Embed Size (px)
Citation preview

REVIEWARTICLE
Oral myiasis: case report and review of literature
Pramod Kumar & Virendra Singh
Received: 18 October 2012 /Accepted: 31 October 2012 /Published online: 20 November 2012# Springer-Verlag Berlin Heidelberg 2012
AbstractIntroduction The term myiasis is applied to the injuriousaction that larvae of certain Diptera cause in vertebrateanimals by growing in living or dead tissue. Because of itsgreat destructive potential, appropriate and preventive treat-ment is necessary. Oral myiasis is a rare pathology inhumans and is associated with poor oral hygiene, alcohol-ism, senility, suppurating lesion, severe halitosis, and otherconditions.Method We have presented a case of oral myiasis in amentally challenged patient.Results Reviewing the literature revealed that most of thecases involved the anterior part of the oral cavity of malepatients living in developing or underdeveloped countriesand also that predisposing factors invariably accompaniedinfestation.
Keywords Myiasis . Infestation . Humans
Introduction
Oral myiasis has been a rarely described condition, eventhough it was first mentioned in literature by Laurence in1909 [1]. Myiasis is an infestation of living humans andvertebrate animals with dipterous larvae which, at least for atime, feed on living or dead host tissue, liquid body sub-stances, or undigested food. Myiasis frequently occurs inrural areas, affecting livestock and pets such as dogs and
cats. In humans, it prevails usually in unhealthy individualsmainly from developing and underdeveloped countries[2–4] and uncommonly in the western developed world[5]. Many cases go unreported as a result of “cultural, socialand medico-political reasons” [6].
Myiasis is caused by members of the Muscidae fly familythat lay eggs or larvae on food, necrotic tissue, open wounds,unbroken skin, or mucosa. The classification of myiasis isbased on their localization on the host body (dermal, subder-mal, nasopharyngeal, internal organs, and urogenital [7]) or, inparasitological terms, on the type of host–parasite relationship(obligatory, facultative, or pseudomyiasis). Clinically, theycan also be classified as primary myiasis caused by biopha-gous larvae feeding on living tissue and is rare in humans. Themost common type in humans is the secondary variety causedby necrobiophagous flies feeding on dead tissue in a necroticcavity or lesion [8, 9]. Depending upon the condition ofinvolved tissue, myiasis can also be classified into accidental(larvae ingested along with the food), semispecific (larvae laidon necrotic tissue in wounds), and obligatory (larvae affectingthe undamaged skin).
In this article, we have reviewed oral myiasis by search-ing PubMed for publications. Only articles with sufficientinformation and data are reviewed here to draw any con-clusions (Table 1). A case report is presented to draw atten-tion towards neglect of these patients in poor socioeconomicclasses.
Case report
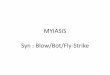
A mentally challenged bedridden 18-year-old female wasbrought by her relatives who had seen “worms” inside theoral cavity of the patient. The patient belonged to an econom-ically backward community of an isolated Indian village withno medical facilities . On examination, it was noted that fewmaggots were peeking from inside a traumatic wound, located
P. Kumar (*)Army Dental Corps, C/O 56 APO,Bathinda, Indiae-mail: [email protected]
V. SinghDepartment of Oral and Maxillofacial Surgery, GDC, PGIMS,Rohtak, Haryana, India
