Embed Size (px)
Citation preview
Optimising Flu Recommendations the European View
Angus Nicoll CBE - Head of Influenza Programme
European Society of Clinical Microbiology & Infectious Diseases –Conference on the Impact of Vaccine on Public Health Prague Czech Republic – April 1st-3rd 2011
Aim and Structure of Talk
To take a forward look on flu immunisation in Europe for the next four years
Identifying general issues that apply for all vaccines but relate especially for seasonal influenza vaccination and more specific seasonal influenza issues
What can we learn from the pandemic experience that is relevant to seasonal influenza and immunisation in general?
Acknowledgements - European Influenza Surveillance NetworkGabriela El Belazi, Hubert Hrabcik, Peter Lachner, Reinhild Strauss, Robert Muchl, Theresia Popow – Kraupp,
Françoise Wuillaume, Leen Meulenbergs, Sophie Quoilin, Mira Kojouharova, Rositsa Kotseva, Teodora Georgieva, Avraam Elia, Chryso Gregoriadou, Chrystalla Hadjianastassiou, Despo Pieridou Bagatzouni, Olga Kalakouta, Jan Kyncl, Jitka Castkova, Martina Havlickova, Andreas Gilsdorf, Brunhilde Schweiger, Gabriele Poggensee, Gerard Krause, Silke Buda, Tim Eckmanns, Anne Mazick, Annette HartvigChristiansen, Kåre Mølbak, Lars Nielsen, Steffen Glismann, Inna Sarv, Irina Dontsenko, JelenaHololejenko, Natalia Kerbo, Olga Sadikova, Tiiu Aro, Amparo Larrauri, Gloria Hernandez – Pezzi, PilarPerez – Brena, Rosa Cano – Portero, Markku Kuusi, Petri Ruutu, Thedi Ziegler, Sophie Vaux, Isabelle Bonmarin, Daniel Lévy-Bruhl, Bruno Lina, Martine Valette, Sylvie Van Der Werf, Vincent Enouf, Ian Fisher, John Watson, Joy Kean, Maria Zambon, Mike Catchpole, Peter Coyle, William F Carman, Stefanos Bonovas, Takis Panagiotopoulos, Sotirios Tsiodras Ágnes Csohán, Istvan Jankovics, KatalinKaszas, Márta Melles, Monika Rozsa, Zsuzsanna Molnár, Darina O'flanagan, Derval Igoe, Joan O’donnell, John Brazil, Margaret Fitzgerald, Peter Hanrahan, Sarah Jackson, Suzie Coughlan, Arthur Löve, Gudrun Sigmundsdottir, Isabella Donatelli, Maria Grazia Pompa, Stefania D'amato, Stefania Iannazzo, Sabine Erne, Algirdas Griskevicius, Nerija Kupreviciene, Rasa Liausediene, Danielle Hansen – Koenig, Joel Mossong, Mathias Opp, Patrick Hau, Pierre Weicherding, Antra Bormane, Irina Lucenko, NatalijaZamjatina, Raina Nikiforova, Charmaine Gauci, Christopher Barbara, Gianfranco Spiteri, Tanya Melillo, Adam Meijer, Frederika Dijkstra, Ge Donker, Guus Rimmelzwaan, Paul Bijkerk, Simone Van Der Plas,Wim Van Der Hoek, Katerine Borgen, Susanne Dudman, Siri Helene Hauge, Olav Hungnes, AnetteKilander, Preben Aavitsland, Andrzej Zielinski, Lidia Brydak, Magdalena Romanowska, MalgorzataSadkowska – Todys, Maria Sulik, Carlos Manuel Orta Gomes, Jose Marinho Falcao, Raquel Guiomar, Teresa Maria Alves Fernandes, Adriana Pistol, Emilia Lupulescu, Florin Popovici, Viorel Alexandrescu, Annika Linde, Asa Wiman, Helena Dahl, Malin Arneborn, Mia Brytting, Eva Grilc, Irena Klavs, Katarina Prosenc, Maja Socan, Hana Blaskovicova, Margareta Slacikova, Mária Avdicová, Martina Molcanová, Šárka Kovácsová
ECDC: Ammon A, Amato Gauci AJ, Zucs P, Snacken R, Ciancio B, Plata F, Broberg E, Nicoll A.
Acknowledgements
Thomas Abraham – China & WHO adviser
Centers for Disease Prevention and Control - USA
Department of Health (London) & the Health Protection Agency
John Spika and Public Health Agency of Canada
Darina O’Flanagan, Jolita Merecikene & VENICE
Yuelong Shu and China CDC – newest WHO Flu Collaborating Centre
WHO–HQ Tony Mounts, Sylvie Briand, Keiji Fukuda
WHO-Copenhagen Caroline Brown, Josh Mott
ECDC Influenza and Vaccine Preventable Disease Teams: Andrew Amato, Eeva Broberg, Bruno Ciancio, Johan Geiseke, Piotr Kramarz, Pierluigi Lopalco, Kari Johansen, Vicente Lopez, Giovanni Mancarella, Ulla-Karin Nurm, Pasi Penttinen, Flaviu Plata, Rene Snacken, J Todd Weber, Philip Zucs.
But Angus Nicoll takes responsibility for the comments
Declaration of Interest
I have no conflict of interest I am aware of – see ECDC Transparencyfor ECDC’s influenza programme team
Janusthe god of gates, doors, doorways, endings & beginnings
7
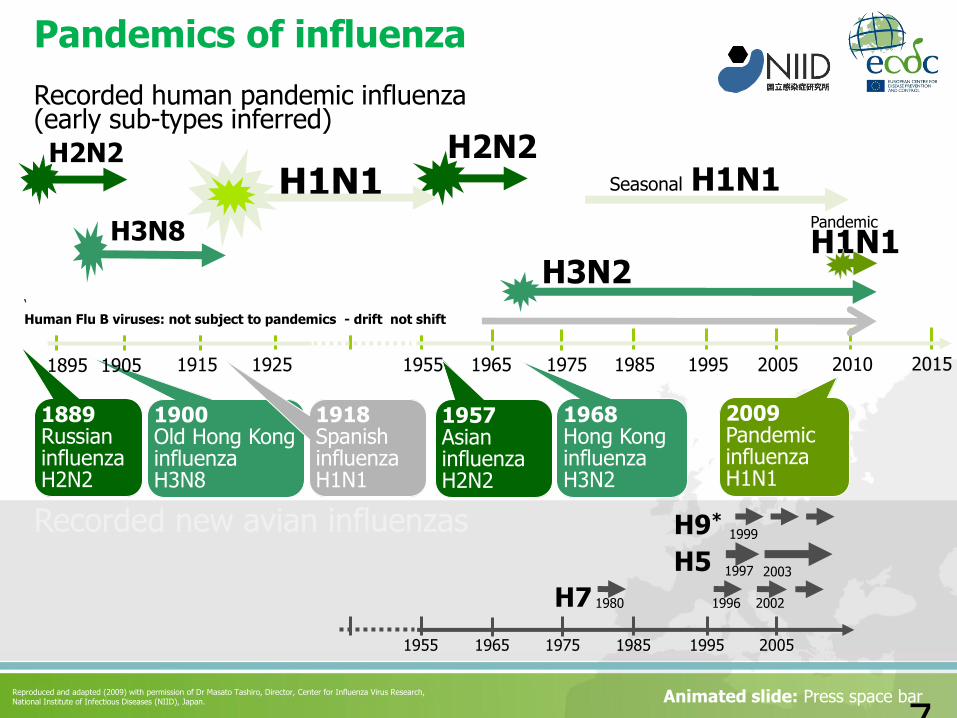
Pandemics of influenza
H7
H5
H9*
1980
1997
Recorded new avian influenzas
1996 2002
1999
2003
1955 1965 1975 1985 1995 2005
Seasonal H1N1H2N2
1889RussianinfluenzaH2N2
H2N2
1957AsianinfluenzaH2N2
H3N2
1968Hong KonginfluenzaH3N2
H3N8
1900Old Hong Kong influenzaH3N8
1918SpanishinfluenzaH1N1
1915 1925 1955 1965 1975 1985 1995 20051895 1905 2010 2015
2009PandemicinfluenzaH1N1
Recorded human pandemic influenza(early sub-types inferred)
Reproduced and adapted (2009) with permission of Dr Masato Tashiro, Director, Center for Influenza Virus Research, National Institute of Infectious Diseases (NIID), Japan. Animated slide: Press space bar
H1N1Pandemic
H1N1
‘
Human Flu B viruses: not subject to pandemics - drift not shift
Consequences of this: • Most influenza morbidity/mortality between pandemics
• Historically there has usually been a single group of A viruses plus B viruses in the interpandemic periods1
• Then an A(H1N1) remerged in 1977 and so there were two groups of influenza A viruses 1977 to 2008.
