Embed Size (px)
Citation preview
OMPT and Cervicogenic Headache
Orthopedic Manual Therapy Techniques in the Diagnosis and Treatment of Cervicogenic
Headaches: A Case Report
A Case Report
Presented to
The Faculty of the Department of Physical Therapy
Florida Gulf Coast University
In Partial Fulfillment
of the Requirement for the Degree of
Doctorate of Physical Therapy
By
Hayley B. Rodgers
May 2014
OMPT and Cervicogenic Headache
APPROVAL SHEET
This case report is submitted in partial fulfillment of
the requirements for the degree of
Doctorate of Physical Therapy
_____________________________________
Hayley B. Rodgers
Approved: May 2014
_____________________________________
Arie J. van Duijn, EdD, PT, OCS
Committee Chair/Advisor
_____________________________________
Jacqueline van Duijn, DPT, OCS
Committee Member
The final copy of this case report has been examined by the signatories, and we find that both
the content and the form meet acceptable presentation standards of scholarly work in the
above mentioned discipline.
OMPT and Cervicogenic Headache 1
Table of Contents
Abstract 1 Introduction 2 Purpose 3 Literature Review 3
Anatomy of the Cervical Spine 3 Biomechanics of the Cervical Spine 5 History and Background of Cervicogenic Headaches (CGH) 6 Pathophysiology of CGH 7 The Relationship between TMD and CGH 8 Diagnosing CGH 10 Manual Therapy Techniques in Treating CGH 14
Case Description 18 Past Medical History 18 Subjective History 19
Neck Disability Index 20 Pain Assessment 21 Behavioral Aspects 22
Objective Findings 22 Posture 22 Range of Motion 22 Manual Muscle Testing 23 Manual Examination and Palpation 23 Neurological Testing 24 Impression 24
Prognosis 25 Patient Goals 25 Intervention 26 Outcomes 33 Discussion 35
Conclusion 42 References 44
OMPT and Cervicogenic Headache 2
Abstract
The inclusion of orthopedic manual therapy in the diagnosis and treatment of
cervicogenic headaches (CGH) has resurfaced as a topic of interest within the field of
physical therapy. The use of manual therapy approaches in the evaluation and treatment
for CGH continues to evolve and grow as higher level pieces of research are published. The
underlying culprit of CGH is a mechanical dysfunction of the cervical spine (Becker, 2010).
Recent studies have provided results that support the use of manual therapy to the cervical
spine, as well as to the temporomandibular joint, thoracic spine, and first rib, in order to
relieve pain, increase range of motion (ROM) and improve overall quality of for patients
who suffer from this chronic disorder (Von Piekartz & Ludtke, 2011; Masaracchio, Cleland,
Hellman & Hagins, 2013). Manual examination skills have also shown to have high
sensitivity and specificity in diagnosing CGH (Jull, Amiri, Bullock-Saxton, Darnell, & Lander,
2007). For this reason, manual approaches for both diagnosing and treating the mechanical
dysfunction underlying CGH are investigated.
The case study involves a 35-year old woman who presented to orthopedic
outpatient physical therapy with signs and symptoms suggestive of cervicogenic headache.
The purpose of the case report is to reflect the reorganization and synthesis of extant
information of orthopedic manual physical therapy interventions for patients with
cervicogenic headaches that took place with completion of the investigator’s independent
study. In addition, the presentation of this case report provides the clinical reasoning
behind the orthopedic manual therapy examination and treatment of a patient with
cervicogenic headaches and discusses the outcomes of her plan of care.
OMPT and Cervicogenic Headache 3
Introduction
The inclusion of orthopedic manual therapy in the diagnosis and treatment of
cervicogenic headaches (CGH) has resurfaced as a topic of interest within the field of
physical therapy. The use of manual therapy approaches in the evaluation and treatment
for CGH continues to evolve and grow as higher level of evidence is published. The
underlying culprit of CGH is a mechanical dysfunction of the cervical spine (Becker, 2010).
Recent studies have provided results that support the use of manual therapy to the cervical
spine, as well as to the temporomandibular joint, thoracic spine, and first rib, in order to
relieve pain, increase range of motion (ROM) and improve overall quality of for patients
who suffer from this chronic disorder (Von Piekartz & Ludtke, 2011; Masaracchio, Cleland,
Hellman & Hagins, 2013). Manual examination skills have also shown to have high
sensitivity and specificity in diagnosing CGH (Jull, Amiri, Bullock-Saxton, Darnell, & Lander,
2007).
As a physical therapy student with a strong interest in manual therapy, this
investigator has found it both challenging and advantageous to explore the use of manual
therapy for treating CGH. With the recent increase in number of high quality research
demonstrating the advantages of utilizing manual therapy in the treatment of cervicogenic
headaches, beneficial insight will be gained into this role. This advancement of orthopedic
manual skills and increase in knowledge of the cervical spine beyond that of an entry-level
physical therapist will be particularly advantageous for the investigator in treating patients
with this condition.
OMPT and Cervicogenic Headache 4
Purpose
The following case report involves a 35-year old woman who presented to
orthopedic outpatient physical therapy with signs and symptoms suggestive of
cervicogenic headache. The purpose of this case report is to reflect the reorganization and
synthesis of extant information of orthopedic manual physical therapy interventions for
patients with cervicogenic headaches that took place with completion of the investigator’s
independent study. In addition, the presentation of this case report provides the clinical
reasoning behind the orthopedic manual therapy examination and treatment of a patient
with cervicogenic headaches and discusses the outcomes of her plan of care.
Literature Review
Anatomy of the Cervical Spine
The cervical spine is composed of seven vertebrae and is divided into upper and
lower regions. The upper cervical spine includes the occipital condyles and the first two
cervical vertebrae, and the lower cervical spine includes C3-C7. The two atlanto-occipital
joints consist of two concave superior facet joint of C1 articulating with the two convex
occipital condyles of the skull. The C1 vertebra is unique in that it is shaped like a ring and
lacks a body and spinous process. The three joints that make up the atlantoaxial joints
include the median atlantoaxial joint between the dens and the atlas (supported by the
transverse ligament) and the two lateral facet joints (Levangie & Norkin, 2011). The lateral
facet joints are oriented approximately 45 degrees from the frontal and horizontal planes,
but this may vary from person to person (Levangie & Norkin).
The joints of the cervical spine are weight bearing structures and can be easily
injured from the weight of the head along with the result of potential high velocity injuries
OMPT and Cervicogenic Headache 5
which occur today and for everyday activities which the neck was never designed for by
evolutionary forces (Becker, 2010). In addition, they are designed for mobility rather than
stability, thereby increasing its chance of injury and trauma (Becker, 2010). Many
potentially painful structures exist in the cervical spine that has a rich nociceptive
innervation. These structures include the zygopophyseal joints, the intervertebral discs, the
ligaments and muscles, and the skin. Of these, the zygopophyseal joints appear to be the
most important pain generators (Becker).
There are four ligaments that are continuous with the longitudinal tract system and
four ligaments that are specific to the cervical spine which provide support to the neck
(Levangie & Norkin, 2011). The posterior atlanto-occipital and antlantoaxial membranes
run continuous with the ligamentum flavum, which connect the each lamina to the next,
however in the cervical spine this structure is less elastic to allow for more range of
motion. The anterior antlanto-occipital and atlantoaxial membranes are continuous with
the anterior longitudinal ligament. The tectorial membrane is a strong and wide ligament
continuous with the posterior longitudinal ligament. The ligamentum nuchae is a thick,
sheetlike structure that runs continuous with the supraspinous ligament. The four
remaining ligaments are unique to the cervical spine and include: the transverse atlantal
ligament, atlantal cruciform ligament, alar ligaments, and apical ligament (Levangie &
Norkin).
The intervertebral discs in the cervical spine are different from the discs of the rest of
the spine. For one, the annulus is a discontinuous ring surrounding a fibrocartilaginous
core (Levangie & Norkin, 2011). Also, the annulus is not arranged in alternating lamellae, is
thick anteriorly, only thin posteriorly, and may be absent laterally.Fissures and clefting of
OMPT and Cervicogenic Headache 6
the disc by occurs typically by 9 years of age at which point these fissures become the
uncovertebral joints (Levangie & Norkin, 2011).
Biomechanics of the Cervical Spine
Levangie and Norkin (2011) outlines the function of the cervical spine as
demonstrating the most flexibility of any of the regions of the vertebral column. It is also
reported that the neck may move on average 600 times for every hour, whether awake or
sleeping. Regarding the cervical spine, most of the flexion-extension comes from the
atlanto-occipital joint and reportedly ranges from 10 degrees to 30 degrees (Levangie &
Norkin). By utilizing the roll and glide rule, one can determine that during flexion of the
antlanto-occipital joint the occipital condyles roll forward and slide backward, and the
reverse is true for extension. Approxiamtely 55-58% of the total rotation of the cervical
spine comes from the antlantoaxial joint, with the alar ligaments limiting rotation to some
degree (Levangie & Norkin)
Lateral flexion and rotation are coupled motions throughout the entire vertebral
column. For the upper cervical segments, lateral flexion is coupled with contralateral
rotation and rotation is coupled with contralateral side flexion (Levangie & Norkin, 2011).
The muscles of the sub-occipital region are responsible for smaller motions such as
nodding and attach from the transverse or posterior prominences of C1/C2 to the occiput
or C1 (Levangie & Norkin).
Discs are absent at the atlantooccipital or atlantoaxial joints, therefore required the
compressive load from the weight of the head to be transferred through the articular facets
(Levangie & Norkin, 2011). Compressive loads are comparatively lower during standing
and sitting postures versus during end range flexion and extension (Levangie & Norkin).
OMPT and Cervicogenic Headache 7
This may explain why muscle imbalances of the anterior and posterior neck muscles may
promote an increase in compressive loads by forcing the cervical spine into poor posture
(forward head and hyperextension), particularly at the upper cervical segments.
History and Background of CGH
From a global epidemiological perspective, it is estimated those with an active
headache disorder is 46% of the adult population (Vavrek, Haas, & Peterson, 2010).
Headache is the most common pain condition causing loss of productive time in the US
workforce, with an average loss of 3.5 h/wk (Vavrek, Haas, & Peterson). Studies estimate
that only 14-18% of chronic headaches occur from musculoskeletal dysfunction in the
cervical spine (Zito, Jull, & Story, 2003; Vavrek, Haas, & Peterson, 2010). Complementary
and alternative medicine practitioner visitation within the last 12 months of receiving
formal physical therapy treatment was 37.5% among those who reported neck problems
(Vavrek, Haas, & Peterson).
In order to genuinely appreciate the budding evolution of the treatment of
cervicogenic headaches, it is important to understand its history. The first medical
description of a headache linked to a dysfunction of the neck was published by
Schutzenberger, in 1853 (Antonaci et al., 2005). In a 1913 report by Holmes described
headaches could originate from the neck and may be associated with the existence of
painful nodules in the posterior muscles of the neck (Antonaci et al.). This description later
provided the basis for the subsequent definition of rheumatic headache (Antonaci et al.). In
1926, French Neurologist Jean Alexandre Barre described a headache with greater
intensity in the occipital region, associated with dizziness and with hearing and visual
disturbances, and called this picture “posterior cervical sympathetic syndrome”,
OMPT and Cervicogenic Headache 8
(Fernandez de-las-Penas et al., 2006). Shortly after Dr. Barre, important research studies by
Ray and Wolff demonstrated the stimulation of the sensory nerve endings above and/or
below the upper surface of the tentorium cerebelli could reproduce pain felt centrally or
frontally (Fernandez de-las-Penas et al.). As a result of these studies, the role of the afferent
nerves of the upper cervical region was investigated (Fernandez de-las-Penas et al.).
Prior to the early 1980’s, headache originating from the neck was nonexistent in the
International Headache Classification (Fernandez de-las-Penas et al., 2006). The term
“cervicogenic headache” was first introduced by Sjaastad in an article published in 1983
and was greeted with skepticism within the medical world (Fernandez de-las-Penas et al.).
Cervicogenic headache still remains a controversial topic nearly thirty years later for a
number of reasons. In a recent 2010 article, Becker explains that cervicogenic headaches
are relatively uncommon compared to other types of headaches such as migraine or
tension-type, have a complex clinical picture, and may require diagnostic testing that is
unavailable at many clinics either due to resources or specialization. All of these reasons
have created historical controversy surrounding the diagnosis of cervicogenic headaches.
With the advent of new research and developments in patient management of cervicogenic
headaches, more information exists to assist practitioners in making clinical decisions.
Pathophysiology of Cervicogenic Headaches
CGH is a sub-group of the classification of secondary headache arising from cervical
spine musculoskeletal dysfunction (Hall, Briffa, Hopper & Robinson, 2010). Becker (2010)
explains that the anatomical convergence of pain fibers from the trigeminal nerve including
the ophthalmic division of this nerve and from the upper cervical nerves is the basis for the
referral of pain from the upper cervical region to the head, including frontal head regions.