Oral Maxillofac Surg (2014) 18:25–29DOI 10.1007/s10006-012-0373-2

Tab
le1
Caserepo
rtsreview
edfrom
theliterature
Species/references
Patient
age/sex
Country
Num
ber
oflarvae
Underlyingdisorder
Locationof
lesion
Methodof
treatm
ent
Other
antib
iotics
Sarcoph
agi[2]
9/F
Iran
3None
Gingiva
anterior
maxilla
Mechanicalremoval
None
Oestrus
ovis(O
estriae)
[10]
3/M
Iran
5None
Gingiva
anterior
maxilla
Mechanicalremoval
None
Cochilio
mia
hominivorax
(Callip
horidae)
[11]
20/F
Brazil
Multip
leHypotonic
cerebral
palsy
Gingiva
anterior
maxilla
Ivermectin
Cefalotin
Cochilio
mia
hominivorax
(Callip
horidae)
[12]
66/F
Brazil
40Adv
ancedperiod
ontal
disease,chronic
alcoholism
Gingiva
anterior
maxilla
Mechanicalremoval
None
Sarcoph
agi[13]
24/M
Brazil
Multip
leAfter
extractio
nGingiva
anterior
maxilla
Mechanicalremoval
None
Not
mentio
ned[14]
34/M
Brazil
55Neurologicdeficit,op
enbite,mouth
breathing,
poor
oral
hygiene
Gingiva
anterior
maxilla
Mechanicalremoval
None
Cochilio
mia
hominivorax
[15]
a.22
/MBrazil
24Dentalextractio
nMaxillarytoothextractio
nsocket
Ivermectin
,mechanical
remov
alCefazolin,
metronidazole
b.65/M
Not
mentio
ned
Senile,dependent,mouth
breather
Maxillarypalatalregion
Ivermectin
Non
e
Not
mentio
ned[16]
32/M
Brazil
Multip
leAlcohol
dependent,
poor
oral
hygiene
Upper
lipIvermectin
,mechanical
remov
alNon
e,checkgentian
violet
Noparasitological
exam
ination[17]
65/M
Brazil
9Cancrum
oris
Right
side
offace
Treatmentforcancrum
oris,mechanical
debridem
ent
Amox
icillin
and
clavulanic
acid
Cochilio
mia
hominivorax
(Callip
horidae)
[18]
5/F
Brazil
2Incompetent
lips,
malocclusion,
poor
oral
hygiene
Palatal
ging
ivamaxillary
anterior
Mechanicalremov
alAmox
icillin
Musca
domesticus
(Muscidae)
[19]
12/M
India
3Learningdisability,
incompetent
lips,
poor
oral
hygiene
Gingiva
anterior
mandible
Mechanicalremoval
None
Musca
domesticus
(Muscidae)
[20]
45/M
India
Multip
leMalno
urished,
mandibularfracture
Lips,floorof
mou
thTurpentineoil,mechanical
remov
alBroad-spectrum
antib
iotics,
metronidazole
Musca
nebulo
(Muscidae)
[21]
42/F
India
12Neurologicdeficit,trauma,
malocclusion,
period
ontal
disease
Gingiva
anterior
maxillary
Turpentineoil,ivermectin
,mechanicalremov
alNon
e
Chrysom
abezziana
(Callip
horidae)
[22]
89/F
Hon
gKon
g7
Bedridden
afterstroke,
nasogastricfeedingtube,
pulm
onaryTB
Gingiva
anterior
maxilla
Mechanicalremoval
Antibioticsforother
cond
itions
Woh
lfahrtia
mag
nifica
(Sarcophagidae)[23]
19/M
Israel
2None
Gingiva
posteriormandible
Mechanicalremoval
None
Not
mentio
ned[25]
12/F
Oman
8Spasticcerebral
palsy,
incompetent
lips,
anterior
open
bite,
poor
oral
hygiene
Maxillarypalatalregion
Mechanicalremoval
Antibioticsfor
pneumonia
Not
mentio
ned[25]
20/F
Oman
9Cerebralpalsy,bedridden,
malno
urished
Maxillarypalatalregion
Mechanicalremoval
Antibioticsfor
system
iccond
ition
26 Oral Maxillofac Surg (2014) 18:25–29

in the anterior maxillary vestibule region (Fig. 1). In general,oral hygiene was poor with incompetent lips and mouthbreathing. The patient lived in unhygienic conditions, oftenkept in the open near animals and unattended. Using a suffo-cation technique with turpentine oil, the extraction of livingmaggots was done with tweezers under local anesthesia(Fig. 2). The wound was debrided, irrigated with normalsaline, and closed on the second day after inspection. Theparasitological report identified the larvae asMusca domesticaor common housefly. The patient was followed for 3 months,and no fresh episode was seen.
