-
7/29/2019 Oral ferrous sulfate supplements increase the free
radicalgenerating capacity of feces from healthy vol
1/6
ABSTRACT
Background: Most dietary iron remains unabsorbed and hence
may be available to participate in Fenton-driven free radical
gen-
eration in conjunction with the colonic microflora, leading to
the
production of carcinogens or direct damage to colonocytes.
Objective: Our aims were to measure the proportion of fecal
iron available to participate in free radical generation and
to
determine the effect of an oral supplement of ferrous sulfate
onfree radical generation.
Design: Eighteen healthy volunteers recorded their food
intake
and collected fecal samples before, during, and after 2 wk
of
supplementation (19 mg elemental Fe/d). Total, free, and
weakly
chelated fecal iron were measured and free radical
production
was determined by using an in vitro assay with dimethyl
sulfox-
ide as a free radical trap.
Results: Fecal iron increased significantly during the period
of
supplementation and returned to baseline within 2 wk. The
con-
centration of weakly bound iron in feces (1.3% of total
fecal
iron) increased from 60 mol/L before to 300 mol/L during
supplementation, and the production of free radicals
increased
significantly (40%). Higher-carbohydrate diets were associ-
ated with reduced free radical generation.Conclusion: Unabsorbed
dietary iron may increase free radical
production in the colon to a level that could cause mucosal
cell
damage or increased production of carcinogens. Am J Clin
Nutr1999;69:2505.
KEY WORDS Dietary iron, free radicals, colon cancer,
feces, ferrous sulfate, Fenton chemistry, humans
INTRODUCTION
The epidemiologic evidence supporting a link between colo-
rectal cancer and diet is strong (1). The stem cells of the
colo-
rectal mucosa lie near the complex, potentially mutagenic
envi-
ronment of the fecal stream; an understanding of the effects
ofdiet on the chemistry of fecal material is therefore essential
in
the development of strategies to prevent colorectal cancer.
A
prospective study showed that high iron consumption is
associ-
ated with an increased risk of colorectal cancer (2). Higher
con-
centrations of plasma iron were associated with distal
tumors,
but a high dietary iron intake, independent of red meat con-
sumption, was specifically associated with an increased risk
of
cancer of the proximal colon.
Colorectal carcinoma develops progressively via the ade-
noma-carcinoma sequence that is associated with the
induction
of mutations, first in proliferating crypt cells and
subsequently in
abnormal clones derived from them. Such mutations may be
mediated by fecal mutagens, free radicals, or both. Free
radical
production in fecal incubates is known to depend on diet (3).
In
many systems the production of superoxide and hydrogen per-
oxide by aerobic metabolism is favored by high concentrationsof
suitably chelated iron. Oxygen radicals are known to damage
protein, lipids, and DNA under in vivo conditions, and this
dam-
age has been implicated in the induction of somatic
mutations
that may favor the development of several forms of cancer (4,
5).
Unabsorbed dietary iron enters the colon and in conjunction
with intraluminal bacteria may become available for
participa-
tion in a combination of Haber-Weiss and Fenton-type
reactions
that generate hydrogen peroxide and hydroxyl radicals at the
mucosal surface (68). Hydrogen peroxide or iron may also
enter colonocytes and increase the risk of DNA damage in a
manner similar to that described for immune cells (9), thus
increasing the risk of a mutation, either as an initiating event
or
later in the adenoma-carcinoma sequence. Alternatively,
iron-
mediated reactions may be involved in the conversion of
procar-cinogens to carcinogens within the lumen of the colon (6).
Iron
has also been shown to increase crypt cell proliferation in
rats
treated with a chemical carcinogen (10) and in rats fed
high-fat
diets (11). Even moderate oral iron supplementation has a
signi-
ficant effect on luminal iron concentrations and increases
mucosal cell proliferation in rat colons (12). Intraluminal
iron
might therefore act in the initiation of carcinogenesis by
causing
DNA damage or at the promotion stage by stimulating polyp
growth. The aim of the present study was to test the
hypothesis
that oral iron supplementation can modify the iron content
of
human feces so as to increase the formation of free
radicals.
