Embed Size (px)
Citation preview
CASE REPORT
Osteoma of long bone: an expanding spectrumof imaging findings
Barry Glenn Hansford & Peter Pytel & Drew D. Moore &
Gregory Scott Stacy
Received: 25 June 2014 /Revised: 19 October 2014 /Accepted: 24 October 2014# ISS 2014
Abstract Osteoma of long bone is an extremely rare, benignbone-forming surface lesion with the largest published caseseries consisting of only 14 patients. The most important andoften most difficult lesion to differentiate from osteoma oflong bone radiographically is parosteal osteosarcoma, whichis a rare, low-grade surface osteosarcomawith the potential fordedifferentiation. Reports of imaging studies of osteoma oflong bone depict a well-defined ossified mass arising from thesurface of the diaphysis or metadiaphysis of a long bone. Acharacteristic feature is the homogeneity of the mass, withuniform density near or equal to that of cortical bone from thebase of the lesion to its periphery. The 45-year-old female inthis case presented with left hip fullness and was subsequentlyfound to have a proximal femoral osteoma, which was uniquein that it contained large fatty marrow spaces thatcorresponded to bands of relatively low density on plainradiography and computed tomography, giving it a heteroge-neous appearance atypical of osteoma of long bone. Further-more, the osteoma reported here was associated with a smallbut separate nodular focus of ossification in the adjacent softtissue. These findings led to a presumptive diagnosis ofparosteal osteosarcoma with a local soft tissue metastasis or
satellite nodule resulting in radical resection of the tumor.Definitive diagnosis of osteoma was made on histology ofboth the parent lesion and ossified nodule as no neoplasticspindle cell proliferation was present to establish a diagnosisof low-grade osteosarcoma. This represents, to the best of ourknowledge, the first such presentation of osteoma of longbone.
Keywords Osteoma of long bone . Parosteal osteosarcoma .
Surface lesion
Introduction
Osteoma is a benign surface tumor of bone that is composedof compact bone [1]. The lesion predominantly affects boneformed by intramembranous ossification, in particular theskull and facial bones. Reports of osteoma appearing on thesurface of any bone remote from the skull and facial bones arescant, with its appearance on long bones initially described in1951 by Geschickter and Copeland, who coined the term“parosteal osteoma” to describe such lesions [2]. Since thatinitial report, the literature describing osteoma of long bonehas been primarily composed of scattered case reports, withthe largest published case series from the Mayo Clinic [3–6].Bertoni et al. reported that of the 10,000-plus bone tumors and30,000 bone tumor consultation cases in theMayo Clinic files,only 14 cases of osteoma arising from bones other than theskull and face were identified [7]. The majority of osteomasnot arising from bone formed by intramembranous ossifica-tion occur in the long bones, with additional case reports oflesions in the iliac bone [8–11]. Reports of imaging studiesdepict a well-defined ossified mass arising from the surface ofthe diaphysis or metadiaphysis of a long bone. A characteristicfeature is the homogeneity of the mass, with uniform densitynear or equal to that of cortical bone from the base of the lesion
B. G. Hansford (*)University of Chicago Medicine, 5841 South Maryland Ave, MC526, Chicago, IL 60637, USAe-mail: [email protected]
P. PytelDepartment of Pathology, University of ChicagoMedicine, Chicago,IL, USA
D. D. MooreDepartment of Orthopaedic Surgery, University of ChicagoMedicine, Chicago, IL, USA
G. S. StacyDepartment of Radiology, University of ChicagoMedicine, Chicago,IL, USA
Skeletal RadiolDOI 10.1007/s00256-014-2046-8

to its periphery [8]. The lesion described in this report isunique in that it contained large fatty marrow spaces thatcorresponded to bands of relatively low density on radiogra-phy and computed tomography (CT), giving it a heteroge-neous appearance atypical of osteoma. Furthermore, the oste-oma in this report was associated with a small but separatenodular focus of ossification in the adjacent soft tissue. Thesefindings led to a presumptive diagnosis of parosteal osteosar-coma with a local soft tissue metastasis or satellite nodule andresulted in radical resection of the tumor.
Case report
A 45-year-old Caucasian female, with no significant pastmedical history, presented to her primary care physician witha left buttock mass. She had noticed the mass for several yearsas a generalized area of fullness over the posterior aspect ofthe left buttock and recently began experiencing radicularsymptoms down her leg. The patient denied any history ofrecent or remote trauma to the area. She underwent radiogra-phy, unenhanced computed tomography (CT) andunenhanced magnetic resonance imaging (MRI) of her lefthip as well as whole-body skeletal scintigraphy at outsideinstitutions before being referred to the Orthopaedic OncologyClinic at our institution for definitive management.
On physical examination, the patient had a hard mass in theposteromedial aspect of her left proximal thigh that wasmildlytender to palpation and seemed to be affixed to underlyingbone. The overlying skin was intact, and there was no painwith internal or external rotation of the hip. The patient wasneurovascularly intact.
