Embed Size (px)
Citation preview

J Med Dent Sci 2011; 58: 69-77
Corresponding Author: Yoshiko UmedaDepartment of Gerodontology, Division of Gerodontology and Gerodontology, Graduate School, Tokyo Medical and Dental University 1-5-45, Yushima, Bunkyo, Tokyo, 113-8549, JapanTel: +81-3-5803-5562 Fax: +81-3-5803-5562E-mail: [email protected] January 19;Accepted March 11, 2011
Original Article
Effect of the reclining position in patients after oral tumor surgery
Yoshiko Umeda1), Shinya Mikushi1), Teruo Amagasa2), Ken Omura3) and Hiroshi Uematsu1)
1) Department of Gerodontology, Division of Gerontology and Gerodontology, Graduate School, Tokyo Medical and Dental University2) Maxillofacial Surgery, Maxillofacial Reconstruction and Function, Division of Maxillofacial and Neck Reconstruction, Graduate School, Tokyo Medical and Dental University3) Oral and Maxillofacial Surgery, Department of Oral Restitution, Division of Oral Health Sciences, Graduate School, Tokyo Medical and Dental University
Objectives: This study investigated the effects of reclining position on swallowing functions in the patients who had undergone surgery for oral tumors. Subjects and Methods: 53 Patients after oral tumor surgery who had undergone the videofluoroscopic swallowing study in the sitting position and reclining position were sampled. We measured Oral transit time (OTT), Pharyngeal transit time (PTT), Penetration-Aspiration scale, Locating of the leading edge of bolus at swallow onset, Route of bolus transit and Transit velocity. Results: Laryngeal penetration and aspiration were less likely to occur in the reclining position. The mean OTT was significantly shorter in the reclining position than in the sitting position. The leading edge of bolus at swallow onset was significantly lower in the reclining position than in the sitting position. The bolus went along the posterior wall of the pharynx in more patients in the reclining position. The mean PTT and the transit velocity did not significantly differ between the reclining position and the sitting position. Conclusion: This study suggested that, in patients after surgery on oral tumors, the reclining position is a useful posture to aid oral transit and to readily prevent aspiration and laryngeal penetration.
Key words: posture, reclining position, oral tumors, dysphagia, Videofluorography
Introduction
Dysphagia is recognized primarily as a sequela of cerebrovascular disorders, but it also appears in association with aging, neuromuscular diseases, and various other conditions, as well as following surgery for oral tumors, and it leads to malnutrition, asphyxia, aspiration pneumonia, and reduced quality of life. Aspiration pneumonia in particular is a serious, intractable and recurrent disease, and the primary objective in the treatment of dysphagia is prevention of aspiration. We perform a videofluoroscopic swallowing study (VFSS) or fibroscopic endoscopic evaluation of swallowing (FEES) to evaluate swallowing function and aspiration. Then we establish postural procedures and to prescribe an appropriate diet to prevent aspiration. Postural procedures are effective as a compensatory intervention for dysphagia and play a role in preventing aspiration1-3. Specifically, these procedures include chin down4-6, head rotation7-9, and a reclining position 10-13, and there are many reports on their effects. Logemann14 first described postural procedures as a very effective compensatory intervention for dysphagia, together with adjustment of food texture. Steefel 15 and Zimmerman et al 16. stated that a sitting position with the trunk almost perpendicular was a good posture during swallowing training, as it ensures safety; for instance, the bolus of food can be held in the oral cavity and does not drop unexpectedly into the pharynx, and it can easily be spat out by facing downward. Meanwhile, Saito et al 10. reported that a reclining

70 J Med Dent SciY. Umeda et al.
position reduced the amount of aspiration based on videofluoroscopic findings in dysphagia patients after stroke. Similarly, in Japan, cases in which aspiration was decreased or eliminated by using a reclining position have also often been reported clinically 10,13. Such reports10,13,17 have discussed its usefulness as follows:1. Since the trachea is posit ioned above the
esophagus in the reclining position, it is physically difficult for the bolus to enter the trachea.
2. Because the posterior wall of the pharynx is inclined, food can slide down along the posterior wall of the pharynx and reach the hypopharynx slowly.
