Embed Size (px)
Citation preview
British Journal of Oral Surgery (1980) 18, 212-220 @ The British Association of Oral Surgeons
0007-117X/80/00320212$02.00
ORAL SURGICAL MANAGEMENT OF CLEIDOCRANIAL DYSOSTOSIS
J. A. MIGLIORISI~ and P. T. BLENKINSOPP, F.D.s.R.c.s.(ENG)., M.B., B.S.(LOND), B.D.S.(LOND)2*
1 Department of Oral Surgery; Faculty of Montevideo. Uruguay. 2 Queen Mary’s Hospital, Roehampton, London S. W.15
Summary. A patient with cleidocranial dysostosis is presented to further support the early active surgical management of the dental complications of this disease. There is good evidence to show that the permanent teeth have the ability to erupt once the deciduous dentition, supernumeraries, and overlying alveolar bone are removed. The aetiology of this failure of eruption is considered to be an abnormality in alveolar bone remodelling, compounded by overactivity of the dental lamina. The clinical experience gained from this patient substantiates this theory.
Introduction Cleidocranial dysostosis is a rare yet well documented, autosomal dominant inherited condition (Jarvis & Keats, 1974), with multiple skeletal and dental abnormalities. The most striking features, partly from which the syndrome derives its name, are the ability to approximate the shoulders, the cranial deformity, and the failure of eruption of the permanent dentition. The osseous dysplasia is not, as originally thought, confined only to bones of membranous origin, but may also involve those formed from cartilaginous precursors (Kalliala & Taskinen, 1962; Jarvis & Keats, 1974).
The combination of predominantly defective membrane bone formation and delayed suture and fontanelle closure in cleidocranial dysostosis produces character- istic craniofacial deformities. The late fusion of the frontal and sagittal sutures increases the transverse diameter of the skull and thus it is broad with pronounced frontal and parietal bossing (brachycephalic deformity). In contrast the face appears small with depression of the bridge of the nose and broadening of its base. The maxilla and zygomatic bones are hypoplastic with poor development of the para-nasal sinuses, the mastoids are also poorly pneumatised secondary to the altered function of the sternocleidomastoid muscle.
Development of the mandible is usually normal producing a pseudo-prognathism in relation to the hypoplastic maxilla, and rarely non-union of the mandibular symphysis may occur. The oral cavity usually exhibits a high arched palate, and a submucous or complete cleft is not uncommon. The deciduous dentition is retained, and the permanent teeth remain unerupted along with multiple supernumerary teeth; cyst formation being a possible sequel.
The affected are of short stature with defective or absent clavicles, producing the abnormal shoulder movement and the apparently long neck. The thorax is conical, posterior wedging of the thoracic and lumbar vertebrae, or lumbar vertebrae spondy- losis may co-exist. Spina bifida occulta with a propensity for the cervico-thoracic spine is common. In addition there may be coxa Vera, delayed closure of the pubic symphysis, iliac hypoplasia with other pelvic abnormalities, and abnormalities of the
(Received 7 June 1979; accepted 21 December 1979)
* For reprints.
212
ORAL SURGICAL MANAGEMENT OF CLEIDOCRANIAL DYSOSTOSIS 213
bones of the hands and feet, .especially pointing of the terminal phalangeal tufts (Kalliala & Taskinen, 1962; Jarvis & Keats, 1974; Gorlin et al., 1976).
The main problems confronting the oral surgeon in cleidocranial dysostosis, are those of the unerupted dentition, and of facial deformity predominantly maxillary hypoplasia. It is our belief that the treatment should be early surgical intervention to achieve as near as possible a normal permanent dentition, and in this we are in agreement with Oksala and Fagerstrom (1971), and Hitchin and Fairley (1974).
