Embed Size (px)
Citation preview

ORTHOPEDIC SURGERY IN THE EUROPEANTHEATER OF OPERATIONS
I IA BRIEF RESUME
COLONEL MATHER CLEVELAND, M.C.Army of the United States (inactive)
SENIOR CONSULTANT IN ORTHOPEDIC SURGERY, E.T.O.
NEW YORK CrrY, N. Y.
THE PROFESSIONAL SERVICE Division of the Surgeon's office of the Euro-pean Theater was established in August or September of I942 under MajorGeneral Paul A. Hawley as Chief Surgeon and Colonel, later General, ElliottCutler as Chief Surgical Consultant and Colonel William Middleton as ChiefMedical Consultant for the Theater. Senior consultants for the Theater in allthe various medical and surgical specialties were soon added. The first SeniorConsultant in Orthopedic Surgery was Colonel Rex Diveley, who served assuch from September of I942 until the middle of May, i944, when he was re-lieved of this assignment to devote his full-time to the Rehabilitation Division.The writer arrived in the Theater on D-Day minus 2o-or about three weeksbefore the invasion of the Normandy beachhead-to assume the duties ofSenior Consultant in Orthopedic Surgery. A tour of duty of one year at theStation Hospital at Fort Jackson had afforded an adequate background ofthe injuries incident to training at a large infantry post. Nine months asOrthopedic Consultant for the Fourth Service Command, with its I31Station and I I General Hospitals offered further opportunity to becomefamiliar with the bone and joint problems found among the soldiers in trainingand returned from overseas. The earlier battle casualties with compound frac-tures and amputations arriving from North Africa, Italy and the Pacific wereseen. At that time the vast majority of these compound fractures had beentreated by the Orr-Trueta method, which left much to be desired. Returningamputees usually had not been subjected to skin traction and exposed boneends were all too commonly encountered.
It was apparent to all surgeons of the various Theaters that there wasroom for improvement in the care of battle casualties with wounds involvingbones and joints.
The newly arrived Senior Consultant in Orthopedic Surgery was han(di-capped by a lack of knowledge of the hospital and personnel situation iiithe Theater. Time was pressing, since the invasion was about to burstmomentarily. In a period of approximately three weeks, in company withLt. Col. William J. Stewart, who had served as assistant to Colonel Divelevbetween 40 and 50 hospitals were visited and the neophyte was indoctrinatedto the extent that time and other circumstances allowed. Our headquarterswere then in Cheltenham, later briefly in London, and even more briefly atVallognes on the Normandy beachhead, and, finally, in Paris. The dutiesof a consultant who serves as eyes and ears for the Chief Surgeon and asteacher and adviser to the younger surgeons who are actually taking care
188

Volume 124Number 2 ORTHOPEDIC SURGERY IN WORLD WAR II
of the wounded, carries him on a constant round of visits to the variousmedical installations of all echelons from Field Hospital, and occasionally evenfurther forward, back to the fixed hospitals. How many thousands of mileswe covered by plane, jeep, command, or in rare instances staff car, will neverhe accurately known.
PRE 1-DAY ACTIVITIES OF THE ORTHOPEDIC SURGEONS IN THE THEATER
The orthopedic or traumiiiatic surgeons were a fortunate group in theArmy, in that theyr were always busv and, therefore, on the wlhole, contentedl.I'he increasing .Armny in the tnited Kingdom that was training so strenuouislIfor the invasion hadl imiany inijuries of varying severity. The Air Force sta-tioned for the most part in East Anglia sustained battle casualties from thetime they became operational, and there were many compound fracturesto treat.
During this period of Army training, the Medical Corps had its trainingprogram. Classes were held constantly for instruction of the officers andenlisted men. Plaster of paris technic was taught continually. There wasunanimity of opinion regarding most of the plaster of paris circular splintsintended for the transportation of the wounded. The Tobruk splint wasthe single exception. This utilization of a full-ring Thomas splint, withadhesive traction and plaster of paris reenforcement, was enthusiasticallyrecommended by our British colleagues for transportation of compound frac-tures of the femur, and prior to the invasion its application was taught andadvocated. Surgeons returning to the Theater from the North Africancampaign reported that this splint was far from satisfactory, stating that aplaster of paris spica was superior in every respect. As time passed we becamemore firmly convinced that the plaster of paris spica splint from the knee ofthe sound leg and from the toes of the fractured leg, reenforced by a posteriorstrut, afforded the safest and most comfortable means of immobilization ofthe fractured femur while in transit.
