal women
were recruited because of the increase in LDL-C and CHD risk in women of this age
and to avoid possible fluctuations in blood lipids related to the menstrual cycle.
Participants were selected who had previously demonstrated LDL-C levels >4.1 mmol/L
(19, 242). No participants were recruited if they had a history of cardiovascular disease,
untreated hypertension (blood pressure >140/90mmHg), diabetes, or renal or liver
disease, or were taking medications known to influence serum lipids apart from stable
doses of thyroxine. All medications and supplements were expected to be taken at a

27
constant dose prior to and during the study. Iron supplementation, ferrous gluconate
7mg tid (Salus-Haus, Bruckmuhl, Germany), was provided to participants on the basis
of a prestudy ferritin of <50mcg/L.
4.3.2 Study Protocol The study followed a randomized parallel design and was carried out between
August 2007 and April 2009. Participants were counselled to follow their own low-
saturated- fat therapeutic diets for 1 month prior to the start of the study. They were
then provided with a very low-saturated-fat dairy and whole-grain cereal metabolically
controlled diet which acted as a stabilization period prior to the high- and low-MUFA
diets. After one month on this metabolically-controlled diet, they were randomized to
take either a high-MUFA or conventional (low-MUFA) dietary portfolio for a final month.
Throughout the study participants attended weekly clinic visits where body weight
was taken and blood pressure was measured three times in the non-dominant arm
using an automated digital blood pressure monitor (OMRON Healthcare Inc, Vernon
Hills, Illinois) by the same observer. At 2-week intervals blood samples were obtained
after 12-hour overnight fasts. A seven-day diet history was obtained for the week prior
to the 2-month metabolic treatment period. Completed menu checklists were returned at
weekly intervals, as well as 7-day exercise records, during the 4-week diet periods and
checked by the dietitians, who also checked the participants’ exercise and ensured that
it was constant over the course of the study period. Exercise was calculated as
metabolic equivalent of tasks (METs) (252).At weekly intervals, participants recorded
their overall feeling of satiety using a 9-point bipolar semantic scale in which −4 was
extremely hungry, 0 was neutral, and +4 was uncomfortably satiated.
Participants were randomized to the low- and high-MUFA portfolio diets and
stratified on the basis of sex and an LDL-C of <4.2mmol/L or >4.2mmol/L during the first
2 weeks of the 4 weeks of the very low-saturated-fat therapeutic control diet by the
statistician using a random number generator and SAS version 9.1 software (SAS
Institute Inc, Cary, NC) (253) in a separate location from the clinic. The dietitians were
not blinded to the diet because they were responsible for patients’ diets and for
checking diet records. The laboratory staff responsible for analyses were blinded to

28
treatment and received samples labelled with name codes and dates. The study was
approved by the ethics committees of the University of Toronto, St. Michael’s Hospital
and the Natural Health Products Directorate of Health Canada. Written informed
consent was obtained from all participants. Participants were offered no financial
compensation for participation in the study. The clinical trial registration number is
NCT00430430.
4.3.3 Diets
The diets eaten before the 8-week study were the participants’ routine
therapeutic low-fat diets, which were similar to current National Cholesterol Education
Program guidelines (<7% energy from saturated fat and <200 mg/d of dietary
cholesterol) (19) and previously referred to as a Step II diet (248) (Table 2). During the
8-week study period, diets were provided based on estimated caloric requirements
using the Harris-Benedict equation. Foods were sourced from Loblaws supermarket in
Toronto and health food stores. All diets were vegetarian. In the case of the high- MUFA
diet, 13.0% dietary calories as carbohydrate was replaced by MUFA in the dietary
portfolio. MUFA was given in the form of a high-MUFA sunflower oil which contained
80% MUFA. Participants were also given the option to substitute a portion of the high-
MUFA oil with a calculated amount of avocado. The aim of the dietary portfolio was to
provide 1.0 g of plant sterols per 1000 kcal of diet in a plant sterol ester–enriched
margarine (Flora Pro-Activ, Unilever, London, England) with a minimum of 2g/d and a
maximum of 3g/d of plant sterols. The diet also provided 10.3 g of viscous fibres per
1000 kcal of diet from oats, barley, and psyllium; 20 g of soy protein per 1000 kcal as
soy milk, tofu and soy meat analogs; and 21.5 g of whole almonds per 1000 kcal of diet.
Emphasis was placed on eggplant and okra as additional sources of viscous fibre (0.2
g/1000 kcal and 0.4 g/1000 kcal, respectively). Eggs (2/wk) were also provided in the
dietary portfolio to balance the saturated fat and dietary cholesterol in the very low-
saturated-fat therapeutic control diet (Table 3). This dietary portfolio has been described
in detail previously (10).
The very low-saturated-fat therapeutic control diet as eaten in the first month
used skim milk, fat-free cheese and yogurt, and egg substitute and liquid egg white to

29
achieve a low intake of saturated fat. High fibre intake was obtained by the use of
wholegrain breakfast cereals (fibre, 2.5g/1000 kcal of diet) and bread (fibre, 3g/1000
kcal of diet) made from 100% whole wheat flour. This diet therefore lacked sources of
viscous fibres, plant sterols, soy protein and nuts. The macronutrient profile of the diet
recorded as consumed over the 4 weeks achieved a saturated fat intake of <5% of total
calories with <50mg cholesterol/1000kcal (Table 3).
Participants were provided with self-tarring electronic scales (Tanita
Corporations, Arlington Heights, USA) and asked to weigh all food items consumed
prior to and during the study period. During the study period, all foods to be consumed
by participants were provided initially by courier and then at weekly clinic visits, with the
exception of fruit and low calorie, non–starch-containing vegetables (8% and 24% of
dietary calories respectively from high- and low-MUFA diets). Okra was the exception
and was provided for the dietary portfolio. Participants were instructed to obtain specific
fruit and vegetables from their local stores and were reimbursed on presentation of
receipts. Participants were provided with 7-day rotating menus (Table 4). The diets have
been described in detail previously (10).
Dietary compliance was assessed from the completed weekly checklists and
from the return of uneaten food items.
4.3.4 Analyses
All serum samples from a given individual were labelled by code and analyzed in
the same batch. Serum was analyzed according to the Lipid Research Clinics protocol
(254) for total cholesterol, triglycerides, and high-density lipoprotein cholesterol (HDL-C)
by detergent solubilization and measurement of HDL-C (Roche Hitachi 917; Roche
Diagnostics, Laval, Quebec, Canada), in the J. Alick Little Lipid Research Laboratory.
Low-density lipoprotein cholesterol (LDL-C) was calculated (255). Serum apoA1 and
apoB were measured by nephelometry, which is a measurement of scattered light by a
dilute suspension of small particles (Dade BehringBNProSpec; Dade Behring Canada
Inc, Mississauga, Ontario) (intra-assay coefficient of variation, 2.2% and 1.9%,
respectively) (256). Serum samples, stored at −70°C, were analyzed for hs-CRP by
end-point nephelometry (coefficient of variation, 3.5%) (Behring BN-100, N high-

30
sensitivity C-reactive protein reagent, Dade- Behring, Mississauga, Ontario). Diets were
analyzed using a program based on US Department of Agriculture data (257) and
developed in our laboratory to allow addition of data on foods relevant to ongoing
studies after analysis in the laboratory for protein, total fat and dietary fibre using
American Organization of Analytical Chemists methods and fatty acids by gas
chromatography (10).
4.3.5 Statistical Analysis Results were calculated as mean±SE. The study was an efficacy study with HDL-
C as the primary outcome in the direct comparison of high- and low-MUFA dietary
portfolio treatments. Since no within treatment difference was seen between weeks 2
and 4 and between weeks 6 and 8, the significance of the differences between
treatments was assessed by the CONTRAST statement in SAS using all post baseline
values (SAS PROC GLM) (258). The analysis used the change from baseline to weeks
2 and 4 for the very low-saturated-fat therapeutic control. The same weeks 2 and 4 of
the control diet, in turn, acted as the baseline for the high- and low-MUFA dietary
portfolios with weeks 6 and 8 as end of treatment response variables. Treatment, sex
and their interaction were main effects, with baseline (mean of control weeks 2 and 4 in
the portfolio analyses) as covariate. A 2-tailed paired t test was used to assess the
significance of the within treatment (weeks 2 and 4) percentage change from baseline
for the control and between weeks 2 and 4 (averaged) versus weeks 6 and 8
(averaged)for the high- and low-MUFA dietary portfolio groups. Means of weeks 2 and 4
data and weeks 6 and 8 data are presented in text and Tables.
With 12 participants per treatment group, and assuming an 8% SD of effect with
α=.05 and 1-β=.80, we had sufficient power to detect a 9.6% change in HDL-C between
treatments as significant.
4.4 RESULTS
4.4.1 Participants Twenty-four healthy, hyperlipidemic participants were randomized to either the
high- or low-MUFA arms of the study (17 men and 7 postmenopausal women) (Figure

31
1).Their baseline characteristics were similar (Table 1). Six participants had been taking
statins and, after obtaining approval from their primary care provider, discontinued them
as required by the study protocol at least 2 weeks prior to the study (3 low-MUFA and 3
high-MUFA dietary portfolio participants).
When expressed as the percentage of prescribed calories recorded as eaten
over the 4 week period, compliance was high for all 3 diets: 93±2% for the very low-
saturated-fat therapeutic control, 95±2% for the high-MUFA, and 91±2% for the low-
MUFA dietary portfolio. At the end of each treatment all participants believed they were
eating as much food as they were capable without experiencing discomfort (rating >3.0).
Satiety ratings for treatments were: control, 2.1±0.2; high-MUFA dietary portfolio,
2.3±0.3; and low-MUFA dietary portfolio, 2.0±0.3. Participants lost a similar amount of
weight on all 3 one- month treatments (control, -1.10±0.2kg; P<.001; high-MUFA dietary
portfolio, -0.78±0.21kg; P=.003; low-MUFA dietary portfolio, -0.98±0.26kg; P=.003).
4.4.2 Blood Lipids and C-Reactive Protein
For the stabilization control diet, no treatment differences in baseline or weeks 2
and 4 blood measurements were observed between the 2 treatment groups (Table 5)
who would subsequently be randomized to either high- or low-MUFA Portfolio diets
(Figures 2 and 3). The mean percentage change from baseline using the data for the 24
participants was -15.6±1.4% (P<.001) for total-C, -21.5±2.0% (P<.001) for LDL-C, and
7.9±2.7% (P=.008) for HDL-C. The percentage changes were also significant for the
total:HDL-C ratio (-21.9±1.9%, P<.001), apoA1 (3.7±1.6%, P=.028), apoB (-17.6±1.5%,
P<.001) and the apoB:A1 ratio (-20.4±1.9%, P<.001). However the change in TG was
not significant (-12.0±6.4%, P=.073).
For the dietary portfolio comparisons (Table 6), there were significant increases
on high-MUFA but not low-MUFA in HDL-C, 13.1±3.6% versus 2.7±3.6% (P=.002); and
apoA1, 7.8± 2.2% versus -0.4±1.5% (P=.001). There were also significant reductions on
high- versus low-MUFA in total:HDL-C, -24.5±2.1% versus -17.6±3.0% (P=.006); and
apoB:A1, -23.2±1.6% versus -17.6±2.3% (P=.013). Similarly, hs-CRP was reduced on
the high-MUFA, -37.5±10.6% but not on the low-MUFA dietary portfolio 45.3±33.4%
(P=.003) (Figures 2 and 3).

32
There were no between treatment differences in LDL-C or apoB. However,
significant within treatment reductions were seen on both high- and low-MUFA for LDL-
C, −20.9±2.6% (P<.001) versus −22.1±3.1% (P<.001) and apoB -17.2±2.1% (P<.001)
versus -18.0±2.2% (P<.001).
4.4.3 Blood Pressure
No significant treatment difference was observed in blood pressure (Tables 5 and 6).
4.4.4 Drop outs and Adverse Events
No participant withdrew from the study after the randomization which occurred
during the first and second week of the control phase. One participant withdrew at the
time of the first control breakfast, and therefore prior to randomization, due to the
perceived inconvenience of a metabolically controlled diet. No adverse events related to
the study protocol were reported.
4.5 DISCUSSION
The present study demonstrated that replacement of 13.0% of total calories from
carbohydrate by MUFA in the dietary portfolio, while not altering the LDL-C reduction,
resulted in a 10.4% greater increase in HDL-C over the 4 weeks. There was also a
6.9% greater reduction in the atherogenic index, total:HDL-C (247, 259) when
compared to the low-MUFA dietary portfolio. This increase in HDL-C is of similar
magnitude to two gemfibrozil studies which raised HDL-C concentrations by 6% and 8%
and resulted in reductions in the relative risk of CHD of 22% and 23%, respectively
(260, 261). The addition of MUFA by increasing HDL-C may therefore further enhance
the cardioprotective effect of the cholesterol-lowering dietary portfolio.
The lines of evidence for a cardioprotective effect for HDL-C include
epidemiologic and especially cohort studies (262-264). Measurements in the
Framingham cohort have resulted in inclusion of the total:HDL-C ratio as the lipid
parameter in the widely used Framingham CHD risk predictive equation (247) and post-
hoc analysis of statin trials have identified HDL-C as predictive of major cardiovascular
events even in participants whose LDL-C levels were optimized with a statin (243).

33
Intervention trials using gemfibrozil have also supported a cardioprotective role for
raising HDL-C (261, 265), as have studies of apoA1 infusion, the apolipoprotein of HDL,
which has been associated with plaque regression documented with intravascular
ultrasound measurements (88, 266). These data together with laboratory studies (267,
268) have supported the concept that HDL is involved in reverse cholesterol transport,
anti-oxidant and anti-inflammatory activities indicative of cardioprotective effects (97,
98).
Consequently, much emphasis has also been placed recently on lifestyle
strategies to raise HDL-C including exercise (16, 17), weight loss (16, 17), moderate
alcohol intake (16, 17), smoking cessation (16, 17), and increased monounsaturated
fatty acid intake (17, 99, 208, 269). The increased MUFA intake is the only strategy
relevant to the present study since participants were instructed to hold exercise
constant, weight loss was similar in all treatments, alcohol intake was very small (a
deviation from the dietary protocol but constant over both treatments), and no
participant smoked.
Although some reservations have been expressed over the use of
monounsaturated fats in preventing arteriosclerosis (270), previous studies have also
noted the advantages of monounsaturated fat on the blood lipid profile, especially in
type 2 diabetes, which is characterized by raised triglyceride and low HDL-C
concentrations (271). Early studies showed that glycemic control was improved, serum
triglycerides reduced and HDL-C increased with 25% substitution of carbohydrate by
MUFA (215). Later studies have shown more variable results using a 15% calorie switch
from carbohydrate to MUFA with reductions in VLDL-cholesterol and triglyceride but no
change in HDL-C (272-274). In the present study, triglyceride was significantly reduced
on the high- MUFA diet compared with the control diet but the treatment difference was
not significant. The higher HDL-C and apoA1 on the high-MUFA compared to the low-
MUFA diet resulted in significant reductions in the total:HDL-C and apoB:A1 ratios.
These changes would be expected to reduce the risk for CHD (247).
The mechanisms by which MUFAs increase HDL-C are likely to be several. They
include the ability of MUFA to scavenge free radicals (203, 275), reduce adipose tissue
synthesis of pro-inflammatory cytokines and the stimulus to hepatic acute phase protein

34
synthesis, such as CRP. This metabolic environment would also allow increased
synthesis of negative acute phase proteins, such as HDL, as seen in the present study.
Our data are consistent with such a hypothesis, since plasma CRP concentration was
reduced with the high-MUFA dietary portfolio. In addition, the displacement of dietary
carbohydrates by MUFA is likely to result in less carbohydrate induced hepatic VLDL-
TG synthesis(238). The resulting lower, VLDL-TG concentration, although not
significant in the present study, may attenuate the impact of cholesterol-ester transfer
protein (CETP) in depleting cholesterol ester of HDL (276, 277), thereby contributing to
a rise in plasma HDL-C concentration. The resulting TG-poor cholesterol-ester-rich HDL
would also be predicted to be less rapidly lost from the circulation by tissue uptake than
a TG-rich cholesterol-ester-poor particle (228, 238, 278) and this is consistent with the
observed increase in apoA1 concentrations after the high-MUFA dietary portfolio (99,
269).
The limitations of the study include the relatively small subject numbers, weight
loss, and the prescriptive nature of the diet, since adherence to the diet may be
considerably less when eaten as a self-selected diet under real-world conditions.
Despite these concerns, the effect size of the measurements of specific interest, HDL-C
and apoA1 and their ratios, were substantial. In our post-hoc analysis, although our
effect size for HDL-C was somewhat larger than expected (10.4% versus 9.6%), the
standard deviation of effect was also larger (12.5% versus 8%) and resulted in only 50%
power (α=0.05). Nevertheless, the apolipoprotein of HDL-C, apoA1, with an effect size
of 8.2% and a standard deviation of 6.6%, provided 83% power to detect the effect size
as significant in favour of MUFA (α=0.05). Even though there was weight loss on all
treatments, the loss of weight was similar and furthermore, did not influence the
outcomes when included as a covariate in the statistical model. In terms of metabolically
controlled conditions of the study, it is true that when the dietary portfolio has been
consumed under self-selected real-world conditions, a mean adherence to the
prescribed diet of only 64% was observed at 1 year (199). On the other hand, the high
degree of adherence (95 and 91%) recorded on the present metabolic diets (low- and
high-MUFA respectively) has allowed treatment differences to be more clearly
demonstrated with relatively small subject numbers.

