Embed Size (px)
Citation preview

1
© The CORE Institute. All rights reserved.
OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION
Debra L. Sietsema, PhD, RN Director, Bone Health Clinical Operations
October 5, 2016 OTA NP/PA Course

2
© The CORE Institute. All rights reserved.
Osteoporosis Definition
A skeletal disorder characterized by compromised bone strength predisposing a person to an
increased risk of fracture
Normal Bone Osteoporotic Bone
NIH Consensus Development Panel on Osteoporosis. JAMA. 2001;285:785-795

3
© The CORE Institute. All rights reserved.
WHO Classification

4
© The CORE Institute. All rights reserved.
Fragility Fracture
Resulting from a: Fall from a standing height Spontaneous fracture
Establishes osteoporosis diagnosis regardless of DXA results Siris, et al. The clinical diagnosis of osteoporosis. Ost Int. 2014; 25:1439-1443.

5
© The CORE Institute. All rights reserved.
Shifting the Osteoporosis Paradigm: Bone Strength
Bone Density
Bone Quality
Bone Strength
•Mineralization •Bone remodeling •Damage accumulation •Trabecular connectivity •Architecture
aBMD = g/cm2
vBMD = g/cm3
NIH Consensus Development Panel on Osteoporosis. JAMA. 2001;285:785-795.

6
© The CORE Institute. All rights reserved.
What’s the problem?

7
© The CORE Institute. All rights reserved.

8
© The CORE Institute. All rights reserved.
Prevalence of Osteoporosis and Low Bone Mass
Americans Age 50 and Above Affected by Osteoporosis/Low Bone Mass, 2010 to 2030 (projected)
0
10
20
30
40
50
60
70
80
2010 2030
Low Bone MassOsteoporosis
Mill
ions
54 million of 99 million Americans age 50+ (2010)
+27% change from 2010 to 2030
17% of the ENTIRE U.S. POPULATION (2010)
Osteoporosis Prevalence of Osteoporosis and Low Bone Mass
• Wright NC, et al. JBMR doi:10.1002/jbmr2269

9
© The CORE Institute. All rights reserved.
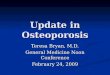
Figure 1. Percent of hospitalizations* for osteoporotic fractures and other serious diseases combined, 2000–2011
*Principal diagnosis codes were used to define the outcomes.
Hospitalization Burden for Osteoporotic Fractures and Other Serious Diseases in Older US Women
Singer AJ, et al. Osteoporosis International. 25(4) suppl:503-522;2014. Singer AJ, et al. Mayo Clinic Proceedings 2015 90, 53-62

10
© The CORE Institute. All rights reserved. Wasnich RD. In: Favus MJ, ed. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. 4th ed. Philadelphia, PA: Lippincott; 1999:257-259.
50 60 70 80
Vertebral
Hip
Wrist
Age (Years)
Annu
al In
cide
nce
per
100
0 W
omen
40
30
20
10
Incidence Rates for Vertebral, Wrist, and Hip Fractures in Women After Age 50
0

11
© The CORE Institute. All rights reserved. Wasnich RD. In: Favus MJ, ed. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. 4th ed. Philadelphia, PA: Lippincott; 1999:257-259.
50 60 70 80
Vertebral
Hip
Wrist
Age (Years)
Annu
al In
cide
nce
per
100
0 W
omen
40
30
20
10
Incidence Rates for Vertebral, Wrist, and Hip Fractures in Women After Age 50
0 Old
est B
aby
Boom
ers
Larg
est B
aby
Boom
er G
roup
Youn
gest
Bab
y Bo
omer
s
2015

12
© The CORE Institute. All rights reserved.
Wasnich RD. In: Favus MJ, ed. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. 4th ed. Philadelphia, PA: Lippincott; 1999:257-259.
50 60 70 80
Vertebral
Hip
Wrist
Age (Years)
Annu
al In
cide
nce
per
100
0 W
omen
40
30
20
10
Incidence Rates for Vertebral, Wrist, and Hip Fractures in Women After Age 50
Old
est B
aby
Boom
ers
Larg
est B
aby
Boom
er G
roup
Youn
gest
Bab
y Bo
omer
s
2030

13
© The CORE Institute. All rights reserved.
Distal Radial Fractures
The lifetime risk of sustaining a distal radial fracture is about 16% for white women. By age 70, about 20% of women have had at least one distal radial fracture.

