Embed Size (px)
Citation preview

•6/27/2011
•1
1Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Chapter 9
Oral Manifestations of Systemic Diseases
2Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Outline Endocrine Disorders Blood Disorders Immunodeficiency Oral Manifestations of Therapy for Oral Cancer Effects of Drugs on the Oral Cavity Oral Manifestations of Systemic Diseases
3Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Systemic Diseases
(pg. 288) Many systemic diseases are reflected in the oral
mucosa, maxilla, and mandible. Mucosal changes may include ulceration or mucosal
bleeding. Immunodeficiency can lead to opportunistic diseases
such as infection and neoplasia. Bone disease can affect the maxilla and mandible. Systemic disease can cause dental and periodontal
changes. Drugs prescribed for a systemic disease can affect oral
tissue.
4Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Systemic Diseases (cont.)
Local factors may be involved in the manifestation of systemic disease in oral mucosa. The mucosa may be more easily injured due to
a systemic disease, and mild irritation and chronic inflammation may cause lesions that otherwise would not occur.
These may include Endocrine disorders, disorders of red and
white blood cells, disorders of platelets and other bleeding and clotting disorders, and immunodeficiency disorders
5Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Endocrine Disorders
Hyperpituitarism Hyperthyroidism Hypothyroidism Hyperparathyroidism Diabetes Mellitus Addison Disease
6Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Endocrine Disorders
(pg. 288) The endocrine system consists of a group
of integrated glands and cells that secrete hormones. The secretion is controlled by feedback
mechanisms. The amount of hormone circulating in blood
triggers factors that control production. Diseases may result from conditions
where too much or too little hormone is produced.
•6/27/2011
•2
7Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hyperpituitarism
(pgs. 288-289) Excess hormone production by the
anterior pituitary gland Caused most often by a benign tumor (pituitary
adenoma) that produces growth hormone Giantism results if it occurs before the closure
of long bones. Acromegaly results when hypersecretion
occurs during adult life.
8Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
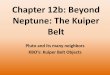
Clinical Features and Oral Manifestations of Hyperpituitarism (pgs. 288-289)
Affects both men and women, most commonly during the fourth decade of life Patients experience poor vision, light sensitivity,
enlargement of hands and feet, and an increase in rib size.
Facial changes Enlargement of maxilla and mandible may cause
separation of teeth and malocclusion. Frontal bossing and an enlargement of nasal bones may
lead to deepening of voice. Mucosal changes
May have thickened lips and macroglossia
9Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Hyperpituitarism (cont.)
10Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Hyperpituitarism
Diagnosis involves measurement of growth hormone.
Treatment often includes pituitary gland surgery.
11Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hyperthyroidism (Thyrotoxicosis)
(pg. 289) Excess production of thyroid hormone
More common in women than men The most common cause is Graves disease
• Graves disease Appears to be due to an autoimmune disorder in
which a substance is produced that abnormally stimulates the thyroid gland
Other causes include hyperplasia of the gland, benign and malignant tumors of the thyroid, pituitary gland disease, and metastatic tumors.
12Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features of Hyperthyroidism
Rosy complexion, erythema of the palms, excessive sweating, fine hair, softened nails The patient may have exophthalmos. Anxiety, weakness, restlessness, and cardiac
problems may also be associated.

•6/27/2011
•3
13Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Hyperthyroidism
May lead to premature exfoliation of deciduous teeth in children and premature eruption of permanent teeth Osteoporosis may affect alveolar bone. Caries and periodontal disease may appear
and develop more rapidly in these patients. Burning tongue also has been reported.
14Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Treatment of Hyperthyroidism
May include surgery, medications to suppress thyroid activity, or administration of radioactive iodine
15Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hypothyroidism
(pg. 289) A decreased output of thyroid hormone
Causes include developmental disturbances, autoimmune disease, iodine deficiency, drugs, and pituitary disease
Cretinism• When it occurs in infancy and childhood
Myxedema• When it occurs in older children and adults
16Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hypothyroidism (cont.)
Oral manifestations In infants
• Thickened lips, enlarged tongue, and delayed eruption of teeth
In adults• Enlarged tongue
17Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hyperparathyroidism
(pgs. 289-290) Due to excessive secretion of parathyroid
hormone from the parathyroid glands The four parathyroid glands are located near
the thyroid gland. Parathyroid hormone plays a role in
calcium and phosphorous metabolism. Hyperparathyroidism is characterized by
elevated blood levels of calcium (hypercalcemia) and low levels of blood phosphorous (hypophosphatemia).
18Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hyperparathyroidism (cont.)

•6/27/2011
•4
19Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hyperparathyroidism (cont.)
May be the result of hyperplasia of parathyroid glands, a benign tumor of one or more parathyroid glands, or a malignant parathyroid tumor Found in middle-aged adults Much more common in women than men
Parathyroid hormone increases the uptake of dietary calcium from the gastrointestinal tract and is able to move calcium from bone to circulating blood when necessary.
20Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Featuresof Hyperparathyroidism
Mild cases may be asymptomatic, or may have joint pain or stiffness. Lethargy and coma may occur with severe
disease.
21Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Hyperparathyroidism
Well-defined unilocular or multilocular radiolucencies Microscopically, they appear to be CGCG
(central giant cell granulomas). Bone may have a mottled appearance.
22Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatmentof Hyperparathyroidism
Measurement of parathyroid hormone blood levels May include serum calcium and phosphorous
measurements Treatment is directed at correcting the
cause of increased hormone production. Causes may include tumors, renal disease,
and vitamin D deficiency.
23Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diabetes Mellitus
(pgs. 290-294) A chronic disorder of carbohydrate
metabolism characterized by abnormally high blood glucose levels These result from a lack of insulin, defective
insulin that does not work to lower blood glucose levels, or increased insulin resistance due to obesity.
24Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diabetes Mellitus (cont.)

•6/27/2011
•5
25Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diabetes Mellitus (cont.)
Glucose normally signals beta cells of the pancreas to make insulin. The hormone is then secreted into the
bloodstream to facilitate the uptake of glucose into fat and skeletal muscle.
In the presence of insulin, fat and skeletal muscle cells can use glucose as an energy source.
26Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diabetes Mellitus (cont.)
Without insulin, tissue is broken down to provide energy and weight loss occurs. A severe hyperglycemia can lead to diabetic
coma. Ketone can be produced by the breakdown of
fatty acids.• Ketoacidosis lowers the pH of blood.
Phagocytic activity of macrophages is reduced and neutrophil chemotaxis is delayed.
Collagen production is abnormal.
27Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Types of Diabetes
Insulin-dependent diabetes mellitus Type 1
Non–insulin-dependent diabetes mellitus Type 2
28Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Insulin-Dependent Diabetes Mellitus
(pgs. 291-292) Thought to be an autoimmune disease
Insulin-producing cells of the pancreas are destroyed.
