Embed Size (px)
Citation preview

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2013
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 893
Effects of Delayed versus EarlyCord Clamping on HealthyTerm Infants
OLA ANDERSSON
ISSN 1651-6206ISBN 978-91-554-8647-1urn:nbn:se:uu:diva-198167

Dissertation presented at Uppsala University to be publicly examined in Rosénsalen, Ingång 95/96, Akademiska Barnsjukhuset, Uppsala, Thursday, May 23, 2013 at 09:30 for the degree of Doctor of Philosophy. The examination will be conducted in English. Abstract Andersson, O. 2013. Effects of Delayed versus Early Cord Clamping on Healthy Term Infants. Acta Universitatis Upsaliensis. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 893. 66 pp. Uppsala. ISBN 978-91-554-8647-1. The aim of this thesis was to study maternal and infant effects of delayed cord clamping (≥180 seconds, DCC) compared to early (≤10 seconds, ECC) in a randomised controlled trial. Practice and guidelines regarding when to clamp the cord vary globally, and different meta-analyses have shown contradictory conclusions on benefits and disadvantages of DCC and ECC.
The study population consisted of 382 term infants born after normal pregnancies and ran-domised to DCC or ECC after birth. The primary objective was iron stores and iron defi-ciency at 4 months of age, but the thesis was designed to investigate a wide range of sug-gested effects associated with cord clamping.
Paper I showed that DCC was associated with improved iron stores at 4 months (45% higher ferritin) and that the incidence of iron deficiency was reduced from 5.7% to 0.6%. Neonatal anaemia at 2-3 days was less frequent in the DCC group, 1.2% vs. 6.3%. There were no differences between the groups in respiratory symptoms, polycythaemia, or hyper-bilirubinaemia.
In paper II we demonstrated that DCC versus ECC was not associated with higher risk for maternal post partum haemorrhage and rendered a comparable ratio of valid umbilical artery blood gas samples.
In paper III, the Ages and Stages Questionnaire was used to assess neurodevelopment at 4 months. The total scores did not differ, but the DCC group had a higher score in the problem-solving domain and a lower score in the personal-social domain. Immunoglobulin G level was 0.7 g/L higher in the DCC group at 2–3 days, but did not differ at 4 months. Symptoms of infection up to 4 months were comparable between groups.
Finally, in paper IV, iron stores and neurodevelopment were similar between groups at 12 months. Gender specific outcome on neurodevelopment at 12 months was discovered, imply-ing positive effects from DCC on boys and negative on girls.
We conclude that delaying umbilical cord clamping for 180 seconds is safe and associated with a significantly reduced risk for iron deficiency at 4 months, which may have neurodevel-opmental effects at a later age. Keywords: active management, birth, breast feeding, cord clamping, ferritin, growth, haemoglobin, human infant, infections, iron, iron deficiency, iron deficiency anemia, iron status, morbidity, neurodevelopment, randomised controlled trial, umbilical cord Ola Andersson, Uppsala University, Department of Women's and Children's Health, Pediatrics, Akademiska barnsjukhuset, ing. 95 nbv, Uppsala, Sweden. © Ola Andersson 2013 ISSN 1651-6206 ISBN 978-91-554-8647-1 urn:nbn:se:uu:diva-198167 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-198167) Cover design: Fröken Fokus www.frokenfokus.se Printed by Elanders Sverige AB, 2013

To Cecilia,for providing the spark in real life
and in my research
To Olle, Måns and Lykke,for being my highly beloved arrows
towards the future


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Andersson O, Hellström-Westas L, Andersson D, Domellöf
M.(2011) Effect of delayed versus early umbilical cord clamp-ing on neonatal outcomes and iron status at 4 months: a ran-domised controlled trial. BMJ. 343:d7157.
II Andersson O, Hellström-Westas L, Andersson D, Clausen J, Domellöf M.(2012) Effects of delayed compared to early um-bilical cord clamping on maternal postpartum hemorrhage and cord blood gas sampling: a randomized trial. Acta Obstetr Gy-necol Scand, 91. doi: 10.1111/j.600-0412.2012.01530.x. [Epub ahead of print].
III Andersson O, Domellöf M, Andersson D, Hellström-Westas L. (2013) Effects of delayed cord clamping on neurodevelopment and infection at four months of age: a randomised trial. Acta Paediatr. 102(5): 525–531. doi: 10.1111/apa.12168
IV Andersson O, Domellöf M, Andersson D, Hellström-Westas L. A randomized trial of delayed versus early cord clamping: iron status and neurodevelopment at 12 months of age. Manuscript.
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 11 The fetal-placental circulation ............................................................. 12 Early and delayed cord clamping - definitions .................................... 13 Overview of previous research on cord clamping ............................... 14 Active management of third stage of labour ........................................ 16 Guidelines for umbilical cord clamping .............................................. 16 Umbilical cord blood gas sampling ..................................................... 18 Iron deficiency ..................................................................................... 19
Aims of the thesis.......................................................................................... 21 Methods ........................................................................................................ 22
Trial design .......................................................................................... 22 Participants .......................................................................................... 22 Randomisation ..................................................................................... 22 Intervention .......................................................................................... 23 Blinding ............................................................................................... 23
Data collection .......................................................................................... 24 Maternal data ....................................................................................... 24 Neonatal data ....................................................................................... 24 4 and 12 month data ............................................................................. 25 Blood samples ...................................................................................... 26 Ages and Stages Questionnaire (ASQ) ................................................ 27 Sample size .......................................................................................... 27
Statistical analysis .................................................................................... 28 Ethical considerations .............................................................................. 28
Results ........................................................................................................... 31 Maternal characteristics ....................................................................... 31 Newborn characteristics ....................................................................... 31 Per protocol analysis of background characteristics ............................ 32
Main results .............................................................................................. 32 Obstetric outcome (paper II) ................................................................ 32 Neonatal outcome (paper I) ................................................................. 35 Haematological status and iron status (papers I and IV) ..................... 37 Neurodevelopment (papers III and IV) ................................................ 40 Morbidity and IgG at 4 months (paper III) .......................................... 41 Growth and nutrition (papers I, III and IV) ......................................... 42

Discussion ..................................................................................................... 44 Conclusions ................................................................................................... 50 Future perspectives ....................................................................................... 51 Swedish summary ......................................................................................... 52 Acknowledgements ....................................................................................... 55 References ..................................................................................................... 59

Abbreviations
ADHD AMTSL ASQ CI CRP DCC ECC ELISA FIGO Hb Hct ICM ID IDA IgG MCHC MCV PPH RetHE Rtc SD TfR TS
Attention-deficit/hyperactivity disorder Active management of third stage labour Ages and Stages Questionnaire Confidence interval C-reactive protein Delayed cord clamping Early umbilical cord clamping Enzyme-linked immunosorbent assay International Federation of Obstetrics and Gynaecology Haemoglobin Haematocrit International Confederation of Midwives Iron deficiency Iron deficiency anaemia Immunoglobulin G Mean cell haemoglobin concentration Mean cell volume Maternal postpartum haemorrhage Reticulocyte haemoglobin Reticulocyte count Standard deviation Soluble transferrin receptors Transferrin saturation


11
Introduction
This thesis is aimed at comparing effects of delayed versus early umbilical cord clamping at birth and during the infant’s first year of life. Despite being an experience all humans have in common; questions still remain regarding the optimal way of managing birth. The optimal time-point for umbilical cord clamping after delivery has been under debate for several decades. Ad-vocates for early cord clamping (ECC) argue that delayed cord clamping (DCC) can be physiologically distressing on the infant’s circulation and that the risk for polycythaemia and jaundice is increased. Other rationales for ECC are the recommendation to practice ‘active management of third stage of labour’ (AMTSL), in which ECC has been a part, and the widely used routine to analyse umbilical arterial blood samples immediately after birth. More recently, the new possibility of harvesting haematopoietic stem cells from the placental-fetal blood has been associated with a need for ECC. Since an increased volume of blood can be collected from the placental cir-culation after early cord clamping, a higher count of stem cells can be har-vested.
Advocates for DCC, on the other hand, argue that this practise is the ‘natural way’ of terminating a delivery. Furthermore, an accumulating num-ber of studies, published after 1997 when the two first modern cord clamping studies including follow-up of 2-3 months were published,1 2 support the finding that the large transfusion to the newborn infant that is accomplished by DCC could prevent iron deficiency. Preventing iron deficiency, and more importantly iron deficiency anaemia, could have important health implica-tions concerning the child’s development, especially in low income countries with a high prevalence of iron deficiency.
In 2006, a telephone survey to Swedish obstetric units showed that 30 out of 48 units practised early cord clamping as clinical standard (O Andersson, unpublished data). The most frequent reason given for practising ECC was to obtain a blood gas sample from the umbilical cord. However, several midwives answering the survey expressed hesitation against the ECC rou-tine. Preconceptions against DCC were also common, especially on the risk for neonatal jaundice. The possible benefit of preventing iron deficiency with DCC was questioned because of the presumed well nurtured Swedish population. It was obvious that, in spite of 130 years of studies on the sub-ject, no firm conclusions could be drawn from previous studies and there

12
was still a need for a large randomised trial aimed to study effects on both the infant and the mother, and with a longitudinal perspective.
The fetal-placental circulation During pregnancy, the fetal-placental circulation transports oxygen and nu-tritional elements from the placenta to the fetus, and metabolic residues from the fetus to the placenta. The total fetal blood volume is approximately 115 ml/kg. The proportion of fetal blood that at any moment circulates in the placenta diminishes during pregnancy, and is estimated to be around 50% at 30 gestational weeks and 35 % at term.3 For a term pregnancy, containing a fetus with a normal weight of 3.5 kg, this distribution corresponds to ap-proximately 140 ml of blood in the placenta and 260 ml in the fetus.
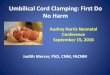
In the 1960s and early 1970s, Lind and colleagues extensively studied the fetal-placental circulation.4-8 After delivery, blood circulates in the umbilical arteries from the newborn infant mainly during the first 25 sec, and after 45 sec the circulation becomes negligible indicating a closure of the fetal-placental circulation. In contrast, the blood flow from the placental side to the infant through the umbilical vein is maintained during the first 3 min of birth, largely influenced by uterine contractions.9 Consequently, a net trans-fusion of blood from the placenta to the infant is accomplished. The total placental transfusion to the infant is about 30 ml/kg, leaving 15 ml/kg in the placenta, Figure 1.
Figure 1. Distribution of the blood volume in the placenta and in the fetus before birth, and after birth in the placenta and infant after early cord clamping (left) and delayed cord clamping (right).

13
The placental transfusion occurs mainly within 1 min, and is usually com-plete after 3 min.6 Also the level of the baby in relation to the placenta af-fects the placental transfusion. If the baby is held 20 cm below the placenta the complete transfusion will be performed within 1 min, but if the baby is held 20 cm over the level of the placenta, the transfusion will be about 20 ml/kg, and at 40 cm above the placenta no transfusion occurs. The rate of the transfusion is also dependent of the contractions of the uterus.7
In agreement with the older studies referred to above, Farrar et al pre-sented data in 2011 on placental transfusion after having weighed newborns with the umbilical cord intact using digital scales that recorded an average weight every 2 sec. Placental transfusion was calculated from the change in weight between birth and either cord clamping or when weighing stopped. Placental transfusion was usually complete by 2 min, but sometimes contin-ued for up to 5 min and contributed with 32 ml/kg (95% CI, 30 to 33 ml) to blood volume,10 a volume very close to the results from Lind et al.
Early and delayed cord clamping - definitions Different definitions of ECC have been used, with the time varying from immediately to within one min after delivery of the baby. In modern trials ECC has usually been defined as clamping within 10-30 sec after birth. The time to cord clamping is also dependent on how the moment of birth is de-fined; after the passage of the shoulders or, more commonly, after total ex-pulsion of the child. In standard obstetric practice the umbilical cord is usu-ally clamped or ligated, and cut, before the delivery of the placenta. To our knowledge, at least since after the introduction of the fetal surveillance method STAN,11 immediate clamping has been the standard of care in sev-eral Swedish obstetric units, including Hospital of Halland, Halmstad, where our study was performed. Two main advantages of ECC have been pro-posed: a reduction of maternal postpartum haemorrhage (PPH) as part of AMTSL12, and facilitation of blood gas sampling from the umbilical cord.13
Late or delayed cord clamping is usually defined as cord clamping 2-3 min after delivery, or after cessation of cord pulsations.14 15 The main pro-posed advantage of DCC is prevention of infant iron deficiency, a condition that is associated with suboptimal neurodevelopment.16 17 The rationale for this strategy is that a placental transfusion of 80-100 ml of blood will supply 40 to 50 mg/kg of additional iron to the basal stores of 75 mg/kg of body iron in a newborn term infant. Delayed cord clamping is associated with higher haemoglobin (Hb) in the neonatal period18 and at 2 months of age,1 and with significantly higher iron stores at 6 months of age.19
Some studies suggest that DCC may have adverse neonatal effects with increased risk of respiratory symptoms,20 polycythaemia,21 hyperbilirubina-emia22 and need of phototherapy.14 16

