Embed Size (px)
Citation preview

Optimal Cord Clamping Clinical Guideline
V2.0

Optimal Cord Clamping Clinical Guideline V2.0
Page 2 of 12
Key Considerations
Warmth – Ensure the baby is kept warm during Optimal Cord Clamping, use
warmed towels from the resucitaire or skin to skin to achieve this
Maternal or Neonatal Deterioration – In the event that the condition of either the
mum or baby deteriorates i.e. maternal PPH or neonatal respiratory distress
Optimal Cord Clamping should be abandoned and emergency measures initiated.
Optimal Cord Clamping should never be performed at the expense of the health of
mother or baby.
Third Stage Management - Syntometrine/Syntocinon or Carbetocin can be
administered as normal if required
Yes
Yes
Yes
No
No
No
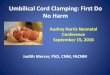
Assess and stimulate baby on warmed towels on mother’s abdomen or at the foot of the bed. Remember, whilst the cord is still pulsating the
neonate is receiving an oxygenated blood supply.
If ventilation is necessary consider initiating this with the cord intact. Cord separation is only
necessary when transfer to the resuscitaire is required.
Timing of cord separation for a compromised infant should ultimately be decided on a case
by case basis.
Has the baby been born in good condition (AT ANY GESTATION) NEW 2018?
Summary: Optimal Cord Clamping
Clamp and cut the cord immediately after birth whilst
initiating skin to skin
Is there meconium? If the baby is born in good
condition and cries immediately Optimal Cord Clamping is appropriate.
However if they do not cry, avoid stimulation as normal and separate the cord for transfer to the resuscitaire
Are there any contraindications to Optimal Cord Clamping? (See
Section 2.3)
Wait to clamp the cord for
three minutes unless the
baby’s condition
deteriorates

Optimal Cord Clamping Clinical Guideline V2.0
Page 3 of 12
1. Aim/Purpose of this guideline To inform all Midwives and Obstetricians on the topic of Optimal Cord Clamping including rationale, contraindications and guidance on when to implement. Optimal Cord Clamping is a routine part of a physiological third stage. It can also be safely implemented when active management is required. There is a growing body of evidence to support Optimal Cord Clamping and it is recommended by the Royal College of Midwives (RCM), World Health Organisation (WHO) and the UK Resuscitation Council. Optimal Cord Clamping has clear benefits to both mum and baby, alongside a discussion on management of the third stage of labour, parents should be informed that Optimal Cord Clamping will:
Increase their baby’s blood volume by up to 40% and subsequently
improve iron stores for the first 6 months of life. Iron is essential for brain
development.
Ensure baby receives stem-cell rich cord blood
Increase their baby’s weight as they receive a normal circulating blood
volume
Maximise the amount of oxygenated blood their baby receives and help
establish breathing
Stabilise blood pressure
Although the benefits are present for all babies the findings have more significance for babies that are: premature, have a low birth weight or are born to an anaemic mother. In preterm infants Optimal Cord Clamping has additionally been shown to decrease infant sepsis, intraventricular haemorrhage, rates of neonatal blood transfusion and the incidence of necrotising enterocollitis.
For the mother Optimal Cord Clamping can decrease the volume of the placenta, reduce rates of feto-maternal transfusion (important for rhesus negative mothers) and assist in creating a calm and unhurried environment.
2. The Guidance
2.1. Active Management of Third Stage of an Uncompromised Baby at any Gestation
Following delivery of the baby give oxytocic
Wait for a minimum of three minutes; clamp the cord before 5 minutes if active management of the third stage is planned. NEW 2018
Clamp and cut the cord
Wait for signs of separation before attempting to deliver the placenta
The position of the baby during Optimal Cord Clamping is not thought to influence the amount of blood the baby receives

Optimal Cord Clamping Clinical Guideline V2.0
Page 4 of 12
2.2. Optimal Cord Clamping for Babies Requiring Resuscitation
Those neonates requiring positive pressure ventilation and resuscitation would especially benefit from Optimal Cord Clamping. A policy of ‘wait a minute’ may be appropriate unless the baby has a heartbeat below 60bpm which is not getting faster NEW 2018. Consider that neonatal assessment and stimulation usually happens during this first minute which can be carried out on warm towels on the delivery bed or on the mother’s abdomen. Remember that while the cord continues to pulsate the baby is still receiving oxygenated blood.
Should transfer to the resuscitaire be deemed necessary the cord should be promptly clamped and cut. In these situations ‘cord milking’ towards the baby may be performed
Timing of cord clamping for a compromised infant should ultimately be decided on a case by case basis, being mindful of the clinical context
2.3. Contraindications to Optimal Cord Clamping
Severe Fetal Growth Restriction (FGR)
If a neonate is at significantly increased risk of polycythaemia i.e. born to a poorly controlled diabetic mother or suffering severe FGR
Severe fetal distress in 1st stage
Meconium Stained Liquor, unless in good condition and cries immediately
Maternal Haemorrhage
Vasa Previa
2.4. Operative Vaginal Delivery Optimal Cord Clamping should be performed at instrumental delivery as for spontaneous vaginal birth. Good communication with the neonatal team is crucial during this time and if at any point they feel that Optimal Cord Clamping should be abandoned this should be respected.
2.5. Caesarean Section (CS)
Upon delivery of the baby Carbetocin/Oxytocin should be given
Cord clamping should be deferred for 45 seconds, evidence suggests that this results in comparable benefits to 3 minutes OCC following vaginal birth. NEW 2018
A short delay in cord clamping at CS may reduce maternal bleeding by allowing more time for separation before the surgeon removes the placenta. Heavy bleeding not controlled by Green Armitage clamps should prompt immediate cord clamping and placenta removal.
2.6. Cord Blood Sampling A delay of three minutes does not appear to adversely affect the validity of umbilical cord blood gas analysis. Samples should, however, be taken immediately after cord clamping. If this is not possible blood should be taken from a segment of cord isolated between two clamps.