Oral ferrous sulfate supplements increase the
freeradicalgenerating capacity of feces from healthy
volunteers13
Elizabeth K Lund, S Gabrielle Wharf, Susan J Fairweather-Tait,
and Ian T Johnson
1 From the Institute of Food Research, Norwich Research Park,
Norwich,
United Kingdom.2 Supported by the Ministry of Agriculture,
Fisheries, and Food of England
and Wales.3 Address reprint requests to EK Lund, Institute of
Food Research, Nor-
wich Research Park, Colney, Norwich, NR4 7UA, United Kingdom.
E-mail:
[email protected].
Received April 16, 1998.
Accepted for publication July 2, 1998.
Am J Clin Nutr1999;69:2505. Printed in USA. 1999 American
Society for Clinical Nutrition250
-
7/29/2019 Oral ferrous sulfate supplements increase the free
radicalgenerating capacity of feces from healthy vol
2/6
SUBJECTS AND METHODS
Subject protocol
Ethical approval was obtained from the Research Ethics Com-
mittee of the Norfolk and Norwich Health Care Trust before
the
start of the study. Twenty healthy members of the staff of
the
Norwich Research Park (10 male and 10 female) gave their
writ-
ten, informed consent to participate. Eight men aged 2248 y
(x:
30 y) with a body mass index (in kg/m
2
) of 1834 (x
: 23) and 10women aged 2154 y (x: 37 y) with a body mass index
of 2027
(x: 23) completed the study. Of the 10 female subjects, 3
were
postmenopausal and 2 of these were receiving hormone
replace-
ment therapy. No subjects were taking vitamin or mineral
sup-
plements during, or had taken them for 6 wk before, the
study.
An initial blood sample was taken from all subjects before
final recruitment to the study and sent for routine
biochemical
screening at the Norfolk and Norwich Hospital. Hemoglobin,
red
blood cell count, total hematocrit, mean red cell volume,
and
zinc protoporphyrin were measured by standard methods to
ensure that no volunteers were anemic. Each volunteer was
asked to weigh and record his or her normal food intake
during
the first 7 d of the study. During this period subjects were
also
asked to collect 3 fecal samples according to normal bowel
habit.Subjects then took a 100-mg supplement of FeSO47H2O (pre-
pared as capsules by a hospital pharmacy) every day for 14 d
(subsequent analysis showed that the capsules contained 19
mg
elemental Fe). During the second week of supplementation,
sub-
jects were asked to collect an additional 3 fecal samples.
Food
intake was again recorded, in this case by portion size with
ref-
erence to a set of photographs of standard portions. In the
second
week after the end of supplementation the subjects were
again
asked to collect 3 fecal samples.
Iron content of fecal samples
Fecal samples were weighed and half of the sample was
homogenized in a blender (Stomacher 400; Seward, London)
with an accurately measured volume of deionized water
ofapproximately equal weight to the feces. The homogenized
material was then subsampled for the subsequent measurement
of free radical production and concentrations of
water-soluble
iron, EDTA-chelatable iron, and heme iron.
The total iron concentration of the feces was measured after
the feces collections were freeze-dried and then ashed in
silica
crucibles at 480 C for 48 h. The ash was dissolved in warm,
con-
centrated hydrochloric acid and the solution diluted to an
appro-
priate volume with distilled water. The iron content was
then
measured with an atomic absorption spectrophotometer (PU
9100X; Philips, Cambridge, United Kingdom). Values were cal-
culated from a standard curve and analytic accuracy was con-
firmed by using National Bureau of Standards standard
reference
material 8431 mixed diet (Office of Standard Reference
Materi-als, Washington, DC).
Free iron in feces was assessed by using an adaptation of
the
method described by Simpson et al (13). A preweighed sample
of fecal homogenate containing 5 g feces (wet weight) was
mixed with a measured volume of water to give a final volume
of water plus feces of15 mL. The sample was centrifuged
for 30 min at room temperature at 6000 g and the supernate
collected. The pellet was washed with an additional 10 mL
water and centrifuged and the 2 supernates were combined and
the volume recorded. Readily exchangeable iron was then
assessed in the same sample by washing it an additional 2
times
in 10 mL TE buffer (10 mol tris HCl/L, 1 mmol EDTA/L)/g
sample and then measuring the iron content of the combined
supernates. The iron content of the resultant solutions was
measured by atomic absorption spectrophotometry as described
above. The water content of the fecal samples was calculated
from a subsample by weighing before and after freeze-drying.
