Embed Size (px)
Citation preview
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 1/7
St. Paul University Dumaguete
College of Nursing
In Partial Fulfillment
Of the
Requirements in R.L.E.
VASCULAR LESIONS
Submitted to :
Mr. Persee James Baybay, RN
Submitted by:
Katherine D. Barote
BSN-III D
Date:
September , 2009
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 2/7
Skin Lesions
A skin lesion is a superficial growth or patch of the skin that does not resemble the
area surrounding it. They may take the form of bumps, blisters, or general sores. While many are benign (such as moles or freckles) some are the result of toxins (such as mosquito bites) or
diseases (such as chicken pox or psoriasis)
Vascular Lesions
Vascular birthmarks are commonly encountered in children and are classified aseither hemangiomas or vascular malformations1,2 (Table 1). Hemangiomas are benign neoplastic
proliferations of vascular endothelial cells characterized by spontaneous involution. In contrast,vascular malformations are not neoplasms but permanent morphogenic abnormalities of
capillaries, veins, arteries or lymphatic vessels. Flat lesions (vascular malformations) tend to persist, while raised lesions (hemangiomas) tend to regress.
Vascular Malformations
Although vascular malformations are by definition present at birth, they may become clinicallyapparent at different ages. Capillary and lymphatic malformations are generally noted at birth;
arterial and venous malformations become visible any time from birth to adulthood. Unlikehemangiomas, capillary and venous malformations are soft, flat, easily compressible and easily
emptied of blood by manual pressure.
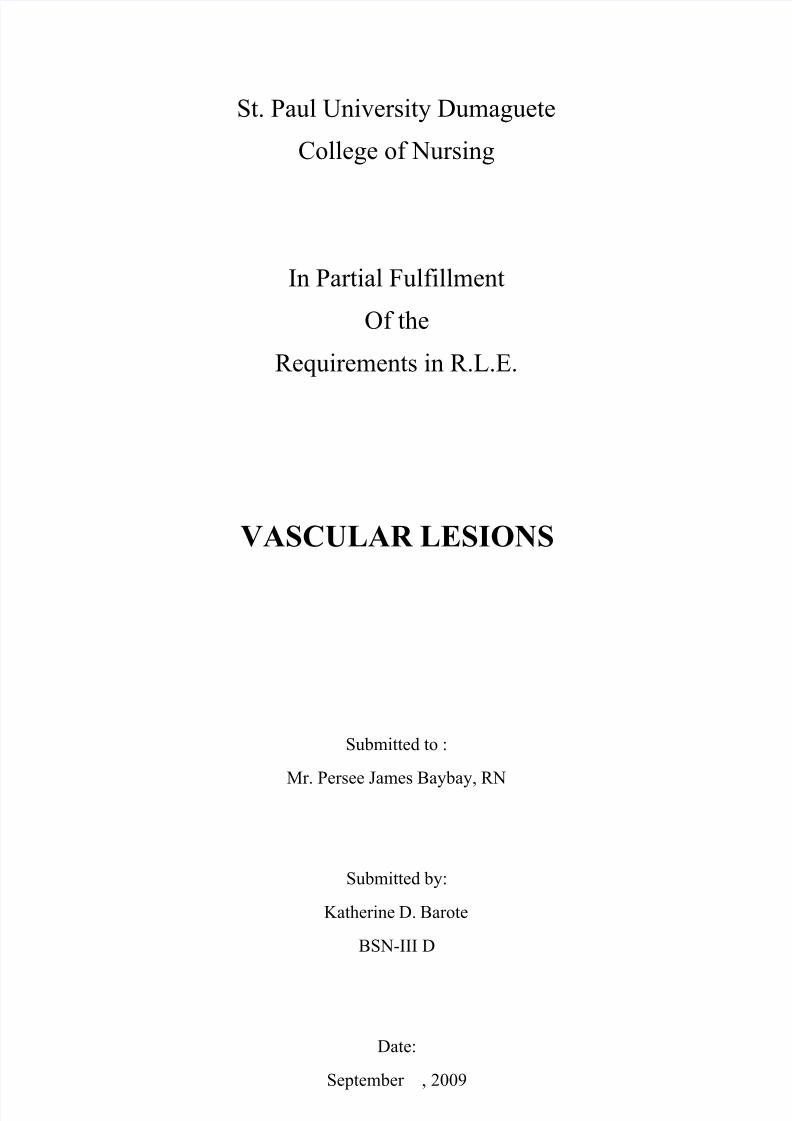
Salmon Patch (Nevus Simplex, Nevus Telangiectaticus) The salmon patch (often called a "stork bite"), composed of dilated dermal capillaries, is the
most common vascular malformation of infancy. It is present as a light-red to pink patch inapproximately 70 percent of white neonates and approximately 60 percent of black neonates.
