-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
Main Search Page Ask A LibrarianDisplay Knowledge
BaseHelpLogoff
Full Text Save Article TextEmail Article TextPrint Preview
Cerebral Hyperemia after Arteriovenous Malformation Resection Is
Related to“Breakthrough” Complications but Not to Feeding Artery
Pressure
ISSN:
0148-
396X
Accession:
00006123-
199606000-
00005
Email
Jumpstart
Find
Citing
Articles
≪
Table
of
Contents
About
this
Journal
≫
Author(s):
Young, William L. M.D.; Kader, Abraham M.D.; Ornstein, Eugene
Ph.D., M.D.; Baker, Kristy Z. M.D.; Ostapkovich,
Noeleen R.EPT.; Pile-Spellman, John M.D.; Fogarty-Mack, Patricia
M.D.; Stein, Bennett M. M.D.; The Columbia
University Arteriovenous Malformation Study Project
Issue: Volume 38(6), June 1996, pp 1085-1095
Publication Type: [Clinical Studies]
Publisher: Copyright © by the Congress of Neurological
Surgeons
Institution(s):
Departments of Anesthesiology (WLY, EO, KZB, NO, PF-M),
Neurological Surgery (WLY, AK, JP-S, BMS), and
Radiology (WLY, JP-S), College of Physicians and Surgeons,
Columbia University, New York, New York
Received, November 27, 1995. Accepted, January 12, 1996.
Reprint requests: William L. Young, M.D., Columbia-Presbyterian
Medical Center, 630 W. 168th Street, New York,
NY 10032.
Keywords: Brain swelling, Cerebral autoregulation, Cerebral
blood flow, Cerebral hemorrhage, Cerebrovascular CO2
reactivity,
Complications, surgical
Table of Contents:
≪ ANNOUNCEMENT. ≫ Long-term Treatment of Malignant Gliomas with
Intramuscularly Administered Polyinosinic-Polycytidylic Acid
Stabilized with Polylysine and Carboxymethylcellulose: An Open
Pilot Study.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (1 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&Main+Search+Page=1&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Ask+A+Librarian=1http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Ask+A+Librarian=1http://ovidsupport.custhelp.com/cgi-bin/ovidsupport.cfg/php/enduser/std_alp.php?p_prods=336http://www.ovid.com/site/help/documentation/ovidsp/en/fulltext.htmhttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Logoff=1&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+Article=1&ftdoc=L%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Email+Article=1&ftdoc=L%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Print+Preview=1&ftdoc=L%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Fulltext%7c%26PAGE%3dfulltext%26AN%3d00006123-199606000-00005%26LSLINK%3d80%26D%3dovfthttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Fulltext%7c%26PAGE%3dfulltext%26AN%3d00006123-199606000-00005%26LSLINK%3d80%26D%3dovfthttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Cited+By+Articles=S.sh.15.16.42%7c5&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Cited+By+Articles=S.sh.15.16.42%7c5&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Cited+By+Articles=S.sh.15.16.42%7c5&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&TOC=S.sh.15.16.42%7c5%7c60&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&TOC=S.sh.15.16.42%7c5%7c60&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&TOC=S.sh.15.16.42%7c5%7c60&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&TOC=S.sh.15.16.42%7c5%7c60&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text=R%7c00006123-199606000-00005%7caboutjournal&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text=R%7c00006123-199606000-00005%7caboutjournal&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text=R%7c00006123-199606000-00005%7caboutjournal&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text=R%7c00006123-199606000-00005%7caboutjournal&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text+Link=S.sh.15.16.42%7c4%7csl_10%7c80%7c2&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text+Link=S.sh.15.16.42%7c6%7csl_10%7c80%7c2&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Full+Text+Link=S.sh.15.16.42%7c6%7csl_10%7c80%7c2&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
Links
AbstractComplete ReferenceExternalResolverBasic
Outline
● Abstract ● PATIENTS AND METHODS
�❍ Overview of study �❍ Intraoperative management
and timing of measurements �❍ Arterial CO2 pressure
(PaCO2) management �❍ CBF methodology �❍ Control group �❍
Correction factors for CBF �❍ Definition of breakthrough
complications �❍ Data analysis
● RESULTS �❍ Incidence of NPPB �❍ Relationship of CBF
changes
to NPPB �❍ Influence of detector location
on CBF results �❍ Relationship of CBF changes
to other clinical and physiological variables
�❍ Relationship of FMAP to CBF changes
Abstract
TO STUDY THE pathophysiology of idiopathic postoperative brain
swelling
or hemorrhage after arteriovenous malformation resection, termed
normal
perfusion pressure breakthrough (NPPB), we performed cerebral
blood flow
(CBF) studies during 152 operations in 143 patients, using the
xenon-133
intravenous injection method. In the first part of the study,
CBF was
intraoperatively measured (isoflurane/N20 anesthesia) during
relative hypocapnia
in 95 patients before and after resection. The NPPB group had a
greater increase (P
< 0.0001) in mean ± standard deviation global CBF (28 ± 6 to
47 ± 16 ml/100 g/min,
n = 5) than did the non-NPPB group (25 ± 7 to 29 ± 10 ml/100
g/min, n = 90);
both arteriovenous malformation groups showed greater increase
(P < 0.05) than
did controls undergoing craniotomy for tumor (23 ± 6 to 23± 6
ml/100 g/min, n =
22). Ipsilateral and contralateral CBF changes were similar. In
a second cohort
of patients with arteriovenous malformations, CBF was measured
at
relative normocapnia and it increased (P < 0.002) from pre-
to postresection (40 ±
13 to 49 ± 15 ml/100 g/min, n = 57). There were no NPPB patients
in this
latter cohort. The feeding mean arterial pressure was
measured
intraoperatively before resection or at the last embolization
before surgery (n =
64). The feeding mean arterial pressure (44 ± 16 mm Hg) was 56%
of the
systemic arterial pressure (78± 12 mm Hg, P < 0.0001) and was
not related to
changes in CBF from pre- to postresection. There was an
association
between increases in global CBF from pre- to postresection and
NPPB-
type complications, but there was no relationship of these CBF
changes
to preoperative regional arterial hypotension. These data do not
support a
uniquely hemodynamic mechanism that explains cerebral hyperemia
as
a consequence of repressurization in hypotensive vascular
beds.