14
© The CORE Institute. All rights reserved.
Vertebral fractures
35 to 50% of all women over fifty have at least one vertebral fracture. Between 30-65% are undiagnosed 1 3X risk 3 9X risk
Siris, et al. Enhanced prediction of fracture risk combining vertebral fracture status and BMD. Ost Int. 2007;18:761-770.

15
© The CORE Institute. All rights reserved.
Proximal Femoral Fractures
A 50-year-old white woman is estimated to have a 17.5% lifetime risk of fracture of the proximal femur.

16
© The CORE Institute. All rights reserved.
Proximal Femoral Fractures
Incidence increases each decade for all populations. Highest incidence is found among men and women ages 80 or older.

17
© The CORE Institute. All rights reserved.
1 out of 2 Women will have an osteoporotic fracture

18
© The CORE Institute. All rights reserved.
1 in 4 Men will have an osteoporotic fx
• More likely to have an osteoporotic fracture than to get prostate cancer
• 80,000 men have a hip fracture annually • Men are more likely to die within a year after hip fracture

19
© The CORE Institute. All rights reserved.
Importance to Orthopedics
Unique opportunity – sentinel event Reduce subsequent fractures Enhance fracture healing Comprehensive, excellent care

20
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

21
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

22
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

23
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

24
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

25
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

26
© The CORE Institute. All rights reserved.
Osteoporotic Disasters

27
© The CORE Institute. All rights reserved.
Advances to Treat these Fractures
Locking technology Cephalomedullary nails Ceramics Osteobiologics

28
© The CORE Institute. All rights reserved.
HEDIS Measure % Compliance Beta-blocker after a heart attack 91.4% Breast cancer screening 82.7% Colorectal cancer screening 73.8% Osteoporosis management after a fracture 20.7% NCQA Medical Evaluation 2013- HMO Statistics
Identified Treatment Gap - NCQA

29
© The CORE Institute. All rights reserved.
Optimal Management of Care
Diagnosis of “fragility” fracture General fracture management Rehabilitation Secondary prevention: Prevent subsequent fx
Identify, assess, treat, & evaluate underlying disease Teach & counsel re: condition & lifestyle behaviors Coordinated, comprehensive manner
Ganda. Models of care. Ost Int. 2012

30
© The CORE Institute. All rights reserved.
Fragility Fracture?
Injury Pattern
• Mechanism of injury • Low trauma • Fall from a standing ht
or less • Fx that occurred during
activity • Did others involved fx?
Risk Assessment
• Risk factors for: • 1° & 2° osteoporosis • Fracture • Fall
No symptoms of low bone mass until fracture. May be 1st indication of osteoporosis!

31
© The CORE Institute. All rights reserved.
Physical Findings Clinical Presentation indicating increased fracture risk
Impaired ambulation Muscle weakness Impaired balance Reduced vision
Macular Degeneration Glaucoma Bifocals
Orthostatic hypotension
Clinical presentation indicating signs of prior fractures
• Loss of height • Kyphosis • Chest deformity • Protuberant abdomen • Rib-pelvis overlap

32
© The CORE Institute. All rights reserved.
Key Risk Factors for Fractures (RR ≥ 2)
Age BMD Prior fragility fx Family hx of fragility fx
Kanis. Ost Int. 2005; 16

33
© The CORE Institute. All rights reserved.
Causes of Secondary Osteoporosis
Endocrine Disorders affecting bone metabolism
Menopause < age 45 Hypercalcuria with or without renal stones Hypogonadism Hyperparathyroidism Hyperthyroidism
Cushing’s syndrome Diabetes (types 1 and 2) Acromegaly Osteogenesis Imperfecta

34
© The CORE Institute. All rights reserved.
Causes of Secondary Osteoporosis
Drugs affecting bone quality Excess/length of time on glucocorticoids Excess thyroid hormones Anticoagulants (heparin) GnRH agonists Anticonvulsants Aromatase inhibitors Thiazolidinediones Opiates
Cyclosporine Chemotherapy Alcohol Loop diuretics PPI long term use

