Embed Size (px)
Citation preview

Fetal cardiovascular parameters for the
prediction of postnatal cardiovascular risk
in intrauterine growth-restriction?
Fàtima Crispi, Monica Cruz-Lemini, Brenda Valenzuela-Alcaraz, Francesc Figueras, Olga Gómez, Marta Sitges, Bart Bijnens, Eduard Gratacós
Department of Maternal-Fetal Medicine, Hospital Clinic; Fetal Medicine Research Center, IDIBAPS; Barcelona, Spain
ICREA, Universitat Pompeu Fabra, Barcelona, Spain
Cardiology Department, Thorax Clinic Institute, Hospital Clinic,, Barcelona, Spain
17th International Conference on Prenatal Diagnosis and Therapy
Lisbon, June 2013
No disclosure
www.medicinafetalbarcelona.org
© w
ww.medicin
afeta
lbarc
elona.org

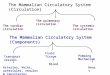
IUGR Fetus Low BW Child CV
Disease Adult
Myocardial infartion
Hypertension
Diabetes/Obesity
introduction
Fetal life Early life Old age Childhood Maturity
IMPACT OF
ENVIRONMENT
OPPORTUNITY
FOR
CORRECTION
How do we choose who to follow up into
childhood?
Barker BMJ 1995, Hecher Circulation 1995, Crispi AJOG 2008, Crispi Circulation 2010 © w
ww.medicin
afeta
lbarc
elona.org

Fetus
Myocardial Performance Index
M-mode
Tissue Doppler
6mo Child 5yr Child
Blood Pressure
Tissue Doppler
Sphericity Index
Cruz-Lemini UOG 2013.
Comas, AJOG 2010.
Comas, AJOG 2011.
Crispi, AJOG 2008.
Cruz-Martínez, UOG 2011.
Crispi, Circulation 2010.
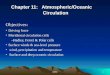
IUGR defined as EFW/birthweight <10th centile
Control
n=100
IUGR
n=100
Conventional Doppler
Fetal
Echocardiography
Control
n=100
IUGR
n=100
Blood Pressure
Aortic IMT
Logistic Regression CV RISK
To evaluate whether fetal echocardiography has a value for the
prediction of postnatal cardiovascular outcome in IUGR
© w
ww.medicin
afeta
lbarc
elona.org

Controls
n= 100
IUGR
n= 100 p
Fetal Parameters
Umbilical artery PI (z-score) 0.1 ± 0.6 0.7 ± 1.4 <0.001
Mean uterine artery PI (z-score) -0.7 ± 1.3 0.7 ± 1.9 0.002
Cerebroplacental ratio (z-score) 0.1 ± 1.3 -0.9 ± 1.6 <0.001
Delivery Data
Gestational age at delivery
(weeks) 39.9 ± 1.2 37.3 ± 3.5 <0.001
Birthweight centile 45 ± 23 3 ± 3 <0.001
Child Demographics
Corrected age at scan (months) 6.5 ± 0.7 6.5 ± 0.7 0.916
Height (cm) 68 ± 2 65 ± 3 <0.001
Weight (g) 7819 ± 767 6892 ± 956 <0.001
Body mass index (kg/m2) 16.9 ± 1.6 16.3 ± 1.8 0.051
PI, pulsatility index; IUGR, intrauterine growth restriction.
Doppler measurements expressed in z-scores, mean ± SD. Differences estimated by Student’s t test.
results Descriptive Data
IUGR: 25% abnormal
postnatal CV outcome (BP >p95 + aIMT >p75)
© w
ww.medicin
afeta
lbarc
elona.org

OR p
Standard criteria
Gestational age at delivery 1.2 (1.0 – 1.4) 0.055
Birthweight centile 1.2 (0.9 – 1.4) 0.134
Mean uterine artery PI 1.4 (0.9 – 1.9) 0.052
Umbilical artery PI 1.8 (1.2 – 2.6) 0.003
Cerebroplacental ratio 2.2 (1.4 – 3.5) 0.001
Ductus venosus PI 2.0 (1.2 – 3.4) 0.007
Aortic isthmus PI 1.0 (0.9 – 1.1) 0.079
Fetal echocardiographic parameters
Right ejection fraction 0.9 (0.9 – 1.1) 0.918
Isovolumetric relaxation time 2.1 (1.2 – 3.7) 0.008
TAPSE 11.4 (3.6 – 35.7) <0.001
Tricuspid S’ 7.5 (1.4 – 50) 0.041
Right sphericity index 9.2 (4.3 – 19.9) <0.001
Right ventricular wall (adjusted) 4.8 (2.7 – 8.5) <0.001
PI, pulsatility index; TAPSE, tricuspid annular plane systolic excursion;
S’, peak systolic velocity. Right wall adjusted by cardiac transverse diameter
results
Univariate Regressions Outcome: MBP>p95 + aIMT>p95
25%
© w
ww.medicin
afeta
lbarc
elona.org