35
It should also be emphasized that the participants were largely non-obese
(15/24), generally physically active, non-smokers on very low-saturated-fat diets. The
MUFA increase therefore represented an addition to an otherwise healthy lifestyle and
does not address the issue of the increased use of MUFA by those whose diet and
lifestyles may be suboptimal (270). It would therefore be of great interest to test how
addition of MUFA to an effective LDL-C lowering dietary portfolio can further increase
plasma HDL-C in individuals with low levels such as those with the metabolic syndrome
and type 2 diabetes.
The strengths of the study include the large effect size and the dietary metabolic
control that ensured the uniform and very specific exchange of carbohydrate for MUFA
in the diet. The study was also unique in determining the effect of adding MUFA to a
diet which already had powerful cholesterol-lowering ability due to the very low-
saturated-fat content and the use of nuts, viscous fibres (279), plant sterols (168, 171)
and soy products (126, 128). The present study therefore demonstrated that MUFA
preserved the HDL-C and apoA1 concentrations and so significantly increased the
therapeutic potential of this dietary approach (246, 260-262, 280).
The total reductions in LDL-C and the total:HDL-C ratio on both the high- and
low-MUFA dietary portfolio treatments which plateaued after 2 weeks were as large as
any reported in previous Portfolio studies (Figures 2 and 3) (10). Expressed as the
reduction from the start of the metabolic diets and including the reductions on both the
therapeutic control diet and the further decrease on the high- or low-MUFA dietary
portfolios, the total LDL-C reductions were 35.0% and 35.2% respectively. These LDL-C
reductions are similar to those recorded in many of the earlier statin trials which resulted
in 30-35% reductions in CHD risk (281).
At present, although there are no guidelines that specifically recommend raising
HDL-C, the NCEP ATP III have a cut point for HDL-C of ≥1.0mmol/L with cut points for
the metabolic syndrome of >1.0mmol/L for men and >1.3mmol/L for women (7) and the
2009 Canadian Cardiovascular Society Guidelines stratify cardiovascular risk for
therapeutic purposes based partially on total:HDL-C ratio of >4 for high, >5 for medium,
and >6 for low risk (18).

36
In conclusion, the CHD risk reduction potential of an effective cholesterol-
lowering diet may be significantly enhanced by inclusion of a moderate amount of
monounsaturated fat.

37
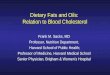
Figure 1: Patient flow diagram. *Chose not to participant (n=12): medical issue arose (n=4), want to lose weight (n=2), not willing to go off statin (n=1), not willing to stop vitamin supplements (n=1), not willing to give blood (n=1), not willing to do kinetics test (n=1), family issue (n=1), not interested (n=1).
Eligible after Telephone Screening (n=84)43M:41F
Excluded (n=59)59–Not meeting inclusion criteria
Drop Out (n=14)6–Chose not to participate*8-unable to contact
Excluded (n=1)1 –Not meeting inclusion criteria
Telephone screening (n=162)76M:86F
Attended Information Session (n=70)39M:31F
Drop Out (n=19)19 – time commitment
Drop Out (n=6)6-chose not to participate*
Clinical Assessment (n=63)34M:29F
Excluded (n=11)11–Not meeting inclusion criteria
Control Diet (n=25)17M:8F
Drop Out (n=27)27–scheduling difficulties
Drop Out (n=1)1-drop out after 1 day on diet
Randomized (n=24)17M:7F
Completion Control (n=24)17M:7F
Allocated to High-MUFA (n=12)8M:4F
12 Completed9M:3F
12 Completed8M:4F
Allocated to Low-MUFA (n=12)9M:3F
Eligible after Telephone Screening (n=84)43M:41F
Excluded (n=59)59–Not meeting inclusion criteria
Drop Out (n=14)6–Chose not to participate*8-unable to contact
Excluded (n=1)1 –Not meeting inclusion criteria
Telephone screening (n=162)76M:86F
Attended Information Session (n=70)39M:31F
Drop Out (n=19)19 – time commitment
Drop Out (n=6)6-chose not to participate*
Clinical Assessment (n=63)34M:29F
Excluded (n=11)11–Not meeting inclusion criteria
Control Diet (n=25)17M:8F
Drop Out (n=27)27–scheduling difficulties
Drop Out (n=1)1-drop out after 1 day on diet
Randomized (n=24)17M:7F
Completion Control (n=24)17M:7F
Allocated to High-MUFA (n=12)8M:4F
12 Completed9M:3F
12 Completed8M:4F
Allocated to Low-MUFA (n=12)9M:3F
Clinical Assessment (n=63)34M:29F
Excluded (n=11)11–Not meeting inclusion criteria
Control Diet (n=25)17M:8F
Drop Out (n=27)27–scheduling difficulties
Drop Out (n=1)1-drop out after 1 day on diet
Randomized (n=24)17M:7F
Completion Control (n=24)17M:7F
Allocated to High-MUFA (n=12)8M:4F
12 Completed9M:3F
12 Completed8M:4F
Allocated to Low-MUFA (n=12)9M:3F
Drop Out (n=1)1-drop out after 1 day on diet
Randomized (n=24)17M:7F
Completion Control (n=24)17M:7F
Allocated to High-MUFA (n=12)8M:4F
12 Completed9M:3F
12 Completed8M:4F
Allocated to Low-MUFA (n=12)9M:3F
Completion Control (n=24)17M:7F
Allocated to High-MUFA (n=12)8M:4F
12 Completed9M:3F
12 Completed8M:4F
Allocated to Low-MUFA (n=12)9M:3F
Allocated to High-MUFA (n=12)8M:4F
12 Completed9M:3F
12 Completed8M:4F
Allocated to Low-MUFA (n=12)9M:3F

38
Figure 2. Mean (SE) percentage change from baseline for both treatments for HDL-C,
high-density lipoprotein cholesterol (P=0.004); apoA1, apolipoprotein A1 (P=0.001);
total:HDL-C, total-cholesterol to high-density lipoprotein cholesterol ratio (P=0.045);
apoB:A1, apolipoprotein B to apolipoprotein A1 ratio (P=0.030) (significance of
difference between treatments) using the CONTRAST statement.
HDL-C
-35-30-25-20-15-10
-505
10
0 2 4 6 8
%C
hang
e B
asel
ine
Wk0
High-MUFA Low-MUFA
ApoA1
-35-30-25-20-15-10
-505
10
0 2 4 6 8Week
%C
hang
e B
asel
ine
Wk0
ApoB:A1 Ratio
-35-30-25-20-15-10
-505
10
0 2 4 6 8Week
%C
hang
e fro
m B
asel
ine
Wk0
Total:HDL-C Ratio
-35-30-25-20-15-10
-505
10
0 2 4 6 8
%C
hang
e fro
m B
asel
ine
Wk0

39
Figure 3. Mean (SE) percentage change from baseline for both treatments for total-C, total
cholesterol (P=0.517); LDL-C, low-density lipoprotein cholesterol (P=0.473); apoB,
apolipoprotein B (P=0.786); TG, triglyceride (P=0.538) (significance of difference between
treatments) using the CONTRAST statement.
Total-C
-40
-30
-20
-10
0
10
20
30
0 2 4 6 8
%C
hang
e fro
m B
asel
ine
Wk0 High-MUFA Low-MUFA
LDL-C
-40
-30
-20
-10
0
10
20
30
0 2 4 6 8Week
% C
hang
e fro
m B
asel
ine
Wk0
ApoB
-40
-30
-20
-10
0
10
20
30
0 2 4 6 8
TG
-40
-30
-20
-10
0
10
20
30
0 2 4 6 8Week

40
Mean ± SEM Range Mean ± SEM RangeAge (y) 55 ± 7 42 - 68 56 ± 11 38 - 69
Sex (female/male) 3/8 8/4
Weight (kg) 83 ± 4 62 - 113 80 ± 2 71 - 89
BMI (kg/m2) 29 ± 4 25 - 36 29 ± 2 26 - 32
Total-C (mmol/L) 6.3 ± 0.2 5.4 -7.7 6.2 ± 0.3 5.2 - 7.6
LDL-C (mmol/L) 4.3 ± 0.2 3.5 - 5.6 4.2 ± 0.2 3.3 - 5.2
HDL-C (mmol/L) 1.14 ± 0.08 0.73 - 1.66 1.22 ± 0.03 1.03 - 1.37
Triglycerides (mmol/L) 1.9 ± 0.2 1.0 - 3.5 1.6 ± 0.2 0.8 - 2.8
Systolic blood pressure (mmHg) 127 ± 3 109 - 142 121 ± 3 105 - 142
Diastlolic blood pressure (mmHg) 77 ± 3 57 - 91 74 ± 2 61 - 89
Exercise, METs 21.7 ± 5.2 1.5 - 55.0 23.2 ± 5.0 2.3 - 55.1
Medications, No. of subjects Blood Pressure 3 2 Thyroxine (0.08mg OD) 0 1 Aspirin 81mg 1 3 Supplements: Iron Supplementation (7mg TID) 7 9 Multivitamin 2 2 Calcium 3 5 Vitamin D 2 3 Glucosamine Chondritin 1 1Discontinued prior to study* Statins: n=3 n=3
Crestor 5mg 1Crestor 10mg 1 2Crestor 20mg 1Lipitor 20mg 1
Abbreviations: MUFA, monounsaturated fatty acid, BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; METs, metabolic equivalent of tasks (an index number expressing the energy cost of physical activities as multiples of Resting Metabolic Rate)SI conversion factors: To convert cholesterol and triglycerides to mg/dL, divide by 0.0259 and 0.0113, respectively.
† Data are expressed as mean±SE. No signficant baseline differences were observed between the high and low-MUFA groups.
Table 1. Baseline characteristics of randomized study participants.†High MUFA (n=12) Low MUFA (n=12)
* participants taking statins were asked to discontinue them 2 weeks prior to beginning the study

41
High MUFA Group(n=12)
Low MUFA Group (n=12)
Calories (kcal) 1882 1914Protein (%) 16.6 15.7Soy Protein (%) 0.0 0.6Available CH2O (%) 57.3 56.1Dietary Fiber (g/1000kcal) 18.6 17.5Viscous Fiber(g/1000kcal) 2.0 1.7Fat (%) 24.0 28.2SFA (%) 6.1 6.7MUFA (%) 9.6 11.5PUFA (%) 5.4 7.2Dietary Cholesterol (mg/1000kcal) 61.6 60.6Alcohol (%) 2.1 1.5
Table 2: Macronutrient Composition of the Participants' Habitual Diet* Habitual Diet:
Abbreviations: CH2O, carbohydrate; SFA, saturated fatty acid; MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid
*Data are expressed as mean percentage of calories per day unless otherwise noted.

42
Table 3: Macronutrient Composition of the Study Diets*NCEP Control Diet
(n=24)Low MUFA
Portfolio(n=12)
High MUFA Portfolio(n=12)
Calories (kcal) 2442a 2345a 2536a
Protein (%) 20.4a 21.7b 20.5a
Soy Protein (%) 0.0a 8.3b 7.7c
Available CH2O (%) 51.9a 49.1b 33.9c
Dietary Fiber (g/1000kcal) 20.1a 35.5b 32.7c
Viscous Fiber (g/1000kcal) 0.0a 11.0b 9.3c
Fat (%) 27.5a 29.3b 45.6c
SFA (%) 4.6a 4.7a 6.7b
MUFA (%) 10.6a 12.9b 25.9c
PUFA (%) 9.9a 11.0b 11.7b
Dietary Cholesterol (mg/1000kcal) 38.9a 29.9b 31.8c
Alcohol (%) 0.14a 0.00b 0.38c
Abbreviations: CH2O, carbohydrate; SFA, saturated fatty acid; MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid; NCEP Control Diet, National Cholesterol Education Program-based Control Diet
*Data are expressed as mean percentage of calories per day unless otherwise noted where different letters as superscripts on the same line indicate significant differences between treatments (P<0.05) as assessed by ANCOVA.

43
Table 4: Example Menuplan of Diets for 2000kcal
Control Diet High MUFA Diet Low MUFA Dietgrams grams
Breakfast: Cereal: Hot Cereal: Hot Cereal: Bran flakes cereal* 30 Oat bran 40 Oat bran 40 Skim milk 220 Unsweetened Soy Beverage 250 Soy Beverage 200Fruit&Yogurt: Strawberries 50 Strawberries 150 Strawberries 100 Drink: Sugar 3 Fat Free Yogurt* 175 Psyllium (+ water 250ml) 7 Drink: Strawberry Jam* 10 Toast:: Psyllium (+ water 250ml) 7
Bread, Oatbran 65 Toast: Strawberry Jam* 15 Oatbran bread 30 Study margarine (Plant sterol-enriched) 12 Strawberry Jam* 12 High-MUFA Sunflower Oil 13 Study margarine (Plant sterol-enriched) 65
Snack Pear 133 Almonds 15 Almonds 15 Skim milk 220 Pear 102 Pear 197
Lunch Soup: Soup: Soup: Pasta & Fagioli Soup* 270 Barley Vegetable Soup* 45 Barley Vegetable Soup* 45Sandwich: Sandwich: Sandwich: Whole wheat bread 90 Oatbran bread 65 Oatbran bread 65 Light Margarine 35 Study margarine (Plant sterol-enriched) 13 Study margarine (Plant sterol-enriched) 13 Fat Free Cheese 42 Soy Deli Slices* 62 Soy Deli Slices* 62Salad: Salad: Salad: Lettuce, Romaine 30 Lettuce, Romaine 30 Lettuce, Romaine 30 Cucumber 50 Cucumber 50 Cucumber 50 Tomato 100 Tomato 100 Tomato 100 Oil, Olive 11 Almonds (chopped) 12 Almonds (chopped) 12 Vinegar 10 High-MUFA Sunflower Oil 12
Snack Ancient Grain Crackers* 10 Almonds 15 Almonds 15 Orange 133 Apple 103 Orange 197
Unsweetened Soy Beverage 250 Soy Beverage 200
Dinner Entre: Soup or stew: Soup or stew: Cheese Cannelloni* 246 Low-Fat Extra-Firm Tofu* 120 Low-Fat Extra-Firm Tofu* 120Bake/grill: Okra 100 Okra 100 Safflower Oil 15 Cauliflower 100 Cauliflower 100 Cauliflower 150 Onions 30 Onions 30 Onions 30 Green pepper 50 Green pepper 50 Green pepper 50 Pearled barley 35 Pearled barley 35 Fat Free Cheese 42 High-MUFA Sunflower Oil 18 Sunflower Oil 6
Snack Skim milk 220 Unsweetened Soy Beverage 225 Soy Beverage 150 Apple 133 Psyllium (+ water 250ml) 7 Psyllium (+ water 250ml) 7
Apple 196*these products were Blue Menu line products (Loblaws, Toronto, Canada)