Heme iron was measured by the HemoQuant assay (14). In
brief,
20 mg fecal homogenate was weighed accurately beforethe addition
of a solution containing 2.5 mol oxalic acid/L and
90 mmol FeSO4/L at 80 C or 1.5 mol citric acid/L at 80 C and
maintained at 80 C for 90 min. The supernate (0.5 mL) was
mixed with 3 mL ethyl acetateacetic acid and 1 mL potassium
acetate (3 mol/L). The upper phase (1.25 mL) was then mixed
with 0.5 mL 1-butanol and 3.8 mL potassium acetate (3 mol/L)
in 1 mol KOH/L. The upper phase (0.5 mL) was added to phos-
phoric acid (2 mol/L):acetic acid (9:1, by vol). The lower
phase
was then measured by fluorometry at an emission wavelength
of
653 nm by using an excitation wavelength of 402 nm.
Standards
were prepared from cyanomethemoglobin up to a concentration
of 8.87 mmol/L. Oxalic acid removes iron from the porphyrin
ring structures whereas citric acid treatment does not.
Porphyrin
rings do not emit light when iron is bound to them; under
theconditions used in this assay, therefore, heme iron could be
cal-
culated as the difference between the 2 values.
Free radical production in fecal samples
The effect of dietary iron on free radical production in
human
feces was explored by using an assay developed by the method
of Babbs and Gale (7, 15) and based on the following
reaction:
Dimethyl sulfoxide + OH methanesulfinic acid + CH3 (1)
Each fecal subsample (12 g) was incubated overnight in tris-
buffered saline (pH 7.0) containing 5% dimethyl sulfoxide
(0.7
mol/L), glucose (0.1%), and Na2EDTA (50 mmol/L) at 37 C. The
sample was then centrifuged at 900 g for 10 min at room
tem-perature, the supernate removed, and the protein removed as
a
precipitate by lowering the pH to 1.0 for 10 min by adding 12
mol
HCl/L. The pH was then returned to 7.4, the sample was cen-
trifuged at 900 g for 10 min at room temperature, and the
supernate was stored at 20 C before batch analysis of the
methanesulfinic acid content. Standards were prepared
freshly
before each assay, with 075 mmol methanesulfinic acid/L in
the
incubation medium, and both samples and standards were
processed identically. A 2-mL aliquot was mixed well with
0.2
mL H2SO4 (1 mol/L) and then with 1-butanol (4 mL). The upper
phase was mixed with 2 mL sodium acetate buffer (0.5 mol/L,
pH
5.0) and then centrifuged at 500 g for 3 min at room
tempera-
ture before 1.8 mL of the lower aqueous phase was removed.
The
lower aqueous phase was then adjusted to a pH of 2.5 by
addingHCl (1 mol/L) before the addition of Fast Blue BB salt
(0.03
mol/L; Sigma, Dorset, United Kingdom) to form the colored
product diazosulfone acid. Once the color reaction reached a
plateau, after 10 min in the dark, 1.5 mL toluene:1-butanol
(3:1,
by vol) was added and the sample was mixed for 120 s before
sep-
aration of the phases by centrifugation at 500 g for 3 min
at
room temperature. The upper phase was then removed, washed
with 1-butanolsaturated water, and measured by scanning
spec-
trophotometry at a peak absorbance between 340 and 520 nm.
Peak absorbance was invariably between 410 and 420 nm.
FECAL FREE RADICALS AND ORAL IRON 251
-
7/29/2019 Oral ferrous sulfate supplements increase the free
radicalgenerating capacity of feces from healthy vol
3/6
Analysis of dietary intake
Diaries from the initial 7-d weighed-intake measurements
were analyzed with the commercial software package FOOD
BASE (Institute of Brain Chemistry and Human Nutrition,
Queen Elizabeth Hospital for Children, London). A second set
of
diaries was used as reminders to the volunteers to consume
sim-
ilar menus during supplementation as during the period when
fecal samples were collected before supplementation began
and
to check for significant variations from the control diet.
Statistical analysis
The data were analyzed by using the MINITAB statisticalpackage
(release 8, Macintosh version; Minitab Inc, State Col-
lege, PA). The general linear models technique was used to
ana-
lyze the repeated measures of iron concentration and free
radi-
cal production, taking into account between-subject
variation.
Linear regression analysis was used to assess the effect of
diet
on the measured variables and the correlation between
measured
variables.
