Embed Size (px)
Citation preview
Outcomes in Behavioral Health
Thomas Smith, MD
Associate Medical Director, NYS Office of Mental Health
Special Lecturer, Columbia University Medical Center
2
OverviewWith the increasing emphasis on value based payment (VBP) strategies,
behavioral health providers need to consider measuring their care and
outcomes. This session will:
• Review process and outcome measures commonly used in oversight,
quality improvement, and accountability (e.g., VBP) programs involving
behavioral health.
• Identify key decisions and activities that behavioral health providers must
pursue in adopting a measurement approach.
• Provide an overview of a tracking system that ACL members are currently
using in the Central region to look at how housing programs impact
hospital usage for people in the behavioral health system.
3
Key Recommendations
• Understand where your agency fits in the larger system of care.
• Know the oversight and payment authorities’ priorities for the system
of care.
• Align some (not all!) of your agency’s priorities and strengths with the
system priorities
• Implement tracking and reporting of key agency practices that align
with the system priorities.
• Have summary reports ready for external audiences—brag about
what you do well.
44
Why do we measure quality and performance?
1. Monitor and understand systems, providers, and populations
2. Internal Quality Improvementa. To support point-of-care decision making
b. For provider continuous quality improvement projects
c. Managed care organization performance improvement
3. Accountabilitya. Public reporting
b. Value-based payment
55
What do we measure?
1. System of Care priorities (understanding)
2. Payers’ priorities (accountability)
3. Provider priorities (quality improvement)
66
System Priorities: Transforming the NYS Medicaid Program
• 2012: Health HomesGoal: Comprehensive care management services for high-need populations
• 2014: Delivery System Reform Incentive Payment (DSRIP) ProgramGoal: Shift locus of care from acute to community; reduce unnecessary readmissions
• 2015: Medicaid Managed Care: Capitated Behavioral HealthGoal: Fully capitated system with managed care plans overseeing integrated behavioral and general medical care.Up to 150,000 members enrolling in fully integrated special needs plans for individuals with serious BH conditions(HARPs)
• 2015: Advanced Primary Care (APC)Goal: 80% of population receives care in APC setting with focus on prevention and coordinated care as well asthrough an alternative payment model
• 2017: Value-Based Payment ModelsGoal: Shift reimbursement model from volume to value: by 2020, 80% of Medicaid Managed Care providerpayments will be in shared savings arrangements, with 35% of those including downside risk to providers
7
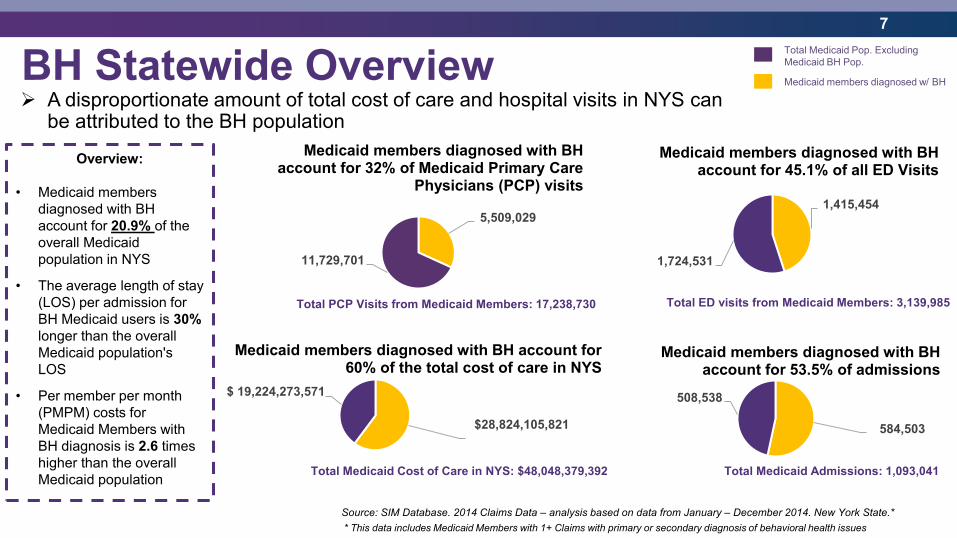
BH Statewide Overview A disproportionate amount of total cost of care and hospital visits in NYS can
be attributed to the BH population
Overview:
• Medicaid members
diagnosed with BH
account for 20.9% of the
overall Medicaid
population in NYS
• The average length of stay
(LOS) per admission for
BH Medicaid users is 30%
longer than the overall
Medicaid population's
LOS
• Per member per month
(PMPM) costs for
Medicaid Members with
BH diagnosis is 2.6 times
higher than the overall
Medicaid population
* This data includes Medicaid Members with 1+ Claims with primary or secondary diagnosis of behavioral health issues
$28,824,105,821
$ 19,224,273,571
Medicaid members diagnosed with BH account for 60% of the total cost of care in NYS
1,415,454
1,724,531
Medicaid members diagnosed with BH account for 45.1% of all ED Visits
584,503
508,538
Medicaid members diagnosed with BH account for 53.5% of admissions
5,509,029
11,729,701
Medicaid members diagnosed with BH account for 32% of Medicaid Primary Care
Physicians (PCP) visits
Total PCP Visits from Medicaid Members: 17,238,730 Total ED visits from Medicaid Members: 3,139,985
Total Medicaid Cost of Care in NYS: $48,048,379,392 Total Medicaid Admissions: 1,093,041
Source: SIM Database. 2014 Claims Data – analysis based on data from January – December 2014. New York State.*
Total Medicaid Pop. Excluding
Medicaid BH Pop.
