Embed Size (px)
Citation preview
Original Research ajog.org
OBSTETRICS
Evaluation of trainees’ ability to perform obstetricalultrasound using simulation: challenges and opportunitiesGihad E. Chalouhi, MD; Valeria Bernardi, MD; Alexandra Gueneuc, MD; Isabelle Houssin, MS;Julien J. Stirnemann, MD, PhD; Yves Ville, MD, PhD
BACKGROUND: Evaluation of trainee’s ability in obstetrical ultrasound examiners and scores of dexterity and also to compare the final scores
is a time-consuming process, which requires involving patients as vol-
unteers. With the use of obstetrical ultrasound simulators, virtual reality
could help in assessing competency and evaluating trainees in this field.
OBJECTIVE: The objective of the study was to test the validity of anobstetrical ultrasound simulator as a tool for evaluating trainees following
structured training by comparing scores obtained on obstetrical ultrasound
simulator with those obtained on volunteers and by assessing correlations
between scores of images and of dexterity given by 2 blinded examiners.
STUDY DESIGN: Trainees, taking the 2013 French national exami-
nation for the practice of obstetrical ultrasound were asked to obtain
standardized ultrasound planes both on volunteer pregnant women and on
an obstetrical ultrasound simulator. These planes included measurements
of biparietal diameter, abdominal circumference, and femur length as well
as reference planes for cardiac 4-chamber and outflow tracts, kidneys,
stomach/diaphragm, spine, and face. Images were stored and evaluated
subsequently by 2 national examiners who scored each picture according
to previously established quality criteria. Dexterity was also evaluated and
subjectively scored between 0 and 10. The Raghunathan’s modification of
Pearson, Filon’s z, Spearman’s rank correlation, and analysis of variance
tests were used to assess correlations between the scores by the 2
Cite this article as: Chalouhi GE, Bernardi V, Gueneuc A,et al. Evaluation of trainees’ ability to perform obstetrical
ultrasound using simulation: challenges and opportu-
nities. Am J Obstet Gynecol 2016;214:525.e1-8.
0002-9378/$36.00ª 2016 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.ajog.2015.10.932
between the 2 different methods.
RESULTS: We evaluated 29 trainees. The mean dexterity scores in
simulation (6.5� 2.0) and real examination (5.9� 2.3) were comparable
(P ¼ .31). Scores with an obstetrical ultrasound simulator were signifi-
cantly higher than those obtained on volunteers (P¼ .027). Nevertheless,
there was a good correlation between the scores of the 2 examiners
judging on simulation (R ¼ 0.888) and on volunteers (R ¼ 0.873)
(P ¼ .81).
CONCLUSION: An obstetrical ultrasound simulator is as good a
method as volunteer-based examination for evaluating practical skills in
trainees following structured training in obstetrical ultrasound. The
threshold for success/failure should, however, be adapted as candidates
obtain higher scores on the simulator. Advantages of the obstetrical
ultrasound simulator include the absence of location and time constraints
without the need to involve volunteers or to interfere with the running of
ultrasound clinics. However, an obstetrical ultrasound simulator still lacks
the ability to evaluate the trainees’ ability to interact with patients.
Key words: evaluation, medical education, simulation, training,ultrasound
ltrasonography is the most used
U imaging tool in prenatal assess-ment. Although it offers an efficientscreening strategy, it still has limitationsin detecting congenital anomalies.1-3 It isdependent on the operator’s technicalskills,4 its practice is standardized, andcertification of competency is oftenrequired.5 Evaluation of trainee’s abilityis a time-consuming process, which re-quires involving patients as volunteers.6Simulation has spread out from edu-cation in aviation and military industryto health care over the last 40 years.7-11 Itis being used as a method to train but
also to assess learners.8-11 Multiple fac-tors have contributed to this expansionincluding limited patient availability,increasing concern for patients’ safety12
and the need to minimize medical er-rors. This development has also beenimposed by technological advances indiagnosis and treatment, which requirenew skills and increased traininghours.8,13,14
With the advent of obstetrical ultra-sound simulators (OUS), training andassessing competency in this field mayalso evolve rapidly. Virtual reality couldhelp solve some of the problems afore-mentioned by providing a virtual patientand a virtual setting in which the ultra-sound examination could take placewithout interfering with the normalactivities and settings of medical units.The aim of our study was to assess the
potential for an obstetrical ultrasoundsimulator to be used as a substitute forthe use of volunteers to evaluate trainees’
APRIL 2016 Ameri
ability to perform obstetrical ultrasound(US).
Materials and MethodsCandidate sonologists to the AnnualFrench National Examination of Ultra-sound in Obstetrics and Gynecologywere recruited at Paris DescartesUniversity in September 2013.
In France, obstetrical sonologists areobstetricians, radiologists, or midwives.They are required to attend more than100 hours of theoretical teaching and aminimum of 40 3 hour sessions undersupervision within a clinical setting ofultrasound in obstetrics and gynecologyover 1 year. They are then subjected to anational written examination, and thosewho score at least 50% are then requiredto sit for a practical evaluation.