44
Control prior to HighMUFA (n=12) Control prior to LowMUFA (n=12)Week 0 Week 2&4 Difference (SE) Week 0 Week 2&4 Difference (SE) P-value£
Body Weight, kg 83.1 (4.1) 82.4 (4.1) - 0.7 (0.3)* 79.9 (1.8) 78.9 (1.7) - 1.0 (0.3)† 0.556Cholesterol, mmol/L
Total-C 6.33 (0.20) 5.48 (0.20) - 0.85 (0.13)‡ 6.19 (0.26) 5.39 (0.26) - 0.80 (0.13)‡ 0.802LDL-C 4.34 (0.20) 3.67 (0.17) - 0.67 (0.11)‡ 4.24 (0.22) 3.53 (0.15) - 0.71 (0.12)‡ 0.803HDL-C 1.14 (0.08) 1.00 (0.05) - 0.14 (0.10)† 1.22 (0.03) 1.08 (0.03) - 0.14 (0.03)† 0.889
Triglycerides 1.87 (0.21) 1.77 (0.12) - 0.10 (0.17) 1.60 (0.17) 1.71 (0.34) 0.11 (0.26) 0.505Apolipoproteins, g/L
ApoA1 1.43 (0.05) 1.28 (0.05) - 0.14 (0.03)‡ 1.49 (0.04) 1.34 (0.05) - 0.15 (0.04)† 0.943ApoB 1.23 (0.05) 1.10 (0.04) - 0.13 (0.02)‡ 1.17 (0.06) 1.05 (0.05) - 0.12 (0.02)‡ 0.754
RatiosTotal:HDL-C 5.84 (0.40) 5.63 (0.29) - 0.21 (0.17) 5.1 (0.24) 5.03 (0.26) - 0.07 (0.18) 0.592LDL:HDL-C 4.01 (0.31) 3.78 (0.23) - 0.23 (0.10)* 3.50 (0.21) 3.30 (0.15) - 0.20 (0.12) 0.863
ApoB:A1 0.88 (0.05) 0.87 (0.05) - 0.01 (0.01) 0.80 (0.05) 0.80 (0.04) 0.00 (0.02) 0.883hs-CRP, mg/L 1.17 (0.25) 1.62 (0.24) 0.44 (0.25) 1.58 (0.42) 1.76 (0.59) 0.18 (0.24) 0.460Blood Pressure, mm Hg
Systolic 126.6 (3.0) 120.5 (2.4) - 6.1 (2.2)* 121.3 (2.8) 120.2 (2.4) - 1.08 (1.9) 0.100Diastolic 76.6 (2.8) 73.6 (2.3) - 3.0 (1.5) 73.5 (2.0) 70.9 (1.7) - 2.6 (1.7) 0.838
Table 5. Effect of Control, very low saturated fat diet, on Blood Lipids, C-Reactive Protein, and Blood Pressure in High- vs. Low-MUFA Groups
Abbreviations: MUFA, monounsaturated fatty acid; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; ApoA1, apolipoprotein A1; ApoB, apolipoprotein B; hs-CRP, high-sensitivity C-reactive protein* significantly different from Week 0 at P<0.05, † at P<0.01, ‡ at P<0.001;£ difference between changes in high- versus low-MUFA groups using the CONTRAST statement
To convert total-C, LDL-C, and HDL-C to mg/dL, divide by 0.0259; for triglycerides to mg/dL, divide by 0.0113; for ApoA1 and B to mg/dL, multiply by 100.

45
Week 2&4 Week 6&8 Difference (SE) Week 2&4 Week 6&8 Difference (SE) P-value£
Body Weight, kg 82.4 (4.1) 81.6 (4.0) - 0.78 (0.21)† 78.8 (1.7) 77.9 (1.6) - 0.98 (0.25)† 0.485Cholesterol, mmol/L
Total 5.48 (0.20) 4.66 (0.09) - 0.82 (0.13)‡ 5.39 (0.26) 4.51 (0.26) - 0.87 (0.11)‡ 0.517LDL-C 3.67 (0.17) 2.89 (0.13) - 0.78 (0.11)‡ 3.53 (0.15) 2.76 (0.18) - 0.77 (0.14)‡ 0.473HDL-C 1.00 (0.05) 1.13 (0.07) 0.13 (0.03)† 1.08 (0.03) 1.11 (0.05) 0.03 (0.05) 0.004
Triglycerides 1.77 (0.12) 1.41 (0.09) - 0.36 (0.07)‡ 1.71 (0.34) 1.43 (0.16) - 0.28 (0.34) 0.538Apolipoproteins, g/L
A1 1.28 (0.05) 1.38 (0.06) 0.10 (0.03)† 1.34 (0.05) 1.33 (0.05) - 0.01 (0.02) 0.001B 1.10 (0.04) 0.90 (0.03) - 0.19 (0.03)‡ 1.05 (0.05) 0.87 (0.05) - 0.19 (0.03)‡ 0.786
RatiosTotal:HDL-C 5.63 (0.29) 4.21 (0.18) - 1.42 (0.17)‡ 5.03 (0.26) 4.12 (0.21) - 0.91 (0.22)‡ 0.045LDL:HDL-C 3.78 (0.23) 2.62 (0.14) - 1.16 (0.12)‡ 3.30 (0.15) 2.52 (0.16) - 0.78 (0.10)‡ 0.040
ApoB:A1 0.87 (0.05) 0.67 (0.03) - 0.21 (0.02)‡ 0.80 (0.04) 0.65 (0.03) - 0.14 (0.02)‡ 0.030hs-CRP, mg/L 1.62 (0.24) 0.82 (0.13) - 0.79 (0.21)† 1.77 (0.59) 1.85 (0.55) 0.22 (0.46) 0.011Blood Pressure, mm Hg
Systolic 120.6 (2.4) 119.6 (2.1) - 1.00 (2.52) 120.3 (2.4) 117.3 (2.4) - 2.96 (1.74) 0.265Diastolic 73.5 (2.3) 72.5 (2.2) - 0.96 (1.36) 71.0 (1.7) 70.1 (1.7) - 0.88 (1.51) 0.428
* significantly different from Week 2&4 at P<0.05, † at P<0.01, ‡ at P<0.001; £ difference between changes in high- versus low-MUFA groups using the CONTRAST statementTo convert total-C, LDL-C, and HDL-C to mg/dL, divide by 0.0259; for triglycerides to mg/dL, divide by 0.0113; for ApoA1 and B to mg/dL, multiply by 100.
Table 6. Effect of High-MUFA and Low-MUFA Dietary Portfolio Treatments on Blood Lipids, C-Reactive Protein, and Blood PressureLow MUFA Portfolio (n=12)High MUFA Portfolio (n=12)
Abbreviations: MUFA, monounsaturated fatty acid; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; ApoA1, apolipoprotein A1; ApoB, apolipoprotein B; hs-CRP, high-sensitivity C-reactive protein

46
5. The Effect on Oxidative Stress of Adding Monounsaturated Fat to a Dietary Portfolio of
Cholesterol-Lowering Foods

47
The Effect on Oxidative Stress of Adding Monounsaturated Fat to a Dietary Portfolio of Cholesterol-Lowering Foods
5.1 Abstract
Background: Higher monounsaturated fat (MUFA) intakes may reduce oxidative damage
and contribute to reduced cardiovascular disease (CVD) risk by decreased oxidative
damage.
Methods: Twenty-four hyperlipidemic subjects took a very low-saturated-fat therapeutic
control diet for one month and then either a high- or low-MUFA dietary portfolio for a
further month. Food was provided for the 2-month period based on Harris-Benedict
estimates for requirement. Oxidative stress was measured as serum protein thiols and
conjugated dienes (CD) and thiobarbituric acid reactive substances (TBARS) in the LDL
fraction.
Results: Although all treatments showed antioxidant activity, there were no significant
differences between the high- and low-MUFA dietary portfolios in any of the measures of
oxidative damage.. For the group as a whole (24 subjects), during the control diet there
were significant increases in protein thiols of 7.6 ± 3.1% (P=0.023) and significant
reductions in CD of 9.3 ± 3.0% (P=0.005) but non-significant reductions in TBARS of 8.5 ±
5.8% (P=0.154). During both the high- and low-MUFA dietary portfolios, protein thiols
increased significantly by 8.8 ± 3.7% (P=0.026) while CD and TBARS decreased
significantly by 9.6 ± 3.5% (P=0.012) and 8.5 ± 3.5% (P=0.021) respectively, indicating a
reduction in oxidative damage.
Conclusions: No effect of MUFA could be detected, although all diets showed antioxidant
activity.

48
5.2 INTRODUCTION
Evidence suggests that dyslipidemia and oxidative stress are key mechanisms
associated with the development of atherosclerosis and cardiovascular disease (CVD)
(282). Dyslipidemia has been closely associated with increased endothelial production
of reactive oxygen species (ROS) and the oxidative modification of low-density
lipoprotein (LDL)-associated lipids which is directly involved in the initiation of
atherosclerotic development (282). The dietary portfolio appears to reduce CVD risk
through reduction of both LDL-C and C-reactive Protein (CRP) (10, 11). Oxidized LDL
(ox-LDL), a further risk factor, may also be reduced because of the nature of the key
components of the dietary portfolio (12). Reductions in ox-LDL have been demonstrated
in studies involving soy protein or almonds (114, 115, 119, 120, 145, 146) and in some
studies on plant sterols and fibres, although the data are not as strong (165, 184, 185,
187). It was therefore of interest to determine whether the addition of monounsaturated
fatty acids (MUFAs) to the dietary portfolio provided a further benefit in terms of
antioxidant since MUFA consumption has been shown to reduce oxidative modification
of LDL (203, 240, 283).
We have therefore compared the effect on oxidative stress of substituting 13.0%
of total calories as MUFA for carbohydrate in an effective cholesterol-lowering dietary
portfolio.
5.3 METHODS
5.3.1 Participants
Men and post-menopausal women with mild to moderate hypercholesterolemia
were recruited and completed the study (17 men and 7 postmenopausal women). Their
mean ± SE age was 55 ± 9 years (range, 38-69 years) and mean body mass index
(BMI) was 28.8 ± 0.7 kg/m2 (range, 24.4-36.0 kg/m2) (refer to Table 1 in Chapter 4). All
participants had previously demonstrated high LDL-C levels >4.1 mmol/L (19, 242). No
participants had a history of cardiovascular disease, untreated hypertension (blood
pressure >140/90mmHg), diabetes, or renal or liver disease, and none were taking
medications known to influence serum lipids apart from 1 women taking stable doses of
thyroxine. Six participants were taking statins and had discontinued them as required at

49
least 2 weeks prior to the study (3 low-MUFA and 3 high-MUFA dietary portfolio
participants). All medications and supplements were expected to be taken at a constant
dose prior to and during the study. Five participants were taking antihypertensive
medications at a constant dose prior to and during the study and 4 were taking aspirin
or other anti-inflammatory drugs. Other, more commonly used non-prescription drugs
and supplements taken throughout the study period included a daily multivitamin (n = 4),
calcium (n = 8), glucosamine (n=2), melatonin (n=2) and vitamin D (n=5). Iron
supplementation (ferrous gluconate 7mg tid) was provided to 16 subjects on the basis of
a prestudy ferritin of <50mcg/L.
5.3.2 Study Protocol The study followed a randomized parallel design and was carried out between
August 2007 and April 2009. Participants followed their own low-saturated-fat
therapeutic diet for 1 month prior to the start of the study. They were then placed on a
very low-saturated-fat dairy and whole-grain cereal diet which acted as a stabilization
period prior to the high- and low-MUFA diets. After one month on this metabolically-
controlled diet, they were randomized to either a high-MUFA or conventional (low-
MUFA) dietary portfolio for a final month. All foods were provided except for fresh fruit
and vegetables which subjects were prescribed and instructed to obtain for themselves.
Throughout the study participants attended weekly clinic visits where body weight
was taken and blood pressure was measured three times in the non-dominant arm
using a mercury sphygmomanometer by the same observer. At 2-week intervals blood
samples were obtained after 12-hour overnight fasts. A seven-day diet history was
obtained for the week prior to the 2-month metabolic treatment period. Completed menu
checklists were returned at weekly intervals during the 4-week diet periods and checked
by the dietitians, who also recorded the participants’ previous week’s exercise and
ensured that it was constant over the course of the study period. At weekly intervals,
participants recorded their overall feeling of satiety using a 9 point bipolar semantic
scale in which −4 was extremely hungry, 0 was neutral, and +4 was uncomfortably
satiated.

50
The statistician stratified the participants on the basis of sex and an LDL-C of
4.2mmol/L in the first 2 weeks of the very low-saturated-fat therapeutic control diet using
a random number generator and SAS version 9.1 software (SAS Institute Inc, Cary, NC)
in a separate location from the clinic. The dietitians were not blinded to the diet because
they were responsible for patients’ diets and for checking diet records. The laboratory
staff responsible for analyses were blinded to treatment and received samples labelled
with name codes and dates. The study was approved by the ethics committees of the
University of Toronto and St. Michael’s Hospital and the Natural Health Products
Directorate of Health Canada. Written informed consent was obtained from all
participants. The clinical trial registration number is NCT00430430.
5.3.3 Diets
The diets eaten before the 8-week study were the participants’ routine
therapeutic low-fat diets, which were similar to current National Cholesterol Education
program guidelines (<7% energy from saturated fat and <200 mg/d of dietary
cholesterol) (19, 284) and previously referred to as a Step II diet (248). During the 8-
week study period, diets were provided based on estimated caloric requirements by the
Harris-Benedict equation and all diets were vegetarian. In the case of the high-MUFA
diet, 14.7% dietary calories as starch was replaced by MUFA in the dietary portfolio.
The aim of the dietary portfolio was the same as previous dietary portfolio studies (10,
198): to provide 1.0 g of plant sterols per 1000 kcal of diet in a plant sterol ester–
enriched margarine with a minimum of 2.0g and a maximum of 3.0g of plant sterols per
day; 10.3 g of viscous fibres per 1000 kcal of diet from oats, barley, and psyllium; 20 g
of soy protein per 1000 kcal as soy milk and soy meat analogs; and 21.5 g of whole
almonds per 1000 kcal of diet. Eggs (2/wk) were provided in the dietary portfolio to
balance the saturated fat and dietary cholesterol in the very low-saturated-fat
therapeutic control diet (refer to Table 4 in Chapter 4). The very low-saturated-fat
therapeutic control diet has been previously described (refer to Chapter 4). The
macronutrient profile of the diet recorded as consumed over the 4 weeks achieved a
saturated fat intake of <5% of total calories with <50mg cholesterol/1000kcal.