The Chief Surgeon, aided by his consultant staff, prepared a Manual ofTherapy for the E.T.O. This was issued in May of I944. This smallvolume contains a good deal of sound basic medicine and surgery and certaintechnics of treatment are described. The surgical authors were handicappedI)y the fact that prior experience in the case of battle casualties was limited,and in some instances nonexistent. This manual of therapy was supple-mented from time to time by circular letters from the office of the ChiefSurgeon as experience was gained. When V-E Day arrived, we had estab-lished a satisfactory technic for the care of battle casualties with bone andjoint injuries, and all that remained was to find and place the surgeonsequipped or trained to carry it out. This brings us to the next problem.
Personnel: The earliest hospitals to arrive in the Theater were affiliatedunits, well-staffed General, Station and Evacuation Hospitals, bursting withmedical and surgical skills. Each of these early hospitals had from two tofour or five officers trained in bone and joint surgery. As time went on and
189

COLONEL MATHER CLEVELAND Annals of SurgeryAugust, 1946
the Army grew, many other hospitals were added, until, finally, there was atotal of 260 hospitals in the Theater. Of these, I43 were I,ooo-bed GeneralHospitals. The orthopedic requirements for these hospitals by Table ofOrganization was approximately a total of 446 medical officer specialists(3153) with a rating of "B" or "C," which was supposed to indicate fullcivilian training and some experience in civilian practice. To produce thisiitumber of specialists would have required a black tail coat, a silklhat and a wand. There were, in June, I944, approximately 820 diplo-miiats of the American Board of Orthopedic Surgery. Three hundredand one of these entered the armed services and some 63 were in theE.T.O. Six of these were immobilized as consultants or commanding officers,etc., or had been returned to the Zone of Interior, so that only 57 were avail-able for the actual care of the wounded. To supplement these "elder states-men," there were some 95 officers who had had partial civilian training inorthopedic surgery and 85 general surgeons who had had training in traumaticsurgery. The remaining officers who filled the additional I75 positions, witha specialist rating in orthopedic surgery, had received their entire trainingin the Army. It was a matter of grim necessity to plunder the original affiliatedunits, rich in trained personnel, to supply those hospitals arriving later withundertrained officers or often none capable of assuming the duty of Chief ofOrthopedic Section. Since our affiliated units formed less than ten per centof the total hospitals, the inroads on these units were heavy and constant.There was, of course, an obvious end to this sort of business of dilution ofthe talent. When V-E Day arrived, the sanity of the Senior Consultant inOrthopedic Surgery was just preserved, as there were some six or eightnewly arrived hospitals calling for an orthopedic specialist, with none in sight.With the cessation of hostilities these frantic cries could finally be answered
"so what"? The amazing fact remains that so much creditable surgerywas done with so little, relatively well-trained personnel available.
An interesting and significant wound study was made prior to D-Day inEast Anglia, where Air Force casualties were received. Three parallel groupsof wounds were treated as follows: (i) Adequate debridement and immediateprimlary closure. (2) Adequate debridement, immediate primary closure andsulfonamides. (3) Adequate debridement, immediate primary closure andpenicillin. There was no essential difference in the healing in these threegroups. The low incidence of infection was almost identical in each group.The one factor each group had in common was the surgical treatment andthe study pointed unquestionably to the fact that surgical treatment was ofparamount importance. It was of course obvious that no parallel regardingimmediate primary closure of wounds existed between the Air Force per-sonnel, wounded at high altitudes in clean surroundings, with ample oppor-tunity to bathe, and the infantrymen, who, unwashed, in dirty clothes, wereto be wounded on the heavily manured soil of France and the low countries.To close immediately wounds under these latter coniditions wouild have beeiutter folly.
190

Volume 124Number 2 ORTHOPEDIC SURGERY IN WORLD WAR II
The Medical Corps set up to service the invasion was carefully planned.Surgical teams were assigned to the LST's and other transports that wouldreturn the wounded. Field Hospital platoons were set up on the far shorewithin a few days. The first Evacuation Hospitals were set up within a weekafter the beachhead was established.