• A pandemic changes the seasonal influenza A viruses – often with significant consequences
• Between pandemics the viruses do not stand still - for examples emergence of the Fujian strain of A(H3N2) in 2003/4 and oseltamivir resistant A(H1N1) in Europe 2007/82,3
1. Kilbourne ED. Influenza pandemics of the 20th century. Emerg Infect Dis. 2006 Jan. Available from http://www.cdc.gov/ncidod/EID/vol12no01/05-1254.htm
2. CDC Update: Influenza Activity United States and Worldwide, 2003--04 Season, and Composition of the 2004--05 Influenza Vaccine MMWR July 2, 2004 / 53(25);547-552 http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5325a1.htm
3. Meijer A, et al. Oseltamivir-resistant influenza A (H1N1) virus, Europe, 2007–08 season. Emerg Infect Dis. 2009 April; http://www.cdc.gov/eid/content/15/4/552.htm
2010 onwards - a most exciting time – the first ‘new’ seasonal influenza since 1970
What is it going to be like?
• Will it be like old seasonal influenza?
• Who will be at risk of severe disease?
– those with chronic conditions? Older people? Children? Pregnant women?
• The social, and political impact of the 2009 pandemic – which varies by country
We just don’t know yet!
Well so far in this inter-pandemic period?
What has it been like (2010-2011)?
It has been different from before the pandemic!
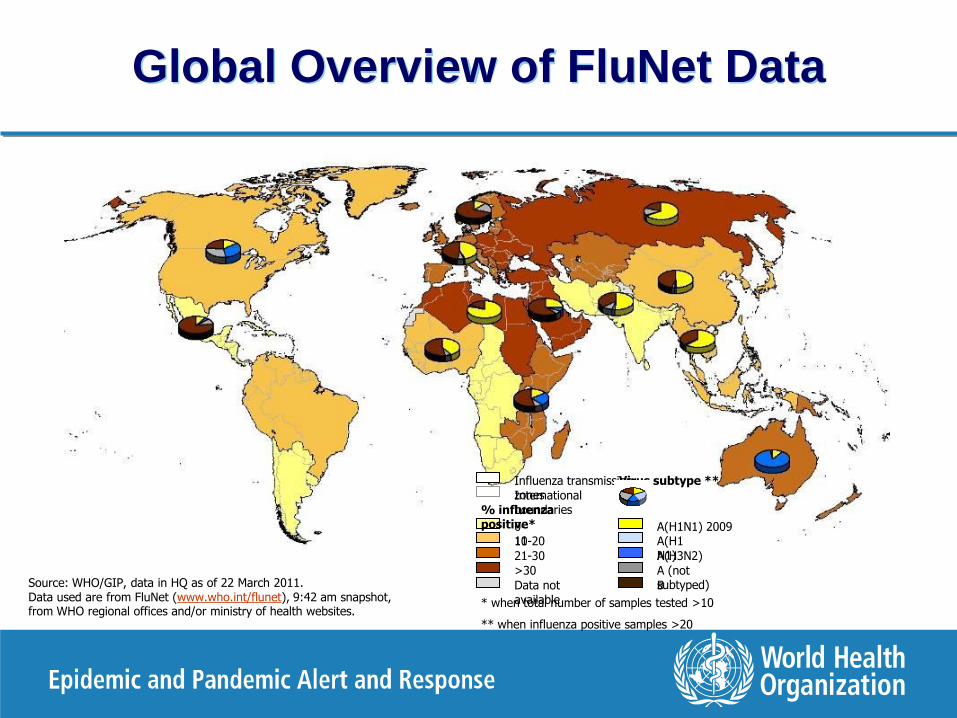
Source: WHO/GIP, data in HQ as of 22 March 2011.Data used are from FluNet (www.who.int/flunet), 9:42 am snapshot, from WHO regional offices and/or ministry of health websites.
0-1011-20
% influenza positive*
21-30
>30
Data not available
Influenza transmission zonesInternational boundaries
A(H1N1) 2009A(H1N1)A(H3N2)
A (not subtyped)B
* when total number of samples tested >10
** when influenza positive samples >20
Virus subtype **
Map_data_zone_global.PercAH1N1
Map_data_zone_global.PercAH1
Map_data_zone_global.PercAH3
Map_data_zone_global.PercANOTSUBTYPED
Map_data_zone_global.PercB
Global Overview of FluNet Data
The Viral Mix has changed
In Europe 2010-2011
• The old seasonal A(H1N1) viruses have gone – and with them most of the oseltamivir resistance
• The B Viruses are still there – both Victoria and Yagamata
• But what about the ‘nasty’ A(H3N2) ?
• …. and A(H1N1)2009 - the pandemic virus?