51
Participants were provided with self-tarring electronic scales (Tanita
Corporations, Arlington Heights, USA) and asked to weigh all food items consumed
prior to and during the study period. During the study period, all foods to be consumed
by participants were provided initially by courier and then at weekly clinic visits, with the
exception of fruit and low-calorie, non–starch-containing vegetables (8% and 24% of
dietary calories respectively from high- and low-MUFA diets). Okra was the exception
and was provided in the dietary portfolio. Participants were provided with 7-day rotating
menus (refer to Table 3 in Chapter 4).
Compliance was assessed from the completed weekly checklists and from the
return of uneaten food items.
5.3.4 Analyses Serum lipids were measured on samples stores at -70°C in the same batch
according to the Lipid Research Clinics protocol (254) for total-C, TG, and HDL-C after
dextran sulphate–magnesium chloride precipitation (285) and LDL-C was calculated
(255). Serum apolipoprotein A1 and B were measured by nephelometry (intra-assay
coefficient of variation, 2.2% and 1.9%, respectively) (256) and hs-CRP by end-point
nephelometry (coefficient of variation, 3.5%) (Behring BN-100, N high-sensitivity C-
reactive protein reagent, Dade- Behring, Mississauga, Ontario). All samples from a given individual were labelled by code and analyzed in the
same batch. Protein oxidation was measured using the 5,5′-dithiobis (2-nitrobenzoic
acid) assay (38) to assess the loss of reduced thiol (−SH) groups as a measure of
oxidation. The coefficient of variation of serum samples analyzed in triplicate was 3.0%.
LDL oxidation was estimated by measuring in the LDL fraction both CD, based on the
method of Ahotupa et al (39), and TBARS, using the malondialdehyde (MDA)–
thiobarbituric acid assay adopted from Jentzsch et al (40). The coefficients of variation
for these analyses were 5.7% and 6.4% for TBARS and CD, respectively.
Diets were analyzed using a program based on US Department of Agriculture
data and developed in our laboratory to allow addition of data on foods relevant to
ongoing studies after analysis in the laboratory for protein, total fat, and dietary fibre

52
using American Organization of Analytical Chemists methods and fatty acids by gas
chromatography (10).
5.3.5 Statistical Analysis Results were calculated as mean±SE. The significance of the differences
between the treatments for the oxidative markers were assessed using ANOVA in SAS
(258) with the change from baseline to week 4 for the very low-saturated-fat therapeutic
control diet and from week 4 to week 8 for the high- and low-MUFA dietary portfolios.
Treatment and sex and their interaction were main effects, with baseline as covariate. A
2-tailed paired t test was used to assess the significance of the within treatment (weeks
0 and 4) percentage change from baseline for the control and between week 0 versus
week 8 for the high- and low-MUFA dietary portfolio groups.
The original power calculation for the study was based on the ability to detect
changes in lipids and lipoproteins (refer to Chapter 4). In the present analysis, with the
observed SD of effect of 16.9% for TBARS and 12 subjects per group, we could be able
to detect a 20.2% difference in the primary measure (α=0.05, 1- β=0.8); for CD , with
the observed SD of effect of 17.6% for CD, we could be able to detect a 21.0%
difference in CD between the 2 treatments; and similarly for protein thiols, with the
observed SD of effect of 18.5%, we could be able to detect a 22.1% difference.
5.4 RESULTS 5.4.1 Participants
No significant differences were found in baseline data between the 2 groups,
both diets were similarly well complied with (>90%), there was no difference between
satiety ratings between the 2 groups, and participants lost a similar amount of weight on
all 3 one- month treatments (control, -1.10 ± 0.2kg; P<.001; high-MUFA dietary portfolio,
-0.78 ± 0.21kg; P=.003; low-MUFA dietary portfolio, -0.98 ± 0.26kg; P=.003).
5.4.2 Markers of Oxidation No differences were observed among the 2 treatment groups in baseline
oxidative measurements and no differences were seen between the high- and low-

53
MUFA diets. Increases in protein thiols and reductions in CD and TBARS were
observed throughout the study on both high- and low-MUFA diets (Tables 1 and 2). The
mean percentage change over the control month using the data for the 24 subjects for
protein thiols was 7.6 ± 3.1% (P=0.023) and for CD and TBARS was 9.3 ± 3.0%
(P=0.005) and 8.5 ± 5.8% (P=0.154), respectively. For the 24 subjects during the
portfolio diets, protein thiols further increased significantly by 8.8 ± 3.7% (P=0.026)
while CD and TBARS further decreased significantly by 9.6 ± 3.5% (P=0.012) and 8.5 ±
3.5% (P=0.021) respectively, indicating a reduction in oxidative damage (Figure 1). In
post-hoc analyses, there were no differences in oxidative measures between subjects
when they were divided into those receiving iron supplementation or those who lost
weight (data not shown).
5.4.3 Drop out and Adverse Events
No participant withdrew from the study after the randomization which occurred
during the first and second week of the control phase. One participant withdrew at the
time of the first control breakfast due to the perceived inconvenience of a metabolically
controlled diet. No adverse events were reported.
5.5 DISCUSSION This study demonstrated that replacement of 13.0% carbohydrate by MUFA
resulted in no differences between treatments for the oxidative markers protein thiols,
CD or TBARS. However, the antioxidant activity of the very low-saturated-fat
therapeutic control diet and both the high- and low-MUFA dietary portfolios were
reflected in the progressive increase in protein thiols and reduction in conjugated dienes
and TBARS and therefore present a potential reduction in LDL atherogenicity (22, 30,
31).
In the present study, the very low-saturated-fat control diet can be seen as a
positive control since low-fat dairy diets emphasizing fruits and vegetables, such as in
the Dietary Approaches to Stop Hypertension (DASH) trial, have previously
demonstrated reductions in markers of oxidation, as well as improved serum lipid
profiles (50). The continued improvement in the oxidative measures during the second

54
month of the study in which the subjects were consuming the dietary portfolio is
anticipated since many of the key components, including plant sterols, soy protein,
viscous fibres and almonds, have previously demonstrated the potential to reduce
oxidative stress such as reductions in ox-LDL (119, 145, 146, 183, 185), thus
suggesting the potential to protect LDL from oxidative damage (147, 148). Additionally,
almonds have demonstrated increases in total antioxidant capacity (120) and their skins
have shown antioxidant activity against free radicals in humans (121, 122) while whole
grains have been associated with reductions in risk of inflammatory diseases (166).
Therefore the dietary portfolio contains a variety of foods which may explain the
observed reduction in oxidative markers.
Although studies adding MUFA to a diet have demonstrated a reduction in
oxidative damage, such as reductions in the oxidative modification of LDL particles
(203), no difference between the high- and low-MUFA treatments were observed in the
present study. However, in the low-MUFA diet, MUFA was replaced by carbohydrates
which came from fruits, which resulted in a diet containing around 24% of its dietary
calories from fruit and vegetable as opposed to the 8% in the high-MUFA diet.
Therefore, since MUFA was replaced by fruits which are known to be rich in
antioxidants, it may be that there was no significant difference between the high- and
low-MUFA diets because both diets were rich in antioxidant foods of a different nature.
For example, some studies have demonstrated an approximate 10-15% reduction in
CDs on a high-MUFA versus low-MUFA diet over 1 month, (203, 286), while the DASH
(Dietary Approaches to Stop Hypertension) diet which contained about 16% of calories
from fruits and vegetables demonstrated a 10% reduction in urinary isoprostanes, a
marker of oxidative damage. Therefore, whether from increased MUFA or from a diet
rich in fruits and vegetables, there were similar reductions in markers of oxidative
damage. These reductions are similar to those observed in the present study where
there were reductions of 8.5% in CDs on the DASH-like control diet and another 10%
during the high-MUFA dietary portfolio. The further 10% reduction in CDs on the low-
MUFA dietary portfolio may be the result of the added fruit as well as the dietary
portfolio components.

55
Additionally, due to the inclusion of multiple foods with antioxidant potential
including a healthy DASH-like control diet, MUFAs, and fruit and vegetables, a
possible reason as to why no additional improvement in oxidative markers resulted from
the high-MUFA treatment is that the dietary benefit may have already been maximal
since some ability to mount an oxidative response is required for normal functioning
including defence by white cells from invading bacteria (287).
However, it is also possible that we did not see treatment differences in the
oxidative measures because of the relatively small sample size of 12.
The present study demonstrates that therapeutic diets rich in fruit, vegetables, soy,
nuts and other antioxidant components result in a reduction in oxidative damage. No
treatment difference was seen when MUFA was included in the diet possibly due to the
displacement of other antioxidant dietary components. Furthermore, because of the
high level of natural antioxidants, no effect of iron status was observed in this relatively
small group of subjects. More extreme situations in which there is a lack of antioxidant
activity provided by the control diet may have to be employed to demonstrate the effect
of dietary antioxidants.

56
Protein Thiols by Treatment
200
250
300
350
400
450
500
550
-2 0 2 4 6 8
Week
Prot
ein
Thio
ls (u
M)
Absolute CD by Treatment
20
30
40
50
60
70
80
90
100
-2 0 2 4 6 8
Week
Abso
lute
Con
juga
ted
Dien
es (u
M)
Absolute TBARS by Treatment
0.0
0.5
1.0
1.5
2.0
-2 0 2 4 6 8
Week
Abso
lute
TBA
RS (u
M)
Figure 1. Means of oxidative stress on high [n=12, ] and low [n=12, ] MUFA diets. 1 outlier was removed from the high-MUFA group in the analysis of CD (127.2, 102.3, 125.0 at Week 0, 4, 8, resp.). 1 outlier was removed from the low-MUFA group in the analysis of protein thiols (200.4 at week 8) and of CD (95.6 at week 8) and another outlier in the analysis of TBARS (2.7, 1.5, 1.4 at week 0, 4, 8, resp.).

57
High vs. Low Group
Week 0 Week 4 Difference (SE) Week 0 Week 4 Difference (SE) P-value
Protein Thiols (mmol/L) 328 ± 21 347 ± 20 20 ± 12 342 ± 15 369 ± 24 27 ± 16 0.261
Conjugated Dienes
Absolute Concentration (umol) 65 ± 6 60 ± 6.4 - 5 ± 3 66 ± 7 57 ± 6 - 8 ± 3* 0.499
Molar ratio of LDL-C (umol/mmol) 15.0 ± 1.5 16.0 ± 1.7 1.0 ± 0.8 14.3 ± 1.2 14.7 ± 1.0 0.4 ± 0.5 0.514
TBARS
Absolute Concentration (umol) 1.28 ± 0.15 1.03 ± 0.07 - 0.25 ± 0.10* 1.16 ± 0.11 1.05 ± 0.09 - 0.11 ± 0.08 0.284
Molar ratio of LDL-C (umol/mmol) 0.29 ± 0.04 0.27 ± 0.02 - 0.02 ± 0.02 0.26 ± 0.02 0.28 ± 0.03 0.02 ± 003 0.330
* significantly different from Week 0 (P<.05)
Table 1. Effect of Control, very low-saturated-fat diet, on Oxidative Markers in High vs. Low Groups
Control-High-MUFA (n=12)Control-Low-MUFA (n=12)
High vs. Low
Week 4 Week 8 Difference (SE) Week 4 Week 8 Difference (SE) P-value
Oxidative Markers:
Protein Thiols (mmol/L) 347 ± 20 376 ± 23 29 ± 15 369 ± 24 391 ± 18 22 ± 21 0.555
Conjugated Dienes
Absolute Concentration (umol) 60 ± 6 53 ± 5 - 7 ± 4 57.± 6 52 ± 7 - 5 ± 4 0.669
Molar ratio of LDL-C (umol/mmol) 16.0 ± 1.7 17.5 ± 1.6 1.6 ± 1.0 14.7 ± 1.0 17.0 ± 1.9 2.3 ± 1.2 0.651
TBARS
Absolute Concentration (umol) 1.03 ± 0.07 0.96 ± 0.06 - 0.07 ± 0.05 1.05 ± 0.09 0.89 ± 0.05 - 0.16 ± 0.06* 0.221
Molar ratio of LDL-C (umol/mmol) 0.27 ± 0.02 0.32 ± 0.02 0.05 ± 0.02* 0.28 ± 0.03 0.30 ± 0.03 0.02 ± 0.01 0.254
* significantly different from Week 4 (P<.05)
Table 2. Effect of Low-MUFA and High-MUFA Dietary Portfolio Treatments on Oxidative Markers
Low MUFA Portfolio (n=12) High MUFA Portfolio (n=12)

58
6. Overall Discussion and Limitations

59
6.1 Overall Discussion Dietary modification has been shown to reduce risk of CVD (19, 269) which
explains the continuous search for better dietary strategies to target multiple risk factors.
Just as 4 foods that had been individually shown to reduce cholesterol demonstrated an
additive effect when combined to form the dietary portfolio, MUFA was added in an effort
to further reduce the overall risk for CVD. As recent studies demonstrate, there is a
residual risk that remains after effective LDL-C reduction. Therefore, strategies to target
this residual risk are of great interest.
In this study, the high-MUFA treatment was able to effectively raise HDL-C
significantly more than the low-MUFA treatment. This is an important result since studies
indicate that there is a 1-3% associated reduction in risk of CVD for every 0.026mmol/L
increase in HDL-C (53-55, 57). Additionally, the lipid results of the high-MUFA treatment
demonstrate that not only is HDL-C being improved, but also apoA1 levels, which may
be an important indication of the quality of HDL since apoA1 has important roles
associated with HDL-C. For example, in RCT apoA1 is the ligand for the ABC (ATP-
binding cassette) transporter, and therefore is the docking point for which HDL can
receive cholesterol from peripheral cells and transport it to the liver (96). It is also the
cofactor for LCAT (lecithin cholesterol acyltransferase) which is important in removing
cholesterol from tissues and transporting them via HDL to the liver (96). Also, this study
demonstrates that in addition to the significant reduction in LDL-C, one of the possible
factors contributing to residual CVD risk, HDL-C, was also improved thereby potentially
providing further CVD risk reduction, especially for those who ~20% of people who attain
low LDL-C but who may still experience a cardiovascular event (53, 288).
The significant increase in HDL-C is also an important finding of the study
because it provides strong support for the idea that MUFA consumption can raise HDL-
C, which has been largely debated. The present study provides strong evidence because
of the following: it included a 4-week metabolically controlled run-in period (the low-
saturated-fat control diet) which acted as a stabilization period for all subjects prior to the
randomization to high- or low-MUFA portfolio diets; it was very well controlled, with all
foods provided to the participants’ homes, as well as reimbursement for any items
purchased for the study diet, there were weekly clinic visits for counselling with

60
suggestions for new recipes and ideas on how to combine foods for each participants’
personal preferences, as well as to assist in any difficulties encountered; and it provided
a moderate but significant amount of MUFA in the form of an enriched sunflower oil
which could easily be consumed in daily food preparation. Therefore, it allowed for all
subjects to attain comparable baseline values as a result of the stabilization period,
provided the tools for successful adherence to the diets, and achieved a significant
difference between treatments making them suitable for comparison.
The significant HDL-C increase on the high-MUFA diet is also promising because
the other methods of raising HDL-C, such as through the use of fibrates or niacin
therapy, have negative side effects making them undesirable. Niacin has been
associated with flushing, dry skin, and gastrointestinal irritation, as well as increased risk
of hepatotoxicity when taken as a monotherapy (17). Fibrates are less effective
compared to niacin therapy in raising HDL-C, and may also increase serum creatinine
and homocysteine levels and thus require close patient follow-up (17). Therefore, the
results of this study are very appealing because the high-MUFA was able to raise HDL-C
to a comparable level to that of the mentioned pharmacotherapies, allowing for a
convenient and effective substitution in the diet without the undesired side effects.
The other beneficial observation in the present study which may provide further
CVD risk reduction was the significant reduction in hs-CRP in the high-MUFA group
compared to the low-MUFA group. Thus, added benefit may arise from the anti-
inflammatory properties of HDL, or the result of apoA1 since evidence exists that the
interaction between apoA1 and the ABC transporter can act as an anti-inflammatory
receptor in a separate pathway from that in RCT (289). CRP is receiving greater
attention due to the recently published JUPITER trial which demonstrated the lowest
cardiovascular event rate was achieved in subjects with an LDL-C level less than
2.0mmol/L and an hs-CRP level less than 2.0mg/L (290). As a result of this trial, hs-CRP
has been incorporated into recommended clinical guidelines, such as in the Canadian
Cardiovascular Society Guidelines in which it is stated that in intermediate-risk groups
with LDL-C levels which do not require treatment, hs-CRP is part of risk stratification in
addition to its inclusion as a secondary target (18). Additionally, the total-HDL-C ratio is
in the guidelines as a secondary target and is included as a specific therapy target in

