Embed Size (px)
Citation preview

Overview of Hemodialysis Patients in Indonesia
Aida Lydia , MD, PhD
Indonesian Society of Nephrology
Division of Nephrology and Hypertension, Department of Internal Medicine
Faculty of Medicine, Universitas Indonesia
Dr. Cipto Mangunkusumo Hospital, Jakarta

17.000 islands
6000 islands inhabitated
Population 260 million
INDONESIA
With this characteristics, we face challenging situations to develop an affordable and equitable
access to kidney care
Indonesian Renal Registry, 2017
2

The Incidence and Prevalence of CKD
Based on the 2018 National Data from MoH in Indonesia
- CKD: 0.38% (CKD-EPI)
The representative data from population based study included
12,000 subjects in 2006 found the prevalence of CKD was 12.5 %
Based on current IRR data it was estimated that the incidence of
ESRD 161 pmp and the prevalence around 452 pmp.
45%
25%
8%
7%
7%
4%1%1% 1% 1%
HypertensionDiabetic nephropathyPrimary GlomerulopathyChronic PyelonephritisOthersObstructive nephropathyLupus nephropathyPolycystic kidney diseaseUric acid nephropathy
Prevalence of Hypertension
Prevalence of DM
Prevalence of Obesity
Prevalence of Smoking
34.1 % 10.9 % 21.8 % 28.8 %
3National Basic Health Research, MoH 2018. NEPHROLOGY 2006; 14, 669–674. Estimated from Indonesian Renal Registry 2016.
General Population
6

Indonesian Renal registry (IRR)
Data Collecting
• Almost all of data presented here based on our data from IRR
• Indonesian Society of Nephrology initiated the development and continuing activity of IRR
• The data are collected 6 monthly by uploading data from renal unit that have already signed up to the IRR website.
Barriers and Solutions
We have 866 registered dialysis unit, 655 unit among them 75.6% submitted regular data to IRR.
InaSN has collaboration with MOH in developing Standard Regulation of Dialysis Care
Uploading data to IRR become one of the condition to have or to prolong the license of running dialysisservice
5

Renal Replacement Therapy
HemodialysisPeritoneal Dialysis
KidneyTransplantation

INDONESIAN
RENAL REGISTRYPROPORTION CAPD AND HD
PATIENTS IN 2017
ACTIVE PATIENT
CAPD: 2%
Renal Replacement Therapy in Indonesia:• Mostly Hemodialysis• Small number Transplantation
We have very limited living donor• Small number Peritoneal Dialysis

Number of New and Active Hemodialysis Patients 2007- 2017
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
New Patient 4977 5392 8193 9649 15353 19621 15128 17193 21050 25446 30831
Active Patient 1885 6543 8603 11484 17259 22140 21759 21165 30554 52835 77892
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
M: 56%F: 44%
1 - 14 15 - 24 25 - 34 35 - 44 45 - 54 55 - 64 ≥ 65
New Patient 0.32% 2.20% 6.56% 14.23% 29.57% 30.45% 16.14%
Active Patient on 31 Dec 0.38% 2.26% 7.67% 16.67% 30.56% 28.57% 13.20%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
Age
Hemodialysis Patients: Age Distribution
Indonesian Renal Registry 20177
7
CVD
10 year of our National DataHD patients keep increasing in number
Mostly Male, the highest number of age group was between 45-64 yr old which actually still productive age.