14
Unclamping the previously clamped and separated umbilical cord, and al-lowing the blood from the placenta to drain freely into an appropriate con-tainer, has been shown to shorten third stage labour and decrease the inci-dence of retained placenta.23 This drainage corresponds to the transfusion occurring from the placenta to the infant during DCC.
Overview of previous research on cord clamping Physiological and health effects of cord clamping in relation to time after delivery, have been studied since 1875.24 In 1967, Moss and Monset-Couchard published an extensive comparison of ECC and DCC based on 84 studies.25 The review was mainly oriented at effects on the newborn infant during the first days after birth and concluded that DCC was associated with higher Hb and haematocrit (Hct). No differences were noticed in bilirubin, and hemodynamic findings were variable. Nelle and co-workers published three studies in the 1990s demonstrating that DCC resulted in higher blood viscosity, which was compensated for by peripheral vasodilatation.26-28 The higher neonatal blood viscosity was still present at 5 days of age and associ-ated with a slower postnatal decrease of pulmonary vascular resistance.
In the largest randomised controlled trial conducted so far, and published in 2006, Ceriani Cernadas et al18 randomly assigned 276 newborn infants into three groups according to time for umbilical cord clamping after deliv-ery: within 15 sec, after 1 min, and after 3 min, respectively. The primary outcome was venous Hct at 6 h postnatal age. Haematocrit was not signifi-cantly different between the three groups at 6 h, but in the 3-min group a Hct above 65% was significantly more prevalent (14.1%), but no infants had clinical signs of polycythaemia. At 24-48 h after birth, the prevalence of anaemia (Hct <45%) was significantly higher in the group randomised to cord clamping < 15 sec as compared to the other two groups. Secondary outcomes, e.g. plasma bilirubin at 24-48 h, early neonatal morbidity and mortality, and health at 1 month did not differ between the groups; neither did maternal factors such as maternal postpartum haemorrhage (PPH) or maternal Hct at 24 h after delivery. The investigators concluded that the practice of DCC for more than 1 min is safe and should be implemented to increase neonatal iron storage at birth.
Only a few controlled trials have assessed effects of DCC on infant health beyond the neonatal period. These studies were all performed in low and middle income populations with a high prevalence of iron deficiency anaemia (India,2 29 Guatemala,1 Mexico,19 and Zambia30). The longest follow up of a randomised controlled trial evaluating ECC versus DCC is 6 months. In addition, at least two studies have been published in other languages than English, a 3-month follow up in Brazil, 31 and a 6-month follow up in Argen-tina.32

15
Chaparro et al19 investigated whether a 2-min delay in cord clamping (af-ter delivery of the infant’s shoulder) would improve iron stores and haemato-logical status in full-term infants at 6 months of age, as compared to ECC around 10 sec after delivery. Of the 476 mother-infant pairs who were re-cruited, 358 (75%) completed the trial. At 6 months, infants who were sub-jected to DCC had higher mean cell volume (MCV), higher ferritin levels and higher iron stores (27-47 mg). The effects of DCC were more pro-nounced in infants born to mothers with low ferritin at delivery, in breastfed infants, and in infants with birth weights 2500-3000 g. Including these re-sults, two meta-analyses have concluded that DCC results in higher levels of serum ferritin at 3-6 months of age.14 16
The timing of umbilical cord clamping could be important also in high-income countries, not least due to the relatively high reported prevalence of ID in Europe and USA.33 34 Still, there is currently no other available data concerning health effects of DCC beyond the neonatal period in term new-born infants in high-income countries.
The growing body of studies has established a theoretical model, here called the ‘placental transfusion model’, Figure 1, consisting of the follow-ing elements:
Figure 2. The placental transfusion model
(1) DCC contributes to a net transfusion of umbilical cord blood. (2) This placental transfusion adds to elevated haemoglobin in the newborn period and at two months of age. (3) As the physiologic haemolysis occurs during the first months of life, haemoglobin is metabolised and transferred to the

16
iron stores throughout the body, reflected in higher levels of ferritin, trans-ferrin saturation (TS), MCV and lower levels of soluble transferrin receptors (TfR).
As a further, hypothetical part of the ‘placental transfusion model’ it is hypothesised that (4) the excess iron received by placental transfusion could prevent iron deficiency and as a result of this also protect from iron defi-ciency anaemia and iron deficiency-associated neurodevelopmental and be-havioural deficits.
Active management of third stage of labour Excessive maternal post partum bleeding is a dangerous complication of childbirth. It is associated with failure of the uterus to contract efficiently during and after the third stage of labour, i.e. after the expulsion of the pla-centa. In order to ‘actively’ prevent PPH, drugs increasing the contractility of the placenta have been used for centuries.35 Preparations of ergot have been known to have oxytocic effects at least for 600 years, and came in to obstetric practise in the 19th century. With development of the alkaloids er-gotoxine and ergotamine in the early 20th century and ergometrine in 1935,36 active management, in the meaning administrating an oxytocic drug, became established.
In 1988, in the ‘Bristol trial’, Prendiville and colleagues randomly as-signed delivering women to physiological (n=849) or active (n=846) man-agement.12 Adherence to the protocol was almost complete in the active arm: 99% received a prophylactic oxytocic drug, early cord clamping (≤ 30 sec), and cord traction before placental delivery. However, only 47% of those randomised to physiological management received the allocated interven-tion; 20% received a prophylactic oxytocic, 40% underwent cord traction and in 51% the cord was clamped before placental delivery. Results in the physiological group showed three times higher prevalence of PPH of more than 500 ml (17.9% vs. 5.9%), and severe PPH of more than 1000 ml (3.1% vs. 0.8%) as compared to the active management, and also an increased need for maternal blood transfusion, 5.7% in the physiological group versus 2.1% in the active group.
Guidelines for umbilical cord clamping In many high-income countries there is an ongoing debate whether to prac-tice ECC or DCC. Early cord clamping is probably the dominating practice worldwide, although recent and reliable data are scarce. An increased awareness of the possible long-term advantages for the infant after DCC is weighted against possible risks, mainly hyperbilirubinaemia. In Europe, as well as in other parts of the world, the practice varies substantially both be-tween and within countries.37 38

17
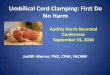
Figure 3 demonstrates cord clamping practices in 1175, out of 2034, hos-pitals participating in the EUropean Project on obstetric Haemorrhage Re-duction: Attitudes, Trial, and Early warning System (EUPHRATES). This project, which included hospitals in 14 countries, demonstrated that a large majority of European hospitals practised early cord clamping in 2002.
Figure 3. Proportion of hospitals practicing immediate cord clamping in 14 Euro-pean countries according to a survey distributed to 1175 delivery units in 2002.37
In order to reduce PPH and need of blood transfusions to the mother, the International Federation of Obstetrics and Gynaecology (FIGO) and the In-ternational Confederation of Midwives (ICM), as well as a Cochrane report, have previously recommended that immediate cord clamping should be per-formed together with controlled cord traction and administration of an oxy-tocic drug.39 40 These recommendations were based on results from five ran-domised controlled trials.12 41-44
In Sweden, no specific recommendations regarding time to cord clamping were issued in the ‘State of the Art’ document published by the National Board of Health and Welfare in 2001.45 After the last years’ growing support for DCC,14 16 the FIGO/ICM in 2006 revised their statement from 2003 and omitted ECC as a part of active management of third stage labour.40 In 2007, the National Institute for Health and Clinical Excellence in UK published new guidelines, recommending ECC.46 In Sweden, recommendations to per-form DCC were published in 2008 by representatives from the national or-ganisations of midwives, obstetricians and neonatologists.47 The WHO pub-lished documents in 2007 and 2009 recommending DCC.48 49
In contrast, the Society of Obstetricians and Gynaecologists of Canada in 2009 recommended that the possible risk for neonatal jaundice requiring phototherapy must be weighed against the benefits of DCC.50 The latest Cochrane review on AMTSL from 2011 do not make any clear recommen-dations on DCC versus ECC but concludes on ‘Active versus expectant

18
management’ that women should be given information on the benefits and harms of both methods to support informed choice.51 The American College of Obstetricians and Gynecologists published a committee opinion in De-cember 2012 stating that there was insufficient evidence to confirm or refute the potential for benefits from DCC.52 The lack of consensus is also reflected by the results in a survey performed in 2008 including replies from 926 ob-stetricians and 1297 midwives in the UK, reporting that 74% of obstetricians and 41% of midwives clamp the cord within 20 sec. Furthermore, 81% of obstetricians and 89% of midwives replied that more evidence from random-ised trials was needed regarding the best time to clamp the cord’.53
Figure 4. Reported practice of early cord clamping, by interview and/or observed practices, in Sweden, UK, Albania, Nigeria and Zambia. 53-56
Umbilical cord blood gas sampling A blood gas sample from the umbilical artery is an important tool for quality control of obstetric care, and the result may also have medicolegal implica-tions.13 57 In order to reflect the acid-base balance at the time of birth, and obtain the sample before the baby’s first breaths, the most commonly rec-ommended technique for umbilical cord blood sampling is to double-clamp the umbilical cord immediately after delivery and then collect the blood sample from the intervening segment.57 To ensure that an arterial sample is obtained, it is proposed that paired arterial and venous samples should be taken for comparison.58 However, this technique excludes the possibility of DCC.
In Sweden, several hospitals have used a modified method for blood sam-pling from the unclamped pulsating cord,59 allowing sampling from the um-bilical artery directly after birth and, at least in theory, at the same time al-lowing for the placental transfusion.60 This alternative method for obtaining umbilical cord blood samples has been mentioned in two previous publica-

19
tions,59 61 but to our knowledge there are no published data evaluating the method in relation to umbilical cord blood gas samples taken from the im-mediately clamped cord in a randomised trial.
Iron deficiency Infants and pre-school children are at particular risk of iron deficiency (ID) due to high iron requirements during rapid growth in combination with low iron intakes.62 A large number of studies have investigated consequences of ID on neurocognitive development in infants and children. A causal connec-tion has not been clearly established, although evidence for adverse effects of ID is increasing63 Associations have been made between ID and altered emotional regulation, impaired motor development and cognitive delays.17 62
64 Two recent meta-analyses conclude that iron supplementation improves psychomotor and mental development in infants and children,65 66 and a re-cent Swedish trial demonstrated that early iron supplementation of margin-ally low birth weight infants significantly reduced the prevalence of behav-ioural problems at 3.5 years of age.67
Gunnarsson et al68 evaluated the possible association between iron status at 1 and 6 years with development at 6 years in a cohort of Icelandic chil-dren. They found that ID at 1 year was associated with lower fine motor development scores at 6 years. Haemoglobin levels at 6 years were posi-tively associated with gross motor development. In French children aged 4-14 years, Konofal et al69 demonstrated that children with attention-deficit/hyperactivity disorder (ADHD) had lower serum ferritin than controls and also that lower ferritin levels correlated with more severe ADHD symp-toms and greater cognitive defects. In a later study, the same group random-ised iron deficient children aged 5-8 years, who met DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition) criteria for ADHD, to either oral iron or placebo for 12 weeks. Iron supplementation was associ-ated with a significant decrease in the ADHD Rating Scale.70 Data from animal studies support these observations, demonstrating impaired myelina-tion, altered neurotransmitter function and neurometabolism in iron deficient juvenile rats.71 72
Iron deficiency anaemia (IDA) is the most severe form of ID and is a large public health problem in children, especially in low-income countries. Iron deficiency anaemia in young children is associated with suboptimal development and long-lasting cognitive and behavioural deficits.17 63 73 Glob-ally, approximately one fourth of all pre-school children are estimated to be affected by IDA.
Most commonly, ID and IDA have been studied in low or middle income countries, where the prevalence of these disorders are higher. In Europe, the prevalence of ID has been reported to be as high as 26%, and the prevalence of IDA is 3-7% among young children.74-76 Consequently, since DCC is as-

20
sociated with improved iron status in infants it could also have an impact on ID-related adverse effects also in high income countries such as Sweden.

21
Aims of the thesis
The overall aim of this thesis was to investigate effects of delayed and early cord clamping on maternal and newborn infant health, and on infant out-comes up to 12 months of age (including iron status, infections, growth and development) in a low risk population randomised at delivery to DCC or ECC. The specific aims were to compare effects of DCC versus ECC on:
• neonatal morbidity and iron status at 4 months of age (paper I);
• the third stage of labour and maternal PPH, and rates of valid um-
bilical cord blood gas samples (paper II);
• Neurodevelopment, Ig G levels and rate of infection symptoms at four months of age (paper III)
• Iron status and neurodevelopment at 12 months of age (paper IV)

22
Methods
Trial design Randomised controlled trial (parallel-group study with 1:1 randomisation) comparing delayed cord clamping (DCC) with early cord clamping (ECC). The study was conducted between April 2008 and May 2010 at the Hospital of Halland, Halmstad, Sweden.
Participants Pregnant women were eligible if they met the following criteria: non-smoking; healthy (no haemolytic disease, no treatment with any of the fol-lowing drugs: anticonvulsants, antidepressants, thyroid hormone, insulin, chemotherapy or cortisone); normal pregnancy (no preeclampsia, no diabe-tes, no prolonged rupture of membranes or signs of infection); singleton; term pregnancy (gestational age 37+0 until 41+6 weeks+days); expected vaginal delivery with cephalic presentation. The mother should be able to master Swedish well enough to participate in the study and should live close enough to the hospital to be willing to return for follow up after four months. Neonatal exclusion criteria were serious congenital malformations, syn-dromes or other congenital diseases that could affect outcomes. Pregnant women were first given information about the trial at the antenatal health care centre at about 34 weeks of gestation. Those fulfilling the inclusion criteria at the time of admission to the delivery ward were again informed about the study by the attending midwife. Written informed consent was obtained before delivery from the pregnant woman, and when possible, from both parents.
Randomisation Randomisation was performed by one of the investigators (MD) in advance by computer in blocks of 20 using the random number generator in MS Ex-cel (Microsoft, Seattle, WA, USA).