61
those classified as intermediate risk (18). Many studies have also concluded that it is one
of the best predictors of long-term risk (17, 18, 291, 292). In the present study, both hs-
CRP and total:HDL-C ratio were significantly reduced in the high-MUFA group, thus
there is the potential for MUFA to assist in improving these targets for CVD risk
reduction. Some more recent studies suggest that the apoB:A1 ratio may be a better
predictor of CVD risk than total:HDL-C ratio, however in the present study, the apoB:A1
ratio was also significantly reduced on the high-MUFA diet versus the low-MUFA diet,
therefore the same dietary interventions would be appropriate to help reduce risk via this
alternative ratio predictor (81).
Since LDL-C has a well established direct relationship with the development of
atherosclerosis and its oxidation appears to accelerate this process, strategies to reduce
oxidative stress are recognized as important (22, 30). Although no treatment differences
were observed in markers of oxidative stress, the diets as a whole were antioxidant and
may assist in CVD risk reduction. Firstly, both dietary portfolios reduced LDL-C by 20-
22%, which was preceded by a 15.5% reduction on the stabilization control diet,
therefore reducing the substrate itself in the atherosclerotic development process. Over
the 2 month period, LDL-C was reduced by about 1.5mmol/L in both treatment groups
which when applied to previously established and well recognized findings that
1.0mmol/L reduction in LDL-C is associated with a 21% reduction in CVD risk (20), these
diets would be associated with a 31.5% reduction in risk of CVD. Secondly, irrespective
of MUFA intake, there was a significant increase in protein thiols and significant
reductions in CD and TBARS, which overall indicate reductions in oxidative damage both
to proteins and lipids. Therefore, diets which are rich in whole grains and low-fat dairy, as
in the control diet, may reduce oxidative damage and diets which also contain soy, nuts,
and are rich in fruits and vegetables or MUFAs, as in the dietary portfolio treatments,
may provide further reductions. Although there is controversy over the effects of
antioxidants on oxidative damage, the majority of studies are looking at supplementation
in which case you may not get the appropriate diversity of antioxidants required to
observe expected benefits. In the present study, the control diet provided reductions due
to a few foods with some potential effects which was followed by greater reductions seen
on the dietary portfolio containing additional foods with potential benefit in addition to

62
either more fruit or high MUFAs. Thus, by providing an increment in variety of foods with
antioxidant potential, the study was able to demonstrate continuous reductions in
oxidative damage. Therefore, by using whole foods, there is a wider variety of
components which may act together to elicit effects on oxidative damage and thus may
contribute to reduction in CVD risk (293).
Overall, through the combination of foods which lower cholesterol and oxidative
damage, including the use of MUFAs, there is potential for greater reductions in CVD
risk.
6.2 Limitations and Future Directions In considering the limitations of the study, the prescriptive nature of the diet must
be addressed since the subjects received all their foods by courier and were given
menuplans indicating all foods to be eaten and at what amounts. The dietary portfolio
has been observed under real-world conditions with an adherence rate of 64% at 1-year.
However, with the suggested inclusion of MUFA, MUFA must be encouraged not to
displace the portfolio components but to replace other sources of fat in the diet and not to
be incorporated as an addition to the existing diet, which could easily result in weight
gain.
Another limitation was the weight loss which occurred throughout the duration of
the study period, as well as the relatively small sample size (n=24). The weight loss may
have been the result of the use of the Harris-Benedict predictive equation for energy
requirement which had quite a large activity factor that the present group of subjects
generally fell just under, so may not have been prescribed amounts that accounted for
their exercises. Also, they may not have actually been consuming the entire amount
prescribed because of remaining amounts in the cooking pans, in transferring, or leftover
on their plates. However, weight loss was consistent throughout the study and similar
among both diet groups and did not influence any study outcomes when included as a
covariate in the statistical model. In terms of our sample size, although small, we had
enough power to detect the effect size in apoA1 as significant in favour of MUFA
(α=0.05).

63
We may have been unable to detect differences in the oxidative markers between
the high- and low-MUFA groups because the nature of the foods which MUFA replaced
have been shown to have antioxidant activity, that is, fruit. Ideally, to be able to observe
the true effects of MUFA on oxidative damage, the reference or control diet would have
had little to no antioxidant effect. However, we wanted to compare the effect of adding
MUFA to a dietary portfolio, which already contains potential antioxidant activity in its
components. Also, in order to keep all the portfolio components at their prescribed levels,
the only carbohydrate source which would be available for replacement was that from
fruit. Therefore the reference diet, low-MUFA, was rich in foods also capable of
antioxidant activity, albeit with an unknown comparability to the activity of MUFAs.
6.3 Future Research Since there was no difference between the high- and low-MUFA dietary portfolios
in the reduction in oxidative damage demonstrated in this study, it would be interesting to
test other measures of oxidative damage given that similar studies have found
differences although the carbohydrates replaced in those studies contained more simple
sugars and low- fat dairy (203). This could include other measures of lipid oxidation, such
as isoprostanes, and protein oxidation, such as protein carbonyls, as well as measures
of oxidative damage to DNA, such as 8-hydroxydeoxyguanosine (8-OHdG) (294). It may
also be interesting to test if the samples from the high-MUFA groups had greater
antioxidant activity by such tests as the radical absorbance capacity (ORAC). For a more
direct measure of HDL-C antioxidant activity, levels of PON-1 could be measured, since
PON1 is the HDL enzyme component which some studies have reported to be
responsible for the antioxidative activity of HDL (13, 74, 75). Additionally, a larger sample
size in future studies will allow for greater power to detect differences in oxidative
markers, as well as the selection of a reference treatment in which MUFA would replace
carbohydrate sources without antioxidant activity in order to detect of the activity of
MUFAs.
HDL-C has also been recognized for its antithrombotic activities and studies done
with recombinant HDL-C or apoA1 have demonstrated regression of plaques and
improvements in atherosclerosis. Therefore, it would be interesting to conduct a larger

64
trial to try to raise HDL-C and apoA1 in subjects, for example with acute coronary
syndrome, and to include such measurements as intravascular ultrasound (IVUS) as a
measure of atheroma volume for which administration of recombinant apoA1Milano has
demonstrated significant improvement (88). This would allow for detection of quality of
HDL-C and functionality of apoA1 to see if raised apoA1 can reach the effectiveness
seen in the mutated version, apoA1Milano. Other groups with low levels of HDL-C, such as
in diabetes or the metabolic syndrome, both of which are also accompanied by
elevations in triglyceride, would be potentially interesting groups to observe effects
because of their increased risk of CVD (295).

65
7. Summary

66
7. Summary In carrying out this thesis the aim was to answer the objectives. We have
demonstrated the following:
1. HDL-C and apoA1 were significantly increased on the high-MUFA versus the
low-MUFA dietary portfolio without compromising the lipid-lowering effectiveness
of the diet.
2. Although there was no treatment difference between the high- and low-MUFA
dietary portfolio groups, in the subject group as a whole, there was a significant
increase in protein thiols and reductions in both CD and TBARS in the LDL
fraction, indicating reduced oxidative damage to serum proteins and lipids.
3. Both dietary portfolio treatments significantly reduced LDL-C and apoB
irrespective of MUFA intake.
4. Total:HDL-C ratio, as well as apoB:A1 ratio were significantly reduced on the
high-MUFA versus the low-MUFA dietary portfolio.

67
8. References 1. Research CIoH. Research About - Cardiovascular Health. Canadian Institutes of
Health Research, 2009:www.cihr-irsc.gc.ca. 2. National Heart L, and Blood Institute. Information for Health Professionals.
National Heart, Lung, and Blood Institute:www.nhlbi.nih.gov/health/prof/heart/. 3. Association AH. Eat a Heart-Healthy diet. American Heart
Association:www.americanheart.org/presenter.jtml?identifier=1510. 4. Ontario HaSFo. The Basci Principles of Healthy Eating. 2009. 5. Association AH. Diet and Lifestyle Recommendations.
2009:http://www.americanheart.org. 6. Statistics. Heart and Stroke Foundation of Ontario,
2009:www.heartandstroke.on.ca. 7. National Heart L, and Blood Institute. Third Report of the National Cholesterol
Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. 2002.
8. Jenkins DJ, Kendall CW, Marchie A, et al. The effect of combining plant sterols, soy protein, viscous fibres, and almonds in treating hypercholesterolemia. Metabolism 2003;52:1478-83.
9. Willcox BJ, Curb JD, Rodriguez BL. Antioxidants in cardiovascular health and disease: key lessons from epidemiologic studies. Am J Cardiol 2008;101:75D-86D.
10. Jenkins DJ, Kendall CW, Marchie A, et al. Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-reactive protein. JAMA 2003;290:502-10.
11. Jenkins DJ, Kendall CW, Marchie A, et al. Direct comparison of dietary portfolio vs statin on C-reactive protein. Eur J Clin Nutr 2005;59:851-60.
12. Jenkins DJ, Nguyen TH, Kendall CW, et al. The effect of strawberries in a cholesterol-lowering dietary portfolio. Metabolism 2008;57:1636-44.
13. Bhattacharyya T, Nicholls SJ, Topol EJ, et al. Relationship of paraoxonase 1 (PON1) gene polymorphisms and functional activity with systemic oxidative stress and cardiovascular risk. JAMA 2008;299:1265-76.
14. Mackness MI, Arrol S, Durrington PN. Paraoxonase prevents accumulation of lipoperoxides in low-density lipoprotein. FEBS Lett 1991;286:152-4.
15. Ansell BJ, Watson KE, Fogelman AM, Navab M, Fonarow GC. High-density lipoprotein function recent advances. J Am Coll Cardiol 2005;46:1792-8.
16. Hausenloy DJ, Yellon DM. Targeting residual cardiovascular risk: raising high-density lipoprotein cholesterol levels. Postgrad Med J 2008;84:590-8.
17. McPherson R, Frohlich J, Fodor G, Genest J, Canadian Cardiovascular S. Canadian Cardiovascular Society position statement--recommendations for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease. Can J Cardiol 2006;22:913-27.
18. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and

68
prevention of cardiovascular disease in the adult - 2009 recommendations. Can J Cardiol 2009;25:567-79.
19. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001;285:2486-97.
20. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267-78.
21. The Lipid Research Clinics Coronary Primary Prevention Trial results. II. The relationship of reduction in incidence of coronary heart disease to cholesterol lowering. JAMA 1984;251:365-74.
22. Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL. Beyond cholesterol. Modifications of low-density lipoprotein that increase its atherogenicity. N Engl J Med 1989;320:915-24.
23. Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med 1997;336:1117-24.
24. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346:393-403.
25. Thomas D, Elliott EJ. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus. Cochrane Database Syst Rev 2009:CD006296.
26. Betteridge DJ. What is oxidative stress? Metabolism 2000;49:3-8. 27. Thompson LU, Yoon JH, Jenkins DJ, Wolever TM, Jenkins AL. Relationship
between polyphenol intake and blood glucose response of normal and diabetic individuals. Am J Clin Nutr 1984;39:745-51.
28. Klebanoff SJ, Locksley RM, Jong EC, Rosen H. Oxidative response of phagocytes to parasite invasion. Ciba Found Symp 1983;99:92-112.
29. Willcox JK, Ash SL, Catignani GL. Antioxidants and prevention of chronic disease. Crit Rev Food Sci Nutr 2004;44:275-95.
30. Witztum JL. The oxidation hypothesis of atherosclerosis. Lancet 1994;344:793-5. 31. Stocker R, Keaney JF, Jr. New insights on oxidative stress in the artery wall. J
Thromb Haemost 2005;3:1825-34. 32. Albertini R, Moratti R, De Luca G. Oxidation of low-density lipoprotein in
atherosclerosis from basic biochemistry to clinical studies. Curr Mol Med 2002;2:579-92.
33. Singh U, Devaraj S, Jialal I. Vitamin E, oxidative stress, and inflammation. Annu Rev Nutr 2005;25:151-74.
34. Rao AV, Agarwal S. Effect of diet and smoking on serum lycopene and lipid peroxidation. Nutrtion Research 1998;18:713-721.
35. Rao AV, Shen H. Effect of low dose lycopene intake on lycopene bioavailability and oxidative stress. Nutrition Research 2002;22:1125-1131.
36. de Zwart LL, Meerman JH, Commandeur JN, Vermeulen NP. Biomarkers of free radical damage applications in experimental animals and in humans. Free Radic Biol Med 1999;26:202-26.

69
37. Piconi L, Quagliaro L, Da Ros R, et al. Intermittent high glucose enhances ICAM-1, VCAM-1, E-selectin and interleukin-6 expression in human umbilical endothelial cells in culture: the role of poly(ADP-ribose) polymerase. J Thromb Haemost 2004;2:1453-9.
38. Hu ML. Measurement of protein thiol groups and glutathione in plasma. Methods Enzymol 1994;233:380-5.
39. Ahotupa M, Ruutu M, Mantyla E. Simple methods of quantifying oxidation products and antioxidant potential of low density lipoproteins. Clin Biochem 1996;29:139-44.
40. Jentzsch AM, Bachmann H, Furst P, Biesalski HK. Improved analysis of malondialdehyde in human body fluids. Free Radic Biol Med 1996;20:251-6.
41. Elwakkad AS, Mohamed SI, Fathalla M. Relation between hypercholesterolaemia and vascular endothelial microinflammation. East Mediterr Health J 2007;13:515-21.
42. Sies H, Stahl W, Sevanian A. Nutritional, dietary and postprandial oxidative stress. J Nutr 2005;135:969-72.
43. Actis-Goretta L, Carrasquedo F, Fraga CG. The regular supplementation with an antioxidant mixture decreases oxidative stress in healthy humans. Gender effect. Clin Chim Acta 2004;349:97-103.
44. Takamatsu S, Takamatsu M, Satoh K, et al. Effects on health of dietary supplementation with 100 mg d-alpha-tocopheryl acetate, daily for 6 years. J Int Med Res 1995;23:342-57.
45. van Tits LJ, de Waart F, Hak-Lemmers HL, et al. Effects of alpha-tocopherol on superoxide production and plasma intercellular adhesion molecule-1 and antibodies to oxidized LDL in chronic smokers. Free Radic Biol Med 2001;30:1122-9.
46. Reaven PD, Herold DA, Barnett J, Edelman S. Effects of Vitamin E on susceptibility of low-density lipoprotein and low-density lipoprotein subfractions to oxidation and on protein glycation in NIDDM. Diabetes Care 1995;18:807-16.
47. MRC/BHF Heart Protection Study of antioxidant vitamin supplementation in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:23-33.
48. Omenn GS, Goodman GE, Thornquist MD, et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med 1996;334:1150-5.
49. Lonn E, Bosch J, Yusuf S, et al. Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial. JAMA 2005;293:1338-47.
50. Miller ER, 3rd, Erlinger TP, Sacks FM, et al. A dietary pattern that lowers oxidative stress increases antibodies to oxidized LDL: results from a randomized controlled feeding study. Atherosclerosis 2005;183:175-82.
51. Miller ER, 3rd, Appel LJ, Risby TH. Effect of dietary patterns on measures of lipid peroxidation: results from a randomized clinical trial. Circulation 1998;98:2390-5.
52. Garcia-Closas R, Berenguer A, Jose Tormo M, et al. Dietary sources of vitamin C, vitamin E and specific carotenoids in Spain. Br J Nutr 2004;91:1005-11.