Case history The 16-year-old South American boy discussed in this paper showed many of the
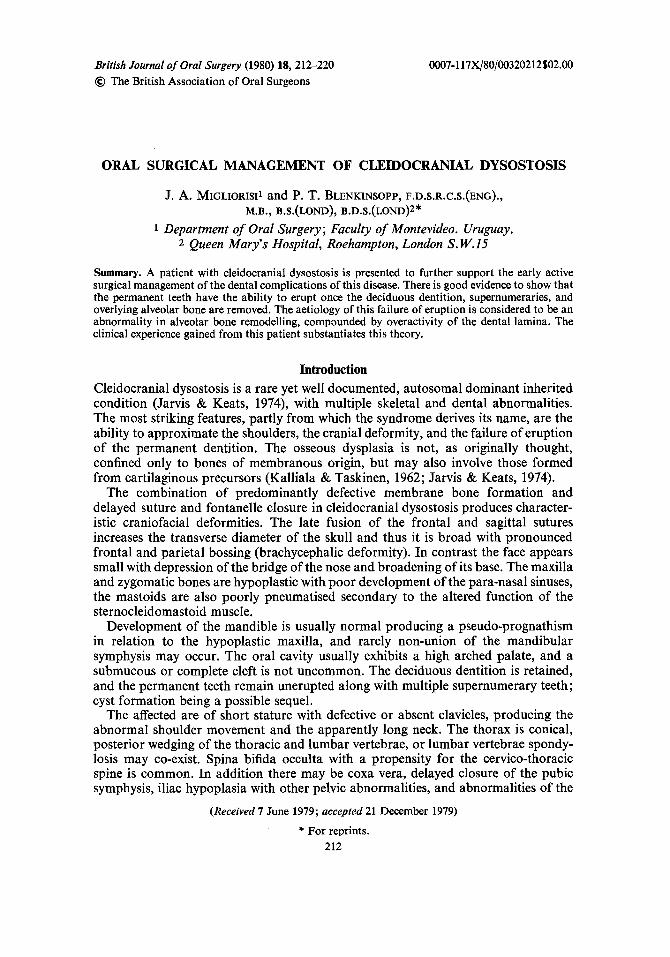
characteristics identifiable with cleidocranial dysostosis. He was of short stature with complete aplasia of the clavicles and associated funnelling of the rib cage towards the thoracic inlet (Figs. 1 & 2). His pelvis was hypoplastic as were the carnal, metacarpal, tarsal, and metatarsal bones. The finger nails showed increased convexity and cornification.
FIG. 1 (left). Sixteen-year-old patient affected by cleidocranial dysostosis, with characteristic shoulder hypermobility.
FIG. 2 (right). Chest radiograph showing absence of clavicles and associated funnelling of the thoracic inlet.
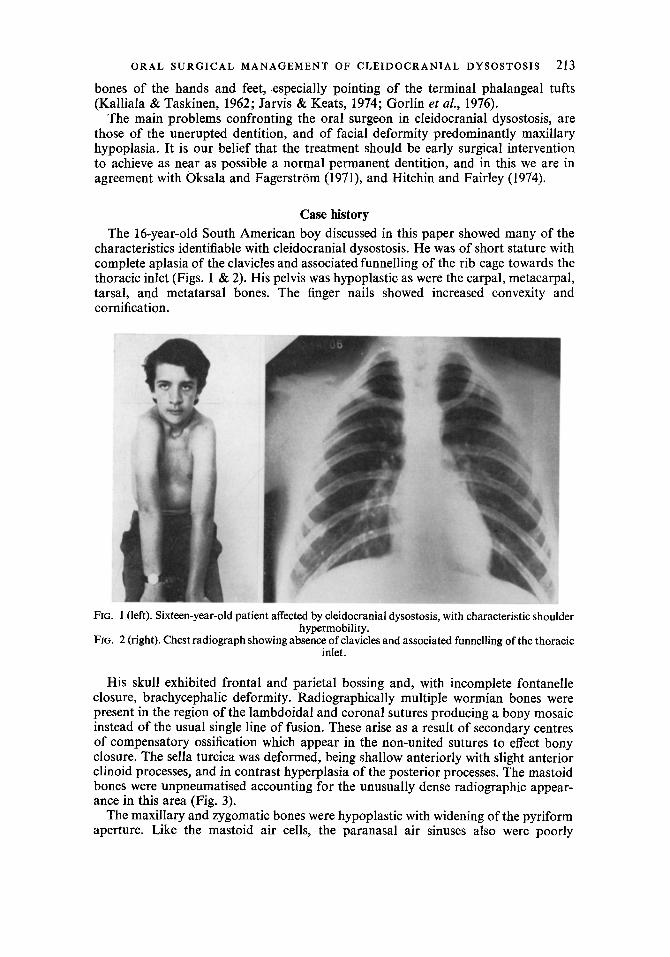
His skull exhibited frontal and parietal bossing and, with incomplete fontanelle closure, brachycephalic deformity. Radiographically multiple wormian bones were present in the region of the lambdoidal and coronal sutures producing a bony mosaic instead of the usual single line of fusion. These arise as a result of secondary centres of compensatory ossification which appear in the non-united sutures to effect bony closure. The sella turcica was deformed, being shallow anteriorly with slight anterior clinoid processes, and in contrast hyperplasia of the posterior processes. The mastoid bones were unpneumatised accounting for the unusually dense radiographic appear- ance in this area (Fig. 3).
