Embed Size (px)
DESCRIPTION
onco
Citation preview
Overview of Breast CancerTRACO Lecture Series - 2009
Farah Zia, MDMedical Officer, DCTD, NCI
November 9, 2009
Definition of Breast CancerCancer that forms in tissues of the breast: Ducts: Tubes that carry milk to the nippleLobules: Glands that make milk
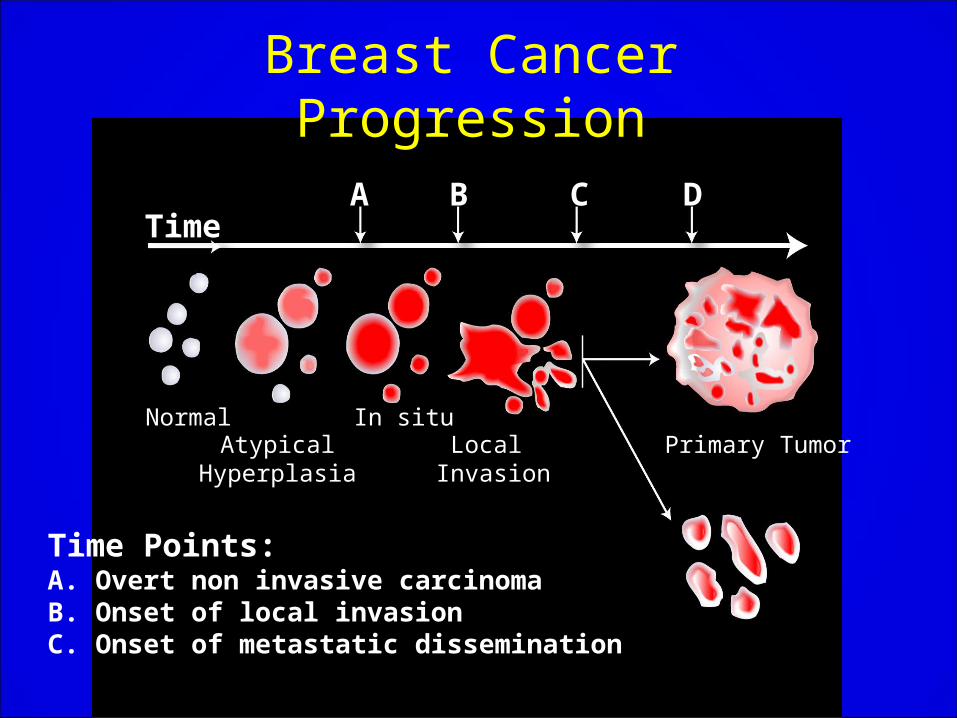
Breast Cancer Progression
A B C D
Primary TumorLocal Invasion
AtypicalHyperplasia
In situNormal
Time
Time Points:A. Overt non invasive carcinomaB. Onset of local invasionC. Onset of metastatic dissemination
Types of Breast Cancer
Ductal Carcinoma in situ(DCIS) Most common type of non-invasive breast cancer.The cancer is only in the ducts and has not spread through the wall of the ducts into the tissue of the breast.Nearly all women with cancer at this stage can be cured.Best form of early detection is with a mammogram (non-palpable, asymptomatic)
Lobular Carcinoma in situ(LCIS)This condition begins in the milk glands, but does not go through the walls of the lobules into the breast tissue.Although not a true cancer, it does increase a woman’s risk of developing cancer later in life.It is important that women with LCIS have regular mammograms.
Invasive Ductal Carcinoma(IDC)This is the most common type of breast ca, accounting for 8 out of 10 invasive breast cancers
Duct breaks thru duct wall invades tissue
From there, it may enter the lymphatics and spread to other parts of the body.
Invasive Lobular Carcinoma(ILC)Lobules breaks thru wall breast tissue
It can then enter the lymphatics and spread to other parts of the body
Accounts for only 1/10 invasive cancers
Inflammatory Breast Cancer (IBC)
• Rare, 1-5% in U.S.• Most aggressive form of breast cancer• Clinical diagnosis
– diffuse erythema involving majority breast– peau d’ orange– erisypeloid edge– often no palpable mass
• Significantly lower overall survival than non-IBC

IBC-patient

Clinical Presentations of IBC
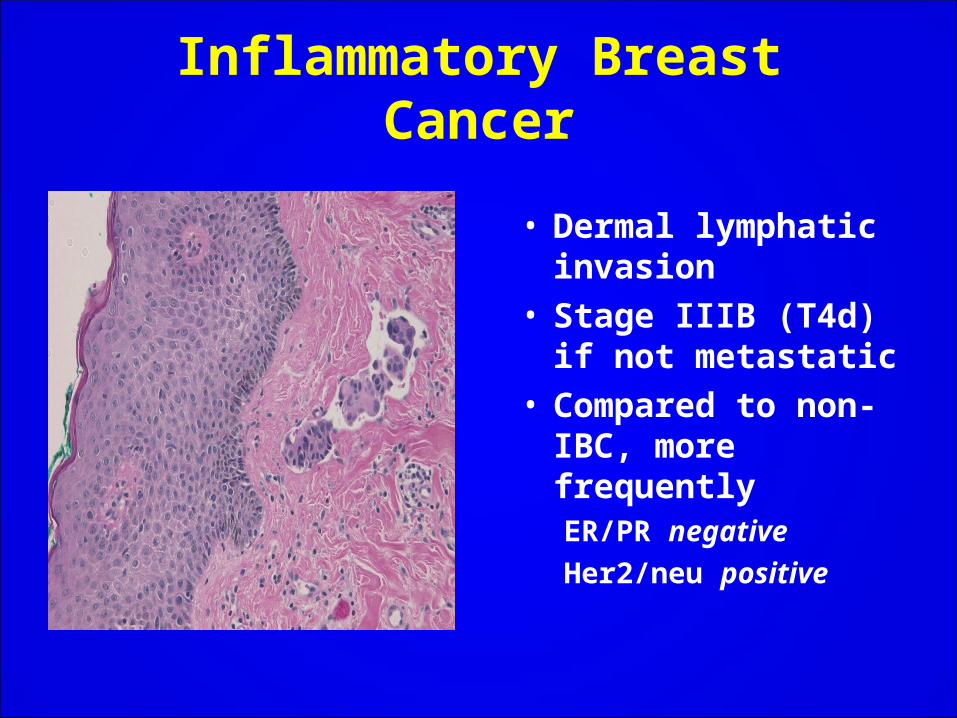
Inflammatory Breast Cancer
• Dermal lymphatic invasion
• Stage IIIB (T4d) if not metastatic
• Compared to non-IBC, more frequently ER/PR negative
Her2/neu positive
Key Statistics For Breast Cancer, 2009
• Chance of developing invasive breast cancer at some point in a woman’s life: 1 in 8 (12%)