Medicaid members diagnosed w/ BH
8
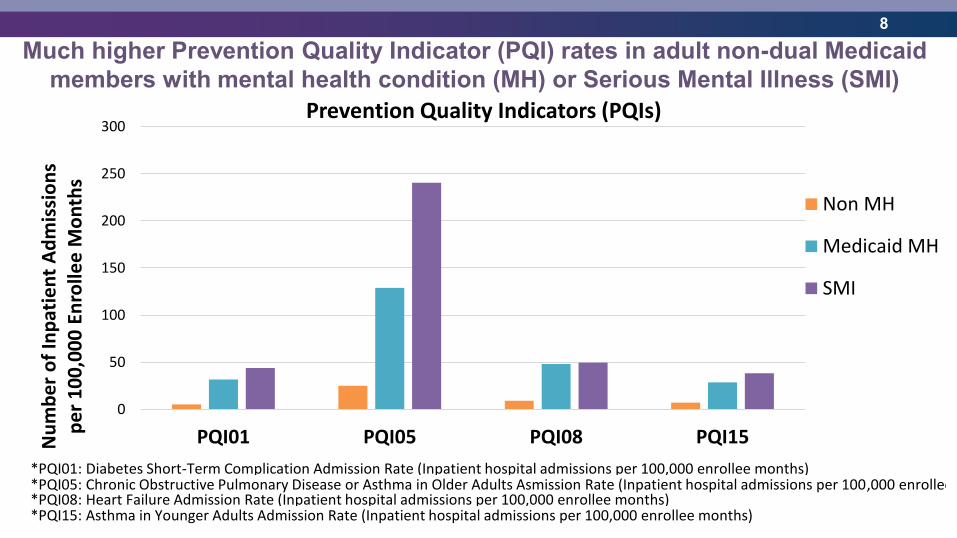
Much higher Prevention Quality Indicator (PQI) rates in adult non-dual Medicaid
members with mental health condition (MH) or Serious Mental Illness (SMI)
0
50
100
150
200
250
300
PQI01 PQI05 PQI08 PQI15Nu
mb
er
of
Inp
atie
nt
Ad
mis
sio
ns
pe
r 1
00
,00
0 E
nro
llee
Mo
nth
s
Prevention Quality Indicators (PQIs)
Non MH
Medicaid MH
SMI
*PQI01: Diabetes Short-Term Complication Admission Rate (Inpatient hospital admissions per 100,000 enrollee months)*PQI05: Chronic Obstructive Pulmonary Disease or Asthma in Older Adults Asmission Rate (Inpatient hospital admissions per 100,000 enrollee months)*PQI08: Heart Failure Admission Rate (Inpatient hospital admissions per 100,000 enrollee months)*PQI15: Asthma in Younger Adults Admission Rate (Inpatient hospital admissions per 100,000 enrollee months)
9
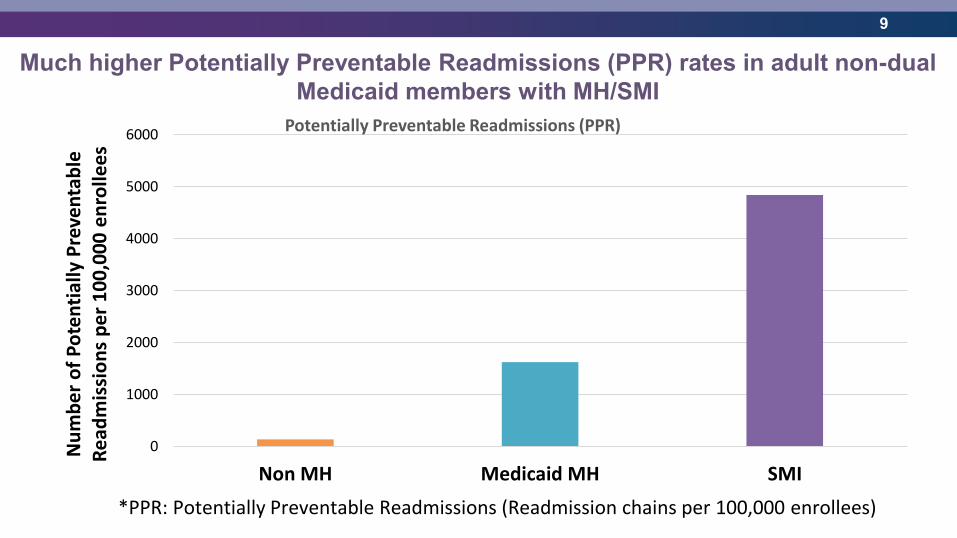
Much higher Potentially Preventable Readmissions (PPR) rates in adult non-dual
Medicaid members with MH/SMI
0
1000
2000
3000
4000
5000
