Embed Size (px)
Citation preview

d
OTITIS EXTERNA
© Bruce Black MD

OTITIS EXTERNA Classification
Infection Bacterial Otomycoses Chronic myringitis Viral
Seborrhoeic Allergic Neurodermatitis EAC Osteitis
© Bruce Black MD

Bacterial Otitis Externa Clinical Features
Ache, pruritis, pain Semisolid debris in EAC Blockage, deafness due to debris Gurgling in ear
© Bruce Black MD
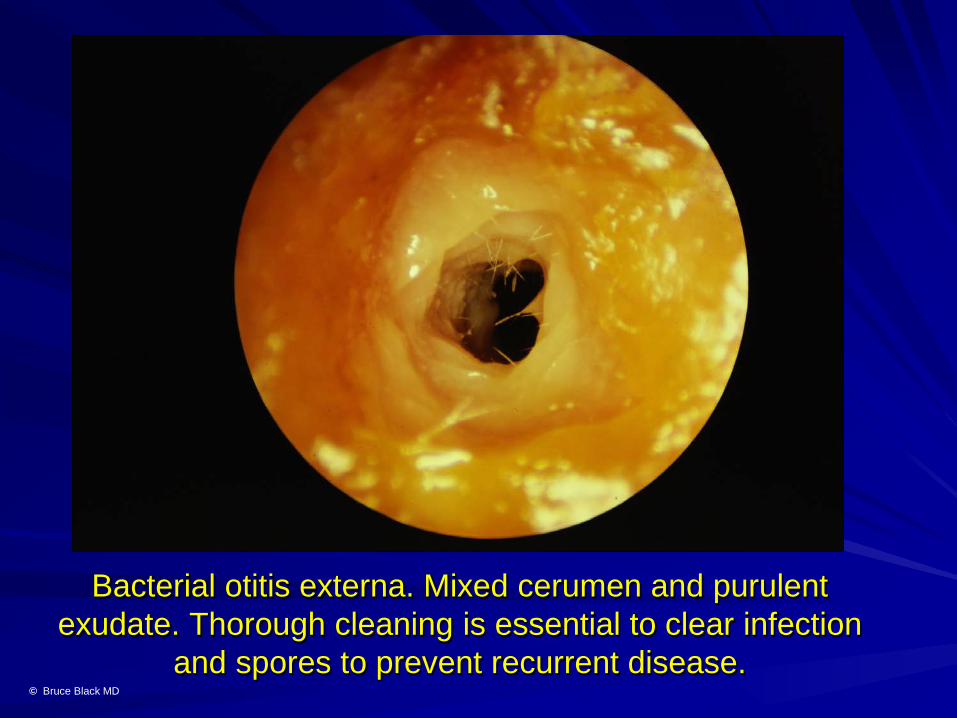
Bacterial otitis externa. Mixed cerumen and purulent exudate. Thorough cleaning is essential to clear infection
and spores to prevent recurrent disease. © Bruce Black MD

Bacterial O. Ext.
Treatment
Clean by suction or wool carrier Wet mopping, re-clean Antibiotic ointment (neomycin, gentamicin, ciprofloxacin) Antibiotic drops (only after cleaning; ineffective without)
© Bruce Black MD

Pseudomonal otitis externa with the green debris characteristic of this infection. Clean, then use gentamicin
or ciprofloxacin topically for optimal effect. © Bruce Black MD

Severe aural furunculosis. Scattered pustules and severe oedema. Micro-suction essential. Follow with a
betamethasone and ciprofloxacin wick, together with anti-staphylococcal antibiotics © Bruce Black MD

Aural Furunculosis Clinical Features
Severe pain, distressing Scanty purulent debris Deaf; severe canal oedema Gurgling noise Pain may be disorientating
© Bruce Black MD

Erythema and oedema secondary to furunculosis. Resembles mastoiditis, but is behind and below the ear rather than the
postero-superior location of a mastoid abscess. © Bruce Black MD

Furunculosis Treatment
Immediate strong pain relief Micro-suction (EAC oedema) Ciprofloxacin-betamethasone wick,
then ciprofloxacin drops Dicloxacillin Review and re-clean EAC
© Bruce Black MD

Aspergillus nigra otomycosis. The black spores are typical. Requires meticulous toilet then prolonged topical
clotrimazole for best outcomes. © Bruce Black MD

Otomycoses Fungal Otitis Externa
Pruritic, pain if drum perforated Semisolid dirty discoloured debris Blocked and deaf Gurgling, possible ringing Resistant to treatment, micro-suction
optimal © Bruce Black MD

Aspergillus flavum mycelium and typical yellow spores. Treat as for A. nigra and follow-up to check for recurrence.
© Bruce Black MD

Candida albicans, causing intense itch and blockage. Treat as for other otomycoses with serial suction toilet and wet
mopping to eliminate infected debris. © Bruce Black MD