The maxillary and zygomatic bones were hypoplastic with widening of the pyriform aperture. Like the mastoid air cells, the paranasal air sinuses also were poorly
214 BRITISH JOURNAL OF ORAL SURGERY
FIG. 3. Skull radiograph with mosaic pattern of wormian bones in the lambdoidal and coronal sutures, elongation of the posterior clinoid processes, and unpneumatised mastoid bones.
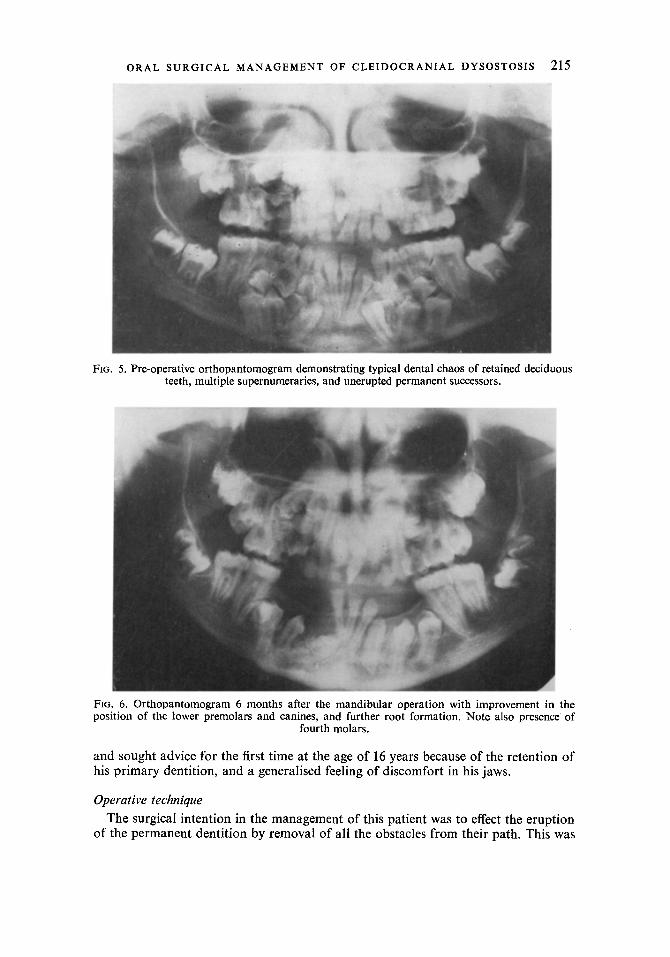
pneumatised, the palate was high vaulted but there was no cleft. Dento-alveolar abnormalities present were consistent with the syndrome, namely retention of the deciduous dentition, delayed eruption of the permanent dentition except the first permanent molars and lower incisors, and the presence of multiple supernumerary teeth. Radiographically the deciduous teeth showed little in the way of root resorption; the supernumeraries lay between and apical to the deciduous roots, displacing the permanent incisors, canines and permolars in the maxilla towards the orbital floor, and in the mandible the canines and premolars to the lower border. The supernumerary teeth as usual were irregular in form, the morphology of the permanent teeth appeared, by and large, normal but had reduced root formation consistent with unerupted teeth (Figs. 4 & 5). A later radiograph demonstrated not only the presence of unerupted third molars but also unerupted fourth molars in all four quadrants (Fig. 6).