Discussion
When the tissues of the oral cavity are invaded by theparasitic larvae of flies, the oral pathologist names thiscondition oral myiasis. The incidence of oral myiasis com-pared to that of cutaneous myiasis is low as oral tissues arenot permanently exposed to the external environment.
At least 86 different species of Diptera can infect manwith larvae that invade skin and body cavities [10]. Fleshflies exist worldwide and are found in a variety of environ-mental conditions, and the history of travel to an endemicarea by a healthy individual should be kept in mind whilemaking a diagnosis. The number of larvae present in variousreports ranges from few [2] to multiple [11–16] dependingon viable eggs deposited by flies which may be in the rangeof a few hundreds. This in turn will determine the extent ofhost damage. The fly can directly lay eggs on its host ordeliver them to the host by laying them on a vector such as abloodsucking arthropod. Warm and humid conditions of thetropics and subtropics with poor hygiene and lack of
medical care allow flies to breed freely and target suscepti-ble individuals freely. This problem can be identified as themajority of these reports are from developing [2, 10–21]countries and less for developed [22, 23] nations.
The life cycle of M. domestica starts with a female flylaying up to 500 eggs in several batches of about 75 to 150eggs. Eggs hatch within 10–24 h in warm weather. Thelegless maggots feed on decomposing tissues and gothrough three instars to reach full size in 5 days. The maturelarvae are 3 to 9 mm long, creamy white in color, cylindri-cal, with a tapering head. The fully developed larva leavesthe tissues to find a cooler drier environment in which topupate. The pupal stage generally lasts a further 5 days. Theemerging fly escapes from the pupal case through the use ofan alternately swelling and shrinking sac, called the ptilinumon the front of its head, which it uses like a pneumatichammer [24].
Although all age groups may be affected, the damagecaused to infants is more serious and may be fatal [4,23–28]. Most of the published reports involved male patientsprobably due to poor oral hygiene, neglect, increased outdoorwork, or travel to endemic areas when compared to females[10, 13–17, 19, 20, 23]. Also, the anterior part of the oralcavity was more commonly affected than the posteriorbecause it is easily accessible to flies [2, 10–16, 18–23, 25].
Oral myiasis is very rare in healthy growing children andadults [4]; most of the cases described in literature weresecondary to medical or anatomical conditions such as mal-nourished patients [17], neglected fractures [20], cerebralpalsy [8], mouth breathing [14, 15], anterior open bite [14,25], cancrum oris [17], poor oral hygiene [12, 14, 16,18–21, 25], mechanical ventilation [29], patient undergoingradiotherapy [30], person living in close proximity to ani-mals [10], and debilitated patient with neglect of nursing orcustodial personnel [31]. The female patient in our case wasmentally challenged with very poor oral hygiene and mouthbreathing habit. Most likely, she suffered from undiagnosedtrauma, and lack of care in a fly-abundant environment ledto infestation by flies. The diagnosis of myiasis at an earlyFig. 1 Traumatic wound and maggot infestation
Fig. 2 Extracted larvae
Oral Maxillofac Surg (2014) 18:25–29 27

stage can prevent involvement of deeper tissues. This isespecially important in individuals with a low socioeconom-ic level that may be unaware of the oral lesions [19, 25, 32].Moreover, a lack of regular oral care in these patients maycause the lesions to go unnoticed until extensive involve-ment occurs.