70
53. Alagona P, Jr. Beyond LDL cholesterol: the role of elevated triglycerides and low HDL cholesterol in residual CVD risk remaining after statin therapy. Am J Manag Care 2009;15:S65-73.
54. Castelli WP. Cholesterol and lipids in the risk of coronary artery disease--the Framingham Heart Study. Can J Cardiol 1988;4 Suppl A:5A-10A.
55. Castelli WP, Garrison RJ, Wilson PW, Abbott RD, Kalousdian S, Kannel WB. Incidence of coronary heart disease and lipoprotein cholesterol levels. The Framingham Study. JAMA 1986;256:2835-8.
56. Goldbourt U, Yaari S, Medalie JH. Isolated low HDL cholesterol as a risk factor for coronary heart disease mortality. A 21-year follow-up of 8000 men. Arterioscler Thromb Vasc Biol 1997;17:107-13.
57. Miller NE, Thelle DS, Forde OH, Mjos OD. The Tromso heart-study. High-density lipoprotein and coronary heart-disease: a prospective case-control study. Lancet 1977;1:965-8.
58. Stampfer MJ, Sacks FM, Salvini S, Willett WC, Hennekens CH. A prospective study of cholesterol, apolipoproteins, and the risk of myocardial infarction. N Engl J Med 1991;325:373-81.
59. Shai I, Rimm EB, Hankinson SE, et al. Multivariate assessment of lipid parameters as predictors of coronary heart disease among postmenopausal women: potential implications for clinical guidelines. Circulation 2004;110:2824-30.
60. Willeit J, Kiechl S, Oberhollenzer F, et al. Distinct risk profiles of early and advanced atherosclerosis: prospective results from the Bruneck Study. Arterioscler Thromb Vasc Biol 2000;20:529-37.
61. Austin MA. Plasma triglyceride and coronary heart disease. Arterioscler Thromb 1991;11:2-14.
62. von Eckardstein A, Nofer JR, Assmann G. High density lipoproteins and arteriosclerosis. Role of cholesterol efflux and reverse cholesterol transport. Arterioscler Thromb Vasc Biol 2001;21:13-27.
63. Mineo C, Deguchi H, Griffin JH, Shaul PW. Endothelial and antithrombotic actions of HDL. Circ Res 2006;98:1352-64.
64. Seetharam D, Mineo C, Gormley AK, et al. High-density lipoprotein promotes endothelial cell migration and reendothelialization via scavenger receptor-B type I. Circ Res 2006;98:63-72.
65. Barter PJ, Nicholls S, Rye KA, Anantharamaiah GM, Navab M, Fogelman AM. Antiinflammatory properties of HDL. Circ Res 2004;95:764-72.
66. Assmann G, Gotto AM, Jr. HDL cholesterol and protective factors in atherosclerosis. Circulation 2004;109:III8-14.
67. Klimov AN, Gurevich VS, Nikiforova AA, et al. Antioxidative activity of high density lipoproteins in vivo. Atherosclerosis 1993;100:13-8.
68. Ng CJ, Shih DM, Hama SY, Villa N, Navab M, Reddy ST. The paraoxonase gene family and atherosclerosis. Free Radic Biol Med 2005;38:153-63.
69. Ninio E. Phospholipid mediators in the vessel wall: involvement in atherosclerosis. Curr Opin Clin Nutr Metab Care 2005;8:123-31.

71
70. Mackness MI, Arrol S, Abbott C, Durrington PN. Protection of low-density lipoprotein against oxidative modification by high-density lipoprotein associated paraoxonase. Atherosclerosis 1993;104:129-35.
71. Watson AD, Berliner JA, Hama SY, et al. Protective effect of high density lipoprotein associated paraoxonase. Inhibition of the biological activity of minimally oxidized low density lipoprotein. J Clin Invest 1995;96:2882-91.
72. Aviram M, Rosenblat M, Bisgaier CL, Newton RS, Primo-Parmo SL, La Du BN. Paraoxonase inhibits high-density lipoprotein oxidation and preserves its functions. A possible peroxidative role for paraoxonase. J Clin Invest 1998;101:1581-90.
73. Mackness M, Mackness B. Paraoxonase 1 and atherosclerosis: is the gene or the protein more important? Free Radic Biol Med 2004;37:1317-23.
74. Li HL, Liu DP, Liang CC. Paraoxonase gene polymorphisms, oxidative stress, and diseases. J Mol Med 2003;81:766-79.
75. Durrington PN, Mackness B, Mackness MI. Paraoxonase and atherosclerosis. Arterioscler Thromb Vasc Biol 2001;21:473-80.
76. Wardlow ML, Cox CP, Meng KE, Greene DE, Farr RS. Substrate specificity and partial characterization of the PAF-acylhydrolase in human serum that rapidly inactivates platelet-activating factor. J Immunol 1986;136:3441-6.
77. Stremler KE, Stafforini DM, Prescott SM, McIntyre TM. Human plasma platelet-activating factor acetylhydrolase. Oxidatively fragmented phospholipids as substrates. J Biol Chem 1991;266:11095-103.
78. Tselepis AD, Elisaf M, Goudevenos J, et al. PAF-acetylhydrolase is an antiinflammatory and antioxidant phospholipase A2 that may be implicated in atherothrombosis. Atheroscler Suppl 1999;144:1.
79. Lewis GF, Rader DJ. New insights into the regulation of HDL metabolism and reverse cholesterol transport. Circ Res 2005;96:1221-32.
80. Moore RE, Navab M, Millar JS, et al. Increased atherosclerosis in mice lacking apolipoprotein A-I attributable to both impaired reverse cholesterol transport and increased inflammation. Circ Res 2005;97:763-71.
81. Williamson R, Lee D, Hagaman J, Maeda N. Marked reduction of high density lipoprotein cholesterol in mice genetically modified to lack apolipoprotein A-I. Proc Natl Acad Sci U S A 1992;89:7134-8.
82. Rubin EM, Krauss RM, Spangler EA, Verstuyft JG, Clift SM. Inhibition of early atherogenesis in transgenic mice by human apolipoprotein AI. Nature 1991;353:265-7.
83. Franceschini G, Sirtori CR, Capurso A, 2nd, Weisgraber KH, Mahley RW. A-IMilano apoprotein. Decreased high density lipoprotein cholesterol levels with significant lipoprotein modifications and without clinical atherosclerosis in an Italian family. J Clin Invest 1980;66:892-900.
84. Sirtori CR, Calabresi L, Franceschini G, et al. Cardiovascular status of carriers of the apolipoprotein A-I(Milano) mutant: the Limone sul Garda study. Circulation 2001;103:1949-54.
85. Parolini C, Marchesi M, Lorenzon P, et al. Dose-related effects of repeated ETC-216 (recombinant apolipoprotein A-I Milano/1-palmitoyl-2-oleoyl phosphatidylcholine complexes) administrations on rabbit lipid-rich soft plaques:

72
in vivo assessment by intravascular ultrasound and magnetic resonance imaging. J Am Coll Cardiol 2008;51:1098-103.
86. Chiesa G, Monteggia E, Marchesi M, et al. Recombinant apolipoprotein A-I(Milano) infusion into rabbit carotid artery rapidly removes lipid from fatty streaks. Circ Res 2002;90:974-80.
87. Shah PK, Nilsson J, Kaul S, et al. Effects of recombinant apolipoprotein A-I(Milano) on aortic atherosclerosis in apolipoprotein E-deficient mice. Circulation 1998;97:780-5.
88. Nissen SE, Tsunoda T, Tuzcu EM, et al. Effect of recombinant ApoA-I Milano on coronary atherosclerosis in patients with acute coronary syndromes: a randomized controlled trial. JAMA 2003;290:2292-300.
89. Luc G, Bard JM, Ferrieres J, et al. Value of HDL cholesterol, apolipoprotein A-I, lipoprotein A-I, and lipoprotein A-I/A-II in prediction of coronary heart disease: the PRIME Study. Prospective Epidemiological Study of Myocardial Infarction. Arterioscler Thromb Vasc Biol 2002;22:1155-61.
90. Ishikawa T, Fidge N, Thelle DS, Forde OH, Miller NE. The Tromso Heart Study: serum apolipoprotein AI concentration in relation to future coronary heart disease. Eur J Clin Invest 1978;8:179-82.
91. Salonen JT, Salonen R, Penttila I, et al. Serum fatty acids, apolipoproteins, selenium and vitamin antioxidants and the risk of death from coronary artery disease. Am J Cardiol 1985;56:226-31.
92. Coleman MP, Key TJ, Wang DY, et al. A prospective study of obesity, lipids, apolipoproteins and ischaemic heart disease in women. Atherosclerosis 1992;92:177-85.
93. Sigurdsson G, Baldursdottir A, Sigvaldason H, Agnarsson U, Thorgeirsson G, Sigfusson N. Predictive value of apolipoproteins in a prospective survey of coronary artery disease in men. Am J Cardiol 1992;69:1251-4.
94. Wald NJ, Law M, Watt HC, et al. Apolipoproteins and ischaemic heart disease: implications for screening. Lancet 1994;343:75-9.
95. Lamarche B, Moorjani S, Lupien PJ, et al. Apolipoprotein A-I and B levels and the risk of ischemic heart disease during a five-year follow-up of men in the Quebec cardiovascular study. Circulation 1996;94:273-8.
96. Walldius G, Jungner I. Apolipoprotein B and apolipoprotein A-I: risk indicators of coronary heart disease and targets for lipid-modifying therapy. J Intern Med 2004;255:188-205.
97. Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med 1977;62:707-14.
98. Chirovsky DR, Fedirko V, Cui Y, Sazonov V, Barter P. Prospective studies on the relationship between high-density lipoprotein cholesterol and cardiovascular risk: a systematic review. Eur J Cardiovasc Prev Rehabil 2009.
99. Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr 2003;77:1146-55.

73
100. Lichtenstein AH, Appel LJ, Brands M, et al. Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. Circulation 2006;114:82-96.
101. Oguma Y, Sesso HD, Paffenbarger RS, Jr., Lee IM. Physical activity and all cause mortality in women: a review of the evidence. Br J Sports Med 2002;36:162-72.
102. Bakhru A, Erlinger TP. Smoking cessation and cardiovascular disease risk factors: results from the Third National Health and Nutrition Examination Survey. PLoS Med 2005;2:e160.
103. Eilat-Adar S, Eldar M, Goldbourt U. Association of intentional changes in body weight with coronary heart disease event rates in overweight subjects who have an additional coronary risk factor. Am J Epidemiol 2005;161:352-8.
104. O'Keefe JH, Bybee KA, Lavie CJ. Alcohol and cardiovascular health: the razor-sharp double-edged sword. J Am Coll Cardiol 2007;50:1009-14.
105. Fraser GE, Sabate J, Beeson WL, Strahan TM. A possible protective effect of nut consumption on risk of coronary heart disease. The Adventist Health Study. Arch Intern Med 1992;152:1416-24.
106. Prineas RJ, Kushi LH, Folsom AR, Bostick RM, Wu Y. Walnuts and serum lipids. N Engl J Med 1993;329:359; author reply 359-60.
107. Grundy SM, Denke MA. Dietary influences on serum lipids and lipoproteins. J Lipid Res 1990;31:1149-72.
108. Kris-Etherton PM, Zhao G, Binkoski AE, Coval SM, Etherton TD. The effects of nuts on coronary heart disease risk. Nutr Rev 2001;59:103-11.
109. Hu FB, Willett WC. Optimal diets for prevention of coronary heart disease. JAMA 2002;288:2569-78.
110. Ellsworth JL, Kushi LH, Folsom AR. Frequent nut intake and risk of death from coronary heart disease and all causes in postmenopausal women: the Iowa Women's Health Study. Nutr Metab Cardiovasc Dis 2001;11:372-7.
111. Hu FB, Stampfer MJ, Manson JE, et al. Frequent nut consumption and risk of coronary heart disease in women: prospective cohort study. BMJ 1998;317:1341-5.
112. Albert CM, Gaziano JM, Willett WC, Manson JE. Nut consumption and decreased risk of sudden cardiac death in the Physicians' Health Study. Arch Intern Med 2002;162:1382-7.
113. Food labeling: health claims; plant sterol/stanol esters and coronary heart disease. Food and Drug Administration, HHS. Interim final rule. Fed Regist 2000;65:54686-739.
114. Spiller GA, Jenkins DA, Bosello O, Gates JE, Cragen LN, Bruce B. Nuts and plasma lipids: an almond-based diet lowers LDL-C while preserving HDL-C. J Am Coll Nutr 1998;17:285-90.
115. Hyson DA, Schneeman BO, Davis PA. Almonds and almond oil have similar effects on plasma lipids and LDL oxidation in healthy men and women. J Nutr 2002;132:703-7.
116. Sabate J, Haddad E, Tanzman JS, Jambazian P, Rajaram S. Serum lipid response to the graduated enrichment of a Step I diet with almonds: a randomized feeding trial. Am J Clin Nutr 2003;77:1379-84.

74
117. Lovejoy JC, Most MM, Lefevre M, Greenway FL, Rood JC. Effect of diets enriched in almonds on insulin action and serum lipids in adults with normal glucose tolerance or type 2 diabetes. Am J Clin Nutr 2002;76:1000-6.
118. Jenkins DJ, Kendall CW, Marchie A, et al. Dose response of almonds on coronary heart disease risk factors: blood lipids, oxidized low-density lipoproteins, lipoprotein(a), homocysteine, and pulmonary nitric oxide: a randomized, controlled, crossover trial. Circulation 2002;106:1327-32.
119. Ros E. Nuts and novel biomarkers of cardiovascular disease. Am J Clin Nutr 2009;89:1649S-56S.
120. Torabian S, Haddad E, Rajaram S, Banta J, Sabate J. Acute effect of nut consumption on plasma total polyphenols, antioxidant capacity and lipid peroxidation. J Hum Nutr Diet 2009;22:64-71.
121. Chen CY, Milbury PE, Chung SK, Blumberg J. Effect of almond skin polyphenolics and quercetin on human LDL and apolipoprotein B-100 oxidation and conformation. J Nutr Biochem 2007;18:785-94.
122. Chen CY, Blumberg JB. In vitro activity of almond skin polyphenols for scavenging free radicals and inducing quinone reductase. J Agric Food Chem 2008;56:4427-34.
123. Sirtori CR, Even R, Lovati MR. Soybean protein diet and plasma cholesterol: from therapy to molecular mechanisms. Ann N Y Acad Sci 1993;676:188-201.
124. Kestin M, Rouse IL, Correll RA, Nestel PJ. Cardiovascular disease risk factors in free-living men: comparison of two prudent diets, one based on lactoovovegetarianism and the other allowing lean meat. Am J Clin Nutr 1989;50:280-7.
125. Sirtori CR, Lovati MR. Soy proteins and cardiovascular disease. Curr Atheroscler Rep 2001;3:47-53.
126. Anderson JW, Johnstone BM, Cook-Newell ME. Meta-analysis of the effects of soy protein intake on serum lipids. N Engl J Med 1995;333:276-82.
127. Carroll KK. Hypercholesterolemia and atherosclerosis: effects of dietary protein. Fed Proc 1982;41:2792-6.
128. Descovich GC, Ceredi C, Gaddi A, et al. Multicentre study of soybean protein diet for outpatient hyper-cholesterolaemic patients. Lancet 1980;2:709-12.
129. Sacks FM, Lichtenstein A, Van Horn L, Harris W, Kris-Etherton P, Winston M. Soy protein, isoflavones, and cardiovascular health: an American Heart Association Science Advisory for professionals from the Nutrition Committee. Circulation 2006;113:1034-44.
130. Lovati MR, Manzoni C, Canavesi A, et al. Soybean protein diet increases low density lipoprotein receptor activity in mononuclear cells from hypercholesterolemic patients. J Clin Invest 1987;80:1498-502.
131. Harland JI, Haffner TA. Systematic review, meta-analysis and regression of randomised controlled trials reporting an association between an intake of circa 25 g soya protein per day and blood cholesterol. Atherosclerosis 2008;200:13-27.
132. Meinertz H, Nilausen K, Faergeman O. Soy protein and casein in cholesterol-enriched diets: effects on plasma lipoproteins in normolipidemic subjects. Am J Clin Nutr 1989;50:786-93.

