Embed Size (px)
Citation preview
Reconstruction of Contracted Eyelids:Outcome of Different Procedures of
Surgery
INTRODUCTION:The eyelids are commonly involved in many typesof facial injury. It results in cosmetic as well asfunctional impairments. Their prompt reconstructionis necessary. A lesion confined to eyelids is seen inonly few patients. Scar contractures of the upperand lower or both eyelids, expose the cornea, whichis frequently found in burns of the face. This canlead to severe exposure keratitis with permanentimpairment or even loss of vision.1 In Pakistan theincreasing ratio of automobile accident, lack of safetymeasures for house wives and cooks, unchecked
Correspondence:Dr. Nisar Ahmed MangiDepartment of Plastic & Reconstructive SurgeryJinnah Post Graduate Medical Centre, KarachiE mail: [email protected]
fits in epileptic patients and criminal assault are majorcauses of this disaster.
The existence of records of eyelid surgery dates asfar back as the beginning of the 10th century whensurgeons Avicenna and Ibn Roshd in Arabia,expressed the difficulty in vision due to the excessskin folds in the upper eyelid and wanted to excisethem. The evolution of eyelid surgery since that timeand especially over the last century, has broughtabout considerable sophistication which is based onimproved surgical and anatomical knowledge.2
The first century Aulus Cornelius Celsus, wasprobably the first to comment on the excision of theskin of the upper eyelids.3 In 1809 Van Greafeconstructed lower eyelid with a cheek rotation flap.His method was modified by Fricke who introduceda procedure for both upper and lower l ids
A B S T R A C T
Objective
Study design Descriptive case series.
Place &Duration ofstudy
Methodology
Key words
Conclusion
R e s u l t s
Department of Plastic & Reconstructive Surgery at Jinnah Post Graduate Medical Centre(JPMC) Karachi, from 2003 to 2008.
Medium thickness skin graft is preferred in up to ¾th loss of eyelid thickness and primaryclosure is appropriate where up to 25% loss is found.
Eyelid contractures, Excision and release of contractures, Reconstruction of lids.
All patients admitted with eyelids contractures were included. A detailed history was taken.Examination of eyes were done, which included visual acuity and near vision test. Test fortear formation, staining of the cornea for any ulcer or rupture of cornea due to injury, werealso performed. Priority was given to vision restoration. Culture and sensitivity of dischargefrom eye, if any, was also done. Patients were subjected to different surgical procedures.
To evaluate the different procedures of the reconstruction of post traumatic eyelidscontractures with regards to the functional and cosmetic results.
There were total of 30 patients with 16 males and 14 females. The age of the patientsranged from 7 years to 58 years. Excision of lesion and primary closure was done in twopatients (6.6%), rotation advancement flap in two (6.6%), release and medium thicknessgrafting in thirteen (43.3%), release and Wolfe grafting in eight patients (26.7%) and Zplasty in five (16.7%) cases.
ORIGINAL ARTICLE
Nisar Ahmed Mangi, Syed Arif Hussain
170Journal of Surgery Pakistan (International) 16 (4) October - December 2011
reconstruction, using zygomatic and temporal skinflaps. Many surgeons of the 19th century, tried touse the technique of applying skin grafts which wasintroduced by Reverdin.4 Reconstruction of eyelidscan be done by many techniques including localflaps including rotation flaps, transposition flaps,and islands flaps, free grafts, split thickness skingrafts (Thiersch), full thickness grafts (Wolfe) andmucous membrane from nasal or buccal mucosa.5
In reconstruct ive surgery of eyel ids al l therequirements should be fulfilled to achieve goodfunctional and cosmetic results. This is only possiblewhen skin, mucous and membrane are in rightproportion. Composite tissues should be soft andpliable. Contractures as a result of scar should beavoided. Pliability is possible when the skin of theeyelid is used. This study was conducted todocument experience of repair of eyelids contractureswith various techniques.