The latter consists of performing asecond-trimester ultrasound examina-tion including the following: identifica-tion of fetal presentation, placental
can Journal of Obstetrics & Gynecology 525.e1
Original Research OBSTETRICS ajog.org
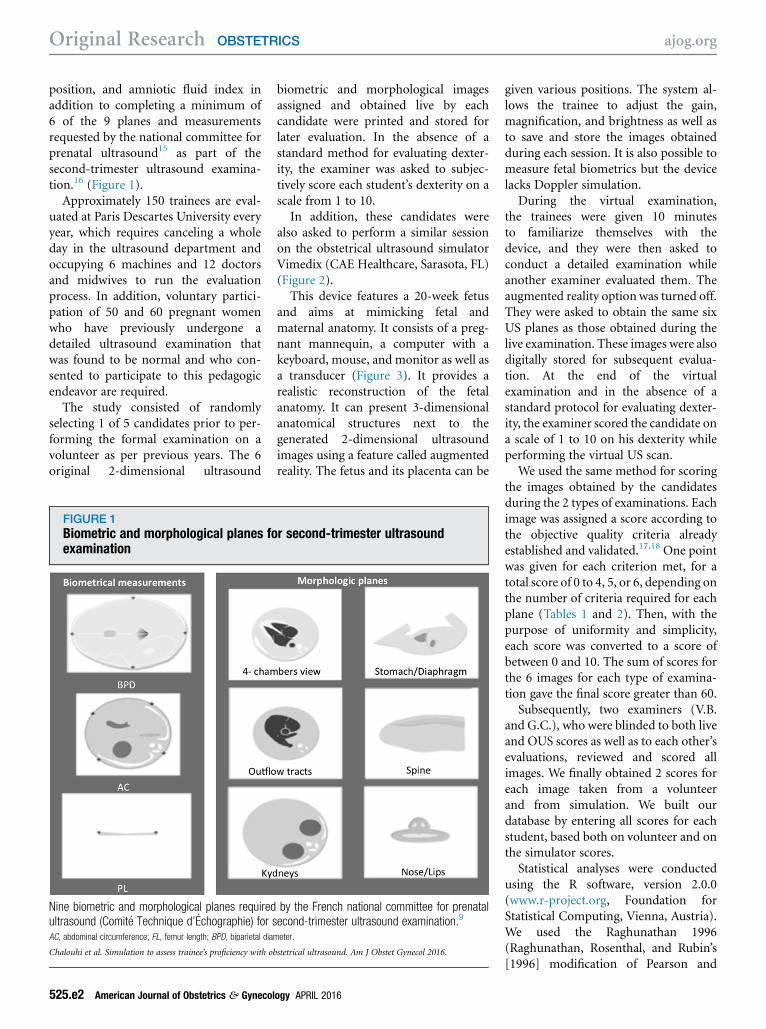
position, and amniotic fluid index inaddition to completing a minimum of6 of the 9 planes and measurementsrequested by the national committee forprenatal ultrasound15 as part of thesecond-trimester ultrasound examina-tion.16 (Figure 1).
Approximately 150 trainees are eval-uated at Paris Descartes University everyyear, which requires canceling a wholeday in the ultrasound department andoccupying 6 machines and 12 doctorsand midwives to run the evaluationprocess. In addition, voluntary partici-pation of 50 and 60 pregnant womenwho have previously undergone adetailed ultrasound examination thatwas found to be normal and who con-sented to participate to this pedagogicendeavor are required.
The study consisted of randomlyselecting 1 of 5 candidates prior to per-forming the formal examination on avolunteer as per previous years. The 6original 2-dimensional ultrasound
FIGURE 1Biometric and morphological planes foexamination
Nine biometric and morphological planes requiredultrasound (Comite Technique d’Echographie) for sAC, abdominal circumference; FL, femur length; BPD, biparietal dia
Chalouhi et al. Simulation to assess trainee’s proficiency with o
525.e2 American Journal of Obstetrics & Gynecol
biometric and morphological imagesassigned and obtained live by eachcandidate were printed and stored forlater evaluation. In the absence of astandard method for evaluating dexter-ity, the examiner was asked to subjec-tively score each student’s dexterity on ascale from 1 to 10.In addition, these candidates were
also asked to perform a similar sessionon the obstetrical ultrasound simulatorVimedix (CAE Healthcare, Sarasota, FL)(Figure 2).This device features a 20-week fetus
and aims at mimicking fetal andmaternal anatomy. It consists of a preg-nant mannequin, a computer with akeyboard, mouse, and monitor as well asa transducer (Figure 3). It provides arealistic reconstruction of the fetalanatomy. It can present 3-dimensionalanatomical structures next to thegenerated 2-dimensional ultrasoundimages using a feature called augmentedreality. The fetus and its placenta can be
r second-trimester ultrasound
by the French national committee for prenatalecond-trimester ultrasound examination.9
meter.
bstetrical ultrasound. Am J Obstet Gynecol 2016.
ogy APRIL 2016
given various positions. The system al-lows the trainee to adjust the gain,magnification, and brightness as well asto save and store the images obtainedduring each session. It is also possible tomeasure fetal biometrics but the devicelacks Doppler simulation.