• In 2009, 192,370 new cases of invasive breast cancer will be diagnosed among women in the US.
• Also, there will be about 62,280 new cases of carcinoma in situ in 2009.
• It is the most common cancer diagnosed among American women
• 2nd leading cause of cancer death, exceeded only by lung cancer.
• In 2009, about 40,170 women will die from breast cancer in the US
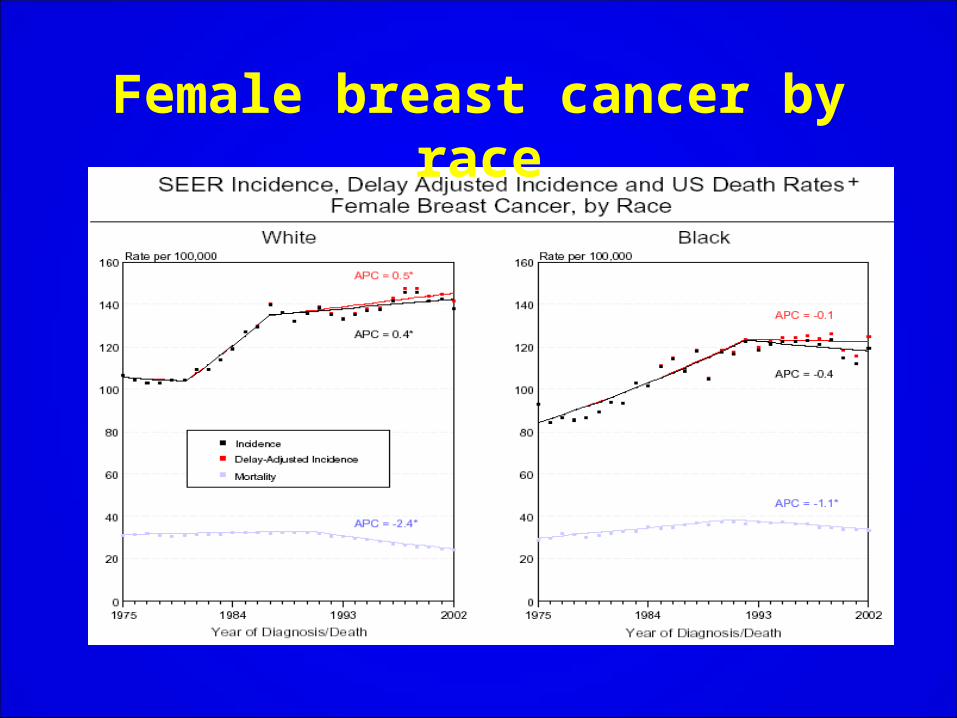
Female breast cancer by race
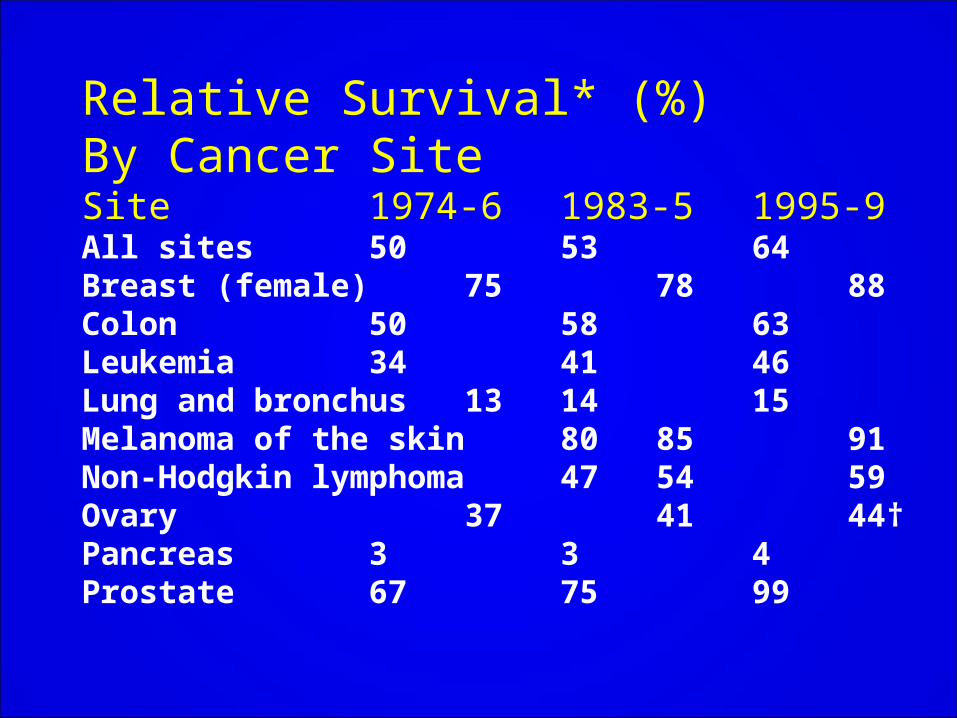
Relative Survival* (%)By Cancer SiteSite 1974-6 1983-5 1995-9All sites 50 53 64Breast (female) 75 78 88Colon 50 58 63Leukemia 34 41 46Lung and bronchus 13 14 15Melanoma of the skin 80 85 91Non-Hodgkin lymphoma 47 54 59Ovary 37 41 44†Pancreas 3 3 4Prostate 67 75 99
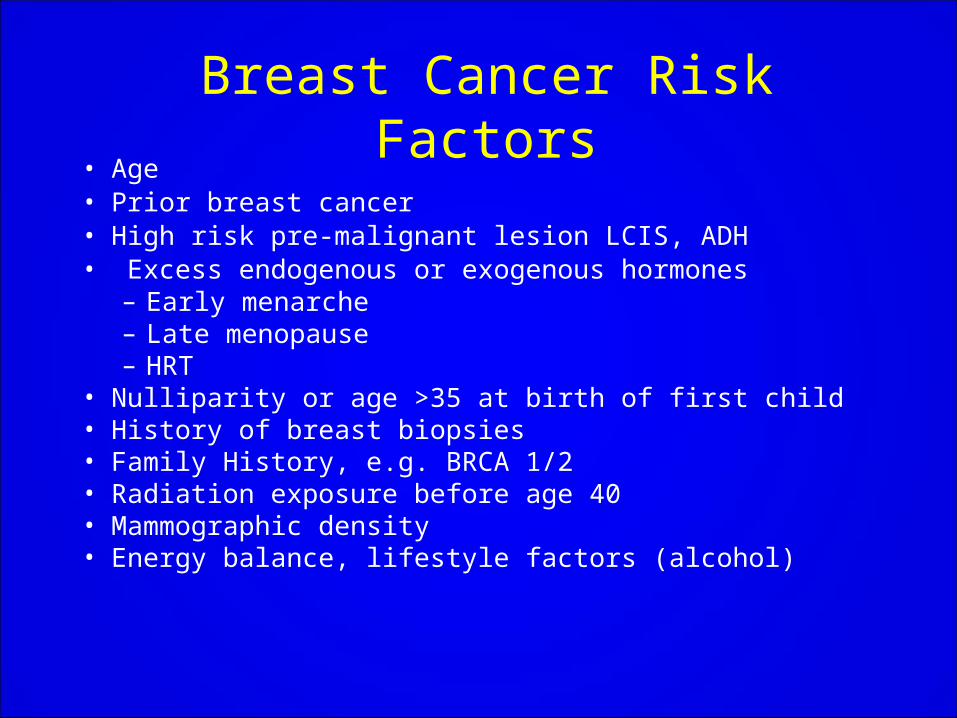
Breast Cancer Risk Factors• Age• Prior breast cancer• High risk pre-malignant lesion LCIS, ADH• Excess endogenous or exogenous hormones
– Early menarche– Late menopause– HRT
• Nulliparity or age >35 at birth of first child• History of breast biopsies• Family History, e.g. BRCA 1/2• Radiation exposure before age 40• Mammographic density • Energy balance, lifestyle factors (alcohol)
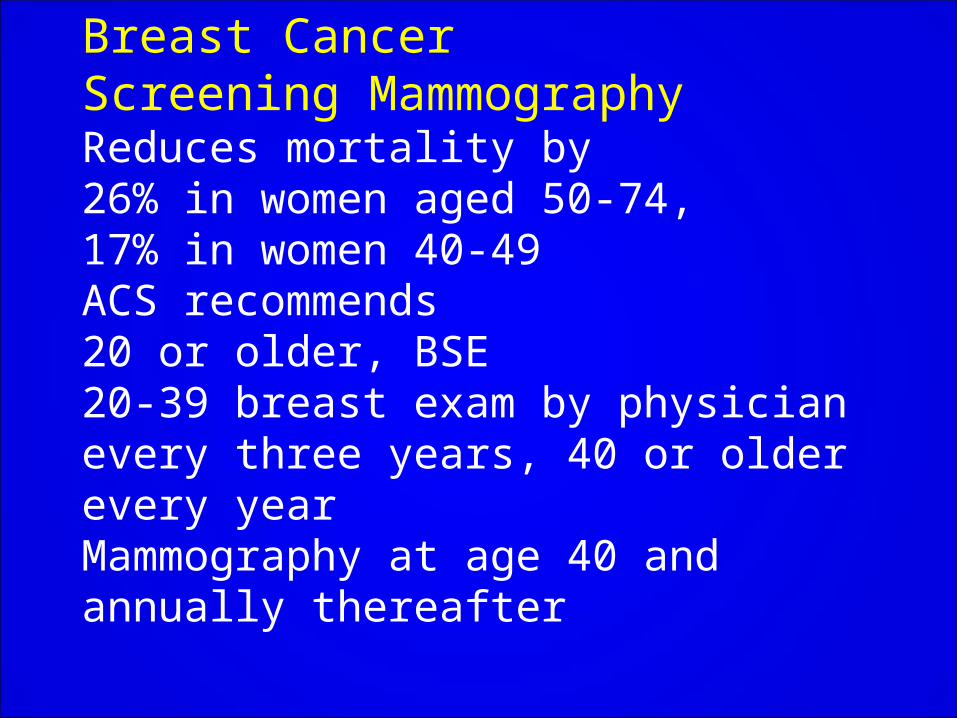
Breast CancerScreening MammographyReduces mortality by 26% in women aged 50-74,17% in women 40-49ACS recommends20 or older, BSE20-39 breast exam by physician every three years, 40 or older every yearMammography at age 40 and annually thereafter
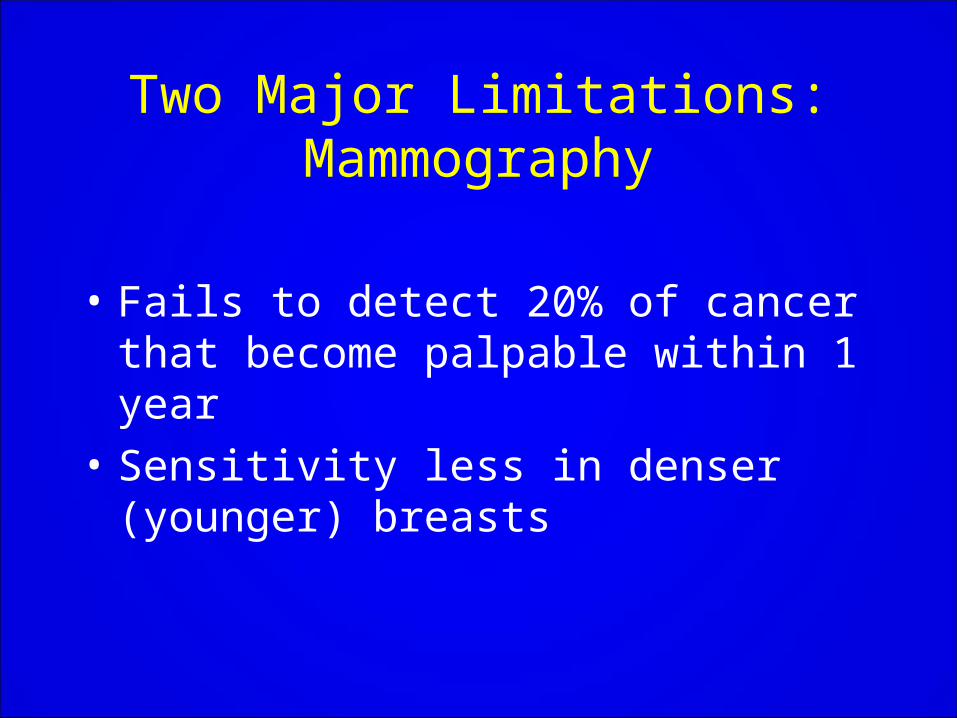
Two Major Limitations:Mammography
• Fails to detect 20% of cancer that become palpable within 1 year
• Sensitivity less in denser (younger) breasts

Other modalities of screening in high risk women
• Digital Mammography– Overall accuracy=to film
mammograms– Better accuracy in
• <50 yrs• Increased mammographic
density• Pre/peri menopauseMRI
– 2-6% of cancers seen only on MRI alone
– Sensitivity for MRI higher than mammo
– Specificity for MRI lower than mammo
• More false + , more biopsies– Promising technique, need longer
follow up and survival data
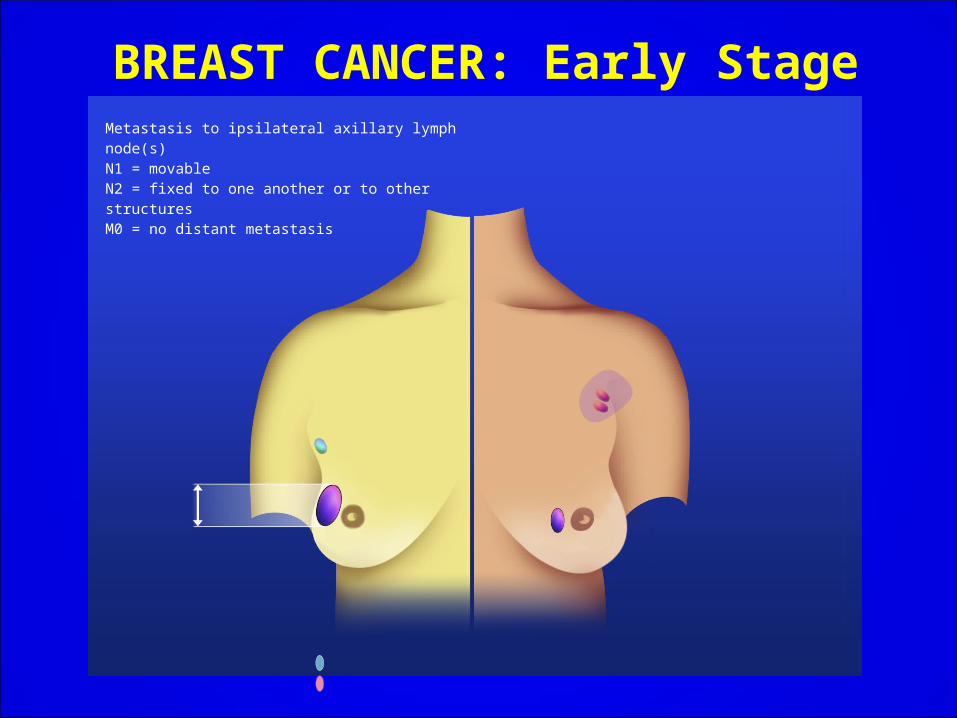
BREAST CANCER: Early StageMetastasis to ipsilateral axillary lymph node(s) N1 = movableN2 = fixed to one another or to other structuresM0 = no distant metastasis
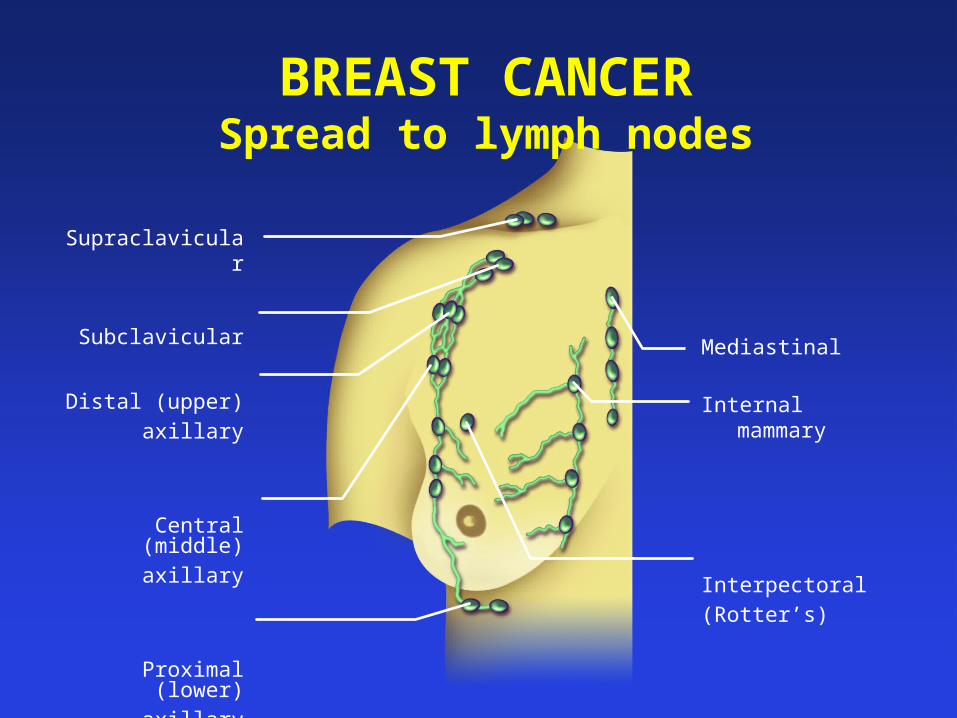
BREAST CANCERSpread to lymph nodes