23
Intervention When delivery was imminent (expected within 10 min), the midwife opened a sealed numbered opaque envelope containing the treatment allocation. The intervention in the DCC group consisted of delayed clamping of the umbili-cal cord (≥ 180 sec) and the ECC group consisted of early clamping of the umbilical cord (≤ 10 sec). In both randomisation groups, the midwife was instructed to hold the newborn infant at a level around 20 cm below the vulva for 30 sec, and then place the baby on the mother’s abdomen. Due to the possibility to fold down the lower part of the delivery bed, 20 cm was chosen as a practically obtainable level. Babies born by caesarean section were placed on their mothers’ lap before clamping according to clinical rou-tines. All other aspects of obstetric care were managed according to standard practice at the hospital. In line with hospital routine, oxytocin (10 IU, corre-sponding to 16.7 µg) was administered intravenously to the mother immedi-ately after cord clamping. The midwives were also instructed to perform controlled cord traction, by putting a clamp on the umbilical cord close to the woman’s perineum, and then push gently with one hand on the lower uterine segment and simultaneously with the other hand pull the cord care-fully until the placenta was delivered. All staff in the delivery unit were trained in the study procedures before the trial started. Early cord clamping was the clinical standard procedure in the hospital before and during the study.
After delivery, the mothers and their babies were cared for according to clinical routines and early breastfeeding was encouraged. Infants stayed at the postnatal ward together with their mothers for 2-3 days, except well ba-bies to mothers who preferred to leave the hospital earlier, or infants who were admitted to the neonatal unit. A physician examined all infants during the first 72 h, according to clinical routines.
Blinding Due to the study design, neither the mother giving birth nor the midwife performing the intervention could be blinded. Physicians performing neona-tal examinations, staff members responsible for collection of blood samples and background data, and laboratory staff performing analyses of blood samples were blinded to the infant’s allocation group. Staff performing the follow up during the first year of life was blinded to randomisation group, and the parents were asked not to tell the randomisation group to the staff unless it was necessary for some reason.

24
Data collection
Maternal data The following information was collected from maternal health care records from the time of admission to antenatal care: reported illness, medication, parity, weight, length and body mass index (BMI), smoking habits, blood group Rhesus factor status, and Hb value. After giving birth, the estimated maternal postpartum blood loss was recorded by the midwife within two h after childbirth by weighing pads, sheets and other textiles, and by measur-ing the volume of blood collected in a pan. The time between the delivery of the infant and the delivery of the placenta was noted. During postnatal care, mothers were interviewed concerning their dietary preferences and use of iron supplements during pregnancy and answers were noted in the study protocol.
Neonatal data The midwife’s assistant measured the time from complete delivery of the baby to the first clamp on the umbilical cord with a stopwatch. Venous and arterial cord blood samples for assessment of acid base status were taken within 30 sec from the unclamped cord in the DCC group and within 10 min from the double clamped segment of the umbilical cord in the ECC group. Additional blood samples included in the study were taken from the clamped umbilical cord in both groups. The remaining fetal blood in the placenta was measured by placing the free end of the cut umbilical cord in a measuring glass and elevating the placenta until all blood had been drained.
The infant was assessed at 1 and 6 h by the midwife, who recorded if the baby had been breastfed and the presence of respiratory symptoms, i.e. respi-ratory rate above 60, presence of nostril flaring, grunting or intercostal re-tractions.
All neonatal diagnoses were reported in the study protocol. At 48-72 h af-ter birth, a midwife or a neonatal nurse collected study samples in conjunc-tion with routine venous blood sampling for metabolic screening. Results from any additional blood samples that were taken on clinical indications were also recorded in the study protocol. A physician reviewed the results from study samples once a week, and appropriate action was taken if neces-sary. Six infants were considered to have anaemia at 2 days of age (for defi-nitions see below) and were referred for further diagnostics, but none of them needed treatment.

25
4 and 12 month data At 4 months of age, infants were scheduled for a follow up visit including blood sampling, weight and length measurements. Venous blood sampling was performed after application of a local anaesthetic (EMLA®, Astra-Zeneca). Before discharge from the postnatal ward, the family was asked to regularly record data regarding their infant’s health (fever, visit to doctors, etc, see details below) until the visit at 4 months (the ‘morbidity question-naire’).
In the morbidity questionnaire, parents were asked to note, on a daily ba-sis, if the child had: symptoms of infection (fever 38.0 or more), abdominal problems (watery diarrhoea; loose stools; hard stools; abdominal pain; vom-iting), airway problems (cough; breathing difficulties; rhinorrhoea/runny nose; nasal congestion), other problems (otitis; rash; excessive crying; tired-ness), visiting a doctor (paediatrician; other doctor), if the child had antibiot-ics and if the child had been admitted to hospital. This questionnaire was previously used by Berglund et al.77
One month before the planned 4 and 12 month visits, parents received a letter including instructions for a food diary, the appropriate Ages and Stages Questionnaire (ASQ) directed to 4 or 12 month old infants, respectively, and the suggested date and time for the visit. Parents were asked to complete the 3-day food diary before the visit to assess whether the infant was exclusively or partially breastfed and whether formula or solids were given at 4 months, and to assess the overall nutritional intake at 12 months. Also the food diary was previously used by Berglund et al.77 The parents could answer the ASQ at home, or at the follow up visit. Table 1 gives a summary of the collected infant data.
Table 1. Overview of collected infant data
Birth 2-3 days 4 months 12 months
Neonatal morbidity§ X
Length and weight X X x
Complete blood count* X x X x
Iron status†, CRP X x X x
Bilirubin x
IgG X x X
Morbidity questionnaire X
Food diary X x
ASQ X x §Neonatal morbidity: Respiratory symptoms, newborn have been breast fed and mid-wife assessed ‘well being’. *Complete blood count: Hb, Hct, MCV, MCHC, Rtc and RetHE. †Iron status: Serum iron, transferrin, serum ferritin, TS and TfR

26
Blood samples All blood samples were analysed for ‘complete blood count’: Hb, Hct, MCV, mean cell haemoglobin concentration (MCHC), reticulocyte count (Rtc), and reticulocyte haemoglobin (RetHE); ‘iron status’: serum iron, transferrin, serum ferritin, TS and TfR, and: C-reactive protein (CRP). Bilirubin was analysed at 2-3 days and IgG at birth, 2-3 days and 4 months, Table 1.
Blood was collected in EDTA tubes (BD Vacutainer®, Plymouth, UK) for complete blood count, and in serum separator tubes (BD Vacutainer®) for iron status, bilirubin and CRP.
Blood samples were stored for a maximum of 1 h in room temperature and then transported to the hospital’s clinical chemistry laboratory where analyses were performed. Complete blood counts were analysed using the automated haematology analyser Sysmex XE 2100 (Sysmex, Kobe, Japan). Iron status indicators, bilirubin and CRP were analysed using Cobas 6000 (Roche Diagnostics, Basel, Switzerland). Immunoglobulin G was analysed with the Beckman IMMAGE Immunochemistry System (Beckman Coulter, Brea, CA, USA).
Definitions and reference range for anaemia and iron status indicators used for defining iron deficiency are presented in Table 2. Iron deficiency was defined as present when at least two (out of four) iron status indicators (MCV, ferritin, TS, TfR) were outside reference ranges.
Table 2. Definitions of anaemia and iron deficiency at different ages, and poly-cythemia and hyperbilirubinaemia at 2-3 days. Iron deficiency was defined as at least two (out of four) iron store indicators (MCV, ferritin, TS, TfR) outside refer-ence range33
2-3 days 4 months 12 months Anaemia
Hb (g/l) < 14578 < 10579 < 11080 Iron deficiency
MCV (fL) < 7379 < 7080 Ferritin (µg/l) < 2079 < 1280 TS (%) < 1081 < 1080 TfR (mg/l) > 779 > 5.9*
Polycythaemia Hematocrit (%) >6582
Hyperbilirubinaemia Bilirubin (µmol/l) >25722
.* Reference range for cut off 2 SD above the mean calculated in paper IV.
The TfR cut-off at 4 months of age for the Roche immunoturbidimetric as-say was calculated from the established cut-off value of 11 mg/l79 for the Ramco enzyme-linked immunosorbent assay (ELISA) assay, using the re-gression equation described by Pfieffer et al.83

27
At 4 months, the log ratio of TfR to ferritin (logTfR/Fer-ratio) was calcu-lated.84 TfR was converted to values corresponding to the Ramco ELISA assay83 then transformed to µg/l. The result was divided with Ferritin and the logarithm (base 10) of the ratio was used. Total body iron (mg/kg), as pre-sented in paper I, was approximated by the equation:
-(logTfR/Fer-ratio-2.8229)/0.1207.85
Ages and Stages Questionnaire (ASQ) The ASQ86 is a series of parent-report questionnaires that span the age range of 4 to 60 months. Each questionnaire is composed of 3 sections: a brief set of demographic items; 30 questions about the infant's or child's development spanning 5 different domains (communication, gross motor, fine motor, problem-solving, and personal/social); and 7 open-ended questions eliciting parental concerns. The choice of responses for each item is ‘yes’, ‘some-times’, or ‘not yet’, which are scored as 10, 5, or 0, respectively. The sum of the scores from the questions in each domain is compared with a cut-off score. It takes about 10 to 15 min to complete the questionnaire and roughly 5 min to score it.
For the purpose of using ASQ in our studies, permission was obtained from Paul H Brookes Publishing Co. (PO Box 10624, Baltimore, MD 21285, USA) to translate and use the ASQ 4 and 12 months questionnaires. The English original was first translated to Swedish, and then re-translated by an English-born professional translator: the two English versions were com-pared and small adjustments were made in the Swedish translation before it was used.
Sample size As ferritin is the most sensitive indicator of iron status and has been shown to be the most efficient indicator of iron supplementation interventions,87 it was chosen for estimating group size. Beyond the neonatal period, the main effect observed in studies comparing DCC versus ECC is that DCC leads to an increase in ferritin at 3-6 months of age, an effect which has been consid-ered of public health significance.14 16 19 We therefore chose iron status at 4 months as our main outcome and powered the study to find a difference in ferritin. A prestudy power analysis showed that a group size of 150 would allow us to find a difference of 29% in geometric mean serum ferritin be-tween groups at 4 months of age with a power of 80% and a significance level of 0.05, assuming a mean serum ferritin of 110 µg/l in the DCC group.88 The study was thus powered to find a slightly smaller difference in ferritin than in a previous study in Mexico,19 in which the DCC group had 34% higher serum ferritin at 6 months. Allowing for an attrition of 25%, we included 200 participants in each randomisation group.

28
Statistical analysis For group comparisons of continuous variables, Student’s t-test was used for variables with normal distribution. For variables with skewed distribution Mann-Whitney U test was used for group comparisons and for confidence interval (CI) across groups Hodges and Lehmann estimator89 was used. Fer-ritin was log10 transformed for analysis. Categorical variables were com-pared between groups by using Fisher’s exact test. The Statistical Package for Social Sciences for Windows, version 18.0, was used (SPSS, Inc., Chi-cago, IL, USA). Numbers needed to treat, Relative risk reduction and their CI were calculated by the web-based JavaStat calculator.90 A p-value less than 0.05 was considered significant.
All analyses were made on an intention to treat basis, after exclusion of 12 cases (DCC; n=4, ECC; n=8) which were erroneously included in the study in spite of not fulfilling inclusion criteria and 6 cases where parents chose to stop participating immediately after the delivery. Of the 382 finally analysed children, 334 received the allocated intervention (DCC; n=168, ECC; n=166), Figure 5.
We redid all analyses for the main and secondary outcomes, including cases of protocol breach at inclusion as well as per protocol (n=334) and this did not alter the results. We also did a sensitivity analysis for outcomes at 4 months of age by calculating imputed results for dropouts after 2 days of age (n=25), and the results did not change
Calculations of Spearman’s rank correlation coefficient (rs) were used to determine neonatal and 4-month variables that were associated with out-comes at 12 months (ferritin and ASQ total score). Variables with a correla-tion significance of <.05 for each outcome were then entered into a linear regression model and analyzed by stepwise backwards selection, leaving only variables with a p-value less than 0.05 in the model.
Ethical considerations All research involving newborn infants and small children need careful ethi-cal considerations, mainly since the subjects themselves can’t agree to whether they want to participate in the study or not. In particular, research that is not immediately of benefit for the patients needs ethical consideration. The included infants were healthy full-term infants undergoing umbilical cord clamping, which is a standard procedure after birth. Previous data indi-cate that delayed cord clamping may be beneficial. The infants were ran-domised to either early or delayed cord clamping in a hospital with the rou-tine of performing early cord clamping. Included infants were either sub-jected to standard care or an intervention that had been standard care at the

29
hospital earlier, and that was standard care in other Swedish hospitals at commence of the study.
The possible benefit of the intervention (DCC) of increasing iron stores was estimated to be higher than the risk of probable risks, such as hyper-bilirubinaemia.
Blood sampling can be a painful procedure and was performed at 4 times during the study. At birth, the sampling of the umbilical cord is not consid-ered painful, and was a routine in the hospital. The second blood sample at 2-3 days was chosen to be performed in connection with the metabolic screening blood sample to minimise pain. The last two blood samples may have caused pain, but all measures possible were considered to minimise the infants’ discomfort, including application of a local anaesthetic cream. Al-though there were only a few cases with IDA, these infants were discovered and treated and thereby had benefit of participating in the study.
The study was approved by the regional research ethics committee at Lund University (41/2008). Written informed parental consent was obtained before the intervention, and parents could withdraw from the study at any time without any need for explanations.