Optimal Cord Clamping Clinical Guideline V2.0
Page 5 of 12
2.7. Documentation The timing of Optimal Cord Clamping must be documented in the maternal delivery notes.
3. Monitoring compliance and effectiveness
Element to be monitored
Correct management of Optimal Cord Clamping
Lead Audit Midwife
Tool Was Optimal Cord Clamping performed when contraindicated
Was Optimal Cord Clamping offered to women having a CS
At CS was Optimal Cord Clamping performed for 45 seconds
Frequency 1% or 10 sets, whichever is the greater, of all health records of women who have delivered will be audited once over the 3 year lifetime of the guideline or
sooner if indicated.
Reporting arrangements
Clinical Audit Forum
During the process if the audit compliance is below 75% or other deficiencies identified, this will be identified by the Audit Midwife and an action plan agreed
Acting on recommendations and Lead(s)
The Audit midwife will set a time frame for the action to be completed
The action plan will be monitored by the Audit midwife
Change in practice and lessons to be shared
Required changes to practice will be identified and actioned within an agreed time frame
The Audit Midwife will lead to take each change forward where appropriate
Maternity Patient Safety Newsletter.
4. Equality and Diversity 4.1. This document complies with the Royal Cornwall Hospitals NHS
Trust service Equality and Diversity statement which can be found in the 'Equality, Diversity & Human Rights Policy' or the Equality and Diversity website.
4.2. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.

Optimal Cord Clamping Clinical Guideline V2.0
Page 6 of 12
Appendix 1. Governance Information
Document Title Optimal Cord Clamping Clinical Guideline V2.0
Date Issued/Approved: 6th September 2018
Date Valid From: 10th October 2018
Date Valid To: 10th October 2021
Directorate / Department responsible (author/owner):
Lizzie Anstey Midwife
Contact details: 01872 252879
Brief summary of contents
This guideline gives guidance to Midwives and Obstetricians in the management of Optimal Cord clamping of the baby’s umbilical cord at delivery
Suggested Keywords:
Delayed, deferred, cord, clamping, DCC, new-born, physiological, placenta, 3rd, third, stage
Target Audience RCHT CFT KCCG
Executive Director responsible for Policy:
Medical Director
Date revised: 6th September 2018
This document replaces (exact title of previous version):
Delayed Cord Clamping (DCC) - Clinical Guideline V1.0
Approval route (names of committees)/consultation:
Maternity Guidelines Group Obs and Gynae Directorate Divisional Board Policy Review Group
Divisional Manager confirming approval processes
Tunde Adewopo
Name and Post Title of additional signatories
Not Required
Name and Signature of Divisional/Directorate Governance Lead confirming approval by specialty and divisional management meetings
{Original Copy Signed}
Name: Caroline Amukusana

Optimal Cord Clamping Clinical Guideline V2.0
Page 7 of 12
Signature of Executive Director giving approval
{Original Copy Signed}
Publication Location (refer to Policy on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Document Library Folder/Sub Folder Clinical/Midwifery and Obstetrics
Links to key external standards CNST 5.2 & 5.4
Related Documents:
Farrar D, Airey R, Law G, Tuffnell D, Cattle B, Duley L. (2011). Measuring placental transfusion for term births: weighing babies with cord intact. BJOG: An International Journal of Obstetrics & Gynaecology. 118 (1), 70-75.
McDonald S, Middleton P, Dowswell T, Morris P. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database of Systematic Reviews (2013) Issue 7. Art. No.: CD004074.
Rabe H et al. Early versus delayed umbilical cord clamping in preterm infants. Cochrane Database of Systematic Reviews (2004) Issue 4. Art. No.: CD003248.
Mercer J, Vohr B, McGrath M, Padbury J, Wallach M, Oh W. (2006). Delayed cord clamping in very preterm infants reduces the incidence of intraventricular haemorrhage and late-onset sepsis: a randomized, controlled trial. Pediatrics. 117 (4), 1235-42.
Airey R, Farrar D, Duley L. Alternative positions for the baby at birth before clamping the umbilical cord. Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No.: CD007555.
World Health Organisation. (2012). Guidelines on Basic Newborn Resuscitation. WHO. Geneva.
Rabe H, Diaz-Rossello J, Duley L, Dowswell T. Effect of timing of umbilical cord clamping and other strategies to influence placental