Otomycoses Treatment
Thorough micro-suction and wet mopping
Clotrimazole and antibiotic wick Clotrimazole drops (if no drum
perforation) 2/52 Review 2/52, re-clean
© Bruce Black MD
Chronic Myringitis Chronic Drum / EAC Ulceration
Minor ache, itch Minor accumulated debris Intermittent blockage Little tinnitus or unsteadiness Reddened, granular or fibrosing
ulceration © Bruce Black MD
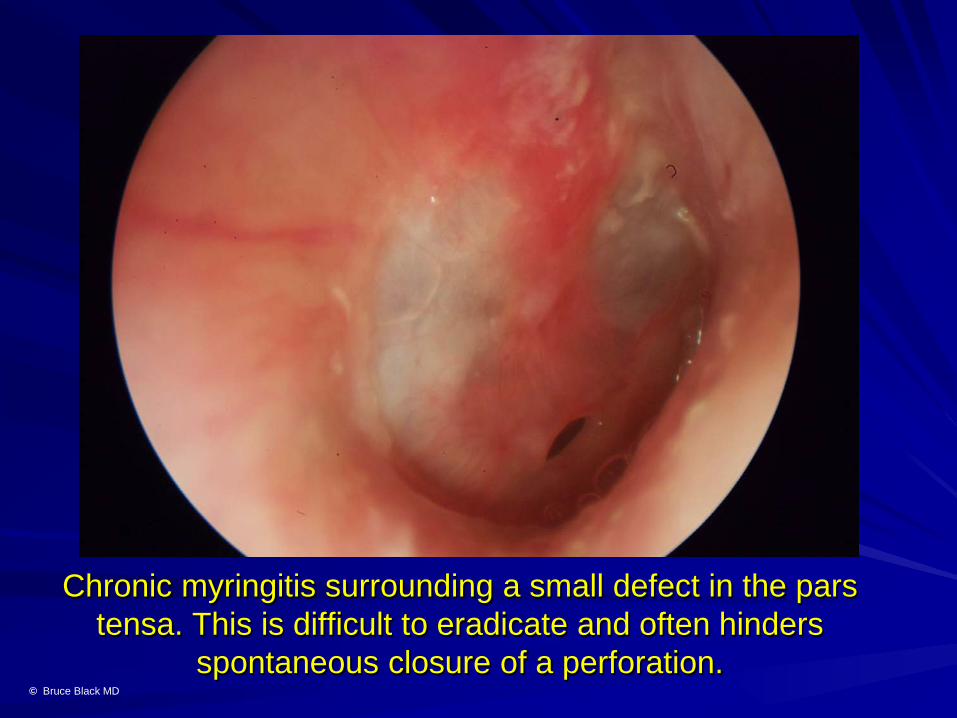
Chronic myringitis surrounding a small defect in the pars tensa. This is difficult to eradicate and often hinders
spontaneous closure of a perforation. © Bruce Black MD

Diffuse thicker myringitis coating the entire pars tensa. Removal off the collagenous drum layer by fine dissection, then using an onlay graft will usually eliminate this problem. © Bruce Black MD

Granular myringitis. Cautery with AgNO3 will shrink the granulations and antibiotic/antiseptic treatment may reduce them further, but surgery may be necessary, particularly in
the anterior angle. © Bruce Black MD
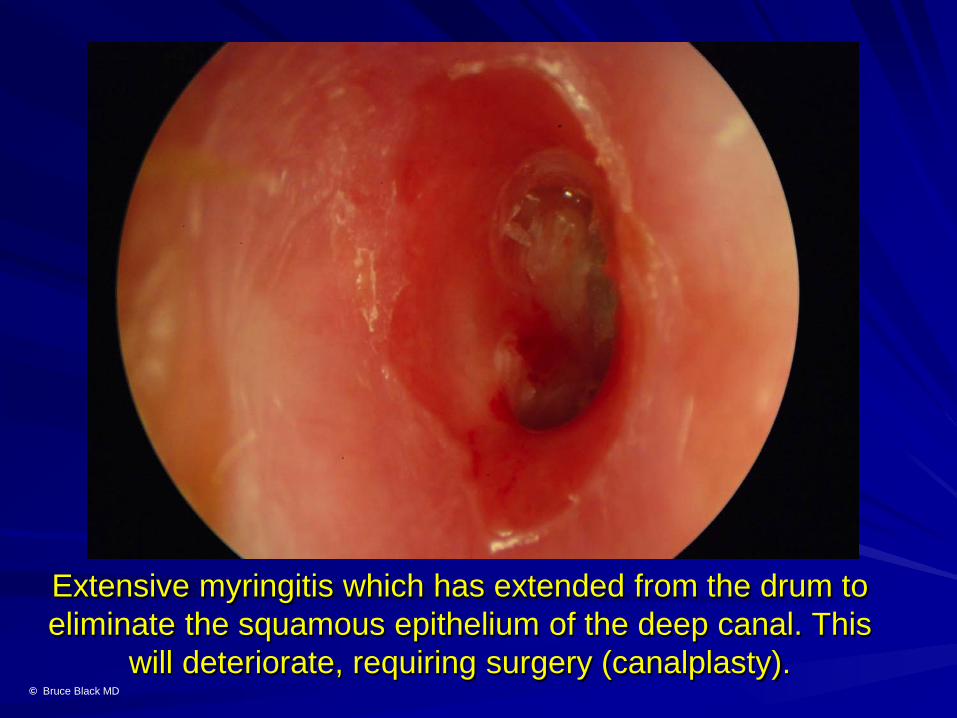
Extensive myringitis which has extended from the drum to eliminate the squamous epithelium of the deep canal. This
will deteriorate, requiring surgery (canalplasty). © Bruce Black MD