The fixed hospitals in the United Kingdom were emptied of all excepturgent cases. Surrounding the ports of embarkation there were some I5 ofthese fixed hospitals, which were designated as Transit Hospitals, and servedfor some six weeks or longer as Evacuation Hospitals for the woundedwhich were transportable from the far shore. These evacuable wounded hadmainly extremity wounds, about half of them with compound fractures
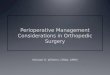
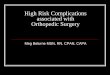
REGIONAL DISTRIBUTION OF WOUNDSIN WIA CASUALTIES DURING 3 WARS
4S. [ CIVIL wAR
WIOULD WARI
6. U_ = * tWORLD WARII
11~~~~1LOWER UPPEt OIST "CAD AIDO
EXTRIEITIES EXTREMITIES EPER CENT Of NICKBODY SURFACE AREA 39 It le 11
CHART I.-A table furnished by the Office of the Surgeon-General, ProfessionalService Division.
This comparison of the wounded in our three major wars is of great interest.The great preponderance of extremity wounds in each war is shown, 73 per cent inthe Civil War, 8I.6 per cent in World War I, and 70.9 per cent in World War II.Since approximately half of the extremity wounds involve bones or joints, it will beseen that between 35 per cent and 40 per cent of all battle casualties require the serviceof a bone and joint surgeon. Surgical personnel of all Army hospitals during hos-tilities should be set-up with this in mind.
The wounded and killed in action are doubtless hit in the various areas of thebody in direct proportion to the per cent of total body-surface area which any part-epresents. These percentages of body-surface areas are indicated on the figures belowthe chart. It will be noted that there is a tremendous surplus of survivors in theextremity wounds and an equally marked deficit of survivors in the chest and abdominalwounds, as would be expected. The abdominal and chest wounds are apt to be imme-diately fatal due to massive hemorrhage.
It is interesting to note that in World War I the surviving chest and abdominalwounds were far below both the Civil War and World War II. This doubtless meansthat first aid and surgery had failed to keep pace with the enormously increaseddestructive force of the high explosive shells and high velocity small arms fire. Thebalance was restored in this war, despite even greater havoc and destruction wroughtby the missiles used.
191

COLONEL MATHER CLEVELAND Annals of Sur ery
(Chart I). Primary surgical treatment was administered in these TransitHospitals, and 12 to 36 hours later the wounded were evacuated to other fixedhospitals for more definitive treatment.
The first of the fixed hospitals to accompany the invading force wasopened on the far shore on August I, I944. The fixed hospitals which re-mained in the United Kingdom had, on the whole, excellent facilities andsplendid equipment, and above all a stable set-up. It was to these hospitalsthat the bone and joint casualties, requiirinig a long-holding period, wereevacuated.
The first fixed hospitals which moved to the conitiinent in Normandy wereunder tentage. Many of these hospitals miioved to a second or third site asthe Army advanced. Most of them were under permanent shelter during thewinter. Their facilities were for the most part not as desirable as those whichthey left behind in the United Kingdom, but they managed to improvise inan amazingly efficient manner. From the standpoint of the orthopedic orbone and joint surgeon, an assignment in the United Kingdom offered greateropportunity for long-time contact with bone and joint casualties than didservice in the continental hospitals which served mainly on a transit basis,evacuating the compound fractures and amputees to the United Kingdom atthe earliest possible moment. Only if evacuation had been or seemed likelyto be unavoidably delayed beyond the optimum period for the use of skeletaltraction (i.e., within 2I days after wounding), were these continental hos-pitals permitted to treat these long bone fractures.
Air evacuation from the continent to the United Kingdom was startedwithin the first week of the invasion and a series of Air Transit Hospitals wereset up near Swindon to receive these casualties. This air evacuation, whichis ideal, continued and grew in importance until finally the great bulk of thepatients were transported within the Theater by this means. During Decemberand January, the period of heavy fogs, air evacuation bogged down almostcompletely due to the weather. This weather "road block" is unavoidableand must always be considered.
CARE OF THE WOUNDED WITH BONE AND JOINT CASUALTIES
I. First Aid: So much has been written about the care of the woundedin hospitals and so little acknowledgment has been given to the devoted, skilfulcare which our wounded received from the corpsmen and officers at thebattalion level. Many of our records state that the wounded were dressedand on the way back within 20 minutes to an hour after wounding. Thegreat bulk of this was done by medical enlisted men. A large number of thesemedical soldiers and officers gave their lives in attempting to secure the highstandard of care which was set for our wounded.