Supraclavicular
Subclavicular
Distal (upper)
axillary
Central (middle)
axillary
Proximal (lower)
axillary
Mediastinal
Internal mammary
Interpectoral
(Rotter’s)
Systemic Therapy
• Endocrine Directed (Hormone) Therapy
• Chemotherapy
• Biologic agents– Trastuzumab (Herceptin)– Bevacizumab (Avastin)

Hormone Therapy
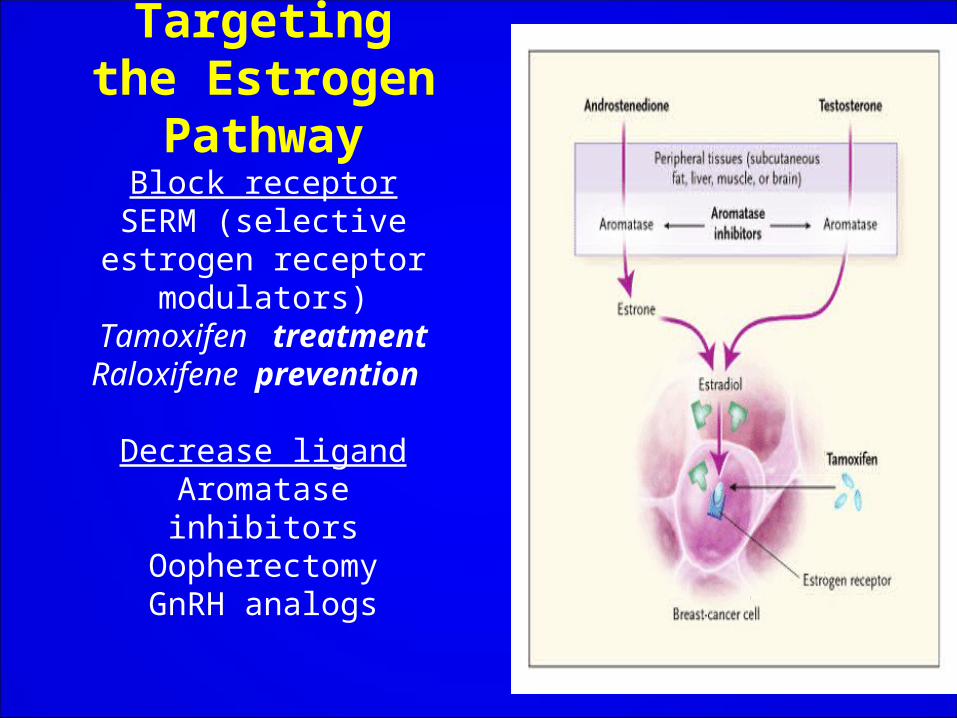
Targeting the Estrogen PathwayBlock receptor
SERM (selective estrogen receptor
modulators)Tamoxifen treatment
Raloxifene prevention
Decrease ligandAromatase inhibitors
OopherectomyGnRH analogs
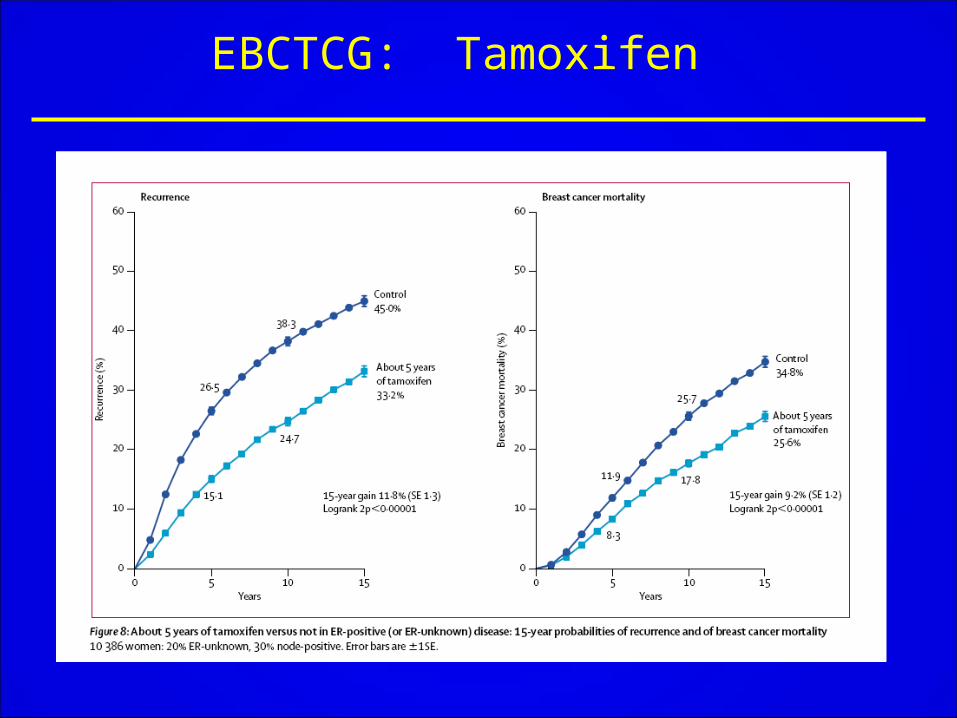
EBCTCG: Tamoxifen
Tamoxifen Pharmacogenetics …. A Developing Area…. JAMA, Oct. 7, 2009 The growth inhibitory effect of tamoxifen is mediated by its metabolites:4-hydroxytamoxifenEndoxifenThe formation of these active metabolites is catalyzed by the polymorphic cytochrome P450 2D6 (CYP2D6) enzyme
CYP 2DG VariantsApproximately 100 CYP 2D6 genetic variants have been identified.These manifest in the population as 4 distinct phenotypes:
Extensive (normal activity)Intermediate (reduced activity)Poor (no activity)Ultra-rapid (high activity)
Thus, it can be speculated that genotype related differences in the formation of active metabolites influence therapeutic response to tamoxifen.
CYP 2DG VARIANTSTo investigate this relationship:
Genotyped tumor tissue DNA for CYP2D6 variations in 1,325 breast cancer patients taking adjuvant tamoxifen.Women were classified as having either: 1. Extensive Metabolism (609 pts) 2. Heterozygous extensive/intermediate (637 pts) 3. Poor metabolism (79)
Researchers found clear evidence that breast cancer was more likely to return in pts with reduced or absent CYP 2D6 function
CYP 2DG ACTIVITYExtensive metabolizers have a 14.9% recurrence at 9 yr FU Heterozygotes have a 20.9% recurrence at 9 yr FU Poor metabolizers have a 29% recurrence at 9 yr FU
Aromatase Inhibitors (AI):AI’s are drugs that reduce the level of estrogen in postmenopausal women.
Aromatase Inhibitors:Currently, 3 AI’s are approved by U.S.
FDA
Anastrozole (Arimidex)
Letrozole (Femara)
Exemestane (Aromasin)
Trials of AIs in the early adjuvant setting. In the ATAC trail patients received tamoxifen x5, anastrozole x 5 or tamoxifen + anastrozole x 5 resulting in a 22% improvement in DFS on anastrozole.