Cicatrising fibrosis, the end phase of chronic myringitis. Correctable only by EAC clearance and total split skin
grafting. © Bruce Black MD
Chronic Myringitis Management
Suction toilet Cauterise granulations Ciprofloxacin drops Excise and graft resistant cases
© Bruce Black MD
Note: Chronic myringitis is notoriously difficult to eradicate. Surgery is frequently the only effective option

Viral External Otitis Viral / Bullous myringitis
Pain and blockage Glairish / haemorrhagic blebs on drum May be confused with advanced AOM
Herpes zoster oticus (Ramsey Hunt Synd.) Lancing pain Vesicles in EAC, pinna Associated facial palsy, vertigo, SND
© Bruce Black MD

Bullous/viral myringitis, exhibiting haemorrhagic blebs totally obscuring the pars tensa.
© Bruce Black MD

Viral myringitis showing the glairish fluid-filled blistering of the drum. Can be confused with the blebs that develop as a
result of AOM. © Bruce Black MD

Herpes zoster oticus. Scattered small crusts cover the sites of recent vesicular formations on the conchal bowl. Facial palsy and severe cochleo-vestibular symptoms may be
present. © Bruce Black MD

Seborrhoeic Otitis Externa
Greasy scaling skin, also face, neck Erythema, exfoliation, inflammation,
oedema Dandruff, oily hair Cause uncertain, possibly Malassezi
furfur (yeast)
© Bruce Black MD

Seborrhoeic dermatitis showing the typical greasy scalp and dandruff.
© Bruce Black MD

Diffuse peri-otic skin with erythema, oedema and dandruff due to seborrhoea.
© Bruce Black MD

Allergic Otitis Externa
Intense pruritis Serous exudate, often profuse Periotic Inflammation, oedema History of recent topical medication
© Bruce Black MD

Erythema of the lower face and neck secondary to ciprofloxacin drops used for otitis externa.
© Bruce Black MD

Conchal bowl erythema and swelling, plus serous exudate, secondary to neomycin drop usage.
© Bruce Black MD

Gross oedema, inflammation and exudate after iodoform paste used on a mastoidectomy cavity.
© Bruce Black MD

Marked exfoliation, oedema and inflammation. Neomycin ear drops
© Bruce Black MD
ALLERGIC OTITIS EXTERNA Management
Clean thoroughly Liberal steroid ointment Avoid further causative agent
exposure
© Bruce Black MD

Neurodermatitis Lichen Simplex Chronicus,
Eczema Pruritis, discomfort Watery otorrhoea, intermittent Blockage: semiliquid powdery otorrhoea Conchal bowl erythema, oedema,
exfoliation Habitual rubbing, scratching Commonly smokers
© Bruce Black MD

Erythema and marked exfoliation of the conchal bowl and tragus. Neurodermatitis in a heavy smoker. The tobacco
tars are irritative, causing chronic pruritis. © Bruce Black MD

Advanced neurodermatitis. Chronic habitual rubbing and scratching. Cleaning and steroid ointment produced rapid
remission. © Bruce Black MD

NEURODERMATITIS Management
Clean debris Moisten well, peel away keratin Steroid and antibiotic ointment Avoid further self-trauma Wash hands after tobacco
© Bruce Black MD

OTHER EAC INFECTIONS
© Bruce Black MD

Infected sebaceous cyst. These classically occur in the floor of the entrance to the EAC. If recurrent, marsupialise.
© Bruce Black MD

Chronic debris accumulation and infection, secondary to a keratosis obturans. This will cause progressive erosion or
even extensive osteitis if not cleaned regularly. © Bruce Black MD

Osteitis in the floor of the EAC, complicating a keratosis obturans. Clean regularly, removing infected bony spicules. Advanced cases may require surgical excision and grafting. © Bruce Black MD

OTITIS EXTERNA Summary
Assess aetiology Clean thoroughly Appropriate management Persistent? Suspect fungal origin
© Bruce Black MD