FINANCIAL BURDEN OF KIDNEY DISEASE
CATASTROPHIC ILLNESS
COST (USD)
2016 2017 2018
CVD 529,486,121 648,097,397 736,720,179
CANCER 182,716,497 222,188,135 237,988,981
STROKE 99,926,171 152,840,665 179,230,864
KIDNEY DISEASE 243,556,653 163,431,676 167,319,732
THALASSAEMIA 34,683,846 37,232,370 34,306,944
HAEMOPHILIA 8,973,699 18,046,676 25,016,353
HEPATIC CIRRHOSIS 18,975,051 22,339,530 23,350,065
LEUKIMIA 14,802,399 22,803,637 23,282,671
TOTAL 1,133,120,437 1,286,980,086 1,427,215,789
National Health Insurancestarted in 2014 covered kidney health
services, including Dialysis and Transplantation
88%
3%9% National Health
Insurance
Private Insurance
Private
HD: The proportion of Public and Private Funding
CKD in Indonesia is one of Catastrophic Illness that spent very high budget of NHI after CVD, Cancer and Stroke. Funds issued in 2018 for kidney disease is more than 167 million USD.
National Health Insurance, 2018
4
88 % of HD patients covered by NHI
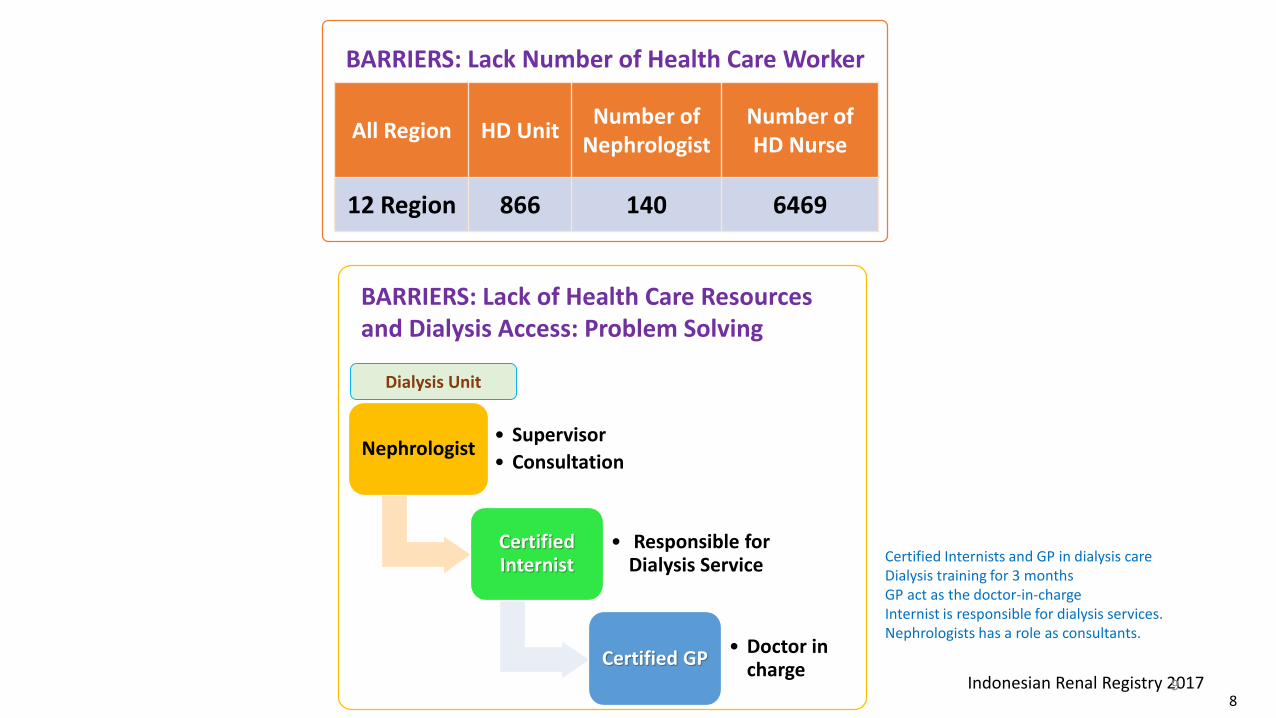
All Region HD UnitNumber of
NephrologistNumber of HD Nurse
12 Region 866 140 6469
BARRIERS: Lack Number of Health Care Worker
Nephrologist• Supervisor
• Consultation
Certified Internist
• Responsible for Dialysis Service
Certified GP• Doctor in
charge
BARRIERS: Lack of Health Care Resources and Dialysis Access: Problem Solving
Dialysis Unit
Indonesian Renal Registry 201798
Certified Internists and GP in dialysis careDialysis training for 3 months GP act as the doctor-in-charge Internist is responsible for dialysis services. Nephrologists has a role as consultants.