Although most eyelid lesions fade by six to 12 months of age and glabellar lesions by five to six
years of age, 50 percent of nuchal-region salmon patches, also called Unna's nevus, persist intoadulthood
3
Salmon patch on the nape
of the neck in a child. Thislesion(termed"stork bite")
occurs in 40 percent of allnewborns. Fifty percent of
the lesions persist intoadulthood but are usually
covered by hair.
FIGURE 1B. Salmon patchon the nape of the neck inan adult.
TreatmentWatchful waiting is usually recommended. Parents must be informed that in fair-skinned
children, erythema may persist or reappear during episodes of crying, physical exertion or breath-holding. If therapy is desired, the flash-lamp pumped pulsed dye laser (FPDL) is the
treatment of choice for these superficial vascular lesions.
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 3/7
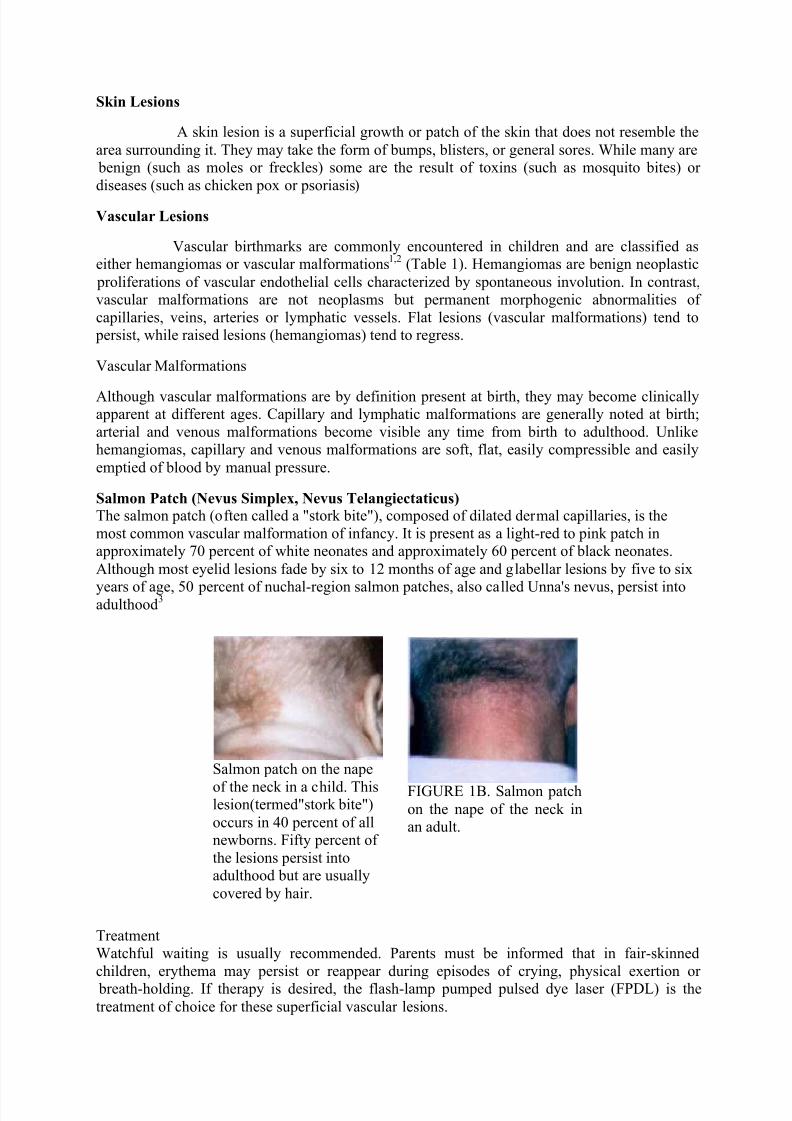
Port-Wine Stain (Nevus Flammeus) Occurring in 0.5 percent of newborns, port-wine stains are present
at birth, persist throughout life and appear as pale pink to red- purple, usually unilateral macules of the face or extremities (Figure
2). The capillary ectasias that make up port-wine stains involve not
only the superficial capillaries that are involved in the salmon patch, but also the deeper vessels of the dermis and subcutaneous tissue.Soft tissue or bony hypertrophy may occur either in an isolated port-
wine stain or in Sturge-Weber syndrome or Klippel-Trénaunay-Weber syndrome.