3% to 5% of all diabetic patients have this type. Can occur at any age, the peak is at 20 Acute onset with polydipsia (excessive
thirst and intake of fluid), polyuria (excessive urination), and polyphagia (excessive appetite)
29Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Insulin-Dependent Diabetes Mellitus (cont.)
These patients will require insulin their entire lives. The current approach to management of these
patients involves multiple insulin injections and proper diet, exercise, and frequent determination of blood glucose levels.
But multiple injections of insulin can more readily lead to low blood sugar (hypoglycemia) and insulin shock (severe hypoglycemia).
30Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Insulin-Dependent Diabetes Mellitus (cont.)
New methods of treatment Nasal spray rather than injection Insulin pump
• A backup may be necessary in case the pump fails• Low insulin can lead to ketoacidosis, resulting in
nausea, abdominal cramps, disorientation, and fatigue
•6/27/2011
•6
31Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Non–Insulin-Dependent Diabetes Mellitus
(pgs. 292-294) Characterized by insulin resistance
95% of all diabetic patients have this type of diabetes.
Usually occurs in patients 35 to 40 years of age or older
Many of these individuals are obese Obesity probably decreases the number of
receptors for insulin binding in sensitive tissues like fat or muscle.
Diet and weight reduction may control it in some individuals; others require oral hypoglycemic agents.
32Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
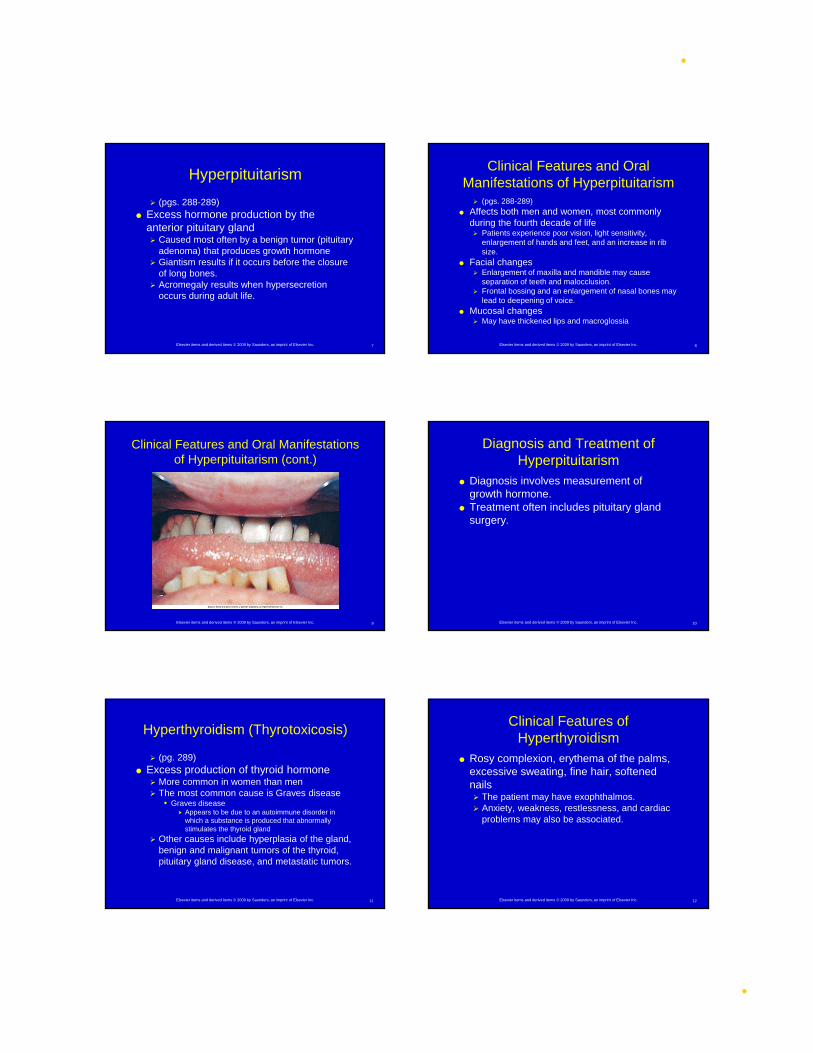
Clinical Features of Non–Insulin-Dependent Diabetes Mellitus
(pg. 293) Atherosclerosis, a thickening of the blood vessel
wall from fibrofatty plaques, can lead to impaired circulation, causing impaired oxygenation and nutrition in tissue. This increases the risk of ulceration and gangrene of the
feet, high blood pressure, kidney failure, and stroke. Diabetic retinopathy in the eye can lead to
blindness. The nervous system may be affected. The person may have decreased resistance to
infection.
33Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features of Non–Insulin-Dependent Diabetes Mellitus (cont.)
34Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
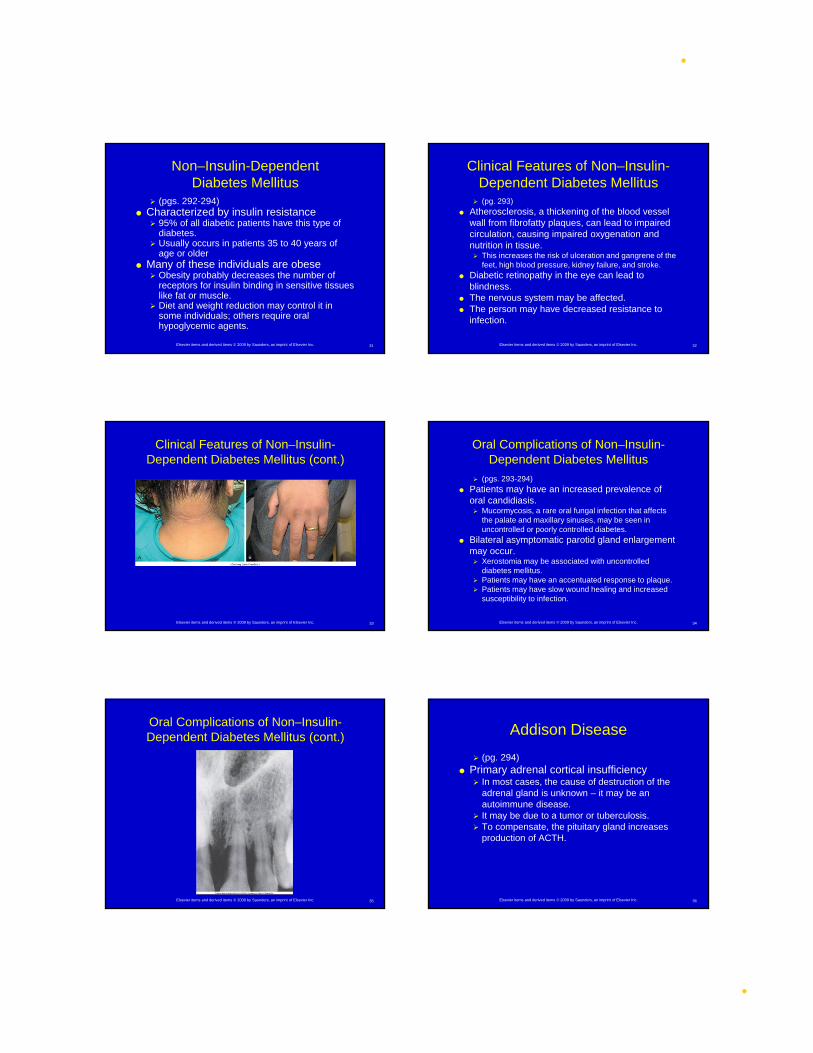
Oral Complications of Non–Insulin-Dependent Diabetes Mellitus
(pgs. 293-294) Patients may have an increased prevalence of
oral candidiasis. Mucormycosis, a rare oral fungal infection that affects
the palate and maxillary sinuses, may be seen in uncontrolled or poorly controlled diabetes.