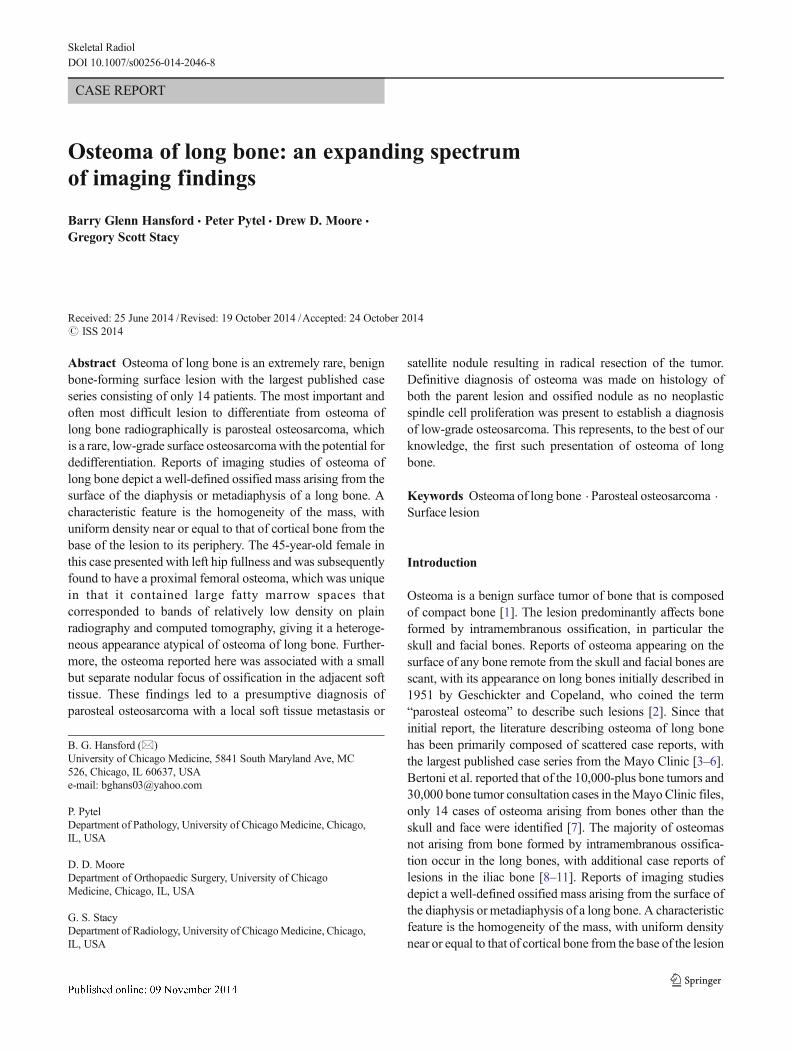
Radiographs revealed a well-demarcated, lobulated, dense-ly ossified mass in close proximity to, if not arising from, theposterior cortex of the proximal femur at the level of the lessertrochanter (Fig. 1a and b). No underlying bone destruction wasevident. The CTscan confirmed that the 7-cmmass arose fromthe posterior cortex of the proximal left femoral diaphysiswithout findings to suggest extension into the intramedullaryspace. The majority of the mass was densely ossified similar tothat of cortical bone with the exception of a branching cleft ofsoft tissue density that traversed the lesion predominantly inthe coronal plane (Fig. 1c and d) as well as a slightly moreheterogeneously ossified region along the anteroinferior aspectof themass (Fig. 1e). A separate, subcentimeter ossified nodulewas identified in the soft tissues approximately 2.5 cm anteriorto the medial margin of the mass, situated between the adduc-tor brevis muscle and distal fibers of the iliopsoas muscle(Fig. 1e). Along the posterior andmedial aspects of the ossifiedmass was a crescentic nonmineralized mass with contentsmeasuring between 5 and 25 HU.