OMPT and Cervicogenic Headache 9
Likewise, stimulation of dural mater also leads to sensitization of the second order sensory
neurons so that they are now more easily activated by neck muscle and greater occipital
nerve stimulation (Becker, 2010). These anatomical and physiological findings logically
demonstrate the possibility for nociceptive afferents from the neck to cause headache, and
also for nociceptive inputs from the dura to potentiate neck pain (Becker). This information
was confirmed in another study by Hall et al. (2010).
Temporomandibular Dysfunction and Cervicogenic Headache
One topic commonly overlooked in the research literature is the close relationship
of temporomandibular dysfunction (TMD) and CGH. Temporomandibular dysfunction
(TMD) is associated with increased headache frequency via convergence of afferent input
at the trigeminal nuclei from trigeminal afferents and afferents from the upper cervical
spine (Fernandez de las Penas, 2006). It is important to consider the impact of TMD on
increasing the severity of CGH in order to provide more comprehensive treatment to the
patient with such comorbidities. Temporomandibular disorders (TMD) are rarely used in
the inclusion and exclusion criteria of randomized, controlled studies examining outcomes
from orthopedic manual therapy for the management of cervicogenic headaches (Von
Piekartz & Ludtke, 2011) even though the prevalence of TMD ranges from 8% to 15% in
women and from 3% to 10% in men and headache patients, the prevalence of TMD is
estimated to be much higher (51.6%) (Von Piekartz & Ludtke, 2011).
Some authors suggest that for patients diagnosed with CGH, the cervical spine is
often overvalued as the source of the symptoms and other contributing favors, such as
TMD, do not receive sufficient attention (Von Piekartz & Ludtke, 2011). The study by von
Piekartz & Ludtke identified the prevalence of TMD in a sample of patients diagnosed with
OMPT and Cervicogenic Headache 10
CGH, determined the tests that are clinically relevant to detect TMD in CGH patients, and
evaluated the effect of additional orofacial physical therapy after three and six months in
comparison with control group. The inclusion criteria for patients to receive orofacial care
for this experiment included a minimum of one of the four signs of TMD: joint sounds,
deviation during mouth opening, extraoral muscle pain at a minimum of two tender points
in the masseter or temporalis muscles and pain during passing mouth opening. The
researchers gathered pre and post measurements using the colored analog scale (CAS),
Neck Disability Index (NDI), Anamnestic Questionnaire CMD (Conti), Noise Registration at
the Mandibular Joint, Graded Chronic Pain Status (GCPS-NL), mandibular deviation, mouth
opening measurement, and pain threshold measurement of the masticatory muscles. The
manual therapy treatment techniques consisted of accessory movements of the
temporomandibular region and/or masticatory muscle techniques, such as tender-trigger
point treatment and muscle stretching. Results from this study provided data that CGH
patients showed a higher prevalence of TMD than the healthy population. This study also
helped to propose that clustering of tests such as mouth opening (range and pain), NDI, and
VAS of headaches, contributes to an improved diagnosis of TMD in chronic CGH patients.
The beneficial treatment effect in the experimental group that remains or is improved at six
months follow-up helps to indicate that TMD may be a contributing or etiological factor in
chronic CGH patients. Unfortunately, other research studies of this quality and
comprehensive nature were absent from the literature, therefore research studies on CGH
should include inclusion and exclusion criteria for TMD for their sample populations.
OMPT and Cervicogenic Headache 11
Diagnosing Cervicogenic Headache
The International Headache Society (IHS) released the first criteria for cervicogenic
headaches in 1998, which included: pain localized in the neck and occipital region, may
project to forehead, orbital region, temples, vertex, or ears, pain precipitated or aggravated
by particular neck movements or posture, either resistance/limitation of passive beck
motion, palpatory changes in neck musculature or altered response to
stretching/contraction, or abnormal neck muscle tenderness (Vavrek, Haas, & Peterson,
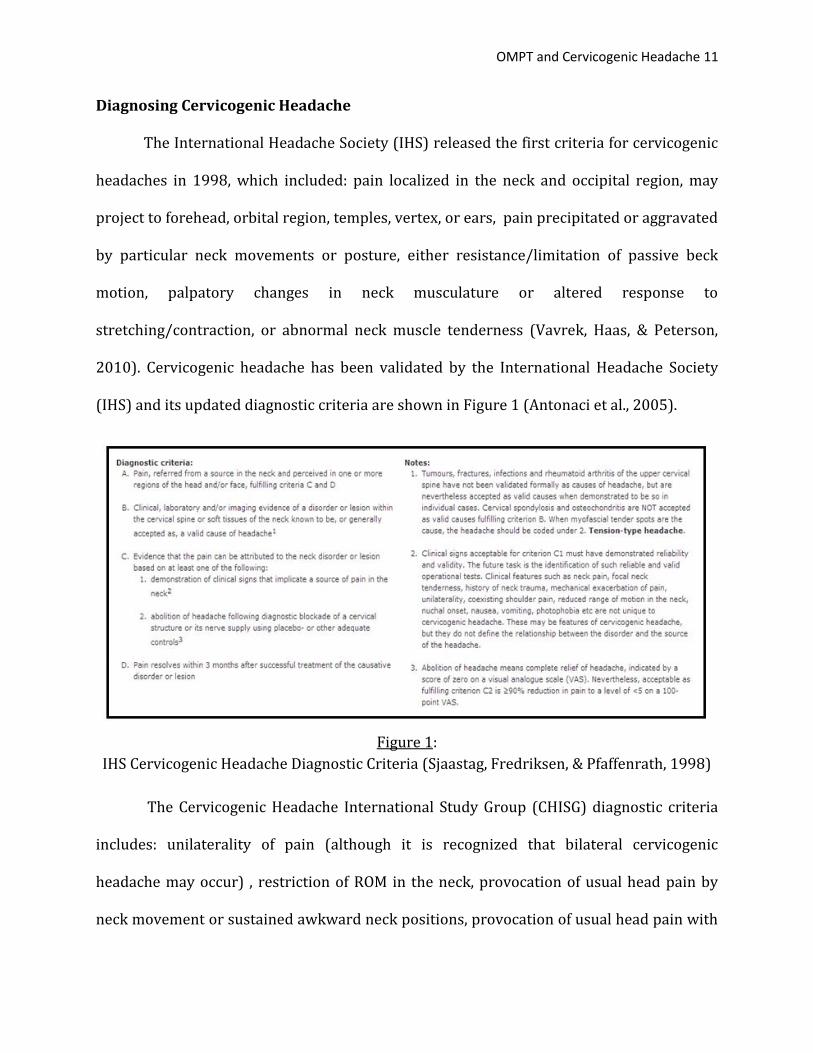
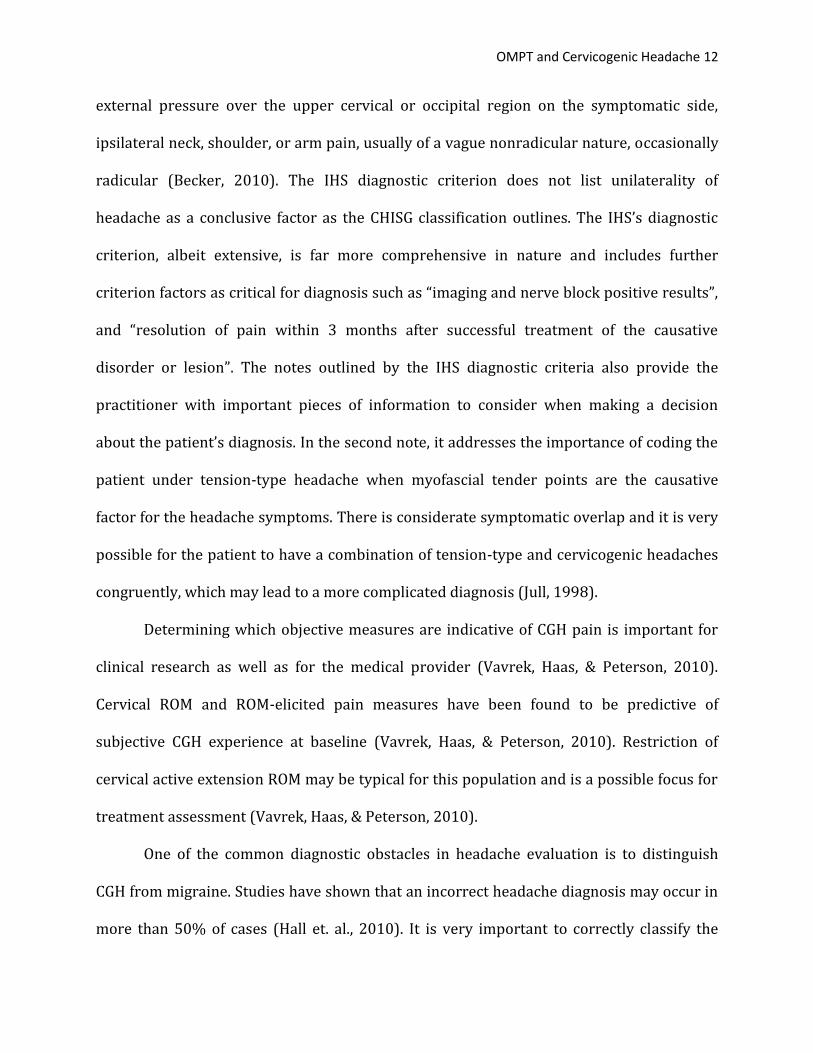
2010). Cervicogenic headache has been validated by the International Headache Society
(IHS) and its updated diagnostic criteria are shown in Figure 1 (Antonaci et al., 2005).
Figure 1:
IHS Cervicogenic Headache Diagnostic Criteria (Sjaastag, Fredriksen, & Pfaffenrath, 1998)
The Cervicogenic Headache International Study Group (CHISG) diagnostic criteria
includes: unilaterality of pain (although it is recognized that bilateral cervicogenic
headache may occur) , restriction of ROM in the neck, provocation of usual head pain by
neck movement or sustained awkward neck positions, provocation of usual head pain with
OMPT and Cervicogenic Headache 12
external pressure over the upper cervical or occipital region on the symptomatic side,
ipsilateral neck, shoulder, or arm pain, usually of a vague nonradicular nature, occasionally
radicular (Becker, 2010). The IHS diagnostic criterion does not list unilaterality of
headache as a conclusive factor as the CHISG classification outlines. The IHS’s diagnostic
criterion, albeit extensive, is far more comprehensive in nature and includes further
criterion factors as critical for diagnosis such as “imaging and nerve block positive results”,
and “resolution of pain within 3 months after successful treatment of the causative
disorder or lesion”. The notes outlined by the IHS diagnostic criteria also provide the
practitioner with important pieces of information to consider when making a decision
about the patient’s diagnosis. In the second note, it addresses the importance of coding the
patient under tension-type headache when myofascial tender points are the causative
factor for the headache symptoms. There is considerate symptomatic overlap and it is very
possible for the patient to have a combination of tension-type and cervicogenic headaches
congruently, which may lead to a more complicated diagnosis (Jull, 1998).
Determining which objective measures are indicative of CGH pain is important for
clinical research as well as for the medical provider (Vavrek, Haas, & Peterson, 2010).
Cervical ROM and ROM-elicited pain measures have been found to be predictive of
subjective CGH experience at baseline (Vavrek, Haas, & Peterson, 2010). Restriction of
cervical active extension ROM may be typical for this population and is a possible focus for
treatment assessment (Vavrek, Haas, & Peterson, 2010).
One of the common diagnostic obstacles in headache evaluation is to distinguish
CGH from migraine. Studies have shown that an incorrect headache diagnosis may occur in
more than 50% of cases (Hall et. al., 2010). It is very important to correctly classify the

OMPT and Cervicogenic Headache 13
headache disorder so that treatment can be directed appropriately (Hall et. al., 2010).
Because the pathophysiology underlying CGH is musculoskeletal dysfunction in the upper
three segments, physical examination of the upper cervical spine is particularly important.
Dysfunction may involve any of the upper three cervical segments and can be
measured by manual examination. Manual examination is a means of determining from
which spinal segment pain arises, and consists of tests of unilateral passive accessory
intervertebral motion (PAIM) and passive physiological intervertebral motion (PPIM)
(Hall, Briffa, Hopper & Robinson, 2010). Manual therapy has high sensitivity (100%) and
specificity (94%) to detect the presence or absence of cervical joint dysfunction from
migraine in neck pain and headache patients (Hall, Briffa, Hopper & Robinson). However,
these tests involve a high degree of skill on the part of the therapist, and their reliability has
been questioned (Hall, Briffa, Hopper & Robinson). C1/2 was the most dominant
symptomatic segment at approximately 63% of positive cases (Hall, Briffa, Hopper &
Robinson). Differences in anatomical morphology of the C1/2 articulation may be a
contributing factor. A study by Hall and Robinson (2004) found the C1/C2 segment to be
the most symptomatic cervical motion segment in 80% of a sample of 28 subjects with
CGH.