Bilateral asymptomatic parotid gland enlargement may occur. Xerostomia may be associated with uncontrolled
diabetes mellitus. Patients may have an accentuated response to plaque. Patients may have slow wound healing and increased
susceptibility to infection.
35Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Complications of Non–Insulin-Dependent Diabetes Mellitus (cont.)
36Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Addison Disease
(pg. 294) Primary adrenal cortical insufficiency
In most cases, the cause of destruction of the adrenal gland is unknown – it may be an autoimmune disease.
It may be due to a tumor or tuberculosis. To compensate, the pituitary gland increases
production of ACTH.
•6/27/2011
•7
37Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Addison Disease (cont.)
Clinical features This hormone causes stimulation of
melanocytes. Bronzing of the skin may occur, as well as
melanotic macules on oral mucosa. Treatment
Steroid replacement therapy
38Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Blood Disorders
Disorders of Red Blood Cells and Hemoglobin
Disorders of White Blood Cells Bleeding Disorders
39Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Blood Disorders (cont.)
(pg. 294) (Box 9-1) The complete blood count examines red
blood cells, white blood cells, and platelets. It provides information about the number of
each type of cell, the ratio of types, and the appearance of the cells.
40Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Disorders of Red Blood Cells and Hemoglobin
Anemia Iron Deficiency Anemia Pernicious Anemia Folic Acid and Vitamin B12 Deficiency
Anemia Thalassemia Sickle Cell Anemia Celiac Sprue Aplastic Anemia Polycythemia
41Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Anemia
(pgs. 294-295) A reduction in the oxygen-carrying
capacity of blood Most often related to a decrease in the number
of circulating red blood cells• Nutritional anemias
A deficiency in a substance required for the normal development of red blood cells, commonly vitamins
• Suppression of bone marrow stem cells
42Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Anemia (cont.)
Clinical features Pallor of skin and oral mucosa Angular cheilitis Erythema and atrophy of oral mucosa Loss of filiform and fungiform papillae on the
dorsum of the tongue
•6/27/2011
•8
43Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Iron Deficiency Anemia
(pg. 295) An insufficient amount of iron is supplied to bone
marrow for red blood cell development. May occur as a result of deficient iron intake, blood loss
from heavy menstrual bleeding or chronic gastrointestinal bleeding, poor iron absorption, or an increased requirement for iron in situations such as pregnancy or infancy
Plummer-Vinson syndrome may result from long standing iron deficiency anemia. Includes dysphagia, atrophy of the upper alimentary
tract, and a predisposition to developing oral cancer
44Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
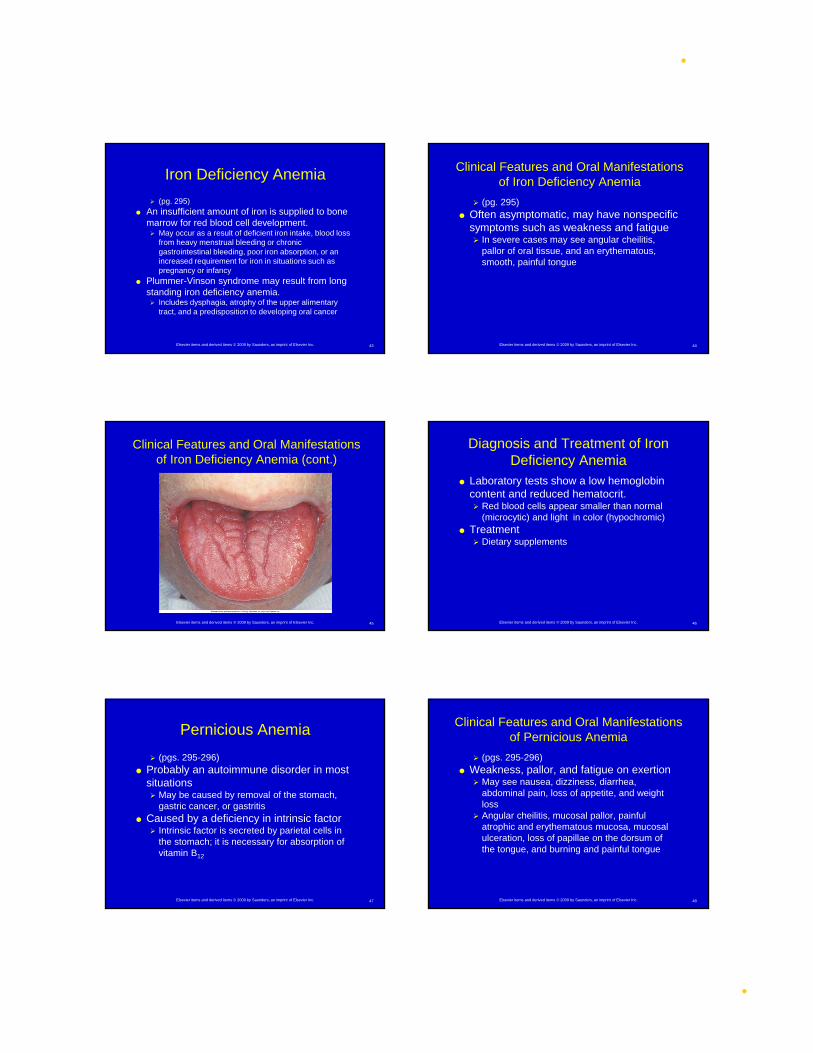
Clinical Features and Oral Manifestations of Iron Deficiency Anemia
(pg. 295) Often asymptomatic, may have nonspecific
symptoms such as weakness and fatigue In severe cases may see angular cheilitis,
pallor of oral tissue, and an erythematous, smooth, painful tongue
45Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Iron Deficiency Anemia (cont.)
46Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Iron Deficiency Anemia
Laboratory tests show a low hemoglobin content and reduced hematocrit. Red blood cells appear smaller than normal
(microcytic) and light in color (hypochromic) Treatment
Dietary supplements
47Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Pernicious Anemia
(pgs. 295-296) Probably an autoimmune disorder in most
situations May be caused by removal of the stomach,
gastric cancer, or gastritis Caused by a deficiency in intrinsic factor
Intrinsic factor is secreted by parietal cells in the stomach; it is necessary for absorption of vitamin B12
48Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
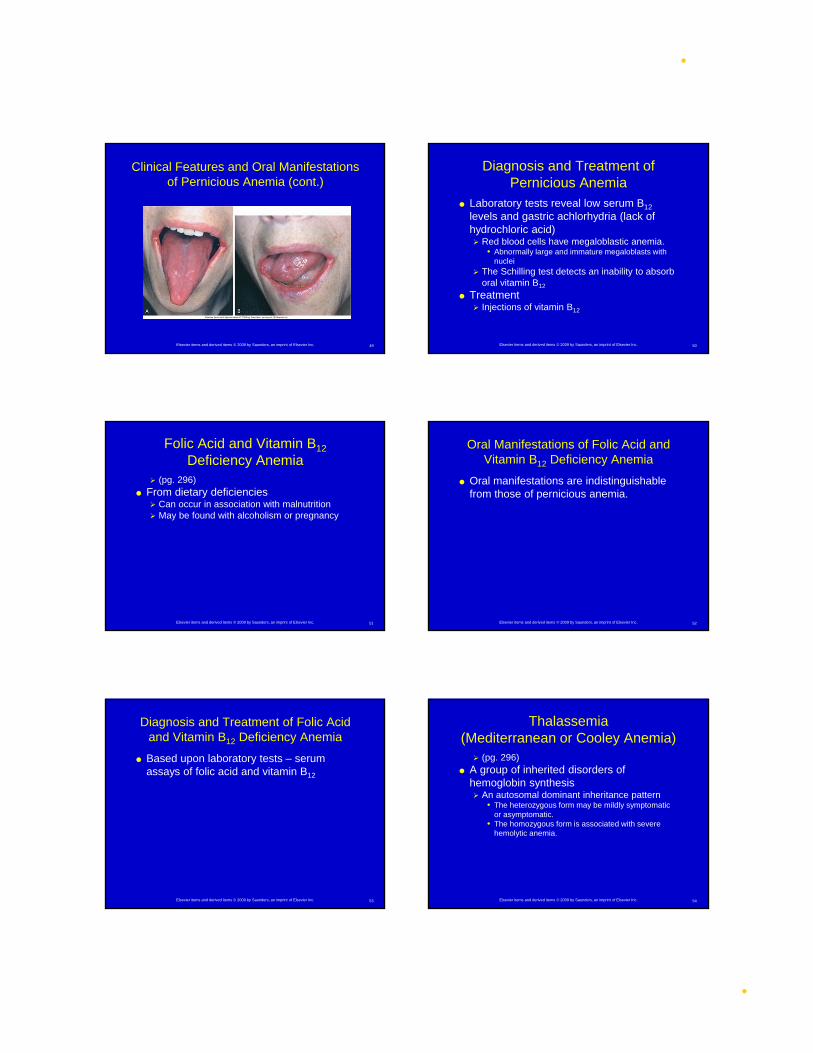
Clinical Features and Oral Manifestations of Pernicious Anemia
(pgs. 295-296) Weakness, pallor, and fatigue on exertion
May see nausea, dizziness, diarrhea, abdominal pain, loss of appetite, and weight loss
Angular cheilitis, mucosal pallor, painful atrophic and erythematous mucosa, mucosal ulceration, loss of papillae on the dorsum of the tongue, and burning and painful tongue
•6/27/2011
•9
49Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Pernicious Anemia (cont.)
50Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Pernicious Anemia
Laboratory tests reveal low serum B12
levels and gastric achlorhydria (lack of hydrochloric acid) Red blood cells have megaloblastic anemia.
• Abnormally large and immature megaloblasts with nuclei
The Schilling test detects an inability to absorb oral vitamin B12
Treatment Injections of vitamin B12
51Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Folic Acid and Vitamin B12
Deficiency Anemia (pg. 296)
From dietary deficiencies Can occur in association with malnutrition May be found with alcoholism or pregnancy
52Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Folic Acid and Vitamin B12 Deficiency Anemia
Oral manifestations are indistinguishable from those of pernicious anemia.
53Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Folic Acid and Vitamin B12 Deficiency Anemia
Based upon laboratory tests – serum assays of folic acid and vitamin B12
54Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Thalassemia (Mediterranean or Cooley Anemia) (pg. 296)
A group of inherited disorders of hemoglobin synthesis An autosomal dominant inheritance pattern
• The heterozygous form may be mildly symptomatic or asymptomatic.
• The homozygous form is associated with severe hemolytic anemia.

•6/27/2011
•10
55Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Thalassemia (pg. 296)
Yellow skin pallor, fever, malaise, and weakness The face includes prominent cheekbones,
depression of the bridge of the nose, a prominent maxilla, and protrusion or flaring of maxillary anterior teeth.
Radiographs may show a “salt and pepper” pattern. Some trabeculae are prominent, and others
are blurred.
56Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Treatment of Thalassemia
Experimental May include blood transfusions and
splenectomy Poor prognosis
57Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Sickle Cell Anemia
(pg. 297) An inherited blood disorder
When someone is heterozygous, it is called sickle cell trait.
When someone is homozygous, they are much more severely affected.
Occurs before age 30 and is more common in women than in men
The red blood cells develop a sickle shape when there is decreased oxygen. This can be triggered by exercise, exertion,
administration of a general anesthetic, pregnancy, or even sleep.
58Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Sickle Cell Anemia
(pg. 297) The person has weakness, shortness of
breath, fatigue, joint pain, and nausea. Radiographic
There is a loss of trabeculation, and large, irregular marrow spaces appear.
A “hair-on-end” pattern may be seen in the skull.
59Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Sickle Cell Anemia (cont.)
60Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Sickle Cell Anemia
(pg. 297) The sickle-shaped cells may be seen on a
blood smear. The number of red blood cells is usually low,
as is the hemoglobin content. Treatment is largely supportive, involves
administration of oxygen and IV and oral fluid.

•6/27/2011
•11
61Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Sickle Cell Anemia (cont.)
62Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Celiac Sprue
(pgs. 297-298) A chronic disorder
Sensitivity to wheat gluten Ingestion causes injury to intestinal
mucosa. This injury may cause malabsorption of
nutrients and a resulting anemia.
63Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Celiac Sprue
Symptoms include diarrhea, nervousness, and paresthesia. Painful, burning tongue, atrophy of papillae,
and ulceration of oral mucosa
64Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Celiac Sprue
The patient must avoid wheat gluten. Oral manifestations resolve when the systemic
disease is controlled.
65Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Aplastic Anemia
(pgs. 298-299) A severe depression of bone marrow
activity causes a decrease in all circulating blood cells. – pancytopenia Primary aplastic anemia – the cause is
unknown Secondary aplastic anemia – a result of a drug
or chemical agent
66Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Aplastic Anemia (cont.)
•6/27/2011
•12
67Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
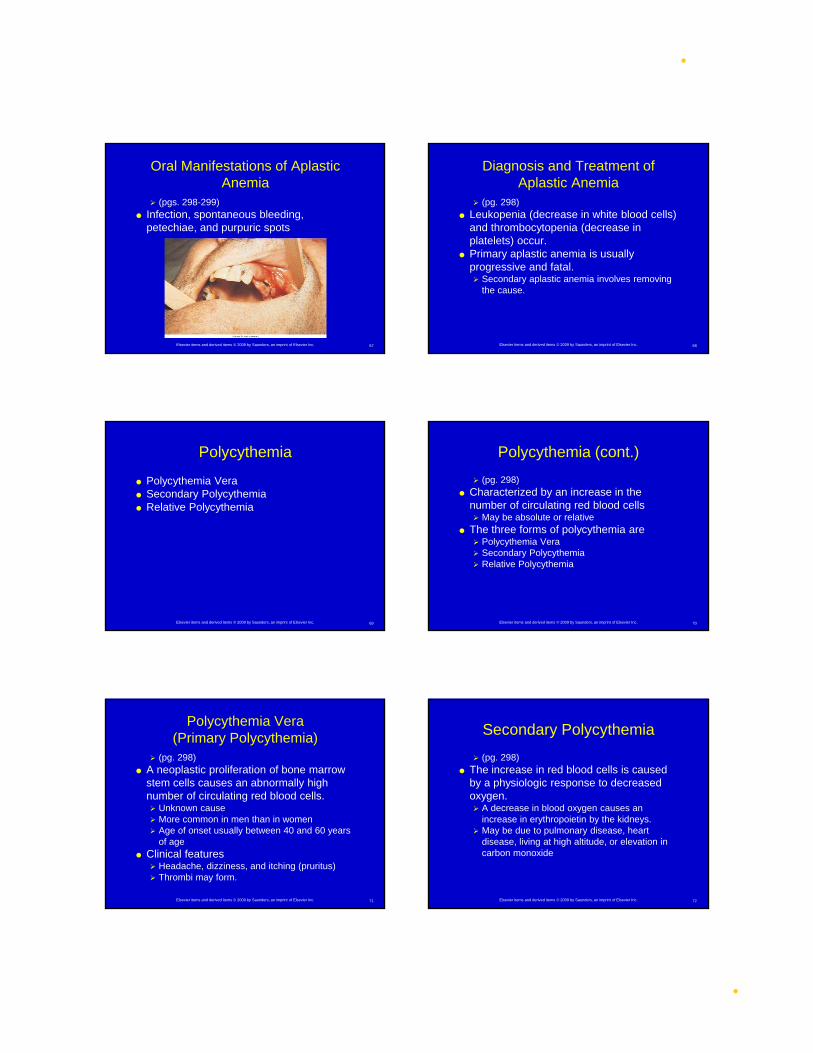
Oral Manifestations of Aplastic Anemia
(pgs. 298-299) Infection, spontaneous bleeding,
petechiae, and purpuric spots
68Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Aplastic Anemia
(pg. 298) Leukopenia (decrease in white blood cells)
and thrombocytopenia (decrease in platelets) occur.
Primary aplastic anemia is usually progressive and fatal. Secondary aplastic anemia involves removing
the cause.
69Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Polycythemia
Polycythemia Vera Secondary Polycythemia Relative Polycythemia
70Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Polycythemia (cont.)
(pg. 298) Characterized by an increase in the
number of circulating red blood cells May be absolute or relative
The three forms of polycythemia are Polycythemia Vera Secondary Polycythemia Relative Polycythemia
71Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Polycythemia Vera (Primary Polycythemia)
(pg. 298) A neoplastic proliferation of bone marrow
stem cells causes an abnormally high number of circulating red blood cells. Unknown cause More common in men than in women Age of onset usually between 40 and 60 years
of age Clinical features
Headache, dizziness, and itching (pruritus) Thrombi may form.
72Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Secondary Polycythemia
(pg. 298) The increase in red blood cells is caused
by a physiologic response to decreased oxygen. A decrease in blood oxygen causes an
increase in erythropoietin by the kidneys. May be due to pulmonary disease, heart
disease, living at high altitude, or elevation in carbon monoxide
•6/27/2011
•13
73Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Relative Polycythemia
(pg. 298) Caused by a decrease in plasma volume
Causes may include diuretics, vomiting, diarrhea, or excessive sweating.
Most patients are middle-aged white men under physiologic stress, mildly overweight, hypertensive, and heavy smokers.
74Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Polycythemia
(pg. 299) The oral mucosa may appear deep red to
purple; the gingiva may be edematous and bleed easily. Submucosal petechiae, ecchymosis, and
hematoma formation may be present.
75Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Polycythemia
(pg. 299) Laboratory testing and measurement of
hemoglobin and hematocrit May include removal of causative factors,
chemotherapy, and phlebotomy
76Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Disorders of White Blood Cells
Agranulocytosis Cyclic Neutropenia Leukemia
77Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Disorders of White Blood Cells (cont.)
(pgs. 299-301) Three groups of white blood cells are
found in circulation. Granulocytes
• Neutrophils (PMNs), eosinophils, and basophils
Lymphocytes Monocytes
78Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Agranulocytosis
(pg. 300) A significant reduction in circulating
neutrophils Leukopenia – an abnormally low white blood
cell count Neutropenia – a reduction in the number of
circulating neutrophils
•6/27/2011
•14
79Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Agranulocytosis (cont.)
Can result from a problem in development of neutrophils or accelerated destruction of neutrophils Primary – the cause is unknown, may be an
immunologic disorder Secondary – a result of chemicals or drugs
80Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Agranulocytosis (pg. 300)
Sudden onset of fever, chills, jaundice, weakness, and sore throat Oral infection
81Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Agranulocytosis
(pg. 300) Laboratory testing Marked reduction in WBC count Treatment
Transfusions, antibiotics Removal of the cause for the secondary form
82Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Cyclic Neutropenia
(pg. 300) A cyclic decrease in the number of
circulating neutrophilic leukocytes Discussed on pages 208-209
83Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Leukemia
(pgs. 300-301) (Box 9-2) Malignant neoplasms of hematopoietic
stem cells Characterized by an excessive number of
abnormal white blood cells in circulating blood Unknown cause; some are investigating
oncogenic viruses There are many different types
categorized as to whether they are acute or chronic.
84Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Acute Leukemias
(pgs. 300-301) Characterized by very immature cells and
a rapidly fatal course if not treated Acute lymphoblastic leukemia – involves
immature lymphocytes• Primarily affects children and young adults• Good prognosis
Acute myeloblastic leukemia – involves immature granulocytes
• Primarily affects adolescents and young adults.• Prognosis is not as good.

•6/27/2011
•15
85Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features of Acute Leukemias
(pg. 301) Weakness, fever, enlargement of lymph
nodes, and bleeding
86Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Acute Leukemias
Gingival enlargement Oral infection Bleeding gums, petechiae and ecchymosis
87Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Acute Leukemias
Laboratory findings include elevated white blood cell count, anemia, and low platelet count
Treatment Bone marrow transplant
88Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Chronic Leukemias
(pg. 301) Slow onset
Primarily affect adults
89Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical Features and Oral Manifestations of Chronic Leukemias
Easy fatigability, weakness, weight loss, anorexia
Pallor of lips and gingiva, gingival enlargement, petechiae and ecchymosis, gingival bleeding
90Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Chronic Leukemias
High white blood cell count Treatment
Bone marrow transplant
•6/27/2011
•16
91Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Bleeding Disorders
Hemostasis Purpura Hemophilia
92Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hemostasis (cont.)
93Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
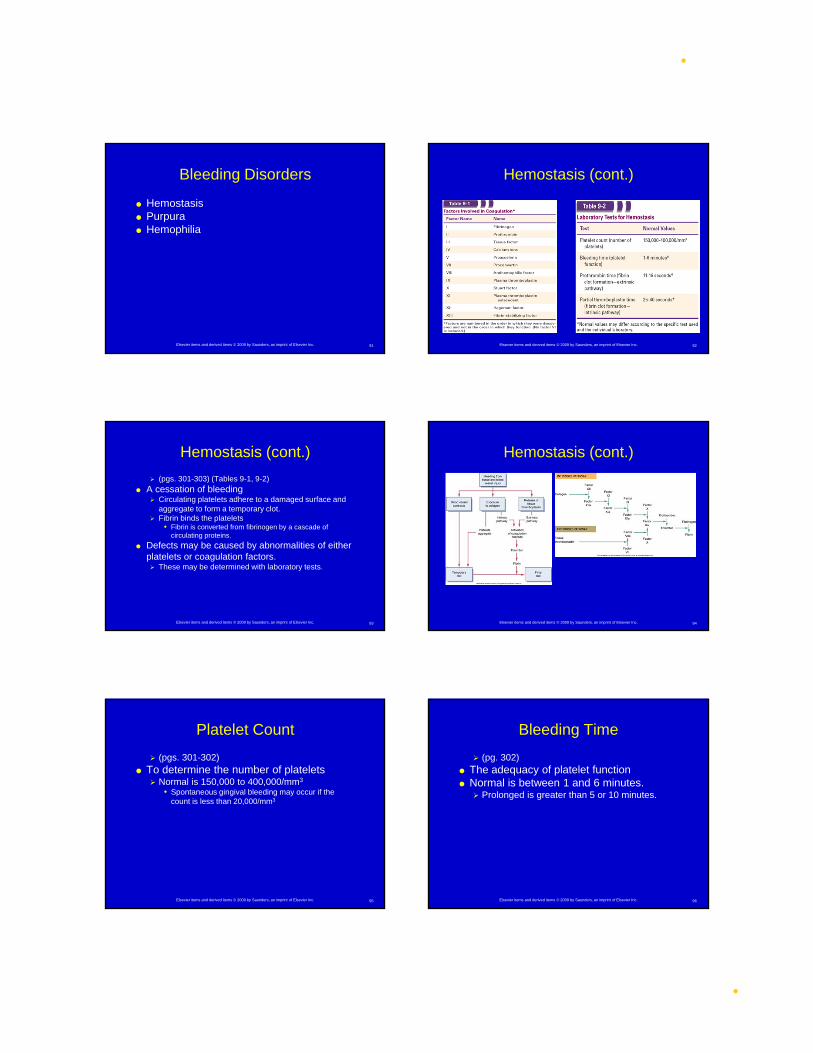
Hemostasis (cont.)
(pgs. 301-303) (Tables 9-1, 9-2) A cessation of bleeding
Circulating platelets adhere to a damaged surface and aggregate to form a temporary clot.
Fibrin binds the platelets• Fibrin is converted from fibrinogen by a cascade of
circulating proteins.
Defects may be caused by abnormalities of either platelets or coagulation factors. These may be determined with laboratory tests.
94Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hemostasis (cont.)
95Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Platelet Count
(pgs. 301-302) To determine the number of platelets
Normal is 150,000 to 400,000/mm3
• Spontaneous gingival bleeding may occur if the count is less than 20,000/mm3
96Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Bleeding Time
(pg. 302) The adequacy of platelet function Normal is between 1 and 6 minutes.
Prolonged is greater than 5 or 10 minutes.

•6/27/2011
•17
97Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Prothrombin Time (PT)
(pgs. 302-303) The ability to form a clot
Normal is usually between 11 and 16 seconds. INR is the ratio of PT to thromboplastin activity. Values less than 3 are considered normal.
• Patients on anticoagulants may have INR values of 4 to 5.
98Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Partial Thromboplastin Time (PTT)
(pg. 303) Measures the other way by which clot
formation occurs A normal PTT is usually 25 to 40 seconds.
Prolongation to 45 or 50 seconds may be associated with bleeding problems.
Over 50 seconds may be severe
99Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Purpura
(pgs. 303-304) A reddish-blue or purplish discoloration of
skin or mucosa from spontaneous extravasation of blood May be due to a defect or deficiency in blood
platelets Blood may ooze from gingival margins.
100Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Thrombocytopenic Purpura
(pgs. 303-304) A bleeding disorder that results from a
severe reduction in circulating platelets Idiopathic thrombocytopenic purpura
• If the cause is unknown
Immune thrombocytopenia• An autoimmune type of process
Secondary thrombocytopenic purpura• Often associated with drugs
101Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Clinical and Oral Manifestations of Thrombocytopenic Purpura
Spontaneous purpuric or hemorrhagic lesions on the skin Patients bruise easily, may have blood in urine,
and have frequent nosebleeds.
102Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Thrombocytopenic Purpura
Laboratory tests show a significant decrease in platelets.