Even though myiasis may be self-limiting and nonfatal insome cases, the patient and relatives report with huge psycho-logical distress. Few larvae can destroy vital tissues, inducingserious or even life-threatening hemorrhage [11]. Surgicaldebridement of the wound and extraction of larvae are mostcommonly done under local anesthetic or general anesthesia.The occlusion or suffocation approach forces aerobic larvae tosurface in search of air where they can be removedwith the aidof forceps or tweezers [33]. Some of the agents that have beenused to suffocate are petroleum jelly, heavy oil, beeswax, rawmeat, mineral oil, nail polish, adhesive tape, butter, chewinggum, turpentine oil [20], whitehead varnish [22], native to-bacco leaf [33], chloroform, and ether [34]. In our patient, weused a cotton bud impregnated with turpentine oil which wasplaced at the orifice of the socket for approximately 10 min,forcing the larvae to come to the surface in search of oxygen,making extraction easy. Secondary infection of the wound bybacteria is uncommon because of the bacteriostatic activity inthe gut of larvae, preventing undesirable overgrowth of pyo-genic bacteria [35]. Systemic antibiotics are only necessarywhen secondary infection is known to be present [22, 25].
Recently, topical and oral ivermectin have been usedagainst maggots in humans [14–16]. Ivermectin is a semi-synthetic macrolide given orally in just a single dose of150–200 μg/kg body weight. It is assumed that ivermectinblocks nerve impulses to the nerve endings through therelease of gamma aminobutryic acid, linking to the receptorsand causing palsy and death of maggots.
According to Rossi-Schneider et al. [14], human my-iasis prevention involves fly population control, generalcleanliness, and informing the public that individualsliving in localities without basic sanitation are morepredisposed to infestation. Limiting myiasis directlyrelates to curbing the fly population by efficient wastedisposal supplemented by spraying with an insecticide,providing the patient with a physical barrier, and goodpersonnel and nursing care.
Prognosis, when there are no complications, is good.Although this is not a lethal disorder, knowledge of thisinfestation is necessary for a preventive, diagnostic, andcurative standpoint. Medical personnel dealing with suscep-tible patients must educate the patient, family members, andcaretakers about preventive measures.
Conflict of interest The authors declare that they have no conflictsof interest.
References
1. Laurence SM (1909) Dipterous larvae infection. BMJ 9:882. Erfan F (1980) Gingival myiasis caused by Diptera (Sarcophaga).
Oral Surg Oral Med Oral Pathol 49:148–1503. Shah HA, Dayal PK (1984) Dental myiasis. J Oral Med 39:210–
2114. Lim ST (1974) Oral myiasis: a review. Singapore Dent J 13:33–345. Konstantindis AB, Zamanis D (1987) Gingival myiasis. J Oral
Med 42:243–2456. Lukin LG (1989) Human cutaneous myiasis in Brisbane. A pro-
spective study. Med J Aust 150:2377. Ogbalu OK, Achufusi TG, Adibe C (2006) Incidence of multiple
myiases in breasts of rural women and oral infection in infantsfrom the human warble fly larvae in the humid Tropic-Niger Delta.Int J Dermatol 45:1069–1070
8. Rey L (1991) Paraasitologia, 2nd edn. Editora Guanabara Koogan,Rio de Janerio
9. Ribeiro FAQ, Pereira CSB, Alves A, Marcon MA (2001) Rata-mento da mlfase humana cavitaria com ivermectina oral. Rev BrasOtorrinolaringl 67:755–761