30
Figure 5. Trial profile (after CONSORT flowchart).

31
Results
The recruitment period lasted 16 April 2008 to 22 May 2009. In total 2025 deliveries took place at the Hospital of Halland in Halmstad during this time period. At the time the calculated sample size of 400 had been randomised, a total of 1063 women were assessed to have been eligible for the study, re-sulting in 663 not having been randomised for various reasons (declined participation or had not been approached by the midwives), Figure 5.
Maternal characteristics There were no significant differences in maternal characteristics between the DCC and ECC groups. Neither did maternal characteristics differ between the randomisation groups among those who continued participation in the study with follow up at 4 and 12 months, respectively.
Not reported elsewhere is maternal dietary preferences and use of iron supplementation during pregnancy: a total of 19 women stated that they were vegetarians, 11(6%) in the DCC group and 8 (4%) in the ECC group, p=0.6. A majority of all women had taken iron supplements during pregnancy, 175 (92%) in the DCC group and 167 (88%) in the ECC group, p=0.24.
Newborn characteristics Randomisation was successful as groups were comparable in most aspects. Data on newborn characteristics are presented in Table 3.
Table 3. Newborn infant characteristics a
DCC (n=193) ECC (n=189) p Gestational age, w 40.0 (1.1) 40.1 (1.1)Birth weight, g 3629 (460) 3533 (486) 0.05b Birth length, cm 50.9 (1.9) 50.8 (1.9)Head circumference, cm 34.9 (1.4) 34.7 (1.4)1-min Apgar score >6 188 (97%) 181 (96%)Male gender 86 (45%) 93 (49%)Umbilical cord haemoglobin, g/l 159 (18) 163 (16) 0.01c Umbilical cord haematocrit, % 47 (5) 49 (4) 0.01d a Data are mean (SD), proportions or counts (%). b Mean difference 96g (95% CI 0.3 to 191), c -4.7 g/l (95% CI -8.4 to -1.1), d -1.3% (95% CI -2.4 to -0.3)

32
The differences between the two groups in birth weight, Hb and Hct were not expected, and a probable explanation is offered in the discussion.
Per protocol analysis of background characteristics When analysing the 334 cases performed per protocol, there were no signifi-cant differences in maternal background data, and the differences between the randomisation groups in birth weight (109 g [7 to 211], p=0.036), um-bilical cord Hb (-5.3 g/l [-9.1 to -1.5], p=.006) and Hct (-1.6% [-2.7 to -0.5], p=.004) were all strengthened.
Main results
Obstetric outcome (paper II)
Post partum haemorrhage There were no differences between the DCC and ECC groups in median volumes of PPH, or in the proportion of women with PPH >500 ml, or se-vere PPH >1000 ml. Per protocol analysis did not change these results, Fig-ure 6.
Figure 6. Proportion of mothers with PPH >500 ml and PPH >1000 ml in relation to time to umbilical cord clamping. There were no significant differences between the two randomisation groups (ECC n=189; DCC n=192). Figures in the bars are num-bers of cases.
Length of third stage labour There were no differences between groups in median time of third stage labour, or in the proportion of cases with third stage labour longer than 30

33
and 60 min, respectively. There were four cases in the ECC group with a duration of third stage labour of more than 60 min, compared to none in the DCC group p=0.058, Figure 7. Per protocol analysis did not change results in any significant way.
Figure 7. Length of third stage labour in the two randomisation groups.
Among the 380 cases with available data on both PPH and length of third stage labour, there was a strong association between PPH >500 ml and length of third stage labour > 30 min, relative risk (RR) 4.6 (95% CI 2.5 to 6.6).
Oxytocin use Oxytocin was administered in comparable ratios to the DCC (73%, n=141) and ECC (78%, n=148) groups, p=0.24, and did not affect PPH significantly. The midwives were instructed to administer oxytocin immediately after clamping, and the time for administration was not recorded. The amount of PPH did not differ between the 289 women who received oxytocin and the 93 that did not receive oxytocin,: median (range) 350 (100-6500) ml vs. 350 (150-2100) ml, p=0.6.

34
Proportion of ‘valid’ blood gases The process of identifying valid arterial umbilical blood gases is described in detail in paper II. In brief, a valid umbilical artery sample has a lower pH (<0.2 units) and higher pCO2 (difference >0.5 kPa according to Westgate et al58, and >0.7 kPa according to Kro et al61). Significantly fewer blood sam-ples were obtained in the DCC group, but the rate of valid samples did not differ between the randomisation groups, neither when using the method proposed by Westgate et al58; difference in proportions -6.2% (95%CI -15.7 to 3.5) nor when using the method by Kro et al61; difference in proportions -5.1% (-14.8 to 4.8). The results did not change significantly when analysed per protocol, difference in proportions -4.4% (95% CI -14.5 to 5.8) and -3.2% (95%CI -13.6% to 7.3). Also when compared to earlier studies on vali-dating paired umbilical blood gas analysis, the proportions in this study were similar, Figure 8.58 61 91
Figure 8. Compilation of data from three studies evaluating proportions of valid blood gas samples, compared to the ECC and DCC groups in this thesis. Figures within bars are actual numbers (n). The sum of valid paired blood gas samples is around 70% in all studies.
Umbilical cord blood gases were similar in the two randomisation groups, both when compared as means (table 2, paper II) and when categorised as proportion of samples with pH<7.1: DCC 2.5% versus ECC 3.3%, p=0.8, or base deficit >12: DCC 4.3% versus ECC 2.8%, p=0.6. These results were comparable also when analysed per protocol.

35
Neonatal outcome (paper I) Infants in the two randomisation group differed significantly in birth weights, and infants in the DCC group had a mean birth weight that was 96 g higher than infants in the ECC group, Table 3.
Apgar scores at 1, 5 and 10 min were similar in the two groups, and in general high, reflecting the selected low-risk population, Figure 9.
Figure 9. Apgar scores at 1, 5, and 10 min in each randomisation group.
Respiratory symptoms Respiratory symptoms, observed when infants were 1 and 6 h, respectively, did not differ between groups, Table 4.
Table 4. Observed early respiratory symptoms in the two randomisation groups.
DCC, n(%) ECC, n(%) p 1 h 183 (95) 175(93)
Tachypnoea (>60 breaths/min) 12 (6.5) 10 (5.7) 0.8 Grunting 6 (3.2) 4 (2.2) 0.8 Nostril flaring 3 (1.6) 1 (0.6) 0.6 Retractions between or under the ribs - -Respiratory symptoms* 17 (9.3) 12 (6.9) 0.4
6 h 151 (80) 160 (83)Tachypnoea (>60 breaths/min) 6 (3.7) 5 (3.3) 1.0 Grunting 2 (1.3) 4 (2.6) 0.4 Nostril flaring 2 (1.3) 1 (0.7) 1.0 Retractions between or under the ribs 1 (0.6) 2 (1.3) 0.6 Respiratory symptoms* 6 (3.8) 8 (5.3) 0.6
*Respiratory symptoms = presence of at least one of the variables tachypnoea, grunting, nostril flaring or retractions
No differences were found between groups in infant well being at 1 and 6 h, as prospectively observed by midwives at 1 and 6 h, see as prospectively observed by midwives at 1 and 6 h, see Table 5.

36
Table 5. Newborns status at 1 and 6 h after birth
DCC, n(%) ECC, n(%) p 1 h
Breastfed 135 (74) 130 (73) 0.9 Appearing well 178 (96) 174 (97) 0.8
6 h Breastfed 131 (82) 131 (82) 0.5 Appearing well 152 (94) 149 (96) 0.8 Examined by paediatrician 8 (5) 7 (5) 1.0 Admitted to NICU 5 (3) 4 (3) 1.0
Bilirubin and jaundice Bilirubin data, measured at 2-3 days, are reported in paper I. Hyper-bilirubinaemia >257 mol/l was present in 4 infants (2.9%) in the DCC group and in 7 infants (5.4%) in the ECC group, p=0.37. Only 3 infants needed treatment with phototherapy, 1 in the DCC group and 2 in the ECC group. Figure 10 presents all bilirubin data, including transcutaneous measurements that were not reported previously. Addition of these data did not change the results.
Figure 10. This figure shows results of bilirubin measurements (blood samples and transcutaneous values) in the two randomisation groups during the first 5 days of life, excluding measurements after phototherapy.
A total of 20 newborns were admitted to the neonatal ward (NICU), 14 (7.7%) in the DCC group compared to 6 (3.4%) in the ECC group, p=0.11.

37
When analysing per protocol, 11 cases remained, 7 (4.5%) in the DCC group, and 4 (2.5%) in the ECC group, p=0.4, Table 6
Table 6. Diagnoses from the neonatal ward.
DCC, n=193 ECC, n=189 DCC, n=168 ECC, n=166
Intention to treat Per protocol Transient tachypnoea 2 (1.0) 2(1.1) 1 (0.6) 1 (0.6) Meconium aspiration 2 (1.0) 1 (0.5) 1 (0.6) Pneumonia 2 (1.0) 1 (0.5) 1 (0.6) Jaundice 1 (0.5) 1 (0.5) 1 (0.6) 1 (0.6) Hypoglycaemia 2 (1.0) 1 (0.5) 2 (1.0) 1 (0.6) Feeding difficulties 2 (1.0) 1 (0.6) Cleft palate 1 (0.5) 1 (0.5) Seizures 1 (0.5) Apgar <4 at 1 min 1 (0.5)
Data are numbers (%)
Haematological status and iron status (papers I and IV)
Neonatal, up 2 to 3 days Blood sampling at 2 to 3 days was coordinated with the planned blood sam-pling for metabolic screening, performed at a median (range) postnatal age of 2.4 (2.0 to 4.9) days in the DCC group and 2.4 (1.9 to 4.2) days in the ECC group, p=0.9.
As presented in Table 3, umbilical cord Hb and Hct were lower in the DCC group. However, at 2-3 days, Hb was higher in the DCC group, mean difference (CI 95%) 13.5 g/l (9.6 to 17.5), p<0.001, as well as Hct; 3.5 % (2.4 to 4.6) higher, p<0.001. Also MCHC was higher in the DCC group; 2.2 g/l (0.6 to 3.9), while all other values from the complete blood count and iron status were comparable between groups.
Anaemia (Hb<145 g/l) at 2-3 days was 5 times more common in the ECC group, relative risk reduction 0.80 (0.22 to 0.95), while no cases of poly-cythaemia was recorded at this time.
4 months The primary endpoint of this randomised controlled study was iron status at 4 months, with sample size calculated using ferritin levels. Blood samples were taken at a median (range) of 121 days (109 to 154) in the DCC group (n=174), and 121 days (110 to 140) in the ECC group (n=176).
Ferritin was 45% (CI 23% to 71%) higher in the DCC group, 117 μg/l versus 81 μg/l in the ECC group, p<0.001). All other indicators of iron status (MCV, TS, TfR) demonstrated significantly higher iron stores in the DCC group. The results remained statistically significant also when analysing per

38
protocol. Hb and Hct did not differ between the groups. Reticulocyte counts were higher in the DCC group, but the difference did not remain statistically significant when analysing per protocol.
Figure 11. Proportion of infants with iron deficiency at 4 months of age.
Iron deficiency, predefined as at least two iron status indicators outside ref-erence range, was significantly reduced from 5.7% in the ECC group to 0.6% in the DCC group, resulting in a relative risk reduction (95% CI) of 90% (38 to 98), Figure 11. Number needed to treat were 20 (17 to 67), sug-gesting that by every 20 births, 1 case of iron deficiency at four months could be prevented by practising DCC.
12 months Iron deficiency at 12 months was predefined as at least two out four iron status indicator out of reference range, (Ferritin < 12 µg/l, MCV<70 fl, TS < 10% and/or TfR>5.9 g/l) and IDA was defined as ID in combination with Hb<110g/l. Blood samples (n=337) were taken at a median (range) age of 365 days with no difference between the groups. Thirty-three samples were excluded (infant >13 months, CRP 10 mg/ml or higher), 22 in the DCC group and 11 in the ECC group, leaving 152 in each group.
No significant differences between DCC and ECC were found in iron status indicators, Hb or Hct, neither by comparing means or ratios outside reference ranges, Figure 12

39
Figure 12. Proportion of infants with iron deficiency at 12 months of age. No sig-nificant differences was found. At 12 months one infant in the ECC group had iron deficiency anaemia.
Trajectory analysis The ‘placental transfusion model’ suggests that a higher Hb after birth would protect against ID at 12 months. To test if the model was consistent with the findings in the present study, a correlation analysis was performed, including Hb at 2-3 days, iron status indicators (MCV, Ferritin, RetHE, TS, sTfR) and Hb at 12 months. No significant correlations were found. Newborns with neonatal anaemia at 2-3 days did not differ in iron status indicators at 12 months, compared with those having normal Hb. These results might imply that the placental transfusion model is not applicable when regarding even-tual protective effects against ID at 12 months of age.
Iron status at 4 months did affect iron status at 12 months. Ferritin at 12 months was strongly correlated with iron status indicator at 4 months (Table 1, paper IV). Infants with ID at 4 months had significantly lower MCV and ferritin at 12 months, Table 7. Two of the infants had IDA at four months of age and were treated with iron supplements.
Table 7. Hemoglobin and iron status indicators at 12 months in relation to presence or absence of iron deficiency (ID) at 4 months. Values are mean (SD).
ID at 4 monthsN=11
No ID at 4 monthsN=329 MD (95% CI) p
Hb (g/l) 117.5 (8.9) 118.9 (8.2) 1.4 (-5.2 to 8.1) 0.7 MCV (fl) 73.5 (3.1) 76.9 (3.2) 3.4 (0.8 to 6.0) 0.01 Ferritin (µg/l) 17.1 (0.23) 35.1 (0.23) 31 (14 to 48)† <0.001 Transferrin satura-tion (%) 12.3 (4.7) 15.5 (6.8) 3.2 (-1.9 to 8.3) 0.22
Transferrin receptors (g/l) 5.24 (1.90) 4.41 (0.88) -0.83 (-2.59 to 0.92) 0.29
†Geometric mean ratio in percentage. MD= mean difference.