METHODOLOGY:A descriptive case series was performed in theDepartment of Plastic & Reconstructive Surgery atJinnah Post Graduate Medical Centre, Karachi from2003 to 2008. All patients with eyelids contracturesdue to any cause were included. A detailed historywas taken. Examination of eyes was done in allcases. Visual acuity and near vision were assessed.Test for tear formation was also done. Staining ofthe cornea for any ulcer or rupture of cornea due toinjury was also sought. Culture and sensitivity ofdischarge from eye, if any, was also done. Patientswere subjected to different surgical proceduresdepending upon the extent and type of contractures.
The results of reconstruction were divided intocosmetic results, functional results, lacrimal drainageand blinking. Results were marked as good,satisfactory and unsatisfactory. Complications werecategorized into early and late groups. Follow upwas done on regular basis in all cases. Descriptivestat is t ics were per formed. Frequency andpercentages were computed for different variables.
RESULTS:There were thirty patients with post traumaticcontractures of eyelids in this series. There were 16females and 14 males. The age ranged from 7 yearsto 58 years with the mean age of 24.7 years. Majorityof the cases were due to thermal burns (n =15).Chemical and mechanical injuries were the causein other cases.
In 13 patients the contractures were released andsplit thickness graft was applied. Wolfe grafting wasdone in 8 patients (table I). Cosmetically good results
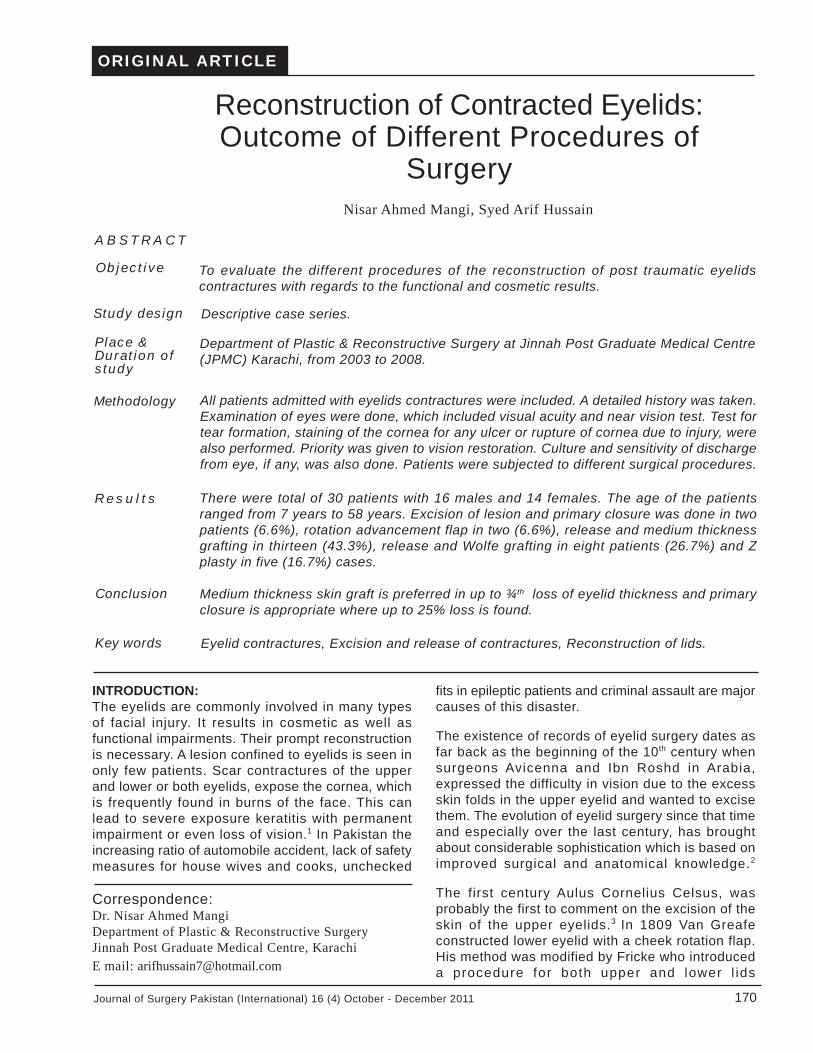
were found in 10 cases and satisfactory in 19patients. In one case result remained unsatisfactory.Functionally 15 patients had good outcome (Fig-I & II). In 13 cases satisfactory function was achievedwhile two were unsatisfactory. The lacrimal drainagein 15 cases was good and satisfactory in others.The blinking was good in 15, satisfactory in 14 casesand unsatisfactory in one case.