Splints: Compound fractures of the femur and tibia and fibula wereimmediately placed in the Army leg splint (a half-ring Thomas splint) witha boot strap to secure traction. This boot strap is dangerous and if appliedfor more than two or three hours may cause pressure necrosis over the dorsum
192

Volume 124Number 2 ORTHOPEDIC SURGERY IN WORLD WAR II
of the foot. Adhesive traction should be substituted if prolonged use of thissplint is necessary.
For compound fractures of the foot and ankle, the well-padded wire laddersplint was used. Upper extremity compound fractures were most comfortablyand effectively treated for transportation by slings or swathes. The Murray-Jones splint is dangerous to circulation and its use was pretty universallycondemned.
2. Resuscitation: At the battalion level, plasma was available and wholeblood was administered at the clearing station. It was quickly learned thatwhole blood alone could serve as adequate replacement where there had beenmassive hemorrhage. Blood was employed extensively in the treatment ofthese wounded at all medical installations from the clearing station to andincluding the General Hospitals.
3. Army Hospitals: The bone and joint casualties for the most part areconsidered transportable, so they were sent to the Evacuation Hospitals whilethe nontransportable abdominal and chest 'wounds were treated at the FieldHospitals. Primary surgical treatment was instituted in these EvacuationHospitals.
Wound Excision or Debridement: This is easier to describe than toachieve. All possible skin should be preserved and only that obviously necroticshould be excised. The wound should be opened with adequate longitudinalincisions and exposure of underlying tissue with adequate retraction secured.A peep-hole debridement invited subsequent infection. To aid exposure andavoid any tension, the fascia should be divided longitudinally and transverselyif necessary. All dead or damaged muscle or fascia must be excised, removingall dirt and available foreign bodies. All bone should be preserved. Evencompletely loose fragments will heal and amalgamate with the general callusif skin coverage is secured by delayed primary closure and infection does notensue. The wanton removal of all loose bone in many instances means a com-plete gap or loss of bone substance which can only be substituted for by subse-quent bone graft. Many of these compound fractures with numerous com-pletely detached fragments of bone heal completely. Occasionally one ortwo fragments may sequestrate before healing ensues. Even if considerablesequestration takes place, the situation is preferable to an immediate completeexcision of all loose bone, resulting in nonunion with loss of substance andthe endless bone grafting that is inevitable.
Dressing of Wound: These compound fractures should be dressed withfine-mesh plain gauze laid over or into the wound. "Packing" of these woundswith vaselined gauze prevents drainage of blood and exudate which is inevitableand invites infection. These wounds which are adequately treated surgically,properly dressed and incased in circular plaster of paris splints and arrive withdressings undisturbed at the Communication Zone Hospitals, are ideal fordelayed primary closure. There is a saying that many a patient has beenbandaged to death. It is a firm conviction among those of us who observedthese wounds that frequent dressing means inevitable contamination of the
$
193

COLONEL MATHER CLEVELAND Annals of Surgery
wound and that the contaminated or infected wounds were perhaps morefrequently infected by subsequent dressings than by the original woundingagent. Those surgeons who employed a meticulous instrument technic andwore a mask had a far higher percentage of successful closures than did thosewho were careless in their treatment of the wounds. Eternal vigilance andcareful attention to seemingly small details paid handsome dividends inwound healing.
Chemotherapy: Those wounded with compound fractures and amputa-tions invariably received penicillin and/or sulfadiazine from the time ofprimary surgery. Local use of these agents was quickly abandoned exceptto instill penicillin into a closed joint cavity or into the pleura. It has beenquite definitely proved that in most instances penicillin is preferable and thatit a.ts best alone.
Splinting of Compound Fractures for Transportation: Circular plasterof paris splints were prescribed, of varying types for each of the longbones involved.
I. Compound fracture of tibia and fibula-a splint extending from toesto groin.
2. Compound fracture of femur--a plaster of paris spica bandage extend-ing from the toes of the wounded leg and from the knee of the sound leg,reenforced with a posterior strut, leg-spread no more than the width ofthe litter.
3. Compound fracture of forearm-a circular plaster splint extendingfrom behind the metacarpal heads to the axilla with the wrist in slight dorsi-flexion and elbow at right angle.