During the virtual examination,the trainees were given 10 minutesto familiarize themselves with thedevice, and they were then asked toconduct a detailed examination whileanother examiner evaluated them. Theaugmented reality option was turned off.They were asked to obtain the same sixUS planes as those obtained during thelive examination. These images were alsodigitally stored for subsequent evalua-tion. At the end of the virtualexamination and in the absence of astandard protocol for evaluating dexter-ity, the examiner scored the candidate ona scale of 1 to 10 on his dexterity whileperforming the virtual US scan.
We used the same method for scoringthe images obtained by the candidatesduring the 2 types of examinations. Eachimage was assigned a score according tothe objective quality criteria alreadyestablished and validated.17,18 One pointwas given for each criterion met, for atotal score of 0 to 4, 5, or 6, depending onthe number of criteria required for eachplane (Tables 1 and 2). Then, with thepurpose of uniformity and simplicity,each score was converted to a score ofbetween 0 and 10. The sum of scores forthe 6 images for each type of examina-tion gave the final score greater than 60.
Subsequently, two examiners (V.B.and G.C.), who were blinded to both liveand OUS scores as well as to each other’sevaluations, reviewed and scored allimages. We finally obtained 2 scores foreach image taken from a volunteerand from simulation. We built ourdatabase by entering all scores for eachstudent, based both on volunteer and onthe simulator scores.
Statistical analyses were conductedusing the R software, version 2.0.0(www.r-project.org, Foundation forStatistical Computing, Vienna, Austria).We used the Raghunathan 1996(Raghunathan, Rosenthal, and Rubin’s[1996] modification of Pearson and

FIGURE 2Biometric and morphological planes for second-trimester US examination on OUS
Nine biometric and morphological planes required by the French national committee for prenatal ultrasound (Comite Technique d’Echographie) forsecond-trimester ultrasound examination as obtained on the obstetrical ultrasound simulator.9
OUS, obstetrical ultrasound simulator.
Chalouhi et al. Simulation to assess trainee’s proficiency with obstetrical ultrasound. Am J Obstet Gynecol 2016.
ajog.org OBSTETRICS Original Research
APRIL 2016 American Journal of Obstetrics & Gynecology 525.e3
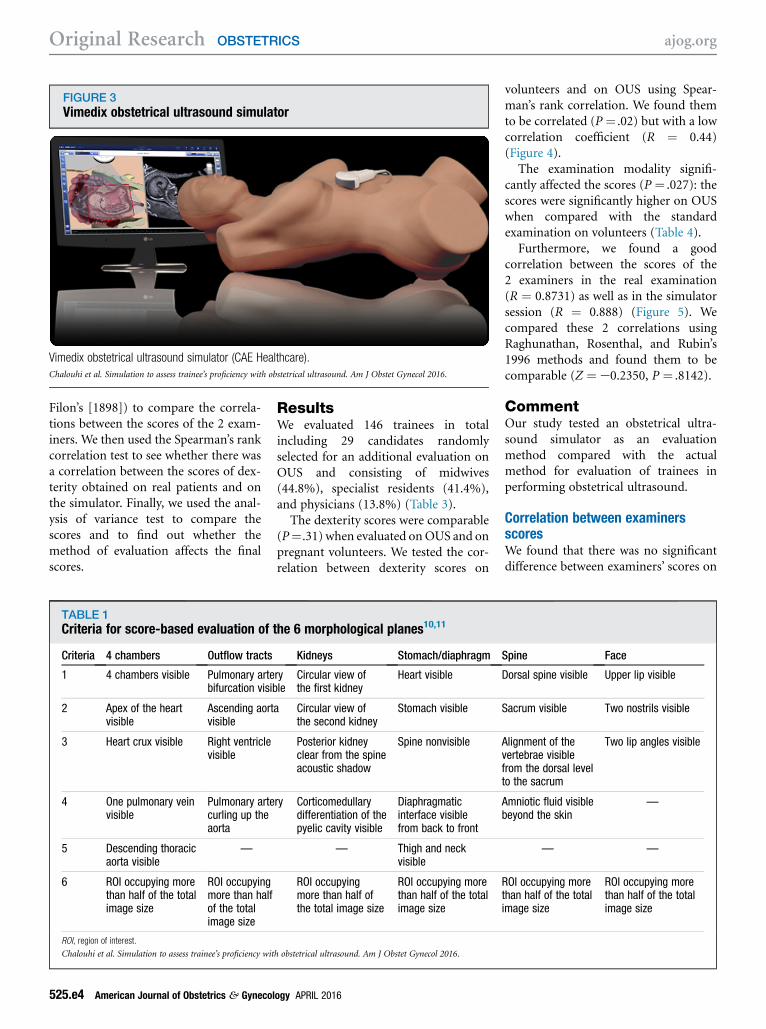
FIGURE 3Vimedix obstetrical ultrasound simulator
Vimedix obstetrical ultrasound simulator (CAE Healthcare).