Like most patients with this condition he was unaware that he had the disease
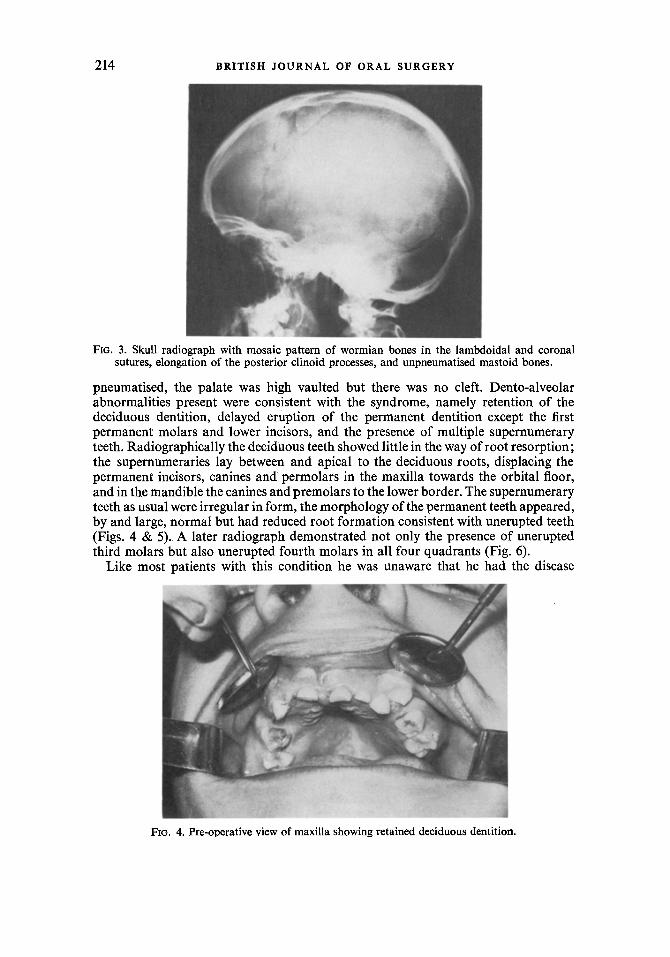
FIG. 4. Pre-operative view of maxilla showing retained deciduous dentition.
ORAL SURGICAL MANAGEMENT OF CLEIDOCRANIAL DYSOSTOSIS 215
FIG. 5. Pre-operative orthopantomogram demonstrating typical dental chaos of retained deciduous teeth, multiple supernumeraries, and unerupted permanent successors.
FIG. 6. Orthopantomogram 6 months after the mandibular operation with improvement in the position of the lower premolars and canines, and further root formation. Note also presence of
fourth molars.
and sought advice for the first time at the age of 16 years because of the retention of his primary dentition, and a generalised feeling of discomfort in his jaws.
Operative technique
The surgical intention in the management of this patient was to effect the eruption of the permanent dentition by removal of all the obstacles from their path. This was
216 BRITISH JOURNAL OF ORAL SURGERY
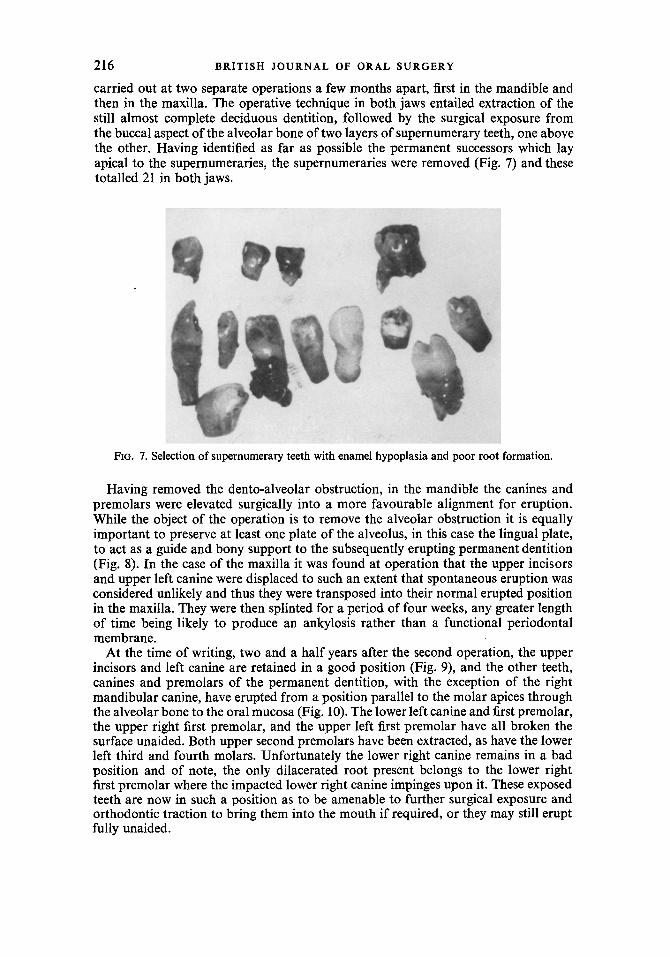
carried out at two separate operations a few months apart, first in the mandible and then in the maxilla. The operative technique in both jaws entailed extraction of the still almost complete deciduous dentition, followed by the surgical exposure from the buccal aspect of the alveolar bone of two layers of supernumerary teeth, one above the other. Having identified as far as possible the permanent successors which lay apical to the supernumeraries, the supernumeraries were removed (Fig. 7) and these totalled 21 in both jaws.