4. Compound fracture of humerus-a plaster of paris shoulder spica orplaster of paris Velpeau splint. In no case can the arm be abducted widelybecause of the limited space in ambulance, plane or hospital train.
All of these circular splints must be split to the skin and slightly spreadto allow for swelling in transit. Failure to observe this rule made the re-sponsible officer subject to disciplinary action. There were reported lossesof extremities due to unsplit plaster splints from other Theaters prior toD-Day, so this Theater was able to profit from the experience of others andinsist on this rule.
The Army hospitals were not held responsible in any sense for reduction ofthese compound fractures. That was a function reserved for the Communi-cation Zone hospitals.
FIXED HOSPITALS IN THE ZONE OF COMMUNICATIONS
Delayed Primtary Closure of Wounds: Here begins the definitive surgicaltreatment of the casualties with wounds involving the bones and joints.Delayed primary closure of these wounds in increasing numbers, as time wenton, was the outstanding improvement in the care of these casualties. The ideaof delayed primary closure of wounds is not new. It was practiced with suc-cess to a limited extent during World War I, but it was pretty well forgotten
194

Volume 124Number 2 ORTHOPEDIC SURGERY IN WORLD WAR II
unfortunately, as most of the lessons of military surgery are apt to be. Theygather dust in a number of imiassive volumes, called in our particular case theSurgeon-General's history. The new crop of military surgeons usually haveto learn all over again the hard way. At the outset of this war, our surgeonswere dominated by the closed-plaster technic of treatment of compound frac-tures. This invites infection of bone and soft tissue and healing ensues slowlyby second intention, with massive granulations which develop into scar tissue.Most of the earlier casualties with wounds involving bones and joints werereturned to the Zone of Interior with their wounds suppurating under cir-cular plaster splints. So firmly ingrained was the idea of closed-plaster tech-nic, that it was not a little difficult to persuade the medical officers at first toattempt closure of these compound fractures. Within a month or six weeksafter the invasion started, delayed primary closure was fairly completelyaccepted, and with experience it became increasingly successful.
The optimum time for delayed primary closure by suture or split-thicknessskin graft is three to five days after wounding, and any time up to ten days isconsidered early. At this period the wound edges are mobile and the skincan readily be drawn together. After ten days there is some granulationtissue and new epithelium to be excised with some undercutting of the skinedges in order to secure approximation. A careful secondary debridementor a few days of wet dressings may be required prior to the later attemptedclosure. This closure by suture is accomplished by widely-spaced, deeply-placed nonabsorbable sutures without tension. Hemostasis must be secured,'and at times a small drain is left in the wound for 24 to 48 hours. Noattempt is made to secure a cosmetic result.
If the delayed primary closure is successful, the advantages which accrueare manifold-underlying exposed bone is conserved and healing of bone andsoft-tissue is accelerated. Repair of divided peripheral nerves, open reductionof fractures, bone grafts where indicated, may all be performed at an earlyperiod. Convalescence is shortened. In an effort to determine the success ofthis form of treatment, 5,042 compound fractures, excluding bones of theface and skull and spine with spinal cord injury, were studied at the i5thHospital Center between D-Day and November I5, I944, a 4.5-month period.The bones of the lower extremity were involved in 2,614 instances and thoseof the upper extremity in I,895. The long bones most frequently fracturedby various missiles were the tibia (757), humerus (702), and femur (684),in that order and number.
Delayed primary closure was attempted in 2,393 patients, by suture in2,o87, by skin graft in 236, and by combination of suture and skin graft in 70.Skin grafting was by split-thickness free grafts and also by pedicle graftswhere loss of bone and soft-tissue was considerable.
The results obtained in these attempted closures were as follows:I. Complete success-healing by primary intention occurred in I,592
cases, or 66.53 per cent of the total.2. Partial failitre occurred in 640 cases, or 26.74 per cent of the total.
195

COLONEL MATHER CLEVELAND Annals of SurgeryAugust. 1946
Those rated partial failures showed a smiall sinus, a stitch abscess, or partialloss of a skin graft. All but a very few of these wounds healed by a secondsuture or skin graft or spontaneously and were classed as healed when thepatient left the hospital. This means that a total of 93 per cent of the patientsupon whom closures were attempted left the hospitals with their wounds healed.