Complications were divided into early and late. Inearly complications 12 patients had infection, 3
171 Journal of Surgery Pakistan (International) 16 (4) October - December 2011
Fig II B Postoperative view
Fig II A Contracture of Right Lower Eyelid.
Fig I A Contracture of Left Lower Eyelid.
Fig I B Postoperative view
Reconstruction of Contracted Eyelids

172Journal of Surgery Pakistan (International) 16 (4) October - December 2011
patients had epiphora along with infection. Twocases had infection, epiphora and partial ptosis.Nine pat ients had no compl icat ions. Latecomplications were noticed at the 3 months and 6months intervals, which included conjunctivitis,epiphora, keratitis and contraction of the grafts(table II).
DISCUSSION:In severely burnt male patients, when suitable donorsite is not available, the prepuce can provideexcellent material for this purpose. It has got asuitable texture and gradation of color.6 In olderpatients with a natural surplus of skin in the upperand lower eyelids and in the area to the outercanthus, it is rarely necessary to look for donor skinelsewhere. In those patients the use of transpositionflaps from the forehead or cheek. Although one mustknow that these flaps may not settle in to the eyelidswell, reducing its pliability.7 Result of surgery is goodwhen perfect symmetry is obtained. In two cases ofthis study rotation advancement flap technique wasused. The results were cosmetically unacceptablebecause of bulky tissue. Later debulking was donefor better appearance.
Reconstruction of upper and lower l ids areconsidered separately as they are some what
different in structure, but Mustarde opines that thisdivision is useless.7 The techniques of reconstructionare virtually inter-changeable. Complete recons-truction of upper lid with the lower lid may besatisfactory in the hands of an experienced surgeon.The reverse however is unacceptable.8 The bestresults are achieved by local flaps. In such situationsskin used resembles quality and color of the defectmore closely than any other tissue. In 13 patientsof present series following release of contracturemedium thickness skin grafting was done. In uppereyelid surgery the outcome was good but in somecases re-grafting was done for lower eyelid. In 8cases where full thickness grafting of lower eyelidwas done results were acceptable.
Main sources of rotation flaps are cheek, the glabellaand forehead.9 With zygomatic cheek flap whenadequate undermining and mobilization done, adefect of a length of the palpebral fissure will easilybe covered.10 Transposition flap may be used toremove the position of eye lashes, eye brows orcanthi. Two transposition flaps, designed as Z-plasty are extremely useful in releasing contracturesor lengthening and changing the direction ofunsatisfactory scars.11 Furnas described island flapof skin and soft tissues of naso-jugal fold, based onsuperior end of angular artery. Disadvantage of this
Table I: Surgical Procedures
Excision and Primary Closure
Management Frequency Percentage
02 6.6%
Rotation Advancement Flap 02 6.6%
Release and Medium Thickness Graft 13 43.3%
Release and Wolfe Graft 08 26.7%
Z-Plasty 05 16.7%
Total 30 100.0%
Table II: Late Complications
Complications At 3 Months At 6 Months
Conjunctivitis10
20
09
21
Epiphora08 04
22 26
Keratitis07 07
23 23
Contracture of Graft03 13
27 17
Nisar Ahmed Mangi, Syed Arif Hussain
Reconstruction of Contracted Eyelids
173 Journal of Surgery Pakistan (International) 16 (4) October - December 2011
Disadvantage of this procedure is the need to trimthe bulkiness of flap in subsequent stages.4 Splitthickness grafts contract and are not durable ascompared to full thickness graft.12
Although medium thick graft (0.014-0.016 inch) isideal for upper eyelid,13 for conjunctival graft someauthorities recommend buccal mucosa in comparisonto nasal mucosa, because of easy approach.14 Insome cases mucosal graft from hard palate can beused.15 When source of injury is burn, diagnosis ofdegree of burn is important. First degree requirescleaning and application of sterile saline with goodantibiotic packs every 3 hours during day for twodays. In 2nd degree, the treatment is same exceptvesicle should be opened and dead epitheliumremoved. 3 rd degree need grafting and otherprocedures of reconstruction. In most cases ofpresent series conjunctiva was not involved thusbucca l o r nasa l mucosa was no t used .