In the BIG I-98 trial patients received tamoxifen x 5, letrosole x 5, tamoxifen x 2 + letrozole x 3 or tamoxifen x 3 + letroxole x 2.
In the IES trial pateients received tamoxifen x 2-3 + tamoxifen x 2-3 or exemestane x 2-3 resulting in a 32% improvement in DFS with exemestane.
In the ABCSGi ARNO 95 Ita trial pateints receive tamofen x 2-3 plus tamoxifen x 2-3 or anastozole x 2-3 resulting in a 43% improvement in DFS on letrozole.
Breast cancer
Should aromatase inhibitors be used in place of tamoxifen?
Is there a role for sequential therapy with an AI and Tam?
SABCS 2008: Meta-analysis: Adjuvant Aromatase Inhibitors vs Tamoxifen in
Postmenopausal Women
Data was pooled from all trials started by 2000, prospectively comparing an AI and tamoxifen.
The large number of events properly powered the subgroup analysis.
In the meta-analysis 9,856 breast cancer patients received:
TAM x 5 yrs vs AI x 5 yrs.The 5 year recurrence with TAM or AI was 12.6% and 9.6% respectively. The 8 year recurrence with TAX or SI was 19.2 and 15.3% respectively.
AI’s reduced breast cancer recurrence.AI’s were associated with an absolute 2.9% lower recurrence rate at 5 years, that improved to a 3.9%
gain at 8 years (15.3% vs 19.2%, P < 0.00001).
Mortality Analysis, although still early at 3.9 years fu, showed a small, non-significant advantage to 5
years of AI mono-therapy. Gains of 1.1 % and 0.5% for 5 and 8 year breast
cancer mortality.
AI’s reduced breast cancer recurrence.In 9015 patients treated with Tam x 2-3 years then aldosterone x 2-3 years, the 3 years recurrence for Tax or AI was 8.1% and 5% respectively.
Patients treated with TAX or AI, the 6 year recurrence was 16.1% and 12.6% respectively.
Switch to an AI (after 2-3 years on TAM):
absolute gain of 3.1% lower recurrence rate at 3 yrs after the switch and 3.5% at 6 years after the switch (P<0.00001)
0.7% lower breast cancer mortality at 3 years and 1.6% at 6 years (P=0.02)
How Long Should You Take AI’s? Studies are ongoingNo current absolute guidelinesAdjuvant options per the oncologists discretion include:
Primary Rx AI x 5 yrsPrimary Rx TAM x 2 or 3 yrs AI x 2 or 3 yrsPrimary Rx TAM x 5 yrs AI x 5 yrs * Note: current standard of care = AI, Max 5 years Rx
SystemicAdjuvant Chemotherapy
Age<50
Age 50-69
Recurrence Mortality
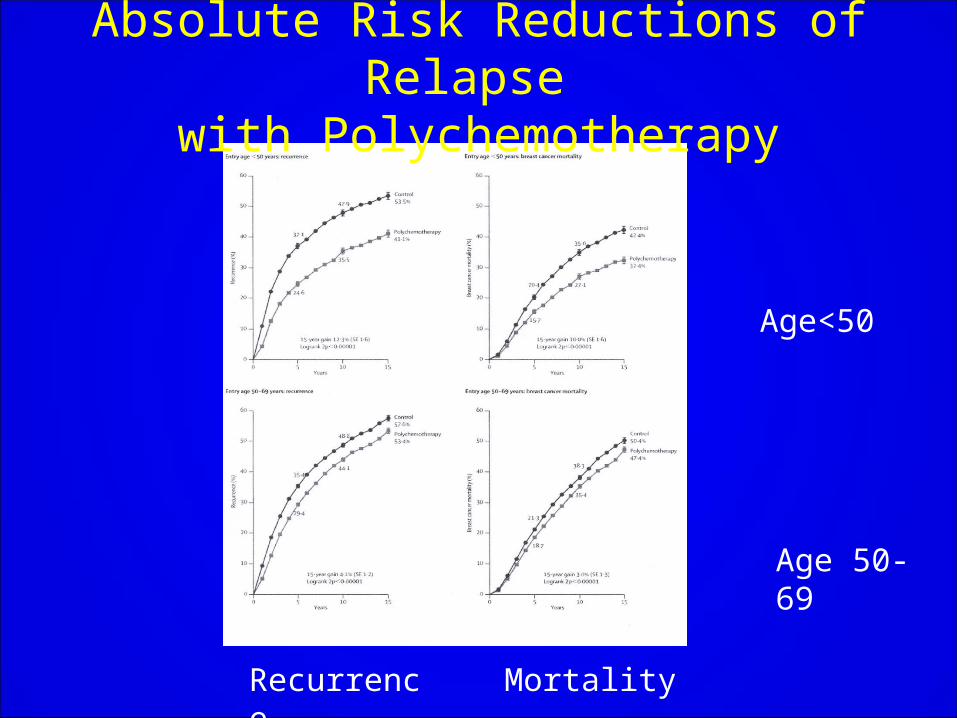
Absolute Risk Reductions of Relapse
with Polychemotherapy
EBCTCG: Systemic therapy28,000 women in 56 trials: Meta-analysisImpact of Polychemotherapy On Absolute Risk Reduction at 5 years (in % )
Subgroup age < 50, Node- had a Recurrenceof 9.9% (SE 1.3).Subgroup Age < 50, Node+ had a recurrence of
14.6% (SE 2.3). Subgroup Age 50-69, Node- had a recurrence of 5.3 (SE 1.0).Subgroup Age 50-69, Node + had a recurrence of 5.9 (SE 1.0).
Adjuvant Systemic Polychemotherapy
• Polychemotherapy is more effective than single agent
• Proportional benefits not affected by nodes, ER, menopausal status, or use of tamoxifen
• Compared with CMF, anthracyclines produced an absolute benefit of 4% in recurrence and survival
Adjuvant Chemotherapy Options
• Low risk/lymph node negative
– AC x 4– CMF x 6– CAF x 6– FEC-100
• Lymph node positive/high risk– Dose dense AC x 4 Paclitaxel x 4 (q2wk)– AC x 4 Docetaxel x 4 (q3wk)– TAC x 6 (q3wk)
• Trastuzumab if HER2 positive

Biologic Agents
ErbB2/HER2 Action in Breast CA Member of the membrane-spanning type I receptor tyrosine kinase family, comprising 4 closely related family members.They dimerize upon ligand stimulation and transduce their signals by subsequent autophosphorylation, catalyzed by the receptor tyrosine kinase activity.This results in recruitment of an array of downstream signaling cascades (survival and mitogenic ) The incidence of ErbB2 amplification is ≈ 30% in breast cancer …Identifying it as a therapeutic target
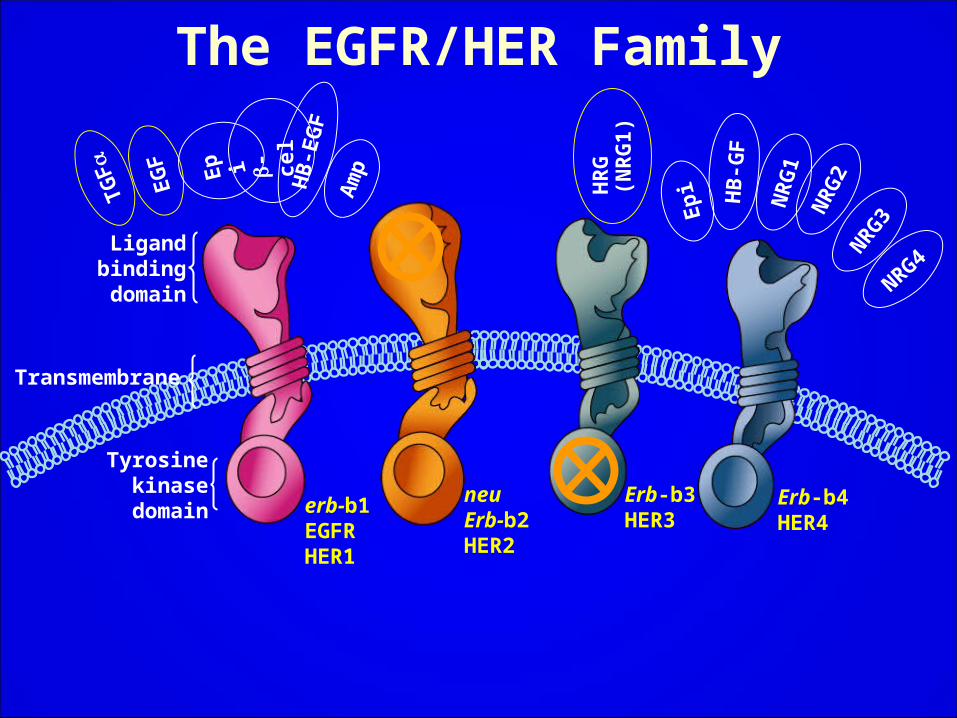
erb-b1EGFRHER1
neu Erb-b2HER2
Erb-b3HER3
Erb-b4HER4
TG
F
EG
F
HR
G(N
RG
1)
Ep
i
-ce
l
HB
-E
GF
Am
p
Ep
i
HB
-GF
NR
G1
NR
G2
NR
G3
NRG4