3. Complete failure occurred in i6i cases, or 6.73 per cent of the total.This means an entire breaking open of the wound or the development of asoft-tissue infection or osteomyelitis, which necessitates wide surgical opening.
Further follow-up on these attempted delayed primary closures of woundsperformed in the European Theater after return to the Zone of Interior wasfurnished by the Office of The Surgeon-General. A small series of 34 com-pound fractures of the femur, tibia, fibula and humerus, treated in the Euro-pean Theater by delayed primary closure of their wounds were reported bythe Ninth Service Command as follows: The delayed primary closure wassuccessful in 73.5 per cent of the cases and the incidence of osteomyelitis was14 per cent. A similar-sized series of compound fractures upon whom noattempt at closure had been made was reported also by the Ninth ServiceCommand, showing an incidence of osteomyelitis in 54 per cent ofthese wounds.
There can be no question that delayed primary closure of these compoundfractures can be successfully accomplished in almost three out of four casesattempted and that, if it is successful, the incidence of osteomyelitis is sharplyreduced. This is in addition to the other beneficial results enumerated above.
TREATMENT OF LONG BONE FRACTUIRESLong bone fractures were treated by skeletal traction, usually with Kirsch-
ner wire. An Army half-ring splint, with Pearson attachment, was utilizedfor balanced suspension. These long bone fractures were for the most partevacuated to fixed hospitals in the United Kingdom Base where the evacua-tion policy allowed a holding-period up to I20 days, whereas that period onthe continent was 6o days maximum. It was our plan to hold these compoundfractures in traction, following closure of the wounds until sufficient "freezing"or union had taken place, so that they would not displace when placed incircular plaster of paris splints for evacuation to the Zone of Interior. Thisholding-period varied from five to I2 weeks and even longer if necessary,depending upon the bone involved. Our principal error was in fractures ofthe shaft of the femur and trochanteric fractures which were not held in someinstances sufficiently long prior to evacuation to the Zone of Interior, anddisplaced within the circular plaster splints with resulting malunion. For-tunately, this was quickly called to our attention and every effort was madeto remedy this particular situation. Malunion in these badly damaged longbones all too often cannot be immediately avoided.
HEALING OF COMPOUND FRACTURESA report from I9 named General Hospitals on compound fractures due
to wounds treated in the European Theater was received from the Surgeon-General at the request of the Chief Surgeon of the Theater. This report
196

Volume 124Number 2 ORTHOPEDIC SURGERY IN WORLD WAR II
was formulated during the month of December, I944, so that the oldest casesreported were six months or less after being wounded. From the standpointof union of the fractures, these 3,190 patients showed the following status oflhealing of their fractures:
2,I89, or 68.6 per cent, were satisfactorily united.417, or I3.3 per cent, were united in malposition.
2,606, or 8I.9 per cent, -total united.584, or i8 per cent, were ununited.
It was too early to consider all of the ununited fractures as nonunions.There was, however, a sizable group that due to the loss of bone by theoriginal wounding agent, or to the overzealous removal of loose bone frag-ments by the inexperienced surgeon resulted in nonunion, requiring bonegrafts to bridge the gap.
AMPUTATIONS
The only amputation allowed in the Theater was the circular type whichis considered an emergency measure. This amputation was done at the lowestpossible level where a viable stump could be expected. It is really an invertedcone. The skin is divided in a circular manner and allowed to retract, themuscles are then divided at the level of the retracted skin, and they, in turn,retract still further and the bone or bones are divided transversely at the levelof the retracted muscle. Traction is applied to the skin immediately and con-tintued until the patienlt arrives at the Amputation Center in the Zone ofInterior. If the amputation is performed for clostridial or other infection,skin traction is not applied for 24 to 48 hours, at which time it should bepossible to determine whether the stump is infected or clean.
It was urgently insisted that continuous skin traction be maintained. Thisis best accomplished by weight and pulley over the foot of the bed while thepatient is in the fixed hospital and by means of a plaster of paris pylon witha wire ladder splint incorporated while the patient is in transit. Stockinettefixed to the skin by Ace, or other adherent substance, and elastic cord or tubingwere almost universally utilized. The amputee was usually advised that hisamputation was necessary after consultation and that the procedure done inthe Theater was an emergency measure which would require revision at theAmputation Center.