6000
Non MH Medicaid MH SMI
Nu
mb
er
of
Po
ten
tial
ly P
reve
nta
ble
R
ead
mis
sio
ns
pe
r 1
00
,00
0 e
nro
llee
s
*PPR: Potentially Preventable Readmissions (Readmission chains per 100,000 enrollees)
Potentially Preventable Readmissions (PPR)
10
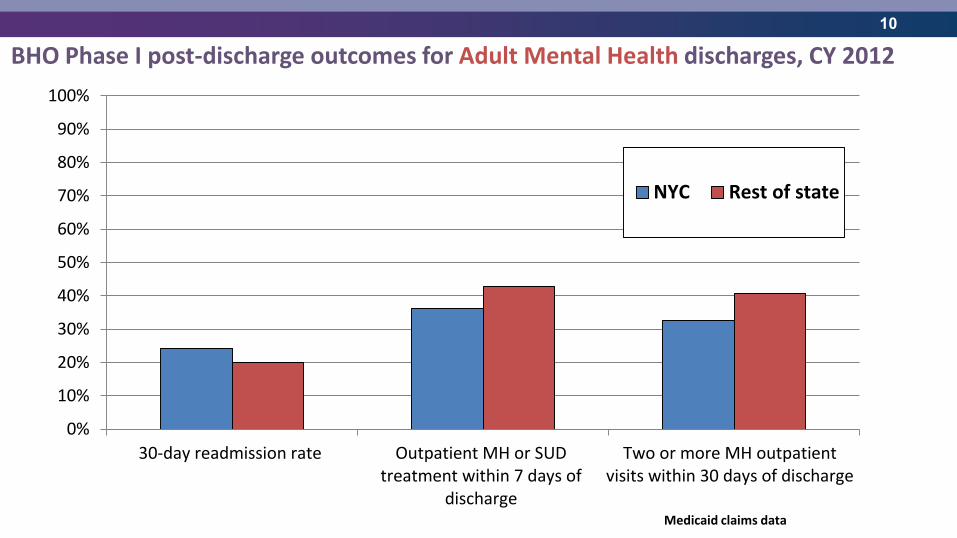
BHO Phase I post-discharge outcomes for Adult Mental Health discharges, CY 2012
Medicaid claims data
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
30-day readmission rate Outpatient MH or SUDtreatment within 7 days of
discharge
Two or more MH outpatientvisits within 30 days of discharge
NYC Rest of state
11
• A Five-Year Roadmap outlining NYS’ plan for Medicaid Payment
Reform was required by the MRT Waiver.
• By DSRIP Year 5 (2020), all Managed Care Organizations (MCOs)
must employ non fee-for-service payment systems that reward value
over volume for at least 80-90% of their provider payments (outlined
in the Special Terms and Conditions of the waiver).
• If Roadmap goals are not met, overall DSRIP dollars from CMS to
NYS will be significantly reduced.