Tyrosinekinase
domain
Ligandbindingdomain
Transmembrane
The EGFR/HER Family
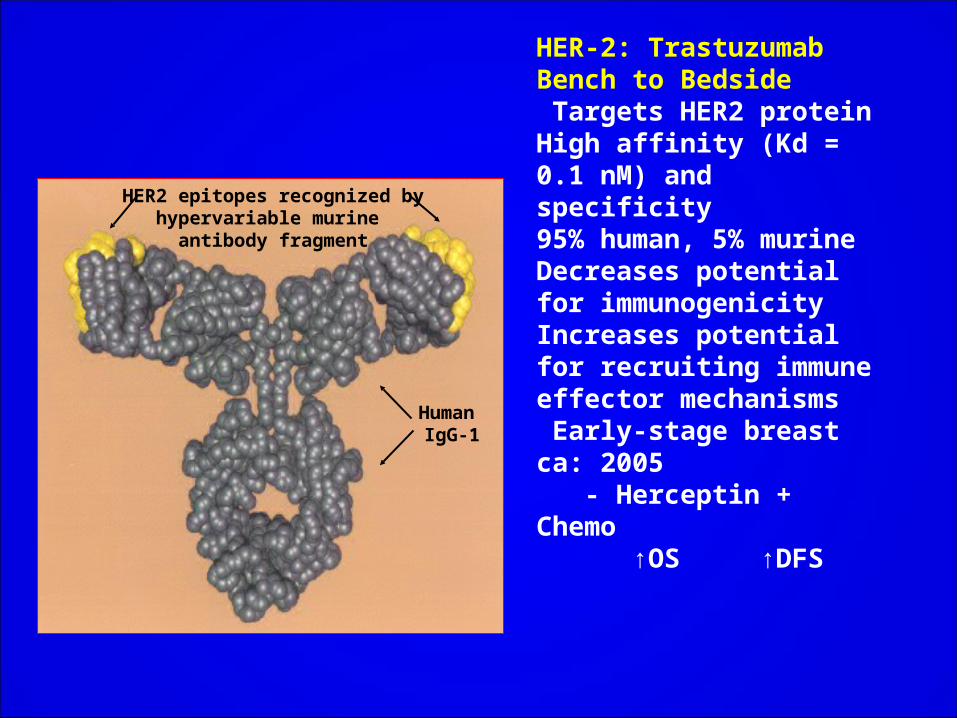
HER2 epitopes recognized by hypervariable murine
antibody fragment
Human IgG-1
HER-2: TrastuzumabBench to Bedside Targets HER2 proteinHigh affinity (Kd = 0.1 nM) and specificity95% human, 5% murineDecreases potential for immunogenicityIncreases potential for recruiting immune effector mechanisms Early-stage breast ca: 2005 - Herceptin + Chemo ↑OS ↑DFS
NSABP B-31Control: ACT
The patient receives4 treatments of doxorubicin/cyclophosphamide (AC) 60/600 mg/m2 q 3 wk x 4 followed by 4 treatments of paclitaxel (T) 175 mg/m2 q 3 wk x 4. Alternatively the patient receives 4 treatments of doxorubicin/cyclophosphamide (AC) 60/600 mg/m2 q 3 wk x 4 followed by 4 treatments of paclitaxel (T) 175 mg/m2 q 3 wk x 4followed by 4.5 treatments of trastuzumab (H) 4mg/kg LD + 2 mg/kg/wk x 51
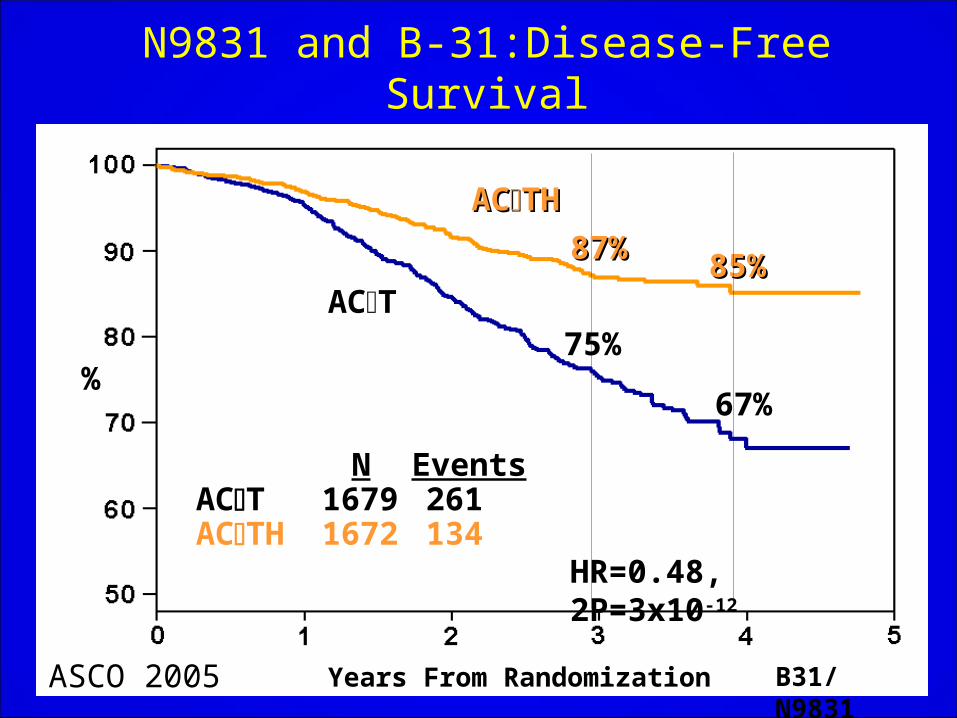
87%87%85%85%
67%
75%
N EventsACT 1679 261ACTH 1672 134
%
HR=0.48, 2P=3x10-12
ACACTHTH
ACT
Years From Randomization B31/N9831ASCO 2005
N9831 and B-31:Disease-Free Survival

Triple NegativeBreast Cancer
Triple –negative breast cancer refers to a specific subtype of breast cancer that does not express the genes for: Estrogen Receptor (ER) Progesterone Receptor (PR) HER2/neu
It is diagnosed more frequently in: Younger women African Americans Hispanics Women with BRCA1 mutations
Triple-negative breast ca is clinically characterized as:More aggressiveLess responsive to standard chemotherapy treatmentAssociated with a poorer overall prognosis
Development of New Treatment Strategies For Triple Negative Breast Cancer ASCO, 2009PARP (poly ADP-ribose polymerase) Inhibitors:
n experimental class of drugs that may have potential for the treatment of triple-negative breast cancer. PARP is an enzyme used by cancer cells to repair DNA damage.PARP inhibitors are being used to target tumors where one pathway is already shut down. - BRCA1/BRCA2 mutations lose a form of DNA repair and rely more heavily on the PARP pathway - Tumors which are either concurrently or pre-treated with chemotherapy also have damaged DNA repair pathways.
Two PARP Inhibitors Currently in Phase I/II
Clinical Trials:
BSI – 201 (IV)
Olaparib (Oral)
BSI-201116 women with triple-negative metastatic breast cancer randomized to standard chemotherapy vs standard chemo therapy + BSI-201. Median survival of 5.7 months with standard chemotherapy versus 9.2 months with BSI-201 plus chemotherapy.………………...
How can we do better? Better selection of chemotherapy regimensGene expression profiling to predict response to particular agents Better selection of patients for treatment with chemotherapyTreat only those patients who are most likely to recur AND who will therefore benefit most from
the addition of chemotherapy… TAILORx Trial
Predicting Response to Chemotherapy
• Neoadjuvant (pre-surgical) chemotherapy allows for assessment of tumor response to treatment
• Allows us to identify factors associated with response
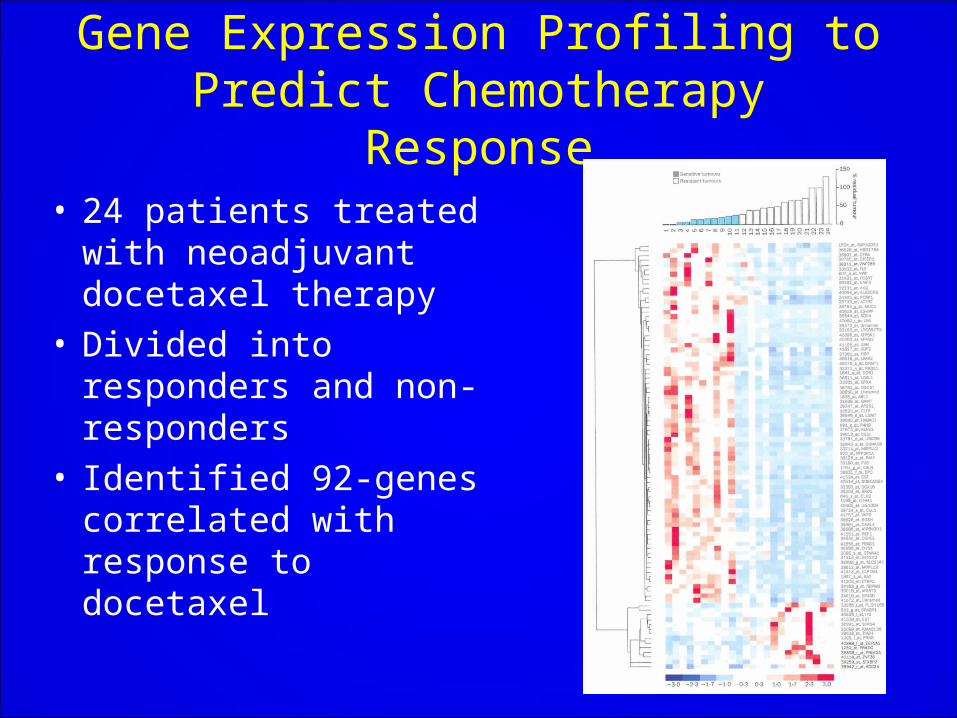
Gene Expression Profiling to Predict Chemotherapy Response
• 24 patients treated with neoadjuvant docetaxel therapy
• Divided into responders and non-responders
• Identified 92-genes correlated with response to docetaxel
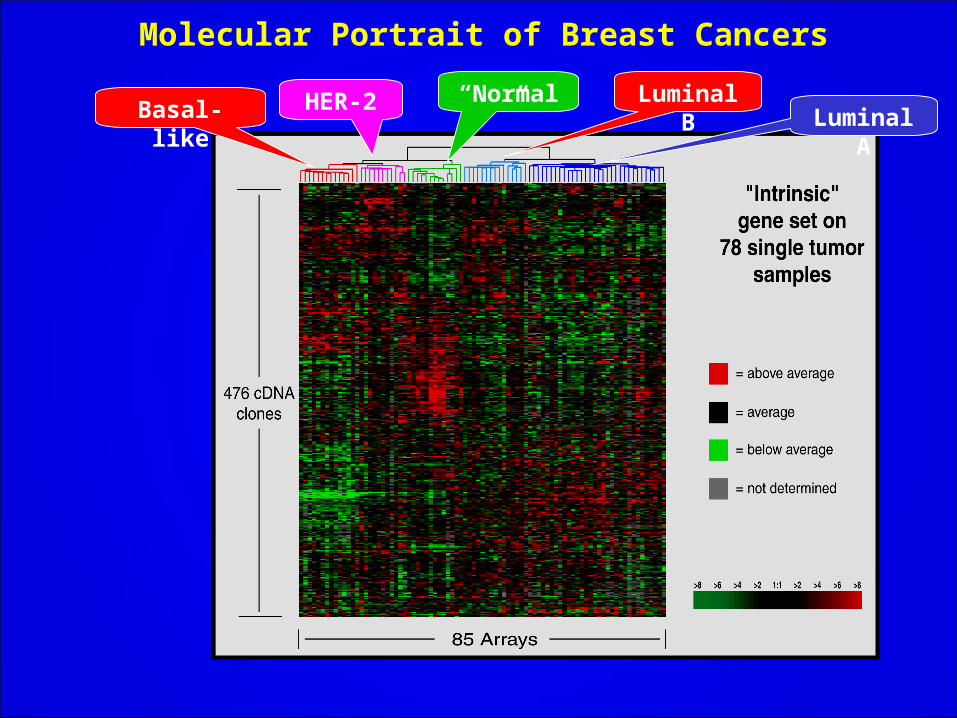
Molecular Portrait of Breast Cancers
HER-2Basal-like Luminal ALuminal B“Normal”
An Important Question in Breast Cancer Treatment What is the likelihood of distant recurrence in patients with breast cancer who have no involved lymph nodes and estrogen-receptor positive tumors? - These patients prognosis is poorly defined by histopathological and clinical measures alone
Oncotype DX A multi-step approach was used to:
Develop an assay for the expression of tumor related genes for use with paraffin-embedded tumor tissue
To validate the assay clinically
RT-PCR method was developed to quantify gene expression with paraffin-embedded tumor tissue.