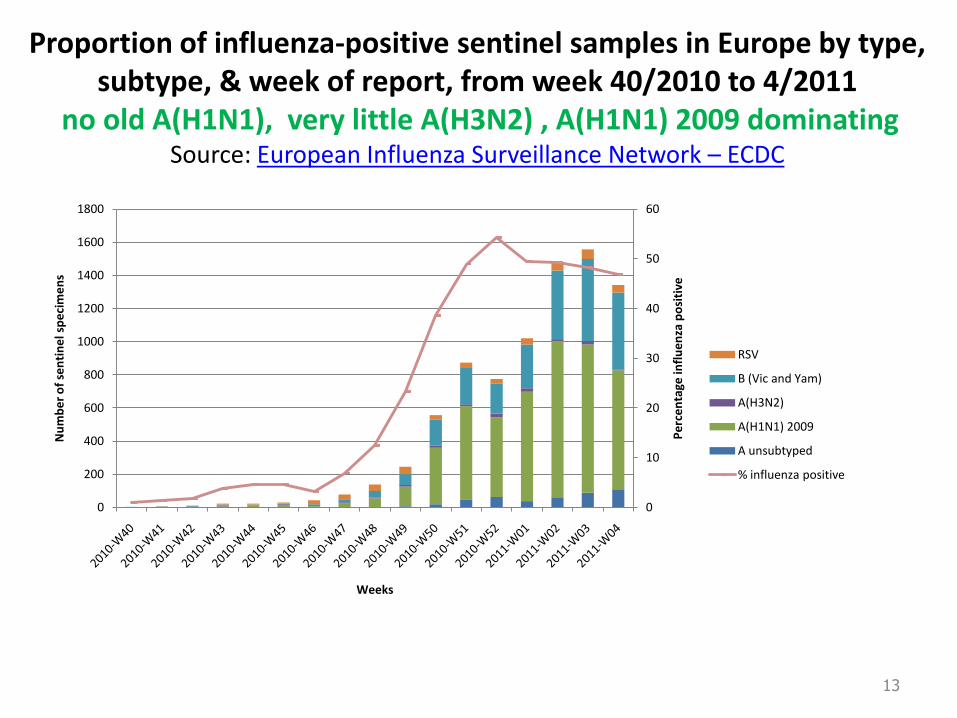
Proportion of influenza-positive sentinel samples in Europe by type, subtype, & week of report, from week 40/2010 to 4/2011
no old A(H1N1), very little A(H3N2) , A(H1N1) 2009 dominatingSource: European Influenza Surveillance Network – ECDC
13
0
10
20
30
40
50
60
0
200
400
600
800
1000
1200
1400
1600
1800
Weeks
Pe
rce
nta
ge in
flu
en
za p
osi
tive
Nu
mb
er
of
sen
tin
el s
pe
cim
en
s
RSV
B (Vic and Yam)
A(H3N2)
A(H1N1) 2009
A unsubtyped
% influenza positive
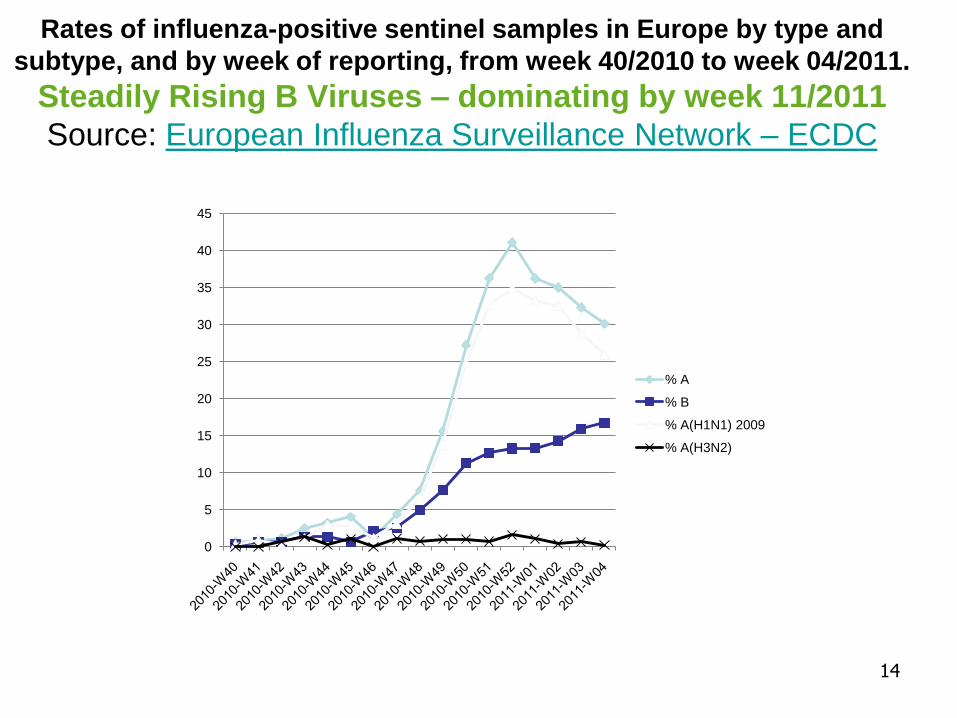
Rates of influenza-positive sentinel samples in Europe by type and
subtype, and by week of reporting, from week 40/2010 to week 04/2011.
Steadily Rising B Viruses – dominating by week 11/2011
Source: European Influenza Surveillance Network – ECDC
14
0
5
10
15
20
25
30
35
40
45
% A
% B
% A(H1N1) 2009
% A(H3N2)
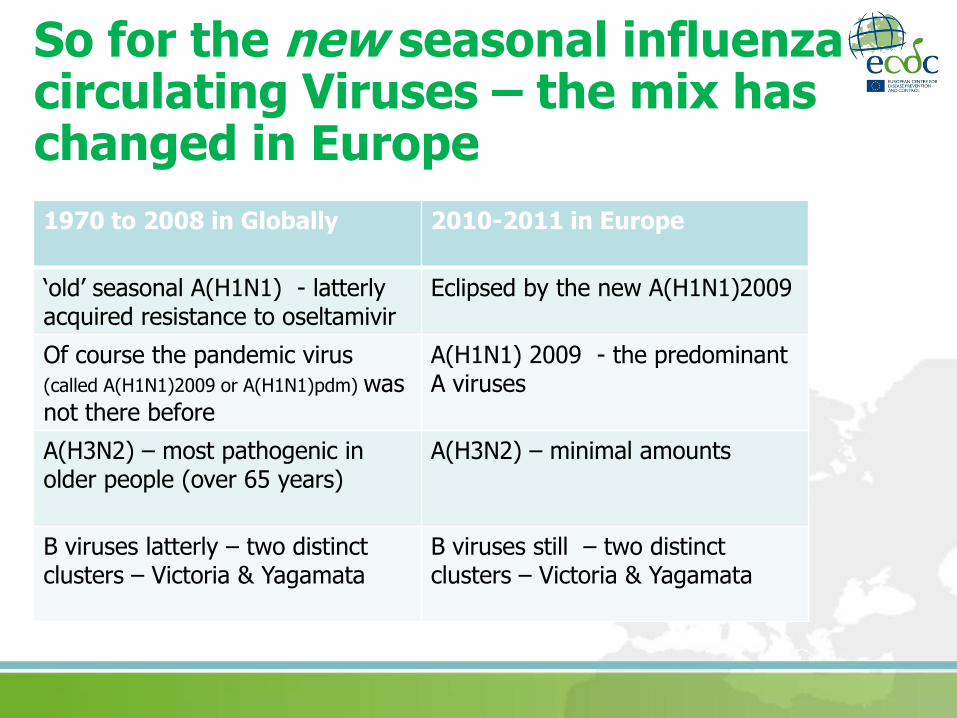
So for the new seasonal influenza circulating Viruses – the mix has changed in Europe
1970 to 2008 in Globally 2010-2011 in Europe
‘old’ seasonal A(H1N1) - latterlyacquired resistance to oseltamivir
Eclipsed by the new A(H1N1)2009
Of course the pandemic virus (called A(H1N1)2009 or A(H1N1)pdm) was not there before
A(H1N1) 2009 - the predominant A viruses
A(H3N2) – most pathogenic in older people (over 65 years)
A(H3N2) – minimal amounts
B viruses latterly – two distinct clusters – Victoria & Yagamata
B viruses still – two distinct clusters – Victoria & Yagamata

Has the change in the viral mix mattered?
Yes – because there has been a change in the clinical and epidemiological pattern
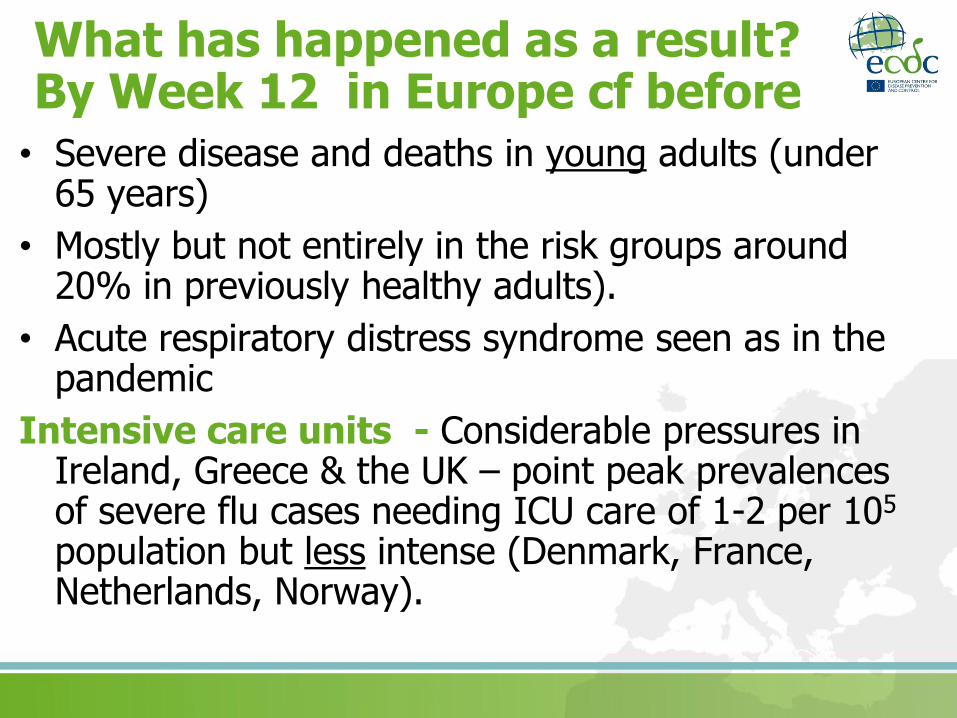
What has happened as a result? By Week 12 in Europe cf before
• Severe disease and deaths in young adults (under 65 years)
• Mostly but not entirely in the risk groups around 20% in previously healthy adults).