Treatment May include transfusions, corticosteroids, and
splenectomy

•6/27/2011
•18
103Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Nonthrombocytopenic Purpura
(pg. 304) Bleeding disorders that can result from
either a defect in capillary walls or disorders of platelet function Vitamin C deficiency and infections or
chemicals and allergy may be the cause of alterations in vascular walls.
Drugs, allergy, and autoimmune disease may cause disorders of platelet function.
Von Willebrand disease is an autosomal dominant disorder of platelet function.
104Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Nonthrombocytopenic Purpura
Spontaneous gingival bleeding, petechiae, ecchymoses, and hemorrhagic blisters
105Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Nonthrombocytopenic Purpura
Systemic corticosteroids, splenectomy, and discontinuation of the causative agent
106Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Hemophilia
(pg. 304) A disorder of blood coagulation
Results in severely prolonged clotting time Due to a deficiency in plasma proteins involved
in coagulation
107Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Types of Hemophilia
(pg. 304) The two most common types are type A
and type B. Transmitted as X-linked diseases through an
unaffected carrier daughter to a son• Type A
Caused by a deficiency of plasma thromboplastinogen or factor VIII
• Type B Christmas disease Less common, the clotting defect is plasma
thromboplastin or factor IX
108Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Hemophilia
Spontaneous gingival bleeding, petechiae, and ecchymosis
•6/27/2011
•19
109Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Diagnosis and Treatment of Hemophilia
The bleeding time and PT in hemophilia are normal; the PTT is prolonged.
Diagnosis involves identifying the missing factor; treatment involves replacing it.
110Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Immunodeficiency
(pgs. 304-305) Can involve the different parts of the
immune system either alone or together May involve a deficiency in cell-mediated or
humoral immunity May involve deficiency in phagocytosis
Divided into Primary immunodeficiency of genetic origin Secondary immunodeficiency from another
underlying disorder
111Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Primary Immunodeficiencies
(pg. 305) Of genetic origin
May involve B cells, T cells, or both Very rare
Bruton disease (X linked congenital agammaglobulinemia)
DiGeorge syndrome (thymic hypoplasia) Severe combined immunodeficiency
112Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Secondary Immunodeficiencies (Cont.)
113Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Secondary Immunodeficiencies (Cont.)
(pg. 305) (Table 9-3) Occur as the result of an underlying
disorder May be malnutrition, viral infection, cancer,
renal disease and Hodgkin’s disease May occur with immunosuppressive drugs,
drugs used along with radiation, chemotherapy
114Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Therapy for Oral Cancer
(pgs. 305-307) Radiation Therapy Chemotherapy
•6/27/2011
•20
115Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Oral Manifestations of Therapy for Oral Cancer (cont.)
(pg. 305) Oral cancer can be treated with surgery,
radiation therapy, or chemotherapy, or a combination.
116Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
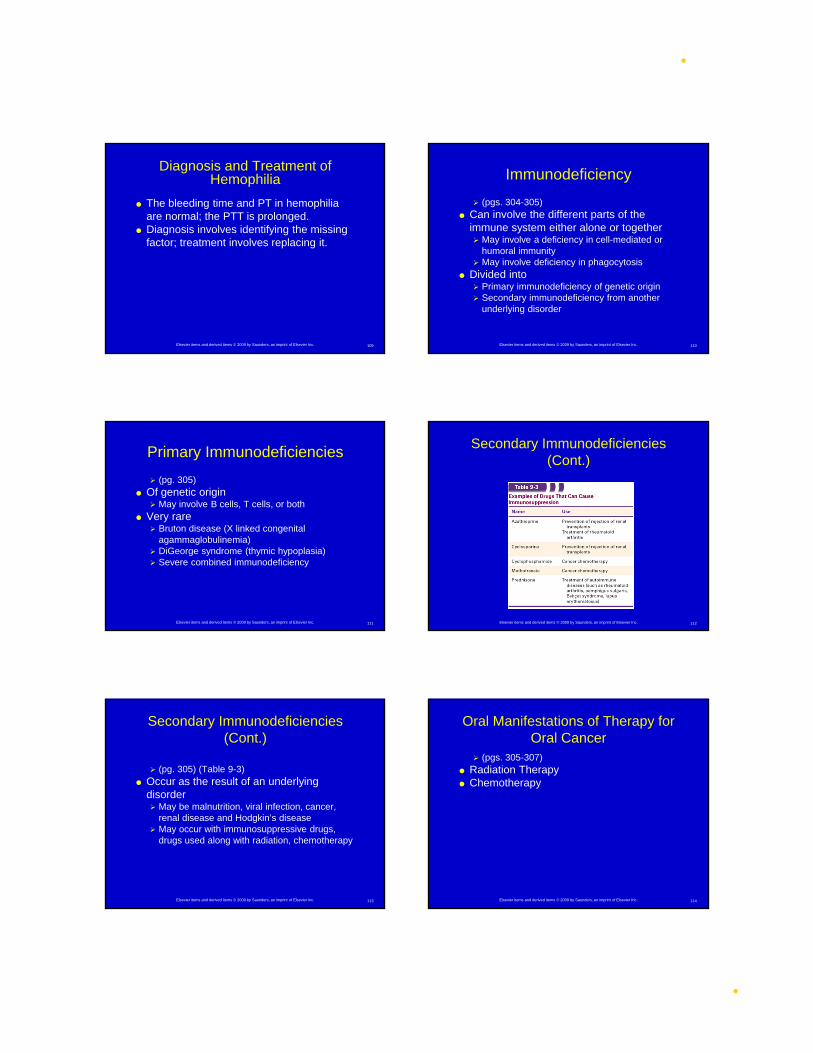
Radiation Therapy
(pgs. 305-306) The patient often experiences
mucositis during radiation therapy. Mucositis begins about the second
week of therapy and subsides a few weeks after its completion.
It is painful and appears as an erythematous and ulcerated mucosa.
The patients may have difficulty eating, pain on swallowing, and loss of taste.