40
Neurodevelopment (papers III and IV)
ASQ at 4 months (paper III) The 4-month ASQ was fully replied by 335 parents, 173 (94%) in the DCC group and 162 (90%) in the ECC group (p=0.3), and partially replied by another 30 (12 DCC and 18 ECC). The two groups had comparable total scores, but DCC had 1.7 (0.1 to 3.3) higher score in the problem solving domain, while ECC had 2.3 (0.5 to 4.1) higher score in the personal-social domain, Table 8.
Table 8. Neurodevelopment at 4 months, as assessed by the ASQ
Delayed cord clamping Early cord clamping p Total score 259 (28) 258 (29) 0.6 Communication 51 (8) 50 (8) 0.6 Gross motor 55 (7) 54 (8) 0.4 Fine motor 49 (10) 48 (11) 0.4 Problem solving 55 (7) 54 (8) 0.03 Personal-social 49 (9) 52 (8) 0.01 Total number of returned questionnaires: Delayed cord clamping=185, Early cord clamping= 180. Data are means (SD).
There were no significant differences regarding number of infants scoring under cut-off score between groups.
Figure 13. Proportion of infants (%) with scores below the cut-off (i.e. lower than minus 2SD) in ASQ domains at 4 months of age. Numbers in columns are the actual numbers of infants (n).
ASQ at 12 months (paper IV) In total 337/382 (88%) questionnaires were answered within one calendar month of the infant’s first birthday, 170/193 (88%) in the DCC group and

41
167/189 (88%) in the ECC group (p=1.0). The mean total score and the scores of the different domains did not differ between groups, Table 9.
Table 9. Neurodevelopment at 12 months, as assessed by the ASQ.
Delayed Cord Clamping Early Cord Clamping p Total score 230 (41) 233 (38) .4 Communication 40 (13) 40 (12) 1.0 Gross motor 47 (15) 48 (14) .4 Fine motor 52 (8) 52 (8) .8 Problem solving 47 (12) 48 (11) .4 Personal-social 44 (12) 44 (11) .6 Total number of returned questionnaires: Delayed cord clamping=170, Early cord clamp-ing=167. Data are means (SD).
The proportion of infants with scores below the cut-off level did not differ between the groups, Figure 14. In total, 27 (16%) of the children in the DCC group had results under cut-off in one or more domains, compared to 24 (14%) in the ECC group, p=0.8.
Figure 14. Proportion of infants (%) with scores below the cut-off (i.e. lower than minus 2SD) in ASQ domains at 12 months of age. Numbers in columns are the ac-tual numbers of infants (n). No significant differences were found.
Morbidity and IgG at 4 months (paper III) The morbidity questionnaire was returned for 360 infants (94%) at 4 months, 184 (95%) in the DCC group and 176 (93%) in the ECC group. There was no difference between the groups in the prevalence of symptoms. When comparing days with symptoms, the two groups only differed in the duration (days) with excessive crying, the mean (range) for the DCC group was 1.9 (0

42
to 71) days and for the ECC group 5.1 (0 to 123) days, p = 0.045. However, the difference was not significant when analysing per protocol, DCC 1.8 (0 to 71) days versus. ECC 4.3 (0 to 123) days, p=0.13.
Presence of fever, reported in 92 (26%) infants, was in 18 instances re-ported by parents as occurring in close relation to vaccinations. Excluding these cases from analysis, or only including reported fever during the first six weeks to avoid vaccination-related fever, did not change the results.
At 2-3 days, IgG was slightly, but significantly, higher in the DCC group, 11.7 (1.9) vs. 11.0 (1.8) g/l, p=0.004. The two groups did not differ at 4 months, 3.4 (0.9) g/l in the DCC group vs. 3.4 (0.9) g/l in the ECC group, p=0.7.
Growth and nutrition (papers I, III and IV)
Length and weight Except for the difference in birth weight, infants’ length and weight were similar at the next control points. At four months; the infants’ weights mean (SD) were in the DCC group 6.8 (0.9) kg vs. the ECC group 6.9 (0.8) kg, p=0.5, and their length were 64 (2) cm vs. 64 (2) cm, p=0.4. Both groups gained approximately 3.2 kg of weight up to 12 months of age; 10.0 (1.0) kg vs. 10.1 (1.1) kg, p=0.3 and grew 12 cm in length; 76 (2) cm vs. 76 (2) cm, p=0.7.
Breastfeeding/ feeding habits at four months Feeding habits were reported in a 3 day diary before the 4 month visit. Dia-ries were returned for 357 (93%) of the infants, 183 (95%) from the DCC and 174 (92%) from the ECC group. No significant differences in feeding habits were found, whether comparing exclusive breastfeeding (DCC 56%, ECC 51%, p=0.4), exclusive formula (DCC 20% vs. ECC 13%, p=0.12) or the specific amount formula and/or solids ingested. Per protocol analysis did not change these results.
Nutritional intake at 12 months Feeding habits were reported in a 3 day diary before the 12 month visit. Dia-ries were returned for 327 (85.6%) of the infants, 169 (87.6%) from the DCC and 158 (83.6%) from the ECC group. Feeding habits was not significantly different between the two groups when comparing energy intake, protein, fat, carbohydrates, minerals or vitamins, including iron.
Gender Presented in paper IV, infant gender correlated independently with both fer-ritin and ASQ at 12 months, as girls had higher ferritin and ASQ total score. Randomisation and gender was entered as fixed factors in an analysis of

43
covariance model. No interaction was found in the model concerning 12-month ferritin, but in the ASQ model there was a significant interaction, and randomisation to DCC was associated with 12 points lower ASQ score for girls, 230 (39) versus 242 (36) and 5 points higher score for boys, 229 (43) versus 224 (39), p=0.042 for the interaction term, Figure 15. The signifi-cance for the interaction was p=0.018, when data were analysed per proto-col.
Figure 15. Effect of randomisation group and gender on ASQ total score
In the different domains of the ASQ, the pattern of inverse results between boys and girls was significant for ‘fine motor’ scores, p=0.010 and ‘problem solving’, p=0.037.

44
Discussion
The time to umbilical cord clamping may have important impact on a popu-lation’s health, as shown by the results in this thesis and previous data. Even small effects on each individual may have great impact when multiplied in a large population. To demonstrate the size of effects cord clamping might have, the result showing that iron deficiency was reduced from 5.7 to 0.6 % at four months of age can be extrapolated. In a country like Sweden, a change of practice from ECC to DCC would spare approximately 5000 four month old infants from ID.
This study was set out to make a broad approach to the subject, and tried to evaluate a wide array of proposed effects of delayed versus early cord clamping, both those considered beneficial and those considered disadvanta-geous. Furthermore, we wanted to have longer outcomes than previous stud-ies, and included measures of neurodevelopment.
Several issues regarding effects of DCC as compared to ECC have shown contradictory results, such as risks for maternal PPH, and infants’ risk for polycythaemia and jaundice. Possible benefits of improved iron status in a high income country are not known. As our main outcome for the study, and also the base for the sample size estimation, ferritin level at 4 months was chosen. The reasons for this choice were mainly two: data on ferritin in this age group were previously published in Swedish infants,88 but ferritin levels as a result of DCC compared to ECC were also published in a large Mexican study.19 We also chose the suggested outcome since we considered the dif-ference in ferritin levels of 29% as clinically relevant.
As a theoretical framework we chose the ‘placental transfusion model’ (see Introduction, Figure 2) for the possible advantages of DCC. The in-creased placental transfusion associated with DCC will result in elevated neonatal haemoglobin, and probably persisting higher haemoglobin during the first two months of age. Through the normal turnover of red blood cells, haemoglobin is metabolised and transferred to iron stores. Increased haemo-globin would then result in increased iron stores, and could thus prevent iron deficiency, and as a consequence also protect infants from iron deficiency anaemia and iron deficiency-associated neurodevelopmental and behavioural deficits.
The main proposed disadvantages of DCC in newborn infants are associ-ated with events occurring close to birth, such as polycythaemia, respiratory distress and hyperbilirubinaemia and need for phototherapy. Reasons for

45
ECC in obstetric practice are decreased maternal post partum haemorrhage and to facilitate umbilical artery blood gas sampling.12 13
As for polycythaemia, usually defined as venous haematocrit above 65%, and increased blood viscosity, Hutton and Hassan16 did find significantly higher rates of polycythaemia associated with DCC, although they com-mented that no infant in any of the included studies in their review had been symptomatic. In the Cochrane report, the risk ratio of polycythemia by ECC compared to DCC was estimated to 0.39 (95%CI 0.12 to 1.27).14 In our study, no case of polycythemia was noted in either group, suggesting that neonatal polycythemia may be more of a problem in risk groups associated with high intrauterine haematocrit such as maternal diabetes and intrauterine growth restriction.92 93
There are conflicting results, also in meta-analyses, regarding the risks for hyperbilirubinaemia after DCC. In a meta-analysis from 2007, Hutton and Hassan16 concluded that DCC was not associated with a higher mean of bilirubin, or a higher risk for, clinical jaundice (8 studies) or use of photo-therapy (3 studies), in contrast to results published in another meta-analysis, by van Rheenen et al three years earlier,22 demonstrating a higher risk of hyperbilirubinaemia after DCC (4 studies). Also the Cochrane analysis14 from 2008 suggested that DCC was associated with increased risk for jaun-dice requiring phototherapy (5 studies) but not for clinical jaundice (5 stud-ies). In this Cochrane analysis also unpublished data were included, contrib-uting with over 50% of the data forming the basis for the conclusions. In the present study, we did not find any indications of neither higher bilirubin, nor of proportion of infants having hyperbilirubinaemia or use of phototherapy in the DCC group. However, our population is a selected healthy population of term infants, and very few infants (<1%) actually needed phototherapy.
A transiently higher respiratory rate after DCC was shown by Yao & al20 in 1971, but neither Hutton & Hassan or the Cochrane report did find any significantly higher risks of respiratory symptoms associated with DCC.14 16 In our study, we observed infants for signs of respiratory distress at 1 and 6 hours, and did not find any differences between the two groups.
In her extensive literature review on cord clamping effects, published in 2001, Mercer mentioned the possibility that the higher neonatal haemoglobin after DCC could be associated with improved breastfeeding and digestion.94 In our cohort of infants, we could not demonstrate find any positive effects of DCC on breastfeeding or bowel symptoms up to four months of age.
Data on obstetric complications, such as PPH, were not consistently re-ported in earlier cord clamping trials. Early cord clamping was previously a part of AMTSL, but has been abandoned in recommendations by the Interna-tional Confederation of Midwives and the International Federation of Gy-naecology and Obstetrics since 2006.40 Still, effects on PPH from time to cord clamping have not been extensively evaluated. In our study we could not demonstrate any effects on PPH in relation to early or delayed cord

46
clamping, which is in concordance to the 2008 Cochrane report.14 The time of third stage labour was comparable between the two groups in our study, although it must be noted that all four cases with a retained placenta after 60 minutes were in the ECC group. In the Cochrane report from 2008, McDon-ald reported an even distribution of retained placenta >60 minutes, (10/483 in the DCC group versus 8/480 in the ECC group).14
Securing a blood gas sample from one of the umbilical arteries has been suggested to be an important part of obstetrical quality management and may also have medicolegal implications.13 57 In the current project we compared the established method of umbilical artery blood gas sampling with an alter-native method that has been described previously59-61. To our knowledge there are no previously published data from a randomised trial evaluating this method for obtaining umbilical cord blood gas samples from an un-clamped cord in relation to samples taken from the immediately clamped cord.
Our results suggest that it is possible to collect umbilical cord blood gas samples in a comparable ratio as for the established method, compensating a somewhat lower ratio of blood samples with a higher accuracy in sampling, i.e. blood samples obtained from an artery.
Iron status In paper I, the first steps of the ’placental transfusion model’ were explored and confirmed, and Hb was significantly higher at 2-3 days in the DCC group. The mean Hb difference between the DCC group and the ECC group was 14 g/L. In agreement to this result, a weighted mean difference of 13.4 g/L was calculated from data from Emhamed and Cernadas in the Cochrane review from 2008.14 18 95 These results support older findings, and already in a review from 1967,25 Moss and Monset-Couchard observed an almost uni-form rise in Hb after DCC compared to ECC.
As to the study’s main finding, ferritin level at four months, a 45% higher ferritin in the DCC infants was shown. Similar results were earlier shown in Mexico (2006), where Chaparro et al demonstrated a 47% higher ferritin level among 6 month old infants who were clamped 2 minutes after birth as compared to infants subjected to ECC. Also in Argentina (2010), Ceriani Cernadas could show a significantly higher ferritin (59%) at 6 months after 3 minutes of DCC as compared to ECC. However, when cord clamping was delayed for only 1 minute, the 22% higher ferritin, compared to the ECC group, was not significant. In summary, the finding in this thesis strengthens the theory of DCC improving iron stores at 4-6 months of age.
Ferritin has been challenged as the most appropriate indicator of iron stores, mainly due to its sensitivity to inflammation. In addition to the ‘tradi-tional’ other iron store indicators MCV and TS, also TfR and RetHE have been suggested to be valuable tools when assessing iron status.96 97 As all indicators were available for analysis in the current study, we did perform

47
this additional evaluation on iron status. We showed that all iron status indi-cators differed significantly between the two groups, in the direction of less iron stores in the ECC group at four months. When defining iron deficiency as two out of four iron status indicators (ferritin, MCV, TS, TfR) outside of reference range, as earlier performed also by Male et al and Berglund et al,33
77 DCC reduced the prevalence of iron deficiency with 90%, avoiding one case of ID by every 20 births with DCC.
Eight months later, when infants were 12 months old, differences in iron status were no longer present and we could not show any remaining effects of delayed cord clamping on blood parameters or iron status (paper IV). Interestingly, iron status seemed to have improved greatly in 12 month in-fants in Sweden, in a cohort examined 1991-1992, 26% of the infants had a ferritin level < 12 µg/l, in comparison with 1.7% in our study, probably re-flecting adherence to a national recommendation issued in 1999 emphasising avoidance of cow’s milk as a beverage and promoting iron-fortified cereals during the second half of the first year.98 We could demonstrate significant correlations between iron status indicators at 4 and 12 months, but other factors, such as the infants’ diet, seem to be more important for iron stores at 12 months.
Neurodevelopment As part of the final step of the ’placental transfusion model’, iron deficiency is hypothesised to affect brain structure and neurodevelopment and by pro-tecting infants against ID, DCC may help to optimise neurodevelopment. To our knowledge, only one study evaluating effects on time to cord clamping has explored the possible association between DCC and neurodevelopment. In 2010, Mercer et al demonstrated a protective effect of DCC on motor disability at 7 months in very low birth weight males.99
We chose to evaluate infants’ neurodevelopment by using the ASQ as a tool, being widely used as a screening instrument for developmental abnor-mality. When comparing total ASQ score, DCC and ECC groups did not differ significantly at either 4 or 12 months of age. However, as for the ASQ subdomains, there were significant differences in the personal-social and problem solving scores at 4 months, although there was no difference in number of infants below cut-off score. ASQ is a screening tool, validated when used for finding children with results under cut off score within the subdomains. ASQ mean scores are based on ordinal data, not continuous, why there is not a clear relationship between higher mean score and better neurodevelopment. However, results from mean total score and mean sub-domain scores have been used in evaluations of development. 100 101
In summary, the results from paper III and IV suggests that neurodevel-opment during the first year of life is not affected in any major way by de-laying cord clamping in a selected population of healthy infants born at term after an uncomplicated pregnancy. The study does not give answers on if