A recent study by Jull from 2007 has shown that the combination of three tests of
cervical spine musculoskeletal function can identify subjects with CGH, from other
headache forms, with 100% sensitivity and 94% specificity. These tests include cervical
range of motion, manual examination of the upper cervical spine, and cervical motor
control evaluated by the craniocervical flexion test (Jull et. a., 2007). The cervical flexion-
rotation test is gaining credibility as a useful aid in the classification of CGH (Smith, Hall, &
OMPT and Cervicogenic Headache 14
Robinson, 2008; Hall, Briffa, Hopper & Robinson, 2010). The FRT consists of pre-
positioning the cervical spine in maximal end range flexion followed by passive rotation of
the head to the left and the right, with the subject relaxed in supine (Hall, Briffa, Hopper &
Robinson). End of range in each direction is determined either by firm resistance or pain,
and compared between left and right. The call for substantiation of efficacy of manual
therapy emphasizes the need for accurate diagnosis to distinguish cervicogenic headache
from other causes of chronic headache so that the appropriate patients receive manual
therapy treatment (Zito, Jull, & Story, 2003). The historical research study conducted by
Zito et al. (2003) determined that the presence of upper cervical joint dysfunction most
clearly differentiated the cervicogenic headache sufferers from those with migraine with
aura and control subjects. The patient with CGH also presented with restriction in cervical
motion, a higher frequency of muscle tightness, and a poorer muscular performance and
strength with cranio-cervical flexion testing. Such musculoskeletal dysfunction was not
apparent in the group with migraine with aura who did not differ from the control group.
These musculoskeletal criteria are in accordance with, but better define those listed by the
HIS diagnostic criteria. Identification of these physical impairments in the musculoskeletal
system linked to clinical features will contribute to the justification and selection of
treatment for CGH. Further work is necessary to address issues of generalizability and
reliability of these results (Zito, Jull, & Story, 2003).
Also, manual examination should be used in conjunction with other physical tests to
improve overall accuracy in identifying CGH (Hall, Briffa, Hopper & Robinson, 2010). In the
most recent version of these diagnostic criteria, confirmatory local anesthetic blocks in the
cervical region are also considered necessary to make a firm diagnosis of cervicogenic
OMPT and Cervicogenic Headache 15
headache (Becker, 2010; Goodman & Fuller 2009). With regard to examination and
treatment for patients with cervicogenic headache, the general recommendation exists to
use less invasive assessment procedures and treatment interventions first (Becker, 2010).
By using a conservative approach for this population, invasive testing and treatments such
as suboccipital nerve blocks and surgery should only be considered when prior
conservative assessment and intervention was unsuccessful (Becker, 2010).
Manual Therapy Techniques in Treating CGH
A study by Hoving, et al., demonstrated that directly referring patients with neck
complaints to a physical therapist specializing in manual therapy is more effective and
cost-saving than guidance from a first-line medical professional (Hoving et al., 2003; Von
Piekartz & Ludtke, 2011). The most common and accepted assumption of spinal
manipulation and mobilization is that it results in an increase in either passive and/or
active range of motion (Whittingham & Nilsson, 2001). Spinal manipulation is the
application of force of varying velocity and frequency ranges on one or more vertebrae
(e.g. sustained, oscillatory, or high-velocity thrust) that may be manually applied as a
passive treatment or combined with active movements of the spine (Fernandez de-las-
Penas et al., 2006).
Numerous pieces of historical research suggest that the afferent input produced by
manipulative therapy procedures may stimulate neural inhibitory systems at various levels
in the spinal cord helping to reduce nociceptive levels perceived by the patient (Christian,
Stanton, & Sissions, 1988; Allen, Terrett, & Vernon, 1984). Spinal manipulative therapy may
also activate descending inhibitory pathways from, for example, the lateral periaqueductal
gray area of the midbrain (Wright, 1995). The lateral periaqueductal gray (PAG) area of
OMPT and Cervicogenic Headache 16
the midbrain has been shown to have an integral role in the behavioral responses to pain,
stress, and other stimuli in maintaining internal homeostasis, which (Fernandez de-las-
Penas et al., 2006). It is able to achieve this through coordination of responses of various
systems throughout the body including the nociceptive system, autonomic nervous system,
and motor system (Depaulis & Bandler, 1991).
Results from a recent systematic review support the use of combined mobilization,
manipulation, and exercise for short-term pain reduction, global perceived effect and
patient satisfaction in acute and chronic neck pain with or without cervicogenic headache
(Miller et. al, 2010). The use of manipulation and mobilization alone provides short-term
pain relief. Exercise appears to improve pain and function over the long-term. The
combination of manual therapy and exercise, however, seems to produce greater short-
term pain reduction than exercise alone and longer-term changes across multiple outcomes
in comparison to manual therapy alone (Miller et. al, 2010).
A Cochrane review has demonstrated the positive effect of specific cervicoscapular
resisted exercises, C1/C2 self-SNAG exercises, craniocervical endurance exercise and low
load endurance exercise, and upper extremity stretching and strengthening exercise , but
the optimal exercises to combine with manual therapy remain unknown (Miller et. al,
2010). Spinal manipulative therapy (SMT) is defined as controlled directional, high-
velocity, low-amplitude thrust. The primary objectives of SMT in the treatment of headache
and neck pain are the alleviation of pain, muscle spasm, and functional impairment
(Vavrek, Haas, & Peterson, 2010).
Another research study looked at the single toggle-recoil thrust (a short-level, high-
velocity technique) technique as one approach to spinal manipulative therapy
OMPT and Cervicogenic Headache 17
(Whittingham & Nilsson, 2001). The study found a consistent and statistically significant
increase in active range of motion in the cervical spine after manipulation; however,
improper sample and examiner blinding techniques may have been a major limitation of
the study (Whittingham & Nilsson, 2001). Moderate quality evidence from one recent
systematic review showed both cervical manipulation and mobilization produced similar
effects on pain, function and patient satisfaction at intermediate-term follow-up. Optimal
technique and dose still needs to be determined by future research studies (Gross, et. al.,
2010).
One mobilization technique may be superior to another, but the findings within the
research are inconclusive and preliminary in nature (Gross, et. al., 2010). A multitude of
approaches to manual therapy for the cervical spine are utilized to treat cervicogenic
headache, including myofascial release, distraction of the upper cervical segments, spinal
mobilization, spinal manipulation using thrust techniques, soft tissue mobilization, and
trigger point release. All of these topics that fall into the category of manual therapy will be
investigated throughout the course of this independent study.
A significant amount of evidence exists for the benefits of cervical manual therapy
techniques in treating cervicogenic headache. A 2001 study by Sterling, Jull, and Wright,
reported significant increases in pressure pain thresholds and a decrease in visual analog
scores when using spinal manipulation interventions compared to control placebo groups.
Spinal manipulation was also found to alter motor responses and facilitate muscle function
that was previously inhibited because of pain or impairment. These crucial findings help to
support the basis for the orthopedic manual therapy interventions utilized to reduce pain
and improve range of motion in cervical spine with the case patient discussed within this

OMPT and Cervicogenic Headache 18
paper. The case report that follows discusses orthopedic manual therapy and therapeutic
exercise interventions that were used in combination to improve pain intensity, headache
frequency, range of motion of the cervical spine, and gain in overall functional capabilities.
A randomized-controlled trial study looking at the effects of manipulative and exercise
interventions found no statistical advantage for short term outcomes when used in
combination (Jull et.al, 2002). It can be inferred from the data, however, that manipulative
therapy supplemented with therapeutic exercise progressions produce a higher optimal
effect across all outcomes over the long term. Therefore, it is clear that manual therapy is a
critical component of producing optimal outcomes for patients with cervicogenic
headaches, particularly when used with an appropriate therapeutic exercise prescription.
OMPT and Cervicogenic Headache 19
Case Description
The patient was referred to an orthopedic outpatient physical therapy clinic by her
primary care physician with the medical diagnosis of “cervicalgia”. Exactly one month
passed between the referral from her physician to the time of initial physical therapy
evaluation. The physical therapist who provided the plan of care for this patient is a Doctor
of Physical Therapy with a certification in Manual Physical Therapy through the University
of Saint Augustine for Health Sciences. He is also recognized as a Board Certified Clinical
Specialist in Orthopedics by the American Board of Physical Therapy Specialties with 14
years of experience of clinical experience. The details of his initial evaluation of the case
patient are an adaptation of the spinal evaluation outlined by University of Saint
Augustine’s founder Stanley Paris and Loubert (1999) and included the following areas.
Past Medical History
The case patient is a 35-year old female audiologist who sought physical therapy
treatment for neck pain. She was seen by the same physical therapist in July of 2012 to
treat similar problems of the neck, with left shoulder involvement. During this prior
episode of care, the neck pain was more symptomatic on the left side and the headaches
she experienced went to the left frontal cranium. Prior to the plan of care she had received
one cortisone injection in her left shoulder which brought some relief. Physical therapy
interventions consisting of a combination of manual therapy and therapeutic exercises was
a success during her past plan of care. The Shoulder Pain and Disability Index, which
examines the overall functional level of the involved shoulder (Roach, 1991), was reduced
from a 26% to a 5.4% over the course of one month. A reliability study published by Roach
et al. in 1991, found that the test-retest reliability of the SPADI total and subscale scores
OMPT and Cervicogenic Headache 20
ranged from 0.63 to 0.65 and internal consistency ranged from 0.86 to 0.95. The scores
were found to be highly negatively correlated with shoulder range of motion measures,
which suggests good criterion validity of the tool. This tool may be an important outcomes
measure when used in addition to the Neck Disabilities Index to measure progress of
patients with cervicogenic headaches and decreased upper extremity function undergoing
physical therapy treatment.
The patient also has a history of TMJ dysfunction on the left TMJ. She has
consistently worn a night guard for this condition since her teenage years. The patient
states that her “jaw frequently pops” and that she is currently on a modified soft diet. The
overall prevalence of TMD ranges from 8% to 15% in women and from 3% to 10% in men
(Von Piekartz & Ludtke, 2011). In headache patients, the prevalence of TMD is estimated
to be much higher (51.6%).
The patient also reports using a gluten-free diet in addition to her modified soft diet.
She has reportedly been using a gluten-free diet since early 2010. She has personally noted
a decrease in pain intensity and a reduction of gastrointestinal irritation as a result of this
diet. The patient had endometriosis (stage 4) which was medically treated with surgery
and ablation therapy after having her first child, who is now 22-months old. She is
currently seeking medical treatment for in-vitro impregnation to have her second child.
Subjective History
The patient stated during the initial evaluation that her current status included
“constant neck pain, decreased neck motion especially when driving, headaches going from
the back of the neck to the right forehead (average of 5 headaches per week), increased
stiffness, and painful jaw function”. Pain was self-reported to be an exacerbation of a
OMPT and Cervicogenic Headache 21
chronic condition she has experienced for over 15 years. Her prior level of function was
self-reported as independent with all ADL’s. Decreases in her current level of function
included having difficulty driving longer distances, using the computer for work, and caring
for her 20-month old son (23 pounds). The patient is an audiologist for the local County
Education Department, which requires her to travel in her car for several hours throughout
the workday.
The patient’s symptoms of neck pain had been persistent and worsening during the
year leading up to her first physical therapy appointment for this specific plan of care.
During that time she had been to see a chiropractor several times without success. She also
has regular massages every two weeks over the past two years with some relief.
The patient reports having frequent headaches (1-2 occurrences per week) that
radiate into the right frontal region of the head. The patient denies having any neurological
symptoms such as numbness or tingling that radiates into the upper extremities, and
denies pain that awakes her at night.
Neck disability index. Upon the initial evaluation, the patient scored a 40% (within
moderate disability range) on the Neck Disability Index (NDI, Appendix 1). The NDI was
developed as a modification to the Oswestry Low Back Pain Disability Index and is a
patient-completed, condition-specific functional status questionnaire (Macdermid et al.,
2009). There are 10 items total, including questions on pain intensity, personal care, lifting,
reading, headaches, concentration, work, driving, sleeping, and recreation. The NDI is
indicated for the following patient populations: chronic neck pain, musculoskeletal or
mechanical neck pain, cervicogenic headaches, whiplash injuries or whiplash associated
injuries, and cervical radiculopathy. One study found that in using the NDI for patient
OMPT and Cervicogenic Headache 22
clinical decision making, a clinically important change was calculated as 5 points, with a
sensitivity of 0.78 and a specificity of 0.80 (Stratford et al, 1999). The NDI has a fair to
moderate test-retest reliability in patients with mechanical neck pain, although intra class
correlations range between 0.50 and 0.98 (Cleland, Childs, & Whitman, 2008). The NDI has
good construct validity in comparison to other outcomes measurement tools including the
Visual Analog Scale, the Northwick Park Neck Pain Questionnaire, the Patient-Specific
Functional Scale, and The Disability Rating Index (Vernon & Mior, 1991; Hoving et al.,
2003).