RESULTS
Initial screening
Mean values for initial hemoglobin concentration,
hematocrit,
mean red cell volume, and zinc protoporphyrin for all
subjectsare summarized in Table 1. Potentially relevant aspects of
the
subjects estimated habitual dietary intakes are given in Table
2.
Iron intakes ranged from 9.0 to 24.7 mg Fe/d in men and from
9.1 to 47.2 mg Fe/d in women. (Two women had exceptionally
high intakes of iron as a result of consuming game.) No
signifi-
cant correlation was found between estimated dietary iron
intake
and any of the indexes measured.
Fecal iron concentrations
Neither the total fecal iron concentration nor heme iron in
feces correlated with dietary iron intake before
supplementation.
The only dietary factor significantly associated with fecal
iron
was dietary starch, which was inversely correlated with the
fecal
iron concentration (r= 0.454, P < 0.05). There was a
tendencyfor fat intake to be positively associated with an
increased fecal
iron concentration (r= 0.419, P = 0.08).
Supplementation with ferrous sulfate caused a highly
signifi-
cant increase in the total iron concentration in feces in both
men
and women. Concentrations returned to baseline within 2 wk
after supplementation ended (Table 3). Just >1% (1.35%)
of
the total iron concentration of feces was in a form that was
likely to be available for participation in free radical
generation
or for mucosal uptake, and this was independent of the total
amount of iron present. Thus, there was a linear relation
between the concentrations of available iron and total iron
in
feces (r= 0.596, P < 0.001):
Available iron = (0.0135 total iron) 1.1 (2)
The increase in both water-soluble and EDTA-chelatable iron
after supplementation with ferrous sulfate was highly
significant
(P < 0.001) in both men and women (Figure 1).
Free radical production
After supplementation there was a significant increase in the
free
radicalgenerating capacity of the fecal samples measured as
molmethanesulfuric acid/kg wet wt feces (P < 0.001; Figure 2).
Analy-
sis of all data collected throughout the experiment showed
signifi-
cant correlations between free radical generation and
water-soluble
iron (r= 0.673, P < 0.001) and between free radical
generation and
EDTA-chelatable iron (r= 0.559, P < 0.001). Before
supplementa-
tion there was no correlation between heme iron concentrations
in
feces and free radical generation, despite some evidence of a
corre-
lation between heme iron concentrations and water-soluble
iron
(r= 0.470, P < 0.05). These effects were not sex dependent
and
there was no significant effect of pre- or postmenopausal state
in
female subjects.
Analysis of the dietary intake data from the women revealed
a
possible inverse correlation between baseline free
radicalgenerat-
ing capacity of feces and the total carbohydrate content of the
diet(r= 0.627, P = 0.05 ). This relation was not significant in
men.
However, in men, the estimated intake of dietary fiber was
inversely
associated with the increase in free radicalgenerating
capacity
caused by the iron supplement (r= 0.711, P < 0.05; Figure
3).
DISCUSSION
Most iron within tissues is bound to protein, but the small
pool of free iron, which is essential for several cellular
252 LUND ET AL
TABLE 1
Hemoglobin, hematocrit, mean red cell volume, and zinc
protoporphyrin concentrations in subjects before the start of
supplementation1
Hemoglobin Hematocrit Mean red cell volume Zinc
protoporphyrin
g/L fL g/g hemoglobin
Women (n = 10) 133.8 2.0 (126147) 0.3815 0.01 (0.3490.431) 89.86
0.80 (87.195.4) 1.85 0.13 (1.32.5)
Men (n = 8) 151.8 2.9 (138164) 0.4280 0.01 (0.3750.459) 92.51
0.79 (90.597.9) 1.74 0.07 (1.42.0)
Both (n = 18) 142.3 11.8 (126164) 0.4035 0.034 (0.3490.431)
91.12 2.74 (87.197.9) 1.80 0.34 (1.32.5)
1x SEM; range in parentheses.
TABLE 2
Subjects daily dietary intakes as calculated from 7-d weighed
intake
diaries1
Men (n = 8) Women (n = 10)
Total energy (kJ/d) 10 217 470 10 878 689
Protein (% of energy) 15.5 0.9 18.7 1.3
Fat (% of energy) 35.8 1.9 31.9 1.9
Carbohydrate (% of energy) 44.2 2.3 44.6 2.2
Starch (% of energy) 26.8 2.0 23.2 1.5
Sugar (% of energy) 17.2 1.2 21.0 1.8
Fiber (g) 15.4 1.7 13.7 1.4
Dietary iron intake (mg Fe/d) 16.4 1.9 26.6 4.4
Phytic acid (g/d) 0.08 0.03 0.08 0.03
1x SEM.