• Acute respiratory distress syndrome seen as in the pandemic
Intensive care units - Considerable pressures in Ireland, Greece & the UK – point peak prevalencesof severe flu cases needing ICU care of 1-2 per 105
population but less intense (Denmark, France, Netherlands, Norway).
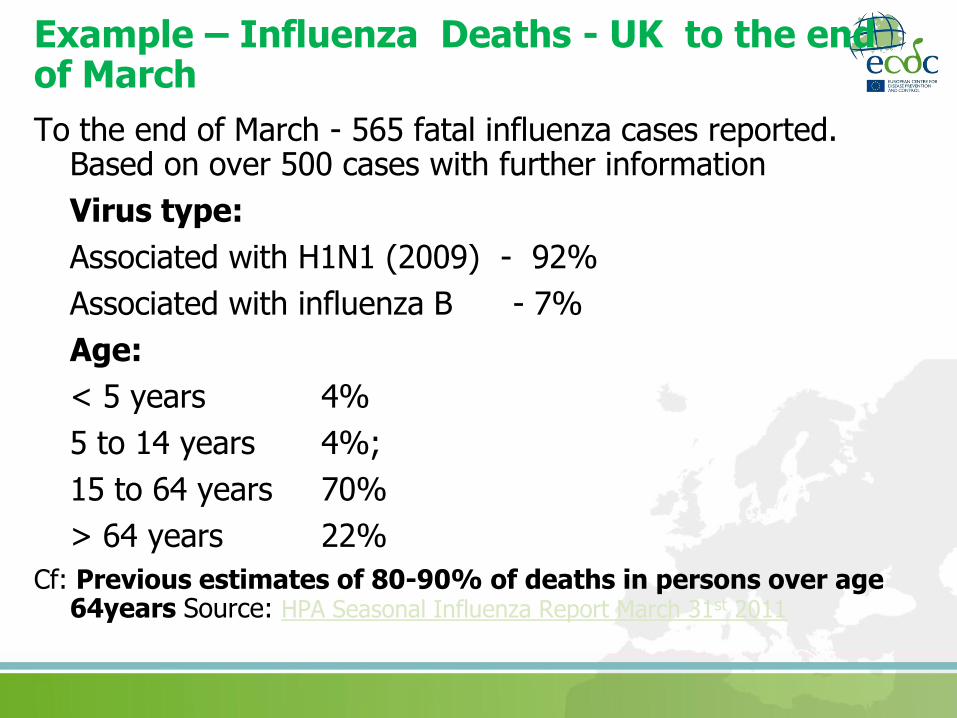
Example – Influenza Deaths - UK to the end of March
To the end of March - 565 fatal influenza cases reported. Based on over 500 cases with further information
Virus type:
Associated with H1N1 (2009) - 92%
Associated with influenza B - 7%
Age:
< 5 years 4%
5 to 14 years 4%;
15 to 64 years 70%
> 64 years 22%
Cf: Previous estimates of 80-90% of deaths in persons over age 64years Source: HPA Seasonal Influenza Report March 31st 2011
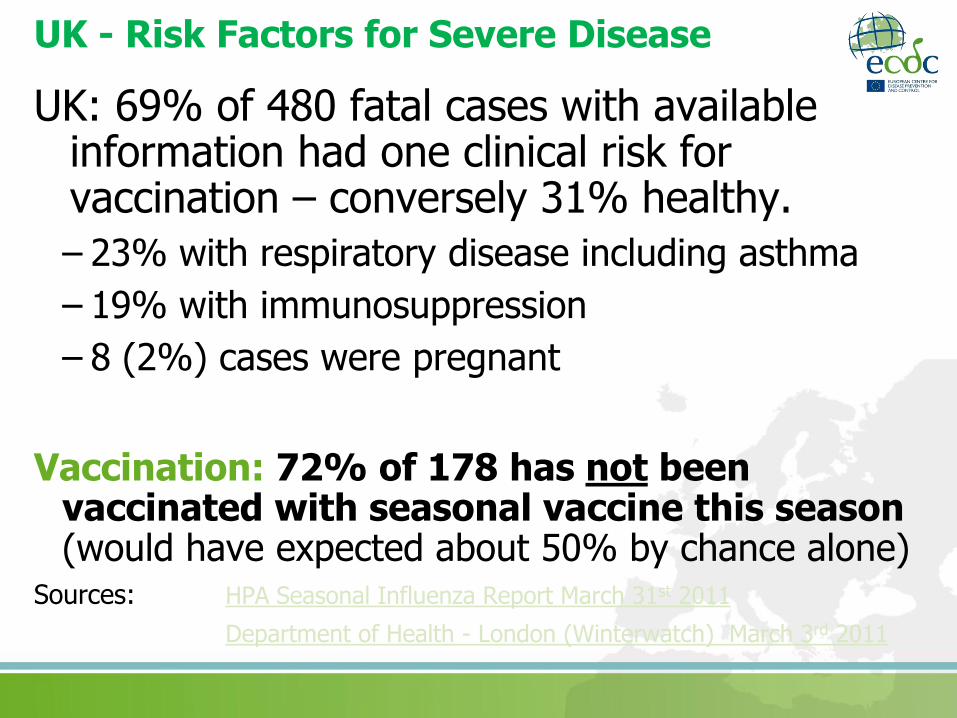
UK - Risk Factors for Severe Disease
UK: 69% of 480 fatal cases with available information had one clinical risk for vaccination – conversely 31% healthy.
– 23% with respiratory disease including asthma
– 19% with immunosuppression
– 8 (2%) cases were pregnant
Vaccination: 72% of 178 has not been vaccinated with seasonal vaccine this season (would have expected about 50% by chance alone)
Sources: HPA Seasonal Influenza Report March 31st 2011
Department of Health - London (Winterwatch) March 3rd 2011
What has the vaccine effectiveness been in the 2010-2011 Season?
2010/11 influenza vaccine effectiveness ranged between 43% and 65% in preventing mild laboratory confirmed influenza infections.
Preliminary results come from an ECDC-funded network of European studies.