Pain assessment. The patient was provided a numerical rating scale (NRS), which
is a patient, self-reported numerical rating of pain. The NRS allows the patient to select a
number from zero to ten with zero being “no pain” and ten being “worst pain imaginable”.
The NRS is a very common tool within the outpatient physical therapy setting, is easy to
reproduce, and has been validated by multiple patient populations (Goodman and Fuller,
2007). It is also important to note that in a recent study conducted on the mechanical neck
pain population, it was found that a point difference of greater than or equal to 1.3 is
suggestive of a minimum clinical important difference (Cleland & Fritz, 2006).
Jensen et al (1999) proposes that using a composite scoring system of current, best,
and worst levels of pain over the last 24 hours was effective at maximizing overall
reliability of this tool. Upon initial visit the patient reported her perceived pain level of the
cervical spine to be 7/10 at rest, 3/10 at its lowest, and 9/10 at its highest within the past
24 hours. The pain is located in bilateral upper trapezius muscles with the pain on the
right side being greater than on the left, in addition to the medial scapular region
bilaterally. The patient described this pain as being constant, dull, and worsens over the
OMPT and Cervicogenic Headache 23
course of the day. The patient also reported using ice, over-the-counter NSAIDs, soaks in
her Jacuzzi, and rest for relief from neck pain.
Behavioral aspects. The patient stated during her first visit that she felt as though
her neck was “out of place”. Because of this feeling, she reports regularly performing
intentional “cracks” of her neck. She states having some pain relief from this, but the
effects are short-lived. When there is hypermobility of the mid-cervical spine and
hypomobility demonstrated above and below these levels, it is possible that such frequent
intentional self-manipulations can have a negative impact on the relative mobility of the
cervical spine in regards to overstretching already relatively loose ligamentous structures.
The hypermobile mid-cervical articulations generally become even more hypermobile
overtime, which as a result predisposes the patient to having an increase of hypomobility
above and below the mid-cervical segments.
Objective Findings
Posture. The patient was found upon postural evaluation to have a resting forward
head position of the head on the cervical spine with hyper-extension of the upper cervical
segments. The resting position of the cervical spine was shown to be slightly bent to the
right. Both scapulae were found to be mildly abducted and demonstrated mild winging at
rest and increased with overhead movement, bilaterally.
Range of motion. Active range of motion of bilateral upper extremities was
screened and was found to be in normal, functional limits and pain-free. Cervical spine
active range of motion was measured using a standard goniometer to be 55 degrees for
forward flexion, 50 degrees for extension, 70 degrees for left rotation, and 54 degrees for
right rotation. Active movements into cervical spine extension, bilateral rotation, and
OMPT and Cervicogenic Headache 24
bilateral side-bending all were reported to be painful for the patient. Passive range of
motion was found to be restricted to only 20 degrees at the atlanto-axial joint (C1-C2) with
right rotation.
Manual muscle testing. Manual muscle testing was performed using the protocol
as outlined by Kendall, McCreary & Provance (2005). All muscles were found to be 5/5,
except for deep neck flexors (longus colli), middle trapezius, and lower trapezius which
were all found to be 3/5, or able to achieve full range of motion against gravity, but unable
to take any manual resistance.
Manual examination and palpation. The cervical spine passive intervertebral
motion examination revealed painful hypomobility (1+/6) with right rotation at the
atlanto-axial (C1-C2) joint. Hypomobility was also noted with passive downslide of the
right C6-C7 facet joint and with inferior glide of the right first rib. Hypermobility was noted
bilaterally with passive downslide of the mid-cervical spine.
Upon manual palpation of the neck region, the patient reported moderate
tenderness at the following anatomical landmarks: left transverse process of C2, right
transverse process of C7, bilateral sternocleidomastoid throughout the muscle bellies,
bilateral suboccipitals. Pressure over the right suboccipital muscle bellies were reported to
increase radicular symptoms into the side of the head. Cervical distraction testing resulted
in a patient-reported decrease of pain symptoms. Right-sided cervical compression (side-
bending with caudal overpressure) resulted in a patient-reported increase of pain
symptoms without radiculopathy. Alar and transverse ligament testing was found to be
negative.
OMPT and Cervicogenic Headache 25
Neurological testing. All dermatome testing resulted in normal findings, except for
the right C3 dermatome which was reported to be slightly diminished compared to the left
side. C5-C6 and C6-C7 reflex testing was found to be normal and symmetrical (2+).
Impression. It can be deduced from the examination findings that the case patient
has the signs and symptoms consistent with cervicogenic headaches. By using the IHS
diagnostic criterion for cervicogenic headaches (Figure 1), the case patient is found to
satisfy criteria A-C1. The case patient also satisfies the CHISG diagnostic criteria on all of
the following accounts: unilaterality of pain and headache, restricted neck ROM,
provocation of usual head pain by neck movement or sustained poor posture, and
provocation of usual head pain with external pressure over the upper cervical or occipital
region on the symptomatic side. It is also clear that this dysfunction is chronic in nature
based on her past history and amount of time that has passed since the beginning of her
symptoms. The major impairments that were gathered upon initial evaluation include:
1. Decreased range of motion of cervical spine
2. Tenderness to palpation of bilateral upper trapezius, sternocleidomastoid, and
suboccipital muscles, left transverse process at C2, and right transverse process
at C7.
3. Headaches into right frontal (supraorbital) region several times/month
4. Multi-level cervical and upper thoracic segmental mobility dysfunction
including: subcranial and lower cervical spine hypomobility and mid-cervical
spine hypermobility.
5. Muscular weakness of scapular stabilizers (middle/lower trapezius) and deep
neck flexors
OMPT and Cervicogenic Headache 26
6. Postural impairment: forward head, subcranial fault resting position of head
(side bent right), hyperextension of upper cervical spine, and abducted and
mildly winged scapula.
7. NDI Score of 40% - moderate severity of functional impact of impairments.
Prognosis
The chronic nature of the patient’s dysfunction complicates the rehabilitation
process and indicates a poorer prognosis overall. One study investigated the prognostic
factors that are associated with chronic neck pain. The patient was able to establish
significant self-reported and clinical progress in the past with physical therapy for similar
conditions in her prior plan of care from 2012. During this time, her SPADI score 26% to a
5.4% over the course of one month (9 visits total) which demonstrates a positive and
successful outcome to physical therapy.
Patient Goals
The original plan of care established included 4 weeks of formal physical therapy, two