Optimal Cord Clamping Clinical Guideline V2.0
Page 8 of 12
transfusion at preterm birth on maternal and infant outcomes. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD003248
UK Resuscitation Council. (2010). Guidelines on Newborn Life Support. Resuscitation Council (UK). London.
Erickson-Owens D, Mercer J. (2012). Rethinking placental transfusion and cord clamping issues. The Journal of Perinatal and Neonatal Nursing. 26 (3), 202-17.
Andersson O et al. (2013). Effects of delayed compared with early umbilical cord clamping on maternal postpartum haemorrhage and cord gas analysis: a randomized trial. Acta Obstet Gynecol Scand. 92, 567-74
RCOG. (2015) Clamping of the Umbilical Cord and Placental Transfusion
Andersson O, Hellström-Westas L, Domellöf M. Elective caesarean: does delay in cord clamping for 30 s ensure sufficient iron stores at 4 months of age? A historical cohort control study. BMJ Open 2016 NEW 2018
Al-Wassia H, Shah PS. Efficacy and Safety of Umbilical Cord Milking at Birth: A Systematic Review and Meta-analysis. JAMA Pediatr. 2015;169(1):18–25. NEW 2018
Training Need Identified? Yes, Multidisciplinary PROMPT training day.
Version Control Table
Date Version No
Summary of Changes Changes Made by
(Name and Job Title)
18th June 2015
V1.0 Initial Issue Elizabeth Cowan
Midwife

Optimal Cord Clamping Clinical Guideline V2.0
Page 9 of 12
6th September 2018
V2.0
Reviewed, ‘deferred’ changed to ‘optimal’, some points clarified, cord milking recommended when Optimal Cord Clamping cannot be facilitated.
Lizzie Anstey Midwife (nee Cowan)
All or part of this document can be released under the Freedom of
Information Act 2000
This document is to be retained for 10 years from the date of expiry. This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust Policy for the Development and Management of Knowledge,
Procedural and Web Documents (The Policy on Policies). It should not be altered in any way without the express permission of the author or their Line
Manager.

Optimal Cord Clamping Clinical Guideline V2.0
Page 10 of 12
Appendix 2. Initial Equality Impact Assessment Form
This assessment will need to be completed in stages to allow for adequate consultation with the relevant groups.
Name of Name of the strategy / policy /proposal / service function to be assessed Optimal Cord Clamping Clinical Guideline V2.0
Directorate and service area: Obs and Gynae Directorate
Is this a new or existing Policy? Existing
Name of individual completing assessment: Lizzie Anstey
Telephone: 01872 252879
1. Policy Aim*
Who is the strategy / policy / proposal /
service function aimed at?
To provide all health professionals guidance on Deferred Cord Clamping for the neonate
2. Policy Objectives*
To maximise the amount of oxygenated blood the baby receives through the cord at delivery
3. Policy – intended Outcomes*
Improved neonatal outcomes
4. *How will you measure the
outcome?
Compliance Monitoring Tool
5. Who is intended to benefit from the
policy?
All new-born babies and their mothers
6a Who did you consult with b). Please identify the groups who have been consulted about this procedure.
Workforce Patients Local groups
External organisations
Other
X
Please record specific names of groups Maternity Guidelines Group Obs and Gynae Directorate Policy Review Group

Optimal Cord Clamping Clinical Guideline V2.0
Page 11 of 12
Are there concerns that the policy could have differential impact on: Equality Strands: Yes No Unsure Rationale for Assessment / Existing Evidence
Age X All new-born babies and their mothers
Sex (male,
female, trans-gender / gender reassignment)
X All new-born babies and their mothers
Race / Ethnic communities /groups
X All new-born babies and their mothers
Disability - Learning disability, physical impairment, sensory impairment, mental health conditions and some long term health conditions.
X All new-born babies and their mothers
Religion / other beliefs
X All new-born babies and their mothers
Marriage and Civil partnership
X All new-born babies and their mothers
Pregnancy and maternity
X All new-born babies and their mothers
Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian
X All new-born babies and their mothers
You will need to continue to a full Equality Impact Assessment if the following have been highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies which have
been identified as not requiring consultation. or
What was the outcome of the consultation?
Guideline agreed
7. The Impact Please complete the following table. If you are unsure/don’t know if there is a negative impact you need to repeat the consultation step.

Optimal Cord Clamping Clinical Guideline V2.0
Page 12 of 12
Major this relates to service redesign or development
8. Please indicate if a full equality analysis is recommended. Yes No X
9. If you are not recommending a Full Impact assessment please explain why.
No areas indicated
Signature of policy developer / lead manager / director Lizzie Anstey
Date of completion and submission 6th September 2018
Names and signatures of members carrying out the Screening Assessment
1. Lizzie Anstey
2. Human Rights, Equality & Inclusion Lead
Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa, Truro, Cornwall, TR1 3HD This EIA will not be uploaded to the Trust website without the signature of the Human Rights, Equality & Inclusion Lead. A summary of the results will be published on the Trust’s web site. Signed Sarah-Jane Pedler Date 6th September 2018