Recap: Moving Towards VBP
12
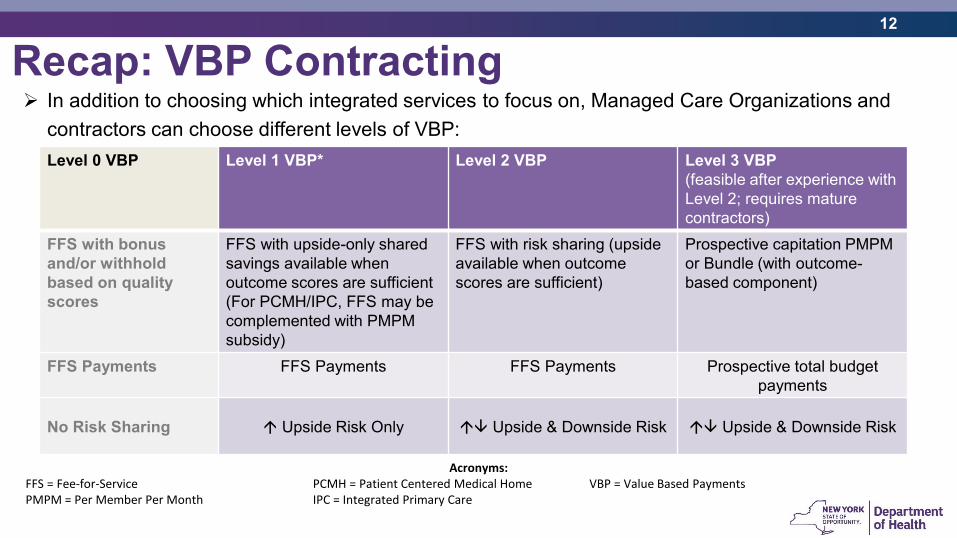
In addition to choosing which integrated services to focus on, Managed Care Organizations and
contractors can choose different levels of VBP:
Level 0 VBP Level 1 VBP* Level 2 VBP Level 3 VBP
(feasible after experience with
Level 2; requires mature
contractors)
FFS with bonus
and/or withhold
based on quality
scores
FFS with upside-only shared
savings available when
outcome scores are sufficient
(For PCMH/IPC, FFS may be
complemented with PMPM
subsidy)
FFS with risk sharing (upside
available when outcome
scores are sufficient)
Prospective capitation PMPM
or Bundle (with outcome-
based component)
FFS Payments FFS Payments FFS Payments Prospective total budget
payments
No Risk Sharing Upside Risk Only Upside & Downside Risk Upside & Downside Risk
Acronyms: FFS = Fee-for-Service PCMH = Patient Centered Medical Home VBP = Value Based PaymentsPMPM = Per Member Per Month IPC = Integrated Primary Care
Recap: VBP Contracting
1313
NYS OMH Mental Health System Transformation Goals
1. Shift locus of care from acute to community-based (outpatient) services
2. Improve early identification and intervention for at-risk populations and for active MH conditions
3. Improve individuals’ experience of health care
4. Improve both general medical health and functional outcomes for individuals with SMI
5. Increase % of individuals identified as in recovery
1414
NYS DOH
Clinical Advisory Groups (CAGs)
15 1515
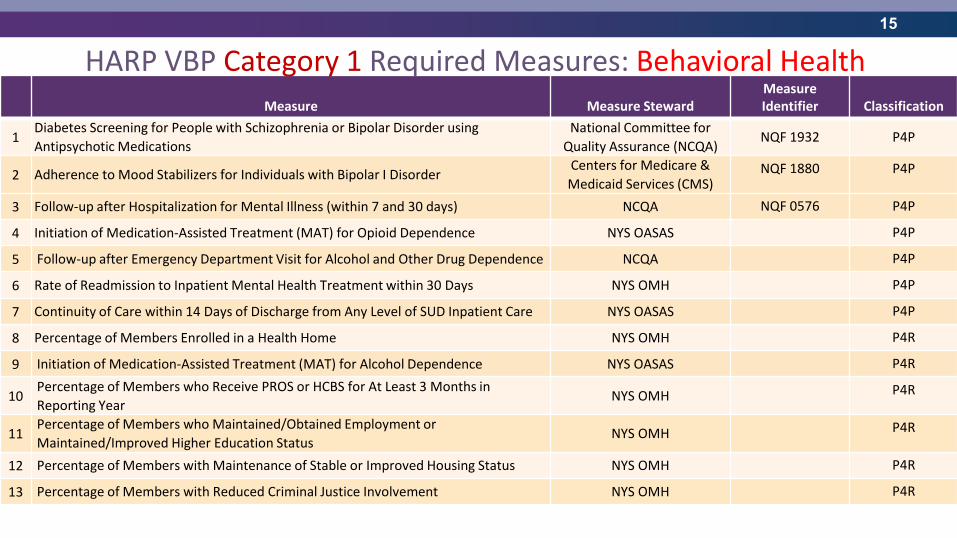
Measure Measure StewardMeasure Identifier Classification
1Diabetes Screening for People with Schizophrenia or Bipolar Disorder using
Antipsychotic Medications
National Committee for
Quality Assurance (NCQA)NQF 1932 P4P
2 Adherence to Mood Stabilizers for Individuals with Bipolar I DisorderCenters for Medicare &
Medicaid Services (CMS)NQF 1880 P4P
3 Follow-up after Hospitalization for Mental Illness (within 7 and 30 days) NCQA NQF 0576 P4P
4 Initiation of Medication-Assisted Treatment (MAT) for Opioid Dependence NYS OASAS P4P
5 Follow-up after Emergency Department Visit for Alcohol and Other Drug Dependence NCQA P4P
6 Rate of Readmission to Inpatient Mental Health Treatment within 30 Days NYS OMH P4P
7 Continuity of Care within 14 Days of Discharge from Any Level of SUD Inpatient Care NYS OASAS P4P