The Influenza Monitoring Vaccine Effectiveness in Europe (I-MOVE) is a network funded by the ECDC and coordinated by EpiConcept to monitor seasonal and pandemic influenza vaccine effectiveness
These estimates are somewhat less than for the adjuvanted pandemic vaccines in 2009-2010 season
See Puig-Barberà J. 2010-2011 influenza seasonal vaccine, preliminary mid-season effectiveness estimates: reason for concern, confounding or are we following the right track?. Euro Surveill. 2011;16(11):pii=19821. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19821
Sources: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19821http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19820 http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19818http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19799 http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19791
One of the lessons of the pandemic
Severe end (hospital) and mortality influenza surveillance is weak in many EU countries - Europe does not have good data on this routinely
What has happened? By Week 5 UK and Ireland
• The impact was first on higher level (intensive) care services (UK). They coped - but pressures were well above the pandemic peak. In the UK 1.4/105
prevalent ITU flu cases cases, in Ireland 1.1/105
• Community consultations rose above autumn 2009 pandemic levels
• Young adults (under 65 years) dying from flu -mostly in clinical risk groups but also some healthy individuals (20%)
• In UK an increase in two invasive bacterial infections and all cause all age mortality – again not seen in the pandemic – but unclear if either related to flu
Rise in invasive bacterial infections in the UKSeen in UK only so far where
Coincided with the rise in severe influenza cases and similar age groups
Confined to invasive Group A Strep (iGAS) and Pneumococci
Not seen for Staph, Haemophilus. Invasive Meningococci has risen but just returning to baseline after a very low year in 2009
Group A Strep are mostly emm1 one of the commoner types
A limited number of proven dual infections (iGAS and influenza) – but unclear if higher risk
Anecdotal but persuasive reports from ITU physicians of severe cases of influenza deteriorating very quickly with invasive bacerial disease
Medical authorities issued an alert to all doctors http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_123647.pdf
ECDC has looked elsewhere in Europe - contact Aftab Jasir [email protected] – has not found evidence of the same – but has more found a weakness of surveillance for these invasive bacterial diseases and the capability of integrating bacterial surveillance with data on influenza
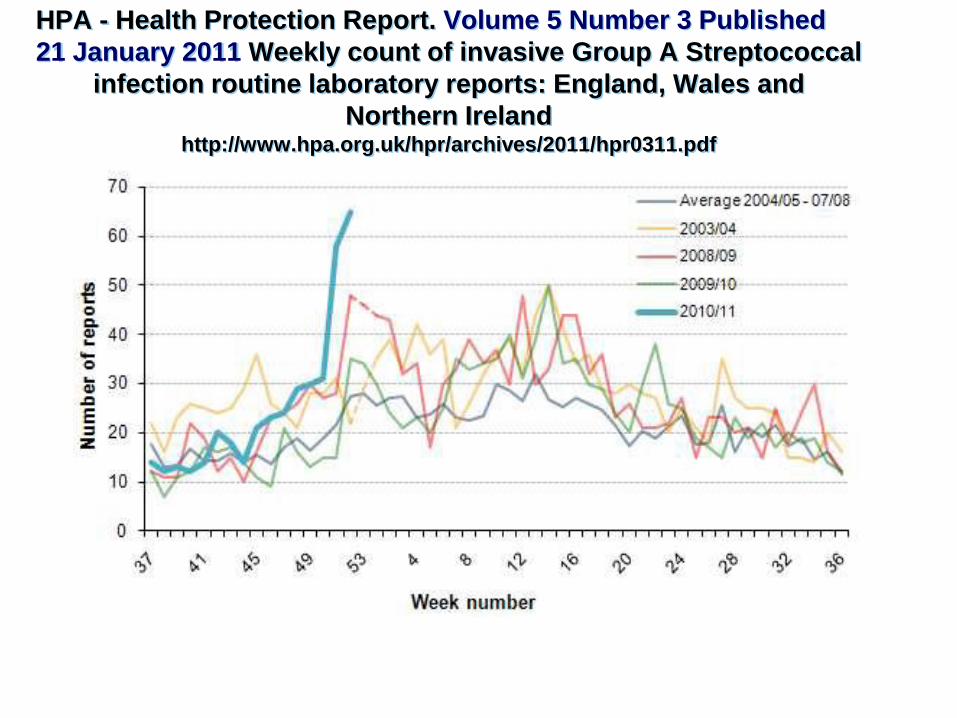
HPA - Health Protection Report. Volume 5 Number 3 Published
21 January 2011 Weekly count of invasive Group A Streptococcal
infection routine laboratory reports: England, Wales and
Northern Ireland http://www.hpa.org.uk/hpr/archives/2011/hpr0311.pdf
Well that is it for Europe – what about elsewhere in the world
It has been different!
Guidelines | 27 July 2006|
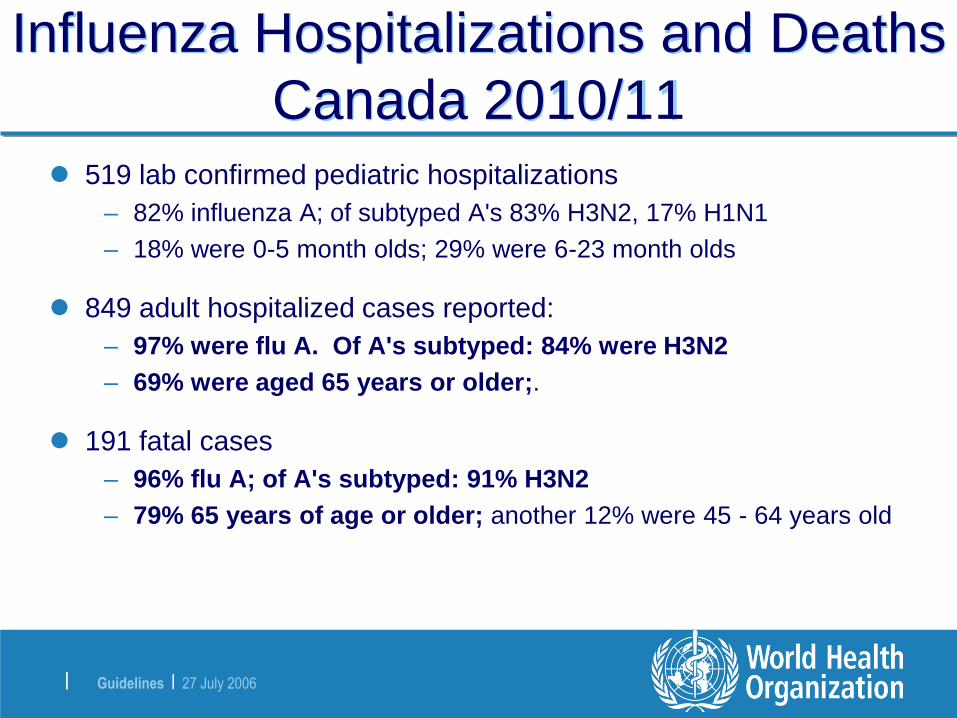
Influenza Hospitalizations and Deaths
Canada 2010/11 519 lab confirmed pediatric hospitalizations
– 82% influenza A; of subtyped A's 83% H3N2, 17% H1N1
– 18% were 0-5 month olds; 29% were 6-23 month olds
849 adult hospitalized cases reported:
– 97% were flu A. Of A's subtyped: 84% were H3N2
– 69% were aged 65 years or older;.