250 candidate genes were selected from published literature, genomic databases, and experiments based on DNA arrays done on fresh-frozen tissue.
Data was analyzed from three independent clinical studies of breast ca involving 447 patients to test the relationship between expression of the 250 candidate genes and the recurrence of breast cancer.
Three Breast Cancer Studies Used To Select 21 Gene Panel 16 Cancer and 5 Reference Genes 4. used the results of the 3 studies to select a panel of 16 cancer related genes and 5 reference genes. - Best RT-PCR performance - Most robust predictionsDesigned an algorithm based on the levels of expression of these genes to compute a recurrence score for each tumor sample being tested.Genes for proliferation (Ki-67, STK15, Survivin, Cyclin B1, MUBL2), estrogen (ER, PR, Bcl2, SCUBE2), invation (Stromolysin 3, Cathepsin L2) HER2 (GRB7, HER2), GSTM1, VD68, BAG1 and reference (Beta-actin, GAPDH, RPLPO, GUS, and TFRC) were studied.
Validation of Onco DX Paraffin-embedded tissue samples from patients previously enrolled in the NSABP B-14 trial were used to validate the ability of the 21 gene RT-PCR assay and RS algorithm to quantify the likelihood of distant recurrence in patients with:
Node-negative, ER+, early stage breast cancer who had been previously treated with tamoxifen.
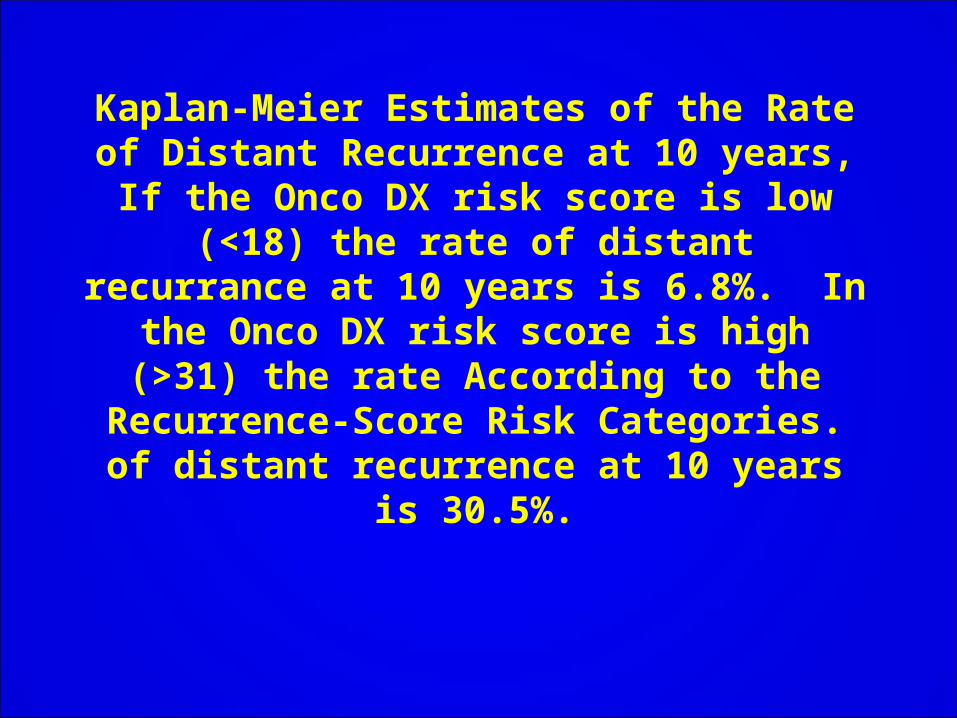
Kaplan-Meier Estimates of the Rate of Distant Recurrence at 10 years, If the Onco DX risk score is low (<18) the rate of distant recurrance at 10 years is 6.8%. In the Onco
DX risk score is high (>31) the rate According to the Recurrence-Score Risk Categories. of distant recurrence at 10
years is 30.5%.
0%
5%
10%
15%
20%
25%
30%
35%
40%
0 5 10 15 20 25 30 35 40 45 50
Recurrence Score
Dis
tan
t R
ec
urr
en
ce
at
10
Ye
ars
Low Risk Group High Risk Group Intermediate Risk Group
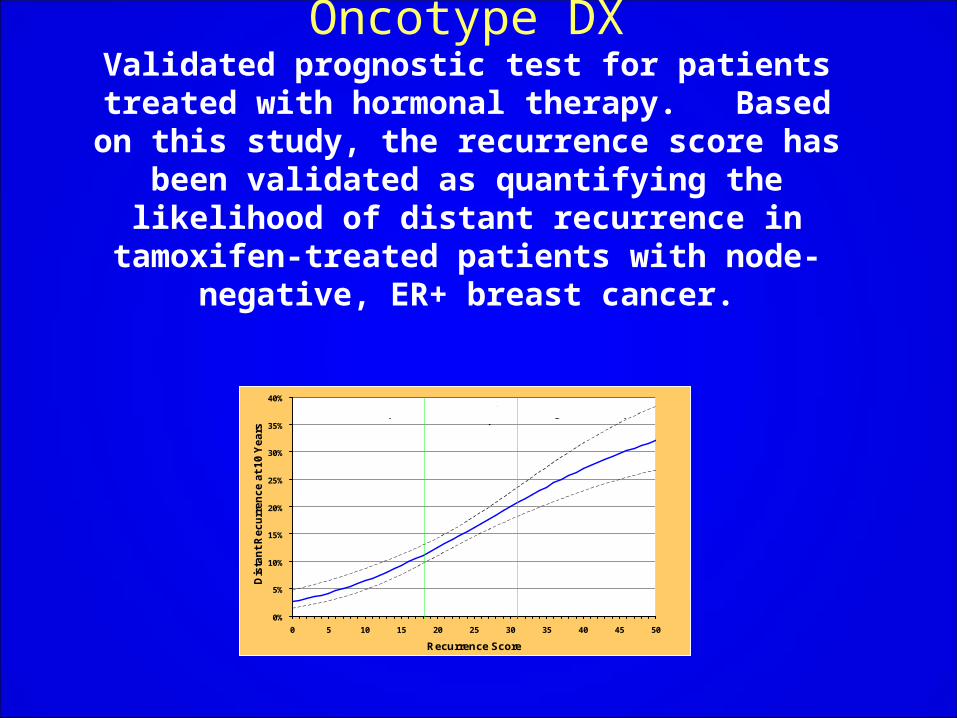
Oncotype DXValidated prognostic test for patients treated with
hormonal therapy. Based on this study, the recurrence score has been validated as
quantifying the likelihood of distant recurrence in tamoxifen-treated patients with node-negative,
ER+ breast cancer.
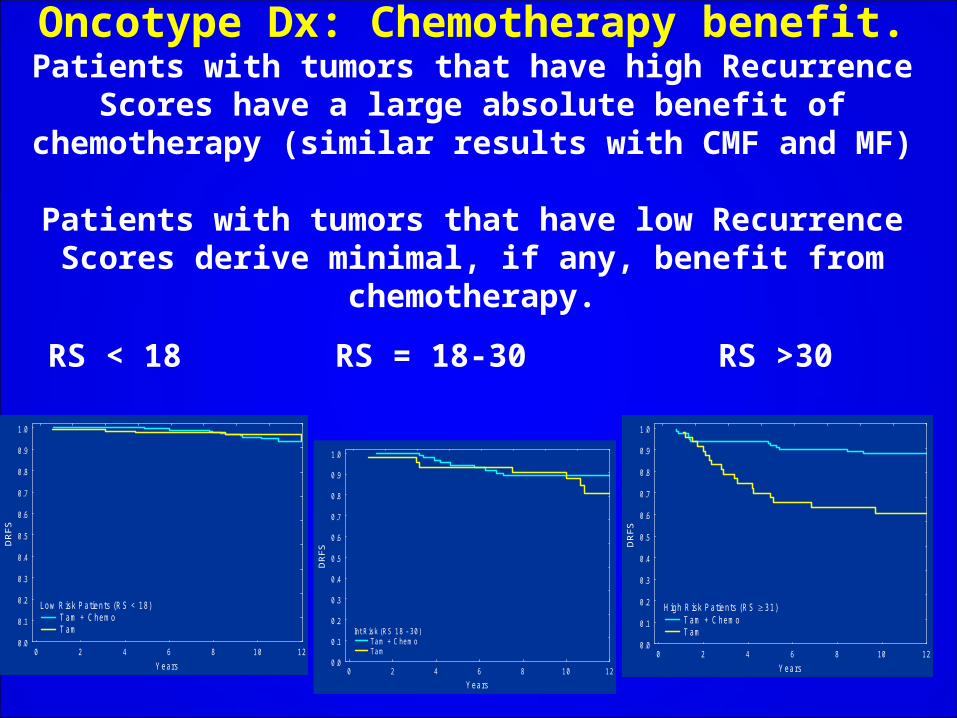
Oncotype Dx: Chemotherapy benefit.Patients with tumors that have high Recurrence Scores have a large absolute benefit of chemotherapy (similar
results with CMF and MF)
Patients with tumors that have low Recurrence Scores derive minimal, if any, benefit from chemotherapy.
RS < 18 RS = 18-30 RS >30
0 2 4 6 8 10 12
Y ears
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
Low R isk P atients (R S < 18) T am + C hemo T am
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
Int Risk (RS 18 - 30) Tam + C hemo Tam 0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
H igh R isk Patients (RS 31) T am + Chemo T am
Ongoing Research: TAILORxLandmark trial - represents the culmination of a major initiative to integrate molecular diagnostic
testing into clinical decision making.