The pathogenesis of idiopathic postoperative brain swelling
and
intracranial hemorrhage (ICH) after arteriovenous malformation
(AVM)
resection, termed normal perfusion pressure breakthrough (NPPB),
is
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (2 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Abstract=S.sh.15.16.42%7c5%7c1&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Complete+Reference=S.sh.15.16.42%7c5%7c1&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005&Link+Set=S.sh.15.16.42%7c5%7csl_1106020
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
�❍ Relationship of CBF changes to general neurological
outcome
�❍ Relationship of CBF changes in AVM patients to that in
control patients
● DISCUSSION �❍ Relationship of CBF and NPPB �❍ Time effect of
volatile
anesthetics �❍ Relationship between
cerebral arterial pressure and CBF changes
�❍ Possible mechanisms for postoperative CBF changes
● CONCLUSION ● ACKNOWLEDGMENTS ● REFERENCES ● APPENDIX ●
COMMENTS
Graphics
● Figure 1 ● Figure 2 ● Table 1 ● Table 2 ● Figure 3 ● Table 3 ●
Table 4 ● Figure 4 ● Plate 9
unclear. Although most large series describe an incidence
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
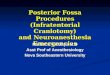
of the sterile field) (Fig. 1). The protocol was modified during
the latter part of the study to address the two following
primary criticisms: 1) that relative hypocapnia may blunt any
hyperemic responses and 2) that the detector placement was
not sensitive to changes occurring at the margins of the
resection. To this end, during the latter third of the study,
pre-
and postresection CBF was measured at relative normocapnia; CO2
was added to the inspired gas mixture for the postresection
CBF measurement (n = 57). In addition, ipsilateral CBF
monitoring was accomplished by placement of a sterilized
detector immediately adjacent to the margin of the resection (n
= 38).
[Help with image viewing] [Email Jumpstart To Image]
FIGURE 1. Depiction of CBF detector placement for “near”
detectors (those placed in the sterile field directly over the
cortex) and“distant” detectors (those placed adjacent to the
sterile field at the margin of the craniotomy). See text
for further explanation.
Intraoperative management and timing of measurements
Anesthetic management was a 0.75 to 0.9% isoflurane/60% N2O/O2
balanced technique, titrated to maintain patient blood
pressure within [approximately equal to]10% below ward values.
After placement of spinal drainage, patients were positioned
in rigid pin fixation. An operating microscope was used in all
patients. With dural exposure, a baseline CBF measurement
was obtained. The final CBF measurement took place after the AVM
was completely removed, during inspection of the surgical
bed for hemostasis.
Expired concentration of anesthetic was adjusted to identical
values for the pre- and postresection CBF measurements. After
the postresection CBF measurement, phenylephrine was generally
used to increase mean arterial pressure 20 to 30% to
further verify hemostasis. Thereafter, use of the isoflurane was
discontinued and, until 1988, propranolol and hydralazine
were used to control emergence and postoperative hypertension.
Esmolol and labetalol were used after this time to maintain
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (4 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00006123-199606000-00005|FF6A&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://www.ovid.com/site/help/documentation/ovidsp/en/imview.htmhttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Image%7c%26PAGE%3dimage%26IMAGE%3d00006123-199606000-00005%7cFF6A%26D%3dovft
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
the mean arterial pressure at approximately 10% below baseline
preoperative values.
When a suitable artery could be identified, the FMAP was
intraoperatively measured with the use of a 26-gauge needle
transduced with a strain gauge. Otherwise, the FMAP was examined
from the last embolization before surgery during which
pressure was measured using a 1.5-French superselective catheter
immediately before injection of N-butyl cyanoacrylate glue
(11).
Arterial CO2 pressure (PaCO2) management
In all patients, after the initial CBF measurement,
cerebrovascular reactivity to CO2 was individually established for
each
patient before resection by increasing PaCO2 by [approximately
equal to]10 mm Hg by adding CO2 to the fresh gas mixture or
by changing minute ventilation. During the first two-thirds of
the study, postexcision measurements were made at
relative hypocapnia and compared with the preresection
hypocapnic measurements. During the latter third of the
study, postexcision measurements were made at relative
normocapnia and compared with the preresection
normocapnic measurements(CO2 was added to the inspired gas
mixture before the final CBF measurement). During the
actual microsurgical resection, however, PaCO2 was managed at
the hypocapnic level in all patients.
CBF methodology
The CBF measurements were performed using a Cerebrograph 10a
(Novo Diagnostic Systems, Bagsvaerd, Denmark), as
previously described (36, 39, 40). The arterial input function
was estimated by a sampling of end-tidal gas from the
endotracheal tube. Because the purpose of this study was to
investigate hemispheric flow derangements that may occur
in anatomically normal vascular beds as a result of surgical
excision, detectors were placed to interrogate normal tissue in
the
same major arterial supply territory as the fistula. One
detector was placed 5 to 6 cm from the margin of the resection,
and
the other was placed in a contralateral homologous position.
In the last 38 patients, a sterilized detector was mounted in
the operative field over the cortex immediately adjacent to the
margin of the AVM in the same arterial supply (Fig. 1). CBF was
measured by the intravenous injection of [approximately equal
to]20 mCi xenon-133 in saline, and tracer washout was recorded
for 11 minutes. CBF data were analyzed by the M2 model
and expressed as the Initial Slope Index, in units of
milliliters per 100 grams per minute, assuming a combined tissue
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (5 of 24) [6/12/2008
5:47:41 PM]
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
partition coefficient of 1.0 (40).
Control group
A control group of 22 patients undergoing craniotomy for mass
lesions(tumors) was also studied. The anesthetic management
and the timing of the CBF measurements were the same. Vascular
pressures were not measured.
Correction factors for CBF
There were small changes in PaCO2 between the CBF measurements
and unavoidable increases in temperature and decreases
in hematocrit over the course of surgery. Such changes might
affect the interpretation of individual data, although group
data
can be analyzed by standard statistical techniques. Therefore,
to evaluate individual patients, we also examined corrected
CBF data (CBFcorrected). The observed CBF was “corrected” to
render the pre-excision CBF value more comparable to
the physiological conditions present at the postresection
measurement. The following corrections were used: 1)
individual preresection CO2 reactivity, calculated as the
absolute increase in CBF per mm Hg change in PaCO2, expressed
as
ml/100 g/min/mm Hg (if missing [n = 7], the group mean was
used), 2) 1% increase in CBF for each 0.1°C increase in
core temperature (37), and 3) 3% increase in CBF for each
percentage increase in hematocrit (12).
Comparisons were made with both uncorrected and corrected values
for absolute and percentage change between preresection
and postresection values. Because no significant difference was
found between the four ways of expressing CBF change,
most comparisons are given as only percent change in
CBFcorrected from baseline (%[DELTA]CBF), for the sake of clarity.
A
histogram of relative and percentage changes was visually
inspected to verify that values were normally distributed.