191 fatal cases
– 96% flu A; of A's subtyped: 91% H3N2
– 79% 65 years of age or older; another 12% were 45 - 64 years old
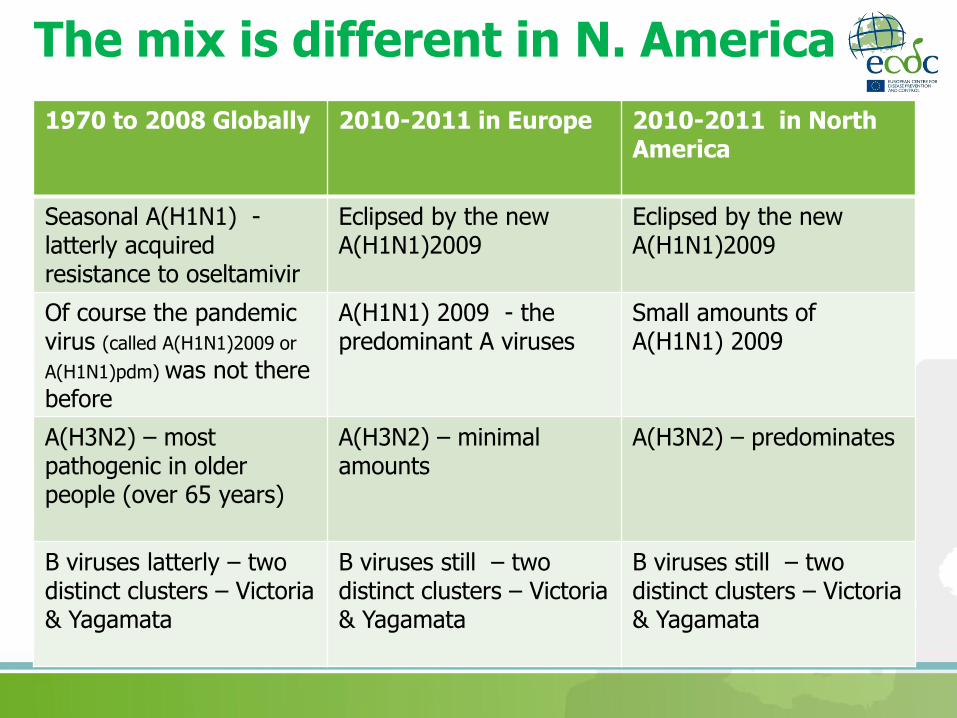
The mix is different in N. America
1970 to 2008 Globally 2010-2011 in Europe 2010-2011 in NorthAmerica
Seasonal A(H1N1) -latterly acquired resistance to oseltamivir
Eclipsed by the newA(H1N1)2009
Eclipsed by the newA(H1N1)2009
Of course the pandemic virus (called A(H1N1)2009 or
A(H1N1)pdm) was not there before
A(H1N1) 2009 - the predominant A viruses
Small amounts of A(H1N1) 2009
A(H3N2) – most pathogenic in older people (over 65 years)
A(H3N2) – minimal amounts
A(H3N2) – predominates
B viruses latterly – two distinct clusters – Victoria & Yagamata
B viruses still – two distinct clusters – Victoria & Yagamata
B viruses still – two distinct clusters – Victoria & Yagamata

And somewhere in between in N. Asia (Northern China) in 2010-20112010-2011 in Europe 2010-2011 in North
America 2010-2011 in North Asia (N. China)
Old A(H1N1) Eclipsed by the new A(H1N1)2009
Old A(H1N1) Eclipsed by the new A(H1N1)2009
Old A(H1N1) Eclipsed by the new A(H1N1)2009
A(H1N1) 2009 - the predominant A viruses
Small amount of A(H1N1)2009
Late appearance and then rise in A(H1N1)2009
A(H3N2) – minimal amounts
A(H3N2) – predominates A(H3N2) predominated initially but as it subsided A(H1N1)2009 rose
B viruses continue to be important still – two distinct clusters – Victoria & Yagamata
B viruses still – two distinct clusters – Victoria & Yagamata
B viruses still – two distinct clusters – Victoria & Yagamata
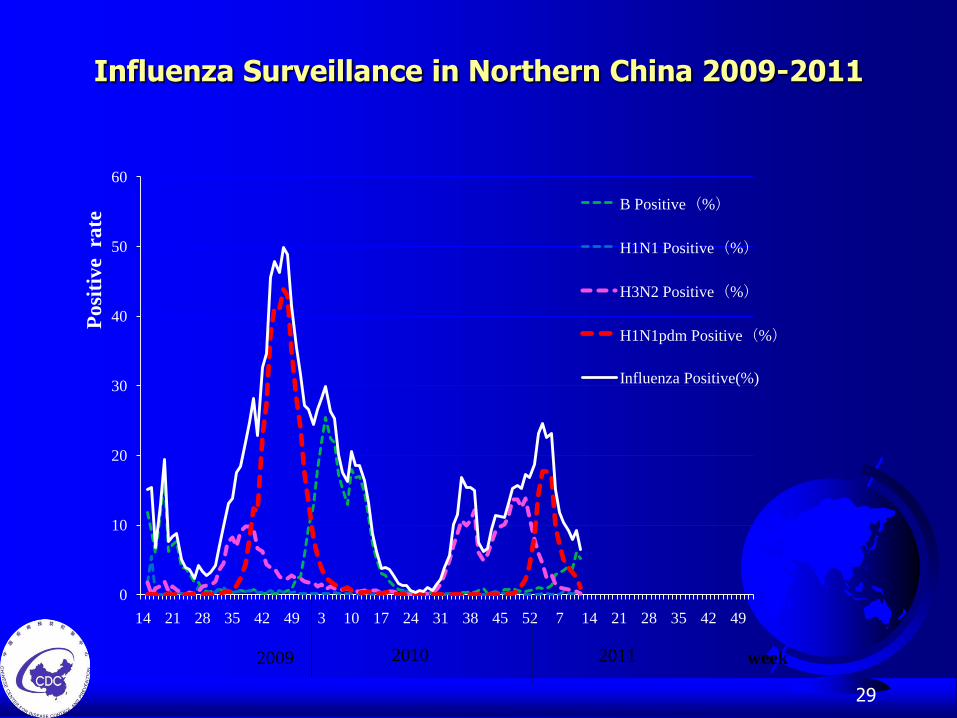
Influenza Surveillance in Northern China 2009-2011
29
0
10
20
30
40
50
60
14 21 28 35 42 49 3 10 17 24 31 38 45 52 7 14 21 28 35 42 49
Po
siti
ve
ra
te
week
B Positive(%)
H1N1 Positive(%)
H3N2 Positive(%)
H1N1pdm Positive(%)
Influenza Positive(%)
2009 20112010
Characteristics of pandemic influenza H1N1 2009 deaths and severe disease
Mainland China 2011 to end March 2011
Influenza Deaths: 66 fatal influenza cases reported
Mainly in middle-aged and younger adults. 51/66 (77.3%) aged 15 to 64 years .
Of 62 with relevant information, 10 were pregnant and another 31 had underlying condition (such as hypertension, diabetes, cirrhosis, etc.). Of the 62 one had received seasonal influenza vaccination, 1 had received pandemic influenza H1N1 2009 vaccination,
Other severe cases: 172 cases : 105 (62.%) were in age-group 15 to 64 years .