NCI is using Oncotype DX to identify and assign treatment to more than 10,000 breast cancer
patients from 1,500 sites in the US, Canada, and Peru.
Purpose: to determine whether adjuvant hormonal therapy is as effective as adjuvant hormonal + chemo for women with a midrange RS. Eligibility: ER+ and/or PR+, Node-negative HER2/neu-negative breast cancerPrimary Objectives: 1. Determine whether adjuvant hormonal tx is not inferior to chemo-hormonal tx in women with a
mid-range OncoDX RS (11-25) 2. Create a tissue and specimen bank for patients enrolled in this trial. To include: tumor specimens, tissue microarrays, plasma, & DNA from peripheral blood.
17
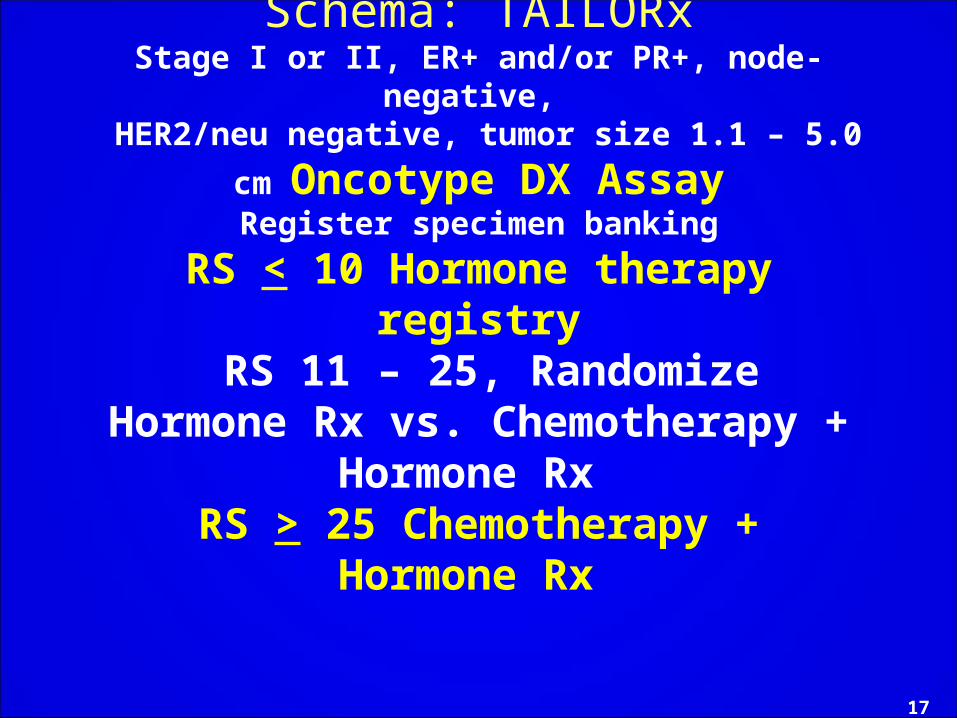
Schema: TAILORxStage I or II, ER+ and/or PR+, node-negative, HER2/neu negative, tumor size 1.1 – 5.0 cm
Oncotype DX AssayRegister specimen banking
RS < 10 Hormone therapy registry RS 11 – 25, Randomize
Hormone Rx vs. Chemotherapy + Hormone Rx
RS > 25 Chemotherapy +Hormone Rx
TAILORx: Key points
• TAILORx will examine whether genes that are frequently associated with recurrence for women with early stage breast cancer can be used to assign patients to the most appropriate and effective treatment.
• The results of this trial could eventually spare many women the unnecessary toxicity of chemotherapy. (currently, ≈ 10% considered low risk; with RS score, 50%).
• It is one of the first trials to examine a methodology to personalize cancer treatment!
Stage IV: Metastatic Breast Cancer

Characteristics of MBC Median survival approximately 2 to 3 years,
with a 5-year survival of about 20%
About 10% of women present at diagnosis with newly diagnosed metastatic breast
cancer (MBC).
Metastatic disease is considered incurable
Goals of Treatment of MBCProlongation of survival
Improvement of quality of life - Improvement of symptoms
- Acceptable toxicity
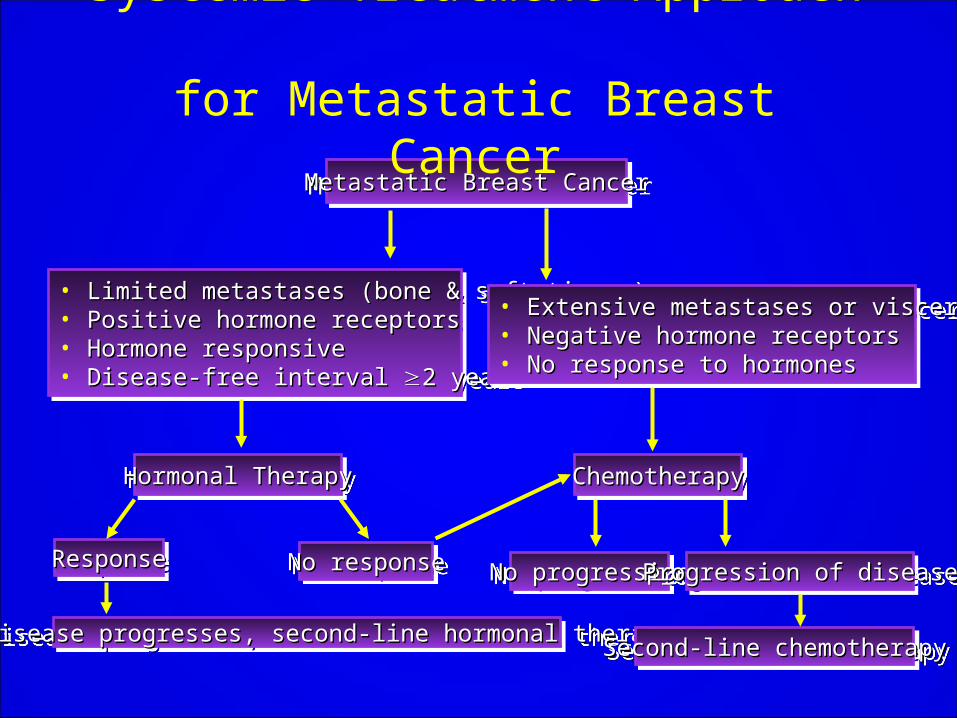
Metastatic Breast CancerMetastatic Breast CancerMetastatic Breast CancerMetastatic Breast Cancer
• Limited metastases (bone & soft tissue)Limited metastases (bone & soft tissue)• Positive hormone receptorsPositive hormone receptors• Hormone responsiveHormone responsive• Disease-free interval Disease-free interval 2 years2 years
• Limited metastases (bone & soft tissue)Limited metastases (bone & soft tissue)• Positive hormone receptorsPositive hormone receptors• Hormone responsiveHormone responsive• Disease-free interval Disease-free interval 2 years2 years
• Extensive metastases or visceral crisisExtensive metastases or visceral crisis• Negative hormone receptorsNegative hormone receptors• No response to hormonesNo response to hormones
• Extensive metastases or visceral crisisExtensive metastases or visceral crisis• Negative hormone receptorsNegative hormone receptors• No response to hormonesNo response to hormones
Hormonal TherapyHormonal TherapyHormonal TherapyHormonal Therapy ChemotherapyChemotherapyChemotherapyChemotherapy
ResponseResponseResponseResponse No responseNo responseNo responseNo responseNo progressionNo progressionNo progressionNo progression Progression of diseaseProgression of diseaseProgression of diseaseProgression of disease
If disease progresses, second-line hormonal therapyIf disease progresses, second-line hormonal therapyIf disease progresses, second-line hormonal therapyIf disease progresses, second-line hormonal therapySecond-line chemotherapySecond-line chemotherapySecond-line chemotherapySecond-line chemotherapy
Systemic Treatment Approach for Metastatic Breast Cancer
Metastatic Breast Cancer: Hormonal therapySelective Estrogen Receptor ModulatorsTamoxifen, toremifene Aromatase Inhibitors (post-menopausal)Anastrozole, letrozole, or exemestane Selective Estrogen Receptor DownregulatorsFulvestrantProgestinsmegace 40 mg po 4 x dailyOvarian suppression (pre-menopausal) luteinizing hormone releasing analogoophorectomy
Hormone positive post-menopausal Metastatic Breast CancerFirst line: Antiestrogen or Nonsteroidal AIAntiestrogen or Nonsteroidal AI Anastrozole or Letrozole. Anastrozole or Letrozole.Second line: Nonsteroidal AI or Antiestrogen.Second line: Nonsteroidal AI or Antiestrogen.Third line: Steroidal AI:exemestane. Third line: Steroidal AI:exemestane. Fourth line: Progestin. Fourth line: Progestin. Fifth line: Androgen. Fifth line: Androgen. If no response use chemotherapyIf no response use chemotherapy
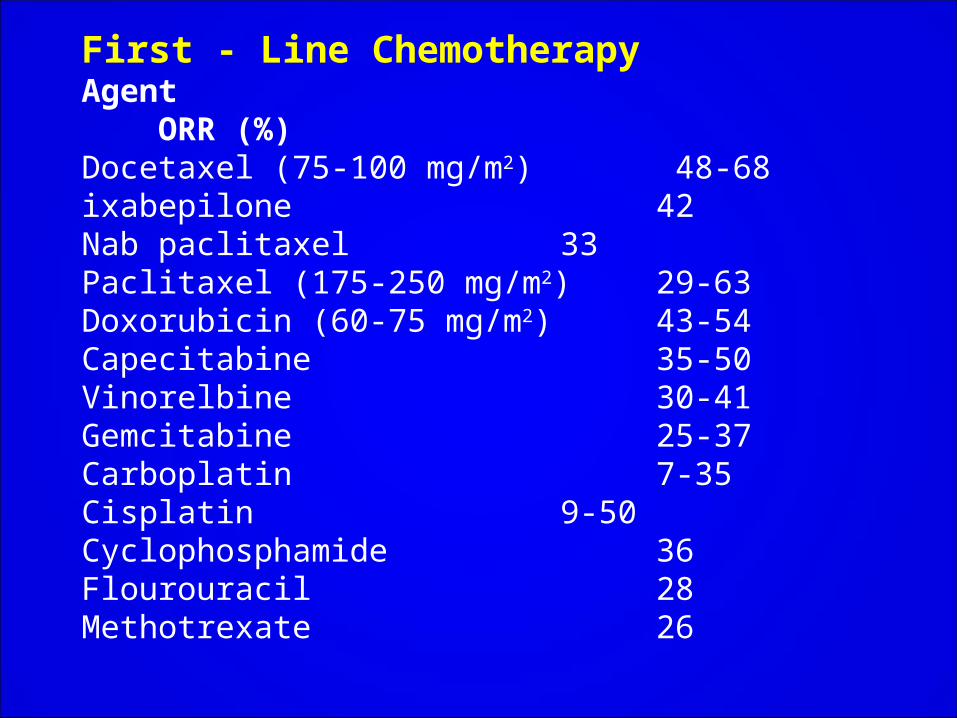
First - Line Chemotherapy Agent ORR (%)Docetaxel (75-100 mg/m2) 48-68ixabepilone 42Nab paclitaxel 33Paclitaxel (175-250 mg/m2)29-63Doxorubicin (60-75 mg/m2) 43-54Capecitabine 35-50Vinorelbine 30-41Gemcitabine 25-37Carboplatin 7-35Cisplatin 9-50Cyclophosphamide 36Flourouracil 28Methotrexate 26
For HER-2 positive patients add Trastuzumab (Herceptin)
Bevacizumab (Avastin)
Bevacizumab (Avastin®):Humanized monoclonal antibody directed against all isoforms of VEGF-A (potent vasodilator and inducer of pathologic angiogenesis). - binds to VEGF, inhibits VEGF receptor binding
Laboratory and clinical evidence supports the central role of angiogenesis in the progression of breast cancer.