The amputations performed in the 3rd United States Army from August1, I944, to February I, 1945, a six-months' period, were analyzed by ColonelCharles Odom, Surgical Consultant of that Army. There were I,365 amputa-tions performed upon 1,290 patients. Since I,012 of these amputees wereUnited States Army personnel among 64,389 battle casualties for that periodof time, the incidence of amputation in this army was a little over I.5 per centof the wounded. Seventy-six per cent of the amputations occurred in thekwer extremity, which is probably an indication of the efficacy of the landmines encountered. The causes of amputation were as follows: Traumaticamputation 66 per cent. Blood vessel injury 20.2 per cent. Clostridial infec-
197

COLONEL MATHER CLEVELAND Annalsof Surgery
tion 13.8 per cent. In the Army area the mortality among these 1,290 amllputeeswas about nine per cent.
There are in World War II about 14,000 surviving mliajor aImlputeesamong an estimated 8,ooo,ooo, or more, soldiers mobilized. In contrast tothis, during the American Civil War, the Union and Confederate armiesmobilized perhaps a total of three million men. There were 27,000 amputeesin the Union Army and almost 25,0o0 among the Confederates, and themortality in patients requiring this procedure at that time was approxi-mately 25 per cent.
With the decrease in amputation as a means of treating the badly damagedextremity in battle casualties, there has been a corresponding increase in thecompound fractures salvaged for treatment as outlined above.
THE WOUNDED HAND
The serious nature of these wounds was appreciated early and effortswere made to expedite their evacuation to Hand Centers which were set upon the continent and in the United Kingdom. These damaged hands wereoften immobilized too long and too extensively, with resulting swelling andfibrosis. There was at times undue delay in transferring them to the HandCenters where plastic and orthopedic surgeons were available to secure healingof the wound and early return of function. In an effort to avoid this pro-longed rigid immobilization, the wounded hand was considered chiefly fromthe standpoint of its soft-parts. A pressure dressing, with the hand andfingers in functional position, was recommended, with elevation of the partand early closure of wounds by suture or skin graft-split-thickness or pedicleas required.
In March of 1945 we decided to try immediate loose primary closure ofthese wounded hands in all possible cases in the Army hospitals (EvacuationHospitals for the most part). A careful and complete scrubbing of thewounded hand and a meticulous debridement were insisted upon prior to theimmediate primary closure. The hand that had been sutured had to be heldnonevacuable for five days. These regulations were put in effect in mid-April, 1945, and within a few weeks hostilities ceased. As an indication ofwhat might be expected from this form of treatment, two surgeons in differentEvacuation Hospitals reported immediate primiiary suture on a total of 8ohand wounds, with only five wound infections occurring. This was a vastimprovement over delayed primary suture, and with early healing, rehabilita-tion of the wounded part could be commenced at an earlier period from thetime of wounding.
Every effort was made to salvage one or two useful fingers in the severelydamaged hands. No tendon replacement or bone grafts were undertaken inthe Theater. Patients requiring this type of surgery were returned to theZone of Interior. The prompt amputation of one or even two irretrievablydamaged fingers with shattered bones and joints and severed flexor tendonswill often afford the early salvage of an excellent three- or four-finger hand.With only one finger lost a soldier can be fairly promptly returned to full
198

Volume 124 ORTHOPEDIC SURGERY IN WORLD WAR IINumber 2
duty. Early in the campaign a good deal of useless effort was expended inattempts to save one badly damaged finger-to the detriment of the hand.
Wounds Involving Joints: These wounds are always troublesome andpotentially dangerous. Their proper treatment is based on sound basic surgicalprinciples. Lt. Colonels Thompson and Cassebaum and Captain Stewartpresented two important reports on the treatment of these joint wounds. Thejoint wound should be carefully explored through adequate incisions, alldevitalized or damaged soft tissue and bone excised, all foreign bodies foundin the joint cavity or overlying soft tissues should be removed and the jointgently lavaged. The capsule should be closed immediately by suture or fascialgraft if necessary. The overlying soft-tissue wound is left open to be closedlater by delayed primary closure. Twenty thousand units of penicillin areinstilled into the closed joint cavity. Immobilization of the joint is securedby adequate and prescribed plaster of paris circular splint with a windowfor inspection of the joint should need arise. The patient with such a woundmust be held nonevacuable for seven to ten days, during which time he re-ceives parenteral penicillin, 20,000 units every three hours. If necessary, anadditional 20,000 units of penicillin is injected into the joint cavity at 24-hourintervals. If healing proceeds uneventfully, the superficial wound is closedthree to five days after primary surgery was done. By this treatment a highpercentage of joint wounds were salvaged with useful motion.