3. Even when active transportation is difficult because of tongue movement disorders or disorders of the anticipatory stage, food can be transported by gravity.
Patients who have undergone surgery for oral tumors may have disorders of the oral and pharyngeal stage, and we have often used the reclining position clinically. However, we can’t find reports about the effect of the reclining position in patients after surgery for oral tumors. The present study investigated the effects of the reclining position on swallowing functions in such patients.
Materials and Methods
1. Subjects We sampled dysphagic patients who underwent VFSS after surgery for oral tumors between April 2008 and April 2010 in the Dental Hospital of Tokyo Medical and Dental University retrospectively. They were asked to swallow 4 ml of nectar-like thickness barium while in a 45-degree reclining position (hereinafter “reclining position”) and then in a sitting position. Each patient was sampled only once. Fifty-three patients (45 men, 8 women; mean age, 65 ± 11 years) were selected. The primary site of the tumor indicated for surgery was the tongue in 22 patients (17 men), mandibular gingiva in 20 (19 men), buccal mucosa in 5 (5 men), the floor of the mouth in 4 (3 men), and others in 2 (1 man). The mean days from the operation to VFSS were 20 days (20 ± 19 days). Informed consent was obtained from each patient for the study. This research was implemented after obtaining the approval of the Ethics Review Board of the Dental Hospital of Tokyo Medical and Dental University (2010-No.490).
2. Methods VFSS images (Medix-900DR, Hitachi Medical Corp, Japan, 30 frames/sec) recorded by a digital video recorder (GV-D1000 NTSC, Sony, Tokyo, Japan) via a video timer (1/100 sec, VTG-33, FOR-A, Japan) were transferred to a PC. Video images were replayed in slow motion using video editing software (iMovie, Apple Inc., USA). Swallowing dynamics were sampled when swallowing 4 ml of nectar-like thickness barium (barium/water 50/50% weight/volume, Barytgen sol, Fushimi Pharmaceutical Co., Ltd., Kagawa, Japan) in the sitting position and in the reclining position (Fig. 1).
①Anatomical evaluationCervical angle We call the angle formed by the horizontal line and straight line passing through the anteroinferior borders of the 3rd and 5th cervical vertebrae the cervical angle19 (Fig. 2).Camper’s plane angle Camper’s plane is defined by the line passing through the base of the nose and inferior margin of the tragus. We attached radiopaque disk markers (gold-silver-palladium alloy, 5 mm diameter, 1 mm thickness) at the base of the nose and at the inferior margin of the tragus as reference points for Camper’s plane20 (Fig. 3). We defined Camper’s plane angle as the angle formed by the vertical line and Camper’s plane (Fig. 3). We used photo editing software (Adobe Photoshop, Adobe Systems Inc., USA) to measure these angles.
°
Figure 1 : Posture

71Effect of the reclining position in patients after oral tumor surgery
②Oral stage evaluationOral transit time (OTT) Based on the method of Logemann21, oral transit time was measured as the time required from onset of tongue movement to propel the bolus posteriorly until the bolus passed the base of the tongue.
③Pharyngeal stage evaluationPenetration/Aspiration scale (Pene/Asp scale) The presence or absence of laryngeal penetration and aspiration was evaluated using the Pene/Asp scale22: 1) Material does not enter the airway; 2) Material enters the airway, remains above the vocal folds and is ejected from the airway; 3) Material enters the airway, remains above the vocal folds and is not ejected from the airway; 4) Material enters the airway, contacts the vocal folds and is ejected from the airway; 5) Material enters the airway, contacts the vocal folds and is not ejected from the airway; 6) Material enters the airway, passes below the vocal fold and is ejected into the larynx or out of the airway with or without effort; 7) Material enters the airway, passes below the vocal folds and is not ejected from the trachea despite effort; 8) Material enters the airway, passes below the vocal folds and no effort is made to reject it.
Pharyngeal transit time (PTT) Based on the method of Logemann 21, pharyngeal transit time was measured as the time from when the bolus passed the base of the tongue until the bolus passed through the cricopharyngeal sphincter.