OnMRI, the ossifiedmass was predominantly isointense tocortical bone on all pulse sequences with the exception of a
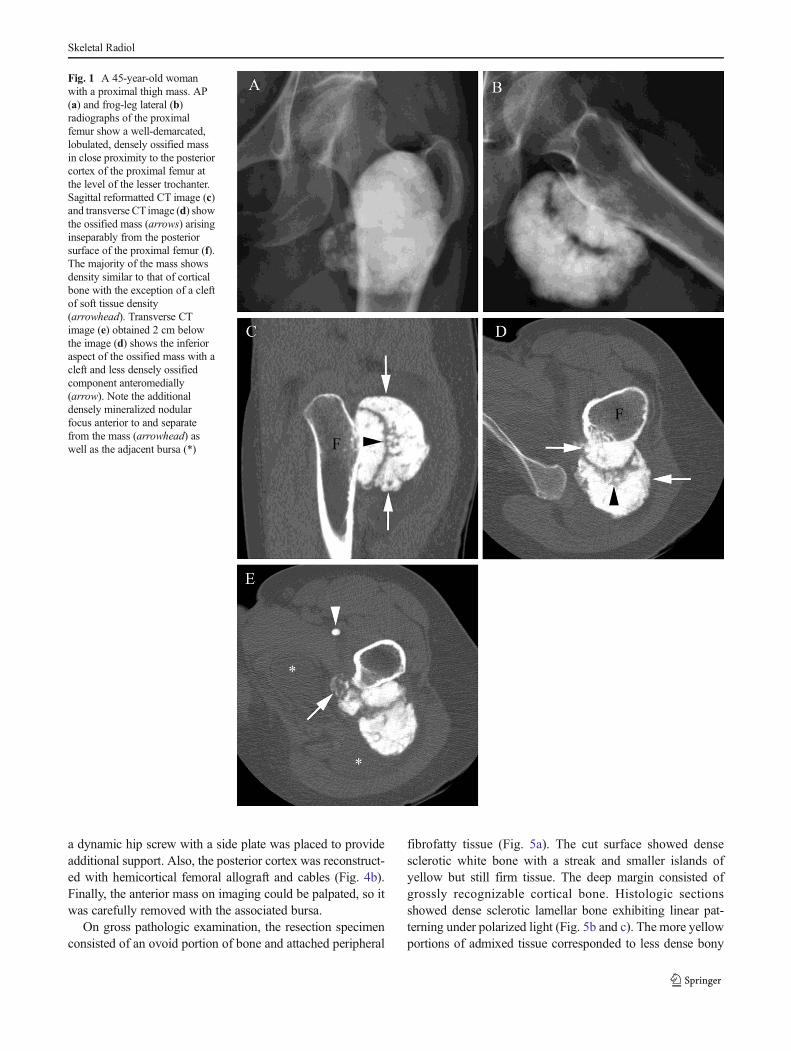
relatively high-density cleft within the lesion corresponding tothe cleft seen on the CT scan (Fig. 2a), as well as a moreheterogeneously low signal intensity region within the inferioraspect of the mass with adjacent soft tissue edema (Fig. 2b).There was no evidence of intramedullary extension, nor wasthere a dominant nonossified peripheral component of themass. The adjacent soft tissue masses seen on the CT scanwere of fluid signal intensity on MRI, compatible with adven-titial bursa formation. The separate ossified nodule in theanterior soft tissues of the hip seen on the CT scan was oflow signal intensity identical to the primary femoral lesionwith a mild hyperintense edema-like signal extending fromthe nodule to the larger ossified mass (Fig. 2b).
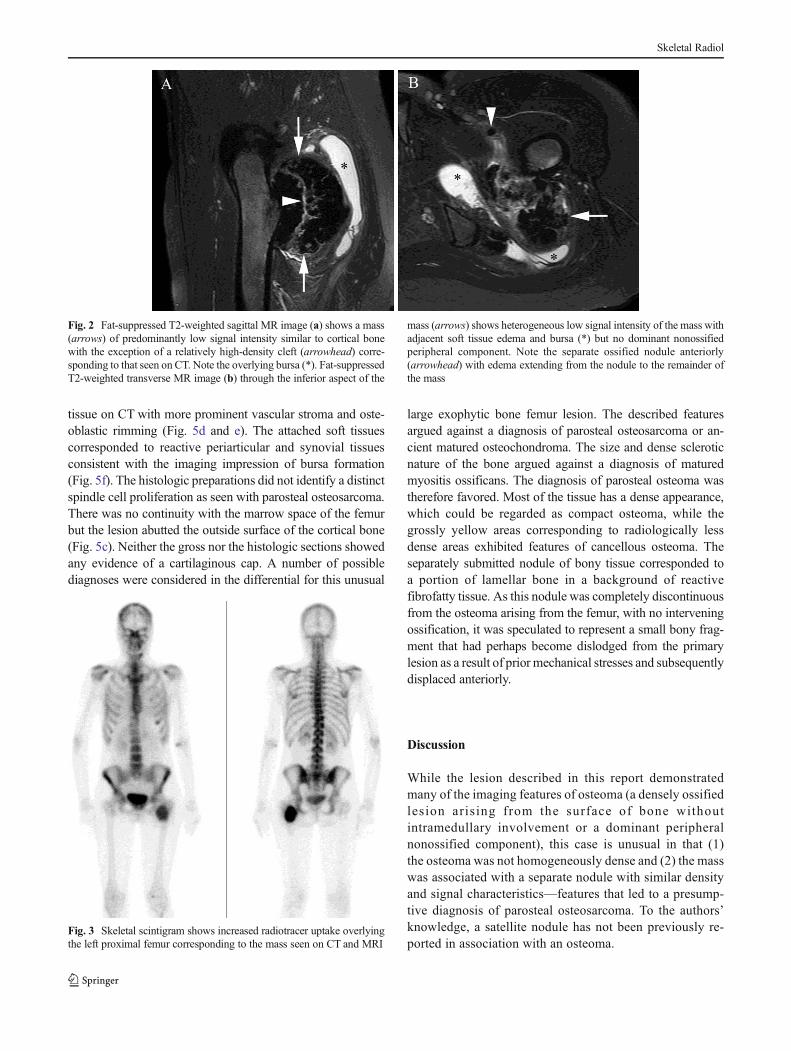
The whole-body bone scan demonstrated increased radio-tracer uptake overlying the left proximal femur lesion but didnot demonstrate any other skeletal lesions (Fig. 3). Subse-quent thoracic CT scan was normal, with no pulmonarynodules.