When To Iniatiate Dialysis in CKD?
• Patients with eGFR <5 mL/min/1.73 m2 regardless of the absence or presence of ESRD-related signs or symptoms → Initiate dialysis.
• For eGFR > 5- 15 mL/min/1.73 m2 depend on uremia related sign and symptom.
• The severity of symptoms varies substantially among patients.
• Younger patients and patients without other comorbid conditions tend to tolerate lower eGFR levels without developing many symptoms.
Cooper BA. N Engl J Med 2010

Intractable volume overload/and or
hypertension
Hyperkalemiarefractory to diet
restriction and treatment
Metabolic acidosis refractory to bicarbonate treatment
Hyperphosphatemia refractory to diet
and medical treatment
Anemia refractory to iron and
Erythropoietin treatment
Unexplain decline in functioning and well
being
Nausea, vomiting and weight loss
When To Iniatiate Dialysis in CKD?
Prompt Initiation
Singh A. Hand book of Dialysis. 2015

When To Iniatiate Dialysis in CKD?
Urgent Initiation
Neurologic Dysfunction
• Encephalopathy
• Seizures
Pleuritis or Pericarditis
• Related to uremia
Bleeding diathesis
• GI bleeding
• Prolonged bleeding time
Respiratory Failure
Singh A. Hand book of Dialysis. 2015
Lung edema
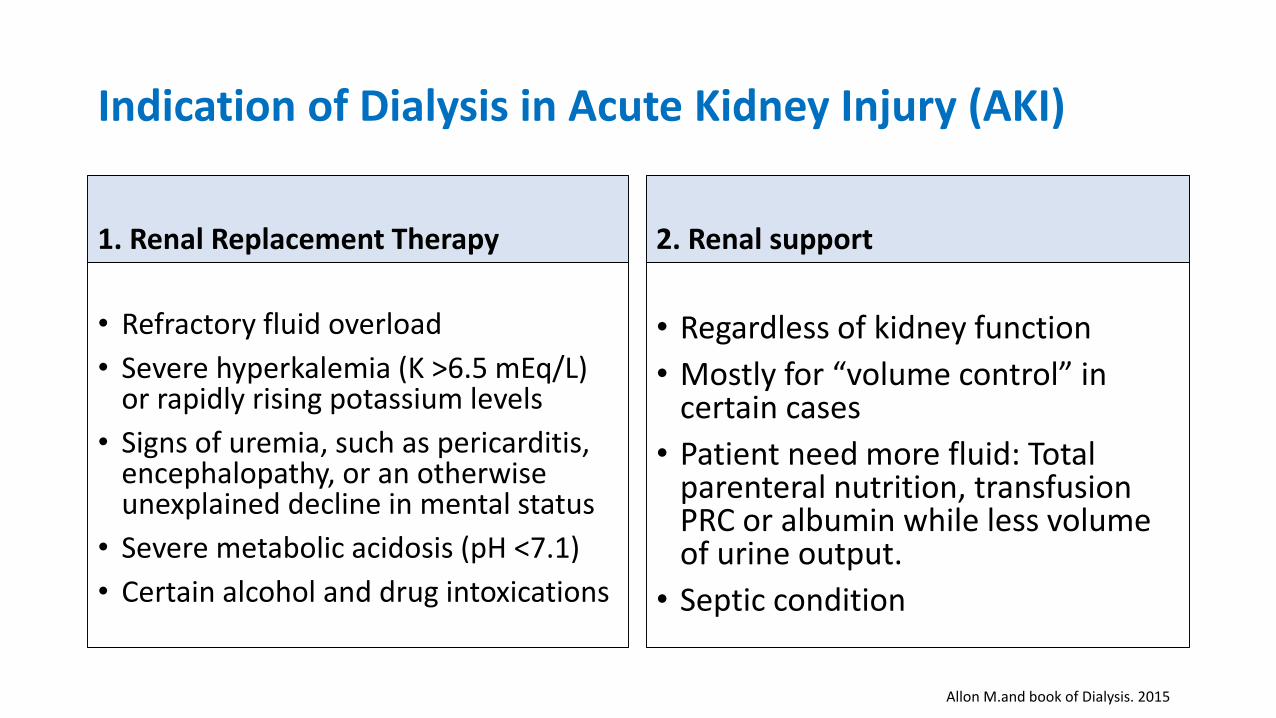
Indication of Dialysis in Acute Kidney Injury (AKI)
1. Renal Replacement Therapy
• Refractory fluid overload
• Severe hyperkalemia (K >6.5 mEq/L) or rapidly rising potassium levels
• Signs of uremia, such as pericarditis, encephalopathy, or an otherwise unexplained decline in mental status
• Severe metabolic acidosis (pH <7.1)
• Certain alcohol and drug intoxications
2. Renal support
• Regardless of kidney function
• Mostly for “volume control” in certain cases
• Patient need more fluid: Total parenteral nutrition, transfusion PRC or albumin while less volume of urine output.
• Septic condition
Allon M.and book of Dialysis. 2015