48
DCC could affect populations with higher risk of ID, such as children born in areas of the world where ID endemic, or in children born prematurely or with intrauterine growth restriction.
Benefits and limitations This study’s major benefit; a long term approach trying to cover both iron status and neurodevelopment while also extensively analysing other out-comes, is also the study’s major limitation as it raises questions on sample size and choosing outcomes to report. Except for the effect on the primary outcome ferritin, this randomised controlled trial could rather be regarded as an exploratory pilot study when it concerns results from the 12 month fol-low-up. Using several different measurements on iron stores could cause contradictory results, but when all indicators point in the same direction, we see this rather as strengthening the conclusion that DCC enhances iron stores at 4 months but has no lasting effect on 12 month iron stores.
Except for the blood samples analysing iron stores, the study rests heavily on parents’ reports by different questionnaires, including the morbidity pro-tocol at 4 months, the food diaries at 4 and 12 month, and most importantly; the ASQ at 4 and 12 months of age. The ASQ has been evaluated for inter-reporter validity, and also reliability in concordance to other tests and has proven qualities within these areas enough to defend it’s place in the study, while such evaluations have not been made on the food diary or morbidity protocols, leaving a higher methodological uncertainty to the results from these questionnaires.
Data concerning maternal outcomes and the newborn postnatal morbidity were observed and reported by midwives on the obstetric and postnatal ward. Although we don’t find it likely, it cannot be ruled out with certainty that the midwifes, even if not being present at the birth of the baby and wit-nessing the intervention, still had knowledge of what intervention the spe-cific newborn had undergone, and by that might have been biased in their assessments.
Gender Perhaps the most uncertain question concerns the possible association be-tween gender and the results of ASQ at 12 months. Boys in general have a higher risk for ID in infancy102 and also had lower mean levels of ferritin in this study. Randomisation to DCC seemed to have positive effects on boy’s ASQ score, while girls, having higher iron stores also in the ECC group, seemed to have no benefits of DCC on ASQ, rather the opposite. Future research in cord clamping and iron deficiency may benefit in taking into account the aspect of gender.
In this study, the main perspective has been on long term (up to 12
months) effects of DCC versus ECC on term healthy infants, with focus on

49
iron stores and neurodevelopment. Two other suggested major benefits of DCC have not been explored: effect on preterms and providing a high con-centration of stem cells in the extra blood transferred. Delayed cord clamp-ing has a fairly established positive effect on preterms hemodynamics during the first days of life, and the following reduction in blood transfusion rates and intraventricular haemorrhage,103 but also possible protective effects on late-onset sepsis, and in male very low birth weight infants against motor disability. 99 104
In the vulnerable group of preterm infants cord milking has also been studied as an alternative to DCC with positive results105-107. In healthy term infants, the need to rush the placental transfusion with cord milking does not seem to be important, but it may be for the second suggested benefit not explored in this thesis; the high content of haematopoietic stem cell in cord blood, and the possible advantage for the asphyxiated newborn to have ac-cess to these cells.108 109
This thesis has shown that DCC improves iron stores at 4 months of age, thereby lending partly support for the ‘placental transfusion model’, while none of the suggested disadvantages of DCC has been demonstrated to have occurred in the study. As for the proposed long term positive effect on iron status and neurodevelopment, no such evidence was discovered up to 12 months of age, but the implied gender difference in neurodevelopmental response raises future questions.

50
Conclusions
In the population studied in this thesis, term infants born after an uncompli-cated pregnancy by healthy mothers, delayed cord clamping improved iron stores and prevented iron deficiency at 4 months of age. This effect was not sustained at 12 months. Neurodevelopment up to 12 months after birth was not affected in any major way by DCC versus ECC, but the study might have been underpowered for this outcome. A question of gender specific outcome after DCC compared to ECC on neurodevelopment at 12 months was dis-covered, implying positive effects on boys and negative on girls after DCC.
DCC could not be found to be associated with any higher risks for mater-nal post partum haemorrhage and did not exclude the possibility to achieve a reliable umbilical artery blood gas sample.
Infant morbidity was not affected of delayed as compared to early cord clamping, neither when regarding the neonatal period (hyperbilirubinae-mia/jaundice, respiratory symtoms, polycythemia), nor the first 4 months of life (infection symptoms, gastro intestinal problems, contact with doctors).
We conclude that delaying umbilical cord clamping for 180 sec is a safe and feasible alternative when handling childbirth. Iron deficiency is signifi-cantly reduced at 4 months of age, and the effects on neurodevelopment may not yet be seen at 12 months, why it cannot be excluded that effects on neu-rodevelopment may be discovered at an older age.

51
Future perspectives
As delayed cord clamping seems to be a safe alternative for childbirth, it might be considered also when handling asphyxiated newborns after i.e. nuchal cord and shoulder dystocia,110 as the placenta in theory could supply the newborn with fresh, oxygenated blood with new available glucose con-tent, as well as a high concentration of stem cells. Recently synergistic neu-roprotective effects when combining hypothermia and mesenchymal stem cells was demonstrated in vitro on neurons from rat.109 Designing a random-ised controlled trial to study suggested benefits of delayed cord clamping on asphyxiated infants would be difficult but might be very important.
Umbilical haematopoietic stem cells are an important source for stem cell transplantations, and a obvious ethical question has arisen as DCC has started to be recommended in several guidelines.111
The thesis has studied healthy, term infants, excluding infants known to have high haemoglobin at birth, for example intra uterine growth restricted newborns, and newborns to mothers with diabetes. Research on effects and safety of DCC compared to ECC in these groups would be very valuable.
Considering the results in this thesis, two questions clearly stand out: long term neurodevelopment and possible contrary gender effects. By the time this thesis is presented, in May 2013, we end a follow up study on the infants at 4 years of age. This follow up study has evaluated neurodevelopment and behaviour by a psychologist performing WPPSI-3 and the fine motor part of Movement ABC, while also asking parents to answer two questionnaires, ASQ 48 months, and the Strengths & Difficulties Questionnaire. Results from this follow up will be analysed and might elucidate the question of long term neurodevelopment further.

52
Swedish summary
Denna avhandling undersöker om tidpunkten för klampning (avklämning) av navelsträngen efter barns födelse påverkar deras hälsa under det första lev-nadsåret. Om man klämmer av navelsträngen direkt efter barnets födelse går barnet miste om att få ett tillskott av blod från moderkakan, jämfört med om man väntar ett par minuter. Det extra blod som barnet får kan uppgå till 30% av barnets blodvolym, eller ca 100 ml för ett barn som väger 3,5 kg.
Med sen klampning menas att barnmorskan väntar minst 2-3 minuter med att sätta en klämma på navelsträngen och tidig klampning sker när barn-morskan klämmer av inom 10-30 sekunder efter barnets födelse.
När denna studie startade praktiserades tidig klampning av navelsträngen på cirka 2/3 av Sveriges förlossningsavdelningar. De två främsta skälen för tidig klampning var dels att tidig klampning ansetts kunna minska moderns blödning efter förlossningen, dels skulle det vara enklare att ta ett blodgas-prov från navelsträngen, en rutin som görs på de flesta sjukhus som del i bedömningen av det nyfödda barnet och för kvalitetssäkring av förlossning-en.
Studien som avhandlingen handlar om har följt 400 barn som lottades till att få sin navelsträng antingen sent eller tidigt klampad efter en okomplice-rad graviditet av friska mödrar,. Data kring barnen samlades in under ny-föddhetsperioden, och vid 4 respektive 12 månaders ålder.
Resultaten från studien har presenterats i fyra artiklar. I artikel 1 visas att järnförråden vid fyra månaders ålder var bättre bland de sent klampade bar-nen. Ferritin, som är ett mått på järnförråd, var 45% högre och det var bara ett barn som hade järnbrist jämfört med 10 barn i den tidigt klampade grup-pen. Sent klampade barns Hb var högre vid 2-3 dagars ålder utan att några påvisbara negativa konsekvenser i form av ökad andel barn med gulsot, and-ningspåverkan eller blodstockning.
I artikel 2 undersöktes mödrarnas blödningsmängd efter förlossningen och den skilde sig inte mellan grupperna, varken vad gäller den totala blöd-ningsmängden, eller andelen kvinnor med större blödning än 500 respektive 1000 ml. Andelen blodgasprover som verkligen säkert var tagna från en na-velartär skilde sig inte åt mellan grupperna, 69% i den sent klampade grup-pen och 73% i den tidigt klampade gruppen.
Artikel 3 handlar om barnet utveckling och hälsa upp till fyra månaders ålder. Föräldrarna fick besvara ett formulär, Ages & Stages Questionnaire (ASQ) om deras barns utveckling. Frågorna i ASQ är fördelade med 6 frågor

53
i 5 domäner: kommunikation, grovmotorik, finmotorik, problemlösning och personligt-socialt. Totalpoängen skilde sig inte åt mellan barnen, men de sent klampade barnen hade något högre poäng i problemlösningsdomänen och de tidigt klampade i personligt-socialt.
De sent klampade barnen hade lite högre mängd immunoglobulin G i blo-det vid 2-3 dagars ålder, men vid 4 månaders ålder var det inte någon skill-nad. Föräldrarna ombads att under barnets första fyra månader dagligen markera på ett blad om deras barn haft olika typer av kroppsliga besvär. För-utom en tendens till att de tidigt klampade barnen hade fler dagar då de var skrikiga, hittades ingen skillnad i besvär mellan de olika grupperna, det vill säga sen klampning verkade inte göra barnen varken friskare, men inte heller sjukare.
Den sista artikeln, artikel 4, handlar om uppföljningen av barnen vid 12 månaders ålder. I den analyseras blod- och järnstatus samt resultatet av ASQ. Det fanns inte några skillnader mellan grupperna i sin helhet. Hypotesen som studien byggde på, att ett högre Hb (efter sen klampning) skulle förhindra järnbrist och förbättra utvecklingen vid 12 månaders ålder gick inte att visa. Däremot fanns tecken på att sen klampning skulle påverka pojkar utveck-lingsmässigt positivt, medan flickor hade bättre utveckling i den tidigt klam-pade gruppen. De lägre järnförråd som den tidigt klampade gruppen hade vid fyra månaders ålder hade barnen på egen hand korrigerat fram till 12 måna-ders ålder, troligen via ett högre upptag av järn via kosten.
Sammanfattningsvis har denna studie tydligt visat att barn som är sent klampade får bättre järnförråd och mindre järnbrist vid fyra månaders ålder, utan att detta har varit kopplat till några negativa följder. Sen klampning verkar var en säker metod att använda vid normala förlossningar. Studien har tillfört kunskapen att även barn födda i ett land med högt inkomstläge har fördel av sen klampning när det gäller deras järnförråd vid 4 månaders ålder.
Vid 12 månaders ålder kan man inte se någon kvarstående effekt av sen klampning vad det gäller järnförråd eller utveckling, men en möjlig skillnad mellan hur pojkar och flickor utvecklas beroende på hur deras navelsträngar har klampats.
Ett flertal frågor gällande sen och tidig klampning återstår. Även om ett flertal studier visat att för tidigt födda barn har stor nytta av sen klampning, så råder det osäkerhet om hur länge man kan vänta med att klampa, och om det eventuellt är bättre att mjölka fram blodet från navelsträngen till barnet.
Sen klampning skulle kunna innebära fördelar för barn som föds med sy-rebrist, dels innehåller navelsträngsblodet syre och socker som barn med syrebrist behöver, dels är koncentrationen av stamceller mycket hög.
För barn som föds tillväxthämmade eller har mödrar med diabetes skulle sen klampning snarare kunna vara till nackdel, dessa barn föds med ett högt blodvärde och det extra tillskottet av blod kanske kan inverka negativt på deras välbefinnande, varför forskning kring detta vore viktigt.

54
Som resultat av denna avhandling återstår det att undersöka om de lägre järnförråd, och högre andel järnbrist, som de tidigt klampade barnen hade vid fyra månaders ålder kan ha påverkan på deras utveckling högre upp i åldrarna. Flera viktiga delar av hjärnans mognad pågår under det första halv-året av barnets liv, och de funktioner som grundläggs då går inte att under-söka på ett bra sätt förrän barnet kommer upp i uppskattningsvis 3 till 5 års ålder. Den möjliga skillnaden mellan pojkar och flickors utveckling och klampning behöver också undersökas vidare. Den underliggande förklaring-en till detta fynd skulle delvis kunna vara att pojkar allmän har lägre järnför-råd tidigt i livet, och skulle därför ha större nytta av sen klampning och den extra tillförsel av järn som sen klampning visat sig kunna ge.