In reconstruction of post traumatic eyelids specialattention should be given to achieve good functionaland aesthetic goals. The functional aspect isconsidered successful when all the factors areeliminated which cause lagophthalmos, ectropionand entropion or aesthetic aspect. There should beno difference in length and width of palpebral fissure.Color matching and thickness of the lid should beappropriate.
CONCLUSIONS:Medium thickness skin grafting is ideal for an eyelidreconstruction when there is loss of more than 75%.Rotation advancement flap with undercover of nasalor buccal mucosa is preferred in such cases. In lessthan 25% loss of lid primary repair is advised.
REFERENCES:
1. Grabosh A, Weyer F, Gruhl L, Bruck JC.Repair of upper eyelid by means of prepuceaf ter severe burn . Ann P las t Surg1991;26:427-30.
2. Mahoffey PJ, Wallac AF. Blindness followingcosmetic blepharoplasty. Br J Plast Surg1986;39:213-21.
3. Katzen LB. The history of cosmeticocuoplastic surgery Putterman M (Editor) 1st
Edition Graune and Stratton New York.1982;2-9.
4. B h a t t D L , G a y l o r D C , L e e R C .Rhambdomylosis due to pulsed electrical
fields. Plast. Recons Surg 1990;86:1-11.
5. Parkash S. The use of prepeutial skin toreplace conjunctiva and to correct ectropionBr J Plast Surg 1983;35:206-08.
6. Vander Meulen JC. The use of mucosa linedflaps in eyel id reconstruction. A newapproach. Plast Reconst Surg 1982;70:139-246.
7. Mustarde JC. Reconstruction of eyelids. AnnPlast Surg 1983;11:149-69.
8. Feldman JJ. Facial burn in plastic surgery.Mc-Carthy JG (Editor) W.B Saunder ’scompany. Phi ladelphia 1990:2153-36.
9. Duke ES. Diseases of l ids. ParsonsDiseases of Eye 14th edition Churchil livingstone, London 1964: 487-509.
10. Hall RMJ. The eyelids and reconstructivesurgery. Stellard eye surgery. 7 th edition,edited by M.J. Roper Hall. Buttler Tannercompany, London 1989:64-132.
11. Jankaukas S, Cohen IK, Grabb WC. Basictechnique of plastic surgery. In PlasticSurgery Smith JG, Aston SJ 4th edition. LittleBrown and company. 1991:3-90.
12. Furnas DW, Furnas H. Angular artery flapfor total reconstruction of lower eyelid. AnnPlast Surg 1983;10:322-5.
13. Hart WM.Jr. The eyelids Adler’s physiologyof eye, 9th edition Laurel Graven (Editor).Mosby Year Book. Inc U.S.A. 1992;1-16.
14. Moss AL, Cooper MA, Lendrum J, Hiles RW.The sanctity of the upper lid in lower lidreconstruction questioned. A modification ofa lid sharing procedure with a long termfollow up. Br J Plast Surg 1987;40: 246-57.
15. S iega l RJ. Pa la ta l g ra f t fo r eye l idreconst ruc t ion. P las t Reconst Surg1985;76:411-4.