Locating the leading edge of the bolus at swallow onset The locations of the leading edge of the bolus at swallow onset were classified as five regions of the oral cavity and pharynx based on a report by Yokoyama23 as follows (Fig. 4) : 1) oral cavity (OC) (from the lips to the posterior nasal spine); 2) upper oropharynx (UOP) (from the posterior nasal spine to the level of the lower border of the mandible); 3) valleculae (VAL) (from the lower border of the mandible to the edge of the epiglottis; 4) upper hypopharynx (HYP) (from the edge of the epiglottis to the upper esophageal sphincter); and 5) floor of the pyriform sinus (FPS). The time of swallow onset was defined as the moment when the hyoid bone begins its rapid superior and anterior motion.
Figure 2 : Cervical angleWe call the angle formed by the horizontal line and straight line passing through the anteroinferior borders of the 3rd and 5th cervical vertebrae the cervical angle.
Figure 3 : Camper’s plane angleCamper’s plane is defined by the line passing through the base of the nose and inferior margin of the tragus. We attached radiopaque disk markers (gold-silver-palladium alloy, 5 mm diameter, 1 mm thickness) at the base of the nose and at the inferior margin of the tragus as reference points for Camper’s plane. We defined Camper’s plane angle as the angle formed by the vertical line and Camper’s plane.

72 J Med Dent SciY. Umeda et al.
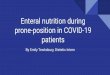
Route of bolus transit Bolus transit was classified into two routes: the anterior route, from the base of the tongue to the pyriform sinus via the valleculae and side of the larynx; and the posterior route, from the base of the tongue to the pyriform sinus via the posterior wall of the pharynx (Fig. 5). The route of bolus transit was investigated in patients in whom the location of the leading edge of the bolus at swallow onset was the upper hypopharynx or the floor of the pyriform sinus (N=13).
Transit velocity The transit velocity was studied in patients in whom swallow onset was initiated after the bolus passed the mandibular inferior border (N=34). The time after the bolus passed the mandibular inferior border until swallow onset was the transit time, and the transit displacement was the displacement from the mandibular inferior border to the leading edge of the bolus at swallow onset. The transit velocity was calculated as the transit displacement divided by the transit time.
3. Data Analysis The paired t-test was used to compare the sitting position with the reclining position in cervical angle, Camper’s plane angle, oral transit time, pharyngeal transit time, and transit velocity; Wilcoxon’s signed-rank test was used to compare the sitting position with the reclining position in the Pene/Asp scale and the locations of the leading edge of the bolus at swallow onset, and Fisher’s exact test was used to compare the sitting position with the reclining position in the route of bolus transit. SPSS11.0J (SPSS Inc. Chicago, IL, USA) was used for statistical processing, and p<0.05 was considered significant.
Results
Cervical angle and Camper’s plane angle The mean cervical angle was 54.4 ± 12.2 degrees in the reclining position and 97.7 ± 13.4 degrees in the sitting position. The mean Camper’s plane angle was 125.6 ± 11.2 degrees in the reclining position and 88.4 ± 10.7 degrees in the sitting position. Both angles showed significant differences between the reclining and sitting positions (Fig. 6).
Pene/Asp scale Compared with the sitting position, the score in the reclining position was 1 point lower in 1 patient, 2 points lower in 8 patients, 4 points lower in 2 patients, 5 points lower in 3 patients, 6 points lower in 1 patient and the same score in 37 patients. The score of Pene/Asp scale in the reclining position showed significantly lower values than the Pene/Asp scale in the sitting position. Laryngeal penetration and aspiration were significantly less likely to occur in the reclining position (Fig. 7).
Oral transit time The mean oral transit time was significantly shorter in the reclining position (1.22 ± 0.51 sec) than in the
Figure 5 : Route of bolus transitBolus transit classified into two routes: the anterior route, from the base of the tongue to the pyriform sinus via the valleculae and side of the larynx; and the posterior route, from the base of the tongue to the pyriform sinus via the posterior wall of the pharynx.