Chalouhi et al. Simulation to assess trainee’s proficiency with obstetrical ultrasound. Am J Obstet Gynecol 2016.
Original Research OBSTETRICS ajog.org
Filon’s [1898]) to compare the correla-tions between the scores of the 2 exam-iners. We then used the Spearman’s rankcorrelation test to see whether there wasa correlation between the scores of dex-terity obtained on real patients and onthe simulator. Finally, we used the anal-ysis of variance test to compare thescores and to find out whether themethod of evaluation affects the finalscores.
TABLE 1Criteria for score-based evaluation of
Criteria 4 chambers Outflow tracts
1 4 chambers visible Pulmonary artebifurcation visib
2 Apex of the heartvisible
Ascending aortvisible
3 Heart crux visible Right ventriclevisible
4 One pulmonary veinvisible
Pulmonary artecurling up theaorta
5 Descending thoracicaorta visible
—
6 ROI occupying morethan half of the totalimage size
ROI occupyingmore than halfof the totalimage size
ROI, region of interest.
Chalouhi et al. Simulation to assess trainee’s proficiency wit
525.e4 American Journal of Obstetrics & Gynecol
ResultsWe evaluated 146 trainees in totalincluding 29 candidates randomlyselected for an additional evaluation onOUS and consisting of midwives(44.8%), specialist residents (41.4%),and physicians (13.8%) (Table 3).The dexterity scores were comparable
(P¼.31) when evaluated onOUS and onpregnant volunteers. We tested the cor-relation between dexterity scores on
the 6 morphological planes10,11
Kidneys Stomach/diaphragm
ryle
Circular view ofthe first kidney
Heart visible
a Circular view ofthe second kidney
Stomach visible
Posterior kidneyclear from the spineacoustic shadow
Spine nonvisible
ry Corticomedullarydifferentiation of thepyelic cavity visible
Diaphragmaticinterface visiblefrom back to front
— Thigh and neckvisible
ROI occupyingmore than half ofthe total image size
ROI occupying morethan half of the totalimage size
h obstetrical ultrasound. Am J Obstet Gynecol 2016.
ogy APRIL 2016
volunteers and on OUS using Spear-man’s rank correlation. We found themto be correlated (P ¼ .02) but with a lowcorrelation coefficient (R ¼ 0.44)(Figure 4).
The examination modality signifi-cantly affected the scores (P ¼ .027): thescores were significantly higher on OUSwhen compared with the standardexamination on volunteers (Table 4).
Furthermore, we found a goodcorrelation between the scores of the2 examiners in the real examination(R ¼ 0.8731) as well as in the simulatorsession (R ¼ 0.888) (Figure 5). Wecompared these 2 correlations usingRaghunathan, Rosenthal, and Rubin’s1996 methods and found them to becomparable (Z ¼ e0.2350, P ¼ .8142).
CommentOur study tested an obstetrical ultra-sound simulator as an evaluationmethod compared with the actualmethod for evaluation of trainees inperforming obstetrical ultrasound.
Correlation between examinersscoresWe found that there was no significantdifference between examiners’ scores on
Spine Face
Dorsal spine visible Upper lip visible
Sacrum visible Two nostrils visible
Alignment of thevertebrae visiblefrom the dorsal levelto the sacrum
Two lip angles visible
Amniotic fluid visiblebeyond the skin
—
— —
ROI occupying morethan half of the totalimage size
ROI occupying morethan half of the totalimage size
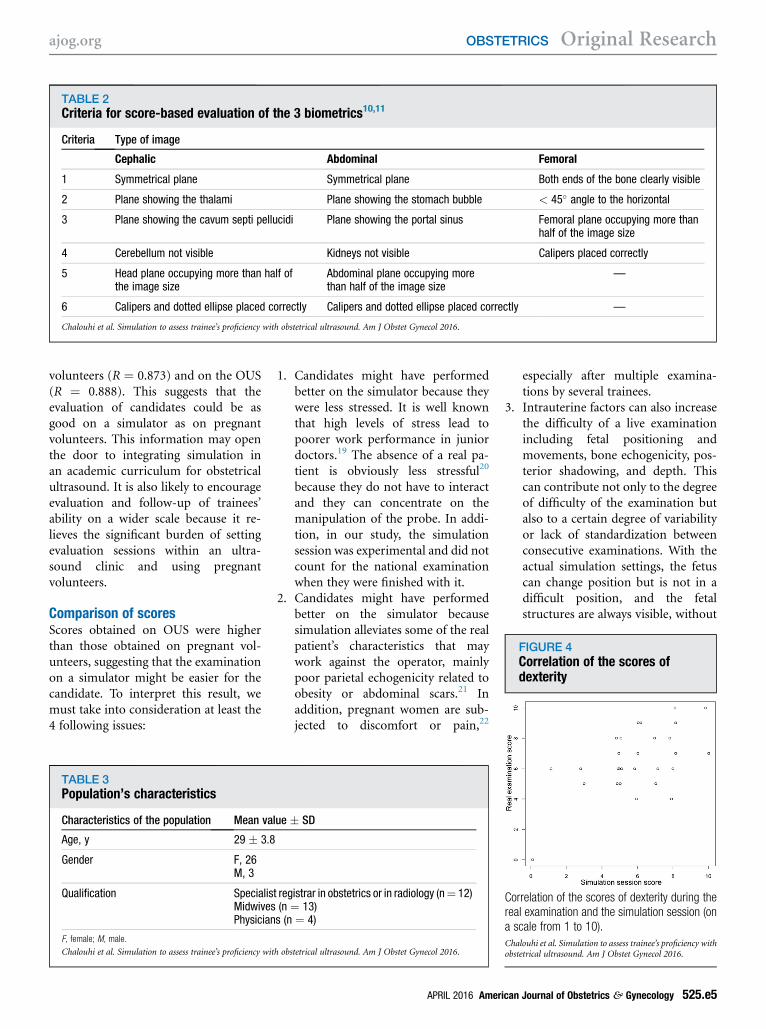
TABLE 2Criteria for score-based evaluation of the 3 biometrics10,11
Criteria Type of image