35
© The CORE Institute. All rights reserved.
Secondary Causes of Osteoporosis
GI Tract Disorders Malabsorption Gastrectomy Inflammatory bowel disease Celiac disease Intestinal bypass surgery Primary biliary cirrhosis Pancreatic insufficiency Hepatitis B, C
Bone Marrow Based Disorders Multiple myeloma Hemolytic anemia, hemoglobinopathies Myelo-and lymphoproliferative disorders Skeletal metastases (diffuse or localized) Gaucher’s disease Mastocytosis

36
© The CORE Institute. All rights reserved.
Secondary Causes of Osteoporosis
Inflammatory Disorders RA SLE Ankylosing spondylitis Polymalgia rheumatica Vasculitis
Other Propensity to fall Immobilization COPD Chronic renal failure AIDS/HIV Organ transplantation Anorexia / Bulemia Malignancy

37
© The CORE Institute. All rights reserved.
Other Significant Risk Factors
Vitamin D insufficiency History of missed menses/estrogen deficiency Smoking Excessive alcohol intake Sedentary lifestyle Environmental risks for fall Collagen deficiency
Hypermobility / flexibility

38
© The CORE Institute. All rights reserved.
Clinical Approach to Managing Osteoporosis
Assessment Detailed osteoporosis risk factor hx r/t fx & falls Physical exam Diagnostic studies 10-year probability of fx
(FRAX) Ultimate Goal
Prevent fractures Plan
Mutual plan

39
© The CORE Institute. All rights reserved.
Clinical Approach to Managing Osteoporosis
Implement Nonmedical interventions
Modify risk factors PT/OT Psychosocial support
Supplements Prescriptive therapies
Evaluate Lifestyle changes Rx Compliance
Diagnostic studies Vertebral imaging Fracture occurrence

40
© The CORE Institute. All rights reserved.
Suggested Laboratory Tests Complete blood count Serum chemistry studies Serum 25-hydroxyvitamin D iPTH Bone turnover markers – CTX & P1NP TSH Testosterone 1, 25 Vitamin D 24 hr urine for calcium Phosphorus
Watts NB, et al. AACE Medical Guidelines for Clinical Practice for the diagnosis and treatment of postmenopausal osteoporosis Endocr Pract. 2010;16(suppl 3):1-37. Cosman, et al. Clinician’s guide to prevention and treatment of osteoporosis. Ost Int. 2015; 26:2045-2047.

41
© The CORE Institute. All rights reserved.
Other Laboratory Tests
Lab Test Purpose Erythrocyte sedimentation rate
Malignancy or inflammatory disease
Urinary cortisol or other tests
Adrenal hypersecretion
Serum protein electrophoresis (SPEP) and light chains
Myeloma
Tissue transglutaminase antibodies
Celiac disease

42
© The CORE Institute. All rights reserved.
Pharmacological Treatment Guidelines
Postmenopausal women and men age 50 and older presenting with one of the following:
Fracture - A vertebral or hip fracture T-Score - T-score ≤ -2.5 at the femoral neck, total hip, or
lumbar spine by DXA FRAX® - 10-year probability of a major fracture ≥ 20%
- 10-year probability of a hip fracture ≥ 3%
Cosman, et al. Clinician’s guide to prevention and treatment of osteoporosis. Ost Int. 2015; 26:2045-2047.

43
© The CORE Institute. All rights reserved.
Assess Risk Factors and Measure BMD if Patient Has Risk Factors
T-score between -1.0 and -2.5
FRAX
10-year Probability of Hip Fracture ≥ 3%
or
Probability of All Major Fractures ≥ 20%
Hip or Vertebral Fractures
or
T-score ≤ -2.5 (Spine, Femoral Neck or Total Hip)
Treatment Guidelines: Post-menopausal Women And Men ≥50
www.shef.ac.uk/FRAX

44
© The CORE Institute. All rights reserved.
Medications for Osteoporosis Inhibit Bone Resorption
Bisphosphonates Alendronate (Fosamax) Risedronate (Actonel, Atelvia) Ibandronate (Boniva) Zolendronate (Reclast)
Monoclonal antibody Denosumab (Prolia)
SERM Raloxifene (Evista)
Other Estrogen (various) Calcitonin(Miacalcin, Fortical)
Stimulate Bone Formation
Anabolic Teriparatide (Forteo)