Of 115 with relevant information, 16 were pregnant, 35 had other underlying condition (such as hypertension, diabetes, Chronicbronchitis, etc.). 6 had received seasonal influenza vaccineation, 1 had received pandemic influenza H1N1 2009 vaccine,
An advantage for Europe … most years
Predominant West to East Progression of Seasonal Influenza Paget J, Marquet R, Meijer A, van d V. Influenza activity in Europe during eight seasons (1999-2007): an evaluation of the indicators used to measure activity and an assessment of the timing, length and course of peak activity (aspreada) across Europe. BMC Infect Dis. 2007;7(1):141. http://www.biomedcentral.com/1471-2334/7/141
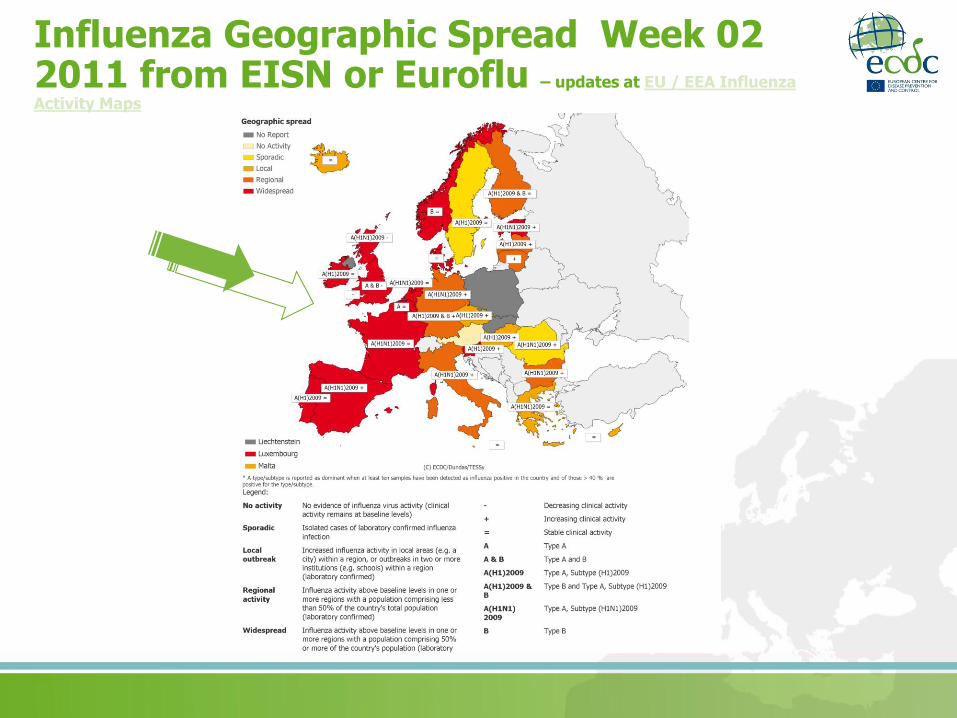
Influenza Geographic Spread Week 02 2011 from EISN or Euroflu – updates at EU / EEA Influenza
Activity Maps
Consequence - can look at each seasons influenza in the West to inform the rest
This was done in 2010-2011
• Initial ECDC Risk Assessment
• WHO-UK-HPA-ECDC Clinicians Teleconferences
• Communication via ESCMID / ERS / ESPID / European Intensivists
• An approach later recommended by the Fineberg Committee!
Fineberg Preview of the Report of the Review Committee on the Functioning of the International Health Regulations (2005) and on Pandemic Influenza A (H1N1) 2009 March 2011 http://www.who.int/ihr/preview_report_review_committee_mar2011_en.pdf

ECDC Interim Risk Assessment – January 2011
http://wwwU.ecdc.europa.eu/en/publications/Publications/110125_RA_Seasonal_Influenza_EU-EEA_2010-2011.pdf
34
Antiviral Resistance 2010-2011
Background – little use of antivirals in Europe overall
In the UK there was more use this year following the severe cases and encouragement from the authorities
Some freely transmitting oseltamivir resistant A(H1N1)2009 cases. Three out of the 27 observed so far in the UK had no known exposure to oseltamivir and were community acquired – see Lazenby et al Eurosurveillance 2011 http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19784
All A(H1N1)2009-H275Y mutation
Needs careful watching

Well if that is the virology, clinical picture and epidemiology
What about the response?

European Council Recommendation on seasonal influenza vaccination 2009 a major step forward
Council Recommendation – an EU Commitment by all the Health Ministers December 2009
Council of the European Union. Council Recommendation of 22 December 2009 on seasonal influenza vaccination (Text with EEA relevance)(2009/1019/EU). Official Journal of the European Union. 2009. L 348/71. Available from: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2009:348:0071:0072:EN:PDF
European Commission and the Swedish EU Presidency Played major roles to get this through
The EU Council Recommendation on Seasonal Influenza Vaccination – Dec 2009
Some Content Link Here
• Reach a target of 75 % vaccination coverage of the older age groups recommended by the WHO as early as possible and preferably by the 2014-2015 winter season.
• This target of 75 % should, if possible, be extended to the risk group of people with chronic conditions,
• Also improve immunisation in health care workers
• Take into account guidance issued by the European Centre for Disease Prevention and Control
For the Council
A CARLGREN (President)
Official Journal of the European Union
December 29th 2009 L 348/71
3

So how is Europe (EU/EEA) doing?
Vaccine Coverage – this relies on the VENICE collaboration
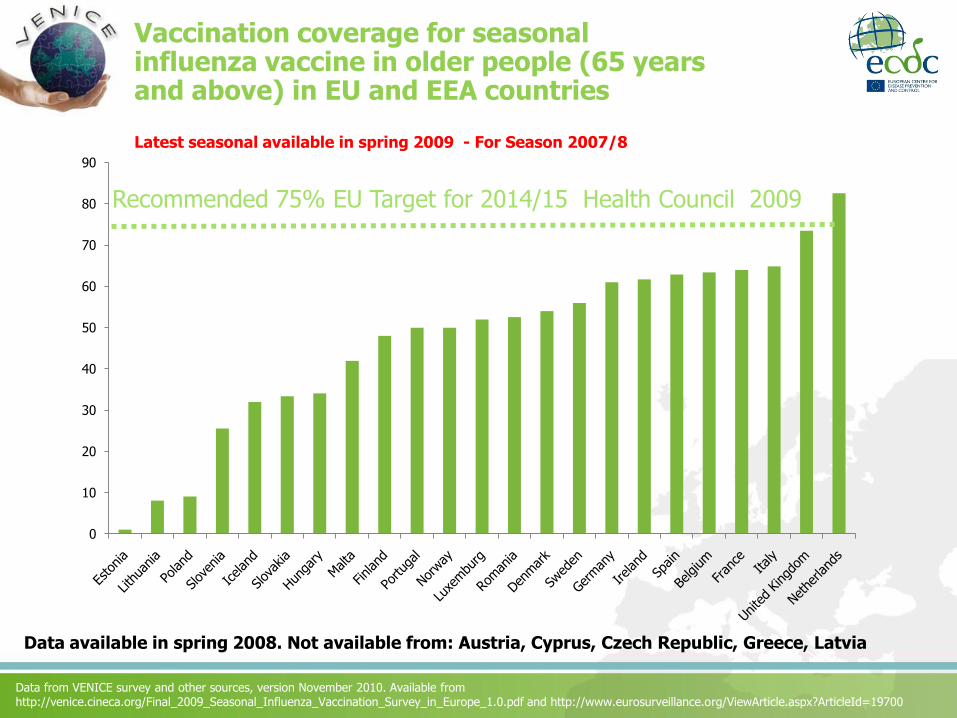
Vaccination coverage for seasonal influenza vaccine in older people (65 years and above) in EU and EEA countries
Latest seasonal available in spring 2009 - For Season 2007/8
0
10
20
30
40
50
60
70
80
90
Recommended 75% EU Target for 2014/15 Health Council 2009
Data available in spring 2008. Not available from: Austria, Cyprus, Czech Republic, Greece, Latvia
Data from VENICE survey and other sources, version November 2010. Available from http://venice.cineca.org/Final_2009_Seasonal_Influenza_Vaccination_Survey_in_Europe_1.0.pdf and http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19700
Some key points
The likelihood of older persons being immunised in EU/EEA countries varies forty-fold! - a major inequality
Reveals differing approaches to immunisation – for some countries it is seen as a public health commitment while for others they just determine policy and it is left to individuals
Note there were at least five countries that cannot report vaccine coverage