Cephalic Abdominal Femoral
1 Symmetrical plane Symmetrical plane Both ends of the bone clearly visible
2 Plane showing the thalami Plane showing the stomach bubble < 45� angle to the horizontal
3 Plane showing the cavum septi pellucidi Plane showing the portal sinus Femoral plane occupying more thanhalf of the image size
4 Cerebellum not visible Kidneys not visible Calipers placed correctly
5 Head plane occupying more than half ofthe image size
Abdominal plane occupying morethan half of the image size
—
6 Calipers and dotted ellipse placed correctly Calipers and dotted ellipse placed correctly —
Chalouhi et al. Simulation to assess trainee’s proficiency with obstetrical ultrasound. Am J Obstet Gynecol 2016.
FIGURE 4Correlation of the scores ofdexterity
ajog.org OBSTETRICS Original Research
volunteers (R ¼ 0.873) and on the OUS(R ¼ 0.888). This suggests that theevaluation of candidates could be asgood on a simulator as on pregnantvolunteers. This information may openthe door to integrating simulation inan academic curriculum for obstetricalultrasound. It is also likely to encourageevaluation and follow-up of trainees’ability on a wider scale because it re-lieves the significant burden of settingevaluation sessions within an ultra-sound clinic and using pregnantvolunteers.
Comparison of scoresScores obtained on OUS were higherthan those obtained on pregnant vol-unteers, suggesting that the examinationon a simulator might be easier for thecandidate. To interpret this result, wemust take into consideration at least the4 following issues:
TABLE 3Population’s characteristics
Characteristics of the population Mean va
Age, y 29 � 3.8
Gender F, 26M, 3
Qualification SpecialisMidwivesPhysician
F, female; M, male.
Chalouhi et al. Simulation to assess trainee’s proficiency wit
1. Candidates might have performedbetter on the simulator because theywere less stressed. It is well knownthat high levels of stress lead topoorer work performance in juniordoctors.19 The absence of a real pa-tient is obviously less stressful20
because they do not have to interactand they can concentrate on themanipulation of the probe. In addi-tion, in our study, the simulationsession was experimental and did notcount for the national examinationwhen they were finished with it.
2. Candidates might have performedbetter on the simulator becausesimulation alleviates some of the realpatient’s characteristics that maywork against the operator, mainlypoor parietal echogenicity related toobesity or abdominal scars.21 Inaddition, pregnant women are sub-jected to discomfort or pain,22
lue � SD
t registrar in obstetrics or in radiology (n¼ 12)(n ¼ 13)s (n ¼ 4)
h obstetrical ultrasound. Am J Obstet Gynecol 2016.
APRIL 2016 Ameri
especially after multiple examina-tions by several trainees.
3. Intrauterine factors can also increasethe difficulty of a live examinationincluding fetal positioning andmovements, bone echogenicity, pos-terior shadowing, and depth. Thiscan contribute not only to the degreeof difficulty of the examination butalso to a certain degree of variabilityor lack of standardization betweenconsecutive examinations. With theactual simulation settings, the fetuscan change position but is not in adifficult position, and the fetalstructures are always visible, without
Correlation of the scores of dexterity during thereal examination and the simulation session (ona scale from 1 to 10).