FIG. 7. Selection of supernumerary teeth with enamel hypoplasia and poor root formation.
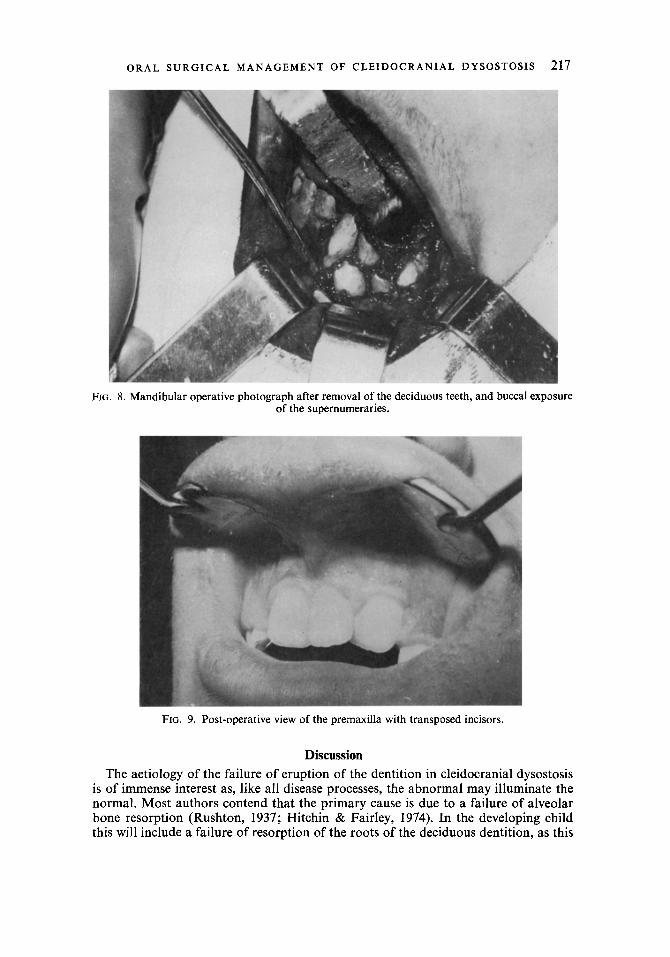
Having removed the dento-alveolar obstruction, in the mandible the canines and premolars were elevated surgically into a more favourable alignment for eruption. While the object of the operation is to remove the alveolar obstruction it is equally important to preserve at least one plate of the alveolus, in this case the lingual plate, to act as a guide and bony support to the subsequently erupting permanent dentition (Fig. 8). In the case of the maxilla it was found at operation that the upper incisors and upper left canine were displaced to such an extent that spontaneous eruption was considered unlikely and thus they were transposed into their normal erupted position in the maxilla. They were then splinted for a period of four weeks, any greater length of time being likely to produce an ankylosis rather than a functional periodontal membrane.
At the time of writing, two and a half years after the second operation, the upper incisors and left canine are retained in a good position (Fig, 9), and the other teeth, canines and premolars of the permanent dentition, with the exception of the right mandibular canine, have erupted from a position parallel to the molar apices through the alveolar bone to the oral mucosa (Fig. 10). The lower left canine and first premolar, the upper right first premolar, and the upper left first premolar have all broken the surface unaided. Both upper second premolars have been extracted, as have the lower left third and fourth molars. Unfortunately the lower right canine remains in a bad position and of note, the only dilacerated root present belongs to the lower right first premolar where the impacted lower right canine impinges upon it. These exposed teeth are now in such a position as to be amenable to further surgical exposure and orthodontic traction to bring them into the mouth if required, or they may still erupt fully unaided.
ORAL SURGICAL MANAGEMENT OF CLEIDOCRANIAL DYSOSTOSIS 217
FIG. 8. Mandibular operative photograph after removal of the deciduous teeth, and buccal exposu of the supernumeraries.