10. Hakimi R, Yazdi I (2002) Oral mucosa myiasis caused by Osterusovis. Arch Iranian Med 5:194–196
11. Shinohara EH, Martini MZ, Oliveira Neto HG, Takahasi A (2004)Oral myiasis treated with ivemectin: case report. Braz Dent J15:79–81
12. Gomez RS, Perdigão PF, Pimenta FJ, Rios Leite AC, Tanosde Lacerda JC, Custódio Neto AL (2003) Oral myiasis byscrewworm Cochliomyia hominivorax. Br J Oral MaxillofacSurg 41:115–116
13. Bozzo L, Lima IA, de Almeida OP, Scully C (1992) Oral myiasiscaused by Sarcophagidae in an extraction wound. Oral Surg OralMed Oral Pathol 74:733–735
14. Rossi-Schneider T, Cherubini K, Yurgel LS, Salum F, FigueiredoMA (2007) Oral myiasis: a case report. J Oral Sci 49:85–88
15. Gealh WC, Ferreira GM, Farah GJ, Teodoro U, Camarini ET(2009) Treatment of oral myiasis caused by Cochliomyia homini-vorax: two cases treated with ivermectin. Br J Oral MaxillofacSurg 47:23–26
16. Abdo EN, Sette-Dias AC, Comunian CR, Dutra CE, Aguiar EG(2006) Oral myiasis: a case report. Med Oral Patol Oral Cir Bucal11:E130–E131
17. Aguiar AM, Enwonwu CO, Pires FR (2003) Noma (cancrum oris)associated with oral myiasis in an adult. Oral Dis 9:158–159
18. de Souza BT, Salvitti Sá Rocha RA, Guirado CG, Rocha FJ,Duarte Gavião MB (2008) Oral infection by Diptera larvae inchildren: a case report. Int J Dermatol 47:696–699
19. Bhatt AP, Jayakrishnan A (2000) Oral myiasis: a case report. Int JPaediatr Dent 10:67–70
20. Lata J, Kapila BK, Aggarwal P (1996) Oral myiasis. A case report.Int J Oral Maxillofac Surg 25:455–456
21. Sharma J, Mamatha GP, Acharya R (2008) Primary oral myiasis: acase report. Med Oral Patol Oral Cir Bucal 13:E714–E716
22. Ng KH, Yip KT, Choi CH, Yeung KH, Auyeung TW, Tsang AC,Chow L, Que TL (2003) A case of oral myiasis due to Chrysomyabezziana. Hong Kong Med J 9:454–456
23. Droma EB, Wilamowski A, Schnur H, Yarom N, Scheuer E,Schwartz E (2007) Oral myiasis: a case report and literaturereview. Oral Surg Oral Med Oral Pathol Oral Radiol Endod103:92–96
24. Roszalina R, Rosalan R (2002) Oral myiasis: case report. Malay-sian J Med Sci 9:47–50
25. al-Ismaily M, Scully C (1995) Oral myiasis: report of two cases.Int J Paediatr Dent 5:177–179
28 Oral Maxillofac Surg (2014) 18:25–29

26. Zumpt F (1965) Myiasis in man and animals in the old world. In:Zumpt F (ed) A textbook for physicians, veterinarians and zoolo-gists. Butterworth and Co. Ltd, London, p 109
27. Schreiber MM, Suhuekmell N, Sampsell J (1964) Human myiasis.JAMA 188:828–829
28. Koh TH (1999) A case report and a role of the internet. J Perinatol19:528–529
29. Yoshitomi A, Sato A, Suda T, Chida K (1997) Nasopharyngealmyiasis during mechanical ventilation. Nihon Kyobu ShikkanGakkai Zassi 35:1352–1355
30. Chung Y, Jung B (2001) Nosocomial submandibular infectionswith dipterous fly larvae. Kor J Parasitol 34:255–260
31. Greenburg (1984) Two cases of human myiasis caused by Phae-nicia sericata (Diptera Calliphoridae) in Chicago area hospitals. JMed Entomol 21:615
32. Dhooria HS, Badhe AG (1984) Oral myiasis: a case report. JIndian Dent Assoc 56:25–27
33. Hubler W, Rudolf A, Dougherty E (1974) Dermal myiasis. ArchDermatol 10:109–110
34. Felices RR, Ogbureke KU (1996) Oral myiasis: report of case andreview of management. J Oral Maxillofac Surg 54:219–220
35. Mac Namara A, Durhan S (1997) Dermatobia hominis in theaccident and emergency department: “I've got you under my skin”.J Accid Emer Med 14:179–180
Oral Maxillofac Surg (2014) 18:25–29 29