Chalouhi et al. Simulation to assess trainee’s proficiency withobstetrical ultrasound. Am J Obstet Gynecol 2016.
can Journal of Obstetrics & Gynecology 525.e5
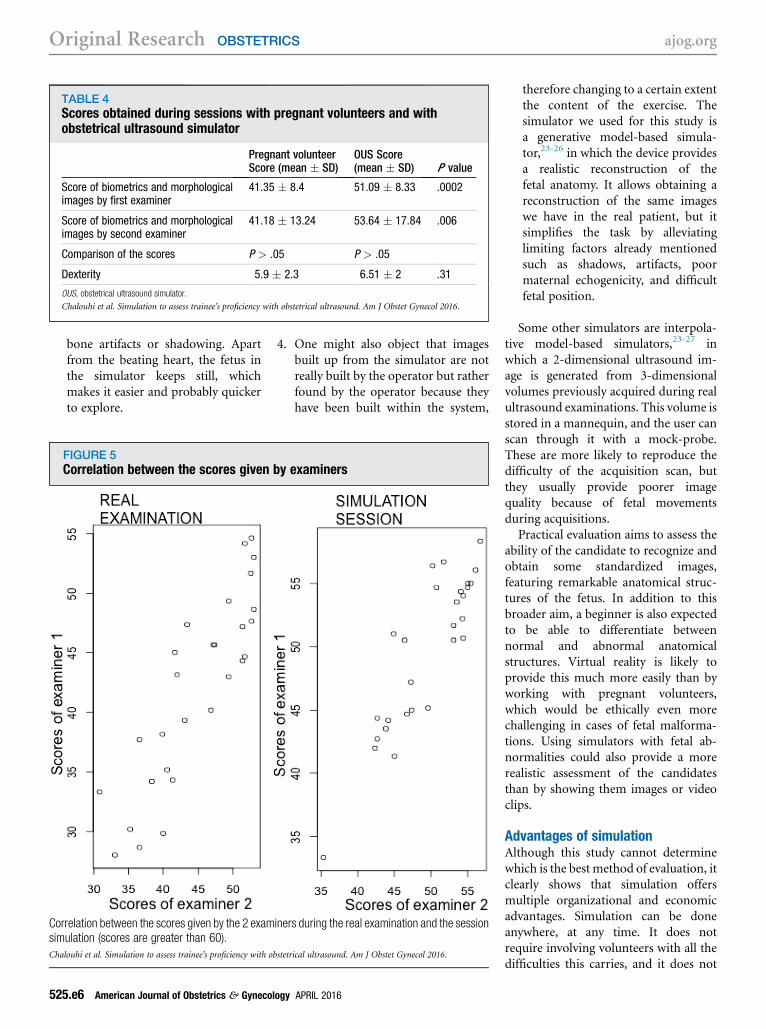
TABLE 4Scores obtained during sessions with pregnant volunteers and withobstetrical ultrasound simulator
Pregnant volunteerScore (mean � SD)
OUS Score(mean � SD) P value
Score of biometrics and morphologicalimages by first examiner
41.35 � 8.4 51.09 � 8.33 .0002
Score of biometrics and morphologicalimages by second examiner
41.18 � 13.24 53.64 � 17.84 .006
Comparison of the scores P > .05 P > .05
Dexterity 5.9 � 2.3 6.51 � 2 .31
OUS, obstetrical ultrasound simulator.
Chalouhi et al. Simulation to assess trainee’s proficiency with obstetrical ultrasound. Am J Obstet Gynecol 2016.
Original Research OBSTETRICS ajog.org
bone artifacts or shadowing. Apartfrom the beating heart, the fetus inthe simulator keeps still, whichmakes it easier and probably quickerto explore.
FIGURE 5Correlation between the scores given
Correlation between the scores given by the 2 examsimulation (scores are greater than 60).
Chalouhi et al. Simulation to assess trainee’s proficiency with o
525.e6 American Journal of Obstetrics & Gynecol
4. One might also object that imagesbuilt up from the simulator are notreally built by the operator but ratherfound by the operator because theyhave been built within the system,
by examiners
iners during the real examination and the session
bstetrical ultrasound. Am J Obstet Gynecol 2016.
ogy APRIL 2016
therefore changing to a certain extentthe content of the exercise. Thesimulator we used for this study isa generative model-based simula-tor,23-26 in which the device providesa realistic reconstruction of thefetal anatomy. It allows obtaining areconstruction of the same imageswe have in the real patient, but itsimplifies the task by alleviatinglimiting factors already mentionedsuch as shadows, artifacts, poormaternal echogenicity, and difficultfetal position.
Some other simulators are interpola-tive model-based simulators,23-27 inwhich a 2-dimensional ultrasound im-age is generated from 3-dimensionalvolumes previously acquired during realultrasound examinations. This volume isstored in a mannequin, and the user canscan through it with a mock-probe.These are more likely to reproduce thedifficulty of the acquisition scan, butthey usually provide poorer imagequality because of fetal movementsduring acquisitions.
Practical evaluation aims to assess theability of the candidate to recognize andobtain some standardized images,featuring remarkable anatomical struc-tures of the fetus. In addition to thisbroader aim, a beginner is also expectedto be able to differentiate betweennormal and abnormal anatomicalstructures. Virtual reality is likely toprovide this much more easily than byworking with pregnant volunteers,which would be ethically even morechallenging in cases of fetal malforma-tions. Using simulators with fetal ab-normalities could also provide a morerealistic assessment of the candidatesthan by showing them images or videoclips.