-
7/29/2019 Oral ferrous sulfate supplements increase the free
radicalgenerating capacity of feces from healthy vol
4/6
processes, is known to catalyze free radical production,
partic-
ularly in diseased states. Iron was first proposed as a
potential
carcinogen > 35 y ago (16) and the role of iron in the
etiology
of various cancers has been discussed extensively in 2
review
papers (17, 18). The overall iron status of the body is
tightly
controlled by regulation of iron uptake in the small
intestine.
Once iron stores are replete, dietary iron remains almost
com-
pletely unabsorbed and high concentrations of iron can
develop
in the distal gut lumen after the reabsorption of water. The
hypothesis that the presence of iron in the fecal stream may
lead to the generation of free radicals, and that this effect
may
be procarcinogenic for colorectal cancer, was advanced by
both
Blakeborough et al (6) and Babbs (7). However, the effect oforal
iron intake on the quantity of iron available for free radi-
cal generation in the human fecal stream has not been
reported
previously.
To participate in reactions leading to free radical
production,
iron must be either freely water soluble or readily bound to
small organic ions such as ascorbic acid and citrate. In his
orig-
inal study, Babbs (7) wanted to establish whether reactive
oxy-
gen species could be generated by fecal bacteria in the
presence
of suitably chelated iron. Iron EDTA was used as the source
of
iron in the assay system because EDTA is considerably more
stable than naturally occurring small organic ions. In the
pres-
FECAL FREE RADICALS AND ORAL IRON 253
TABLE 3
Iron concentration of feces before, during, and after
supplementation with ferrous sulfate (100 mg/d)1
Baseline During supplementation After supplementation
Iron concentration
(g/g wet wt)
Men (n = 8) 108.5 6.8a 277.6 30.0b 123.2 25.2a
Women (n = 10) 90.6 10.6a 284.2 44.6b 108.9 17.9b
(g/g dry wt)
Men (n = 8) 369.1
21.7a
969.5
96.5b
465.7
103.6a
Women (n = 10) 352.4 21.7a 985.3 96.7b 391.5 37.8a
1x SEM. Values in the same row with different superscript
letters are significantly different, P < 0.05.
FIGURE 1. Mean (SEM) concentrations of water-soluble iron in
feces and iron that was soluble in the presence of EDTA at pH
7.5 (read-
ily chelatable iron) before (initial), during (supplement), and
after (post)
supplementation with 100 mg FeSO4/d. The increase in both forms
of
iron during supplementation was significant (P < 0.001). Sex
had no
significant effect.
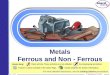
FIGURE 2. Effect of iron supplementation (100 mg FeSO4/d) on
mean (SEM) free radical production in feces determined by
using
methanesulfinic acid (MSA) as an end product in an in vitro
assay. The
increase during iron supplementation was significant (P <
0.001). Sex
had no significant effect.
-
7/29/2019 Oral ferrous sulfate supplements increase the free
radicalgenerating capacity of feces from healthy vol
5/6
ent study, we wished to determine whether an increase in the
concentration of intraluminal iron derived from the oral
routewould lead to any quantifiable variation in free radical
produc-
tion in feces; we therefore used sodium EDTA as the
chelating
agent, to avoid adding iron to the system from an external
source.
The present results clearly indicate that oral iron
supplemen-
tation increases the concentration of fecal iron in a form
poten-
tially available for the generation of free radicals. Using
rat
feces, Babbs (7) showed an increase in free radical
generation
over iron concentrations ranging from 0 to 100 mol/L. In the
present study, we showed that the concentration of
water-soluble
iron is normally equivalent to 25 mol/L in human feces and
that with oral supplementation concentrations rose to
>100
mol/L. If the pool of easily chelatable iron is also available
for
free radical production, then the total concentration of iron in
theactive intraluminal pool rose from 60 to 350 mol/L, which
far
exceeds the concentration required for maximal free radical
pro-
duction in Babbss system (7). It was also clearly established
in
the present study that consumption of 100 mg FeSO4/d was
asso-
ciated with a marked increase in the production of free
radicals
in feces. The mean increase in free radical production was
less
than the rise in the putative active pool of fecal iron, but
this is
explicable if, as the previous results of Babbs (7) suggest,
free
radical production in feces is maximal at 100 mol/L.