45
© The CORE Institute. All rights reserved.
FDA Approved Medications: Evidence for Fracture Reduction
Medication BMD Vertebral Fx Nonvertebral Fx Hip Fx
Alendronate X X * X
Risedronate XX X X * Ibandronate XX X No effect No effect
Zoledronic acid XX X X X Denosumab XXX X X X Raloxifene X X No effect X Teriparatide XXX X X X
* Evidence for effect, but not FDA approved indication

46
© The CORE Institute. All rights reserved.
Challenges of Osteoporosis Rx
• Success = absence of fracture
• $$$
• Other costs of treatment: – Nuisance of taking another medication – Reminder of illness/condition – Worry about consequences of therapy
• Adverse effects of treatment

Atypical Femoral Fractures With every 50 hip fractures prevented with bisphosphonates,
1 atypical femoral fracture may result. 500/1000 women will suffer a fracture without treatment
Out of 1,000 people on bisphosphonates for 5 years, < 1 will have an atypical fx (.16/1000) & < 1 will have osteonecrosis of the jaw (.01/1000).

48
© The CORE Institute. All rights reserved.
Adherence & Persistence
Patient Pain & Disability “Teachable Moment” Begin regimen early Purposes
Enhance fracture healing Prevent subsequent fractures
Treatment Team Fracture liaison service (FLS) Recognizable face Consistent message Coordinated or Separate appointments Education, counseling and guidance Assure follow-up

49
© The CORE Institute. All rights reserved.
Treatment: Summary Safe and effective therapies are available
Anti-remodeling (antiresorptive) agents • Prevent bone loss and preserve architecture • Reduce the risk of vertebral fractures (all agents) • Alendronate, risedronate, zoledronic acid and denosumab reduce the risk of
nonvertebral and hip fractures Bone building (anabolic) agent: (teriparatide) • Increases bone density and size • Improves quality of bone • Reduces the risk of vertebral and nonvertebral fractures
New Drugs: • Abaloparatide (anticipated Q2 2017): anabolic • Romosozumab (anticipated late 2017): antisclerostin antibody
Patient factors determine the most appropriate drug to use

50
© The CORE Institute. All rights reserved.
Treatment: Summary, continued BMD Change Doesn’t Fully Predict the Reduction in Fracture Risk
Fracture Risk Anti-remodeling treatment decreases fracture risk more rapidly and to a larger extent than one would predict from the relatively small changes in BMD
• Fracture protection can be observed in the absence of a significant change in BMD
Fracture protection persists even when the BMD reaches a plateau • BMD stability does not mean “nonresponse”

51
© The CORE Institute. All rights reserved.
Treatment: Summary, continued
The fracture risk is determined by the complex interactions among bone mineral density (BMD), bone quality, and trauma Contemporary pharmacologic treatments will typically reduce vertebral fracture risk by 30%-70%, with smaller reductions in non-vertebral fracture risk No pharmacologic treatment is likely to reduce fracture risk to zero, in part because of the inability to eliminate trauma There are a number of promising pharmacologic agents—with most of the emphasis to be placed on the development of novel anabolic agents

52
© The CORE Institute. All rights reserved.
Integrate Own The Bone Program: Ten Important Measures to Achieve Success
• NUTRITION COUNSELING* 1. Calcium supplementation 2. Vitamin D supplementation
• PHYSICAL ACTIVITY COUNSELING* 3. Exercise, especially weight-bearing and muscle strengthening 4. Fall prevention education
• LIFESTYLE COUNSELING* 5. Smoking cessation 6. Limiting excessive alcohol intake
• PHARMACOLOGY* 7. Pharmacology for the treatment of osteoporosis
• TESTING* 8. DXA to test bone mineral density
• COMMUNICATION 9. Physician referral letter 10. Follow-up notes and educational materials provided to patient
*Unless contraindicated.
Measures listed here are consistent with recommendations from the National Osteoporosis Foundation, the Centers for Medicare & Medicaid Services, the Joint Commission, the World Health Organization, and the American Medical Association.

53
© The CORE Institute. All rights reserved.
Rewards of Osteoporosis Treatment Reduction in the risk of fracture Reduction in pain and disability Preservation of independence Reduction in height loss Positive effect on mortality (?) Positive effect of being “proactive” Positive effect on BMD Decrease in subsequent fractures Unique benefit to community

54
© The CORE Institute. All rights reserved.
Bone Health Across the Lifespan

55
© The CORE Institute. All rights reserved.
Keep Life in Motion!

56
© The CORE Institute. All rights reserved.
Questions?