Definition of breakthrough complications
NPPB was defined as intraoperative brain swelling interfering
with the course of surgery, postoperative computed tomography
or magnetic resonance imaging evidence of brain swelling that
went beyond the immediate proximity of the surgical bed,
or postoperative ICH that could not be explained by other
causes. The assignment of NPPB was made by the senior
neurosurgeon (BMS) without knowledge of CBF results. In
addition, all cases of postoperative hemorrhage or swelling
that
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (6 of 24) [6/12/2008
5:47:41 PM]
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.occurred during the time period of the
study but were not included in the CBF protocol were reviewed.
Data analysis
Data are reported as mean ± standard deviation (SD) (except in
Fig. 2 for clarity, in which the standard error of the mean is
given). Continuous data were analyzed by repeated-measures
analysis of variance and linear regression or Spearman
rank correlation. Category data were analyzed by [chi]2 or
Fisher's exact test.
[Help with image viewing] [Email Jumpstart To Image]
FIGURE 2. Mean ± standard error of the mean changes in
uncorrected CBF from pre- to postresection in 95 patients
undergoing AVM resection under relative hypocapnia. Patients
with NPPB (n = 5) had a greater(P < 0.0001) increase in
CBF from pre- to postresection than did AVM patients without
NPPB (n = 90). Both NPPB(P < 0.001) and non-NPPB (P<
0.05) patients had a greater increase in CBF after resection
than did control patients (n = 22).
RESULTSIncidence of NPPB
During the entire study period, there were 260 operations
performed in 235 patients with AVMs. All cases of
postoperative hemorrhage or significant bilateral or
holohemispheric brain swelling in this period were reviewed and are
listed
in Table 1. There were six cases attributed to NPPB, for a total
incidence of 2.3% per surgery (or 2.6% per patient). As shown
in Table 1, two patients had immediate (
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
[Help with image viewing] [Email Jumpstart To Image]
TABLE 1. Postoperative Hemorrhage or Hemispheric Swelling in 260
Arteriovenous Malformation Operations in 235
Patientsa
There were also five hemorrhages that were not assigned to the
NPPB group. Two were caused by residual AVMs documented
by angiogram, one of which was fatal 3 days postoperatively.
There were two hemorrhages into the operative bed without
mass effect seen on routine postoperative computed tomographic
scans, which were not clinically significant. Finally, there
was one epidural hematoma.
Relationship of CBF changes to NPPB
CBF studies were performed during 152 operations in 143
patients. There were 125 patients with AVMs who had
single-stage
surgery and 18 who had two-stage surgery. Of the 18 patients
undergoing two stages, 9 patients underwent CBF monitoring
during both stages, 5 underwent it during the first surgery
only, and 4 underwent it during the second surgery only.
There were five patients with NPPB in the group that underwent
CBF monitoring (one patient with severe brain swelling in the
NPPB group did not have CBF measured). All NPPB complications
occurred during the first phase of the study when
CBF measurements were made at relative hypocapnia; preoperative
embolization was performed in 28% of patients in this group.
In the second half of the study, in which CBF was measured at
relative normocapnia, 76% had undergone preoperative
embolization.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (8 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00006123-199606000-00005|TT2B&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://www.ovid.com/site/help/documentation/ovidsp/en/imview.htmhttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Image%7c%26PAGE%3dimage%26IMAGE%3d00006123-199606000-00005%7cTT2B%26D%3dovft
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
There was no difference between changes in ipsilateral and
contralateral CBF. For the patients studied during relative
hypocapnia, the NPPB group had a greater increase in both global
CBF and CBFcorrected (P < 0.0001), as shown in Table 2 and
Figure 2. Figure 3 shows the%[DELTA]CBF from pre- to
postresection. CBF and physiological variables for the group
studied
during relative normocapnia are shown in Table 3. Other than
differences in PaCO2, there was no difference in
physiological variables between the patients studied during
relative hypocapnia and relative normocapnia. The
relative%[DELTA]
CBF from pre- to postresection was similar for both groups (18 ±
47 versus 16 ± 26%, P = 0.80). Therefore, the PaCO2 level did
not influence the magnitude of pre- to postresection CBF
increases. The%[DELTA]CBF in four patients with
postoperative hemorrhages not assigned to the NPPB was not
different(P > 0.8) from that of the other non-NPPB patients.
[Help with image viewing] [Email Jumpstart To Image]
TABLE 2. Cerebral Blood Flow and Associated Physiological
Variables Measured Pre- and Postresection at Relative
Hypocapnia (n = 95)a
[Help with image viewing] [Email Jumpstart To Image]
FIGURE 3. Individual values for%[DELTA]CBF (see text for
explanation) from pre- to postresection in 95 patients
undergoing AVM resection under relative hypocapnia. Values for
mean ± SD are also shown. Patients with NPPB had a
greater (
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
[Help with image viewing] [Email Jumpstart To Image]
TABLE 3. Cerebral Blood Flow and Associated Physiological
Variables Measured before and after Resection at
Relative Normocapnia (n = 57)a
In the relative hypocapnic group, global CO2 reactivity tended
to be slightly higher in the NPPB (n = 5) than in the non-NPPB (n
=
83) group (2.4± 0.9 versus 1.8 ± 0.8 ml/100 g/min/mm Hg, P =
0.12) but there was no difference between ipsilateral
and contralateral values. CO2 reactivity was not different
between the hypo- and normocapnic groups (1.8 ± 0.8 versus 2.0
±
1.4 ml/100 g/min/mm Hg).
In the cohort studied at relative normocapnia, both the percent
(14± 35%) and absolute (3 ± 10 ml/100 g/min) changes
in CBFcorrected were used to estimate the sensitivity of CBF
monitoring to detect NPPB. For the NPPB group, 60% (three of
five patients) had a >2 SD increase from pre- to
postresection for both percent and absolute CBF values. For the
non-NPPB
group, this was 4 and 7%, respectively, approximating the
expected values >2 SD in a normal distribution.
Influence of detector location on CBF results
There was no influence of detector location on CBF results. The
increase in CBF (P < 0.0001) from pre- to postresection was
similar whether the detector was adjacent to the AVM nidus or
mounted 5 to 6 cm distant. Values for ipsilateral and
contralateral CBF in both groups of patients are shown in Table
4.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (10 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00006123-199606000-00005|TT3&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://www.ovid.com/site/help/documentation/ovidsp/en/imview.htmhttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Image%7c%26PAGE%3dimage%26IMAGE%3d00006123-199606000-00005%7cTT3%26D%3dovft
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
[Help with image viewing] [Email Jumpstart To Image]
TABLE 4. Comparison of Detector Location on Cerebral Blood Flow
Changes in 57 Patients Studied During
Normocapniaa
Relationship of CBF changes to other clinical and physiological
variables
There was no relationship between CBF changes and size, feeding
artery, or number of embolizations. Patient age was 35 ±
11 years. There was, as might be expected, a weak inverse
correlation between age and preresection CBF(r = 0.24, P =
0.003). However, changes in CBF were not related to age. The
largest AVM diameter was 4.3 ± 1.8 cm, with no difference
between NPPB and non-NPPB groups. Primary location was in the
cerebral hemispheres in 139 (91%) patients, the basal
ganglia/diencephalon in 7 (5%), and the posterior fossa in 6
(4%). There was no influence of location on CBF changes.
