Embed Size (px)
Citation preview

Roma, 7-9 novembre 2014
Indicazioni alla radioterapia e chirurgia orbitaria
Orbitopatia basedowiana: percorso diagnostico-terapeutico
Claudio Marcocci Dipartimento di Medicina Clinica e Sperimentale
Universita’ di Pisa U.O Endocrinologia 2
Azienda Ospedaliero-Universitaria di Pisa

Roma, 7-9 novembre 2014
Rationale for the use of orbital radiotherapy for GO
• Nonspecific anti-inflammatory effect
• Radiosensitivity of T-lymphocytes infiltrating the orbit
• Reduction of glycosaminoglycan secretion

Roma, 7-9 novembre 2014
Protocol of orbital radiotherapy for GO
• Supervoltage apparatus (linear accelerator, 4-6 MeV)
• 2 Gy per day in 10 daily doses over a 2-week period [cumulative dose, 20 Gy; lower cumulative doses (10 Gy) may be as effectiv]
• Irradiation field: 4x4 cm lateral field, slightly angled posteriorly

Roma, 7-9 novembre 2014
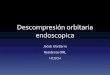
Comparison of orbital radiotherapy and glucocorticoids for GO
0
3
6
9
12
15
18
Responders Nonresponders
Radiotherapy+placebo
Steroids+sham irradiation
N. o
f pat
ient
s
(Prummel, 1993)

Roma, 7-9 novembre 2014
Radiotherapy for Graves’ orbitopathy: randomized placebo-controlled study
Mourits MP et al, Lancet 2000
• Treatment outcome was successful in about 60% of irradiated patients, compared 30% of sham irradiated patients at 24 weeks
• This difference was mostly due to improvement of eye muscle motility
• A more rapid fall of disease activity occurred in irradiated patients
• No difference between the two groups in eyelid swelling and proptosis

Roma, 7-9 novembre 2014
Prummel et al. JCEM 2004
• Improvement of eye muscle motility and diplopia • Less need for further treatments

Roma, 7-9 novembre 2014
Oral glucocorticoids or radiotherapy alone vs combined therapy for GO
OI
(Bartalena, 1983, Marcocci, 1991)
p< 0.005 p< 0.01

Roma, 7-9 novembre 2014
Orbital irradiation combined with oral glucocorticoids
• The combined regimen exploits the prompter effect of glucocorticoids and the more sustained action of irradiation
• Orbital radiotherapy reduces the rate of recurrence observed with glucocorticoids alone, by shortening the active phase of the disease
• Glucocorticoids prevent the transient exacerbations of eye manifestations caused by irradiation

Roma, 7-9 novembre 2014
Side effects and complications of orbital radiotherapy
Acute effects Skin irritation and temporal hair loss Transient exacerbation of inflammatory signs
Late effects Cataract Retinopathy Radiation-induced tumors

Roma, 7-9 novembre 2014
Radiation cataract
13/160
8.0%
LA
8/44
18.0 %
CU
p=0.1
21/204
10.2 % Total
Mean age 61 yr Mean latency 12 yr

Roma, 7-9 novembre 2014
Orbital radiotherapy and radiation cataract
Marcocci 2004

Roma, 7-9 novembre 2014
Orbital RT and secondary tumors
Medical history (n=204)
157 patients CT scan of the orbit and adjacent regions

Roma, 7-9 novembre 2014
Retinal changes vs retinopathy
median (range)
< 5 1.5 (1-5)
>5 23 (10-50)
n= 18 5 patients
9 4 2 1 2
micro’s 1 2 3 4 5
patients 1 1 1 1 1
micro’s 10 11 23§ 35§ 50§
Visual acuity 0.85 ± 0.2
0.66 ± 0.2*
* p<0.05
§ DM
Wakelkamp et al., Ophthalmology 2004

Roma, 7-9 novembre 2014
Management of moderate to severe GO: Orbital radiotherapy
! OR should be considered in patients with active GO who have diplopia or restricted motility (Ib, A)
! Lower cumulative doses (10 Gy) may be as effective as and better tolerated than higher doses (20 Gy) (Ib, A). Doses >20 Gy are not recommended (IV, C)
! Caution should be exercised about administering OR to patients younger than 35 yr; OR must be avoided in patients with diabetic retinopathy and/or severe hypertension (III, B)
! Combination of oral GCs and OR is more effective than either treatment alone (Ib, A), but RCTs indicating that combination of iv GCs with OR is better than iv GCs alone are lacking (IV, C)

Roma, 7-9 novembre 2014
Orbital decompression: Rationale
Provides means for immediate expansion of orbital contents into a more capacious volume
– 0.67 ml in orbital volume = 1 mm reduction in proptosis
– N of orbital walls removed: 1 wall = 2-3 mm reductionin proptosis 4 walls = 14-16 mm reduction in
proptosis

Roma, 7-9 novembre 2014
Orbital decompression: Indications
Orbital decompression is a common treatment for Graves’ orbitopathy (GO)
Indications: • Optic neuropathy (not responsive to high dose ivGC) • Severe proptosis
• Corneal exposure • Subluxation/luxation of eye globes
• Cosmetic/Rehabilitative purposes

Roma, 7-9 novembre 2014
Clin Endocrinol 2005

Roma, 7-9 novembre 2014
Clin Endocrinol 2005

Roma, 7-9 novembre 2014
Orbital decompression: Indications
Orbital decompression is a common treatment for Graves’ orbitopathy (GO)
Indications: • Optic neuropathy (not responsive to high dose ivGC) • Severe proptosis
• Corneal exposure • Subluxation/luxation of eye globes
• Cosmetic/Rehabilitative purposes

Roma, 7-9 novembre 2014
• Dural damage with cerebrospinal fluid leak and/or pneumocephalus
• Iatrogenic damage of the optic nerve
• Intraorbital haemorrhage
• Periorbital hypoesthesia
• Worsening of a pre-existent diplopia or de-novo development of diplopia
Complications

Roma, 7-9 novembre 2014
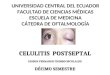
SQUINT SURGERY
PRE-OP.
2 months POST-OP.

Roma, 7-9 novembre 2014
Functional
EYELID SURGERY

Roma, 7-9 novembre 2014
Functional
Aesthetic
EYELID SURGERY

Roma, 7-9 novembre 2014
Management of moderate to severe GO:Surgery
! The timing and order of surgical interventions should be carefully planned (IV, C)
! A fixed sequence of correction (if needed) has to be respected: orbital decompression, squint surgery, lid lengthening with or followed by blepharoplasty/browplasty (III, B)
! Rehabilitative decompression surgery should only be performed in euthyroid patients with GO quiescent for at least 6 months (III, B)
! Rehabilitative surgery should only be undertaken in centres with appropriate expertise (IV, C)

Roma, 7-9 novembre 2014