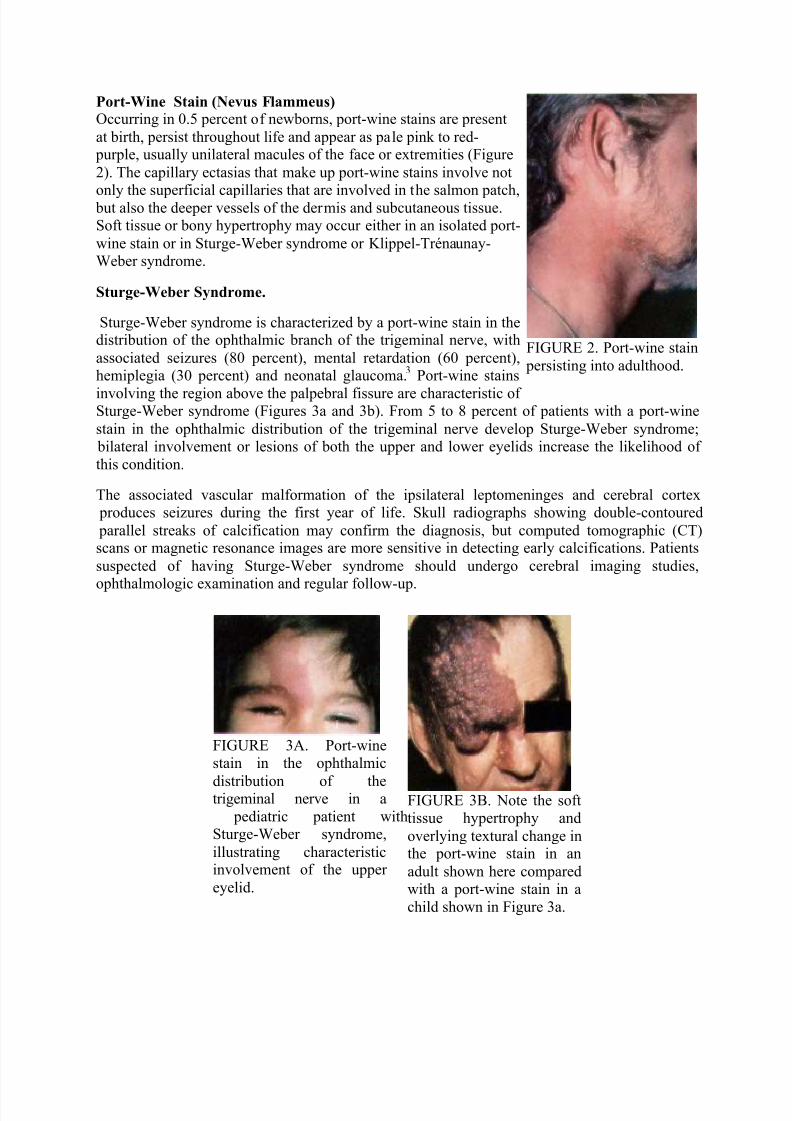
Sturge-Weber Syndrome.
Sturge-Weber syndrome is characterized by a port-wine stain in thedistribution of the ophthalmic branch of the trigeminal nerve, with
associated seizures (80 percent), mental retardation (60 percent),hemiplegia (30 percent) and neonatal glaucoma.
3Port-wine stains
involving the region above the palpebral fissure are characteristic of Sturge-Weber syndrome (Figures 3a and 3b). From 5 to 8 percent of patients with a port-wine
stain in the ophthalmic distribution of the trigeminal nerve develop Sturge-Weber syndrome; bilateral involvement or lesions of both the upper and lower eyelids increase the likelihood of
this condition.
The associated vascular malformation of the ipsilateral leptomeninges and cerebral cortex produces seizures during the first year of life. Skull radiographs showing double-contoured
parallel streaks of calcification may confirm the diagnosis, but computed tomographic (CT)scans or magnetic resonance images are more sensitive in detecting early calcifications. Patients
suspected of having Sturge-Weber syndrome should undergo cerebral imaging studies,
ophthalmologic examination and regular follow-up.
FIGURE 3A. Port-winestain in the ophthalmic
distribution of thetrigeminal nerve in a
pediatric patient withSturge-Weber syndrome,
illustrating characteristicinvolvement of the upper
eyelid.
FIGURE 3B. Note the softtissue hypertrophy and
overlying textural change inthe port-wine stain in an
adult shown here comparedwith a port-wine stain in a
child shown in Figure 3a.
FIGURE 2. Port-wine stain
persisting into adulthood.
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 4/7
K lippel-Trénaunay-Weber Syndrome.