Central venous and pulmonary artery pressures were measured in
83 patients. There was no relationship between CBF and
central filling pressures. There was a small increase (P <
0.0001) from pre- to postresection for both pulmonary artery
diastolic pressure (11 ± 4 to 12 ± 5 mm Hg) and central venous
pressure (7 ± 4 to 9 ± 4 mm Hg). Cardiac output was measured in
69 patients and tended to increase (P = 0.064) from pre- to
postresection (6.7 ± 1.7 to 7.1 ± 2.2 L/min). There was no
relationship to changes in CBF.
The change in CBF from pre- to postresection was not related to
the time elapsed from induction of anesthesia to the final
CBF measurement. Isoflurane-expired concentration did not change
(0.83 ± 0.20 versus 0.84 ± 0.17%), and small individual
changes had no relationship to changes in CBF.
Relationship of FMAP to CBF changes
The FMAP (44 ± 16 mm Hg) was 56% of the systemic arterial
pressure(78 ± 12 mm Hg, P < 0.0001) and was not related to%
[DELTA]CBF from pre- to postresection (y = 0.2x + 13, r = 0.07,
P= 0.57, n = 64), as shown in Figure 4. There was no
apparent influence of prior embolization on this relationship;
patients who had undergone prior embolization are indicated in
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (11 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00006123-199606000-00005|TT4&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://www.ovid.com/site/help/documentation/ovidsp/en/imview.htmhttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Image%7c%26PAGE%3dimage%26IMAGE%3d00006123-199606000-00005%7cTT4%26D%3dovft
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
Figure 4. When limited to the 20 FMAP measurements taken
intraoperatively immediately before the preresection CBF
measurement (at the same time under similar physiological
conditions), there was still no evidence for larger increases in
CBF to
be associated with low FMAP. Only one patient who developed NPPB
had FMAP measured.
[Help with image viewing] [Email Jumpstart To Image]
FIGURE 4. Individual values for%[DELTA]CBF from pre- to
post-resection in 64 patients who had FMAP measured during
craniotomy or during the last embolization session before
surgery. There was no relationship(y = 0.2x + 13, r = 0.07, P =
0.57). The findings were similar when patients were restricted
to only those who had FMAP measured during craniotomy.
Relationship of CBF changes to general neurological outcome
Excluding the cases of hemorrhage, there was no relationship
between changes in CBF and other neurological deficits.
Relationship of CBF changes in AVM patients to that in control
patients
CBF changes for the control group are shown in Table 2 and
Figure 2. Unlike the AVM group, there was no significant change
from pre- to postresection. Preresection CO2 reactivity in the
control group (1.6 ± 1.0 ml/100 g/min/mm Hg) was not different
from that in the AVM group. Compared with that in the AVM group,
the postresection CBF measurement was performed sooner (P
< 0.05) after the induction of anesthesia (6.0 ± 1.8 versus
7.4 ± 1.7 h). Systemic mean arterial pressure at the
postresection
CBF was higher(P < 0.05) in the control group (83 ± 12 versus
79± 11 mm Hg).
DISCUSSION
The primary focus of this study was to systemically delineate
the relationship of altered cerebral hemodynamics as a result
of arteriovenous shunt ablation on the pathophysiology of
certain postoperative complications. There are three main
findings.
First, patients who have complications, such as swelling or
hemorrhage attributable to NPPB, have greater increases in CBF
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (12 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?View+Image=00006123-199606000-00005|FF6D&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://www.ovid.com/site/help/documentation/ovidsp/en/imview.htmhttp://ovidsp.tx.ovid.com/spb/ovidweb.cgi?S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&Save+As+Jumpstart=Image%7c%26PAGE%3dimage%26IMAGE%3d00006123-199606000-00005%7cFF6D%26D%3dovft
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
after resection than those who do not display NPPB. These
changes, however, are global. Second, these CBF changes are not
related to the degree of hypotension caused by the shunt; that
is, there was no relationship to increases in CBF and
preresection FMAP. Third, the placement of CBF detectors,
whether immediately adjacent to or removed from the margin of
the nidus, influences neither the detection nor the degree of
hyperemia after resection.
Relationship of CBF and NPPB
This investigation confirms previous reports that NPPB is a
relatively rare occurrence, and studies to investigate its
pathophysiology are inherently limited by statistical power
issues. This study is the largest series to date to
investigate cerebrovascular phenomena related to NPPB.
There is a wide range of definitions given for NPPB
or“hyperemic” complications in the literature (2, 3, 4, 9, 15, 23,
25, 30,
35). This is an inherent problem in any study in which an
attempt is made to determine the pathophysiological conditions
that
are associated with NPPB. There is no universally acceptable way
to independently verify the existence of NPPB. We
have attempted to constrain our assignment of this syndrome to
patients in whom swelling and hemorrhage did not have
another proximate cause. As a practical matter, we emphasize
that the diagnosis of“hyperemic complications” should be
a diagnosis of exclusion only after all possible causes of
swelling or hemorrhage have been carefully considered. In our
series,
it may be that, for example, our patient with postoperative ICH,
without an angiogram or an autopsy, may have had a residual
AVM that was not identified during surgical re-exploration.
Therefore, our reported incidence of NPPB (2.3% per surgery)
may actually overestimate the true incidence.
Compared with control patients, patients with AVMs had a larger
increase in global CBF after resection, but the difference
was small. We used a series of correction factors for our CBF
values to ascertain whether decreases in hematocrit and
increases
in temperature introduced systematic error into our data. It
does not seem that increases seen after resection are
entirely attributable to these physiological factors.
NPPB-type complications are associated with a greater increase
in CBF than that which occurs in those patients who do not
have evidence of“hyperemic” complications. However, these
changes are not restricted to the brain sharing the same
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (13 of 24) [6/12/2008
5:47:41 PM]
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.circulatory bed as the AVM and are global
in nature. Despite the consistent presence of hyperemia after AVM
resection,
monitoring of xenon-133 CBF does not seem to have great
sensitivity(60%) to discriminate potential cases of NPPB.
All of our complications attributable to NPPB occurred in
patients in the first part of the series. PaCO2 management was
identical except for the brief period of CBF measurement.