Implication in Clinical Practice
• There is a need to focus on regular symptom assessment as
part of CKD review in those with lower eGFR values.
• Individual assessment for non-medical issues dictate specific timing of therapies: • Patient’s readiness (mentally, financially)
• Availability of resources (RRT modalities available)
KDIGO 2012

Preparation for Renal Replacement Therapy (RRT)
• Patient education: start if eGFR < 30ml/m/1.73m2
• Inform the benefit and risk among 3 modalities of RRT (HD, CAPD, Transplantation
• KDOQI Guideline: AVF is vascular access of choice for HD
• For those choosing Hemodialysis, AV Fistula should be place 3-6 months prior to HD initiation.
• Indonesia: - Problem of late referral
- Majority of patients need dialysis catheter at initiation of dialysis.
KDOQI 2015

Selected factors Favoring Temporary Catheter Insertion Sites
1. Right internal jugular
Venous pathway to the right atrium is short and straight.
2. Femoral
3. Left internal jugular
- If contraindication to R-internal jugular and femoral site
4. Subclavian- Contra indication to internal jugular
- Prefer to use R-subclavian vein
KDOQI 2015

SClav6%
AVF 75%
Jug 6%
Vascular Access: IRR 2017
• Dialysis Catheter can be inserted by:
• Surgeon • Nephrologist• Intensivist
At initiation of dialysis:Around 80% using dialysis catheter

One study in US published in KI showed that ‘ The adjusted risk of mortality much lower in patients using AVF compare to AVG or CVC, Both in DM and non DM patients.


Incidence of mortality in the first 3 month:
Dr. CiptoMangunkusumoHospital, Jakarta
Indonesian Renal Registry 2017
20
Incidence of mortality in the first 6 month:
Sanglah Hospital,Bali
2013
1.4%
2011
31.7%
2000
44.8%
8.11 %
7
CVD
HemodialysisOutcome ?
Some data from the main teaching hospital in Jakarta foundthat the incidence of mortality in the first 3 months was high in 2000 (44.8%), then decreased in 2011 and 2013 (31.7% and 16.4% respectively). Meanwhile, data from Bali showed that the incidence of mortality in the first 6 months was 8.11%. The main cause of death was CVD, contributing as many as 56% of total number of deaths.

• We are facing many challenges in order to be able to deliver an affordable and equitable kidney care, such as limited number of healthcare worker, access to kidney care and financial constraints.
• Hemodialysis is the most RRT modalities available in Indonesia.
• In the future we need to increase PD service and kidney transplantation with cadaveric donor.
• Improving collaboration with all stakeholders especially the government, NHI, and all layers of health services is important.
• Encourage the MoH to place kidney disease as one of priority in prevention program of NCD.
SUMMARY
9






















![Ultrasound guidance versus anatomical landmarks for ...€¦ · [Intervention Review] Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization Patrick](https://img.pdfslide.us/doc/110x75/5f9beef95154c7333f47d212/ultrasound-guidance-versus-anatomical-landmarks-for-intervention-review-ultrasound.jpg)