The inverse associations between free radical production and
carbohydrate intake in women and fiber intake in men provide
some limited evidence that habitual intake of dietary fiber
may
suppress the production of reactive oxygen species. In a
recent
study, Erhardt et al (3), using a similar approach to measure
freeradical production, reported a significant reduction in the
free
radicalgenerating capacity of feces from volunteers
consuming
high-fiber, low-fat diets compared with low-fiber, high-fat
diets.
This reduction was associated with a 42% reduction in total
fecal
iron. In the present study, we found no effect of fiber on
baseline
total fecal iron concentrations, but starch intake was
negatively
correlated with fecal iron concentrations. The range of
fiber
intakes in our study was low compared with those in the study
by
Erhardt et al (3) and was nearer to the intake of the
low-fiber
group. The fat intake of our subjects was intermediate to that
in
the high- and low-fat diets studied by Erhardt et al (3), as
was
carbohydrate intake. Clarification of such interactions
betweenmajor dietary components, iron concentrations in the feces,
and
free radical production will require more detailed dietary
analy-
sis with a larger number of subjects.
Graf and Eaton (19) suggested that the putative protective
effects of fiber-rich foods against colorectal cancer are not
neces-
sarily due to the carbohydrate constituents of cell walls, but
to the
associated phytate content of plant cells. We attempted to
explore
this hypothesis indirectly by using the information on phytate
con-
tent available in the computerized food database used to
analyze
the food diaries. No relation was found between estimated
habitual
phytate intake and free radicalgenerating capacity, but the
pro-
gram indicated that the reliability of the data on the phytate
content
of foods was low; thus, the findings cannot be regarded as
defini-
tive. A recent in vitro study by Lu et al (20) showed that
lignin canact as a free radical scavenger, yet we found no
reduction in free
radical generation with increasing concentrations of dietary
lignin.
The present results clearly establish that orally
administered
iron increases the rate at which reactive oxygen species are
gen-
erated within fecal material in an artificial in vitro system.
To
what extent do these results provide information relevant to
the
intraluminal environment in vivo? The first obvious
difference
between the 2 systems is that the colonic lumen is
predominantly
anaerobic whereas atmospheric oxygen is available in the in
vitro assay system. However, the existence of a microclimate
near the intestinal mucosal surface is widely recognized, and
it
seems probable that, as Babbs (7) proposed, sufficient
oxygen
tension is present at the mucosal surface to enable the
production
of reactive oxygen species. In rats, intracolonic oxygen
tensionwas reported to be 11.1 mm Hg as determined by mass
spec-
trometry (21), and in a more recent study the mucosal oxygen
tension measured by a surface probe was 9 mm Hg compared
with 65 mm Hg in serosal tissue (22). The pH of the colonic
con-
tents may also affect free radical production. In the
proximal
human colon, the pH of the bulk phase varies between 5.5 and
7 depending on the rate of fermentation of carbohydrate. In
ani-
mal models a microclimate has been shown to exist in the
colon
(23) such that the pH at the mucosal surface is buffered close
to
7.0, the pH used in the in vitro incubations in the present
study.
254 LUND ET AL
FIGURE 3. Inverse correlation between the presence of fiber in
the diet and the increase in the free radicalgenerating capacity of
feces after iron
supplementation in men (P < 0.05).
-
7/29/2019 Oral ferrous sulfate supplements increase the free
radicalgenerating capacity of feces from healthy vol
6/6
FECAL FREE RADICALS AND ORAL IRON 255
The reactions observed in vitro are also dependent on the
presence of small organic molecules that are not present in
vivo.
In our preliminary experiments, no detectable free radical
gener-
ation was found unless EDTA was added to the incubation
medium (data not shown). However, it has been shown that
heme
breakdown products such as bilirubin and biliverdin, which
are
known to be present in the lumen of the large intestine, can
pro-
mote iron-induced free radical generation in vitro (7). Thus,
the
conditions necessary for the generation of oxygen free
radicalsmay well exist in the proximal colon, which is where
epidemio-
logic evidence for an association between iron intake and an
increased risk of bowel cancer has been observed (2). In view
of
the widespread use of iron supplements and the fortification
of
foods as a prophylactic measure against iron deficiency
disor-
ders, further studies on the significance of free radical
produc-
tion in the human fecal stream seem warranted.