A number of previous lower performance countries have shown improvements since 2006-7
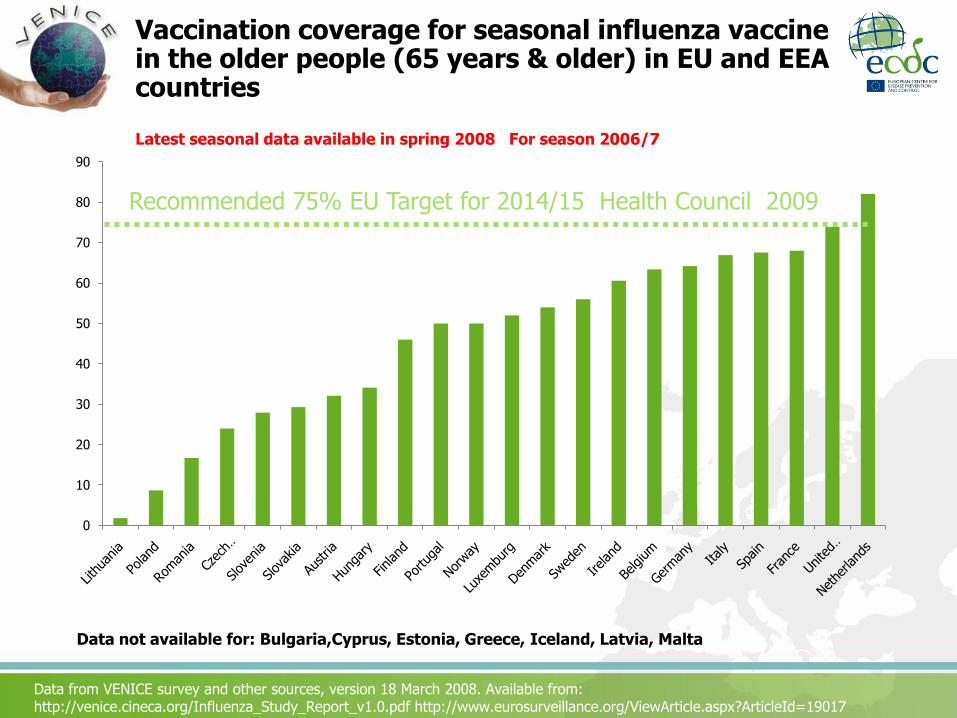
Vaccination coverage for seasonal influenza vaccine in the older people (65 years & older) in EU and EEA countries
Latest seasonal data available in spring 2008 For season 2006/7
0
10
20
30
40
50
60
70
80
90
Recommended 75% EU Target for 2014/15 Health Council 2009
Data not available for: Bulgaria,Cyprus, Estonia, Greece, Iceland, Latvia, Malta
Data from VENICE survey and other sources, version 18 March 2008. Available from:http://venice.cineca.org/Influenza_Study_Report_v1.0.pdf http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19017

Developments from the Pandemic Experience
Important points about the pandemic experience
A schizophrenic virus – usually mild or no illness. But occasionally lethal even in healthy young people – a real challenge for those doing risk communication
In some countries the unexpected experience of deaths in healthy young people was a tipping point for the acceptance of vaccine. The Meningococcal Experience
There was an expectation that it would be worse and so many people feel they were misled (what Thomas Abraham refers to as Risk Advocacy)
In other countries perceived that the need for influenza vaccination was over-sold and risks underemphasised
Whatever the experience was in your country remember it was probably different elsewhere
Antivirals were generally under-used – but where they were used they worked well
Some countries immunised higher proportion of health care workers or entire populations than for seasonal flu
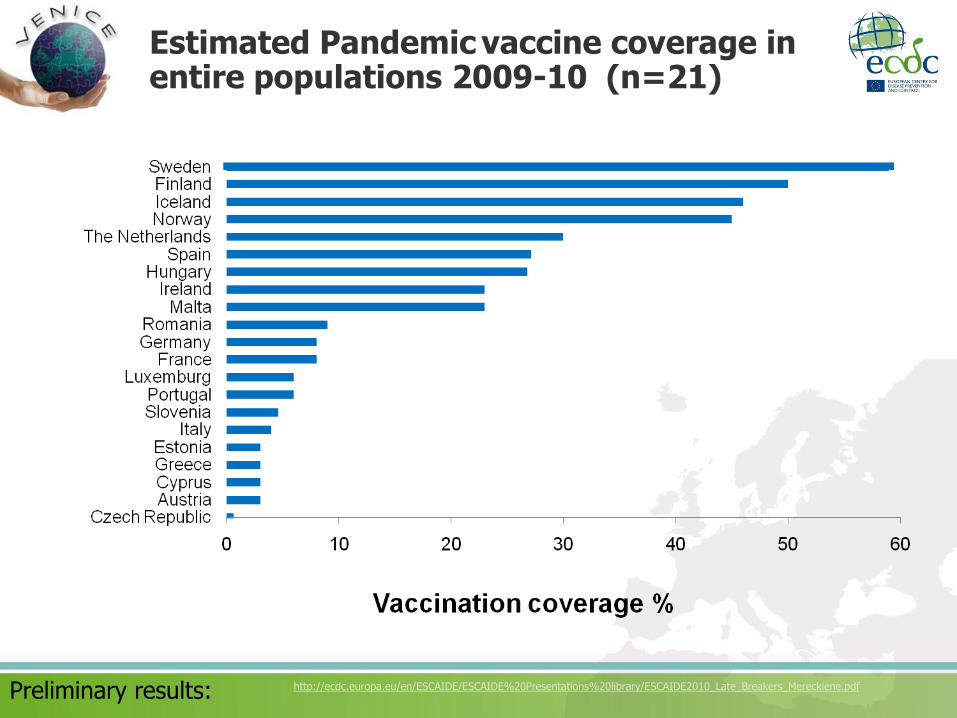
Estimated Pandemic vaccine coverage in entire populations 2009-10 (n=21)
Preliminary results: http://ecdc.europa.eu/en/ESCAIDE/ESCAIDE%20Presentations%20library/ESCAIDE2010_Late_Breakers_Mereckiene.pdf
Scientific UncertaintiesThese are legion but they include:-
• What are the risk groups for the new seasonal flu – do they include pregnant women and children?
• What is the effectiveness of antivirals against the new seasonal influenza?
• What is the effectiveness of the seasonal vaccines for severe disease?
• What is the impact of repeated immunisation against seasonal flu on long-term immunity?
• What will be the source of the next pandemic an A(H2 virus or an novel animal influenza; A(H5, H7 or H9?
• What is the pathogenesis mechanism of the Acute Respiratory Distress Syndrome caused by A(H1N1)2009?
• Why do some people suffer so severely from ARDS following flu and are there any specific treatments?
• What is the level of premature mortality due to the new seasonal influenza in Europe?
Some Needed Developments• Updating of risk groups initially annually
• Model for annual risk assessments of seasonal influenza in Europe
• Hospital surveillance for influenza
• Intensive care unit networks for severe respiratory disease
• Sustainable annual influenza vaccine effectiveness based on I-Move model
• Routine safety assessments for seasonal vaccines: through signal detection, assessment and hypothesis testing-VAESCO
• Sustainable annual reporting of vaccine policies, practises and performance of vaccination – based on VENICE
• Annual estimates of premature mortality attributable to
• Health economic tools for the new influenza
Conclusions on this season’s influenza
Not like the previous seasonal influenza
A mix of A(H1N1)2009 & B viruses – very little A(H3N2). No old A(H1N1)
Severe pathology associated with the influenza A(H1N1)2009
Clinical risk groups experiencing most of the disease
Some young healthy adults and children also affected
Some severe disease and deaths in older people
Considerable vulnerability in the community – immunisation gaps
Hence considerable potential health gain from continuing immunisation
Evidence that A(H1N1)2009 containing vaccines work well, and quickly –2010-2011 vaccine also works but less effective and having had both is best
Antivirals also of value though need to watch for oseltamivir resistance
Worth considering if higher level care services are ready for a surge
ITU networks have been invaluable where they exist








![WHOLE OF - SOCIETY PANDEMIC READINESS€¦ · • Pandemics ARE worldwide epidemics • Pandemics ARE unpredictable [Origin - Timing - Severity - Duration] • Pandemics HAVE happened](https://img.pdfslide.us/doc/110x75/60219e6a89cf726c976d409c/whole-of-society-pandemic-readiness-a-pandemics-are-worldwide-epidemics-a.jpg)