8 Percentage of Members Enrolled in a Health Home NYS OMH P4R
9 Initiation of Medication-Assisted Treatment (MAT) for Alcohol Dependence NYS OASAS P4R
10Percentage of Members who Receive PROS or HCBS for At Least 3 Months in
Reporting YearNYS OMH P4R
11Percentage of Members who Maintained/Obtained Employment or
Maintained/Improved Higher Education StatusNYS OMH P4R
12 Percentage of Members with Maintenance of Stable or Improved Housing Status NYS OMH P4R
13 Percentage of Members with Reduced Criminal Justice Involvement NYS OMH P4R
HARP VBP Category 1 Required Measures: Behavioral Health
16 1616
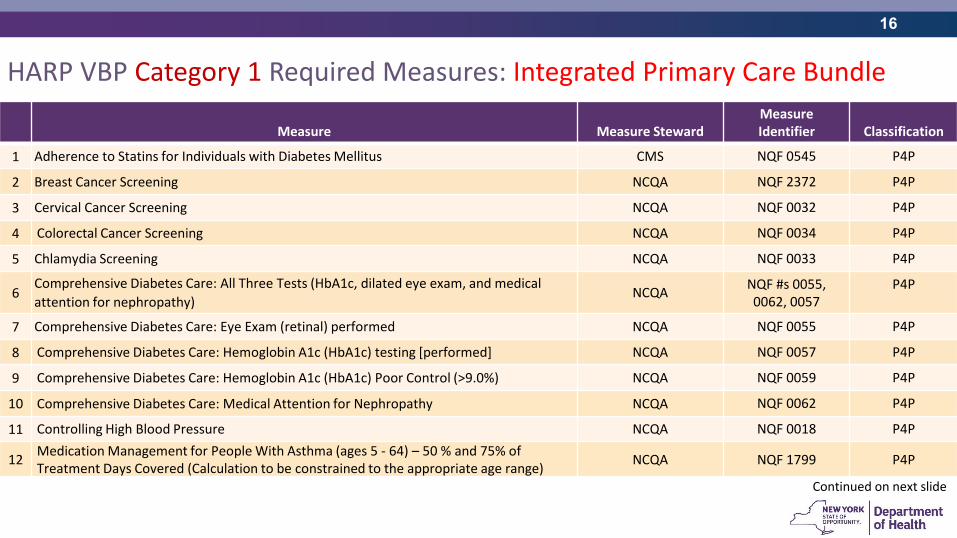
Measure Measure StewardMeasure Identifier Classification
1 Adherence to Statins for Individuals with Diabetes Mellitus CMS NQF 0545 P4P
2 Breast Cancer Screening NCQA NQF 2372 P4P
3 Cervical Cancer Screening NCQA NQF 0032 P4P
4 Colorectal Cancer Screening NCQA NQF 0034 P4P
5 Chlamydia Screening NCQA NQF 0033 P4P
6Comprehensive Diabetes Care: All Three Tests (HbA1c, dilated eye exam, and medical
attention for nephropathy)NCQA
NQF #s 0055, 0062, 0057
P4P
7 Comprehensive Diabetes Care: Eye Exam (retinal) performed NCQA NQF 0055 P4P
8 Comprehensive Diabetes Care: Hemoglobin A1c (HbA1c) testing [performed] NCQA NQF 0057 P4P
9 Comprehensive Diabetes Care: Hemoglobin A1c (HbA1c) Poor Control (>9.0%) NCQA NQF 0059 P4P
10 Comprehensive Diabetes Care: Medical Attention for Nephropathy NCQA NQF 0062 P4P
11 Controlling High Blood Pressure NCQA NQF 0018 P4P
12Medication Management for People With Asthma (ages 5 - 64) – 50 % and 75% of Treatment Days Covered (Calculation to be constrained to the appropriate age range)
NCQA NQF 1799 P4P
HARP VBP Category 1 Required Measures: Integrated Primary Care Bundle
Continued on next slide
17 1717
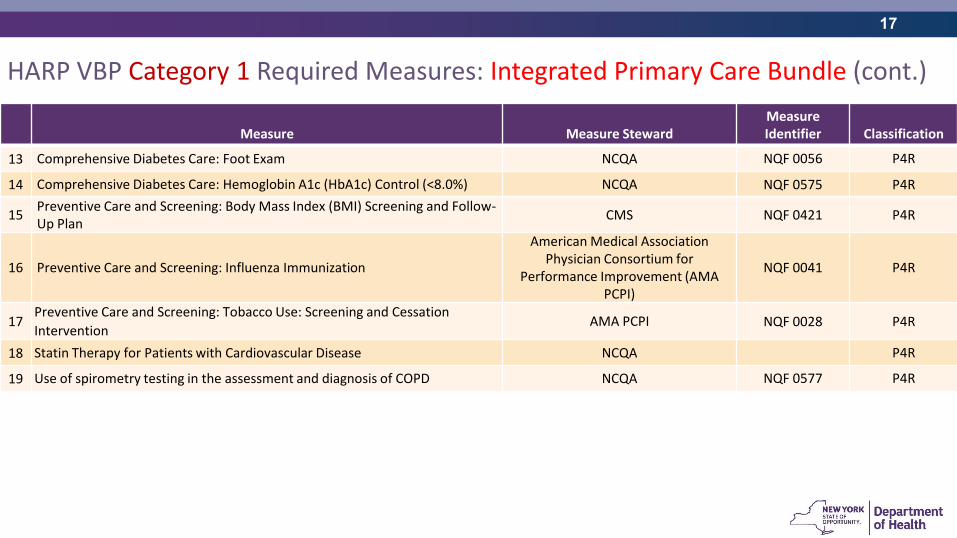
Measure Measure StewardMeasure Identifier Classification
13 Comprehensive Diabetes Care: Foot Exam NCQA NQF 0056 P4R
14 Comprehensive Diabetes Care: Hemoglobin A1c (HbA1c) Control (<8.0%) NCQA NQF 0575 P4R
15Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan
CMS NQF 0421 P4R
16 Preventive Care and Screening: Influenza Immunization
American Medical Association Physician Consortium for
Performance Improvement (AMA PCPI)
NQF 0041 P4R
17Preventive Care and Screening: Tobacco Use: Screening and Cessation