REFERENCES
1. Willett WC, Stampfer JM, Colditz GA, Rosner BA, Speizer FE.
Rela-
tion of meat, fat, and fiber intake to the risk of colon cancer
in a
prospective study among women. N Engl J Med 1990;323:
166472.
2. Wurzemann JI, Silver A, Schreinemachers DM, Sandler RS,
Ever-
son RB. Iron intake and risk of colon cancer. Cancer Epidemiol
Bio-
markers Prev 1996;5:5037.
3. Erhardt JG, Lim SS, Bode JC, Bode C. A diet rich in fat and
poor in
dietary fiber increases the in-vitro formation of reactive
oxygen
species in human feces. J Nutr 1997;127:7069.
4. Knekt P, Reunanen A, Takkunen H, Aromaa A, Heli-vaara M,
Hakulinen
T. Body iron stores and risk of cancer. Int J Cancer 1994;56:
37982.
5. Nelson RL, Davis F, Sutter E, Sobin LH, Kikendall JW, Bowen
P.
Body iron stores and risk of colonic neoplasia. J Natl Cancer
Inst
1994;86:45560.
6. Blakeborough MH, Owen RW, Bilton RF. Free radical
generating
mechanisms in the colon: their role in the induction and
promotion
of colorectal cancer. Free Radic Res Commun 1989;6:35967.
7. Babbs CF. Free radicals and the etiology of colon cancer.
Free Radic
Biol Med 1990;8:191200.
8. Graf E, Eaton JW. Dietary suppression of colonic cancerfiber
or
phytate? Cancer 1985;56:7178.9. Buttke TM, Sandstrom PA.
Oxidative stress as a mediator of apo-
ptosis. Immunol Today 1994;15:710.
10. Nelson RL, Yoo JC, Tanure JC, Andrianopoulos G, Misumi
A.
Effect of iron on experimental colorectal carcinogenesis.
Anti-
cancer Res 1989;9:147782.
11. Thompson LU, Zhang L. Phytic acid and minerals: effect
on
early markers of risk for mammary and colon carcinogenesis.
Carcinogenesis 1991;12:20415.
12. Lund EK, Wharf SG, Fairweather-Tait SJ, Johnson IT.
Increases
in the concentrations of available iron in response to dietary
iron
supplementation are associated with changes in crypt c ell
prolif-
eration in rat large intestine. J Nutr 1998;128:1759.
13. Simpson RS, Sidhar S, Peters TJ. Application of selective
extrac-
tion to the study of iron species present in diet and rat
gastroin-
testinal tract contents. Br J Nutr 1992;67:43744.
14. Schwartz S, Dahl J, Ellefson M, Ahlquist D. The
HemoQuant
test: a specific and quantitative determination of heme
(hemo-
globin) in feces and other materials. Clin Chem
1983;29:20617.
15. Babbs CF, Gale MJ. Colorimetric assay for methanesulfinic
acid
in biological samples. Anal Biochem 1987;163:6773.
16. Richmond HG. Induction of sarcoma in the rat by iron
dextran
complex. Br Med J 1959;1:9479.
17. Sahu SC. Dietary iron and cancer: a review. Environ
Carcinog
Ecotox Rev 1992;10:20537.
18. Weinberg ED. The role of iron in cancer. Eur J Cancer Prev
1996;5:1936.
19. Graf E, Eaton JW. Suppression of colonic cancer by
dietary
phytic acid. Nutr Cancer 1993;19:119.
20. Lu F-J, Chu L-H, Gau R-J. Free radical-scavenging properties
of
lignin. Nutr Cancer 1998;30:318.
21. Bornside GH, Donovan WE, Meyers MD. Intracolonic
tensions
of oxygen and carbon dioxide in germfree, conventional, and
gnotobiotic rats. Proc Soc Exp Biol Med 1976;151:43741.
22. Zabel DD, Hopf HW, Hunt TK. The role of nitric oxide in
sub-
cutaneous and transmural gut tissue oxygenation. Shock
1996;5:3413.
23. Rechkemmer G, Wahl M, Kuschinsky W, von Engelhardt W.
pH-
microclimate at the luminal surface of the intestinal mucosa
of
guinea pig and rat. Pflugers Arch 1986;401:3340.