75
133. Taku K, Umegaki K, Sato Y, Taki Y, Endoh K, Watanabe S. Soy isoflavones lower serum total and LDL cholesterol in humans: a meta-analysis of 11 randomized controlled trials. Am J Clin Nutr 2007;85:1148-56.
134. Reynolds K, Chin A, Lees KA, Nguyen A, Bujnowski D, He J. A meta-analysis of the effect of soy protein supplementation on serum lipids. Am J Cardiol 2006;98:633-40.
135. Zhan S, Ho SC. Meta-analysis of the effects of soy protein containing isoflavones on the lipid profile. Am J Clin Nutr 2005;81:397-408.
136. Sirtori CR, Eberini I, Arnoldi A. Hypocholesterolaemic effects of soya proteins: results of recent studies are predictable from the anderson meta-analysis data. Br J Nutr 2007;97:816-22.
137. Sadler M. Soy and health 2006: Clinical evidence - dietetic application. British Nutrition Foundation: Nutrition Bulletin 2007:85-90.
138. Hoie LH, Sjoholm A, Guldstrand M, et al. Ultra heat treatment destroys cholesterol-lowering effect of soy protein. Int J Food Sci Nutr 2006;57:512-9.
139. Chen HM, Muramoto K, Yamauchi F, Fujimoto K, Nokihara K. Antioxidative Properties of Histidine-Containing Peptides Designed from Peptide Fragments Found in the Digests of a Soybean Protein. J Agric Food Chem 1998;46:49-53.
140. Okuda M, Inoue N, Azumi H, et al. Expression of glutaredoxin in human coronary arteries: its potential role in antioxidant protection against atherosclerosis. Arterioscler Thromb Vasc Biol 2001;21:1483-7.
141. Manzoni C, Duranti M, Eberini I, et al. Subcellular localization of soybean 7S globulin in HepG2 cells and LDL receptor up-regulation by its alpha' constituent subunit. J Nutr 2003;133:2149-55.
142. Duranti M, Lovati MR, Dani V, et al. The alpha' subunit from soybean 7S globulin lowers plasma lipids and upregulates liver beta-VLDL receptors in rats fed a hypercholesterolemic diet. J Nutr 2004;134:1334-9.
143. Bricarello LP, Kasinski N, Bertolami MC, et al. Comparison between the effects of soy milk and non-fat cow milk on lipid profile and lipid peroxidation in patients with primary hypercholesterolemia. Nutrition 2004;20:200-4.
144. Mitchell JH, Collins AR. Effects of a soy milk supplement on plasma cholesterol levels and oxidative DNA damage in men--a pilot study. Eur J Nutr 1999;38:143-8.
145. Jenkins DJ, Kendall CW, Jackson CJ, et al. Effects of high- and low-isoflavone soyfoods on blood lipids, oxidized LDL, homocysteine, and blood pressure in hyperlipidemic men and women. Am J Clin Nutr 2002;76:365-72.
146. Scheiber MD, Liu JH, Subbiah MT, Rebar RW, Setchell KD. Dietary inclusion of whole soy foods results in significant reductions in clinical risk factors for osteoporosis and cardiovascular disease in normal postmenopausal women. Menopause 2001;8:384-92.
147. Jenkins DJ, Kendall CW, Vidgen E, et al. Effect of soy-based breakfast cereal on blood lipids and oxidized low-density lipoprotein. Metabolism 2000;49:1496-500.
148. Jenkins DJ, Kendall CW, Garsetti M, et al. Effect of soy protein foods on low-density lipoprotein oxidation and ex vivo sex hormone receptor activity--a controlled crossover trial. Metabolism 2000;49:537-43.

76
149. Tikkanen MJ, Wahala K, Ojala S, Vihma V, Adlercreutz H. Effect of soybean phytoestrogen intake on low density lipoprotein oxidation resistance. Proc Natl Acad Sci U S A 1998;95:3106-10.
150. Wiseman H, O'Reilly JD, Adlercreutz H, et al. Isoflavone phytoestrogens consumed in soy decrease F(2)-isoprostane concentrations and increase resistance of low-density lipoprotein to oxidation in humans. Am J Clin Nutr 2000;72:395-400.
151. Zhang X, Shu XO, Gao YT, et al. Soy food consumption is associated with lower risk of coronary heart disease in Chinese women. J Nutr 2003;133:2874-8.
152. Anderson JW, Baird P, Davis RH, Jr., et al. Health benefits of dietary fiber. Nutr Rev 2009;67:188-205.
153. Bazzano LA. Effects of soluble dietary fiber on low-density lipoprotein cholesterol and coronary heart disease risk. Curr Atheroscler Rep 2008;10:473-7.
154. Brown L, Rosner B, Willett WW, Sacks FM. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr 1999;69:30-42.
155. Ripsin CM, Keenan JM, Jacobs DR, Jr., et al. Oat products and lipid lowering. A meta-analysis. JAMA 1992;267:3317-25.
156. Ellegard L, Andersson H. Oat bran rapidly increases bile acid excretion and bile acid synthesis: an ileostomy study. Eur J Clin Nutr 2007;61:938-45.
157. Daggy BP, O'Connell NC, Jerdack GR, Stinson BA, Setchell KD. Additive hypocholesterolemic effect of psyllium and cholestyramine in the hamster: influence on fecal sterol and bile acid profiles. J Lipid Res 1997;38:491-502.
158. Nishina PM, Freedland RA. The effects of dietary fiber feeding on cholesterol metabolism in rats. J Nutr 1990;120:800-5.
159. Schneeman BO, Gallaher D. Effects of dietary fiber on digestive enzyme activity and bile acids in the small intestine. Proc Soc Exp Biol Med 1985;180:409-14.
160. Shrestha S, Freake HC, McGrane MM, Volek JS, Fernandez ML. A combination of psyllium and plant sterols alters lipoprotein metabolism in hypercholesterolemic subjects by modifying the intravascular processing of lipoproteins and increasing LDL uptake. J Nutr 2007;137:1165-70.
161. Ma Y, Griffith JA, Chasan-Taber L, et al. Association between dietary fiber and serum C-reactive protein. Am J Clin Nutr 2006;83:760-6.
162. Ajani UA, Ford ES, Mokdad AH. Dietary fiber and C-reactive protein: findings from national health and nutrition examination survey data. J Nutr 2004;134:1181-5.
163. Streppel MT, Arends LR, van 't Veer P, Grobbee DE, Geleijnse JM. Dietary fiber and blood pressure: a meta-analysis of randomized placebo-controlled trials. Arch Intern Med 2005;165:150-6.
164. Whelton SP, Hyre AD, Pedersen B, Yi Y, Whelton PK, He J. Effect of dietary fiber intake on blood pressure: a meta-analysis of randomized, controlled clinical trials. J Hypertens 2005;23:475-81.
165. Kuo DC, Hsu SP, Chien CT. Partially hydrolyzed guar gum supplement reduces high-fat diet increased blood lipids and oxidative stress and ameliorates FeCl3-induced acute arterial injury in hamsters. J Biomed Sci 2009;16:15.
166. Jacobs DR, Jr., Andersen LF, Blomhoff R. Whole-grain consumption is associated with a reduced risk of noncardiovascular, noncancer death attributed

77
to inflammatory diseases in the Iowa Women's Health Study. Am J Clin Nutr 2007;85:1606-14.
167. Kerckhoffs DA, Brouns F, Hornstra G, Mensink RP. Effects on the human serum lipoprotein profile of beta-glucan, soy protein and isoflavones, plant sterols and stanols, garlic and tocotrienols. J Nutr 2002;132:2494-505.
168. de Jong A, Plat J, Mensink RP. Metabolic effects of plant sterols and stanols (Review). J Nutr Biochem 2003;14:362-9.
169. Chen JT, Wesley R, Shamburek RD, Pucino F, Csako G. Meta-analysis of natural therapies for hyperlipidemia: plant sterols and stanols versus policosanol. Pharmacotherapy 2005;25:171-83.
170. Clifton PM, Noakes M, Sullivan D, et al. Cholesterol-lowering effects of plant sterol esters differ in milk, yoghurt, bread and cereal. Eur J Clin Nutr 2004;58:503-9.
171. Devaraj S, Jialal I, Vega-Lopez S. Plant sterol-fortified orange juice effectively lowers cholesterol levels in mildly hypercholesterolemic healthy individuals. Arterioscler Thromb Vasc Biol 2004;24:e25-8.
172. Polagruto JA, Wang-Polagruto JF, Braun MM, Lee L, Kwik-Uribe C, Keen CL. Cocoa flavanol-enriched snack bars containing phytosterols effectively lower total and low-density lipoprotein cholesterol levels. J Am Diet Assoc 2006;106:1804-13.
173. Richelle M, Enslen M, Hager C, et al. Both free and esterified plant sterols reduce cholesterol absorption and the bioavailability of beta-carotene and alpha-tocopherol in normocholesterolemic humans. Am J Clin Nutr 2004;80:171-7.
174. Assmann G, Cullen P, Erbey J, Ramey DR, Kannenberg F, Schulte H. Plasma sitosterol elevations are associated with an increased incidence of coronary events in men: results of a nested case-control analysis of the Prospective Cardiovascular Munster (PROCAM) study. Nutr Metab Cardiovasc Dis 2006;16:13-21.
175. Hubacek JA, Berge KE, Cohen JC, Hobbs HH. Mutations in ATP-cassette binding proteins G5 (ABCG5) and G8 (ABCG8) causing sitosterolemia. Hum Mutat 2001;18:359-60.
176. Weggemans RM, Zock PL, Tai ES, Ordovas JM, Molhuizen HO, Katan MB. ATP binding cassette G5 C1950G polymorphism may affect blood cholesterol concentrations in humans. Clin Genet 2002;62:226-9.
177. Miwa K, Inazu A, Kobayashi J, et al. ATP-binding cassette transporter G8 M429V polymorphism as a novel genetic marker of higher cholesterol absorption in hypercholesterolaemic Japanese subjects. Clin Sci (Lond) 2005;109:183-8.
178. Pinedo S, Vissers MN, von Bergmann K, et al. Plasma levels of plant sterols and the risk of coronary artery disease: the prospective EPIC-Norfolk Population Study. J Lipid Res 2007;48:139-44.
179. Wilund KR, Yu L, Xu F, et al. No association between plasma levels of plant sterols and atherosclerosis in mice and men. Arterioscler Thromb Vasc Biol 2004;24:2326-32.
180. Fassbender K, Lutjohann D, Dik MG, et al. Moderately elevated plant sterol levels are associated with reduced cardiovascular risk--the LASA study. Atherosclerosis 2008;196:283-8.

78
181. Korpela R, Tuomilehto J, Hogstrom P, et al. Safety aspects and cholesterol-lowering efficacy of low fat dairy products containing plant sterols. Eur J Clin Nutr 2006;60:633-42.
182. Kwiterovich PO, Jr., Chen SC, Virgil DG, Schweitzer A, Arnold DR, Kratz LE. Response of obligate heterozygotes for phytosterolemia to a low-fat diet and to a plant sterol ester dietary challenge. J Lipid Res 2003;44:1143-55.
183. Berger A, Jones PJ, Abumweis SS. Plant sterols: factors affecting their efficacy and safety as functional food ingredients. Lipids Health Dis 2004;3:5.
184. Bouic PJ. The role of phytosterols and phytosterolins in immune modulation: a review of the past 10 years. Curr Opin Clin Nutr Metab Care 2001;4:471-5.
185. Homma Y, Ikeda I, Ishikawa T, Tateno M, Sugano M, Nakamura H. Decrease in plasma low-density lipoprotein cholesterol, apolipoprotein B, cholesteryl ester transfer protein, and oxidized low-density lipoprotein by plant stanol ester-containing spread: a randomized, placebo-controlled trial. Nutrition 2003;19:369-74.
186. Wang T, Hicks KB, Moreau R. Antioxidant activity of phytosterols, oryzanol, and other phytosterol conjugates. J Am Oil Chem Soc 2002;79:1201-1206.
187. De Jong A, Plat J, Bast A, Godschalk RW, Basu S, Mensink RP. Effects of plant sterol and stanol ester consumption on lipid metabolism, antioxidant status and markers of oxidative stress, endothelial function and low-grade inflammation in patients on current statin treatment. Eur J Clin Nutr 2008;62:263-73.
188. Krauss RM, Eckel RH, Howard B, et al. AHA Dietary Guidelines: revision 2000: A statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Circulation 2000;102:2284-99.
189. Adminstration USFaD. Food Labeling: Health Claims; Soluble Fiber from Whole Oats and Risk of Coronary Heart Disease. Washington, DC: United States Food and Drug Adminstration, 2001:15343-15344.
190. Administration USFaD. FDA Final Rule for Food Labelling: Health Claims; Soy Protein and Coronary Heart Disease. United States Food and Drug Administriation, 1999:Federal Register 64:57699-57733.
191. Anderson JW, Story L, Sieling B, Chen WJ, Petro MS, Story J. Hypocholesterolemic effects of oat-bran or bean intake for hypercholesterolemic men. Am J Clin Nutr 1984;40:1146-55.
192. Kritchevsky D, Story JA. Binding of bile salts in vitro by nonnutritive fiber. J Nutr 1974;104:458-62.
193. Jenkins DJ, Wolever TM, Rao AV, et al. Effect on blood lipids of very high intakes of fiber in diets low in saturated fat and cholesterol. N Engl J Med 1993;329:21-6.
194. Lees AM, Mok HY, Lees RS, McCluskey MA, Grundy SM. Plant sterols as cholesterol-lowering agents: clinical trials in patients with hypercholesterolemia and studies of sterol balance. Atherosclerosis 1977;28:325-38.
195. Heinemann T, Leiss O, von Bergmann K. Effect of low-dose sitostanol on serum cholesterol in patients with hypercholesterolemia. Atherosclerosis 1986;61:219-23.
196. Kurowska EM, Carroll KK. Effect of high levels of selected dietary essential amino acids on hypercholesterolemia and down-regulation of hepatic LDL receptors in rabbits. Biochim Biophys Acta 1992;1126:185-91.

79
197. Baum JA, Teng H, Erdman JW, Jr., et al. Long-term intake of soy protein improves blood lipid profiles and increases mononuclear cell low-density-lipoprotein receptor messenger RNA in hypercholesterolemic, postmenopausal women. Am J Clin Nutr 1998;68:545-51.
198. Jenkins DJ, Kendall CW, Faulkner D, et al. A dietary portfolio approach to cholesterol reduction: combined effects of plant sterols, vegetable proteins, and viscous fibers in hypercholesterolemia. Metabolism 2002;51:1596-604.
199. Jenkins DJ, Kendall CW, Faulkner DA, et al. Assessment of the longer-term effects of a dietary portfolio of cholesterol-lowering foods in hypercholesterolemia. Am J Clin Nutr 2006;83:582-91.
200. Jenkins DJ, Kendall CW, Faulkner DA, et al. Long-term effects of a plant-based dietary portfolio of cholesterol-lowering foods on blood pressure. Eur J Clin Nutr 2008;62:781-8.
201. Jenkins DJ, Kendall CW, Nguyen TH, et al. Effect on hematologic risk factors for coronary heart disease of a cholesterol reducing diet. Eur J Clin Nutr 2007;61:483-92.
202. Gigleux I, Jenkins DJ, Kendall CW, et al. Comparison of a dietary portfolio diet of cholesterol-lowering foods and a statin on LDL particle size phenotype in hypercholesterolaemic participants. Br J Nutr 2007;98:1229-36.
203. Ashton EL, Best JD, Ball MJ. Effects of monounsaturated enriched sunflower oil on CHD risk factors including LDL size and copper-induced LDL oxidation. J Am Coll Nutr 2001;20:320-6.
204. Clarke R, Frost C, Collins R, Appleby P, Peto R. Dietary lipids and blood cholesterol: quantitative meta-analysis of metabolic ward studies. BMJ 1997;314:112-7.
205. Berry EM, Eisenberg S, Haratz D, et al. Effects of diets rich in monounsaturated fatty acids on plasma lipoproteins--the Jerusalem Nutrition Study: high MUFAs vs high PUFAs. Am J Clin Nutr 1991;53:899-907.
206. Horwitz DL, Rubenstein AH, Reynolds C, Molnar GD, Yanaihara N. Prolonged suppression of insulin release by insulin-induced hypoglycemia: demonstration by C-peptide assay. Horm Metab Res 1975;7:449-52.
207. Mattson FH, Grundy SM. Comparison of effects of dietary saturated, monounsaturated, and polyunsaturated fatty acids on plasma lipids and lipoproteins in man. J Lipid Res 1985;26:194-202.
208. Berglund L, Lefevre M, Ginsberg HN, et al. Comparison of monounsaturated fat with carbohydrates as a replacement for saturated fat in subjects with a high metabolic risk profile: studies in the fasting and postprandial states. Am J Clin Nutr 2007;86:1611-20.
209. Cicero AF, Nascetti S, Lopez-Sabater MC, et al. Changes in LDL fatty acid composition as a response to olive oil treatment are inversely related to lipid oxidative damage: The EUROLIVE study. J Am Coll Nutr 2008;27:314-20.
210. Reaven P, Parthasarathy S, Grasse BJ, et al. Feasibility of using an oleate-rich diet to reduce the susceptibility of low-density lipoprotein to oxidative modification in humans. Am J Clin Nutr 1991;54:701-6.

