Embed Size (px)
DESCRIPTION
New Perspective for Expanding Donor’s Pool -Resuscitation Kidney In Uncontrolled Donors by Normothermic Perfusion “In Situ” with Oxygenation and Leucocyte Depletion Saint-Petersburg, Russia State Research Institute for Emergency, ISODP-2011 Buenos-Aires, Argentina. - PowerPoint PPT Presentation
Citation preview

New Perspective for Expanding Donor’s Pool -Resuscitation Kidney In Uncontrolled Donors by Normothermic Perfusion “In Situ” with Oxygenation and Leucocyte Depletion
Saint-Petersburg, RussiaState Research Institute for Emergency, ISODP-2011Buenos-Aires, Argentina
O.Reznik, A. Skvortsov, A.Reznik, Y.Moysyuk, S.Bagnenko, and S.Gautier

The authors don’t have the conflict of interests
The design of this study, protocols of perfusion, and procurement and transplantation procedures were approved by the Scientific Board and Ethics Committee of the Saint Petersburg State Research Institute for Emergency (Decision 7/0615/09)
and authorized for clinical application by the Federal Advisory Service of the Health Ministry of the Russian Federation (Resolution N2010/299)

In the US, the number of potential uncontrolled donors after cardiac death was estimated at 22,000 per year in 2006
IOM: Organ Donation: Opportunities for Action. Washington, DC: National Academies Press; 2006
Hanto DW, Veatch RM. Uncontrolled Donation after Circulatory Determination of Death (UDCDD) and the
Definition of Death. Am J Transplant 2011; 11(7): 1351-1352.
Hoogland ERP, et al. Kidney Transplantation from Donors after Cardiac Death: Uncontrolled versus Controlled
Donation. AJT 2011; 11(7): 1427-1434.Wall SP, et al. Derivation of the Uncontrolled Donation after
Circulatory Determination of Death Protocol for New York City. Am J Transplant 2011; 11(7): 1417-1426
Introduction

backgroundbackground
• The number of patients died form irreversible number of patients died form irreversible sudden asystole was 173 in 2009 sudden asystole was 173 in 2009
in Saint Petersburgin Saint Petersburg • Most of potential grafts from uDCD are lost
due to irreversible ischemic damage during warm ischemic time
• The main task our work was the development procurement protocol which would lead to the organ resuscitation after ischemical damage and due to this expanding the donor pool

“Compilation approach”
Sanchez-Fructuoso A.I.,et al. Non-heart beating donors: experience from the Hospital Clinico of Madrid, J. Nephrol;2003;16(3);387-92.
Steen S., Ingemansson R. et. al. First Human Transplantation of Nonacceptable donor lung after reconditioning ex vivo Ann of Thor Surgery,2007,83(6),2191-95
Talbot D. et al. How to improve the quality of kidneys from non-heart-beating donors: a randomized controlled trial of thrombolysis in non-heart-beating donors,Transplantation,2003,76(12),1714-19
Jamieson R. W., Friend P. J. Normothermic organ preservation, Tr Rev,2006,Vol. 20,P.172-8
Nicholson M. L., Simon J. F., Harper L.W. et. al. The Effect of Warm Ischemic Time on Renal Function and Injury in the Isolated Hemoperfused Kidney,Transplantation,2008,86(3), 445-51
Fondevila C., et al., Am J Tr 2007;7;1849 Liver transplant using donors after unexpectedcardiac death: novel preservation protocol andacceptance criteria

Sergei S. Brukhonenko, 1890-1960
«Soviet Experiments in the Revival of Whole
Organisms and Isolated Dog Head» 1927
Konstantinov I.E., Alexi-Meskishvili V.V. Sergei s. Brukhonenko: the Development of the First Heart-Lung Machine for Total Body Perfusion
Ann. Thorac. Surg. – 2000. - Vol. 69. - P. 962 – 966.
Probert W.R., Melrouse D.G. An Early Russian Heart-Lung Machine BMJ, 1960 April. -12. - Р.104

material & methodsmaterial & methods
New logistic procurement model Extracorporal perfusion circuit Perfusat (modificated donor’s blood)
17 uncontrolled donors, 2009-2010 34 recipients of kidney from uDCD