Figure 4 : Regions of the oral cavity and pharynxThe locations of the leading edge of bolus at swallow onset were classified as five regions of the oral cavity and pharynx based on a report by Yokoyama:1)oral cavity (OC) (from the lips to the posterior nasal spine); 2) upper oropharynx (UOP) (from the posterior nasal spine to the level of the lower border o the mandible); 3) valleculae (VAL) (from the lower border of the mandible to the edge of the epiglottis; 4) upper hypopharynx (HYP) (from the edge of the epiglottis to the upper esophageal sphincter); and 5) floor of pyriform sinus (FPS).

73Effect of the reclining position in patients after oral tumor surgery
sitting position (2.07 ± 1.37 sec) (Fig. 8).
Pharyngeal transit time The mean pharyngeal transit time was not significantly different between the reclining position (0.63 ± 0.27 sec) and the sitting position statistically (1.06 ± 0.94 sec) (Fig. 8).
The locations of the leading edge of barium at swallow onset The leading edge of barium at swallow onset was
significantly deeper in the sitting position than in the reclining position (Fig. 9). The score in the sitting position was 2 in 11 patients, 3 in 19 patients, 4 in 16 patients, and 5 in 7 patients. On the other hand, the score in the reclining position was 2 in 16 patients, 3 in 21 patients, 4 in 11 patients, and 5 in 5 patients. Fifteen patients had a lower score in the reclining position than in the sitting position.
Route of bolus transit Among patients in whom the location of the leading
)
*
Figure 6 : Cervical angle and Camper’s plane angleThe cervical angle in the reclining position showed significantly narrower than the cervical angle in the sitting position. The Camper’s plane angle in the reclining position showed significantly wider than the Camper’s plane angle in the sitting position. Both angles showed significant differences between the reclining and sitting positions.
Figure 7 : Pene/Asp scaleLaryngeal penetration and aspiration were less likely to occur in the reclining position.

74 J Med Dent SciY. Umeda et al.
edge of barium at swallow onset was the upper hypopharynx or the floor of the pyriform sinus (N=13), the route in the sitting position was the anterior route in 13, whereas the route in the reclining position was the anterior route in 4 and the posterior route in 9. The bolus went along the posterior wall of the pharynx in more patients in the reclining position (Table 1). The route of bolus transit showed a significant difference between the reclining and sitting positions. table 1
)
*
*
Posture Route
Anterior Posterior
Sitting position 13 0
Reclining position 4 9
* P<0.01 (Fisher’s exact probability test)
Figure 8 : Oral transit time and Pharyngeal transit timeThe mean Oral transit time was significantly shorter in the reclining position than in the sitting position.The mean Pharyngeal transit time was not significantly different between the reclining position and the sitting position statistically.
Figure 9 : The locations of the leading edge of bolus at swallow onsetThe leading edge of bolus at swallow onset was significantly deeper in the sitting position than in the reclining position.
Table 1. Route of bolus transit (N=13)The bolus went along the posterior wall of the pharynx in more patients in the reclining position. The route of bolus transit showed significant difference between the reclining and sitting positions.
P=0.052

75Effect of the reclining position in patients after oral tumor surgery
Bolus velocity The bolus velocity did not significantly differ between the reclining position (103.7 ± 82.6 mm/sec) and the sitting position (114.1 ± 103.0 mm/sec) (Fig. 10).
Discussion
To date, several authors have reported patients in whom the reclining position was useful for swallowing training10-13,17. In the present study, an improvement in aspiration and laryngeal penetration was also observed in the reclining position compared to the sitting position in patients after surgery for oral tumors. The following is a discussion of the factors that showed improvement.
Oral stage Since oral stage disorders occur markedly in patients following surgery for oral tumors, prolongation of the oral transit time has been reported24. In the present study as well, prolongation of the oral transit time was confirmed in the sitting position compared with the oral transit time in healthy people (1–1.5 sec)25,26. But in the reclining position, the value was shortened to a value close to that in healthy people. These findings are in agreement with the reported improvements in oral stage disorders due to the reclining position in surveys on other diseases13. Camper’s plane angle is significantly more inclined in the reclining position than in the sitting position. We considered that gravity assisted transport of the bolus because the oropharynx is lower than the oral cavity in the reclining position. Hence, we considered the reclining position to be useful
in patients with oral stage disorders, such as those who have undergone surgery for oral tumors.