Possible influences may have been the difference in agents used
for emergence and postoperative blood pressure control
(hydrazine and propranolol early, labetalol and esmolol later)
or improvements in techniques of preoperative endovascular
embolization.
Time effect of volatile anesthetics
Anesthetic agents influence CBF; some authors have described a
time effect of the volatile agents, such as isoflurane. In
several nonprimate animal models, volatile anesthetics induced
cerebral hyperemia, which resolved over time (1, 7, 8, 33, 34).
The mechanism was not related to O2 consumption (8) or pH
changes (34). In primates, an opposite effect was observed;
CBF progressively increased over time during isoflurane
anesthesia, and the increases were blocked by arginine analogs
(21), suggesting involvement of a nitric oxide pathway.
Such effects are controversial, however, because they could not
be demonstrated in at least one canine model (27) or in one of
our previous studies in humans undergoing craniotomy for tumor
resection (24). A time effect does not seem likely in the
present study. First, there was no increase in CBF over time in
the control group. In addition, the increase in CBF in AVM
patients from pre- to postresection was not related to the time
elapsed between induction of anesthesia to the final
postresection CBF measurement. Therefore, it is unlikely that
our observations in patients with AVMs were simply an artifact
of
the anesthetic technique.
Relationship between cerebral arterial pressure and CBF
changes
One of the main reasons for the current approach to staged
treatment of patients with AVMS (either by embolization or
staged surgery) is to prevent complications resulting from too
rapidly changing local cerebral hemodynamics after interruption
of the AVM shunt. This notion is largely based on the assumption
that restoration of normal perfusion pressure to
previously hypotensive brain regions will overwhelm local
autoregulatory capacity and result in hyperperfusion injury
(31).
There are two observations in the present series that argue
against such a mechanism. First, there was no relationship between
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (14 of 24) [6/12/2008
5:47:41 PM]
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
CBF changes after resection and preresection FMAP. If CBF
changes were uniquely caused by reperfusion in a paralyzed
vascular bed, the beds with the greatest CBF changes would be
expected to have the lowest pretreatment perfusion pressure;
this was not the case. Second, the CBF changes were global, even
in patients who developed NPPB. We have recently
presented further arguments against loss or autoregulatory
capacity in regions adjacent to AVMs; even severe hypotension
in apparently eloquent brain regions does not necessarily result
in loss of autoregulatory vasoconstriction (38).
Our data do not exclude, however, the possibility that there is
some“microenvironment” immediately adjacent to the nidus
that may be affected by local hemodynamic changes after
treatment. Cortical areas adjacent to AVMs may be unable to
dilate
to reductions in local perfusion pressure, as assessed in a
previous study using acetazolamide-enhanced single photon
emission tomography (13) (these adjacent regions generally
retained intact autoregulatory vasoconstriction to blood
pressure increases with phenylephrine). In the present study,
however, the possibility of severe local CBF changes in our
cohort studied with a detector 5 to 6 cm distant from the edge
of the nidus cannot be absolutely ruled out. The cohort in
which
a detector was placed immediately adjacent to the AVM displayed
global hyperemia after resection, but none of this
group developed NPPB. We emphasize that the highly localized
hyperemia that our detectors may have missed cannot
explain hemispheric swelling.
Possible mechanisms for postoperative CBF changes
Besides the NPPB theory, other alternative mechanisms for
swelling or hemorrhage after treatment include reversal of
decreased pulsatility (10, 16, 17), venous hypertension (2), and
technical complications of surgery (14, 26, 32). Another
mechanism is related to autonomic perivascular innervation,
which can profoundly influence CBF in various
pathophysiological states (18, 19). A derangement in autonomic
perivascular innervation to normal circulatory beds in AVM
patients in compatible with certain paradoxical CBF responses in
AVM patients to pharmacological challenges (6, 36, 39).
For example, Batjer (5) argues that post-treatment hyperemia is
caused by a deranged vascular bed that actively participates
in swelling and not simply by passive behavior of a paralyzed
vascular bed. Although feeding vessels themselves seem to be
devoid of all autonomic or peptidergic innervation (20, 22),
local changes in peptidergic activity in adjacent circulatory
regions
may somehow affect distant beds by collateral innervation. Such
a mechanism might explain why there seem to be global
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (15 of 24) [6/12/2008
5:47:41 PM]
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
increases in CBF after many cases of AVM resection, which cannot
be explained by local changes in perfusion pressure.
Global changes are also seen after carotid endarterectomy (28,
29), another instance in which repressurization of a
previously hypotensive vascular territory should, intuitively,
lead to regional rather than global changes in perfusion.
CONCLUSION
This study does not support a uniquely hemodynamic mechanism
that explains cerebral hyperemia as a consequence
of repressurization in hypotensive vascular beds. Further
efforts should be aimed at elucidating a mechanism that can
explain global changes in CBF after treatment.
ACKNOWLEDGMENTS
This work was supported by National Institutes of Health Grant
RO1-NS27713. We thank Joyce Ouchi and Steven Marshall, B.S.,
for assistance in preparation of the manuscript and Dennis Lu,
M.S., and the Neuroradiology technologist staff for expert
technical assistance. We gratefully acknowledge the support and
contributions of the other members of the Columbia
University AVM Study Project.
REFERENCES
1. Albrecht RF, Miletich DJ, Madala LR: Normalization of
cerebral blood flow during prolonged halothane anesthesia.
Anesthesiology 58:26-31, 1983. Ovid Full Text
ExternalResolverBasic Bibliographic Links [Context Link]
2. Al-Rodhan NRF, Sundt TM Jr, Piepgras DG, Nichols DA,
Rufenacht D, Stevens LN: Occlusive hyperemia: A theory for
the hemodynamic complications following resection of
intracerebral arteriovenous malformations. J Neurosurg
78:167-175,
1993. ExternalResolverBasic Bibliographic Links [Context
Link]
3. Awad IA, Magdinec M, Schubert A: Intracranial hypertension
after resection of cerebral arteriovenous
malformations: Predisposing factors and management strategy.