Multiple angiogenic factors are expressed by invasive breast cancers - 121-amino-acid isoform of VEGF predominates
Bevacizumab in the First –line Treatment of Locally Recurrent or MBC
ECOG 2100 TrialStratify: DFI < 24 mos. vs. > 24 mos. < 3 vs. > 3 metastatic sites Adjuvant chemotherapy yes vs. no ER+ vs. ER- vs. ER unknownRandomize and treat with paclitaxel + Bevacizumab or paclitaxel alone
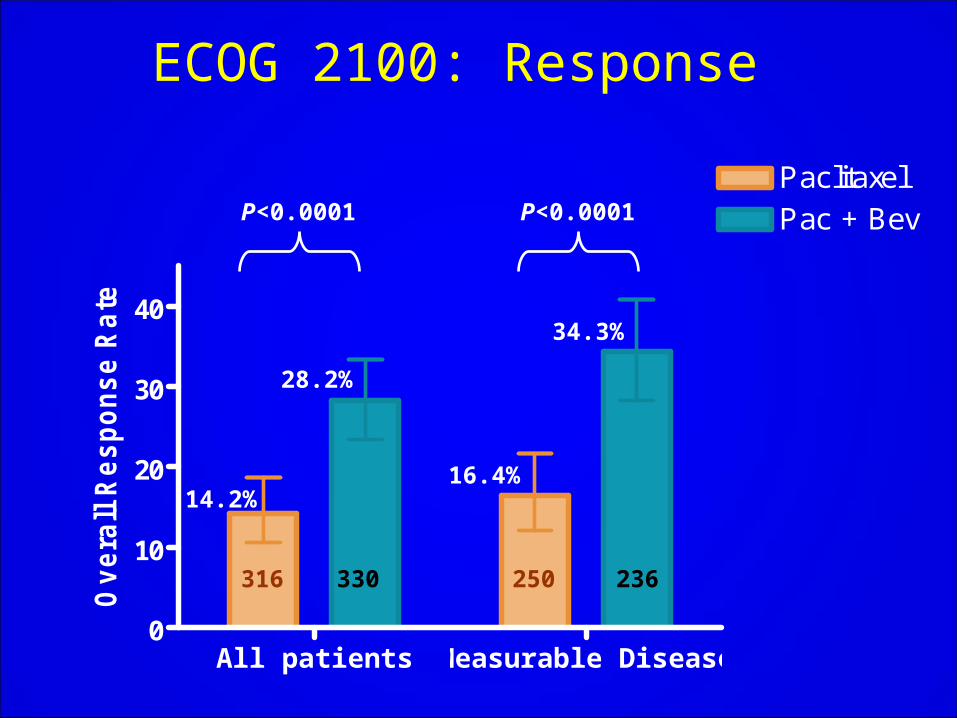
All patients Measurable Disease0
10
20
30
40
Paclitaxel
Ov
era
ll R
es
po
ns
e R
ate
Pac + Bev
ECOG 2100: Response
316 236330 250
34.3%
16.4%
28.2%
14.2%
P<0.0001P<0.0001
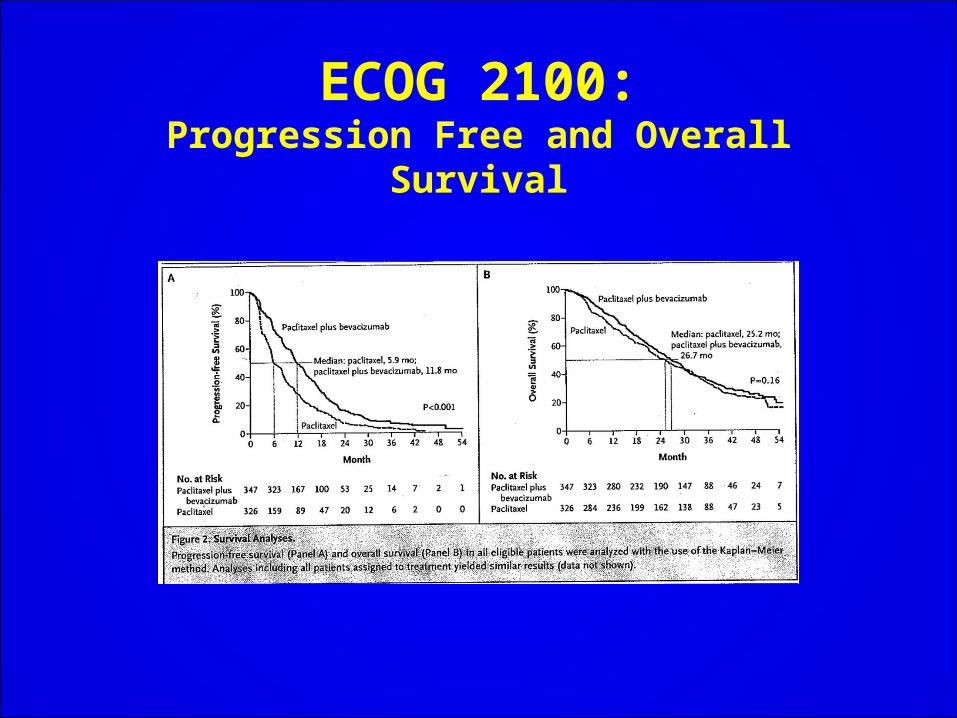
ECOG 2100:Progression Free and Overall Survival
Bevacizumab: Future Directions
• Addition of bevacizumab to paclitaxel– Significantly prolongs progression free survival,
but not overall survival– Increases objective response rate
• Further studies are:– Exploring the role of Bevacizumab in the adjuvant
setting (BEATRICE Trial: Phase III/Triple-negative breast)
– Developing methods to identify patients who are most likely to benefit from VEGF-targeted therapies
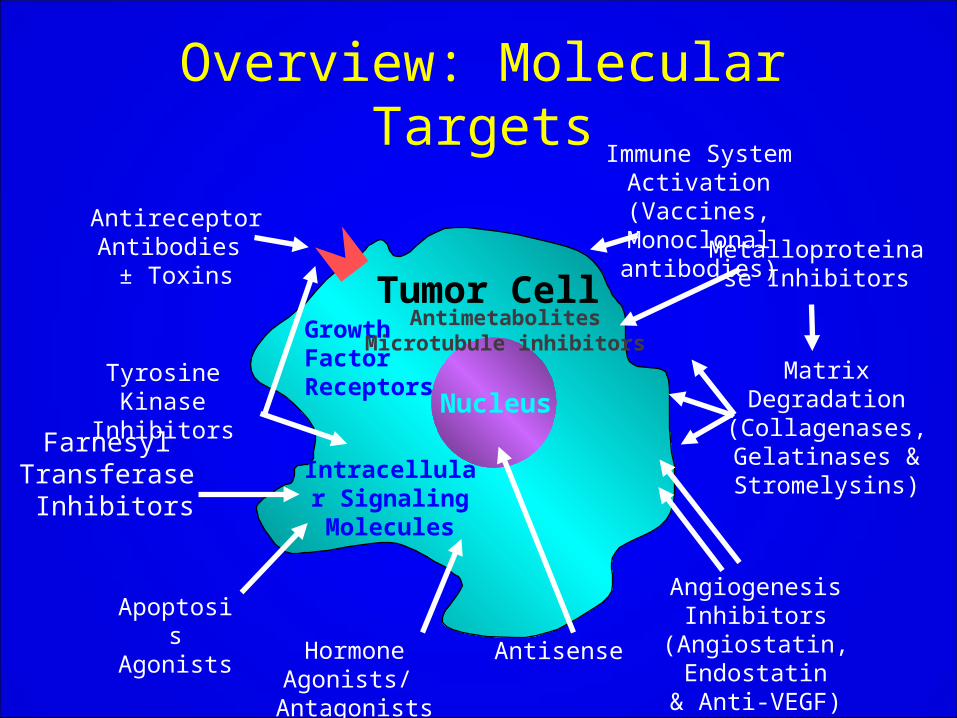
Nucleus
Antireceptor Antibodies
± Toxins
Tyrosine Kinase Inhibitors
Hormone Agonists/ Antagonists
Farnesyl Transferase
Inhibitors
Apoptosis Agonists
Antisense
Angiogenesis Inhibitors (Angiostatin, Endostatin
& Anti-VEGF)
Metalloproteinase Inhibitors
Matrix Degradation(Collagenases,Gelatinases &Stromelysins)
Immune System Activation (Vaccines,
Monoclonal antibodies)
Tumor CellGrowth Factor Receptors
Intracellular Signaling Molecules
AntimetabolitesMicrotubule inhibitors
Overview: Molecular Targets
Challenges for the future
• Identify women more specific risk profiles and tailor preventive interventions
• Identify subsets of patients for whom systemic therapy can be avoided
• Tailor systemic therapy to individual tumor/host characteristics
– Targeted therapy: ER, HER2, EGF-R, PARP Inhib
– Novel targets and pathways





