Pharyngeal stage Based on VFSS findings, in the sitting position, the bolus could not be transported into the pharynx at once, and the bolus transport from the oral cavity into the pharynx was also slower. It takes a certain amount of time for the bolus to move from the oral cavity into the pharynx after the leading edge has passed the base of the tongue. Therefore, the location of the leading edge of barium at swallow onset was deep, and the pharyngeal transit time tended to be prolonged. Once the bolus was in the pharynx, it moved easily along the anterior wall of the pharynx, and the bolus appeared to easily traverse the larynx.
Effect of the reclining position In the reclining position, movement from the oral cavity into the pharynx was faster, because gravity facilitated bolus movement, the bolus entered the pharynx as a single lump, and swallow onset could occur subsequently. Therefore, the pharyngeal transit time was about the same as that in healthy people (0.54–1.5 sec)26. In addition, since the pharynx was significantly inclined in the reclining position compared with the sitting position, the bolus moved gradually along the posterior wall of the pharynx, and the location of the leading edge of barium at swallow onset was low. Furthermore, in the reclining position, the trachea is positioned superior to the esophagus in terms of both anatomy and gravity, and so the bolus is likely to move
Figure 10 : Transit velocityThe transit velocity did not significantly differ between the reclining position and the sitting position.
P=0.37(t-test)

76 J Med Dent SciY. Umeda et al.
easily along the posterior wall of the pharynx, but have difficulty in traversing the larynx. Concerning the bolus velocity, it is reported that in the reclining position, because the posterior wall of the pharynx is inclined posteriorly, food can slide down the posterior wall of the pharynx, causing the bolus to reach the upper hypopharynx slowly; however, the bolus velocity in the present study showed no significant difference based on posture. In the sitting position, the bolus passed the anterior of the pharynx and then temporarily stopped at the valleculae, resulting in attenuation of the bolus velocity. Based on these findings, it appears that in patients following surgery for oral tumors, laryngeal penetration and aspiration are reduced in the reclining position for the following reasons: smooth oral and pharyngeal transit are possible; the bolus passes easily far from the vocal cords; the location of the leading edge of the bolus at swallow onset is in a low position; and the respiratory tract is in a superior position in terms of gravity. Although the above effects are achieved in the reclining position, some patients exhibited aspiration and laryngeal penetration before swallow onset as a result of excessive promotion of transit to the pharynx. Therefore, caution is required for liquids and jellies in particular, because they are transited to the pharynx faster than nectar-like thickness. In the present study, the effects of the reclining position were surveyed by sampling patients following surgery for oral tumors, but factors such as the primary site of the tumor and the operative procedure differed among the patients. In the future, we hope to increase the number of patients and examine other diseases and properties to further clarify the effects and mechanisms of the reclining position.
Conclusion
The results of the present study suggest that, in patients after surgery for oral tumors, the reclining position is a useful posture to aid oral transit and to readily prevent aspiration and laryngeal penetration.
Acknowledgements
This work was the partly supported by Grant for Longevity Sciences (19kou-2) from the Ministry of Health, Labour and Welfare of Japan.
References1. Horner J, Massey EW, Riski JE, et al. Aspiration following
stroke: Clinical correlates and outcome. Neurology. 1988 Sep; 38(9): 1359-1362.
2. Logemann JA. Swallowing disorders and rehabilitation. J Head Trauma Rehabil. 1989; 4(4).
3. Rasley A, Logemann JA, Kahrilas PJ, et al. Preventing of barium aspiration during videofluoroscopic swallowing studies: value of change in posture. AJR Am Roentgenol. 1993 May; 160(5): 1005-1009.
4. Ekberg O. Posture of the head and pharyngeal swallowing. Acta Radiol Diagn, 1986 Nov-Dec; 27(6): 12: 691-696.
5. Welch MV, Logemann JA, Rademaker AW, et al. Changes in pharyngeal dimensions effected by chin tuck. Arch Phys Med Rehabil. 1993 Feb; 74(2): 178-181.