Klippel-Trénaunay-Weber syndrome consists of a port-wine stain
over an extremity, with associated soft tissue and bonyhypertrophy that may result in hypertrophy of the extremity
(Figure 4). An arteriovenous fistula is present in 25 percent of these patients; the condition is then referred to as Parkes-Weber
syndrome. In cases of suspected Klippel-Trénaunay-Weber syndrome, the length and girth of the extremity should be
measured every three to six months and, if elongation of anextremity is noted, imaging studies to evaluate the patient for the
presence of an arteriovenous fistula or venous atresia should be performed. Surgical vascular intervention remains controversial.
4
Treatment
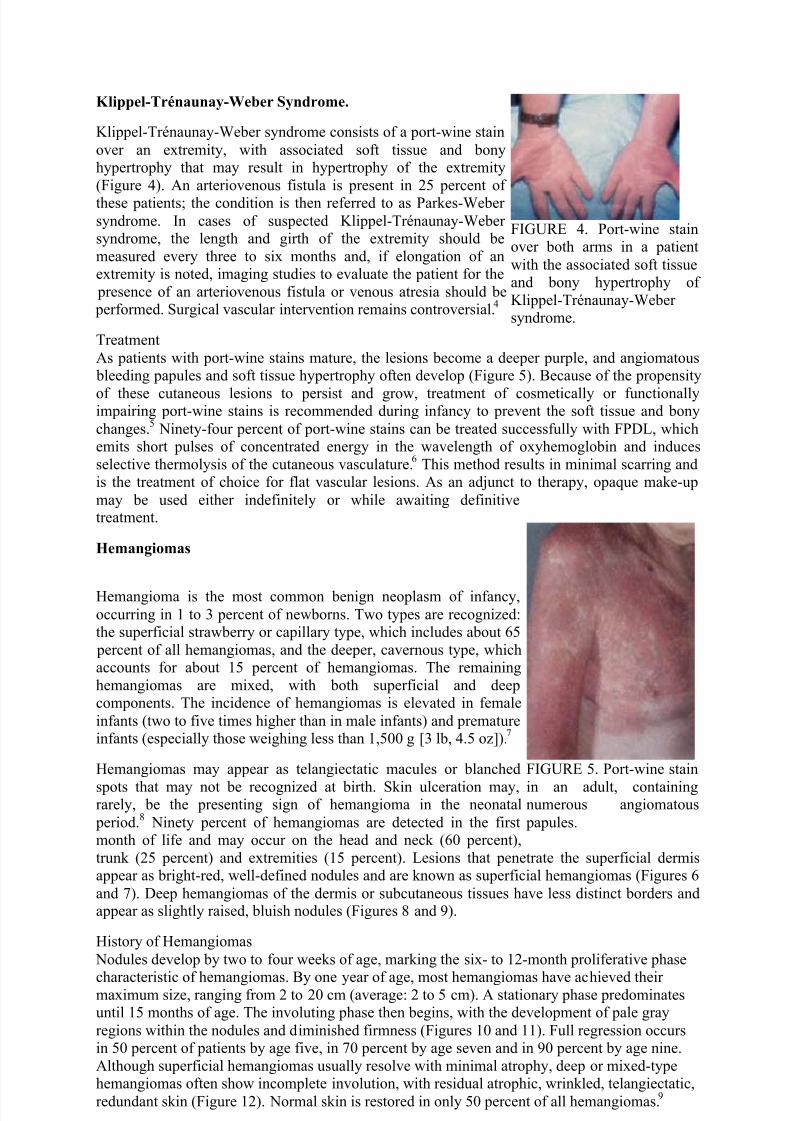
As patients with port-wine stains mature, the lesions become a deeper purple, and angiomatous bleeding papules and soft tissue hypertrophy often develop (Figure 5). Because of the propensity
of these cutaneous lesions to persist and grow, treatment of cosmetically or functionallyimpairing port-wine stains is recommended during infancy to prevent the soft tissue and bony
changes.5
Ninety-four percent of port-wine stains can be treated successfully with FPDL, whichemits short pulses of concentrated energy in the wavelength of oxyhemoglobin and induces
selective thermolysis of the cutaneous vasculature.6
This method results in minimal scarring andis the treatment of choice for flat vascular lesions. As an adjunct to therapy, opaque make-up
may be used either indefinitely or while awaiting definitivetreatment.
Hemangiomas
Hemangioma is the most common benign neoplasm of infancy,
occurring in 1 to 3 percent of newborns. Two types are recognized:the superficial strawberry or capillary type, which includes about 65
percent of all hemangiomas, and the deeper, cavernous type, whichaccounts for about 15 percent of hemangiomas. The remaining
hemangiomas are mixed, with both superficial and deepcomponents. The incidence of hemangiomas is elevated in female
infants (two to five times higher than in male infants) and prematureinfants (especially those weighing less than 1,500 g [3 lb, 4.5 oz]).