In the irretrievably damaged joint or where infection is developing, anearly resection of the joint will promote healing of the wound. In the jointsof the lower extremity and wrist, fusion or arthrodesis is the goal to be sought,with the joint in the position to secure optimum function in the remainingmobile joints. In the elbow and shoulder joints after resection and healingof the wounds, early mobilization will give a surprisingly good range of motionwith useful though by no means complete stability.
COMBINED NEUROSURGICAL AND FRACTURE PROBLEMS
Approximately 75 per cent of the compound fractures complicated bynerve lesions occur in the upper extremity with the compound fracture ofthe humerus and injury to the radial nerve comprising the vast majority ofthese. The compound fracture of the femur with division of the sciatic nerveis fortunately not very frequently encountered, forming perhaps ten per centof the total of these combined injuries. There is apparent4y no means ofascertaining in the first few weeks after wounding whether a nerve has beendivided or merely badly contused. A high percentage of the nerves exploredrequired only a neurolysis. The Senior Consultant in Neurosurgery, ColonelGlen Spurling, and the Senior Consultant in Orthopedic Surgery were inaccord that the divided or potentially divided major peripheral nerve shouldbe given precedence over the compound fracture.
The plan of treatment of these combined nerve and fracture problems wasas follows: They were transferred immediately to a Neurosurgical Center.The wound was closed by delayed primary suture or skin graft. The fracturewas meanwhile placed in balanced suspension. No effort was made to secure
199

COLONEL MATHER CLEVELAND Aiiiials of Sutgery
anatomic length because this might defeat the attempt to get the nerve endstogether. Three weeks after wound-healing had ensued, the nerve was exploredand sutured if found divided. If it were necessary in order to get the nerveends together, the bone was shortened up to 2.5 cm. This shortening wasnot frequently required. In the humerus it was of no moment, and in thefew cases of the femur which required shortening, little or no disability dueto the procedure was anticipated. These openly reduced fractures weretreated by internal fixation. Needless to say, penicillin was quite extensivelyemployed in these combined surgical procedures.
OBSERVATlONS ON THE COMPARISON OF MEDICAL CARE OF THE WOUNDEDIN WORLD WAR I AND WORLD WAR II
Having served as a medical officer in both wars, it may be permissibleto make a few comparisons. The 25 years which elapsed between the warshas seen progress in the training of the young surgeons and this was reflectedlin the fact that more and better trained surgeons were available to do bettersurgery. There never were enough to completely fill all the existing vacancies.but the situation was vastly improved over World War I. In the EuropeanTheater the general level of care of bone and joint casualties was vastly im-proved. Superior care was unquestionably rendered by many of the affiliatedhospitals in World War I, but in other less favored units it left much tobe desired.
There was a more complete and general understanding of resuscitation inWorld War II. No blood or plasma was available or used in most of the Armyhospitals in World War I. The great stocks of plasma and whole bloodwhich were made available and were used so extensively saved many of thewounded who would otherwise have succumbed.
The evacuation of the wounded in World War II was more rapidlyaccomplished.
The overseas hospitals were very much better equipped for their workin this war.
The low incidence of infection was probably due to better surgery in theforward areas. In this matter of lower infection, the role of sulfonamides andpenicillin is not absolutely clear. These new drugs probably exerted a bene-ficial effect, but controlled experimental data is not available.
The European Theater was singularly fortunate in having a Chief Sur-geon whose sole aim was to improve the standard of care of the sick andwounded American soldier. Nothing deterred him from this aim. The pro-fessional service division had a group of consultants who worked harmoniouslyas a team under inspiring leadership of the Chief Surgeon and the ChiefConsultants in Surgery and Medicine.
REFERENCECleveland, Lt. Col. Mather; Grove, Maj. John A., M.C., A.U.S., Delayed Primary
Closure of Wounds with Compound Fracttures. J. Bone and Joint Surg., Vol. xxvii,No. 3, pp. 452-456, July, 1945.
200