times per week for a total of 8 visits. The following short term goals were established for
the patient to be met within 2 weeks:
1. Independence with home exercise program.
2. Patient to take an active role in rehabilitation program.
The following long term goals were established for the plan of care to be met within 4
weeks:
1. Reduced NDI from 40% to 18%.
2. Ability to look over either shoulder to see oncoming traffic while driving.
OMPT and Cervicogenic Headache 27
3. Improved strength (4/5 or above) for deep neck flexors, and scapular stabilizers.
4. 75%-100% reduced in frequency and intensity of headaches.
5. Ability to perform computer activities for work and pick up son with 75% decrease
of pain complaints.
Intervention
The patient was seen for a total of seven outpatient physical therapy visits with one
visit constituting the initial evaluation and the other six as follow-up visits. The patient was
not seen for a formal final visit and was discharged from the clinic at the end of February
due to her inability to attend physical therapy secondary to conflicts of schedule, both from
work and from prioritizing her efforts of in vitro fertilization in hopes of having her second
child.
During her initial evaluation, the patient was provided with manual therapy and
therapeutic exercise services. Gentle kneading and soft tissue massage was performed
bilaterally to the posterior cervical paraspinal musculature for five minutes. Two
therapeutic exercises were instructed, performed, and established for her home exercise
program: supine chin tucks in hooklying (3 sets of 10 repetitions, twice per day), and
doorway stretches for corrective posture (3 30-second stretches, twice per day).
Subsequent visits consisted of progressive manual therapy including soft tissue
massage and joint mobilization to the cervical spine and progressive strengthening
exercises to improve the postural balance of the upper quarter and stabilization of the
cervical spine as outline by Jull. All intervention sessions were tolerated well by the patient
and no reports were ever provided that described any adverse reactions to the physical
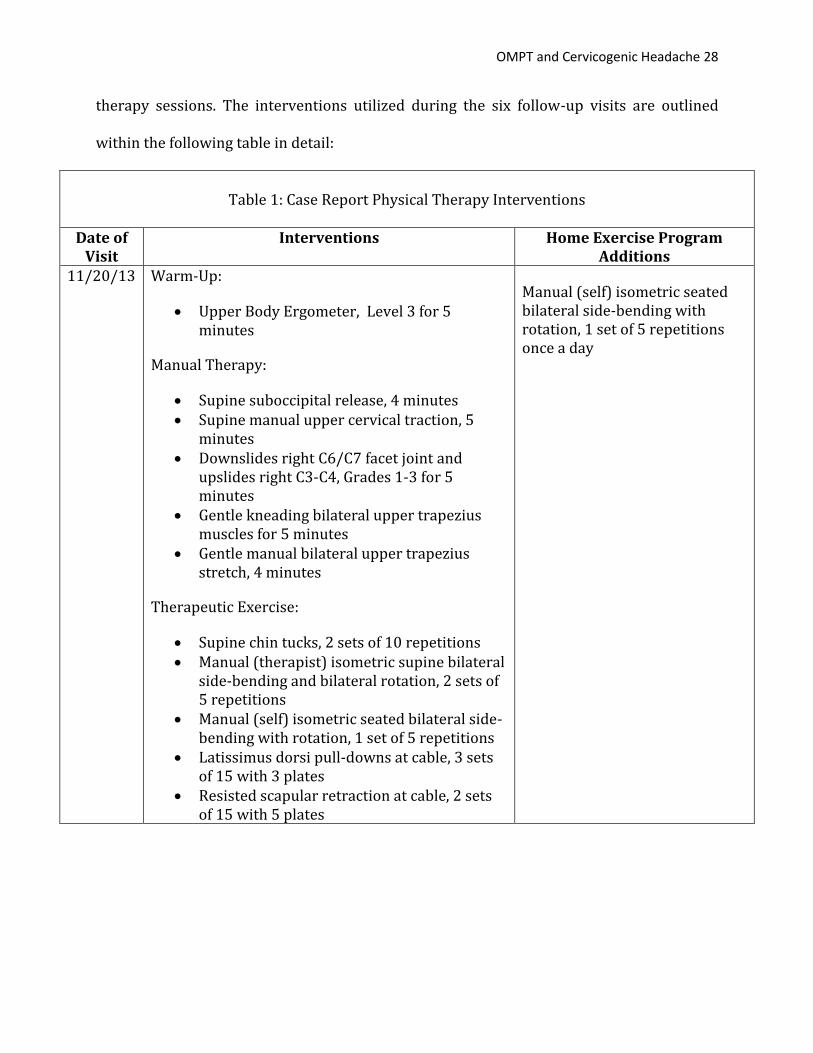
OMPT and Cervicogenic Headache 28
therapy sessions. The interventions utilized during the six follow-up visits are outlined
within the following table in detail:
Table 1: Case Report Physical Therapy Interventions
Date of
Visit Interventions Home Exercise Program
Additions 11/20/13 Warm-Up:
Upper Body Ergometer, Level 3 for 5 minutes
Manual Therapy:
Supine suboccipital release, 4 minutes Supine manual upper cervical traction, 5
minutes Downslides right C6/C7 facet joint and
upslides right C3-C4, Grades 1-3 for 5 minutes
Gentle kneading bilateral upper trapezius muscles for 5 minutes
Gentle manual bilateral upper trapezius stretch, 4 minutes
Therapeutic Exercise:
Supine chin tucks, 2 sets of 10 repetitions Manual (therapist) isometric supine bilateral
side-bending and bilateral rotation, 2 sets of 5 repetitions
Manual (self) isometric seated bilateral side-bending with rotation, 1 set of 5 repetitions
Latissimus dorsi pull-downs at cable, 3 sets of 15 with 3 plates
Resisted scapular retraction at cable, 2 sets of 15 with 5 plates
Manual (self) isometric seated bilateral side-bending with rotation, 1 set of 5 repetitions once a day
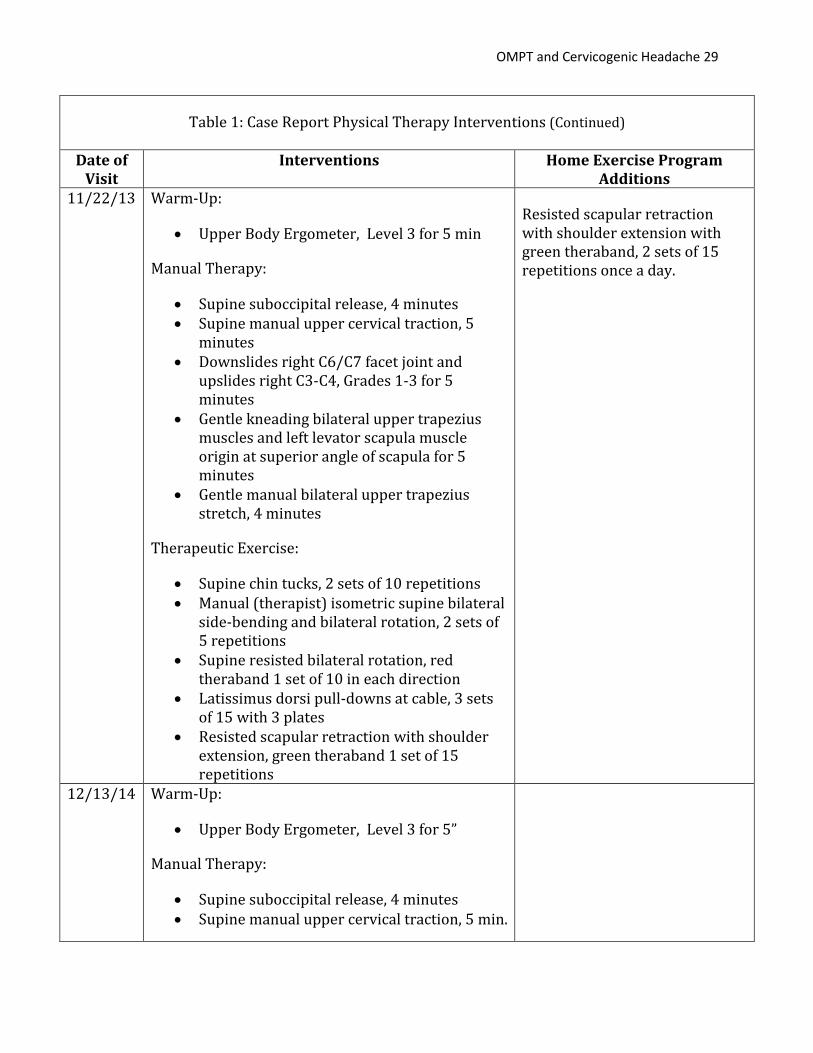
OMPT and Cervicogenic Headache 29
Table 1: Case Report Physical Therapy Interventions (Continued)
Date of Visit
Interventions Home Exercise Program Additions
11/22/13 Warm-Up:
Upper Body Ergometer, Level 3 for 5 min
Manual Therapy:
Supine suboccipital release, 4 minutes Supine manual upper cervical traction, 5
minutes Downslides right C6/C7 facet joint and
upslides right C3-C4, Grades 1-3 for 5 minutes
Gentle kneading bilateral upper trapezius muscles and left levator scapula muscle origin at superior angle of scapula for 5 minutes
Gentle manual bilateral upper trapezius stretch, 4 minutes
Therapeutic Exercise:
Supine chin tucks, 2 sets of 10 repetitions Manual (therapist) isometric supine bilateral
side-bending and bilateral rotation, 2 sets of 5 repetitions
Supine resisted bilateral rotation, red theraband 1 set of 10 in each direction
Latissimus dorsi pull-downs at cable, 3 sets of 15 with 3 plates
Resisted scapular retraction with shoulder extension, green theraband 1 set of 15 repetitions
Resisted scapular retraction with shoulder extension with green theraband, 2 sets of 15 repetitions once a day.
12/13/14 Warm-Up:
Upper Body Ergometer, Level 3 for 5”
Manual Therapy:
Supine suboccipital release, 4 minutes Supine manual upper cervical traction, 5 min.
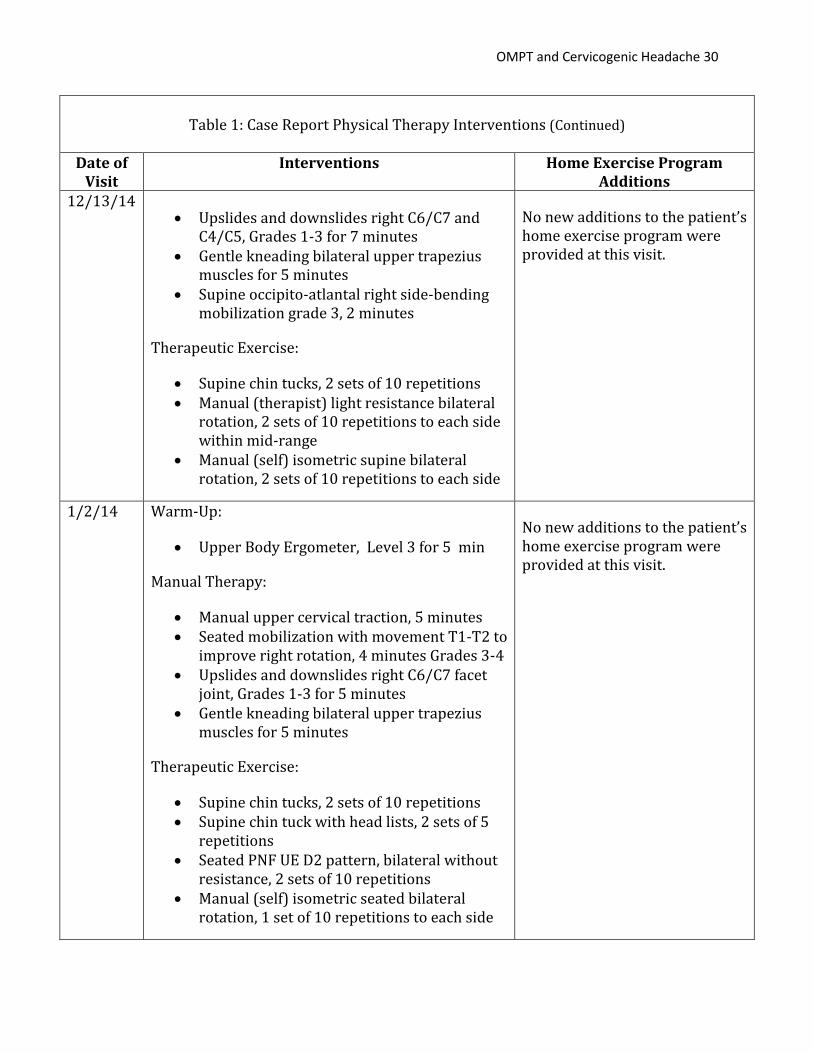
OMPT and Cervicogenic Headache 30
Table 1: Case Report Physical Therapy Interventions (Continued)
Date of
Visit Interventions Home Exercise Program
Additions 12/13/14
Upslides and downslides right C6/C7 and C4/C5, Grades 1-3 for 7 minutes
Gentle kneading bilateral upper trapezius muscles for 5 minutes
Supine occipito-atlantal right side-bending mobilization grade 3, 2 minutes
Therapeutic Exercise:
Supine chin tucks, 2 sets of 10 repetitions Manual (therapist) light resistance bilateral
rotation, 2 sets of 10 repetitions to each side within mid-range
Manual (self) isometric supine bilateral rotation, 2 sets of 10 repetitions to each side
No new additions to the patient’s home exercise program were provided at this visit.
1/2/14 Warm-Up:
Upper Body Ergometer, Level 3 for 5 min
Manual Therapy:
Manual upper cervical traction, 5 minutes Seated mobilization with movement T1-T2 to
improve right rotation, 4 minutes Grades 3-4 Upslides and downslides right C6/C7 facet
joint, Grades 1-3 for 5 minutes Gentle kneading bilateral upper trapezius
muscles for 5 minutes
Therapeutic Exercise:
Supine chin tucks, 2 sets of 10 repetitions Supine chin tuck with head lists, 2 sets of 5
repetitions Seated PNF UE D2 pattern, bilateral without
resistance, 2 sets of 10 repetitions Manual (self) isometric seated bilateral
rotation, 1 set of 10 repetitions to each side
No new additions to the patient’s home exercise program were provided at this visit.
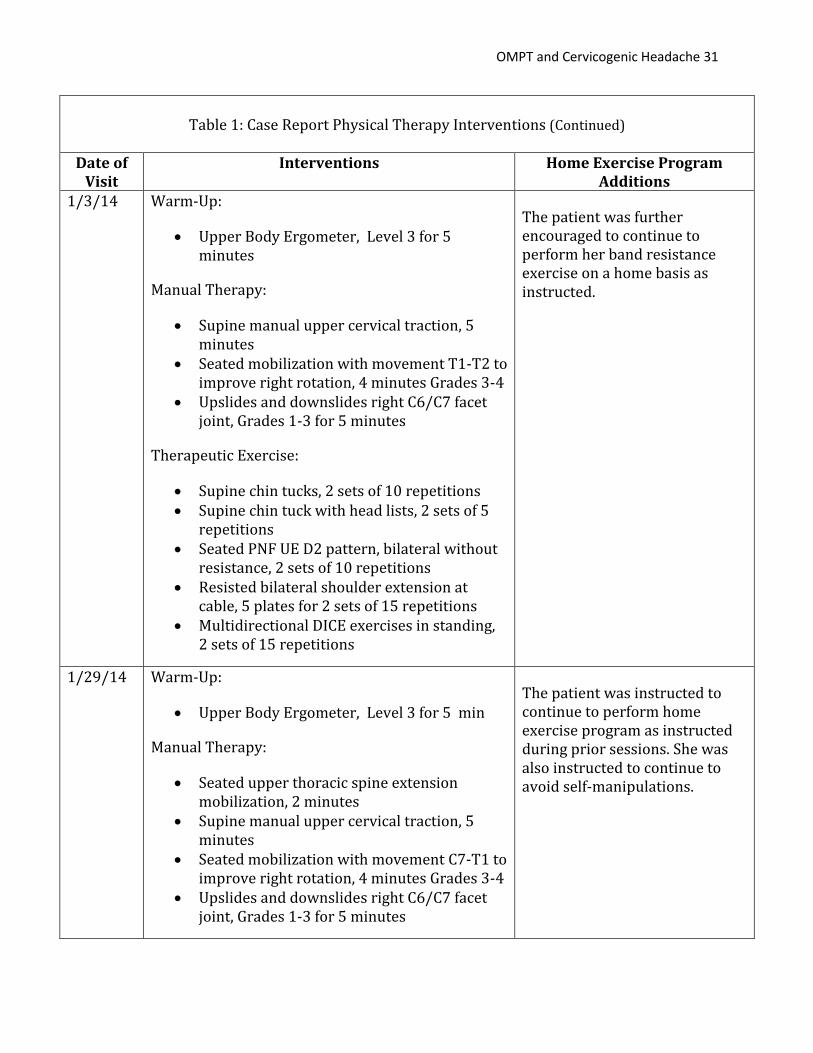
OMPT and Cervicogenic Headache 31
Table 1: Case Report Physical Therapy Interventions (Continued)
Date of
Visit Interventions Home Exercise Program
Additions 1/3/14 Warm-Up:
Upper Body Ergometer, Level 3 for 5 minutes
Manual Therapy:
Supine manual upper cervical traction, 5 minutes
Seated mobilization with movement T1-T2 to improve right rotation, 4 minutes Grades 3-4
Upslides and downslides right C6/C7 facet joint, Grades 1-3 for 5 minutes
Therapeutic Exercise:
Supine chin tucks, 2 sets of 10 repetitions Supine chin tuck with head lists, 2 sets of 5
repetitions Seated PNF UE D2 pattern, bilateral without
resistance, 2 sets of 10 repetitions Resisted bilateral shoulder extension at
cable, 5 plates for 2 sets of 15 repetitions Multidirectional DICE exercises in standing,
2 sets of 15 repetitions
The patient was further encouraged to continue to perform her band resistance exercise on a home basis as instructed.
1/29/14 Warm-Up:
Upper Body Ergometer, Level 3 for 5 min
Manual Therapy:
Seated upper thoracic spine extension mobilization, 2 minutes
Supine manual upper cervical traction, 5 minutes
Seated mobilization with movement C7-T1 to improve right rotation, 4 minutes Grades 3-4
Upslides and downslides right C6/C7 facet joint, Grades 1-3 for 5 minutes
The patient was instructed to continue to perform home exercise program as instructed during prior sessions. She was also instructed to continue to avoid self-manipulations.