Material and Methods: New Uncontrolled Donation Logistics Chain
Warm Ischemic Time
45-91 minutes

surgical femoral vessels access and three-lumen double balloon catheterization of abdominal region

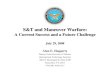
Scheme of isolated abdominal perfusion procedure

Composition of perfusat
OXYGEN
1
2
3
4
5
6
1. Reservoir
2. MARS pump device
3. Oxygenator
4. Leukocytes filter
5. Preservation solution
6. Oxygen supply
• Modificated donor blood (27°-32°C)
• 25000 U heparin• 1,5 mln U streptokinase• 400 ml perfluorocarbonic
emulsion • for primary filling of
perfusion circuit is used the HTK-solution

CharacteristicValue (percentage)
(N = 17)
Age, years 43.6 ± 2.2
Gender: Male Female
14 (82.4%)3 (17.6%)
Cause of death: Brain injury Cerebrovascular disease
11 (64.7%)
6 (35.3%)
Dopmine dose, mkg/kg/min 6.82 ± 0.65
Creatinine, mg/dL 1.48 ± 0.11
Diuresis during the last hour, 0.35 ± 0.06
Warm ischemia, min 68 ± 4
Donors characteristics

Donors’ Perfusion procedure data
Variable Value (N = 17)
Hemoglobin, g/L 33.6 ± 3.75
Hematocrit 0.32 ± 0.02
рН of perfusate 7.0–7.3
Perfusion flow, initial, ml/min 500
Perfusion flow, final, ml/min 3500
Oxygen supply initial, ml/min 150
Final oxygen supply, ml/min 350
Average рО2* in perfusate, mmHg 297.8 ± 27.5
Average рСО2** in perfusate, mmHg 99.8 ± 7.4
Duration NECP and LD***, min 152.1 ± 6.9
Leukocyte count in perfusion contour, initial
16.4 ± 1.2
Leukocyte count in perfusion contour, final 0.77 ± 0.13
*рО2: partial pressure of oxygen
**рСО2: partial pressure of carbon dioxide
***NECP and LD: normothermic extracorporeal perfusion and leukocyte depletion


Recipients characteristicsCharacteristic Value (percentage)
(N = 34)Age, years 51.4 ± 1.3
Type of dialysis: Hemodialysis Peritoneal dialysis Mixed dialysis
28 (82.4%)6 (17.6%)
-
Years on dialysis prior to transplant 3.32 ± 0.33
Cause of end-stage renal disease: Glomerulonephritis Pyelonephritis Polycystic kidney
31 (91.2%)1 (2.9%)2 (5.9%)
Cold ischemic time before transplantation, hrs
14.8 ± 0.67
Graft function: IGF DGF
11 (32.4%)23 (67.6%)
Number of dialysis/1 month for DGF group 5.8 ± 0.96
Creatinine at 90 days, mg/dL 2.4 ± 0.02
Creatinine at 1 year, mg/dL 1.81 ± 0.05cGFR3, ml/min/1.73 m2 53.4 ± 2.18Acute rejection kidney/90 days 2 (5.8%)
Surgical complications 1 (2.9%)

Conclusion
• The results of the 1-year follow-up of our initial clinical experience with this procedure provide evidence that transplantation of organs that are “resuscitated” using this method are satisfactory and meet the generally accepted criteria for graft survival and functioning.
• The implementation of NECP with oxygenation and leukocyte depletion allows expanding the donor pool due to inclusion of the resource of donors with unexpected cardiac death

Sergei Brukhonenko 1890-1960
THANK YOU FOR YOUR ATTENTION