Ire
FIG. 9. Post-operative view of the premaxilla with transposed incisors.
Discussion The aetiology of the failure of eruption of the dentition in cleidocranial dysostosis
is of immense interest as, like all disease processes, the abnormal may illuminate the normal. Most authors contend that the primary cause is due to a failure of alveolar bone resorption (Rushton, 1937; Hitchin & Fairley, 1974). In the developing child this will include a failure of resorption of the roots of the deciduous dentition, as this

BRITISH JOURNAL OF ORAL SURGERY
FIG. 10. Orthopantomogram two and a half years after the maxillary operation with retained upper incisors. Apart from-ji, further eruption and good root formation of the canines and premolars.
Note also calcification of a new supernumerary adjacent 31.
as also brought about by large multinucleated giant cells lying in Howships lacunae on the roots of the deciduous dentition (Scott & Symons, 1967). This concept is supported firstly by the normal appearance of the deciduous dentition, the crowns of which have no bony obstacle in their paths of eruption, and the usually slightly delayed but full eruption of the first permanent molars which only have a thin covering of bone. Secondly by the non-eruption of the permanent incisors, canines, and premolars which, at the chronological times for their eruption, have considerable distance to travel through the investing bone. In addition they normally rely on the shedding of the deciduous teeth for their appearance in the mouth.
Further evidence for this theory is obtained from histological examination of the alveolar bone removed from patients with this disease. Sections of bone supporting deciduous teeth (Hitchen & Fairley, 1974), and further sections from the bone supporting the unerupted third and fourth molars in the case described (Fig. ll), all showed abnormally dense trabeculation with multiple reversal lines, indicating incomplete resorption phases. In addition examination of the roots of the deciduous teeth described by Hitchin and Fairley (1974) showed some areas of resorption but elsewhere areas of dense bone formation and ankylosis.
Finally the frequently reported abnormality of inadequate deformed spike-shaped roots, crown distortion and hypoplasia in areas of compression from adjacent teeth, strongly suggests a disturbance in bony remodelling, to accommodate the developing dentition and later eruption (Rushton 1937; Hitchin & Fairley 1947). Moreover Hitchin (1975) noted histological findings in extracted teeth from patients with cleidocranial dysostosis suggestive of flattening of the epithelial sheath of Hertwig, and that the spiked apices arose from growth of this same sheath into the only space available, namely the bony neuro-vascular canals. In addition those teeth which have been surgically exposed, or by this hypothesis, decompressed (Hitchin & Fairley, 1974), and the case described in this paper, later show normal straight tapering root formation without distortion.
The absence of cellular cementum as originally reported by Rushton (1956) is difficult to elucidate. He observed histologically an almost total absence of this cementum on the roots of the unerupted incisors that were extracted from a patient with cleidocranial dysostosis, and this was true for one erupted lower incisor that was also removed. The deciduous dentition, however, had a normal complement of

ORAL SURGICAL MANAGEMENT OF CLEIDOCRANIAL DYSOSTOSIS 219
FIG. 11. Decalcified section of alveolar bone from the third molar region, showing abnormally dense trabeculation and multiple reversal lines (medium power).
cementum. He also demonstrated cellular cementum in the sectioned roots of unerupted teeth of people not affected by the disease. Normally cellular cementum is a prominent feature of the premolar and molar dentition and tends to be confined to the apical portion of the root, with its thickness increasing apically (Scott & Symons 1967). The fact that in the normal person cellular cementum may be sparse or absent from incisor teeth, that it is predominantly a feature of the apical third, that is, that part of the root which is formed once the tooth has erupted, and that it may be deposited in large amounts with age at the apices to compensate for attrition, suggests a more important role in the process of passive eruption rather than active eruption. Histo- logical examination of four exposed and subsequently functional permanent incisor teeth in a patient with the disease (Hitchin, 1975), demonstrated the presence of normal acellular cementum and definite evidence of formation of some cellular cementum. Smith (1968), however, failed to demonstrate cellular cementum of any consequence on the functional incisor and molar permanent teeth that he extracted from a patient, with cleidocranial dysostosis. Its absence therefore in unerupted teeth in the disease may represent lack of function, compounded by mechanical resistance to its formation from the abnormally dense and totally unyielding alveolar bone. It is also possible that this mechanical factor may be operating in functional teeth, thus accounting for the variation in the reporting of its presence, albeit always of a small amount. However, in the absence of significant numbers of functional teeth for investigation from patients with the disease, the case is not proven and some innate defect of cementum production may co-exist.