OMPT and Cervicogenic Headache 32
Table 1: Case Report Physical Therapy Interventions (Continued)
Date of
Visit Interventions Home Exercise Program
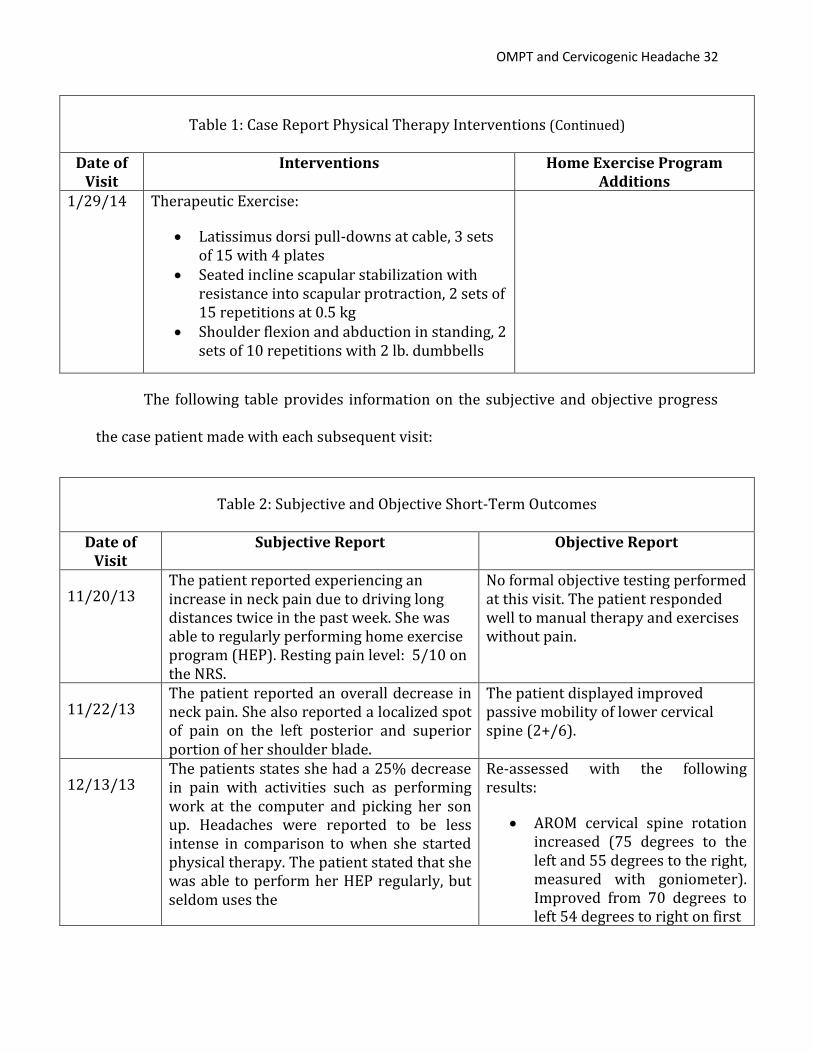
Additions 1/29/14 Therapeutic Exercise:
Latissimus dorsi pull-downs at cable, 3 sets of 15 with 4 plates
Seated incline scapular stabilization with resistance into scapular protraction, 2 sets of 15 repetitions at 0.5 kg
Shoulder flexion and abduction in standing, 2 sets of 10 repetitions with 2 lb. dumbbells
The following table provides information on the subjective and objective progress
the case patient made with each subsequent visit:
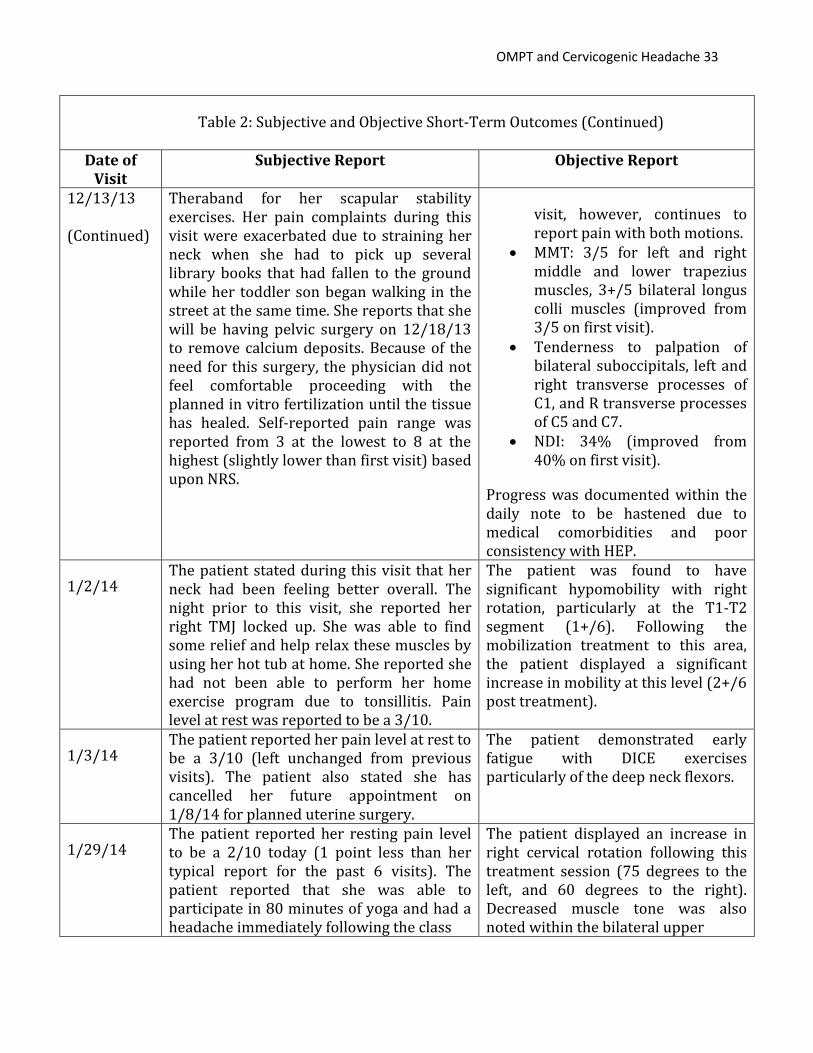
Table 2: Subjective and Objective Short-Term Outcomes
Date of Visit
Subjective Report Objective Report
11/20/13 The patient reported experiencing an increase in neck pain due to driving long distances twice in the past week. She was able to regularly performing home exercise program (HEP). Resting pain level: 5/10 on the NRS.
No formal objective testing performed at this visit. The patient responded well to manual therapy and exercises without pain.
11/22/13 The patient reported an overall decrease in neck pain. She also reported a localized spot of pain on the left posterior and superior portion of her shoulder blade.
The patient displayed improved passive mobility of lower cervical spine (2+/6).
12/13/13 The patients states she had a 25% decrease in pain with activities such as performing work at the computer and picking her son up. Headaches were reported to be less intense in comparison to when she started physical therapy. The patient stated that she was able to perform her HEP regularly, but seldom uses the
Re-assessed with the following results:
AROM cervical spine rotation increased (75 degrees to the left and 55 degrees to the right, measured with goniometer). Improved from 70 degrees to left 54 degrees to right on first
OMPT and Cervicogenic Headache 33
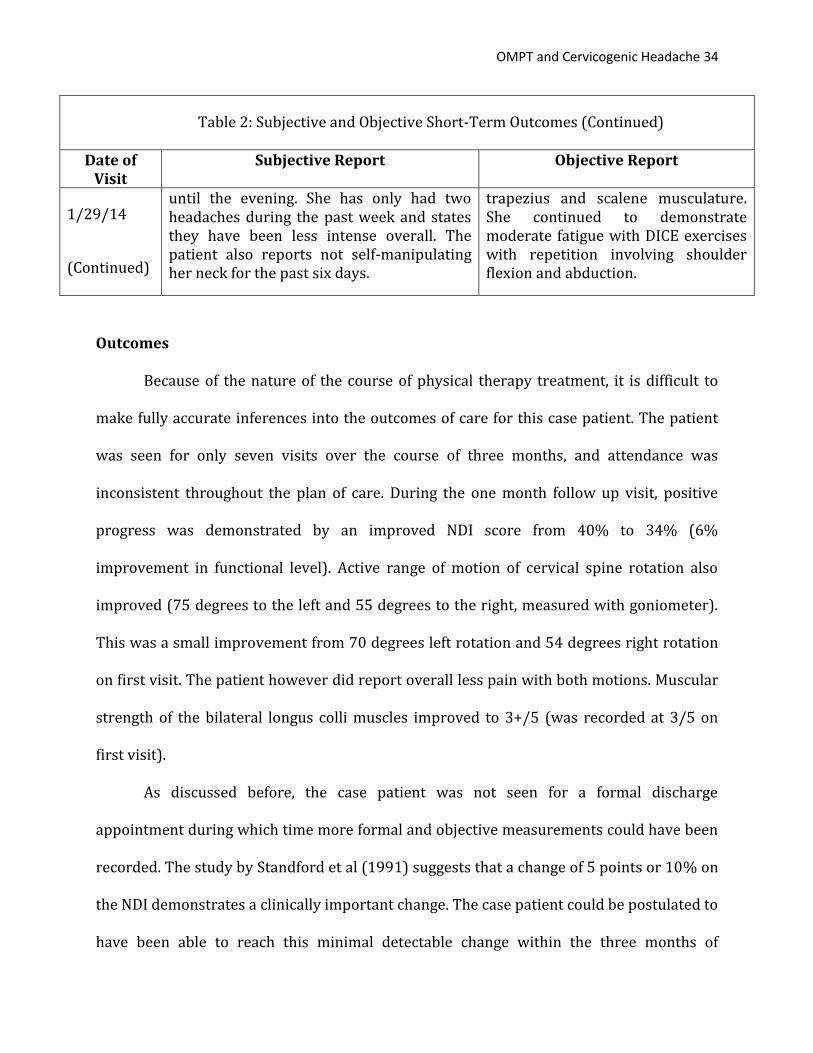
Table 2: Subjective and Objective Short-Term Outcomes (Continued)
Date of Visit
Subjective Report Objective Report
12/13/13
(Continued)
Theraband for her scapular stability exercises. Her pain complaints during this visit were exacerbated due to straining her neck when she had to pick up several library books that had fallen to the ground while her toddler son began walking in the street at the same time. She reports that she will be having pelvic surgery on 12/18/13 to remove calcium deposits. Because of the need for this surgery, the physician did not feel comfortable proceeding with the planned in vitro fertilization until the tissue has healed. Self-reported pain range was reported from 3 at the lowest to 8 at the highest (slightly lower than first visit) based upon NRS.
visit, however, continues to report pain with both motions.
MMT: 3/5 for left and right middle and lower trapezius muscles, 3+/5 bilateral longus colli muscles (improved from 3/5 on first visit).
Tenderness to palpation of bilateral suboccipitals, left and right transverse processes of C1, and R transverse processes of C5 and C7.
NDI: 34% (improved from 40% on first visit).
Progress was documented within the daily note to be hastened due to medical comorbidities and poor consistency with HEP.
1/2/14 The patient stated during this visit that her neck had been feeling better overall. The night prior to this visit, she reported her right TMJ locked up. She was able to find some relief and help relax these muscles by using her hot tub at home. She reported she had not been able to perform her home exercise program due to tonsillitis. Pain level at rest was reported to be a 3/10.
The patient was found to have significant hypomobility with right rotation, particularly at the T1-T2 segment (1+/6). Following the mobilization treatment to this area, the patient displayed a significant increase in mobility at this level (2+/6 post treatment).
1/3/14 The patient reported her pain level at rest to be a 3/10 (left unchanged from previous visits). The patient also stated she has cancelled her future appointment on 1/8/14 for planned uterine surgery.
The patient demonstrated early fatigue with DICE exercises particularly of the deep neck flexors.