7
Hemangiomas may appear as telangiectatic macules or blanched
spots that may not be recognized at birth. Skin ulceration may,rarely, be the presenting sign of hemangioma in the neonatal
period.8
Ninety percent of hemangiomas are detected in the firstmonth of life and may occur on the head and neck (60 percent),
trunk (25 percent) and extremities (15 percent). Lesions that penetrate the superficial dermisappear as bright-red, well-defined nodules and are known as superficial hemangiomas (Figures 6
and 7). Deep hemangiomas of the dermis or subcutaneous tissues have less distinct borders andappear as slightly raised, bluish nodules (Figures 8 and 9).
History of Hemangiomas
Nodules develop by two to four weeks of age, marking the six- to 12-month proliferative phase
characteristic of hemangiomas. By one year of age, most hemangiomas have achieved their maximum size, ranging from 2 to 20 cm (average: 2 to 5 cm). A stationary phase predominatesuntil 15 months of age. The involuting phase then begins, with the development of pale gray
regions within the nodules and diminished firmness (Figures 10 and 11). Full regression occursin 50 percent of patients by age five, in 70 percent by age seven and in 90 percent by age nine.
Although superficial hemangiomas usually resolve with minimal atrophy, deep or mixed-typehemangiomas often show incomplete involution, with residual atrophic, wrinkled, telangiectatic,
redundant skin (Figure 12). Normal skin is restored in only 50 percent of all hemangiomas.9
FIGURE 4. Port-wine stainover both arms in a patient
with the associated soft tissueand bony hypertrophy of
Klippel-Trénaunay-Weber syndrome.
FIGURE 5. Port-wine stain
in an adult, containingnumerous angiomatous
papules.
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 5/7
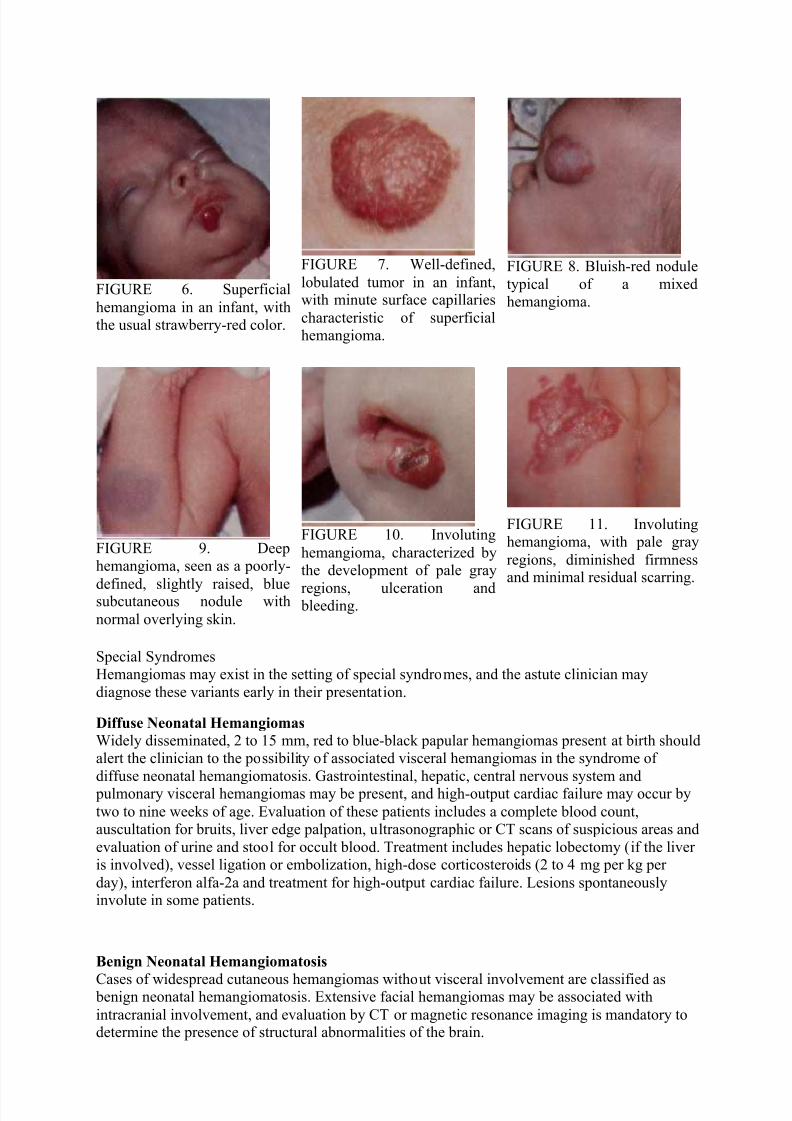
FIGURE 6. Superficial
hemangioma in an infant, withthe usual strawberry-red color.