InterventionAMA PCPI NQF 0028 P4R
18 Statin Therapy for Patients with Cardiovascular Disease NCQA P4R
19 Use of spirometry testing in the assessment and diagnosis of COPD NCQA NQF 0577 P4R
HARP VBP Category 1 Required Measures: Integrated Primary Care Bundle (cont.)
1818
What do we measure?
1. System of Care priorities (understanding)
2. Payers’ priorities (accountability)
3. Provider priorities (quality improvement)
1919
NYS Mental Health Performance Measurement Priority Focus Areas
1. Shift the locus of care: Improve care transitions; offer prevention, early intervention, and crisis services; decrease inpatient admission and ED visit rates.
2. Promote Integrated Care: strategies to incentivize integrated (medical - behavioral health) care.
3. Improve functioning and recovery: Increase the numbers of individuals returning to work or school; decrease criminal justice contacts; promote individuals’ pathways to recovery.
2020
What should a community-based organization measure?
1. Shift the locus of care: Don’t need to measure readmission rates, but consider tracking adherence to your agencies relevant P&P, e.g.: – Check-ins with all clients within 7 days of discharge from hospital or emergency
department to check symptoms, reconcile medications, and review aftercare appointments;
– Accompany clients to aftercare appointments in first 30 days following discharge from hospital;
– Enrollment in a Health Home, and regular communications with HH Care Manager
2. Promote Integrated Care: What measurement strategies will best incentivize integrated (medical - behavioral health) care?
3. Improve functioning and recovery: How do we measure functional and recovery outcomes?
2121
What should a community-based organization measure?
1. Shift the locus of care
2. Promote Integrated Care: Don’t need to measure blood sugar and cholesterol, but consider tracking:1. Attendance at annual primary care appointments/wellness appointments
2. Monthly medication reconciliation for both psychotropic and general medical medications
3. Regular reviews (e.g., monthly or more when in crisis) of safety plans for individuals with depression or history of suicidal thinking/behavior
3. Improve functioning and recovery: How do we measure functional and recovery outcomes?
2222
What should a community-based organization measure?