1/29/14 The patient reported her resting pain level to be a 2/10 today (1 point less than her typical report for the past 6 visits). The patient reported that she was able to participate in 80 minutes of yoga and had a headache immediately following the class
The patient displayed an increase in right cervical rotation following this treatment session (75 degrees to the left, and 60 degrees to the right). Decreased muscle tone was also noted within the bilateral upper
OMPT and Cervicogenic Headache 34
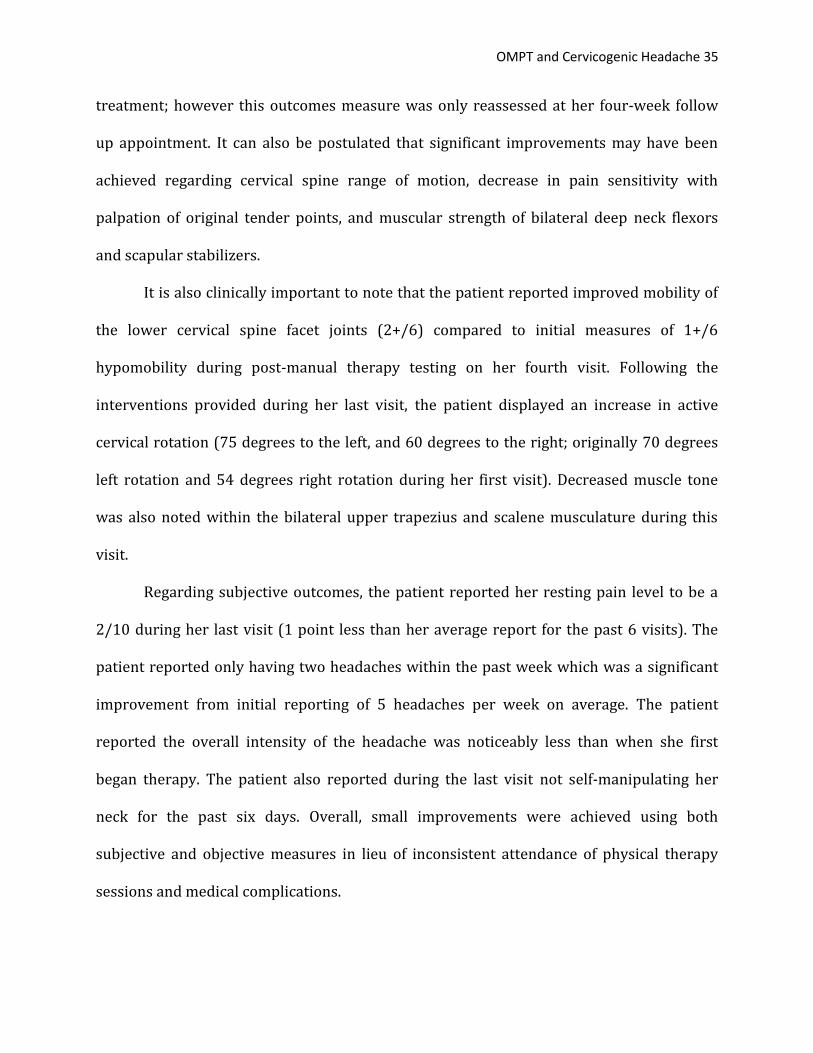
Table 2: Subjective and Objective Short-Term Outcomes (Continued)
Date of Visit
Subjective Report Objective Report
1/29/14
(Continued)
until the evening. She has only had two headaches during the past week and states they have been less intense overall. The patient also reports not self-manipulating her neck for the past six days.
trapezius and scalene musculature. She continued to demonstrate moderate fatigue with DICE exercises with repetition involving shoulder flexion and abduction.
Outcomes
Because of the nature of the course of physical therapy treatment, it is difficult to
make fully accurate inferences into the outcomes of care for this case patient. The patient
was seen for only seven visits over the course of three months, and attendance was
inconsistent throughout the plan of care. During the one month follow up visit, positive
progress was demonstrated by an improved NDI score from 40% to 34% (6%
improvement in functional level). Active range of motion of cervical spine rotation also
improved (75 degrees to the left and 55 degrees to the right, measured with goniometer).
This was a small improvement from 70 degrees left rotation and 54 degrees right rotation
on first visit. The patient however did report overall less pain with both motions. Muscular
strength of the bilateral longus colli muscles improved to 3+/5 (was recorded at 3/5 on
first visit).
As discussed before, the case patient was not seen for a formal discharge
appointment during which time more formal and objective measurements could have been
recorded. The study by Standford et al (1991) suggests that a change of 5 points or 10% on
the NDI demonstrates a clinically important change. The case patient could be postulated to
have been able to reach this minimal detectable change within the three months of
OMPT and Cervicogenic Headache 35
treatment; however this outcomes measure was only reassessed at her four-week follow
up appointment. It can also be postulated that significant improvements may have been
achieved regarding cervical spine range of motion, decrease in pain sensitivity with
palpation of original tender points, and muscular strength of bilateral deep neck flexors
and scapular stabilizers.
It is also clinically important to note that the patient reported improved mobility of
the lower cervical spine facet joints (2+/6) compared to initial measures of 1+/6
hypomobility during post-manual therapy testing on her fourth visit. Following the
interventions provided during her last visit, the patient displayed an increase in active
cervical rotation (75 degrees to the left, and 60 degrees to the right; originally 70 degrees
left rotation and 54 degrees right rotation during her first visit). Decreased muscle tone
was also noted within the bilateral upper trapezius and scalene musculature during this
visit.
Regarding subjective outcomes, the patient reported her resting pain level to be a
2/10 during her last visit (1 point less than her average report for the past 6 visits). The
patient reported only having two headaches within the past week which was a significant
improvement from initial reporting of 5 headaches per week on average. The patient
reported the overall intensity of the headache was noticeably less than when she first
began therapy. The patient also reported during the last visit not self-manipulating her
neck for the past six days. Overall, small improvements were achieved using both
subjective and objective measures in lieu of inconsistent attendance of physical therapy
sessions and medical complications.
OMPT and Cervicogenic Headache 36
Discussion
This case report describes the physical therapy diagnosis, management,
interventions including therapeutic exercise and orthopedic manual therapy, outcomes,
and other considerations of a patient with cervicogenic headache. The patient was a 35-
year old female referred by her primary care physician with complaints of chronic neck
pain. The patient presented at her initial evaluation with decreased range of motion of
cervical spine , tenderness to palpation of bilateral upper trapezius, sternocleidomastoid,
and suboccipital muscles, left transverse process at C2, and right transverse process at C7,
headaches into right frontal (supraorbital) region several times/month, multi-level cervical
and upper thoracic segmental mobility dysfunction, muscular weakness of scapular
stabilizers (middle/lower trapezius) and deep neck flexors, and postural impairments. The
Neck Disability Index (NDI) and Numerical Rating Scale (NRS) was a validated and reliable
outcomes measure tool used to determine progress over the course of treatment. Her
initial score was a 40%, moderate severity of functional impact of impairments. Patient
management of her condition consisted of various non-thrust manipulations, soft tissue
mobilizations, postural re-education, progressive therapeutic exercise, and patient
education for improved self-prevention of neck pain to address her impairments.
Although the patient made some minor improvements as indicated above within the
outcomes portion of this report, the overall progress was clinically insignificant most likely
due to poor compliance with home program, numerous medical comorbidities, and her
inability to regularly attend physical therapy. The patient’s improvement on the NDI and
NRS did not meet clinically important differences and minimal detectable change, however
did show minor improvement. Although outcomes for this case patient were not significant,
OMPT and Cervicogenic Headache 37
the progress indicated as supported by current evidence, suggest that a multi-modal
physical therapy treatment program approach using orthopedic manual physical therapy
interventions in addition to soft tissue manipulation, patient education, and therapeutic
exercise may be effective in the management of a patient diagnosed with cervicogenic
headache.
The mobilization techniques utilized for the case patient to improve overall cervical
spine mobility and decrease pain are based upon the manual therapy approaches
popularized by Stanley Paris of the University of Saint Augustine. These techniques include
upslides and downslides that utilize posterior-anterior mobilization combined with cranial
or caudal (respectively) glides to promote motion at restricted zygopophyseal joints.
A recent study examined the short-term biomechanical effects of non-thrust
(Maitland, Grade III techniques) PA manipulation techniques on the cervical spine (Lee et
al, 2005). Although this manual therapy technique is relatively common in the evaluation
and treatment of neck pain, little is known about the actual biomechanical effects. Much of
the research has historically been focused on the benefits within lumbar spine for patients
with low back pain. Within this study, the cervical spines of nineteen healthy subjects were
scanned using an open interventional magnetic resonance imaging scanner.
Posteroanterior (PA) mobilization forces were applied to the fifth cervical vertebra in the
prone position. It was shown from sagittal images obtained before and during the
mobilization that PA mobilization of the cervical spine generally produced extension of the
upper motion segments and flexion of the lower segments when forces were applied at the
5th cervical vertebrae. The cervical lordosis was found to increase with repeated PA loading
cycles, which is particularly important to know when clinically providing interventions to
OMPT and Cervicogenic Headache 38
restore cervical lordosis that may be significantly reduced with a resting forward head
posture. It was also found that forces applied at one spinous process produced not only
movements at the target vertebra, but also movements throughout the entire cervical spine
helping to restore cervical lordosis and overall mobility. The most interesting
interpretation from this research study was that mobilizations to this area should be
interpreted as three-point bending of the entire cervical spine, rather than simple gliding of
one vertebra upon another. Several of the mobilizations provided to the case patient were
applied to the fifth cervical vertebrae which may explain her improvements in overall
range of motion even after just seven visits.
The patient also reported a decrease in pain overall within the neck region and
decreases in headache intensity and frequency which may very well be related to the
nociceptive inhibitory effect spinal manipulation therapy is able to produce. As stated
before, spinal manipulative therapy has been shown to help activate descending inhibitory
pathways from, the lateral periaqueductal gray area of the midbrain (Wright, 1995). The
lateral periaqueductal gray (PAG) is closely related to the behavioral responses to pain,
stress, and other stimuli in maintaining internal homeostasis, which (Fernandez de-las-
Penas et al., 2006). Although the overall patient outcomes were minimal due to poor
consistency and adherence to a regular physical therapy program, positive gains were
made regarding cervical spine range of motion, pain level, and headache intensity and
frequency. From this information, it can be inferred that spinal manipulative therapy
utilizing PA forces for the cervical spine may help to improve clinical outcomes for patients
with cervicogenic headaches.
OMPT and Cervicogenic Headache 39
Because the case patient had been experiencing headaches and neck pain for many
months and had entered a chronic stage of her condition, evidence for the use of thoracic
spine manipulation to improve neck pain may not have been indicated as outlined by a
recent clinical prediction rule by Childs et al (2007). When 5-6 of the clinical prediction
rule factors (symptoms <30 days, no symptoms distal to the shoulder, looking up does not
aggravate symptoms, Fear Avoidance Beliefs Questionnaire Physical Activity (FABQPA
<12), diminished upper thoracic spine kyphosis based on visual estimate, and cervical
extension ROM <30 degrees) are satisfied a positive likelihood ratio of greater than 12 is
indicated for positive outcomes in reducing neck pain from thoracic spine manipulation. In
a later validation study of this clinical prediction rule, patients with mechanical neck pain
who received thoracic spine manipulation and exercise exhibited significantly greater
improvements in disability and pain at both the short- and long-term follow-up periods
compared with patients who received exercise only. The benefits of targeting manipulation
to patients who were positive on the CPR were marginal and were evident only at the
short-term follow-ups visits. From this information, it may be inferred that the even though
the case patient may not have met the clinical prediction rule, she may have still benefitted
from thoracic spine manipulations during each treatment session to help decrease overall
disability and pain.
To consider patient management for chronic-type conditions of cervicogenic
headaches it is important to consider the benefits of utilizing a combined approach of
manipulative therapy with therapeutic exercise. A recent study investigated the effects of
low load cranio-cervical flexion verses neck flexor strengthening exercises on deep cervical
flexor muscle activation, neck pain intensity score, neck disability index, and perceived
OMPT and Cervicogenic Headache 40
benefit of exercise (Jull et al, 2009). In this study forty-six subjects with chronic neck pain
were randomly assigned to one of following two groups for a 6-week training program:
o Low Load training: 10 reps of 10 seconds at progressively higher
biofeedback pressure unit levels (20mmHg – 30mmHg)
o Higher load strength training:
Stage one: 12-15 reps at a load that could initially be only lifted 12
times
Stage two: 3 sets of 10 reps using 50% 10 repetition max load, then
75% RM, then 100% RM.
Based upon electromyographic activity data of the neck musculature before and after
exercise intervention, the low load-training group had increases in EMG activity of the deep
cervical flexors, with decreases in EMG amplitude for the sternocleidomastoid and anterior
scalene muscles across all stages of the cranio-cervical flexion test. The cranio-cervical
flexion low load training has been study extensively by Jull and colleagues, and have been
shown to be an effective intervention for patients with chronic mechanical neck pain (Jull
et al., 2002; Jull et all., 2008).
Canegie et al (2007) also found similar results previously by examining functional
MRI results to evaluate cervical flexor activity during different cervical flexion exercises.