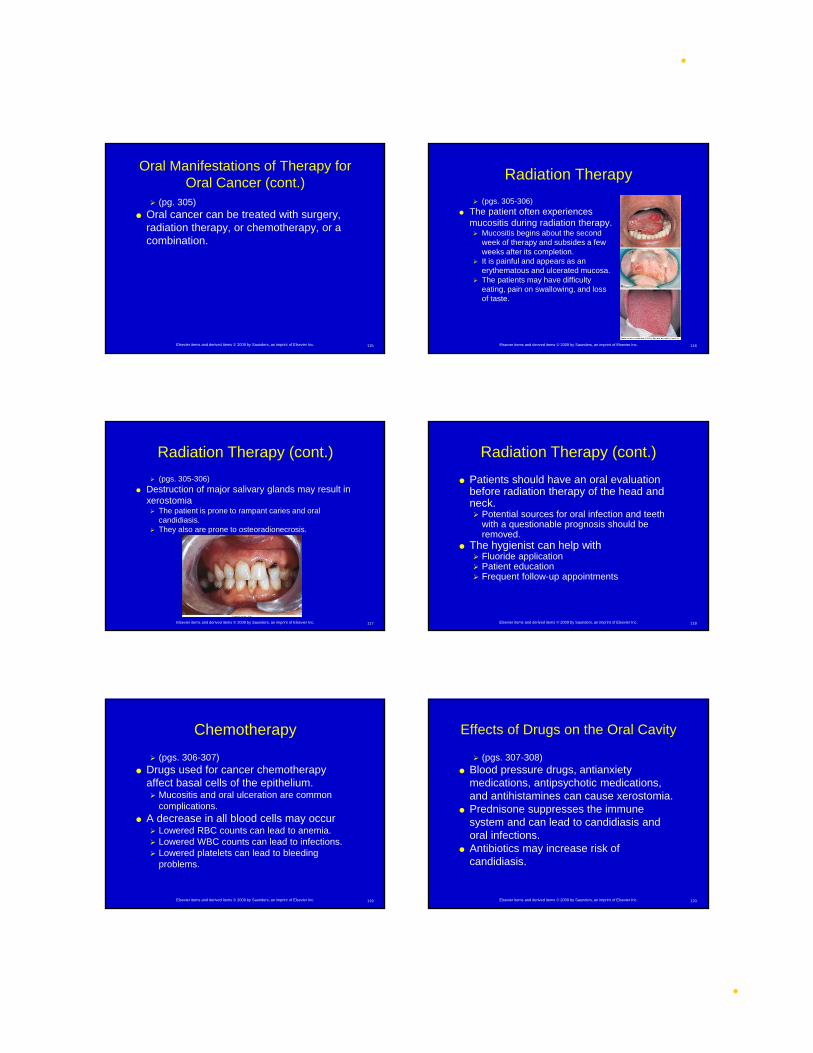
117Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
(pgs. 305-306) Destruction of major salivary glands may result in
xerostomia The patient is prone to rampant caries and oral
candidiasis. They also are prone to osteoradionecrosis.
Radiation Therapy (cont.)
118Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Patients should have an oral evaluation before radiation therapy of the head and neck. Potential sources for oral infection and teeth
with a questionable prognosis should be removed.
The hygienist can help with Fluoride application Patient education Frequent follow-up appointments
Radiation Therapy (cont.)
119Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Chemotherapy
(pgs. 306-307) Drugs used for cancer chemotherapy
affect basal cells of the epithelium. Mucositis and oral ulceration are common
complications. A decrease in all blood cells may occur
Lowered RBC counts can lead to anemia. Lowered WBC counts can lead to infections. Lowered platelets can lead to bleeding
problems.
120Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Effects of Drugs on the Oral Cavity
(pgs. 307-308) Blood pressure drugs, antianxiety
medications, antipsychotic medications, and antihistamines can cause xerostomia.
Prednisone suppresses the immune system and can lead to candidiasis and oral infections.
Antibiotics may increase risk of candidiasis.
•6/27/2011
•21
121Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Effects of Drugs on the Oral Cavity (cont.)
122Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
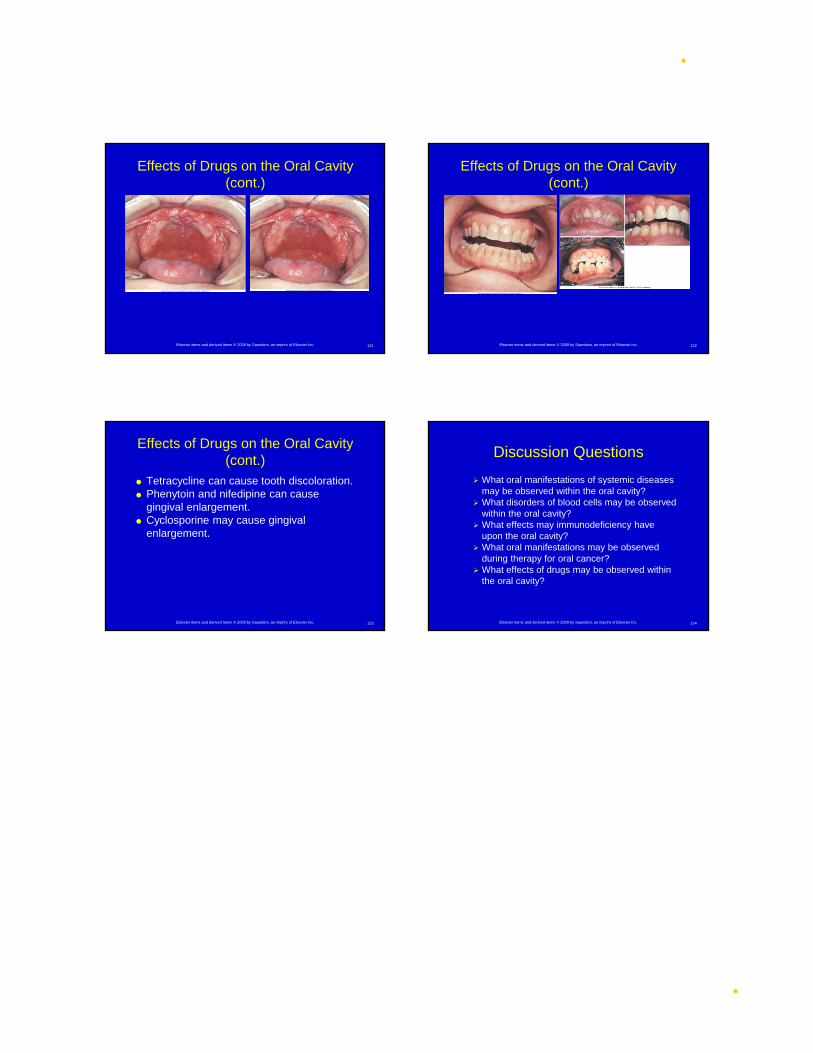
Effects of Drugs on the Oral Cavity (cont.)
123Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Effects of Drugs on the Oral Cavity (cont.)
Tetracycline can cause tooth discoloration. Phenytoin and nifedipine can cause
gingival enlargement. Cyclosporine may cause gingival
enlargement.
124Elsevier items and derived items © 2009 by Saunders, an imprint of Elsevier Inc.
Discussion Questions
What oral manifestations of systemic diseases may be observed within the oral cavity?
What disorders of blood cells may be observed within the oral cavity?
What effects may immunodeficiency have upon the oral cavity?
What oral manifestations may be observed during therapy for oral cancer?
What effects of drugs may be observed within the oral cavity?