Advantages of simulationAlthough this study cannot determinewhich is the best method of evaluation, itclearly shows that simulation offersmultiple organizational and economicadvantages. Simulation can be doneanywhere, at any time. It does notrequire involving volunteers with all thedifficulties this carries, and it does not

ajog.org OBSTETRICS Original Research
interfere with the normal activity of anultrasound unit. The cost-effectivenessof such a shift in practice still must beevaluated, but it is obvious that it willbring a significant decrease in costs forthe certifying institutions.
Dexterity evaluationWe also analyzed the dexterity param-eter, which was subjectively evaluatedin real time, during the examinationfor both volunteer and OUS sessionsby 2 different examiners. It gives anidea of the candidate’s ability to handleand manipulate the probe as wellas on the ergonomy at obtaining therequested images and measurements.We observed a significant correlationbetween the scores given in the 2different settings (P ¼ .02; correlationcoefficient 0.43). The limited learningtime (10 minutes) each student wasgiven to learn how to use the simulatormight have been a factor making thedexterity correlation coefficient low.Although it is difficult to transformthis parameter into a more objectiveone during live sessions, some keyparameters can be objectively quanti-fied by the simulator, including ex-amination time, number of probestops, and time stops as well as totaldistance screened by the probe.
Human factorInteraction between the operator and thepatient is an important factor of everymedical examination that cannot betested by the OUS itself. This would needto be addressed specifically with rolegames.28,29 However, interaction assess-ment during a practical examination ona pregnant volunteer is currently limi-ted because of the specific conditionson which the operator is being evalua-ted and is subjected to examination-related stress. Also, the pregnantvolunteer has undergone a previousdetailed examination that was found tobe normal.
ConclusionThis study suggests that evaluatingtrainees on a simulator followingstructured theoretical and practicaltraining is comparable with doing the
same evaluation on pregnant volun-teers. This evaluation technique hasmany organizational and economic ad-vantages over the current method ofevaluation.Some limitations of the simulator may
be the absence of fetal movements dur-ing the examination along with theabsence of interaction between thecandidate and the patient. Such limita-tions could be resolved by improving thequality of simulation systems.Simulation answers directly the
10th point of the ultrasound researchagenda published by the Fetal ImagingJoint Workshop30 because it helps inimproving teaching and education aswell as identifying metrics to measurequality in ultrasonography. This methodof assessment could also be more suit-able for continuous self-assessment inmaintaining competency and inacquiring new skills by using variousmodules and levels of technicaldifficulties.31 n
References
1. Baer RJ, Norton ME, Shaw GM, et al. Riskof selected structural abnormalities in infantsafter increased nuchal translucency measure-ment. Am J Obstet Gynecol 2014;211:675.e1-19.2. Salomon LJ, Bernard JP, Millischer AE, et al.MRI and ultrasound fusion imaging for prenataldiagnosis. Am J Obstet Gynecol 2013;209:148.e1-9.3. Ehrenberg-Buchner S, Stapf AM,BermanDR,et al. Fetal lung lesions: can we start to breatheeasier? Am J Obstet Gynecol 2013;208:151.e1-7.4. Hibbeln JF, Shors SM, Byrd SE. MRI: is therea role in obstetrics? Clin Obstet Gynecol2012;55:352-66.5. Hall R, Ogburn T, Rogers RG. Teaching andevaluating ultrasound skill attainment:competency-based resident ultrasound trainingfor AIUM accreditation. Obstet Gynecol ClinNorth Am 2006;33:305-23.6. Heinzow HS, Friederichs H, Lenz P, et al.Teaching ultrasound in a curricular courseaccording to certified EFSUMB standardsduring undergraduate medical education:a prospective study. BMC Med Educ 2013;13:84.7. Friedrich MJ. Practice makes perfect: risk-free medical training with patient simulators.JAMA 2002;288(2808):2811-2.8. Vogell A, Gujral H, Wright KN, Wright VW,Ruthazer R. Impact of a robotic simulation pro-gram on resident surgical performance. Am JObstet Gynecol 2015;213:874-5.