Outcome: MBP>p95 + aIMT>p95
25% results
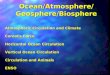
Conventional parameters: poor prediction of postnatal CV risk
GA at delivery AUC: 0.51 (95% CI 0.42 – 0.60, p=0.070)
Birthweight centile AUC: 0.60 (95% CI 0.51 – 0.68, p=0.066)
Umbilical artery PI AUC: 0.67 (95% CI 0.59 – 0.75, p=0.070)
GA at delivery
BW Centile
Umbilical artery PI
0 20 40 60 80 100
100
80
60
40
20
0
100-Specificity
Se
nsitiv
ity
© w
ww.medicin
afeta
lbarc
elona.org

OR p
Standard criteria
Gestational age at delivery 1.2 (1.0 – 1.4) 0.055
Birthweight centile 1.2 (0.9 – 1.4) 0.134
Mean uterine artery PI 1.4 (0.9 – 1.9) 0.052
Umbilical artery PI 1.8 (1.2 – 2.6) 0.003
Cerebroplacental ratio 2.2 (1.4 – 3.5) 0.001
Ductus venosus PI 2.0 (1.2 – 3.4) 0.007
Aortic isthmus PI 1.0 (0.9 – 1.1) 0.079
Fetal echocardiographic parameters
Right ejection fraction 0.9 (0.9 – 1.1) 0.918
Isovolumetric relaxation time 2.1 (1.2 – 3.7) 0.008
TAPSE 11.4 (3.6 – 35.7) <0.001
Tricuspid S’ 7.5 (1.4 – 50) 0.041
Right sphericity index 9.2 (4.3 – 19.9) <0.001
Right ventricular wall (adjusted) 4.8 (2.7 – 8.5) <0.001
PI, pulsatility index; TAPSE, tricuspid annular plane systolic excursion;
S’, peak systolic velocity. Right wall adjusted by cardiac transverse diameter
results
Univariate Regressions Outcome: MBP>p95 + aIMT>p95
25%
© w
ww.medicin
afeta
lbarc
elona.org

Fetal Echocardiographic Parameters
results
Outcome: MBP>p95 + aIMT>p95
25%
sphericity index
OR 5.6 (2.6-12.2)
OR 2.4 (1.4-3.9)
isovolumic relaxation time
aorta
E A
TAPSE
OR 10.2 (4.2-36)
© w
ww.medicin
afeta
lbarc
elona.org

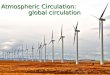
Composite CV Score AUC: 0.87 (95% CI 0.79 – 0.93, p<0.001)
Sensitivity 90%, Specificity 77%
Gestational Age at Birth AUC: 0.50
(95% CI 0.41 – 0.59, p=0.071)
Birthweight AUC: 0.59
(95% CI 0.50 – 0.68, p=0.066)
Umbilical Artery AUC: 0.67
(95% CI 0.59 – 0.76, p=0.070) 0 20 40 60 80 100
100
80
60
40
20
0
100-Specificity
Se
nsitiv
ity
results
Cardiovascular Score: TAPSE + CPR + RSI + IRT
Outcome: MBP>p95 + aIMT>p95
n = 25%
1.907 + (TAPSEz*-0.589) + (CPRz*-0.286) + (RSI*-1.938) + (IRTz*0.342)
≥ 0.1253
© w
ww.medicin
afeta
lbarc
elona.org

conclusions
• Fetal echocardiographic parameters help identifying a high-risk
group within the IUGR fetuses, which could be targeted for
early screening of blood pressure, as well as for promoting
healthy diet and physical exercise.
• Larger studies are warranted to assess clinical utility of
algorithms based on fetal echocardiography to select IUGR
cases with higher cardiovascular risk later in life.
THANK YOU
© w
ww.medicin
afeta
lbarc
elona.org