Stroke 25:611-620, 1994. Ovid Full Text
ExternalResolverBasic Bibliographic Links [Context Link]
4. Barnett GH, Little JR, Ebrahim ZY, Jones SC, Friel HT:
Cerebral circulation during arteriovenous malformation
operation.Neurosurgery 20:836-842, 1987. ExternalResolverBasic
Bibliographic Links [Context Link]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (16 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1983_58_26_albrecht_normalization_%7c00006123-199606000-00005%23xpointer%28id%28R1-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00000542-198301000-00005&P=81&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1983_58_26_albrecht_normalization_%7c00006123-199606000-00005%23xpointer%28id%28R1-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00000542-198301000-00005&P=81&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1983_58_26_albrecht_normalization_%7c00006123-199606000-00005%23xpointer%28id%28R1-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00000542-198301000-00005&P=81&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1993_78_167_rodhan_complications_%7c00006123-199606000-00005%23xpointer%28id%28R2-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=82&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1993_78_167_rodhan_complications_%7c00006123-199606000-00005%23xpointer%28id%28R2-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=82&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00007670_1994_25_611_awad_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R3-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00007670-199403000-00012&P=83&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00007670_1994_25_611_awad_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R3-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00007670-199403000-00012&P=83&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00007670_1994_25_611_awad_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R3-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00007670-199403000-00012&P=83&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1987_20_836_barnett_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R4-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=84&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1987_20_836_barnett_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R4-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=84&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
5. Batjer HH: Evidence for adaptive autoregulatory displacement
in hypotensive cortical territories adjacent to
arteriovenous malformations. Neurosurgery 34:610, 1994
(comment). [Context Link]
6. Batjer HH, Devous MD Sr: The use of acetazolamide-enhanced
regional cerebral blood flow measurement to predict risk
to arteriovenous malformation patients. Neurosurgery 31:213-218,
1992. Ovid Full Text ExternalResolverBasic Bibliographic
Links [Context Link]
7. Boarini DJ, Kassell NF, Coester HC, Butler M, Sokoll MD:
Comparison of systemic and cerebrovascular effects of
isoflurane
and halothane. Neurosurgery 15:400-409, 1984.
ExternalResolverBasic Bibliographic Links [Context Link]
8. Brian JE Jr, Traystman RJ, McPherson RW: Changes in cerebral
blood flow over time during isoflurane anesthesia in dogs.
J Neurosurg Anesth 2:122-130, 1990. [Context Link]
9. Drake CG: Cerebral arteriovenous malformations:
Considerations for and experience with surgical treatment in 166
cases.
Clin Neurosurg 26:145-208, 1979. ExternalResolverBasic
Bibliographic Links [Context Link]
10. Duckwiler G, Dion J, Viñuela F, Jabour B, Martin N, Bentson
J: Intravascular microcatheter pressure monitoring:
Experimental results and early clinical evaluation. AJNR Am J
Neuroradiol 11:169-175, 1990. ExternalResolverBasic
Bibliographic Links [Context Link]
11. Fleischer LH, Young WL, Pile-Spellman J, terPenning B, Kader
A, Stein BM, Mohr JP: Relationship of transcranial Doppler
flow velocities and arteriovenous malformation feeding artery
pressures.Stroke 24:1897-1902, 1993. [Context Link]
12. Gaehtgens P, Marx P: Hemorheological aspects of the
pathophysiology of cerebral ischemia. J Cereb Blood Flow Metab
7:259-265, 1987. ExternalResolverBasic Bibliographic Links
[Context Link]
13. Hacein-Bey L, Nour R, Pile-Spellman J, Van Heertum R, Esser
PD, Young WL: Adaptive changes in autoregulation to
chronic cerebral hypotension with arteriovenous malformations:
An acetazolamide-enhanced single-photon emission CT study.
AJNR Am J Neuroradiol (in press). [Context Link]
14. Hassler W: Hemodynamic Aspects of Cerebral Angiomas. Vienna,
Springer-Verlag, 1986. [Context Link]
15. Heros RC, Korosue K, Diebold PM: Surgical excision of
cerebral arteriovenous malformations: Late results.
Neurosurgery
26:570-578, 1990. ExternalResolverBasic Bibliographic Links
[Context Link]
16. Jungreis CA, Horton JA, Hecht ST: Blood pressure changes in
feeders to cerebral arteriovenous malformations during
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (17 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1992_31_213_batjer_acetazolamide_%7c00006123-199606000-00005%23xpointer%28id%28R6-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00006123-199208000-00006&P=86&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1992_31_213_batjer_acetazolamide_%7c00006123-199606000-00005%23xpointer%28id%28R6-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00006123-199208000-00006&P=86&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1992_31_213_batjer_acetazolamide_%7c00006123-199606000-00005%23xpointer%28id%28R6-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00006123-199208000-00006&P=86&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1992_31_213_batjer_acetazolamide_%7c00006123-199606000-00005%23xpointer%28id%28R6-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00006123-199208000-00006&P=86&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1984_15_400_boarini_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R7-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=87&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1984_15_400_boarini_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R7-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=87&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00003073_1979_26_145_drake_considerations_%7c00006123-199606000-00005%23xpointer%28id%28R9-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=89&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00003073_1979_26_145_drake_considerations_%7c00006123-199606000-00005%23xpointer%28id%28R9-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=89&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000388_1990_11_169_duckwiler_intravascular_%7c00006123-199606000-00005%23xpointer%28id%28R10-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=90&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000388_1990_11_169_duckwiler_intravascular_%7c00006123-199606000-00005%23xpointer%28id%28R10-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=90&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00004647_1987_7_259_gaehtgens_hemorheological_%7c00006123-199606000-00005%23xpointer%28id%28R12-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=92&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00004647_1987_7_259_gaehtgens_hemorheological_%7c00006123-199606000-00005%23xpointer%28id%28R12-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=92&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_26_570_heros_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R15-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=95&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_26_570_heros_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R15-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=95&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
therapeutic embolization. AJNR Am J Neuroradiol 10:575-578,
1989. ExternalResolverBasic Bibliographic Links [Context Link]
17. Lindegaard K-F, Grolimund P, Aaslid R, Nornes H: Evaluation
of cerebral AVMs using transcranial Doppler ultrasound.
J Neurosurg 65:335-344, 1986. ExternalResolverBasic
Bibliographic Links [Context Link]
18. Macfarlane R, Moskowitz MA, Sakas DE, Tasdemiroglu E, Wei
EP, Kontos HA: The role of neuroeffector mechanisms in
cerebral hyperperfusion syndromes. J Neurosurg 75:845-855, 1991.
[Context Link]
19. Macfarlane R, Tasdemiroglu E, Moskowitz MA, Uemura Y, Wei
EP, Kontos HA: Chronic trigeminal ganglionectomy or
topical capsaicin application to pial vessels attenuates
postocclusive cortical hyperemia but does not influence
postischemic hypoperfusion. J Cereb Blood Flow Metab 11:261-271,
1991. ExternalResolverBasic Bibliographic Links [Context Link]
20. Maynard KI, Ogilvy CS: Patterns of peptide-containing
perivascular nerves in the circle of Willis: Their absence in
intracranial arteriovenous malformations. J Neurosurg
82:829-833, 1995. ExternalResolverBasic Bibliographic Links
[Context Link]
21. McPherson RW, Kirsch JR, Tobin JR, Ghaly RF, Traystman RJ:
Cerebral blood flow in primates is increased by isoflurane
over time and is decreased by nitric oxide synthase inhibition.