At this point, the differential diagnosis included a surfaceosteosarcoma, most likely a parosteal osteosarcoma, despitethe fact that there was no dominant peripheral nonossifiedcomponent of the mass. Myositis ossificans was considered inthe differential diagnosis as well, although the adherence ofthe lesion to the underlying bone and the lack of zonal archi-tecture were atypical features, and the patient denied anyprevious trauma. Other reactive ossifying processes such asflorid reactive periostitis/periostitis ossificans and bizarreparosteal osteochondromatous proliferation were also thoughtto be unlikely because of the location, imaging appearanceand clinical features of the lesion. The imaging features alsowere not typical of an osteochondroma, as there was nodefinable medullary continuity between the mass and theunderlying femur. The ossified nodule situated anterior toand separate from the mass was considered to represent thesame process as the mass, as it had similar signal intensity tothe mass and appeared to be associated with it via a trail ofedema-type signal intensity; given the favored diagnosis ofparosteal osteosarcoma, a local soft tissue metastasis or satel-lite nodule, perhaps occurring as a result of prior mechanicalstresses to the lesion, was proposed.
Since parosteal osteosarcoma was the favored diagnosiswith a possible soft tissue satellite nodule, surgical resectionwas recommended. A standard posterior lateral approach tothe hip was utilized, with the insertion of the gluteus maximusreleased to allow adequate exposure. The sciatic nerve wasadjacent to the mass and its overlying bursa but not adherentand was carefully isolated. The external rotators were attenu-ated over the mass and divided in order to allow completeexposure of the mass. A sagittal saw was used withosteotomes to remove the posterior hemicortex of the proxi-mal femur in order to completely resect the mass with ade-quate margins (Fig. 4a). Care was taken to preserve thefemoral neck. In order to diminish the risk of a future fracture,
Skeletal Radiol
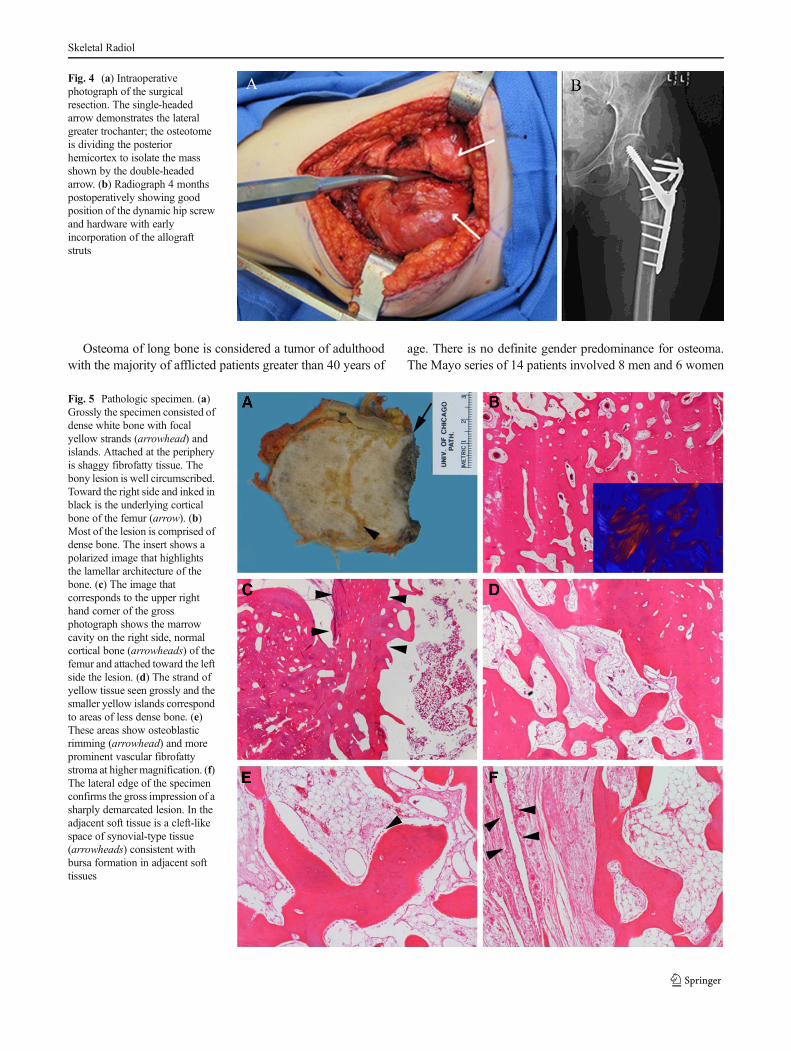
a dynamic hip screw with a side plate was placed to provideadditional support. Also, the posterior cortex was reconstruct-ed with hemicortical femoral allograft and cables (Fig. 4b).Finally, the anterior mass on imaging could be palpated, so itwas carefully removed with the associated bursa.