FIGURE 7. Well-defined,
lobulated tumor in an infant,with minute surface capillaries
characteristic of superficialhemangioma.
FIGURE 8. Bluish-red nodule
typical of a mixedhemangioma.
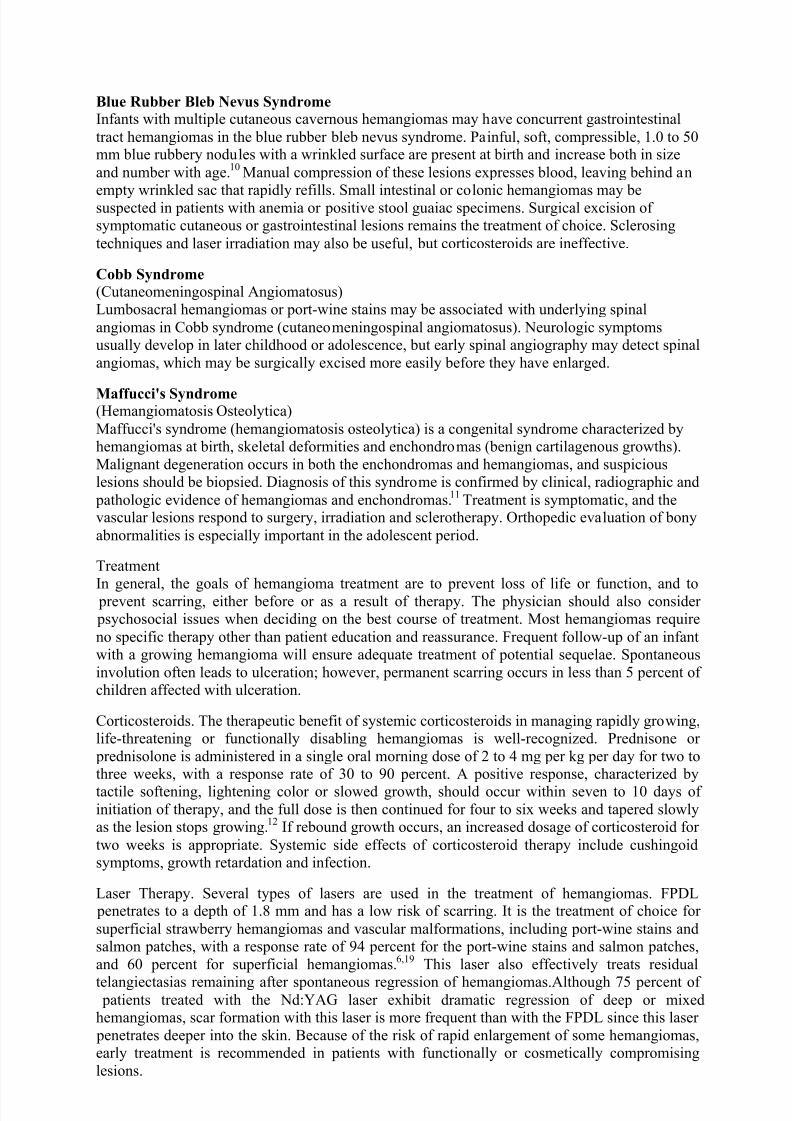
FIGURE 9. Deephemangioma, seen as a poorly-
defined, slightly raised, bluesubcutaneous nodule with
normal overlying skin.
FIGURE 10. Involuting
hemangioma, characterized bythe development of pale gray
regions, ulceration and bleeding.
FIGURE 11. Involutinghemangioma, with pale gray
regions, diminished firmnessand minimal residual scarring.
Special SyndromesHemangiomas may exist in the setting of special syndromes, and the astute clinician may
diagnose these variants early in their presentation.
Diffuse Neonatal Hemangiomas
Widely disseminated, 2 to 15 mm, red to blue-black papular hemangiomas present at birth shouldalert the clinician to the possibility of associated visceral hemangiomas in the syndrome of
diffuse neonatal hemangiomatosis. Gastrointestinal, hepatic, central nervous system and pulmonary visceral hemangiomas may be present, and high-output cardiac failure may occur by
two to nine weeks of age. Evaluation of these patients includes a complete blood count,auscultation for bruits, liver edge palpation, ultrasonographic or CT scans of suspicious areas and
evaluation of urine and stool for occult blood. Treatment includes hepatic lobectomy (if the liver is involved), vessel ligation or embolization, high-dose corticosteroids (2 to 4 mg per kg per
day), interferon alfa-2a and treatment for high-output cardiac failure. Lesions spontaneouslyinvolute in some patients.