APRIL 2016 Ameri
9. DeStephano CC, Chou B, Patel S, Slattery R,Hueppchen N. A randomized controlled trial ofbirth simulation for medical students. AmJ Obstet Gynecol 2015;213:91.e1-7.10. Connor RS, Dizon AM, Kimball KJ. Loopelectrosurgical excision procedure: an effec-tive, inexpensive, and durable teachingmodel. Am J Obstet Gynecol 2014;211:706.e1-3.11. Hoffman MS. Simulation of robotic hyster-ectomy utilizing the porcine model. Am J ObstetGynecol 2012;206:523.e1-2.12. Programme National pour la Sécuritédes Patients (PNSP) Site Santé du Mnistère desAffaires Sociales et de la Santé Mnistèredes Affaires Sociales et de la Santé 2013.Available from: http://www.sante.gouv.fr/programme-national-pour-la-securite-des-patients-pnsp.html. Accessed July 19, 2014.13. Issenberg SB, Scalese RJ. Simulation inhealth care education. Perspect Biol Med2008;51:31-46.14.Wilford A, Doyle JT. Integrating simulationtraining into the nursing curriculum. Br J Nurs2006;15:926-30.15. Français Collège National des Gynéco-logues Obstétriciens Français. Rapport duComité National Technique de l’Échographie deDépistage Prénatal; 2005. Available at: http://www.cngof.asso.fr/D_TELE/100513_rapport_echo.pdf. Accessed July 15, 2015.16. Rapport du comité technique de l’échogra-phie de dépistage prénatal (www.cfef.org2005).Available from: https://www.cfef.org/archives/lettres/DocusCTE/01.html. Accessed July 15,2014.17. Salomon LJ, Alfirevic Z, Berghella V,et al. Practice guidelines for performance ofthe routine mid-trimester fetal ultrasoundscan. Ultrasound Obstet Gynecol 2011;37:116-26.18. Salomon LJ, Winer N, Bernard JP, Ville Y.A score-based method for quality control offetal images at routine second-trimester ultra-sound examination. Prenat Diagn 2008;28:822-7.19.Williams S, Dale J, Glucksman E,Wellesley A. Senior house officers’ work relatedstressors, psychological distress, and confi-dence in performing clinical tasks in accidentand emergency: a questionnaire study. BMJ1997;314:713-8.20. Heer IM, Middendorf K, Muller-Egloff S,Dugas M, Strauss A. Ultrasound training: thevirtual patient. Ultrasound Obstet Gynecol2004;24:440-4.21. Benacerraf B. The use of obstetrical ultra-sound in the obese gravida. Semin Perinatol2013;37:345-7.22. Kinsella SM, Lohmann G. Supine hypoten-sive syndrome. Obstet Gynecol 1994;83:774-88.23. Konge L, Albrecht-Beste E, Nielsen MB.Virtual-reality simulation-based training in ultra-sound. Ultraschall Medizin 2014;35:95-7.24. Lewiss RE, Hoffmann B, Beaulieu Y,Phelan MB. Point-of-care ultrasound
can Journal of Obstetrics & Gynecology 525.e7

Original Research OBSTETRICS ajog.org
education: the increasing role of simulationand multimedia resources. J Ultrasound Med2014;33:27-32.25. Make learning ultrasound faster and easier.Available at: http://caehealthcare.com/eng/ultrasound-simulators/vimedix. Accessed July15, 2015.26. ScanTrainer. Available at: http://www.medaphor.com/scantrainer/training/. AccessedJuly 15, 2015.27. Schallware Ultrasound Simulator. Availableat: http://www.schallware.com/. Accessed July15, 2015.28. de laCroixA,Skelton J. The simulationgame:an analysis of interactions between students andsimulated patients. Med Educ 2013;47:49-58.29. Bouter S, van Weel-Baumgarten E,Bolhuis S. Construction and validation of theNijmegen Evaluation of the Simulated Patient
525.e8 American Journal of Obstetrics & Gynecol
(NESP): assessing simulated patients’ ability torole-play and provide feedback to students.Acad Med 2013;88:253-9.30. Reddy UM, Abuhamad AZ, Levine D,Saade GR; Fetal Imaging Workshop InvitedParticipants. Fetal imaging: executive summaryof a Joint Eunice Kennedy Shriver NationalInstitute of Child Health and Human Develop-ment, Society for Maternal-Fetal Medicine,American Institute of Ultrasound in Medicine,American College of Obstetricians and Gyne-cologists, American College of Radiology,Society for Pediatric Radiology, and Society ofRadiologists in Ultrasound Fetal ImagingWorkshop. Am J Obstet Gynecol 2014;210:387-97.31. Ehrlinger J, Johnson K, Banner M,Dunning D, Kruger J. Why the unskilledare unaware: further explorations of (absent)
ogy APRIL 2016
self-insight among the incompetent. OrganBehav Hum Decis Proc 2008;105:98-121.
Author and article informationFrom the Department of Obstetrics and Fetal Medicine,
Necker-Enfants-Malades Hospital, APHP, Universite Paris
Descartes, Sorbonne Paris Cite, Paris, France (Drs Cha-
louhi, Gueneuc, Stirnemann, and Ville and Ms Houssin),
Department of Women and Children Health, Universita
degli Studi di Padova, Padova, Italy (Dr Bernardi), and
SimECHOle, Ecole de simulation pour l’enseignement et
le perfectionnement en echographie (all authors), Paris,
France.
Received Aug. 4, 2015; revised Oct. 6, 2015;
accepted Oct. 29, 2015.
The authors report no conflict of interest.
Corresponding author: Gihad E. Chalouhi, MD. gihad.