1. Shift the locus of care
2. Promote Integrated Care
3. Improve functioning and recovery: How do we measure functional and recovery outcomes?

2323
Measuring functioning and recovery
2424
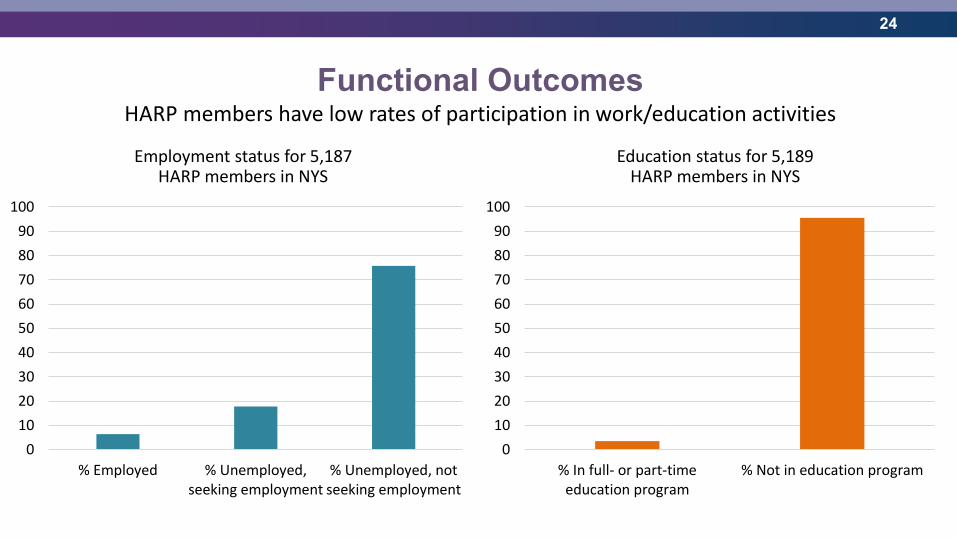
Functional OutcomesHARP members have low rates of participation in work/education activities
Education status for 5,189 HARP members in NYS
Employment status for 5,187 HARP members in NYS
0
10
20
30
40
50
60
70
80
90
100
% Employed % Unemployed,seeking employment
% Unemployed, notseeking employment
0
10
20
30
40
50
60
70
80
90
100
% In full- or part-timeeducation program
% Not in education program
2525
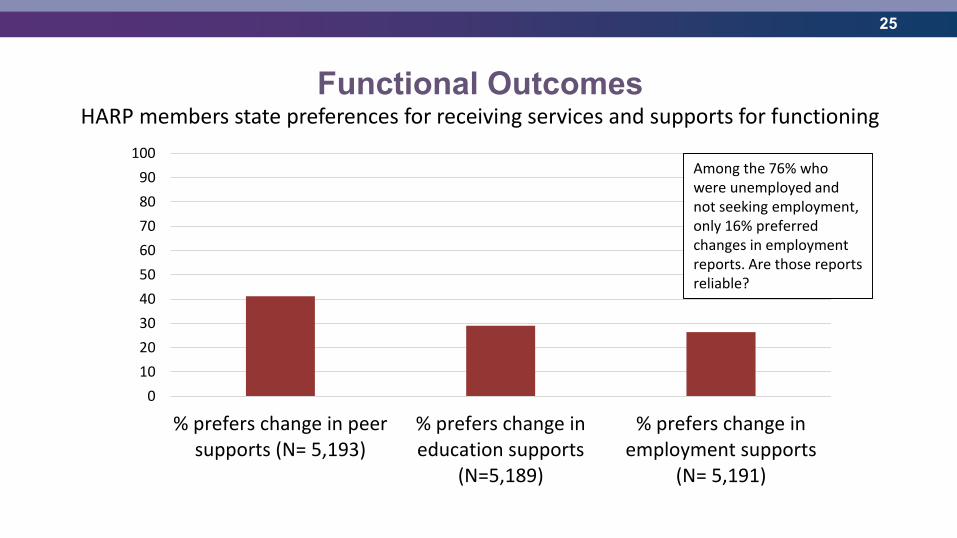
Functional OutcomesHARP members state preferences for receiving services and supports for functioning
0
10
20
30
40
50
60
70
80
90
100
% prefers change in peersupports (N= 5,193)
% prefers change ineducation supports
(N=5,189)
% prefers change inemployment supports
(N= 5,191)
Among the 76% who were unemployed and not seeking employment, only 16% preferred changes in employment reports. Are those reports reliable?