6. Shanahan TK, Logemann JA, Rademaker AW, et al. Chin-down posture effect on aspiration in dysphagic patients. Arch Phys Med Rehabil. 1993 Jul; 74(4): 736-739.
7. Logemann JA, Kahrilas PJ, Kobara M, et al. The benefit of head rotation on pharyngoesophageal dysphagia. Arch Phys Med Rehabil. 1989 Oct; 70(10): 767-771.
8. Logemman JA, Rademaker AW, Pauloski BR, et al. Effects of postural change on aspiration in head and neck surgical patients. Otolaryngol Head Neck Surg. 1994 Feb; 110(2): 222-227.
9. Logemman JA. The dysphagia diagnostic procedure as a treatment efficacy trial. Clin Commun Disord. 1993 Fall; 3(4): 1-10.
10. Saitoh E, Kimura A, Yamori S, et al. Videofluorography in rehabilitation of dysphagia. (in Japanese, English abstract) Reha Med. 1986; 23(3): 121-124.
11. Drake W, O’Donoghue S, Bartram C, et al. Eating in side-lying facilitates rehabilitation in neurogenic dysphagia. Brain Inj. 1997 Feb; 11(2) :137-142.
12. Larnet G, Ekberg O. Positioning improves the oral and pharyngeal swallowing function in the children with cerebral palsy. Acta Paediatr. 1995 Jun; 84(6): 689-692.
13. Fujishima I, Kojima C, Fujishima Y, et al. Postural effects on dysphagia due to pseudobulbar and bulbar palsy. (in Japanese) J Clin Rehabil. 1993; 2(7): 593-597.
14. Logemann JA. Evaluation and Treatment of Swallowing Disorders. College-Hill Press, San Diego. 1983.
15. Steefel JS. Dyaphagia rehabilitation for neurologically impaired adults. Charles C Thomas publisher, Illinois. 1988.
16. Zimmerman JE, Oder LA. Swallowing Dysfunction in Acutely Ill Patients. Phys Ther. 1981 Dec; 61(12): 1755-1763.
17. Okada S. Reexamination about Posture Technique. (in Japanese) MB Med Rehabil. 2007; 83: 26-20.
18. Baba S, Saitoh E. Indication of dysphagia rehabilitation (in Japanese). Rinsho Reha. 2000; 9: 857-863.
19. Yokoyama M, Mitomi N, Tetsuka K, et al. Role of Laryngeal Movement and Effect of Aging on Swallowing Pressure in the Pharynx and Upper Esophageal Sphincter. Laryngoscope. 2000 Mar; 110(3 Pt 1): 434-439.

77Effect of the reclining position in patients after oral tumor surgery
20. Nakane A, Tohara H, Ouchi Y, et al. Videofluoroscopic Kinesiologic Analysis of Swallowin: Defining a Standard Plane. J Med Dent Sci. 2006 Mar; 53(1): 7-15.
21. Logemann JA, Pauloski BR, Colangelo L, et al. Effects of a sour bolus on oropharyngeal swallowing measures in patients with neurogenic dysphagia. J Speech Hear Res. 1995 Jun; 38(3): 556-563.
22. Rosenbek JC, Robbins JA, Roecker EB, et al . A penetration-aspiration scale. Dysphagia. 1996 Spring; 11(2): 93-98.
23. Yokoyama M. A Study of the Chew-Swallow Complex in Hemispheric Stroke Patients: Comparisons with Normal
Subjects. (in Japanese) The Fujita Medical Society. 2007; 293-317.
24. McConnel FM, Paukoski BR, Logemann JA, et al. Functional Results of Primary Closure vs Flaps in Oropharyngeal Reconstruction. Arch Otolaryngol Head Neck Surg. 1998 Jun; 124(6): 625-630.
25. Tracy JF, Logemann JA, Kahrilas PJ, et al. Preliminary observations on the effects of age on oropharyngeal deglutition. Dysphagia. 1989; 4(2): 90-94.
26. Langemore SE. Endoscopic evaluation and treatment of swallowing disorders, thieme medical publishers, New York. 2001.