On gross pathologic examination, the resection specimenconsisted of an ovoid portion of bone and attached peripheral
fibrofatty tissue (Fig. 5a). The cut surface showed densesclerotic white bone with a streak and smaller islands ofyellow but still firm tissue. The deep margin consisted ofgrossly recognizable cortical bone. Histologic sectionsshowed dense sclerotic lamellar bone exhibiting linear pat-terning under polarized light (Fig. 5b and c). The more yellowportions of admixed tissue corresponded to less dense bony
Fig. 1 A 45-year-old womanwith a proximal thigh mass. AP(a) and frog-leg lateral (b)radiographs of the proximalfemur show a well-demarcated,lobulated, densely ossified massin close proximity to the posteriorcortex of the proximal femur atthe level of the lesser trochanter.Sagittal reformatted CT image (c)and transverse CT image (d) showthe ossified mass (arrows) arisinginseparably from the posteriorsurface of the proximal femur (f).The majority of the mass showsdensity similar to that of corticalbone with the exception of a cleftof soft tissue density(arrowhead). Transverse CTimage (e) obtained 2 cm belowthe image (d) shows the inferioraspect of the ossified mass with acleft and less densely ossifiedcomponent anteromedially(arrow). Note the additionaldensely mineralized nodularfocus anterior to and separatefrom the mass (arrowhead) aswell as the adjacent bursa (*)
Skeletal Radiol
tissue on CT with more prominent vascular stroma and oste-oblastic rimming (Fig. 5d and e). The attached soft tissuescorresponded to reactive periarticular and synovial tissuesconsistent with the imaging impression of bursa formation(Fig. 5f). The histologic preparations did not identify a distinctspindle cell proliferation as seen with parosteal osteosarcoma.There was no continuity with the marrow space of the femurbut the lesion abutted the outside surface of the cortical bone(Fig. 5c). Neither the gross nor the histologic sections showedany evidence of a cartilaginous cap. A number of possiblediagnoses were considered in the differential for this unusual
large exophytic bone femur lesion. The described featuresargued against a diagnosis of parosteal osteosarcoma or an-cient matured osteochondroma. The size and dense scleroticnature of the bone argued against a diagnosis of maturedmyositis ossificans. The diagnosis of parosteal osteoma wastherefore favored. Most of the tissue has a dense appearance,which could be regarded as compact osteoma, while thegrossly yellow areas corresponding to radiologically lessdense areas exhibited features of cancellous osteoma. Theseparately submitted nodule of bony tissue corresponded toa portion of lamellar bone in a background of reactivefibrofatty tissue. As this nodule was completely discontinuousfrom the osteoma arising from the femur, with no interveningossification, it was speculated to represent a small bony frag-ment that had perhaps become dislodged from the primarylesion as a result of prior mechanical stresses and subsequentlydisplaced anteriorly.
Discussion
While the lesion described in this report demonstratedmany of the imaging features of osteoma (a densely ossifiedlesion arising from the surface of bone withoutintramedullary involvement or a dominant peripheralnonossified component), this case is unusual in that (1)the osteoma was not homogeneously dense and (2) the masswas associated with a separate nodule with similar densityand signal characteristics—features that led to a presump-tive diagnosis of parosteal osteosarcoma. To the authors’knowledge, a satellite nodule has not been previously re-ported in association with an osteoma.