2626
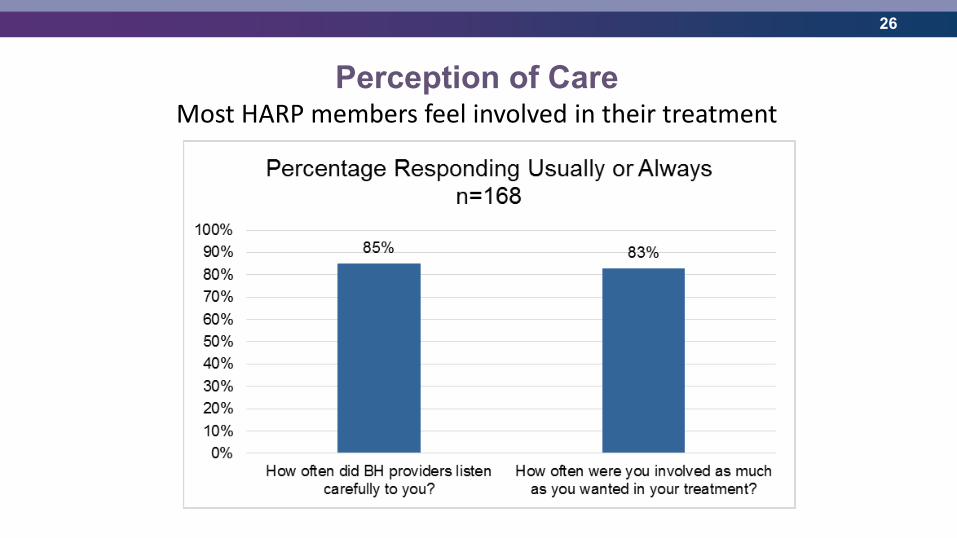
Perception of CareMost HARP members feel involved in their treatment
2727
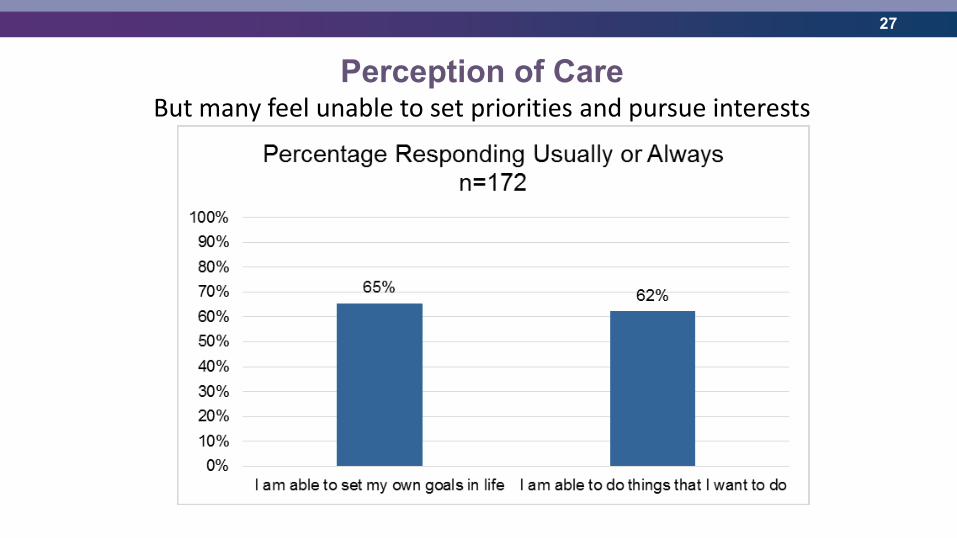
Perception of CareBut many feel unable to set priorities and pursue interests
28
Measuring Functioning and Recovery• Much work to do to outline domains for measurement and data collection
strategies
• NYS will use a participatory process to engage individuals and providers in planning efforts
• Providers can adopt the same strategy described previously to identify key elements of your vision and measure adherence to related P&P
• Examples include rates of clients with: – Complete, comprehensive Plans of Care;
– Personalized recovery goals;
– Housing stability;
– Involvement with justice system
– Etc.
29
ConclusionsEfforts to identify value and efficiency in health care are here to stay. What you can do:
• Understand where your agency fits in the larger system of care.
• Know the oversight and payment authorities’ priorities for the system of care.
• Align some (not all!) of your agency’s priorities and strengths with the system priorities
• Implement tracking and reporting of key agency practices that align with the system priorities.
• Have summary reports ready for external audiences—brag about what you do well.
• Retain your unique identity, and brag about that too!
3030
Thank you