Benign Neonatal Hemangiomatosis
Cases of widespread cutaneous hemangiomas without visceral involvement are classified as benign neonatal hemangiomatosis. Extensive facial hemangiomas may be associated with
intracranial involvement, and evaluation by CT or magnetic resonance imaging is mandatory todetermine the presence of structural abnormalities of the brain.
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 6/7
Blue Rubber Bleb Nevus Syndrome Infants with multiple cutaneous cavernous hemangiomas may have concurrent gastrointestinal
tract hemangiomas in the blue rubber bleb nevus syndrome. Painful, soft, compressible, 1.0 to 50mm blue rubbery nodules with a wrinkled surface are present at birth and increase both in size
and number with age.10
Manual compression of these lesions expresses blood, leaving behind an
empty wrinkled sac that rapidly refills. Small intestinal or colonic hemangiomas may besuspected in patients with anemia or positive stool guaiac specimens. Surgical excision of symptomatic cutaneous or gastrointestinal lesions remains the treatment of choice. Sclerosing
techniques and laser irradiation may also be useful, but corticosteroids are ineffective.
Cobb Syndrome
(Cutaneomeningospinal Angiomatosus)Lumbosacral hemangiomas or port-wine stains may be associated with underlying spinal
angiomas in Cobb syndrome (cutaneomeningospinal angiomatosus). Neurologic symptomsusually develop in later childhood or adolescence, but early spinal angiography may detect spinal
angiomas, which may be surgically excised more easily before they have enlarged.
Maffucci's Syndrome (Hemangiomatosis Osteolytica)
Maffucci's syndrome (hemangiomatosis osteolytica) is a congenital syndrome characterized byhemangiomas at birth, skeletal deformities and enchondromas (benign cartilagenous growths).
Malignant degeneration occurs in both the enchondromas and hemangiomas, and suspiciouslesions should be biopsied. Diagnosis of this syndrome is confirmed by clinical, radiographic and
pathologic evidence of hemangiomas and enchondromas.11
Treatment is symptomatic, and thevascular lesions respond to surgery, irradiation and sclerotherapy. Orthopedic evaluation of bony
abnormalities is especially important in the adolescent period.
Treatment
In general, the goals of hemangioma treatment are to prevent loss of life or function, and to prevent scarring, either before or as a result of therapy. The physician should also consider psychosocial issues when deciding on the best course of treatment. Most hemangiomas require
no specific therapy other than patient education and reassurance. Frequent follow-up of an infantwith a growing hemangioma will ensure adequate treatment of potential sequelae. Spontaneous
involution often leads to ulceration; however, permanent scarring occurs in less than 5 percent of children affected with ulceration.
Corticosteroids. The therapeutic benefit of systemic corticosteroids in managing rapidly growing,life-threatening or functionally disabling hemangiomas is well-recognized. Prednisone or
prednisolone is administered in a single oral morning dose of 2 to 4 mg per kg per day for two tothree weeks, with a response rate of 30 to 90 percent. A positive response, characterized by
tactile softening, lightening color or slowed growth, should occur within seven to 10 days of initiation of therapy, and the full dose is then continued for four to six weeks and tapered slowlyas the lesion stops growing.
12If rebound growth occurs, an increased dosage of corticosteroid for
two weeks is appropriate. Systemic side effects of corticosteroid therapy include cushingoidsymptoms, growth retardation and infection.
Laser Therapy. Several types of lasers are used in the treatment of hemangiomas. FPDL penetrates to a depth of 1.8 mm and has a low risk of scarring. It is the treatment of choice for
superficial strawberry hemangiomas and vascular malformations, including port-wine stains andsalmon patches, with a response rate of 94 percent for the port-wine stains and salmon patches,
and 60 percent for superficial hemangiomas.6,19 This laser also effectively treats residual
telangiectasias remaining after spontaneous regression of hemangiomas.Although 75 percent of patients treated with the Nd:YAG laser exhibit dramatic regression of deep or mixedhemangiomas, scar formation with this laser is more frequent than with the FPDL since this laser
penetrates deeper into the skin. Because of the risk of rapid enlargement of some hemangiomas,early treatment is recommended in patients with functionally or cosmetically compromising
lesions.
8/8/2019 Out Patient Dept.
http://slidepdf.com/reader/full/out-patient-dept 7/7
The carbon dioxide laser is effective in treating subglottic hemangiomas unresponsive tocorticosteroids and may prevent the need for tracheostomy in patients with airway obstruction.