Fig. 2 Fat-suppressed T2-weighted sagittal MR image (a) shows a mass(arrows) of predominantly low signal intensity similar to cortical bonewith the exception of a relatively high-density cleft (arrowhead) corre-sponding to that seen on CT. Note the overlying bursa (*). Fat-suppressedT2-weighted transverse MR image (b) through the inferior aspect of the
mass (arrows) shows heterogeneous low signal intensity of the mass withadjacent soft tissue edema and bursa (*) but no dominant nonossifiedperipheral component. Note the separate ossified nodule anteriorly(arrowhead) with edema extending from the nodule to the remainder ofthe mass
Fig. 3 Skeletal scintigram shows increased radiotracer uptake overlyingthe left proximal femur corresponding to the mass seen on CT and MRI
Skeletal Radiol
Osteoma of long bone is considered a tumor of adulthoodwith the majority of afflicted patients greater than 40 years of
age. There is no definite gender predominance for osteoma.The Mayo series of 14 patients involved 8 men and 6 women
Fig. 4 (a) Intraoperativephotograph of the surgicalresection. The single-headedarrow demonstrates the lateralgreater trochanter; the osteotomeis dividing the posteriorhemicortex to isolate the massshown by the double-headedarrow. (b) Radiograph 4 monthspostoperatively showing goodposition of the dynamic hip screwand hardware with earlyincorporation of the allograftstruts
Fig. 5 Pathologic specimen. (a)Grossly the specimen consisted ofdense white bone with focalyellow strands (arrowhead) andislands. Attached at the peripheryis shaggy fibrofatty tissue. Thebony lesion is well circumscribed.Toward the right side and inked inblack is the underlying corticalbone of the femur (arrow). (b)Most of the lesion is comprised ofdense bone. The insert shows apolarized image that highlightsthe lamellar architecture of thebone. (c) The image thatcorresponds to the upper righthand corner of the grossphotograph shows the marrowcavity on the right side, normalcortical bone (arrowheads) of thefemur and attached toward the leftside the lesion. (d) The strand ofyellow tissue seen grossly and thesmaller yellow islands correspondto areas of less dense bone. (e)These areas show osteoblasticrimming (arrowhead) and moreprominent vascular fibrofattystroma at highermagnification. (f)The lateral edge of the specimenconfirms the gross impression of asharply demarcated lesion. In theadjacent soft tissue is a cleft-likespace of synovial-type tissue(arrowheads) consistent withbursa formation in adjacent softtissues
Skeletal Radiol

with a mean age of 45 years. The youngest reported patientwith an osteoma was 10 years old and the oldest was 75 yearsold. In the Mayo Clinic bone tumor series, the authors report-ed 67 cases of parosteal osteosarcoma, with an additional 159parosteal osteosarcomas in the consultation case files. Thisreflects a 16:1 ratio of parosteal osteosarcoma to osteoma oflong bone, emphasizing just how rare osteoma of long bone is[7].
Osteoma of long bone is considered a distinct entity on thebasis of radiographic, clinical and histologic features. Theprognosis for osteoma is excellent without a propensity forlocal recurrence after complete surgical excision or significantregrowth after surgical debulking [7, 12]. Classically, osteomaof long bone presents as an asymptomatic, long-standinglesion, although it may present with a history of chronic pain.Larger lesions may result in a hard mass, adventitial bursaformation and impingement upon adjacent neurovascularstructures [8, 12, 13].
Prior reports of osteomas of long bone describe bonylesions that histologically consist of dense sclerotic lamellarbone with haversian systems [7]. These lesions do not extendinto or invade the medullary cavity. Osteomas can be dividedhistologically into compact, spongious and mixed subtypes.Cancellous areas show bone lined by osteoblasts and have amore well-vascularized stroma [1]. A distinct spindle cellproliferation as characteristic for parosteal osteosarcoma isabsent [7, 8].
Radiographically, osteoma of long bone typically appearsas a uniform, dense sclerotic lesion (as dense as cortical bone)attached to the surface of the diaphysis or metadiaphysis of along bone with smooth margins but without intervening ra-diolucencies [7, 8, 12, 14]. However, larger osteomas mayhave prominently lobulated margins, as demonstrated byBertoni et al., which could be susceptible to physical activity[7]. On CT, the periphery of the tumor is as dense as the basewithout an associated soft tissue mass. The cortex from whichosteoma arises is sclerotic without findings of intramedullaryextension. CT is useful to demonstrate the density of osteoma,similar to normal cortical bone, and classically devoid of focalradiolucent or aggressive osteolytic features [14, 15]. Howev-er, the osteoma described in this case report contained cancel-lous areas that corresponded to less dense foci on CT, which inpart prompted a leading diagnosis of parosteal osteosarcoma.MRI typically reveals a lesion that follows the signal intensityof normal cortical bone on all sequences (extremely T1 and T2hypointense) without findings to suggest intramedullary ex-tension or an associated soft tissue component [8, 12, 15]. Inour case, areas of higher signal intensity corresponded tocancellous regions histologically.
The distinction between parosteal osteosarcoma and oste-oma of long bone is critical given that osteoma is a benignentity and parosteal osteosarcoma is a low-grade malignantneoplasm. Parosteal osteosarcoma, while accounting for only
4 % of all types of osteosarcoma, is the most common surfaceosteosarcoma (65 %). Parosteal osteosarcoma has a slightfemale predominance (unusual for a bone tumor) and has abetter prognosis than other types of osteosarcoma, with a 5-year survival rate of 90–95 % [16]. Similar to osteoma,parosteal osteosarcoma most often occurs in the 3rd and 4thdecades of life and presents with a mass that is typically notpainful, although low-grade pain is not unusual. Parostealosteosarcoma is a primarily metaphyseal lesion (90 %) witha strong site preference for the posterior cortex of the distalfemoral metadiaphysis (65 %) [16–18].