Anesthesiology 80:1320-1327, 1994. Ovid Full
Text ExternalResolverBasic Bibliographic Links [Context
Link]
22. Muraszko K, Wang HH, Pelton G, Stein BM: A study of the
reactivity of feeding vessels to arteriovenous
malformations: Correlation with clinical outcome. Neurosurgery
26:190-200, 1990. ExternalResolverBasic Bibliographic
Links [Context Link]
23. Nornes H, Grip A: Hemodynamic aspects of cerebral
arteriovenous malformations. J Neurosurg 53:456-464,
1980. ExternalResolverBasic Bibliographic Links [Context
Link]
24. Ornstein E, Young WL, Fleischer LH, Ostapkovich N:
Desflurane and isoflurane have similar effects on cerebral blood
flow
in patients with intracranial mass lesions. Anesthesiology
79:498-502, 1993. [Context Link]
25. Pasqualin A, Scienza R, Cioffi F, Barone G, Benati A,
Beltramello A, Da Pian R: Treatment of cerebral
arteriovenous malformations with a combination of preoperative
embolization and surgery.Neurosurgery 29:358-368,
1991. ExternalResolverBasic Bibliographic Links [Context
Link]
26. Peerless SJ: Successful treatment of the normal perfusion
pressure breakthrough syndrome. Neurosurgery 11:629-630,
1982 (comment). [Context Link]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (18 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000388_1989_10_575_jungreis_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R16-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=96&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000388_1989_10_575_jungreis_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R16-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=96&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1986_65_335_lindegaard_transcranial_%7c00006123-199606000-00005%23xpointer%28id%28R17-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=97&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1986_65_335_lindegaard_transcranial_%7c00006123-199606000-00005%23xpointer%28id%28R17-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=97&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00004647_1991_11_261_macfarlane_ganglionectomy_%7c00006123-199606000-00005%23xpointer%28id%28R19-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=99&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00004647_1991_11_261_macfarlane_ganglionectomy_%7c00006123-199606000-00005%23xpointer%28id%28R19-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=99&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1995_82_829_maynard_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R20-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=100&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1995_82_829_maynard_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R20-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=100&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1994_80_1320_mcpherson_isoflurane_%7c00006123-199606000-00005%23xpointer%28id%28R21-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00000542-199406000-00020&P=101&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1994_80_1320_mcpherson_isoflurane_%7c00006123-199606000-00005%23xpointer%28id%28R21-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00000542-199406000-00020&P=101&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1994_80_1320_mcpherson_isoflurane_%7c00006123-199606000-00005%23xpointer%28id%28R21-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00000542-199406000-00020&P=101&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1994_80_1320_mcpherson_isoflurane_%7c00006123-199606000-00005%23xpointer%28id%28R21-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00000542-199406000-00020&P=101&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_26_190_muraszko_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R22-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=102&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_26_190_muraszko_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R22-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=102&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_26_190_muraszko_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R22-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=102&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1980_53_456_nornes_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R23-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=103&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1980_53_456_nornes_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R23-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=103&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1991_29_358_pasqualin_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R25-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=105&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1991_29_358_pasqualin_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R25-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=105&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
27. Roald OK, Forsman M, Steen PA: The effects of prolonged
isoflurane anaesthesia on cerebral blood flow and metabolism in
the dog.Acta Anaesthesiol Scand 33:210-213, 1989.
ExternalResolverBasic Bibliographic Links [Context Link]
28. Schroeder T, Holstein PE, Engell HC: Hyperperfusion
following endarterectomy. Stroke 15:758, 1984 (letter). [Context
Link]
29. Schroeder T, Sillesen H, Sorensen O, Engell HC: Cerebral
hyperperfusion following carotid endarterectomy. J Neurosurg
66:824-829, 1987. ExternalResolverBasic Bibliographic Links
[Context Link]
30. Spetzler RF, Martin NA, Carter LP, Flom RA, Raudzens PA,
Wilkinson E: Surgical management of large AVMs by
staged embolization and operative excision. J Neurosurg
67:17-28, 1987. ExternalResolverBasic Bibliographic Links [Context
Link]
31. Spetzler RF, Wilson CB, Weinstein P, Mehdorn M, Townsend J,
Telles D: Normal perfusion pressure breakthrough theory.
Clin Neurosurg 25:651-672, 1978. ExternalResolverBasic
Bibliographic Links [Context Link]
32. Stein BM, Wolpert SM: Arteriovenous malformations of the
brain: I-Current concepts and treatment. Arch Neurol 37:1-5,
1980. ExternalResolverBasic Bibliographic Links [Context
Link]
33. Turner DM, Kassell NF, Sasaki T, Comair YG, Boarini DJ, Beck
DO: Time-dependent changes in cerebral and
cardiovascular parameters in isoflurane-nitrous
oxide-anesthetized dogs. Neurosurgery 14:135-141, 1984.
ExternalResolverBasic Bibliographic Links [Context Link]
34. Warner DS, Boarini DJ, Kassell NF: Cerebrovascular adaption
to prolonged halothane anesthesia is not related to
cerebrospinal fluid pH. Anesthesiology 63:243-248, 1985. Ovid
Full Text ExternalResolverBasic Bibliographic Links [Context
Link]
35. Wilson CB, Spetzler RF: Factors responsible for improved
results in the surgical management of intracranial aneurysms
and vascular malformations. Am J Surg 134:33-38, 1977.
ExternalResolverBasic Bibliographic Links [Context Link]
36. Young WL, Kader A, Prohovnik I, Ornstein E, Fleischer LH,
Ostapkovich N, Jackson LD, Stein BM: Pressure autoregulation is
intact after arteriovenous malformation resection. Neurosurgery
32:491-497, 1993. Ovid Full Text
ExternalResolverBasic Bibliographic Links [Context Link]
37. Young WL, Ornstein E: Cerebral and spinal cord blood flow,
in Cottrell JE, Smith DS (eds): Anesthesia and Neurosurgery.
St. Louis, Mosby Year Book, 1994, ed 3, pp 17-57. [Context
Link]
38. Young WL, Pile-Spellman J, Prohovnik I, Kader A, Stein BM,
Columbia University AVM Study Project: Evidence for
adaptive autoregulatory displacement in hypotensive cortical
territories adjacent to arteriovenous malformations.