80
211. Dreon DM, Vranizan KM, Krauss RM, Austin MA, Wood PD. The effects of polyunsaturated fat vs monounsaturated fat on plasma lipoproteins. JAMA 1990;263:2462-6.
212. O'Byrne DJ, Knauft DA, Shireman RB. Low fat-monounsaturated rich diets containing high-oleic peanuts improve serum lipoprotein profiles. Lipids 1997;32:687-95.
213. Morgan SA, O'Dea K, Sinclair AJ. A low-fat diet supplemented with monounsaturated fat results in less HDL-C lowering than a very-low-fat diet. J Am Diet Assoc 1997;97:151-6.
214. Garg A, Grundy SM, Unger RH. Comparison of effects of high and low carbohydrate diets on plasma lipoproteins and insulin sensitivity in patients with mild NIDDM. Diabetes 1992;41:1278-85.
215. Garg A, Bonanome A, Grundy SM, Zhang ZJ, Unger RH. Comparison of a high-carbohydrate diet with a high-monounsaturated-fat diet in patients with non-insulin-dependent diabetes mellitus. N Engl J Med 1988;319:829-34.
216. Perez-Jimenez F, Espino A, Lopez-Segura F, et al. Lipoprotein concentrations in normolipidemic males consuming oleic acid-rich diets from two different sources: olive oil and oleic acid-rich sunflower oil. Am J Clin Nutr 1995;62:769-75.
217. Karmally W. Balancing unsaturated fatty acids: what's the evidence for cholesterol lowering? J Am Diet Assoc 2005;105:1068-70.
218. Mensink RP, Katan MB. Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arterioscler Thromb 1992;12:911-9.
219. Yu S, Derr J, Etherton TD, Kris-Etherton PM. Plasma cholesterol-predictive equations demonstrate that stearic acid is neutral and monounsaturated fatty acids are hypocholesterolemic. Am J Clin Nutr 1995;61:1129-39.
220. Blum CB, Levy RI, Eisenberg S, Hall M, 3rd, Goebel RH, Berman M. High density lipoprotein metabolism in man. J Clin Invest 1977;60:795-807.
221. Brinton EA, Eisenberg S, Breslow JL. A low-fat diet decreases high density lipoprotein (HDL) cholesterol levels by decreasing HDL apolipoprotein transport rates. J Clin Invest 1990;85:144-51.
222. Lamarche B, Rashid S, Lewis GF. HDL metabolism in hypertriglyceridemic states: an overview. Clin Chim Acta 1999;286:145-61.
223. Patsch JR, Prasad S, Gotto AM, Jr., Patsch W. High density lipoprotein2. Relationship of the plasma levels of this lipoprotein species to its composition, to the magnitude of postprandial lipemia, and to the activities of lipoprotein lipase and hepatic lipase. J Clin Invest 1987;80:341-7.
224. Patsch JR, Karlin JB, Scott LW, Smith LC, Gotto AM, Jr. Inverse relationship between blood levels of high density lipoprotein subfraction 2 and magnitude of postprandial lipemia. Proc Natl Acad Sci U S A 1983;80:1449-53.
225. Lewis GF, O'Meara NM, Soltys PA, et al. Fasting hypertriglyceridemia in noninsulin-dependent diabetes mellitus is an important predictor of postprandial lipid and lipoprotein abnormalities. J Clin Endocrinol Metab 1991;72:934-44.
226. Lewis GF, O'Meara NM, Soltys PA, et al. Postprandial lipoprotein metabolism in normal and obese subjects: comparison after the vitamin A fat-loading test. J Clin Endocrinol Metab 1990;71:1041-50.

81
227. Syvanne M, Taskinen MR. Lipids and lipoproteins as coronary risk factors in non-insulin-dependent diabetes mellitus. Lancet 1997;350 Suppl 1:SI20-3.
228. Tall AR. Plasma high density lipoproteins. Metabolism and relationship to atherogenesis. J Clin Invest 1990;86:379-84.
229. Eisenberg S. Lipoprotein abnormalities in hypertriglyceridemia: significance in atherosclerosis. Am Heart J 1987;113:555-61.
230. Mann CJ, Yen FT, Grant AM, Bihain BE. Mechanism of plasma cholesteryl ester transfer in hypertriglyceridemia. J Clin Invest 1991;88:2059-66.
231. Foger B, Ritsch A, Doblinger A, Wessels H, Patsch JR. Relationship of plasma cholesteryl ester transfer protein to HDL cholesterol. Studies in normotriglyceridemia and moderate hypertriglyceridemia. Arterioscler Thromb Vasc Biol 1996;16:1430-6.
232. Clay MA, Newnham HH, Forte TM, Barter PI. Cholesteryl ester transfer protein and hepatic lipase activity promote shedding of apo A-I from HDL and subsequent formation of discoidal HDL. Biochim Biophys Acta 1992;1124:52-8.
233. Brinton EA, Eisenberg S, Breslow JL. Human HDL cholesterol levels are determined by apoA-I fractional catabolic rate, which correlates inversely with estimates of HDL particle size. Effects of gender, hepatic and lipoprotein lipases, triglyceride and insulin levels, and body fat distribution. Arterioscler Thromb 1994;14:707-20.
234. Brinton EA, Eisenberg S, Breslow JL. Increased apo A-I and apo A-II fractional catabolic rate in patients with low high density lipoprotein-cholesterol levels with or without hypertriglyceridemia. J Clin Invest 1991;87:536-44.
235. Horowitz BS, Goldberg IJ, Merab J, Vanni TM, Ramakrishnan R, Ginsberg HN. Increased plasma and renal clearance of an exchangeable pool of apolipoprotein A-I in subjects with low levels of high density lipoprotein cholesterol. J Clin Invest 1993;91:1743-52.
236. Vajo Z, Terry JG, Brinton EA. Increased intra-abdominal fat may lower HDL levels by increasing the fractional catabolic rate of Lp A-I in postmenopausal women. Atherosclerosis 2002;160:495-501.
237. Pont F, Duvillard L, Florentin E, Gambert P, Verges B. High-density lipoprotein apolipoprotein A-I kinetics in obese insulin resistant patients. An in vivo stable isotope study. Int J Obes Relat Metab Disord 2002;26:1151-8.
238. Rashid S, Watanabe T, Sakaue T, Lewis GF. Mechanisms of HDL lowering in insulin resistant, hypertriglyceridemic states: the combined effect of HDL triglyceride enrichment and elevated hepatic lipase activity. Clin Biochem 2003;36:421-9.
239. Jenkins DJ, Kendall CW, Marchie A, et al. Direct comparison of a dietary portfolio of cholesterol-lowering foods with a statin in hypercholesterolemic participants. Am J Clin Nutr 2005;81:380-7.
240. Berry EM, Eisenberg S, Friedlander Y, et al. Effects of diets rich in monounsaturated fatty acids on plasma lipoproteins--the Jerusalem Nutrition Study. II. Monounsaturated fatty acids vs carbohydrates. Am J Clin Nutr 1992;56:394-403.
241. Berliner JA, Navab M, Fogelman AM, et al. Atherosclerosis: basic mechanisms. Oxidation, inflammation, and genetics. Circulation 1995;91:2488-96.

82
242. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004;110:227-39.
243. Barter P, Gotto AM, LaRosa JC, et al. HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events. N Engl J Med 2007;357:1301-10.
244. Gordon DJ, Probstfield JL, Garrison RJ, et al. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation 1989;79:8-15.
245. Nicholls SJ, Tuzcu EM, Sipahi I, et al. Statins, high-density lipoprotein cholesterol, and regression of coronary atherosclerosis. JAMA 2007;297:499-508.
246. Garfagnini A, Devoto G, Rosselli P, Boggiano P, Venturini M. Relationship between HDL-cholesterol and apolipoprotein A1 and the severity of coronary artery disease. Eur Heart J 1995;16:465-70.
247. Anderson KM, Wilson PW, Odell PM, Kannel WB. An updated coronary risk profile. A statement for health professionals. Circulation 1991;83:356-62.
248. Grundy SM. Comparison of monounsaturated fatty acids and carbohydrates for lowering plasma cholesterol. N Engl J Med 1986;314:745-8.
249. Mensink RP, Katan MB. Effect of monounsaturated fatty acids versus complex carbohydrates on high-density lipoproteins in healthy men and women. Lancet 1987;1:122-5.
250. Hu FB, Stampfer MJ. Nut consumption and risk of coronary heart disease: a review of epidemiologic evidence. Curr Atheroscler Rep 1999;1:204-9.
251. Halton TL, Willett WC, Liu S, et al. Low-carbohydrate-diet score and the risk of coronary heart disease in women. N Engl J Med 2006;355:1991-2002.
252. Ainsworth BE, Haskell WL, Leon AS, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 1993;25:71-80.
253. SAS/STAT User's Guide, Version 9. Cary, NC: SAS Institute Inc, 2005. 254. Clinics LR. Manual of Laboratory Operations: Lipid and Lipoprotein Analysis. . In:
(NIH) UDoHaHSp, ed. Washington, DC: US Government Printing Office, 1982:75-678.
255. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972;18:499-502.
256. Fink PC, Romer M, Haeckel R, et al. Measurement of proteins with the Behring Nephelometer. A multicentre evaluation. J Clin Chem Clin Biochem 1989;27:261-76.
257. US Department of Agriculture ARS. USDA nutrient database for standard reference, release 19. Washington, DC, 2006:Nutrient Data Laboratory Web site.
258. SAS/STAT User's Guide, Version 9.1. Cary, NC: SAS Institute Inc, 1997. 259. Kinosian B, Glick H, Garland G. Cholesterol and coronary heart disease:
predicting risks by levels and ratios. Ann Intern Med 1994;121:641-7. 260. Manninen V, Tenkanen L, Koskinen P, et al. Joint effects of serum triglyceride
and LDL cholesterol and HDL cholesterol concentrations on coronary heart

83
disease risk in the Helsinki Heart Study. Implications for treatment. Circulation 1992;85:37-45.
261. Robins SJ, Collins D, Wittes JT, et al. Relation of gemfibrozil treatment and lipid levels with major coronary events: VA-HIT: a randomized controlled trial. JAMA 2001;285:1585-91.
262. Schaefer EJ, Lamon-Fava S, Ordovas JM, et al. Factors associated with low and elevated plasma high density lipoprotein cholesterol and apolipoprotein A-I levels in the Framingham Offspring Study. J Lipid Res 1994;35:871-82.
263. Boden WE. High-density lipoprotein cholesterol as an independent risk factor in cardiovascular disease: assessing the data from Framingham to the Veterans Affairs High--Density Lipoprotein Intervention Trial. Am J Cardiol 2000;86:19L-22L.
264. Pedersen TR, Olsson AG, Faergeman O, et al. Lipoprotein changes and reduction in the incidence of major coronary heart disease events in the Scandinavian Simvastatin Survival Study (4S). Circulation 1998;97:1453-60.
265. Frick MH, Elo O, Haapa K, et al. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med 1987;317:1237-45.
266. Tardif JC, Gregoire J, L'Allier PL, et al. Effects of reconstituted high-density lipoprotein infusions on coronary atherosclerosis: a randomized controlled trial. JAMA 2007;297:1675-82.
267. Brown G, Albers JJ, Fisher LD, et al. Regression of coronary artery disease as a result of intensive lipid-lowering therapy in men with high levels of apolipoprotein B. N Engl J Med 1990;323:1289-98.
268. Whitney EJ, Krasuski RA, Personius BE, et al. A randomized trial of a strategy for increasing high-density lipoprotein cholesterol levels: effects on progression of coronary heart disease and clinical events. Ann Intern Med 2005;142:95-104.
269. Appel LJ, Sacks FM, Carey VJ, et al. Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: results of the OmniHeart randomized trial. JAMA 2005;294:2455-64.
270. Brown JM, Shelness GS, Rudel LL. Monounsaturated fatty acids and atherosclerosis: opposing views from epidemiology and experimental animal models. Curr Atheroscler Rep 2007;9:494-500.
271. Executive summary: standards of medical care in diabetes--2009. Diabetes Care 2009;32 Suppl 1:S6-12.
272. Garg A, Bantle JP, Henry RR, et al. Effects of varying carbohydrate content of diet in patients with non-insulin-dependent diabetes mellitus. JAMA 1994;271:1421-8.
273. Gill JM, Brown JC, Caslake MJ, et al. Effects of dietary monounsaturated fatty acids on lipoprotein concentrations, compositions, and subfraction distributions and on VLDL apolipoprotein B kinetics: dose-dependent effects on LDL. Am J Clin Nutr 2003;78:47-56.
274. Kris-Etherton PM, Pearson TA, Wan Y, et al. High-monounsaturated fatty acid diets lower both plasma cholesterol and triacylglycerol concentrations. Am J Clin Nutr 1999;70:1009-15.

84
275. Nalsen C, Vessby B, Berglund L, et al. Dietary (n-3) fatty acids reduce plasma F2-isoprostanes but not prostaglandin F2alpha in healthy humans. J Nutr 2006;136:1222-8.
276. Lewis GF. Determinants of plasma HDL concentrations and reverse cholesterol transport. Curr Opin Cardiol 2006;21:345-52.
277. Tall AR. Cholesterol efflux pathways and other potential mechanisms involved in the athero-protective effect of high density lipoproteins. J Intern Med 2008;263:256-73.
278. Lewis GF, Rashid S, Uffelman KD, Lamarche B. Mechanism of HDL lowering in insulin resistant states. Adv Exp Med Biol 2001;498:273-7.
279. Jenkins DJ. F.F.A., intestinal bypass, and arterial lipid accumulation. Lancet 1978;2:786-7.
280. Joy T, Hegele RA. The end of the road for CETP inhibitors after torcetrapib? Curr Opin Cardiol 2009;24:364-71.
281. Wilt TJ, Bloomfield HE, MacDonald R, et al. Effectiveness of statin therapy in adults with coronary heart disease. Arch Intern Med 2004;164:1427-36.
282. Rizzo M, Kotur-Stevuljevic J, Berneis K, et al. Atherogenic dyslipidemia and oxidative stress: a new look. Transl Res 2009;153:217-23.
283. O'Bryne DJ, O'Keefe SF, Shireman RB. Low-fat, monounsaturate-rich diets reduce susceptibility of low density lipoproteins to peroxidation ex vivo. Lipids 1998;33:149-57.
284. Health NIo. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Final Report. In: National Heart L, and Blood Institute, ed., 2002.
285. Warnick GR, Benderson J, Albers JJ. Dextran sulfate-Mg2+ precipitation procedure for quantitation of high-density-lipoprotein cholesterol. Clin Chem 1982;28:1379-88.
286. Moreno JA, Lopez-Miranda J, Perez-Martinez P, et al. A monounsaturated fatty acid-rich diet reduces macrophage uptake of plasma oxidised low-density lipoprotein in healthy young men. Br J Nutr 2008;100:569-75.
287. Raha S, Robinson BH. Mitochondria, oxygen free radicals, disease and ageing. Trends Biochem Sci 2000;25:502-8.
288. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-9.
289. Tang C, Liu Y, Kessler PS, Vaughan AM, Oram JF. The macrophage cholesterol exporter ABCA1 functions as an anti-inflammatory receptor. J Biol Chem 2009.
290. Ridker PM, Danielson E, Fonseca FA, et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet 2009;373:1175-82.
291. Grover SA, Coupal L, Hu XP. Identifying adults at increased risk of coronary disease. How well do the current cholesterol guidelines work? JAMA 1995;274:801-6.

85
292. Ridker PM, Rifai N, Cook NR, Bradwin G, Buring JE. Non-HDL cholesterol, apolipoproteins A-I and B100, standard lipid measures, lipid ratios, and CRP as risk factors for cardiovascular disease in women. JAMA 2005;294:326-33.
293. Fito M, Guxens M, Corella D, et al. Effect of a traditional Mediterranean diet on lipoprotein oxidation: a randomized controlled trial. Arch Intern Med 2007;167:1195-203.
294. Mayne ST. Antioxidant nutrients and chronic disease: use of biomarkers of exposure and oxidative stress status in epidemiologic research. J Nutr 2003;133 Suppl 3:933S-940S.
295. Standards of medical care in diabetes--2009. Diabetes Care 2009;32 Suppl 1:S13-61.