Because of the increased risk for scarring with both carbon dioxide and argon lasers, these lasersare not recommended in the initial treatment of cutaneous hemangiomas. Surgery. Surgical
excision is occasionally advocated as primary treatment of hemangiomas. Surgical excision is
clearly indicated in the management of visceral or ocular lesions unresponsive to corticosteroids,and in the cosmetic revision of redundant skin remaining after spontaneous involution of deeper hemangiomas.
12,20Embolization is a primary treatment for inoperable lesions, and it may be used
preoperatively to minimize intraoperative blood loss. Potential side effects includecerebrovascular accident from the backflow of particles into the internal carotid artery.
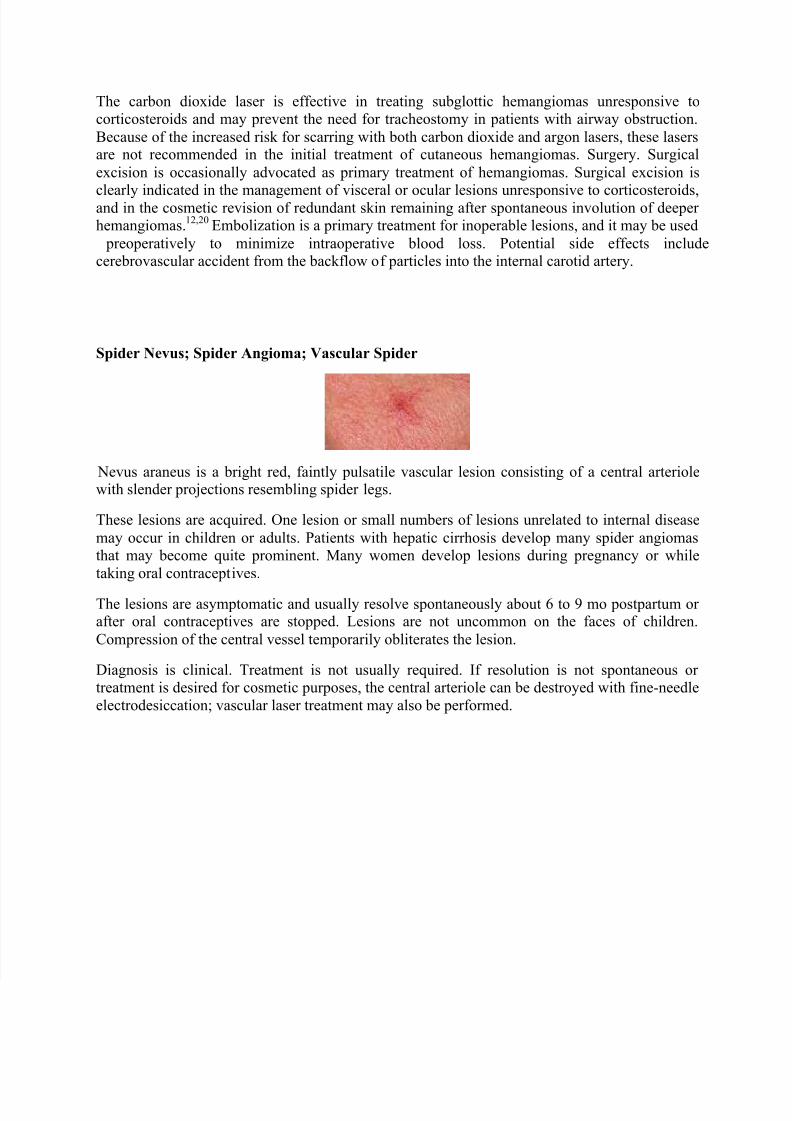
Spider Nevus; Spider Angioma; Vascular Spider
Nevus araneus is a bright red, faintly pulsatile vascular lesion consisting of a central arteriolewith slender projections resembling spider legs.
These lesions are acquired. One lesion or small numbers of lesions unrelated to internal disease
may occur in children or adults. Patients with hepatic cirrhosis develop many spider angiomasthat may become quite prominent. Many women develop lesions during pregnancy or while
taking oral contraceptives.
The lesions are asymptomatic and usually resolve spontaneously about 6 to 9 mo postpartum or after oral contraceptives are stopped. Lesions are not uncommon on the faces of children.
Compression of the central vessel temporarily obliterates the lesion.
Diagnosis is clinical. Treatment is not usually required. If resolution is not spontaneous or treatment is desired for cosmetic purposes, the central arteriole can be destroyed with fine-needle
electrodesiccation; vascular laser treatment may also be performed.





