The presence of cellular cementum in unerupted teeth from patients not affected by the disease (Rushton, 1956), is not inconsistent, as uneruption here normally implies some form of impaction, and the normal potential to produce some cellular cementum is in this case not inhibited by a failure of bone resorption.
Overactivity of the dental lamina is also a feature of this syndrome producing multiple supernumerary teeth. This will produce mal- or non-eruption in the ordinary
18/3-c
220 BRITISH JOURNAL OF ORAL SURGERY
individual, and thus compounds the problem in cleidocranial dysostosis. It is of interest that the supernumerary teeth tend to be confined to the areas of the jaws supporting the primary dentition. The permanent molars develop from an extension of the same dental lamina as the deciduous dentition, whereas those permanent teeth with deciduous predecessors develop quite differently from a medial extension of the dental lamina. This presumably is under separate genetic control which may be abnormal in this condition.
If the failure of eruption is due to defective alveolar bone resorption, then the logical treatment would be to remove the impediment to eruption, namely, alveolar bone, the deciduous dentition, and the supernumeraries. Once this is done at 11 to 12 years of age, when the permament dentition is fairly advanced in formation, the teeth, contrary to some authors, show considerable ability to erupt. This should be supplemented where necessary by orthodontic traction post-operatively, or transposi- tion at operation if the initial position is deemed unfavourable for eventual eruption of the teeth into occlusion.
The advantages of having one’s own teeth are obvious, and a functional permanent dentition may help to reduce any tendency towards maxillary hypoplasia, but if considerable deformity remains maxillary osteotomy may still be performed. This, however, would be complex in the presence of multiple unerupted teeth and the absence of maxillary air sinuses may still preclude the operation. The prosthetic alternative of an overlay denture to disguise the hypoplastic maxilla as described by Hitchin and Fairley (1974), is also possible when the permanent teeth have erupted. The final support for the method must of course depend on the long-term clinical and radiological appearance of the dentition, but even with failure, this more aggres- sive management avoids the problems of multiple unerupted teeth, dentigerous cyst formation, infection, and potential mandibular fracture; and is more likely to provide a stable alveolus for any future prosthesis.
Acknowledgements
We wish to thank the photographic departments at Queen Mary’s Hospital, Roehampton, and at the Klinik ftir Zahn-, Mund- und Kieferkrankheiten Mtinster, for the preparation of the illustrations, and Frau Bordewick for typing the script.
References
Gorlin, R. J., Pindborg, J. J. & Cohen, N. M. (1976). Syndromes of the head and neck, 2nd Ed., pp. 180-184. New York, Toronto & London: McGraw-Hill.
Hitchin, A. D. & Fairley, J. M. (1974). Dental management in cleidocranial dysostosis. British Journal of Oral Surgery, 12,46.
Hitchin, A. D. (1975). Cementum and other root abnormalities of permanent teeth in cleidocranial dysostosis. British Dental Journal, 139, 313.
Jarvis, J. L. & Keats, I. E. (1974). Cleidocranial dysostosis: A review of 40 new cases. American Journal of Roentgenology, 121, 5.
Kalliala, E. & Taskinen, P. T. (1962). Cleidocranial dysostosis: Report of six typical cases and one atypical case. Oral Surgery, Oral Medicine and Oral Pathology, 15, 808.
Oksala, E. & Fagerstriim, G. (1971). Two stage autotransplantation of fourteen teeth in a patient with cleidocranial dysostosis. &omen Hiimmasliiiikseuran Toimtuksia, 67, 333.
Rushton, M. A. (1937). The failure of eruption in cleidocranial dysostosis. British Dental Journal 63, 641.
Rushton, M. A. (1956). An anomaly of cementum in cleidocranial dysostosis, British Dental Journal, 100,81.
Scott, J. H. & Symons, N. B. B. (1967). Introduction to dental anatomy. 5th Ed., pp. 116, 229. Edinburgh & London: Livingstone.
Smith, N. H. H. (1968). A histologic study of cementum in a case of cleidocranial dysostosis. Oral Surgery, Oral Medicine and Oral Pathology, 25, 470.





