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (19 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000013_1989_33_210_roald_anaesthesia_%7c00006123-199606000-00005%23xpointer%28id%28R27-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=107&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000013_1989_33_210_roald_anaesthesia_%7c00006123-199606000-00005%23xpointer%28id%28R27-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=107&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1987_66_824_schroeder_hyperperfusion_%7c00006123-199606000-00005%23xpointer%28id%28R29-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=109&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1987_66_824_schroeder_hyperperfusion_%7c00006123-199606000-00005%23xpointer%28id%28R29-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=109&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1987_67_17_spetzler_embolization_%7c00006123-199606000-00005%23xpointer%28id%28R30-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=110&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00005088_1987_67_17_spetzler_embolization_%7c00006123-199606000-00005%23xpointer%28id%28R30-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=110&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00003073_1978_25_651_spetzler_breakthrough_%7c00006123-199606000-00005%23xpointer%28id%28R31-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=111&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00003073_1978_25_651_spetzler_breakthrough_%7c00006123-199606000-00005%23xpointer%28id%28R31-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=111&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000816_1980_37_1_stein_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R32-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=112&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000816_1980_37_1_stein_arteriovenous_%7c00006123-199606000-00005%23xpointer%28id%28R32-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=112&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1984_14_135_turner_cardiovascular_%7c00006123-199606000-00005%23xpointer%28id%28R33-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=113&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1984_14_135_turner_cardiovascular_%7c00006123-199606000-00005%23xpointer%28id%28R33-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=113&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1985_63_243_warner_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R34-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00000542-198509000-00001&P=114&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1985_63_243_warner_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R34-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00000542-198509000-00001&P=114&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000542_1985_63_243_warner_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R34-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00000542-198509000-00001&P=114&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000479_1977_134_33_wilson_malformations_%7c00006123-199606000-00005%23xpointer%28id%28R35-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=115&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00000479_1977_134_33_wilson_malformations_%7c00006123-199606000-00005%23xpointer%28id%28R35-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=115&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1993_32_491_young_autoregulation_%7c00006123-199606000-00005%23xpointer%28id%28R36-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00006123-199304000-00001&P=116&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1993_32_491_young_autoregulation_%7c00006123-199606000-00005%23xpointer%28id%28R36-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00006123-199304000-00001&P=116&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1993_32_491_young_autoregulation_%7c00006123-199606000-00005%23xpointer%28id%28R36-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00006123-199304000-00001&P=116&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005
-
Ovid: Cerebral Hyperemia after Arteriovenous Malformation
Resection Is Related to"Breakthrough" Complications but Not to
Feeding Artery Pressure.
Neurosurgery 34:601-611, 1994. Ovid Full Text
ExternalResolverBasic Bibliographic Links [Context Link]
39. Young WL, Prohovnik I, Ornstein E, Ostapkovich N, Sisti MB,
Solomon RA, Stein BM: The effect of arteriovenous
malformation resection on cerebrovascular reactivity to carbon
dioxide. Neurosurgery 27:257-267, 1990.
ExternalResolverBasic Bibliographic Links [Context Link]
40. Young WL, Prohovnik I, Schroeder T, Correll JW, Ostapkovich
N: Intraoperative 133Xe cerebral blood flow measurements
by intravenous versus intracarotid methods. Anesthesiology
73:637-643, 1990. Ovid Full Text ExternalResolverBasic
Bibliographic Links [Context Link]
1. Takayasu M, Dacey RG Jr: Spontaneous tone of cerebral
parenchymal arterioles: A role in cerebral hyperemic phenomena.
J Neurosurg 71:711-717, 1989. ExternalResolverBasic
Bibliographic Links [Context Link]
APPENDIX
The following members of the Columbia University Arteriovenous
Malformation Study Project also contributed to this work:
Andrei Osipov, M.D.; Tara Jackson, B.S.; LaSandra Jackson, B.S.;
Lofti Hacein-Bey, M.D.; Robert R. Sciacca, Eng.Sc.D.; J.P.
Mohr,
M.D.; Isak Prohovnik, Ph.D.; Lauren H. Fleischer, M.D.; Michael
B. Sisti, M.D.; Robert A. Solomon, M.D.
COMMENTS
In this article, Young et al. make another very significant
contribution to our understanding of the hemodynamics of
cerebral arteriovenous malformations(AVMs) as part of their
large experience in the Columbia University AVM Study Project.
They have measured cerebral blood flows (CBFs) and feeding
cerebral artery pressures in 152 operative procedures for
patients
with cerebral AVMs. They have demonstrated a significant
increase in global CBF in the small number of patients who go
on
to develop normal perfusion pressure breakthrough(NPPB). The CBF
changes were similar both ipsilateral and contralateral to
the AVM resection. The authors were unable to correlate feeding
mean arterial pressure, however, with the propensity of
patients to develop NPPB. These findings call into question the
hypothesis that chronic low perfusion pressures in the
feeding arteries of cerebral AVMs are the sole explanation for
this type of cerebral hyperemic phenomenon (1). The authors do
not propose a significant alternative hypothesis.
As the authors indicate, they have made some significant changes
in their experimental paradigm since the initiation of
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi (20 of 24) [6/12/2008
5:47:41 PM]
http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1994_34_601_young_autoregulatory_%7c00006123-199606000-00005%23xpointer%28id%28R38-5%29%29%7c10%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.5c103e04ef61e5550ce593f7adca05af0334ad3d6d38a1f400230673b342cfb54bea84c4ae6dba622ed2fc4eb4096d3967.gif%7covftdb%7c00006123-199404000-00006&P=118&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1994_34_601_young_autoregulatory_%7c00006123-199606000-00005%23xpointer%28id%28R38-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c00006123-199404000-00006&P=118&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1994_34_601_young_autoregulatory_%7c00006123-199606000-00005%23xpointer%28id%28R38-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c00006123-199404000-00006&P=118&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_27_257_young_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R39-5%29%29%7c1106020%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.ccd906fbb0d5d1e2fe78c9d6280c7073981935f350d8b92c099d1cc211dbeb2c9b2959687d4195ddbb79cfd01aac3819062b6ab2eca5625cd4b479336bb9254ca05849ce6cd91a958d.gif%7covftdb%7c&P=119&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-199606000-00005http://ovidsp.tx.ovid.com/spb/ovidweb.cgi?Link+Set+Ref=00006123-199606000-00005|00006123_1990_27_257_young_cerebrovascular_%7c00006123-199606000-00005%23xpointer%28id%28R39-5%29%29%7c60%7chttp%3a%2f%2facs.tx.ovid.com%2facs%2f.14038a58de48ffa86f4ee5c84b99ffb3634b4b40918581081964493cf03a9948ecbddf0655fc0acf8b.gif%7covftdb%7c&P=119&S=EAJDFPODPEDDOKFDMCHLGBOKNPPPAA00&WebLinkReturn=Full+Text%3dL%7cS.sh.15.16.42.46%7c0%7c00006123-19960