There is little in the literature regarding parosteal osteosar-coma with metastases at initial presentation since mostparosteal osteosarcomas are slow-growing, low-grade malig-nancies that come to clinical attention before metastases occur.Parosteal osteosarcoma may be associated with late lungmetastases as well as local recurrence if the primary lesionhas been incompletely treated/excised. Up to 24 % ofparosteal osteosarcomas have foci of dedifferentiation at thetime of initial presentation or recurrence, which radiographi-cally may be represented by pockets of relatively lucent fociwithin regions of more dense-appearing bone. Thesededifferentiated lesions have a worse prognosis, which issimilar to that of conventional osteosarcoma [18]. There havebeen case reports of parosteal osteosarcoma with local softtissue metastases at initial presentation [19, 20]. Furthermore,local soft tissue metastases are not uncommon in cases ofparosteal osteosarcoma recurrence, and multiple calcified softtissue metastases have been observed in a case of recurrentconventional osteosarcoma without pulmonary metastases[21, 22].
Differentiating between osteoma of long bone andparosteal osteosarcoma can be challenging radiographicallywith many cases, including the current case, requiring biopsy/total excision for definitive diagnosis. When differentiatingbetween osteoma and parosteal osteosarcoma, there are sev-eral key imaging features that may help one suggest the mostlikely diagnosis. Perhaps most importantly, on radiographyand CT, osteoma is typically composed of well-marginateddense, solid bone, typically without interposed regions offocal lucency, although as we have shown, this is not auniversal feature of osteoma. The lobulated or smooth periph-ery of osteoma is as dense as the base of the tumor [14].Parosteal osteosarcoma may have a lobular appearance; how-ever, the lesion is rarely as homogeneous and dense as oste-oma, with scattered internal regions of radiolucency. Also, theperiphery of parosteal osteosarcoma is typically more irregu-lar and less ossified than at the base of the lesion with a cloud-like appearance and unmineralized peripheral components[12]. Parosteal osteosarcoma usually wraps around the cir-cumference of the long bone as it grows, with parts of thelesion lying directly adjacent to the cortex without attaching toit, resulting in a plane of cleavage known as the “cleft” sign
Skeletal Radiol

[23]. Parosteal osteosarcoma demonstrates progressivegrowth and will often invade adjacent soft tissue structuresas well as bone; therefore, on MRI, evaluation of parostealosteosarcoma with fluid-sensitive sequences demonstrateshigh signal intensity at the periphery of the lesion and possiblywithin the cortex and marrow as well [24]. While osteoma oflong bone may be associated with adventitial bursa formation,a non-ossified soft tissue component should not be present [7],and osteoma will not extend into the intramedullary space [12,24]. Little has been published on the bone scan appearance ofosteoma. One experiential report by Lambiase et al. regardingthree-phase bone scans states that osteoma tends to not showincreased radiotracer uptake on blood-flow or blood-poolimaging with faint uptake on delayed imaging. Meanwhile,parosteal osteosarcoma usually shows increased radiotraceruptake on blood-flow and blood-pool imaging as well asintense uptake on delayed imaging [12].
The treatment of osteoma of long bone hinges on the abilityto definitively differentiate it from malignant entities such asparosteal osteosarcoma. Therefore, if biopsy can be performedin such a manner to provide adequate tissue for the pathologistand not jeopardize limb salvage options for definitive surgery,it should be pursued. If biopsy demonstrates osteoma, thelesion could be followed closely with serial radiographs ifthe patient is asymptomatic. It may continue to grow slowlyover time. However, rapid growth to suggest malignancy,pain, or functional impairment would all justify surgical re-section. If biopsy would jeopardize limb salvage options, as inthe presented case, then wide excision is recommended as itwill be curative regardless of whether the mass is an osteomaor low-grade surface osteosarcoma [18].
In summary, we report a case of a 45-year-old female withosteoma of long bone, which mimics parosteal osteosarcomawith a local soft tissue metastasis or satellite nodule. Thisrepresents, to the best of our knowledge, the first such presen-tation of osteoma. Pathology provided a definitive diagnosisof osteoma rather than osteosarcoma, with the ossified noduleperhaps representing a fragment that had dislodged from theparent lesion. In light of this case, it is important not to excludethe diagnostic possibility of osteoma when encountering adensely ossified surface lesion of bone without a dominantnonossified peripheral component, even if the mass showssome internal components of cancellous bone that are not asdense as cortical bone.
Conflict of interest No conflict of interest
References
1. Fletcher CDM, Unni KK, Mertens F (Eds): World HealthOrganization classification of tumours. pathology and genetics oftumours of soft tissue and bone. IARC Press: Lyon 2002.
2. Geschickter CF, Copeland MM. Parosteal osteoma of bone: a newentity. Ann Surg. 1951;133:790–807C.
3. Meltzer CC, Scott JrWW,McCarthy EF. Case report 698: osteoma ofthe clavicle. Skelet Radiol. 1991;20:555–57.
4. Cervilla V, Haghighi P, Resnick D, Sartoris DJ. Case report 596:parosteal osteoma of the acetabulum. Skelet Radiol. 1990;19:135–37.