55
Acknowledgements
From the time the idea of this study was just an embryo, I have met over-whelming interest and support from so many people, without whom this thesis would not have been accomplished.
First of all I would like to thank all the participating children and in par-ticular their parents for daring to let their newborn be included in the study, and for so loyally returning for the follow-ups. Your contribution has already had an impact on cord clamping practice in Sweden.
Lena Hellström-Westas, my principal supervisor, for your brilliant mind, infinite patience and warm and empathetic personality. You started as a role model by your clinical work, and have shown to be even more so in research and as a friend. Thank you for encouraging me to strive further than I ever imagined, and for your never failing support at dire moments.
Magnus Domellöf, my co-supervisor, for sharing your extensive knowledge on iron and statistics. Your enthusiasm, curiosity and quick thinking have been an invaluable part of this study, as your generous contribution with materials and experience from the JOHN study.
Dan Andersson, my first and most important role model in neonatology and my co-author. As head of the Paediatrics department in Halmstad have you been of most importance by providing an unsurpassed support for the study
Monika Nygren and Eivor Kjellberg, for your everlasting work and energy in performing almost all data collection in the study, for meeting every sin-gle family with warmth and professionalism, and for convincing so many to stay in the study. Without you, there would be no study.
Birgitta Bengtsson, Meta Elwing, Agneta Hall, Susanne Isaksson, Mats Sundqvist, Anne-Lie Larsson, Anette Wiedesheim-Paul, Ingela Larsson and my co-author Jesper Clausen for participating in the planning and im-plementation of the study at the Obstetrics department in Halmstad, and all of your colleagues who helped to recruit pregnant women into the study.
All midwives at the antenatal units in Halland and northern Skåne for in-forming expecting parents and recruiting them into the study.

56
Josefin Roswall, my sister-in-arms when it comes to research work. Thanks for being a most vital part of the study, in planning, coordinating and co-operation. But most of all for "just being there" when I needed it, sharing your steady support and understanding. It's your turn soon...
Anna Kasemo, my "second wife", close friend and colleague, for working with the 4 months ASQ, making place for research time in my work sched-ule and for being a role model when it comes to loyalty and dutifulness.
Amir Baigi, Anders Holmén, Anna Nilsdotter, Annika Flink-Persson, Hanna Svensson, Marit Petrius, Pia Gruber, Ulf Strömberg and Yvonne Johnelius at the R&D department in Halmstad, for providing all kinds of support you could ever imagine was needed when planning and performing a trial. Most of all for always sharing laughs, friendship and free coffee.
Per Herrström and Birger Wandt for having created a R&D environment in Halmstad that now harvest so much important research in so many areas.
Eva-Stina Karlsson, Tom Lundahl and all staff at the department of Clini-cal Chemistry, Hallands hospital for taking such good care of all our blood samples and for being among the first in Sweden to analyse RetHE.
Jens Ladekjaer, my fellow neonatologist in Halmstad, for being there for all the newborns at our NICU while I was busy with research, but also for being the one who made me realise that I would suffice as a neonatologist.
Jan Rydnert, former head of the Department of Obstetrics and Gynaecology in Halmstad, for saying "yes" that lunch in June 2006.
Stefan Aronsson, for your curiosity, imagination, vast knowledge of ‘every-thing’ and for your valuable input to paper I.
Nils Östen Nilsson, for making me aware of the fact that iron deficiency does affect neurodevelopment by itself, not only through causing anaemia.
Anders Löfving and Karolina Mehkri for you interest and willingness to perform research work with data from the study.
Gregor Shapiro, for providing professional help on proof reading paper III and taking part in the ASQ translations.
Mattias Karlén, for making the illustration in paper II on how blood gas sampling can be performed without clamping the cord.

57
Magnus Hellstöm, Annika Hed, Lisa Almelund and Linn Källman for meticulous help with entering data into the computer.
Lotta and John Webb, for friendship and English proofreading and transla-tion.
Gerd Tangen, Bernt Alm, Stefan Bergman and Jovanna Dahlgren, Josefins collaborators in the ‘Growth project’, and thereby an integral part also of this study.
Uwe Ewald, Hugo Lagecrantz, Lennart Nordström, Mikael Norman and Ingela Wikström for support and interest throughout the study.
Judy Mercer, ‘grand old lady of cord clamping’, for kind interest, good advice and for being a living example of the saying: ‘a steady drop hollows a stone’.
Sten Bengtsson-Kihlvik at the publishing house ‘Egmont Kärnan’ for gen-erously letting us buy books to the included infants for a good price.
Anita Tilander at Minimundus, for helping us to give all the newborns in the study the softest of clothing, bodies with the text ‘Järnkoll på tillväxt!’
Ing-Marie Persson at ‘Furuvikens djurpark’ for generously sharing your knowledge on how chimpanzees handle their delivery and placenta.
All colleagues, friend and staff at the Paediatric department in Halmstad, for providing an environment characterised by play, joy, participation and safety. I am proud of being a part of your work.
All friends, for lots of fun and distractions from seriousness, but also inter-est and patience with me explaining, explaining, explaining how important the issue of cord clamping is.
Kerstin, my mother in law, and her Bo for providing a peaceful refuge for me, and my family in Kåseberga, ‘where the coastline plunge between sea and sky’.
Kitta, my aunt and godmother, and Jonas, my cousin, for being close and caring though all my life.
Åsa, my little sister, for your proud support but also for all teasing remarks, knowing my weaknesses like nobody else, and for finding Johnny and giv-ing us Lukas and Teres, the best cousins in the world.

58
Mamma, for being everything a mother should be and for continuous love.
Pappa, in living memory.
My wife Cecilia for making me aware of the issue of cord clamping, and thereby providing the spark that became this thesis, and for being my loved life companion and the mother to our children Olle, Måns and Lykke, more important to me than anything else.
The studies of this thesis were supported by grants from:
The Regional Scientific Council of Halland; the Framework of Positive Sci-entific Culture, Hospital of Halland, Halmstad; HRH Crown Princess Lovisa’s Foundation for Child Care, Stockholm; the HASNA Foundation, Halmstad; Uppsala University funds (ALF) and The Southern Healthcare Region common funds for development and research.

59
References
1. Grajeda R, Perez-Escamilla R, Dewey KG. Delayed clamping of the umbilical cord improves hematologic status of Guatemalan infants at 2 mo of age. Am. J. Clin. Nutr. 1997;65(2):425-31.
2. Geethanath RM, Ramji S, Thirupuram S, Rao YN. Effect of timing of cord clamping on the iron status of infants at 3 months. Indian Pediatr. 1997;34(2):103-6.
3. Linderkamp O. Placental transfusion: determinants and effects. Clin. Perinatol. 1982;9(3):559-92.
4. Oh W, Lind J. Venous and capillary hematocrit in newborn infants and placental transfusion. Acta Paediatr. Scand. 1966;55(1):38-48.
5. Oh W, Wallgren G, Hanson JS, Lind J. The effects of placental transfusion on respiratory mechanics of normal term newborn infants. Pediatrics 1967;40(1):6-12.
6. Yao AC, Hirvensalo M, Lind J. Placental transfusion-rate and uterine contraction. Lancet 1968;1(7539):380-3.
7. Yao AC, Lind J. Effect of gravity on placental transfusion. Lancet 1969;2(7619):505-8.
8. Yao AC, Moinian M, Lind J. Distribution of blood between infant and placenta after birth. Lancet 1969;2(7626):871-3.
9. Yao AC, Lind J. Blood flow in the umbilical vessels during the third stage of labor. Biol. Neonate 1974;25(3-4):186-93.
10. Farrar D, Airey R, Law GR, Tuffnell D, Cattle B, Duley L. Measuring placental transfusion for term births: weighing babies with cord intact. BJOG: An International Journal of Obstetrics & Gynaecology 2011;118(1):70-75.
11. Amer-Wåhlin I, Kjellmer I, Marsál K, Olofsson P, Rosén KG. Swedish randomized controlled trial of cardiotocography only versus cardiotocography plus ST analysis of fetal electrocardiogram revisited: analysis of data according to standard versus modified intention-to-treat principle. Acta Obstet. Gynecol. Scand. 2011;90(9):990-96.
12. Prendiville WJ, Harding JE, Elbourne DR, Stirrat GM. The Bristol third stage trial: active versus physiological management of third stage of labour. BMJ 1988;297(6659):1295-300.
13. Armstrong L, Stenson BJ. Use of umbilical cord blood gas analysis in the assessment of the newborn. Arch. Dis. Child. Fetal Neonatal Ed. 2007;92(6):F430-34.
14. McDonald SJ, Middleton P. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst. Rev. 2008:CD004074.

60
15. Begley CM, Gyte GM, Murphy DJ, Devane D, McDonald SJ, McGuire W. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst. Rev. 2010;7(7):CD007412.
16. Hutton EK, Hassan ES. Late vs Early Clamping of the Umbilical Cord in Full-term Neonates: Systematic Review and Meta-analysis of Controlled Trials. JAMA 2007;297(11):1241-52.
17. Lozoff B, Beard J, Connor J, Barbara F, Georgieff M, Schallert T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 2006;64(5 Pt 2):S34-43.
18. Ceriani Cernadas JM, Carroli G, Pellegrini L, Otano L, Ferreira M, Ricci C, et al. The effect of timing of cord clamping on neonatal venous hematocrit values and clinical outcome at term: a randomized, controlled trial. Pediatrics 2006;117(4):e779-86.
19. Chaparro CM, Neufeld LM, Tena Alavez G, Eguia-Liz Cedillo R, Dewey KG. Effect of timing of umbilical cord clamping on iron status in Mexican infants: a randomised controlled trial. Lancet 2006;367(9527):1997-2004.
20. Yao AC, Lind J, Vuorenkoski V. Expiratory grunting in the late clamped normal neonate. Pediatrics 1971;48(6):865-70.
21. Saigal S, Usher RH. Symptomatic neonatal plethora. Biol. Neonate 1977;32(1-2):62-72.
22. van Rheenen P, Brabin BJ. Late umbilical cord-clamping as an intervention for reducing iron deficiency anaemia in term infants in developing and industrialised countries: a systematic review. Ann. Trop. Paediatr. 2004;24(1):3-16.
23. Soltani H, Dickinson F, Symonds I. Placental cord drainage after spontaneous vaginal delivery as part of the management of the third stage of labour. Cochrane Database Syst. Rev. 2005(4):CD004665.
24. Budin P. A quel moment doit-on pratiquer la ligature du cordon ombilical? Progr. Med. (Paris) 1875;3:765.
25. Moss AJ, Monset-Couchard M. Placental transfusion: early versus late clamping of the umbilical cord. Pediatrics 1967;40(1):109-26.
26. Nelle M, Zilow EP, Kraus M, Bastert G, Linderkamp O. The effect of Leboyer delivery on blood viscosity and other hemorheologic parameters in term neonates. Am. J. Obstet. Gynecol. 1993;169(1):189-93.
27. Nelle M, Zilow EP, Bastert G, Linderkamp O. Effect of Leboyer childbirth on cardiac output, cerebral and gastrointestinal blood flow velocities in full-term neonates. Am. J. Perinatol. 1995;12(3):212-6.
28. Nelle M, Kraus M, Bastert G, Linderkamp O. Effects of Leboyer childbirth on left- and right systolic time intervals in healthy term neonates. J. Perinat. Med. 1996;24(5):513-20.
29. Gupta R, Ramji S. Effect of delayed cord clamping on iron stores in infants born to anemic mothers: a randomized controlled trial. Indian Pediatr. 2002;39(2):130-5.
30. van Rheenen P, de Moor L, Eschbach S, de Grooth H, Brabin B. Delayed cord clamping and haemoglobin levels in infancy: a randomised controlled trial in term babies. Trop. Med. Int. Health 2007;12(5):603-16.

61
31. Venâncio SI, Levy RB, Saldiva SRDM, Mondini L, Alves MCGP, Leung SL. Efeitos do clampeamento tardio do cordão umbilical sobre os níveis de hemoglobina e ferritina em lactentes aos três meses de vida. Cad. Saude Publica 2008;24:323-31.
32. Ceriani Cernadas JM, Carroli G, Pellegrini L, Ferreira M, Ricci C, Casas O, et al. Efecto del clampeo demorado del cordón umbilical en la ferritina sérica a los seis meses de vida: Estudio clínico controlado aleatorizado. Arch. Argent. Pediatr. 2010;108:201-08.
33. Male C, Persson LA, Freeman V, Guerra A, van't Hof MA, Haschke F. Prevalence of iron deficiency in 12-mo-old infants from 11 European areas and influence of dietary factors on iron status (Euro-Growth study). Acta Paediatr. 2001;90(5):492-98.
34. Looker AC, Dallman PR, Carroll MD, Gunter EW, Johnson CL. Prevalence of Iron Deficiency in the United States. JAMA 1997;277(12):973-76.
35. Baskett T. A flux of the reds: evolution of active management of the third stage of labour. JRSM 2000;93(9):489-93.
36. Dudley HW, Moir C. The substance responsible for the traditional clinical effect of ergot. BMJ 1935;1(3871):520-23.
37. Winter C, Macfarlane A, Deneux-Tharaux C, Zhang WH, Alexander S, Brocklehurst P, et al. Variations in policies for management of the third stage of labour and the immediate management of postpartum haemorrhage in Europe. BJOG 2007;114(7):845-54.
38. Festin MR, Lumbiganon P, Tolosa JE, Finney KA, Ba-Thike K, Chipato T, et al. International survey on variations in practice of the management of the third stage of labour. Bull. World Health Organ. 2003;81:286-91.
39. Prendiville WJ, Elbourne D, McDonald S. Active versus expectant management in the third stage of labour.[update in Cochrane Database Syst Rev. 2000;(3):CD000007; PMID: 10908457]. Cochrane Database Syst. Rev. 2000(2):CD000007.
40. Lalonde A, Daviss BA, Acosta A, Herschderfer K. Postpartum hemorrhage today: ICM/FIGO initiative 2004-2006. Int. J. Gynaecol. Obstet. 2006;94(3):243-53.
41. Begley CM. A comparison of ‘active’ and ‘physiological’ management of the third stage of labour. Midwifery 1990;6(1):3-17.
42. Khan GQ, John IS, Wani S, Doherty T, Sibai BM. Controlled cord traction versus minimal intervention techniques in delivery of the placenta: A randomized controlled trial. Am. J. Obstet. Gynecol. 1997;177(4):770-74.
43. Thilaganathan B, Cutner A, Latimer J, Beard R. Management of the third stage of labour in women at low risk of postpartum haemorrhage. European Journal of Obstetrics & Gynecology and Reproductive Biology 1993;48(1):19-22.
44. Rogers J, Wood J, McCandlish R, Ayers S, Truesdale A, Elbourne D. Active versus expectant management of third stage of labour: the Hinchingbrooke randomised controlled trial. The Lancet 1998;351(9104):693-99.
45. Nordström L, Waldenström U. Handläggning av normal förlossning. State of the Art (SOTA). Stockholm: Socialstyrelsen, 2001.