The results from this study demonstrated that combined cranio-cervical flexion and
cervical flexion (chin tuck with head lift) produced the highest increase between rest and
post exercise, demonstrating that all synergists were active and that this exercise is useful
for strengthening the sternocleidomastoid (SCM), longus capitis, and longus colli. During
OMPT and Cervicogenic Headache 41
cervical flexion (head lift), it was found that the longus colli is more active than longus
capitis and SCM, although the differences were found to be statistically insignificant.
The therapeutic exercises used for this case patient both within the clinical setting
and for her home exercise program are consistent with the recommendations made based
on these studies and involved low load, high repetitions at progressively higher demands
over time. In addition, the therapeutic exercises were gradually progressed in order to
allow the patient to develop proper recruitment of deep neck flexors in order to prevent
further neck strain and overuse of superficial anterior neck muscles, as commonly seen
with this population. By also including exercises which required the recruitment of deep
neck flexors immediately prior to active upper extremity resisted movements (DICE
exercises), the patient was able theoretically able to facilitate coordination with functional
overhead and lifting activities. Unfortunately, the final two physical therapy sessions were
the only sessions that included these exercises; continued sessions with such interventions
may have provided more significant outcomes.
It is important to discuss the issues of compliance and inconsistent attendance of
physical therapy for this case patient. The patient was seen for a total of seven visits over
the course of three months, which relative to the typical physical therapy plan of care, were
spread out over a long period of time. In addition, the patient had several medical
comorbidities during her plan of care and was dually seeking in vitro fertilization
treatment. As a result, she was unable to attend in a consistent manner as she had been
able to in her prior plan of care from 2012. During her prior plan of care, the patient was
able to regularly attend several times over the course of 5 weeks and made significant
progress in decreasing overall pain and improving functional use of her right upper
OMPT and Cervicogenic Headache 42
extremity. The Shoulder Pain and Disability Index, which examines the overall functional
level of the involved shoulder (Roach, 1991), was reduced from a 26% to a 5.4% over the
course of one month of her prior period of care during 2012. This was a clinically
significant and powerful reduction of overall disability which can be attributed, in part, to
her compliance with her home exercise program and ability to regularly attend physical
therapy during this time.
One recent study found strong evidence that poor treatment adherence was
associated with low levels of physical activity at baseline or in previous weeks, low in-
treatment adherence with exercise, low self-efficacy, depression, anxiety, helplessness,
poor social support/activity, greater perceived number of barriers to exercise and
increased pain levels during exercise (Jack, McLean, Moffett, & Gardiner, 2010). Although
this systematic review analyzed mostly prior studies that examined prognostic factors for
patients with chronic low back pain, these psychosocial aspects can also be applied to a
patient with chronic neck pain.
Another systematic review examined 70 articles on the course and prognostic
factors in neck pain and its associated disorders. It was found within the review that
younger age predicted better outcome. Psychosocial factors, including psychological health,
coping patterns, and need to socialize, were the strongest prognostic factors. It was also
found that factors including: higher initial pain intensity, longer duration, and increased
pain-related difficulties in performing activities, prior neck/shoulder symptoms, prior neck
injury, co-morbid low back pain, and self-perceived poor general health. Determining
prognosis for a patient with chronic neck pain can be difficult at times due to the complex
nature and combination effect of various demographic, socioeconomic, and psychosocial
OMPT and Cervicogenic Headache 43
factors. Future systematic reviews should continue to examine the major prognostic factors
for patients with chronic neck pain and headaches.
In summary, although the patient demonstrated inconsistencies in physical therapy
treatment attendance and poor compliance of her home exercise program, minor
improvements were made in regards to all initial impairments and particularly with overall
functional level as shown by the improved NDI score. It is likely that the patient had
multiple poor prognostic factors that also played a negative role in the degree of positive
outcomes that were made during this plan of care. A significant amount of evidence exists
to help support the basis for using orthopedic manual therapy interventions to reduce pain
and improve range of motion in cervical spine, and one can make the case that these
interventions combined with therapeutic exercises was able to create overall
improvements for this patient.
Conclusion
This case report demonstrates the physical therapy diagnosis, management,
interventions including therapeutic exercise and orthopedic manual therapy, and outcomes
of a patient with cervicogenic headache. The patient presentation corresponded with the
diagnostic criteria for cervicogenic headaches as outlined by the IHS and CHISG (Becker
2010; Antonaci et al., 2005). Comprehensive physical therapy treatment was provided to
this case patient for seven visits over a total of three months using orthopedic manual
therapy spinal mobilizations, soft tissue manipulation, patient education, and progressive
therapeutic exercises to improve strength of deep neck flexors and improve postural
impairments. Although outcomes for this case patient were not significant and all short
term and long term goals were not fully met, the progress indicated as supported by

OMPT and Cervicogenic Headache 44
current evidence, suggest that a multi-modal physical therapy treatment program
approach using orthopedic manual physical therapy interventions in addition to soft tissue
manipulation, patient education, and therapeutic exercise may be effective in the
management of a patient diagnosed with cervicogenic headache. This case report also
demonstrates the importance of considering prognostic factors and patient compliance in
providing treatment for patients with chronic neck pain and cervicogenic headaches. It can
OMPT and Cervicogenic Headache 45
References
Allen C. J., Terrett, D., & Vernon, H. (1984). Manipulation and pain tolerance. American Journal of Physical Medicine, 63:217–25.
Antonaci, F., Bono, G., Mauri, M., Drottning, M. & Buscone, S. (2005). Concepts leading to the
definition of the term cervicogenic headache: a historical overview. Journal of Headache Pain, 6, 462-466.
Becker, W. J. (2010). Cervicogenic headache: evidence that the neck is a pain generator.
Headache Currents, April, 699-705. Christian, G. F., Stanton, G. J., & Sissions, D. (1988). Immunoreaction ACTH, betaendorphins,
and cortisol levels in plasma following spinal manipulative therapies. Spine, 13: 1411-17.
Cleland, J. A., & Fritz, J. M. (2006). The reliability and construct validity of the Neck
Disability Index and patient specific functional scale in patients with cervical radiculopathy. Spine, 31(5):598-602.
Cleland, J. A, Childs , J. D., & Fritz J. M. (2007). Development of a clinical prediction rule for
guiding treatment of a subgroup of patients with neck pain: use of thoracic spine manipulation, exercise, and patient education. Physical Therapy, 87(1): 9-23.
Cleland, J. A., Childs, J. D., & Whitman, J.M. (2008). Psychometric properties of the neck
disability index and numeric pain rating scale in patients with mechanical neck pain. Archives of Physical Medicine and Rehabilitation, 89(1), 69-74.
Cleland, J. A., Mintken, P .E., Carpenter, K. , Fritz, J. , Glyn, P., Whitman, J. & Childs, J. D.
(2010). Examination of a clinical prediction rule to identify patient with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: a multi-center randomized clinical trial. Physical Therapy, 90:1239-1250.
Depaulis, A., & Bandler R. (1991). The Midbrain Periaqueductal Gray Matter. New York:
Prenum Press. Ferdandez de-las-Penas, C., Alonso-Blanco, C., San-Roman, J.,& Miangolarra-Page, J. C.
(2006). Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. Journal of Orthopedic and Sports Physical Therapy, 36, 160-169.
Goodman, C. C., & Fuller, K. S. (2009). Pathology: implications for the physical therapist.
Elsevier 3rd Edition.
OMPT and Cervicogenic Headache 46
Gross A., Miller J., D'Sylva, J., Burnie, S. J., Goldsmith, C.H., & Graham, N. (2010). Manipulation or mobilisation for neck pain: a cochrane review. Manual Therapy, 15(4):315-33.
Hall, T., Robinson, K. (2004). The flexion-rotation test and active cervical mobility – a
comparative measurement study in cervicogenic headache. Manual Therapy, 9(4), 197-202.
Hall, T. M., Briffa, K., Hopper, D., & Robinson, K. (2010). Comparative analysis and
diagnostic accuracy of the cervical flexion-rotation test. Journal of Headache Pain, 11, 391-397.
Hall, T., Briffa, K., Hopper, D., & Robinson, K. (2010). Reliability of manual examination and
frequency of symptomatic cervical motion segment dysfunction in cervicogenic headaches. Manual Therapy, 15, 542-546.
Hoving, J. L., O’Leary, E. F., Niere, K. R., Green, S., & Buchbinder, R. (2003). Validity of the
neck disability index, Northwick park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders, pain. Journal of Orthopedic and Sports Physical Therapy, 102(3), 273-281.
Jack, K., McLean, S. M., Moffett, J. M., & Gardiner, E. (2010). Barriers to treatment adherence
in physiotherapy outpatient clinics: a systematic review. Manual Therapy, 15(3-2): 220-228.
Jensen, M. P., Turner, J. A., Romano, J. M., Fisher, & L. D. (1999). Comparative reliability and
validity of chronic pain intensity measures. Pain; 83(2): 157-162. Jull, G. (1997). Management of cervical headache. Manual Therapy; 2: 182-190. Jull, G. (1998). Characterization of cervicogenic headache. Journal of Physical Therapy; 3:
95-105. Jull, G., Trott, P., & Potter, H. (2002). A randomized controlled trial of exercise and
manipulative therapy for cervicogenic headache. Spine, 27: 1835-1843. Jull, G., Amiri, M., Bullock-Saxton, J., Darnell R., & Lander, C. (2007). Cervical
musculoskeletal impairment in frequent intermittent headache. Part 1: subjects with single headaches. Cephalgia, 27(7), 793-802.
Jull, G. A., Falla, D., Vicenzino, B., & Hodges, P. (2009). The effect of therapeutic exercise on
activation of the deep cervical flexor muscles in people with chronic neck pain. Manual Therapy, 14: 696-701.
Kendall, F., McCreary, E., & Provance, P (2005). Muscle Testing and Function. Williams and
Wilkins. Fourth Edition.
OMPT and Cervicogenic Headache 47
Lee R. Y., McGregor, A. H., Bull, A. M., & Wragg, P (2005). Dynamic response of the cervical spine to posteroanterior mobilization. Clinical Biomechanics, 20: 228-231.
Macdermid, J. C., Walton, D. M., Avery, S., Blanchard, A., Etruw, E, & Goldsmith, C. H. (2009).
Measurement properties of the neck disability index: a systematic review. Journal of Orthopedic and Sports Physical Therapy, 39(5), 400-417.
Masaracchio, M., Cleland, J. A., Hellman, M., & Hagins, M. (2013). Short-term combined
effects of thoracic spine thrust manipulation and cervical spine nonthrust manipulation in individuals with mechanical neck pain: a randomized clinical trial. Journal of Orthopaedic and Sports Physical Therapy, 43(3).
Miller, J., Gross, A., D’Sylva, J., Burnie, S. J., Goldsmith, C. H., Graham, N., Haines, T., Bronfort,
G., & Hoving, J. L. (2010). Manual therapy and exercise for neck pain: A systematic review. Manual Therapy, 15, 334-354.
Paris, S. V., Loubert, P. V. (1999). Foundations of Clinical Orthopedics. 3rd Edition. St.
Augustine, FL, Institute Press. Roach, K. E., Budiman-Mak, E., Songsiridej, N., & Lertratanakul, Y (1991). Development of a
shoulder pain and disability index. Arthritis Care Research, 4(4): 143-149. Sterling, M., Jull, G., Wright, A. (2001). Cervical mobilization: concurrent effects on pain,
sympathetic nervous system activity and motor activity. Manual Therapy, 6, 72-81. Stratford, P. W., Riddle, D. L., & Binkley, J. M. (1999). Using the neck disability index to make
decisions concerning individual patients. Physiotherapy Canada, 2, 107-112. Vavrek, D., Haas, M., Peterson, D. (2010). Physical examination and self-reported pain
outcomes from a randomized trial on chronic cervicogenic headache. Journal of Manipulative Physical Therapy, 33, 338-348.
Vernon, H., & Mior, S. (1991). The neck disability index: a study of reliability and validity.
Journal of Manipulative and Physiological Therapeutics, 14, 409-15. Von Piekartz, H., Ludtke, K. (2011). Effect of treatment of temporomandibular disorders
(TMD) in patients with cervicogenic headache: a single-blind, randomized controlled study. Journal of Craniomandibular Practice, 29(1), 43-56.
Whittingham, W., & Nilsson, N. (2001). Active range of motion in the cervical spine
increases after spinal manipulation (toggle recoil). Journal of Manipulative and Physiological Therapeutics, 24(9), 552-555.
Wright, A. (1995). Hypoalgesia postmanipulative therapy: A review of the potential
neurophysiological mechanisms. Manual Therapy: 1, 11–16.

OMPT and Cervicogenic Headache 48
Zito, G., Jull, G., & Story, I. (2003). Clinical tests of musculoskeletal dysfunction in the diagnosis of cervicogenic headache. Manual Therapy, 11, 118-129.