5. Baum PA, Nelson MC, Lack EE, Bogumill GP. Case report560: parosteal osteoma of the tibia. Skelet Radiol. 1989;18:406–09.
6. Chikuda H, Goto T, Ishida T, Iijima T, Nakamura K. Juxtacorticalosteoma of the ulna. J Orthop Sci. 2002;7:721–30.
7. Bertoni F, Unni KK, Beabout JW, Sim FH. Parosteal osteoma ofbones other than the skull and face. Cancer. 1995;75:2466–73.
8. Sundaram M, Falbo S, McDonald D, Janney C. Surface osteomas ofthe appendicular skeleton. AJR Am J Roentgenol. 1996;167:1529–33.
9. Houghton MJ, Heiner JP, De Smet AA. Osteoma of the innominatebone with intraosseous and parosteal involvement. Skelet Radiol.1995;24:455–57.
10. Ehara S. Parosteal osteoma of the iliac bone. Skelet Radiol. 1998;27:650.
11. Soler Rich R, Martinez S, de Marcos JA, Salas A, Lluc P,Granados J. Parosteal osteoma of the iliac bone. Skelet Radiol.1998;27:161–63.
12. Lambiase RE, Levine SM, Terek RM,Wyman JJ. Long bone surfaceosteomas: imaging features that may help avoid unnecessary biop-sies. AJR Am J Roentgenol. 1998;171:775–80.
13. O’Connell JX, Rosenthal DI, Mankin HJ, Rosenberg AE. Solitaryosteoma of a long bone. J Bone Joint Surg Am. 1993;75:1830–34.
14. Seeger LL, Yao L, Eckardt JJ. Surface lesions of the bone. Radiology.1998;206:17–33.
15. Yun S, Jin W, Park YK, et al. Simultaneously detected parostealosteoma and osteochondroma in the distal femur of a single patient.Clin Imaging. 2013;37:950–53.
16. Murphey MD, Robbin MR, McRae GA, Flemming DJ, Temple HT,Kransdorf MJ. The many faces of osteosarcoma. Radiographics.1997;17:1205–31.
17. Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK.Parosteal osteosarcoma. A clinicopathological study. J Bone JointSurg Am. 1994;76:366–78.
18. Bertoni F, Bacchini P, Staals EL, Davidovitz P. Dedifferentiatedparosteal osteosarcoma: the experience of the Rizzoli Institute.Cancer. 2005;103:2373–82.
19. Murashkovskii MA. Parosteal osteosarcoma with soft tissue metas-tasis. Vestn Rentgenol Radiol. 1977;3:86–8.
20. Takeuchi K, Morii T, Yabe H, Morioka H, Mukai M, Toyama Y.Dedifferentiated parosteal osteosarcoma with well-differentiated me-tastases. Skelet Radiol. 2006;35:778–82.
21. DingY, Cai YB, ZhangQ. Parosteal osteosarcoma: a clinical study of48 cases. Zhongua Wai Ke Za Zhi. 2003;41:832–36.
22. Wolf R, Wolf RF, Hoekstra HJ. Recurrent, multiple, calcified softtissue metastases from osteogenic sarcoma without pulmonary in-volvement. Skelet Radiol. 1999;28:710–13.
23. Papathanassiou ZG, Alberghini M, Thiesse P, et al. Parosteal osteo-sarcoma mimicking osteochondroma: a radio-histologic approach ontwo cases. Clin Sarcoma Res. 2011;1:1–7.
24. Donmez FY, Tuzun U, Basaran C, Tunaci M, Bilgic B, Acunas G.MRI findings in parosteal osteosarcoma: correlation with histopa-thology. Diagn Interv Radiol. 2008;14:142–52.
25. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, GannonFH. Imaging of osteochondroma: variants and complicationswith radiologic-pathologic correlation. Radiographics. 2000;20:1407–34.
26. McCarthy EF, Sundaram M. Heterotopic ossification. A review.Skelet Radiol. 2005;34:609–19.
Skeletal Radiol



![Peripheral osteoma of the mandibular crest: a short case study · Osteoma is a benign osseous lesion characterized by the proliferation of cancellous and/or cortical bone [1]. It](https://img.pdfslide.us/doc/110x75/5fcec12c32d22e4f667c7367/peripheral-osteoma-of-the-mandibular-crest-a-short-case-study-osteoma-is-a-benign.jpg)














![Percutaneous image-guided ablation of bone and soft tissue ... · oid osteoma [23, 24]. Ever since, for the therapy of this benign tumour, thermal ablation constitutes a first-line](https://img.pdfslide.us/doc/110x75/5cbf758888c9932c128b8add/percutaneous-image-guided-ablation-of-bone-and-soft-tissue-oid-osteoma-23.jpg)