62
46. Intrapartum care - Care of healthy women and their babies during childbirth. CG55. London: NICE - National Institute for Health and Clinical Excellence 2007.
47. Wiklund I, Nordstrom L, Norman M. [Care program for umbilical cord clamping of newborn children]. Lakartidningen 2008;105(45):3208-10.
48. WHO. WHO recommendations for the prevention of postpartum haemorrhage. Geneva: World Health Organization, 2007.
49. Abalos E. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes: RHL commentary (last revised: 2 March 2009). The WHO Reproductive Health Library. Geneva: World Health Organization.
50. Leduc D, Senikas V, Lalonde AB, Ballerman C, Biringer A, Delaney M, et al. Active management of the third stage of labour: prevention and treatment of postpartum hemorrhage. J. Obstet. Gynaecol. Can. 2009;31(10):980-93.
51. Begley CM, Gyte GM, Devane D, McGuire W, Weeks A. Active versus expectant management for women in the third stage of labour. Cochrane Database Syst. Rev. 2011;11:CD007412.
52. Committee Opinion No. 543: Timing of Umbilical Cord Clamping After Birth. Obstet. Gynecol. 2012;120(6):1522-26 10.097/01.AOG.0000423817. 47165.48.
53. Farrar D, Tuffnell D, Airey R, Duley L. Care during the third stage of labour: A postal survey of UK midwives and obstetricians. BMC Pregnancy and Childbirth 2010;10(1):23.
54. Bimbashi A, Ndoni E, Dokle A, Duley L. Care during the third stage of labour: obstetricians views and practice in an Albanian maternity hospital. BMC Pregnancy and Childbirth 2010;10(1):4.
55. Vivio D, Fullerton JT, Forman R, Mbewe RK, Musumali M, Chewe PM. Integration of the Practice of Active Management of the Third Stage of Labor Within Training and Service Implementation Programming in Zambia. J. Midwifery Womens Health 2010;55(5):447-54.
56. Oladapo OT, Akinola OI, Fawole AO. Active management of third stage of labor: evidence versus practice. Acta Obstetricia & Gynecologica Scandinavica 2009;88(11):1252-61.
57. Perlman JM. Intrapartum Hypoxic-Ischemic Cerebral Injury and Subsequent Cerebral Palsy: Medicolegal Issues. Pediatrics 1997;99(6):851-59.
58. Westgate J, Garibaldi JM, Greene KR. Umbilical cord blood gas analysis at delivery: a time for quality data. BJOG 1994;101(12):1054-63.
59. Nordström L, Fogelstam K, Fridman G, Larsson A, Rydhström H. Routine oxytocin in the third stage of labour: a placebo controlled randomised trial. BJOG 1997;104(7):781-86.
60. Wiberg N, Källén K, Olofsson P. Delayed umbilical cord clamping at birth has effects on arterial and venous blood gases and lactate concentrations. BJOG 2008;115(6):697-703.
61. Kro GAB, Yli BM, Rasmussen S, Norèn H, Amer-Wåhlin I, Saugstad OD, et al. A new tool for the validation of umbilical cord acid–base data. BJOG 2010;117(12):1544-52.

63
62. Thomas DG, Grant SL, Aubuchon-Endsley NL. The Role of Iron in Neurocognitive Development. Developmental Neuropsychology 2009;34(2):196 - 222.
63. McCann JC, Ames BN. An overview of evidence for a causal relation between iron deficiency during development and deficits in cognitive or behavioral function. The American Journal of Clinical Nutrition 2007;85(4):931-45.
64. Grantham-McGregor S, Ani C. A Review of Studies on the Effect of Iron Deficiency on Cognitive Development in Children. The Journal of Nutrition 2001;131(2):649S-68S.
65. Szajewska H, Ruszczynski M, Chmielewska A. Effects of iron supplementation in nonanemic pregnant women, infants, and young children on the mental performance and psychomotor development of children: a systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2010;91(6):1684-90.
66. Sachdev H, Gera T, Nestel P. Effect of iron supplementation on mental and motor development in children: systematic review of randomised controlled trials. Public Health Nutr. 2005;8(2):117-32.
67. Berglund SK, Westrup B, Hägglöf B, Hernell O, Domellöf M. Effects of Iron Supplementation of LBW Infants on Cognition and Behavior at 3 Years. Pediatrics 2013;131(1):47-55.
68. Gunnarsson BS, Thorsdottir I, Palsson G, Gretarsson SJ. Iron status at 1 and 6 years versus developmental scores at 6 years in a well-nourished affluent population. Acta Pædiatrica 2007;96(3):391-95.
69. Konofal E, Lecendreux M, Arnulf I, Mouren M-C. Iron Deficiency in Children With Attention-Deficit/Hyperactivity Disorder. Arch. Pediatr. Adolesc. Med. 2004;158(12):1113-15.
70. Konofal E, Lecendreux M, Deron J, Marchand M, Cortese S, Zaïm M, et al. Effects of Iron Supplementation on Attention Deficit Hyperactivity Disorder in Children. Pediatr. Neurol. 2008;38(1):20-26.
71. Beard J. Recent evidence from human and animal studies regarding iron status and infant development. J. Nutr. 2007;137(2):524S-30S.
72. Lozoff B. Early Iron Deficiency Has Brain and Behavior Effects Consistent with Dopaminergic Dysfunction. The Journal of Nutrition 2011;141(4):740S-46S.
73. Lozoff B, Brittenham GM, Wolf AW, McClish DK, Kuhnert PM, Jimenez E, et al. Iron Deficiency Anemia and Iron Therapy Effects on Infant Developmental Test Performance. Pediatrics 1987;79(6):981-95.
74. Bramhagen AC, Axelsson I. Iron status of children in southern Sweden: effects of cow's milk and follow-on formula. Acta Pædiatrica 1999;88(12):1333-37.
75. Thane CW, Walmsley CM, Bates CJ, Prentice A, Cole TJ. Risk factors for poor iron status in British toddlers: further analysis of data from the National Diet and Nutrition Survey of children aged 1.5-4.5 years. Public Health Nutr. 2000;3(4):433-40.
76. Persson LA, Lundstrom M, Lonnerdal B, Hernell O. Are weaning foods causing impaired iron and zinc status in 1-year-old Swedish infants? A cohort study. Acta Paediatr. 1998;87(6):618-22.
77. Berglund S, Westrup B, Domellöf M. Iron Supplements Reduce the Risk of Iron Deficiency Anemia in Marginally Low Birth Weight Infants. Pediatrics 2010;126(4):e874-e83.

64
78. Dallman PR. Red blood cell values at various ages. In: Rudolph A, editor. Pediatrics. 16 ed. New York: Appleton-Centrury-Crofts, 1977:1111.
79. Domellöf M, Dewey KG, Lönnerdal B, Cohen RJ, Hernell O. The diagnostic criteria for iron deficiency in infants should be re-evaluated. J. Nutr. 2002;132:3680-86.
80. Dallman PR, Siimes MA, Stekel A. Iron deficiency in infancy and childhood. The American Journal of Clinical Nutrition 1980;33(1):86-118.
81. Saarinen UM, Siimes MA. Developmental changes in serum iron, total iron-binding capacity, and transferrin saturation in infancy. J. Pediatr. 1977;91(6):875-77.
82. Pappas A, Delaney-Black V. Differential diagnosis and management of polycythemia. Pediatr. Clin. North Am. 2004;51(4):1063-86.
83. Pfeiffer CM, Cook JD, Mei Z, Cogswell ME, Looker AC, Lacher DA. Evaluation of an automated soluble transferrin receptor (sTfR) assay on the Roche Hitachi analyzer and its comparison to two ELISA assays. Clin. Chim. Acta 2007;382(1-2):112-16.
84. Malope BI, MacPhail AP, Alberts M, Hiss DC. The ratio of serum transferrin receptor and serum ferritin in the diagnosis of iron status. Br. J. Haematol. 2001;115(1):84-89.
85. Cook JD, Flowers CH, Skikne BS. The quantitative assessment of body iron. Blood 2003;101(9):3359-63.
86. Squires J, Bricker D, Potter L. Revision of a Parent-Completed Developmental Screening Tool: Ages and Stages Questionnaires. J. Pediatr. Psychol. 1997;22(3):313-28.
87. Mei Z, Cogswell ME, Parvanta I, Lynch S, Beard JL, Stoltzfus RJ, et al. Hemoglobin and Ferritin Are Currently the Most Efficient Indicators of Population Response to Iron Interventions: an Analysis of Nine Randomized Controlled Trials. The Journal of Nutrition 2005;135(8):1974-80.
88. Domellof M, Cohen RJ, Dewey KG, Hernell O, Rivera LL, Lonnerdal B. Iron supplementation of breast-fed Honduran and Swedish infants from 4 to 9 months of age.[see comment]. J. Pediatr. 2001;138(5):679-87.
89. Hodges JL, Jr., Lehmann EL. Estimates of Location Based on Rank Tests. The Annals of Mathematical Statistics 1963;34(2):598-611.
90. Pezzullo JC. JavaStat - 2-way Contingency Table Analysis. 91. Tong S, Egan V, Griffin J, Wallace EM. Cord blood sampling at delivery: do we
need to always collect from both vessels? BJOG 2002;109(10):1175-77. 92. Hay W, Jr. Care of the Infant of the Diabetic Mother. Curr. Diab. Rep.
2012;12(1):4-15. 93. Halliday HL. Neonatal management and long-term sequelae. Best Pract. Res.
Clin. Obstet. Gynaecol. 2009;23(6):871-80. 94. Mercer JS. Current best evidence: a review of the literature on umbilical cord
clamping. J. Midwifery Womens Health 2001;46(6):402-14. 95. Emhamed MO, van Rheenen P, Brabin BJ. The early effects of delayed cord
clamping in term infants born to Libyan mothers. Trop. Doct. 2004;34(4):218-22.

65
96. Baker RD, Greer FR, The Committee on Nutrition. Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0-3 Years of Age). Pediatrics 2010;126(5):1040-50.
97. Ullrich C, Wu A, Armsby C, Rieber S, Wingerter S, Brugnara C, et al. Screening Healthy Infants for Iron Deficiency Using Reticulocyte Hemoglobin Content. JAMA 2005;294(8):924-30.
98. Axelsson I, Gebre-Medhin M, Hernell O, Jakobsonn I, Michaelsen KF, Samuelson G. [Recommendations for prevention of iron deficiency. Delay cow's milk intake as a beverage to infants until 10-12 months of age!]. Lakartidningen 1999;96(18):2206-8.
99. Mercer JS, Vohr BR, Erickson-Owens DA, Padbury JF, Oh W. Seven-month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping. J. Perinatol. 2010;30(1):11-16.
100. Henriksen C, Haugholt K, Lindgren M, Aurvag AK, Ronnestad A, Gronn M, et al. Improved Cognitive Development Among Preterm Infants Attributable to Early Supplementation of Human Milk With Docosahexaenoic Acid and Arachidonic Acid. Pediatrics 2008;121(6):1137-45.
101. Miltoft CB, Ekelund CK, Hansen BM, Lando A, Petersen OB, Skovbo P, et al. Increased nuchal translucency, normal karyotype and infant development. Ultrasound Obstet. Gynecol. 2012;39(1):28-33.
102. Domellof M, Lonnerdal B, Dewey KG, Cohen RJ, Rivera LL, Hernell O. Sex differences in iron status during infancy. Pediatrics 2002;110(3):545-52.
103. Rabe H, Diaz-Rossello JL, Duley L, Dowswell T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst. Rev. 2012;8:CD003248.
104. Mercer JS, Vohr BR, McGrath MM, Padbury JF, Wallach M, Oh W. Delayed cord clamping in very preterm infants reduces the incidence of intraventricular hemorrhage and late-onset sepsis: a randomized, controlled trial.[see comment]. Pediatrics 2006;117(4):1235-42.
105. Rabe H, Jewison A, Alvarez RF, Crook D, Stilton D, Bradley R, et al. Milking compared with delayed cord clamping to increase placental transfusion in preterm neonates: a randomized controlled trial. Obstet. Gynecol. 2011;117(2 Pt 1):205-11.
106. Hosono S, Mugishima H, Fujita H, Hosono A, Minato M, Okada T, et al. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks' gestation: a randomised controlled trial. Arch. Dis. Child. Fetal Neonatal Ed. 2008;93(1):F14-19.
107. Hosono S, Mugishima H, Fujita H, Hosono A, Okada T, Takahashi S, et al. Blood pressure and urine output during the first 72 hours in infants born less than 29 weeks' gestation related to umbilical cord milking. Arch. Dis. Child. Fetal Neonatal Ed. 2009:adc.2008.142935.
108. Tolosa JN, Park DH, Eve DJ, Klasko SK, Borlongan CV, Sanberg PR. Mankind's first natural stem cell transplant. J. Cell. Mol. Med. 2010;14(3):488-95.

66
109. Kaneko Y, Tajiri N, Su TP, Wang Y, Borlongan CV. Combination treatment of hypothermia and mesenchymal stromal cells amplifies neuroprotection in primary rat neurons exposed to hypoxic-ischemic-like injury in vitro: role of the opioid system. PLoS ONE 2012;7(10):e47583.
110. Mercer J, Erickson-Owens D, Skovgaard R. Cardiac asystole at birth: Is hypovolemic shock the cause? Med. Hypotheses 2009;72(4):458-63.
111. Brown N. Contradictions of value: between use and exchange in cord blood bioeconomy. Sociol. Health Illn. 2013;35(1):97-112.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 893
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine.
Distribution: publications.uu.seurn:nbn:se:uu:diva-198167
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2013